
Abstract
Objective
This study investigates the key factors influencing users’ intention to continue using telehealth platforms in Vietnam. Specifically, it examines the temporal relationships among hedonic value, utilitarian value, perceived privacy, perceived security, doctor–patient communication quality (DPCQ), trust, and continuance intention.
Methods
A longitudinal two-wave survey design was employed, with data collected from telehealth users at two time points (Time 1: N = 427; Time 2: N = 392). The Cross-Lagged Panel Model (CLPM) was applied to analyze causal and directional relationships among the study constructs over time.
Results
The findings indicate that hedonic value, utilitarian value, perceived privacy, perceived security, and doctor–patient communication quality at Time 1 all significantly predict user trust at Time 2. Trust, in turn, significantly influences users’ continuance intention toward telehealth services. The analysis confirms the temporal precedence of trust and highlights the crucial role of high-quality communication in fostering long-term engagement with telehealth platforms.
Conclusions
By integrating emotional, functional, and relational drivers within a validated longitudinal framework, this study advances the theoretical understanding of telehealth adoption and continuance behavior. The results provide practical implications for telehealth platform developers and healthcare providers seeking to strengthen user trust and sustain long-term engagement.
Introduction
Telehealth has emerged as a transformative advancement in digital healthcare, utilizing online technologies and interactive platforms to enable remote interactions between patients and medical professionals. Its adoption has grown significantly in recent years, with the COVID-19 pandemic serving as a major accelerant by highlighting the necessity for accessible, contactless, and scalable healthcare options. 1 While early telemedicine efforts were limited in functionality, current systems support real-time consultations, remote monitoring, and electronic prescriptions, reshaping the way healthcare is delivered. 2 Although definitions of telehealth may vary, it is commonly understood as the use of digital communication tools to facilitate healthcare delivery without requiring physical presence. 3 The rapid rise of telehealth has been driven by advances in digital infrastructure, growing patient familiarity with online services, and the need for continuous care amid public health disruptions. It also aligns with broader healthcare trends favoring convenience, personalization, and long-term patient engagement. 4 As both providers and patients increasingly embrace telehealth as a practical and sometimes preferred alternative to in-person care, researchers have turned their attention to understanding the psychological, technological, and behavioral factors that shape its adoption and sustained use.5,6 Importantly, recent digital health research increasingly conceptualizes telehealth not merely as a technological innovation, but as an integrated form of innovation that combines technological systems with organizational processes, professional practices, and relational mechanisms within healthcare delivery. 7 Understanding telehealth adoption, therefore, requires attention to both system-level capabilities and human-centric service interactions.
As of early 2023, Vietnam had approximately 77.93 million internet users and 70 million social media users, indicating a high level of digital engagement with the Internet and social platforms reaching over 79% and 71% of the population, respectively. 8 This digital momentum presents significant opportunities for expanding telehealth services nationwide. While the COVID-19 pandemic played a critical role in accelerating the adoption of remote healthcare solutions, especially in urban areas, challenges such as uneven access in rural regions, low trust, and varying levels of digital literacy still hinder widespread use. Although sectors like e-commerce and digital banking are well established, telehealth remains in its developmental phase, with limited provider adoption and ongoing concerns about privacy and system reliability. 9 Most existing research on telehealth intentions stems from international contexts, 5 and few studies address the Vietnamese healthcare environment. Given the country's unique cultural and technological landscape, it is essential to investigate context-specific factors that shape user trust, perceptions of security and privacy, perceived value, and willingness to adopt telehealth platforms. Moreover, as emerging healthcare systems increasingly incorporate data-driven and intelligent technologies, including machine learning–enabled analytics for diagnosis, triage, and decision support, 10 understanding patient trust and behavioral acceptance becomes a critical complement to algorithm-focused healthcare analytics research.
Understanding patient behavior in the telehealth context is increasingly essential for healthcare providers aiming to improve service delivery and foster long-term engagement, particularly in digitally advancing countries like Vietnam. Various theoretical models have been used to explain users’ acceptance of digital health technologies, with the TAM and the UTAUT frequently applied to highlight the roles of perceived usefulness and ease of use. 11 In addition to these technology-driven models, social science perspectives such as trust transfer theory and social learning theory emphasize the influence of peer interactions and social norms on behavioral intention. 12 Psychological frameworks like the TPB and the TRA also underscore the importance of beliefs and attitudes in shaping health-related behaviors. 13 Among these, the S–O–R model offers a particularly comprehensive approach, explaining how external factors such as system features and communication quality impact users’ internal responses—such as trust and perceived value—which in turn affect their intention to adopt telehealth services. 14 By adopting this perspective, telehealth can be viewed as a socio-technical system in which technological stimuli and organizational communication practices jointly shape patients’ psychological evaluations and behavioral outcomes.
Table 1 highlights previous research related to digital health platforms and the range of theoretical models applied to explain factors influencing patients’ behavior toward telehealth services. Several studies have investigated user behavior in connection with virtual healthcare platforms and online health communities. 15 Notably, some findings suggest that patients often express low levels of trust in telehealth systems, which may reduce their willingness to engage with or continue using such services. 16 A decline in user confidence can hinder the growth of telehealth by discouraging appointment bookings and digital consultations. This concern is particularly relevant in health contexts, where limited interaction and a lack of transparent medical information can result in uncertainty and poor decision-making. To address this gap, the present study investigates the critical roles of perceived privacy and perceived security in shaping patient trust and their usage intention toward telehealth services—two factors that are increasingly important in the digital transformation of healthcare delivery. 17 This focus responds to recent calls in digital healthcare and analytics literature to complement system performance and algorithmic capability with user-centric perspectives on trust, ethics, and organizational transparency.18,19
Prior research on telehealth adoption.

Moreover, prior research confirms that using digital platforms such as telehealth can deliver both utilitarian and hedonic value to users. 31 In the context of virtual healthcare, hedonic value refers to the emotional and psychological satisfaction patients experience, such as comfort, reassurance, or reduced stress during remote consultations. In contrast, utilitarian value reflects the practical benefits of telehealth, including time savings, immediate access to care, and convenience, emphasizing rational, task-focused outcomes. 32 While hedonic value is rooted in the user's experiential enjoyment, utilitarian value centers on efficiency and effectiveness in achieving health-related goals. Many scholars have highlighted the need to explore how these value perceptions influence outcomes like trust and behavioral intention, especially in digital health contexts. 33
Additionally, a critical yet often overlooked factor in telehealth success is perceived doctor–patient communication quality, which captures the extent to which patients feel heard, understood, and supported during remote interactions. 34 High-quality communication fosters trust and positively influences patients’ willingness to continue using telehealth services. Despite increasing adoption, there is still a gap in understanding how these combined factors, value perceptions, privacy and security concerns, communication quality, and trust, jointly shape telehealth usage behavior. Therefore, this study investigates their roles in influencing trust and usage intention toward telehealth services over time. Specifically, this research addresses the following questions: (1) What are the effects of perceived service values, perceived security, and doctor–patient communication quality on patients’ usage intention toward telehealth services? (2) Does trust in the telehealth platform mediate the relationships among perceived service values, perceived security, communication quality, and usage intention? (3) How do the relationships among these factors (value dimensions, privacy/security, communication quality, trust, and usage intention) hold up over time when analyzed using the cross-lagged panel method (CLPM) with longitudinal data?
This study contributes to the existing body of literature in several important ways. First, it offers an in-depth examination of how perceived service values, perceived security, and doctor–patient communication quality influence patient trust and usage intention toward telehealth services. Additionally, it explores the mediating role of trust in linking these key predictors to behavioral intention within the telehealth context. By addressing these relationships, the study responds to previous scholarly calls for a deeper understanding of how privacy and security concerns affect trust and usage behavior in digital health platforms. 35 More broadly, this study positions telehealth adoption as an integrated innovation process that connects technological advancement, organizational communication, and patient-centered service experience. A further contribution lies in the application of the CLPM to assess the temporal and causal relationships among these variables. While most prior studies in this area have relied on cross-sectional data and descriptive insights,5,6 this research utilizes CLPM to capture how these factors impact trust and usage intention over time. The empirical data comprises two waves collected from telehealth users in Vietnam during 2023 (T1) and 2024 (T2), allowing for a robust longitudinal analysis. The remainder of this paper is organized as follows: Section “Theoretical background” presents the literature review and theoretical background; Section “Hypotheses development and conceptual model” outlines the conceptual framework and research hypotheses; Section “Method” describes the research methodology; Section “Results” reports the results; Section “Discussion and implications” discusses the findings and their implications; and Section “Limitations and future research directions” addresses the study's limitations and proposes directions for future research.
Theoretical background
Telehealth services
Although there is no universally standardized definition, telehealth generally refers to the integration of digital technologies—such as mobile applications, video conferencing, and web-based platforms—into healthcare delivery to facilitate remote consultations, diagnoses, and treatments. 36 Telehealth services can typically be categorized into two major forms. The first involves healthcare providers leveraging general digital communication platforms (e.g., Zoom, WhatsApp, or SMS) to offer medical consultations and support. The second includes dedicated telemedicine platforms that incorporate features like appointment booking, electronic prescriptions, patient feedback, and interactive chat functions. Compared to traditional in-person healthcare, telehealth introduces two distinctive elements. 37 First, it integrates communication technologies that promote personalized, real-time interaction between patients and medical professionals, often using familiar interfaces that resemble everyday digital tools. Second, rather than relying exclusively on face-to-face clinical structures, telehealth emphasizes technology-driven engagement, encouraging patients to share their health experiences, seek peer advice in virtual communities, and build trust through transparent, continuous doctor–patient communication. 38
From the perspective of patient empowerment, understanding behavioral intentions toward telehealth services has become increasingly important for healthcare providers aiming to enhance patient engagement and utilize the potential of digital communication technologies. 5 Numerous theoretical models have been applied to explain the factors that drive successful telehealth adoption from a behavioral standpoint. 21 However, despite the widespread use of these frameworks, findings across studies often reveal inconsistencies. Among the most frequently employed models is the TAM, which posits that a patient's usage intention toward telehealth is largely influenced by their attitude, shaped by perceived ease of use and usefulness—two key features of telehealth systems. 39 In addition, motivation theory has also gained traction in digital health research, suggesting that patients’ intention to adopt telehealth is influenced by both utilitarian motivations (e.g., efficiency, convenience) and hedonic motivations (e.g., emotional relief, comfort). 40 These insights underscore the need to consider both functional and emotional factors when investigating telehealth acceptance and usage.
In the context of telehealth, researchers have drawn from marketing and information systems literature to propose models that deepen our understanding of digital health behavior. For instance, Hong, Deng 41 introduced a framework showing how key system features influence patients’ trust and their usage intention toward healthcare platforms. Elements such as peer feedback, referrals, and virtual health communities were found to significantly shape user perceptions and decision-making. 42 To offer a more integrated perspective, several studies have adopted the S–O–R model, originally rooted in psychology, to examine how system stimuli—such as platform usability, interactive guidance, credibility of information, and service visibility—affect internal responses like patient trust, perceived value, and emotional experience, which in turn impact behavioral outcomes like usage intention toward, sustained engagement, or adherence to teleconsultations. 43 Building on this foundation, our study employs the lens of utilitarian and hedonic motivations to explore how these values influence perceived doctor–patient communication quality, trust, and ultimately, patients’ intention to adopt telehealth services.
Utilitarian/hedonic value
Motivation theory has been increasingly recognized as a foundational lens in understanding digital consumer behavior, including in the telehealth context. 5 Consumer value in digital services can be categorized into two core types: utilitarian value and hedonic value. The former is associated with goal-oriented and efficient experiences, while the latter emphasizes emotional gratification and experiential satisfaction. 44 Although hedonic motivations have been shown to influence impulsive behaviors more strongly than utilitarian ones in traditional retail environments, both play important roles in digital service engagement. 45
In the context of telehealth, utilitarian value stems from practical benefits such as time savings, ease of appointment scheduling, quick access to professional advice, and streamlined information retrieval. These features appeal to users seeking efficiency and effectiveness in healthcare delivery. Conversely, hedonic value may arise from emotionally positive experiences such as feeling reassured during a consultation, enjoying the comfort of receiving care from home, or experiencing satisfaction from personalized interactions and visual interfaces. 46
While prior research has extensively examined these motivational dimensions in brick-and-mortar stores and e-commerce settings, 45 recent studies suggest that they are equally relevant in technology-enabled healthcare services like telemedicine. 29 Importantly, the impact of these values may differ across demographic and cultural contexts. Building on this foundation, the present study investigates how both utilitarian and hedonic values influence patients’ trust in telehealth platforms and their intention to continue using such services.
Perceived security and privacy in telehealth platforms
A growing body of research highlights critical ethical concerns in digital service environments, particularly regarding privacy, security, data reliability, and potential misuse. 47 In the context of telehealth, patients may face risks such as unauthorized access to sensitive health records, fraudulent medical advice, or unethical data handling practices. Despite the convenience and innovation of remote medical services, users often remain wary of how their personally identifiable information—including medical history, prescriptions, or biometric data—may be collected, monitored, and exploited. 48 This has prompted heightened attention to the dual importance of information privacy and platform security.
As telehealth platforms evolve from basic communication tools into integrated systems for diagnosis, treatment, and digital prescriptions, there is an urgent need to fortify both technological safeguards and data governance policies. These platforms must protect users not only from cyber threats but also from deceptive practices, such as manipulated patient reviews or biased health recommendations. Widespread concerns over past data breaches and unethical use of patient information, particularly on large digital platforms, 49 have intensified skepticism about the integrity of online health services. Ethical dilemmas arise when patient data—such as consultation records or symptom logs—are repurposed for targeted advertising, algorithmic profiling, or unauthorized third-party analysis.
Although telehealth offers vital benefits, including access to online support groups and remote consultations, many users hesitate to fully engage due to perceived privacy risks. Patients often find themselves in a trade-off between receiving digital care and safeguarding their medical data. 50 Effective telehealth systems must implement comprehensive security protocols, encompassing encrypted transactions, secure data storage, access control, and compliance with health data regulations. According to Belfrage, Helgesson, 35 privacy protection is unattainable without a robust security infrastructure, yet security alone does not guarantee full privacy unless trust is also established. Therefore, this study aims to examine how patients’ perceptions of privacy and security influence their trust in telehealth services, and how this trust, in turn, affects their usage intention toward or recommend such services.
Perceived doctor–patient communication quality in telehealth platforms
In telehealth environments, the quality of communication between doctors and patients plays a crucial role in shaping user trust, satisfaction, and subsequent behavioral intentions. As digital consultations replace traditional face-to-face encounters, effective communication becomes a central determinant of care quality and perceived service legitimacy. 51 Perceived doctor–patient communication quality (PDPCQ) refers to the patient's evaluation of how empathetically and effectively a healthcare provider conveys medical information, listens to concerns, and engages in shared decision-making, regardless of whether the interaction is virtual or in-person.
Unlike physical consultations, telehealth interactions may face barriers such as reduced nonverbal cues, technological disruptions, and limited relational warmth, all of which can impair patient understanding and emotional connection. 52 Inadequate communication in teleconsultations may result in confusion about treatment plans, diminished trust in professional competence, and reluctance to follow medical advice. Conversely, high-quality digital communication—characterized by attentiveness, clarity, responsiveness, and personalized interaction—can enhance patients’ sense of being heard and respected, thereby promoting stronger trust in both the provider and the telehealth system.
Effective communication is particularly essential in sensitive healthcare contexts, such as mental health counseling, chronic disease management, or post-operative care, where patients expect not only technical expertise but also emotional support and reassurance. 53 Research shows that positive perceptions of provider communication are strongly linked to increased treatment adherence, satisfaction, and ongoing engagement with digital health services. 54 Moreover, in culturally nuanced settings like Vietnam, where interpersonal warmth and respect for authority influence healthcare interactions, the quality of doctor–patient communication may significantly moderate trust development and usage behavior.
Given these considerations, this study incorporates perceived DPCQ as a key construct influencing patient trust and usage intention toward telehealth services. It also explores whether DPCQ mediates or strengthens the effects of other influencing factors—such as perceived value, privacy, or service usefulness—on patients’ behavioral outcomes. In the digital healthcare era, fostering meaningful and transparent communication is not merely an operational challenge but a strategic imperative for building enduring relationships with users.
Customer trust in telehealth platforms
In virtual healthcare environments, where direct, face-to-face interactions are absent, patients often experience heightened uncertainty and perceived risks, especially concerning clinical accuracy, data protection, and the legitimacy of remote services. This makes trust a pivotal determinant in patient decision-making and engagement with telehealth platforms. 55 From the perspective of relationship marketing, trust serves as the foundation for establishing and maintaining successful relationships. 56 It is broadly defined as a patient's belief in the reliability, integrity, and competence of their healthcare provider or digital health service.
In the context of telehealth, especially in regions like Vietnam where the adoption of digital medical services is still emerging, trust becomes even more critical. Patients must often rely on limited cues—such as platform reputation, provider communication style, and system reliability—to form judgments about the trustworthiness of virtual healthcare. 57 To better understand how trust operates in this setting, prior research has proposed multidimensional frameworks. For instance, there are three key components of trust: competence (the perceived ability of the provider to deliver quality care), integrity (adherence to ethical and professional norms), and benevolence (the belief that the provider prioritizes the patient's interests). 58
As telehealth involves both technological and human elements, trust can be influenced by multiple sources, including the healthcare provider, the platform itself, and even peer reviews or system features. Building on socio-technical theory, trust is categorized into domains such as trust in medical platforms, trust in system interfaces, trust in provider–patient interactions, and trust in peer-generated health information. 59 Moreover, trust in teleconsultation services is often defined as a patient's willingness to depend on medical guidance delivered via digital platforms, despite not having in-person verification or physical presence. 43
Research suggests that low trust in online healthcare services can significantly reduce user participation and willingness to follow digital medical advice. 60 Patients may hesitate to book appointments or share sensitive health data if they suspect providers of lacking professionalism, transparency, or ethical rigor. This hesitancy is intensified by the presence of user-generated health content, some of which may be inaccurate, sponsored, or misleading. 61 When patients are unable to verify such information or perceive bias in virtual endorsements or testimonials, their trust may erode.
Furthermore, several studies have conceptualized trust as either unidimensional (focusing solely on credibility) or multidimensional, including aspects such as credibility, benevolence, and integrity. 62 These dimensions are particularly relevant in digital healthcare, where patients are expected to place faith not only in the provider's clinical expertise but also in their ethical commitment and digital communication. In line with this, the present study investigates how trust mediates the relationships between hedonic and utilitarian value, privacy/security perceptions, and communication quality, and its role in shaping patients’ intention to continue using telehealth services.
Hypotheses development and conceptual model
Building upon the utilitarian and hedonic value perspective 33 and prior research on digital healthcare and telehealth adoption,5,6 this study develops an integrated model to explore the factors that influence patients’ usage intention toward telehealth services. As shown in Figure 1, perceived service values, perceived privacy/security, and perceived DPCQ are proposed as key antecedents of patient trust in telehealth platforms. In turn, this trust is expected to significantly affect patients’ intention to adopt telehealth services.

Conceptual model.
Perceived service values, doctor–patient communication, trust, and usage intention
Existing literature has affirmed that both hedonic and utilitarian motivations play a crucial role in shaping users’ behavioral intentions in technology-driven environments. For example, Sagala and Sumiyana (2020) found that incorporating both values into digital platforms enhances user satisfaction and platform sustainability. In healthcare contexts, hedonic value may stem from the emotional comfort, reduced anxiety, or satisfaction patients feel when using convenient, tech-enabled consultations, while utilitarian value reflects the practical benefits such as time savings, accessibility, and accurate information. Prior studies (Chen et al., 2017; Akram et al., 2021) confirm that both dimensions can positively influence trust and the likelihood of engaging with digital health services.
In addition, perceived doctor–patient communication quality has emerged as a crucial factor in virtual healthcare delivery. High-quality communication—marked by empathy, clarity, responsiveness, and shared decision-making—can foster trust in the physician and the platform as a whole (Zhao et al., 2023). Patients who perceive their interactions with online doctors as personalized and effective are more likely to trust the system and continue using it.
Prior research has also highlighted that trust in the provider or platform is essential for reducing uncertainty and promoting adoption, especially in the absence of physical interaction (Lee, 2016; Sharma et al., 2019). Trust is a multidimensional concept involving competence, integrity, and benevolence (Chen & Dhillon, 2003), and these dimensions are particularly salient in telehealth, where patients must rely on virtual consultations and data-driven diagnostics. Therefore, patients’ perceived service values, privacy concerns, and communication experiences can shape their trust and usage decisions.
Thus, we propose the following hypotheses: H1: Hedonic value positively influences patients’ trust in telehealth platforms. H2: Hedonic value positively influences patients’ usage intention toward telehealth services. H3: Utilitarian value positively influences patients’ trust in telehealth platforms. H4: Utilitarian value positively influences patients’ usage intention toward telehealth services. H5: Perceived doctor–patient communication quality positively influences patients’ trust in telehealth platforms. H6: Perceived doctor–patient communication quality positively influences patients’ usage intention toward telehealth services.
Perceived privacy and security in telehealth, patient trust, and usage intention
Concerns surrounding privacy and security have long been central topics in healthcare marketing ethics. 48 In particular, digital health platforms—including telehealth systems—have drawn increasing scrutiny due to patients’ apprehension about the safety and confidentiality of their personal information. 63 Perceived security in this context refers to patients’ confidence in the telehealth platform's ability to protect their data and ensure safe digital interactions. Given the growing anxiety about potential data breaches and unauthorized access, it is important to understand how patients form security-related judgments when using telehealth services. 64
Patients’ perceptions of security reflect their sense of control over how their medical information is stored and shared. 65 When patients believe that a healthcare platform is secure and trustworthy, they are more likely to continue using its services, rely on digital consultations, and disclose sensitive information. As noted by Belfrage, Helgesson, 35 trust in digital health services is shaped by perceptions of safety, credibility, and technological protection. Previous studies 17 have typically evaluated perceived security from a technical standpoint, such as encryption, authentication, and secure login, but recent research emphasizes a broader understanding that includes emotional safety and confidence in system integrity. 52
Similarly, perceived privacy involves patients’ beliefs about how their health data is collected, accessed, and used by telehealth platforms.
50
It reflects the extent to which patients feel in control of their personal information. Clear communication of privacy policies, use of privacy seals, and user-friendly data control settings all contribute to building this perception.
9
When patients are assured that their private health information is protected and handled ethically, it fosters a sense of trust and increases their willingness to engage in telehealth consultations.
63
Recent findings have shown that privacy and security concerns significantly shape patients’ trust and behavioral intentions in using telehealth services.
35
Therefore, the following hypotheses are proposed: H7: Perceived privacy positively influences patients’ trust in telehealth platforms. H8: Perceived privacy positively influences patients’ usage intention toward telehealth services. H9: Perceived security positively influences patients’ trust in telehealth platforms. H10: Perceived security positively influences patients’ usage intention toward telehealth services.
Patient trust in telehealth platforms and usage intentions
Prior research has consistently shown that patient trust is a pivotal determinant of intention to adopt and continue using telehealth services. For instance, Liu, Wang 55 demonstrated that patient trust in digital healthcare platforms is a significant predictor of service usage intention. Multiple studies have emphasized that trust plays a foundational role in the successful delivery and acceptance of telehealth and other digital health services. 6 Yingngam, Khumsikiew 40 confirmed that trust exerts a stronger influence on usage intention compared to many other determinants in digital health environments.
Further, both trust and perceived credibility substantially enhance patient satisfaction and their willingness to engage in digital consultations. 60 Similarly, Liu, Wang 55 support the notion that trust directly influences patients’ intention to continue using telehealth services over time. Additional findings suggest that critical trust-building elements—such as provider reputation, information accuracy, and perceived safety of data transmission—positively shape patients’ readiness to use these services. 66 These insights are consistent with broader digital healthcare research, which highlights how trust reduces perceived risk, strengthens confidence in service providers, and encourages sustained patient engagement. 67
Given this evidence, it is clear that patient trust serves as a central mechanism influencing telehealth usage behavior. Therefore, we hypothesize: H11: Patients’ trust in telehealth platforms positively influences usage intention.
Therefore, the conceptual model is proposed (Figure 1):
Longitudinal research
Most existing studies on telehealth adoption have relied on cross-sectional data, capturing user perceptions at a single point in time.5,37 While such designs provide valuable insight into relationships among constructs such as utilitarian and hedonic value, perceived privacy and security, doctor–patient communication quality, trust, and usage intention toward telehealth services, they fall short in capturing how these factors evolve with continued use. Given the dynamic nature of digital healthcare experiences, particularly in contexts where ongoing interaction and communication are central, a longitudinal approach becomes essential. Importantly, cross-sectional designs are limited in their ability to assess temporal directionality and may suffer from reverse-causality concerns, 68 especially when examining trust formation and continuance intention in digital health contexts.
In telehealth settings, constructs like DPCQ are not static; their influence tends to accumulate through repeated interactions, shaping user trust and behavioral intentions over time. As patients gain more experience with virtual consultations, their perceptions of communication quality, system reliability, and privacy protection may shift, potentially reinforcing or weakening their intention to continue using telehealth services. Studies have emphasized the importance of time-series data in understanding such behavioral trajectories. 69 A longitudinal design allows these experiential learning effects to be empirically captured rather than inferred from single-wave perceptions.
Cross-sectional data may overstate or understate the immediate impact of telehealth value propositions or security features, ignoring the time needed for trust to form or communication norms to solidify. Longitudinal analyses, by contrast, enable researchers to trace how trust in telehealth providers, shaped by privacy/security perceptions, functional value, and communication quality at time 1, translates into usage behavior at time 2. This perspective is particularly valuable in telehealth, where adoption may not occur instantly but builds gradually through positive, consistent service experiences. Accordingly, a two-wave panel design with a one-year interval was adopted to balance theoretical relevance and practical feasibility, allowing sufficient time for perceptual and behavioral changes to emerge while minimizing sample attrition. Therefore, our study advocates for future research to adopt longitudinal designs to better capture the evolving impact of telehealth service features on trust and sustained adoption behavior.
Method
Data collection and procedure
To explore the factors influencing patients’ adoption of telehealth services, we designed a structured questionnaire based on well-established measures from previous studies in the fields of digital health and online service usage. The questionnaire was developed in Vietnamese, pre-tested, and refined to ensure clarity and cultural relevance.
The study protocol was reviewed and approved by the Institutional Review Board (IRB) of Ho Chi Minh City University of Economics and Finance under approval number 720/QD-UEF. All procedures involving human participants complied with the ethical standards of this committee and with the 1964 Declaration of Helsinki and its later amendments. Written informed consent was obtained from all participants before study initiation. For online participants, informed consent was obtained electronically through the survey platform, where respondents were required to read the consent statement and provide explicit agreement before accessing the questionnaire. For offline participants, written informed consent was collected in paper form before completing the survey. No waiver of written informed consent was requested or granted by the IRB. Participation was entirely voluntary, and no personal identifying information was collected. All responses were treated confidentially and used solely for academic research purposes.
Data were collected through self-administered surveys distributed both online and offline. Participants were recruited through university networks, local health forums, and public health centers across Ho Chi Minh City and nearby provinces. A non-probability purposive sampling methodology was employed, targeting individuals with prior experience using telehealth services, which was appropriate given the study's focus on experienced users and its longitudinal panel design. The inclusion criteria required participants to (1) be at least 18 years old and (2) have used telehealth services—such as online doctor consultations, e-prescriptions, or virtual follow-ups—at least once in the past six months. Exclusion criteria included respondents with no prior telehealth experience and those who provided incomplete or inconsistent survey responses.
A two-wave longitudinal design was employed. The first wave of data collection (T1) was conducted in April 2024, during which a total of 427 valid responses were collected after removing eight incomplete entries. One year later, in April 2025 (T2), we followed up with the same participants, receiving 399 matched responses. After eliminating seven records due to missing or inconsistent answers, 392 complete cases were retained for final analysis. The one-year interval was selected to allow sufficient time for changes in trust, communication experiences, and continuance intention to materialize, while maintaining panel stability and response consistency.
Table 2 presents the demographic profile of the sample. Most respondents were female (55%), held a university degree (60%), and reported using telehealth services at least once every two months (47%). Before the main survey, a pilot test with 30 users was conducted. Based on their feedback, minor adjustments were made to improve question wording and contextual fit.
Participant demographics.

Measurement instruments
To ensure content validity and reliability, this study employed measurement scales adapted from previously validated research in the fields of digital health and online service adoption. Specifically, utilitarian value and hedonic value were each assessed using three items adapted from Vayghan, Baloglu, 70 revised to reflect the context of telehealth service usage.
Perceived privacy and perceived security were measured using three and two items, respectively, adapted from Salah and Ayyash, 71 focusing on users’ perceptions of data protection and safety within telehealth platforms. Customer trust in telehealth services was measured with three items adapted from Dhagarra, Goswami, 72 reflecting confidence in the service providers and system integrity.
The construct of usage intention was replaced with intention to continue using telehealth services, measured using three items revised from Pham Thi and Duong 73 to align with the healthcare context. Additionally, doctor–patient communication quality was assessed using four items adapted from Zheng, Jiang, 34 emphasizing clarity, responsiveness, and empathy in remote consultations.
This study is purely quantitative in nature and did not involve open-ended questions, interviews, or qualitative thematic coding. All constructs were operationalized using structured, multi-item Likert-scale measures adapted from prior validated studies. All items were measured using a seven-point Likert scale ranging from 1 (“strongly disagree”) to 7 (“strongly agree”).
Common method variance (CMV)
To mitigate the risk of CMV, this study adopted both procedural and statistical remedies. 74 Procedurally, the questionnaire was carefully designed by organizing items into separate sections for each construct and using different scale anchors for independent and dependent variables. Anonymity was assured to reduce evaluation apprehension and socially desirable responses. 75
Post hoc, we applied the marker variable technique by incorporating two theoretically unrelated items. The correlation coefficients between the marker variable and the study constructs were low and statistically non-significant (ranging from −0.276 to 0.042; P > .05), indicating that CMV was unlikely to bias the results.
Additionally, non-response bias was tested by comparing early and late respondents based on the timing of survey submission. 76 An independent-samples t-test revealed no significant differences in the mean scores of key variables between the two groups, suggesting that non-response bias was not a serious issue in our dataset.
Sample representativeness
The demographic characteristics (Table 2) are consistent with the profile of current telehealth users in Vietnam, as indicated by recent digital health reports and government health statistics. Specifically, national reports highlight that telehealth users in Vietnam are predominantly younger and middle-aged adults with relatively high levels of digital literacy, smartphone usage, and internet access, particularly in urban areas such as Ho Chi Minh City.77,78 In addition, national statistics indicate that individuals with higher education levels and frequent internet use are more likely to engage with e-health and telemedicine services. 79 Furthermore, our sample aligns with participant profiles commonly used in telehealth adoption research, 6 which often include younger adults and individuals with moderate-to-high digital literacy.
The final sample size for Time 1 (n = 427) and Time 2 (n = 392) satisfies the minimum sample size criteria suggested for structural equation modeling. Specifically, it exceeds the commonly accepted guideline of having at least 10 cases per estimated parameter or most complex construct in the model (Hair et al., 2010). The relatively low attrition rate between Time 1 and Time 2 further supports the stability and adequacy of the longitudinal sample. The KMO measure of sampling adequacy was 0.812, well above the acceptable threshold of 0.60, indicating that the sample was suitable for factor analysis. Additionally, Bartlett's test of sphericity was significant (χ2 = 1287.46, P < .001), supporting the appropriateness of applying data reduction techniques such as structural equation modeling for our analysis.
Results
This study utilized the PLS-SEM technique to assess the proposed research model and hypotheses. We applied WarpPLS version 7.0 to examine both the measurement and structural models. As emphasized by Hair Jr, Hult, 80 PLS-SEM is well-suited for evaluating predictive models, especially when dealing with complex mediation effects and longitudinal data structures.
Given our moderate sample sizes at Time 1 (n = 427) and Time 2 (n = 392), PLS-SEM was preferred over covariance-based SEM due to its robustness in handling smaller datasets, non-normal data distributions, and multicollinearity. This methodological choice aligns well with the longitudinal and exploratory nature of our telehealth adoption study.
Following Chin and Marcoulides, 81 the application of PLS-SEM is justified when the research involves prediction, multiple latent constructs, and moderate sample sizes. In our model, all seven latent variables—including the newly added construct of doctor–patient communication quality—demonstrated satisfactory indicator loadings exceeding 0.75. Moreover, all inter-construct correlations met the minimum acceptable threshold (r ≥ 0.10), supporting the model's validity and predictive strength. 80
Measurement model
This study adopted the recommended two-stage approach to PLS-SEM. 82 In the first phase, we conducted a CFA to evaluate the psychometric robustness of the constructs across both data collection phases (Time 1 and Time 2). The CFA allowed us to assess the constructs’ reliability, convergent validity, and discriminant validity, as shown in Table 3.
Cronbach's alpha, CR, AVE.
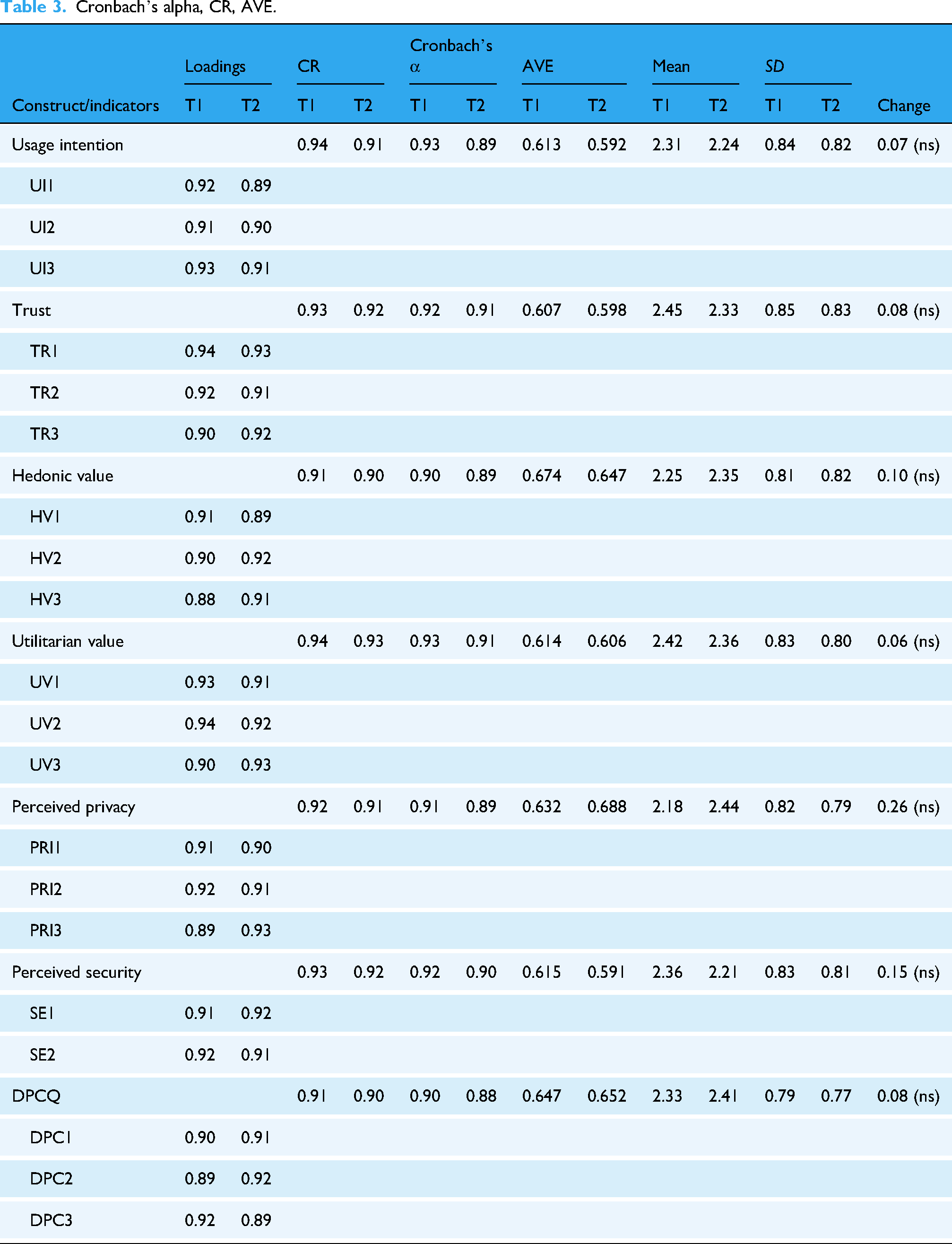
The results from Table 3 demonstrate strong item loadings on their respective latent variables at both Time 1 and Time 2, confirming convergent validity. All factor loadings exceeded the acceptable threshold of 0.70 and were statistically significant. Moreover, the cross-loadings on unrelated constructs were low and nonsignificant, indicating good discriminant validity. Composite reliability values for all constructs—including the newly added variable of doctor–patient communication quality—were above 0.70, affirming internal consistency and reliability. 83
To further confirm model adequacy, we checked full collinearity variance inflation factor values, which ranged from 1.013 to 2.069, all below the critical threshold of 3.3, 80 indicating that multicollinearity was not a concern. Table 4 presents the inter-construct correlations and the square roots of the AVE. In each case, the square root of the AVE exceeded the inter-construct correlations, confirming satisfactory discriminant validity.
Discriminant validity.

UI: usage intention, TR: trust, HV: hedonic value, UV: utilitarian value, PRI: perceived privacy, SE: perceived security.
Lastly, a comparison of mean scores across the two time points revealed a modest decline in the average scores of several constructs from Time 1 to Time 2, suggesting evolving user perceptions in the context of telehealth adoption.
CLPM
In the second stage of our PLS-SEM approach, we evaluated the predictive validity of the structural model by testing the hypothesized relationships (H1–H9) using a CLPM. This technique is widely used in longitudinal research to assess the directional and causal relationships between variables across multiple time points. 84 By applying the CLPM, we were able to examine how constructs such as perceived privacy, perceived security, doctor–patient communication quality, user trust, and telehealth usage intention influence one another over time.
This modeling approach allowed us to test whether changes in a variable measured at Time 1 (e.g., privacy_T1) significantly predicted the corresponding outcome variable at Time 2 (e.g., TR_T2), while also controlling for the autoregressive effects of the variable itself (e.g., TR_T1 → TR_T2). Following Martens and Haase, 85 we assessed temporal precedence by comparing the strength and significance of the forward paths (e.g., PRI_T1 → TR_T2) against potential reverse causality (e.g., TR_T1 → PRI_T2).
To satisfy CLPM assumptions, we ensured synchronicity by measuring all key constructs—including hedonic motivation (HV), utilitarian motivation (UV), perceived privacy (PRI), perceived security (SE), doctor–patient communication quality (DPC), user trust (TR), and telehealth usage intention (UI)—simultaneously at both time points (T1 and T2). The stationarity assumption was tested to confirm that the structural relationships among variables remained stable across both phases. Additionally, stability was confirmed by the presence of significant autoregressive paths (e.g., PRI_T1 → PRI_T2), indicating consistent patterns over time. 86
The results of the CLPM analysis are summarized in Table 5, which illustrates the forward and reverse path coefficients, providing empirical evidence for the hypothesized directional influences among key constructs in the telehealth context.
Longitudinal PLS-SEM results.
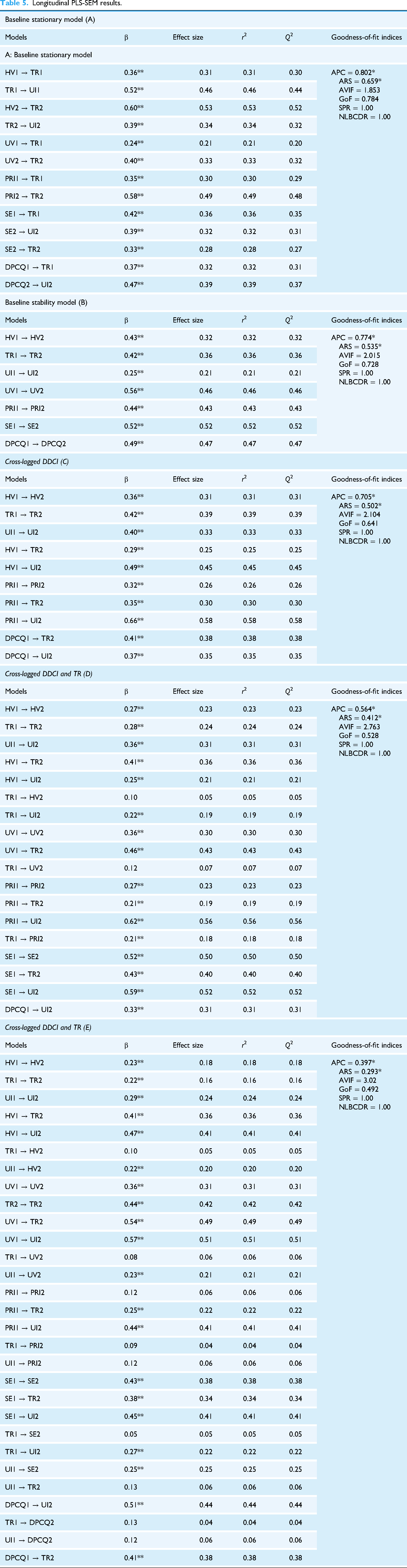
Model A represents the foundational stationary model, outlining the hypothesized relationships among the seven core constructs in our telehealth adoption framework: hedonic value, utilitarian value, perceived privacy, perceived security, trust, DPCQ, and intention to adopt telehealth. This model was independently estimated for both Time 1 (T1) and Time 2 (T2). All intratime path coefficients linking the constructs were statistically significant at both time points, supporting the model's structural validity. To evaluate the assumption of stationarity, we conducted Fisher's z-difference tests (Diedenhofen & Musch, 2015) comparing path coefficients across time. The z-values obtained were 1.317 (P = .35) and 1.087 (P = .41), indicating no statistically significant differences at the 0.05 level. These results confirm the stationarity of relationships over time.
Model B introduces autoregressive paths to form the baseline model, where values of each variable at T1 are regressed onto their corresponding values at T2. This allows for the evaluation of temporal stability and internal consistency across measurement waves. 85 The subsequent models (C through E) represent CLPM, which incrementally add cross-lagged effects to capture the causal dynamics between constructs across time. These models assess the directional influence of T1 constructs—such as trust or DPCQ—on related outcomes at T2, beyond simple autocorrelation.
Model E, the final and most comprehensive model, integrates both autoregressive and cross-lagged paths to examine the predictive power of telehealth perceptions and communication quality over time. The model exhibited acceptable goodness-of-fit indices, validating its use for hypothesis testing in a longitudinal framework. These findings underscore the causal significance of early doctor–patient communication quality and trust in shaping patients’ continued intention to adopt telehealth services.
Hypothesis testing
The cross-lagged analysis confirms that hedonic value at Time 1 (HV1) significantly predicts patient trust at Time 2 (TR2) (β = 0.41**, r2 = 0.36), representing a medium effect size. In contrast, the reverse influence of TR1 on HV2 is not significant (β = 0.10, r2 = 0.05). Fisher's z-test (z = 2.2674, P < .05) supports the dominant forward direction, thereby validating Hypothesis H1.
Similarly, HV1 exerts a significant positive impact on usage intention at Time 2 (UI2) (β = 0.47**, r2 = 0.41), while the path from UI1 to HV2 is weaker (β = 0.22**, r2 = 0.20). The directional difference is statistically significant (z = 2.1206, P < .05), supporting H2.
For utilitarian value, the path from UV1 to TR2 is strongly significant (β = 0.54**, r2 = 0.49), while the reverse is not (β = 0.08, r2 = 0.06). Fisher's z = 3.5062 (P < .01) confirms H3. Likewise, UV1 → UI2 is significant (β = 0.57**, r2 = 0.51), surpassing the reverse UI1 → UV2 path (β = 0.23**, r2 = 0.21), with z = 2.7638 (P < .01), confirming H4.
Regarding DPCQ, DPCQ1 positively affects TR2 (β = 0.41**, r2 = 0.38), while the reverse is minimal (β = 0.13, r2 = 0.04). Fisher's z = 3.9104 (P < .001) affirms the causal direction, supporting H5. Likewise, DPCQ1 → UI2 is significant (β = 0.51**, r2 = 0.44), while UI1 → DPCQ2 is not (β = 0.12, r2 = 0.06), with z = 3.4253 (P < .01), supporting H6.
For perceived privacy, PRI1 significantly predicts TR2 (β = 0.25**, r2 = 0.22), whereas the reverse is negligible (β = 0.09, r2 = 0.04). Fisher's z = 3.0921 (P < .01) supports H7. Similarly, PRI1 → UI2 is strong (β = 0.44**, r2 = 0.41), while UI1 → PRI2 is weak (β = 0.12, r2 = 0.06), with z = 3.1786 (P < .01), supporting H8.
In terms of perceived security, SE1 → TR2 is significant (β = 0.38**, r2 = 0.34), whereas TR1 → SE2 is not (β = 0.05, r2 = 0.05), z = 3.0087 (P < .01), confirming H9. Moreover, SE1 positively influences UI2 (β = 0.45**, r2 = 0.41), while the reverse (UI1 → SE2) has a smaller effect (β = 0.25**, r2 = 0.25), with z = 2.0794 (P < .05), supporting H10.
Finally, TR1 significantly predicts UI2 (β = 0.27**, r2 = 0.22), with the reverse path (UI1 → TR2) being nonsignificant (β = 0.13, r2 = 0.06). Fisher's z = 2.1372 (P < .05) confirms the directional superiority of trust over intention, validating Hypothesis H11.
Discussion and implications
Discussions
The primary objective of this research was to examine the dynamic relationships among key drivers influencing users’ continued intention to adopt telehealth services. Drawing from the dual perspective of hedonic and utilitarian value, as well as trust-based models in digital service adoption, we developed an integrated framework including hedonic value (HV), utilitarian value (UV), perceived privacy (PRI), perceived security (SE), DPCQ, trust (TR), and continuance intention (UI). A two-wave longitudinal survey (Time 1 = 427; Time 2 = 392) was conducted, and the relationships were analyzed using CLPM.
The results revealed that perceived security and perceived privacy were the most influential predictors of trust in the telehealth context. These findings reinforce earlier studies17,63 that stress the importance of safeguarding personal and medical information to foster user confidence in digital healthcare platforms. In environments where users may be concerned about data breaches and system vulnerabilities, a secure infrastructure becomes foundational to trust formation.
In addition, both hedonic and utilitarian value showed significant predictive effects on user trust and continued intention. Notably, utilitarian value emerged as the strongest predictor of continuance intention, indicating that patients prioritize practical benefits such as convenience, effectiveness, and efficiency when deciding whether to keep using telehealth services. On the other hand, hedonic value played a meaningful role in shaping trust, suggesting that users also value emotionally positive, comfortable, or enjoyable experiences when interacting with telehealth platforms—an area often underappreciated in healthcare technology design.
A novel and important contribution of this study is the integration of DPCQ into the trust-building framework. The findings confirmed that high-quality communication between patients and healthcare providers significantly improves trust, which subsequently enhances users’ intention to continue using telehealth services. 34 This highlights the irreplaceable human element in virtual care settings: even when mediated by technology, empathetic, clear, and responsive communication remains a critical determinant of successful patient engagement.
Importantly, the use of CLPM allowed us to test for temporal causality, moving beyond mere associations. The findings confirmed that HV, UV, PRI, SE, and DPCQ at Time 1 significantly predicted trust and intention at Time 2, while the reverse effects were weak or nonsignificant. This offers strong evidence for the directional and predictive validity of our model and mitigates concerns about reverse causation—an issue often overlooked in prior cross-sectional research.5,46
In conclusion, this study provides compelling longitudinal evidence that users’ long-term engagement with telehealth services is shaped by a combination of emotional satisfaction, practical functionality, data security, effective communication, and trust. These insights contribute to both academic theory and practical design strategies aimed at strengthening patient-centered digital health systems.
Theoretical implications
This study contributes to the growing body of knowledge on user behavior in telehealth contexts by uncovering how various psychological, experiential, and trust-related factors interact over time to influence continued use. It provides fresh insights for scholars in digital health, particularly those interested in technology adoption in emerging healthcare markets such as Vietnam.
First, this study expands the theoretical understanding of digital trust formation and behavioral intention in health technology environments. While prior literature in marketing and health informatics17,71 has emphasized the importance of privacy, security, and trust, our research empirically integrates these constructs within a longitudinal framework. By doing so, it verifies that users’ trust in telehealth platforms is shaped not only by their perceptions of data protection and system security, but also by their evolving interactions over time. This trust, in turn, significantly predicts their intention to continue using telehealth services, confirming and extending prior models by demonstrating causal temporal patterns.
Second, our findings validate the dual importance of hedonic and utilitarian value in influencing trust and behavioral outcomes in the telehealth setting. 33 While utilitarian value—such as efficiency, convenience, and functionality—had a stronger impact on continuance intention, hedonic value—reflected in enjoyment or emotional satisfaction—played a critical role in shaping trust. This dual-value framework enhances the theoretical richness of value-based adoption models and offers a more nuanced understanding of how emotional and practical motivations work in tandem to influence user engagement.
Third, the inclusion of DPCQ represents a novel theoretical contribution. Despite growing digitalization in healthcare, the interpersonal dimension of healthcare delivery remains essential. This study empirically validates that high-quality communication with healthcare providers significantly boosts users’ trust in telehealth services, positioning DPCQ as a central mechanism for bridging the gap between digital efficiency and relational warmth in remote healthcare delivery. Its significance supports the broader sociotechnical perspective that emphasizes human interaction even in tech-mediated service environments.
Finally, by employing CLPM and collecting two-wave longitudinal data, this research advances the methodological rigor in telehealth adoption studies. It moves beyond static, cross-sectional designs and contributes theoretically by illustrating causal, lagged relationships between experiential value, perceptions of security/privacy, interpersonal communication, trust, and behavioral intention. This dynamic perspective strengthens the theoretical foundation for understanding how adoption intentions evolve in complex digital health systems.
In sum, this study offers an integrated and longitudinally validated model that enriches the theoretical discourse on telehealth adoption by addressing both system-level and human-centric factors, including privacy, trust, communication, and value perceptions.
Practical implications
This study provides actionable insights for healthcare technology designers, telehealth platform developers, and policy-makers aiming to enhance the long-term adoption of telehealth services. Beyond platform-level design, the findings also offer explicit policy and professional guidance for public health authorities and physicians on how telehealth and broader e-health ecosystems can be strategically leveraged to improve patients’ quality of life (QoL), while proactively managing inherent tensions related to trust, privacy, and data governance. 87
First, our findings emphasize the critical role of perceived privacy and security in influencing users’ trust and continued use of telehealth platforms. Healthcare providers and developers must prioritize robust data protection measures to address patients’ concerns regarding personal health information. Technical safeguards such as end-to-end encryption, multi-factor authentication, and compliance with data protection regulations (e.g., HIPAA or local laws) should be clearly communicated to users to build confidence. Without such transparency and protection, it is difficult to convert user interest or initial use into consistent engagement with telehealth services. From a public policy perspective, health authorities should establish clear, enforceable, and harmonized digital health governance frameworks that define accountability, data ownership, and ethical AI use—particularly as telehealth increasingly integrates with e-health systems, IoT-enabled remote monitoring, and machine learning–based medical analytics, which are rapidly reshaping healthcare research and practice. 88
Second, to foster trust and reduce resistance, telehealth platforms must offer a user experience that reduces discomfort related to privacy intrusions or security breaches. For example, patients managing sensitive or stigmatized conditions (e.g., mental health or sexual health) should not be subjected to intrusive follow-up messages or irrelevant health suggestions. Systems should allow personalized communication control, giving patients confidence in how their data is used. Regular security audits and transparent data policies can further reinforce users’ sense of safety and accountability. For regulators and healthcare institutions, this implies the need to set minimum standards for consent management, data minimization, and patient-controlled information sharing—especially in IoT-based and continuously monitored care environments, where excessive data collection may otherwise undermine trust and QoL.
Third, the study highlights that utilitarian value, such as saving time, accessing timely care, and receiving accurate medical advice, significantly motivates users to continue using telehealth. Healthcare providers should ensure that telehealth services deliver reliable and goal-oriented outcomes, such as reduced waiting time, clear diagnosis, and efficient prescriptions. Users who experience tangible benefits are more likely to perceive the platform as effective and return to it when facing similar healthcare needs. At the system level, policymakers can facilitate these outcomes by promoting interoperability across telehealth platforms, electronic health records, and national e-health infrastructures, enabling continuity of care and supporting long-term population-level QoL improvements rather than fragmented digital services.
Fourth, while utilitarian value drives functional satisfaction, hedonic value—such as comfort, convenience, and emotional relief from remote consultations—plays a strong role in cultivating trust. Designing telehealth interfaces that are visually soothing, easy to navigate, and respectful in tone can enhance the emotional experience. Given that trust is an essential bridge between initial use and long-term loyalty, designing for emotional as well as functional satisfaction becomes vital. This implication is particularly salient for chronic disease management, elderly patients, and individuals with mobility or access constraints, for whom emotionally supportive e-health interactions can meaningfully enhance daily well-being and perceived quality of life beyond clinical outcomes.
Finally, this study underscores the importance of DPCQ as a key trust-building mechanism. High-quality interpersonal interaction—characterized by empathy, clarity, responsiveness, and respect—can compensate for the lack of physical presence in virtual care. Training healthcare professionals in digital bedside manners and equipping them with real-time communication tools (e.g., secure video chats, prompt messaging) can reinforce patient confidence. From a policy and professional development standpoint, public health authorities and medical associations should invest in structured digital health training programs for physicians, ensuring that advances in telehealth, IoT, and data-driven healthcare analytics translate into patient-centered QoL improvements rather than purely technical efficiency gains.
In summary, telehealth stakeholders should adopt a multi-faceted strategy that combines technical security, emotional engagement, practical usefulness, and strong communication to drive trust and sustained platform usage. When supported by coherent public policy, physician engagement, and integrated e-health infrastructures, telehealth technologies have the potential to substantially enhance healthcare accessibility, continuity, and overall quality of life, despite persistent tensions surrounding privacy, security, and trust.
Limitations and future research directions
First, the data were collected in Vietnam, which may limit generalizability to other cultural or healthcare settings. Future research should test the model in diverse regions to validate its broader applicability. Second, the model focuses on key predictors—hedonic and utilitarian value, perceived security, trust, and DPCQ—influencing users’ intention to adopt telehealth. Future studies could include other relevant factors such as satisfaction, perceived health benefits, or technology readiness. Additionally, the moderating effects of demographic traits or prior telehealth experience warrant further exploration. Third, this study considered general telehealth platforms without distinguishing between types of providers (e.g., public hospitals vs. private apps). Future research should investigate how platform type may affect user behavior. Finally, all data were self-reported, which may introduce common method bias. Future work should incorporate behavioral or system-based data (e.g., usage logs) to strengthen the validity of findings. Addressing these limitations will enhance understanding of telehealth adoption and help design more effective digital healthcare strategies.
Conclusion
This study provides longitudinal evidence on the mechanisms driving patients’ continuance intention toward telehealth services. By integrating hedonic and utilitarian value, perceived privacy, perceived security, DPCQ, and trust within a cross-lagged panel framework, the findings demonstrate that telehealth adoption evolves through both technological and relational processes over time.
Utilitarian value emerged as the strongest predictor of continued usage intention, underscoring the importance of efficiency and practical benefits in digital healthcare. At the same time, hedonic value and high-quality doctor–patient communication significantly contributed to trust formation, highlighting the continued relevance of emotional reassurance and empathetic interaction in virtual care. Perceived privacy and security also played foundational roles in strengthening trust and sustaining engagement.
By employing a two-wave longitudinal design and CLPM, this study advances prior cross-sectional research by establishing temporal precedence and reducing reverse-causality concerns. Overall, the findings support a sociotechnical perspective in which secure system infrastructure and meaningful human communication jointly foster long-term telehealth adoption.
Footnotes
Acknowledgments
We would like to thank all the participants for supporting this work.
Ethics declaration
Not applicable.
Ethics approval and consent to participate
Ethics approval for this study was obtained from our institution before data collection. All participants were informed about the purpose, procedures, and voluntary nature of the study and provided their consent to participate.
Ho Chi Minh City University of Economics and Finance granted the authors permission to use the scale for this academic research. This study was conducted in accordance with ethical guidelines for research involving human participants. Informed consent was obtained from all participants. No personal identifying information was collected.
Consent to participate
All human participants provided informed consent before participating in the study.
Consent for publication
The authors declare their consent for publication.
Clinical trial number
Not applicable.
Clinical trial registration details
Not applicable.
Contributionship
Linh Thi Thuy Tran: conceptualization, literature review, questionnaire design, data collection, writing—original draft preparation. Thuy Dung Pham Thi: methodology design, statistical analysis, data interpretation, writing—review and editing. Nam Tien Duong: research supervision, theoretical framework development, validation, writing—review and editing, project administration, corresponding author responsibilities. All authors have read and approved the final version of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Availability of data and material
The data that support the findings of this study are available from the corresponding author upon request.