
Abstract
Background
Telehealth services have gained popularity in Malaysia, providing convenient consultations during the COVID-19 pandemic. However, there is limited research on their usage, user demographics and prescribed medications. This study aims to fill that gap by investigating telehealth service utilisation in community pharmacies and identifying trends in common diagnoses and medications prescribed.
Methods
A retrospective observational study was conducted using a telehealth services database in Malaysian community pharmacies. Consultation records from January 2019 to December 2021 were extracted using a data collection form. The study identified the service usage over time, demographic profiles of users and the most common diagnoses and prescribed medications. Diagnoses were classified using the International Classification of Disease, 10th Revision (ICD-10), and medications were classified using the Anatomical Therapeutic Chemical (ATC) system.
Results
The study included 835,826 telehealth service records, with 88.8% being assisted consultations with e-prescriptions and 11.2% direct consultations. The user population consisted of primarily Malaysians (96.9%), with a mean age of 50 ± 21 years. Both telehealth services saw an increase in unique users over the 3-year study period. There was a moderate correlation between active COVID-19 cases and monthly user count. Assisted consultations were more widely used than direct consultations.
Conclusion
This study found an increased usage of telehealth services and its potential to remain as a healthcare system feature in community pharmacies. Further investigation into the impact on medication safety, quality and healthcare delivery is warranted.
Introduction
Telehealth is defined as the utilisation of telecommunications or digital communication technologies for the remote delivery of healthcare services or the transmission of medical information.1,2 A common telehealth service includes e-consultation, which may include prescribing of electronic prescriptions (e-prescribing), and typically occurs between clinicians or clinicians and patients.3,4 These consultations may involve prescribing e-prescriptions, which are directly transmitted from prescribers to community pharmacies via digital devices for dispensing. 5 Recent studies have reported satisfaction among community pharmacy customers using such services, with the convenience of access to telehealth being the primary reason. 6 In some instances, e-prescribing has been reported to support safe prescribing following reduced prescription errors. 7 As highly accessible healthcare professionals in primary care, community pharmacists hold a pivotal position in fostering and assisting patients in utilising telehealth services, including consultations with doctors. Moreover, they play a role in medication review and in promoting the continuity of medication supply. 8 By working in collaboration with prescribers through telehealth services, community pharmacists can provide a holistic approach to patient care, ultimately resulting in enhanced health outcomes.
Telehealth services effectively tackle numerous challenges, such as enhancing accessibility for patients and ensuring regulatory compliance for healthcare professionals. One of the challenges for patients on long-term medications is accessing prescriptions to obtain their medications when supplies run out. This inconvenience, in turn, can compromise adherence to prescribed regimens and, ultimately, impinge upon the desired health outcomes for patients. The situation is compounded by the illegal purchasing and dispensing of medications, including antibiotics, without a prescription. 9 Inappropriate prescribing and dispensing of antibiotics in community pharmacies can potentially contribute to the emergence of antimicrobial resistance, ultimately causing serious public health concern. 10 Additionally, manually written prescriptions can lead to medication errors, particularly when healthcare providers’ handwriting is illegible, affecting patient safety.11,12 Collectively, telehealth services including e-prescribing may help ensure the management of minor ailments, continuity of supply of medications, improvement of adherence and increase in medication safety.13,14 By harnessing telehealth services, patients can receive timely access to medications while minimising the risk of medication errors and misuse.
Malaysia's healthcare system is comprised of both the public and private sectors. Traditionally, in the private sector, patients in Malaysia have obtained their medications directly from clinics, primarily due to the lack of dispensing separation within private primary care settings. 15 However, recently in 2022, there was an amendment to the Poisons Act 1952, which now incorporates electronic prescriptions. 16 Now, with the integration of telehealth services into community pharmacies, patients have the convenience of obtaining their medications from these pharmacies using legitimate e-prescriptions prescribed and issued by virtual doctors upon consultation.
Although telehealth services have increased exponentially, particularly in the wake of the COVID-19 pandemic, 17 to date, there is a lack of studies investigating telehealth services across community pharmacies in Malaysia in terms of frequency of use, user demographics and the medical conditions the telehealth services cater for. Studies on telehealth are crucial and are much needed as the findings will assist policymakers in navigating the rapidly evolving landscape of digital health and provide guidance for the future of pharmacy practice. Hence, this study aims to investigate the usage of telehealth services across community pharmacies in Malaysia and determine trends of the most common diagnoses and medications prescribed.
Methods
Study design and setting
This study was a retrospective study using data from a local telehealth services provider, DOC2US, which is one of the major private commercial companies providing technologies (software, website, mobile applications and platform) for the provision of telehealth across Malaysia, with their paid services available nationwide. Their telehealth services encompass a comprehensive range of consultation options, offering both assisted and direct consultations between physicians and patients. Assisted consultations involve pharmacists aiding users to consult qualified virtual physicians affiliated with the service to obtain their medications. Pharmacists play a crucial role by providing supporting information, such as medical histories and relevant clinical data like blood pressure and blood glucose readings measured at the pharmacy. This information is then electronically transmitted and reviewed by the physician. The physician, upon review, has the discretion to reject the request, seek additional information or approve the request and issue the corresponding e-prescription. These e-prescriptions can then be conveniently filled and dispensed at affiliated pharmacies. This service is particularly beneficial for users requiring refills of chronic medications, as it provides convenience to the user by removing the need to visit a physician to obtain a prescription physically. However, patients are still strictly required to attend their usual physical follow-ups with their regular doctors, as scheduled accordingly. In contrast, direct consultation services typically involve a text chat, audio chat or video call with a physician in situations where the diagnosis or follow-up can be made remotely. If required, physicians may provide a diagnosis and an e-prescription or recommend a physical follow-up. This service is typically utilised by users seeking diagnosis for relatively minor ailments or regular follow-up for stable conditions. Both types of consultations, assisted and direct, involve the electronic transmission of medical information and the delivery of healthcare services remotely and therefore are classified as telehealth. These services can be accessed through either a dedicated mobile application or a web-based portal. At the time of study, affiliated community pharmacies and physicians were primarily distributed among urban and suburban areas within the country. To ensure patient safety, the telehealth services provider also issues internal guidelines to pharmacists and physicians affiliated with the service. These guidelines provide limitations to ensure physical consultations are still carried out where necessary by stipulating the conditions which can be managed by remote consultation, medications which are allowed to be prescribed electronically and maximum durations for e-prescriptions issued before physical consultations are required.
Data collection form
The data collection form was developed to collect data on demographic of users, health records and medication-related information. A pilot study was conducted to extract 10–20 records before the actual data extraction to examine the data collection form's feasibility and appropriateness. Feedback and comments from a panel of experts were considered and incorporated into the final data collection form.
Data extraction and analysis
Data was extracted from the internal database of the aforementioned telehealth services provider for the 3-year period between January 2019 and December 2021 (Figure 1). To ensure the protection of patient data, extensive measures were taken. The data was acquired in an anonymised format, and rigorous protocols for access control, secure storage and transmission were implemented. The data was provided by the telehealth services provider in an anonymised format with no personally identifiable information. Data included the following: patient demographics, type of consultation, the status of the e-prescription (if applicable), the reason for rejection, timestamps, location of the pharmacy, past medical and medication histories, relevant clinical data, medication(s) prescribed, medication(s) dispensed and optional remarks by physicians or pharmacists. The duration of service was determined based on the timestamps, where it is defined as the length of time used for a service (i.e. real-time interactive communication between a patient and a healthcare provider) from its commencement to the end. The individuals responsible for extracting the data remained independent from the subsequent data analysis, ensuring a clear separation of roles and minimising any potential bias. The data was stored in a password-protected file on a secured device accessible only to the researchers directly involved in the data analysis.
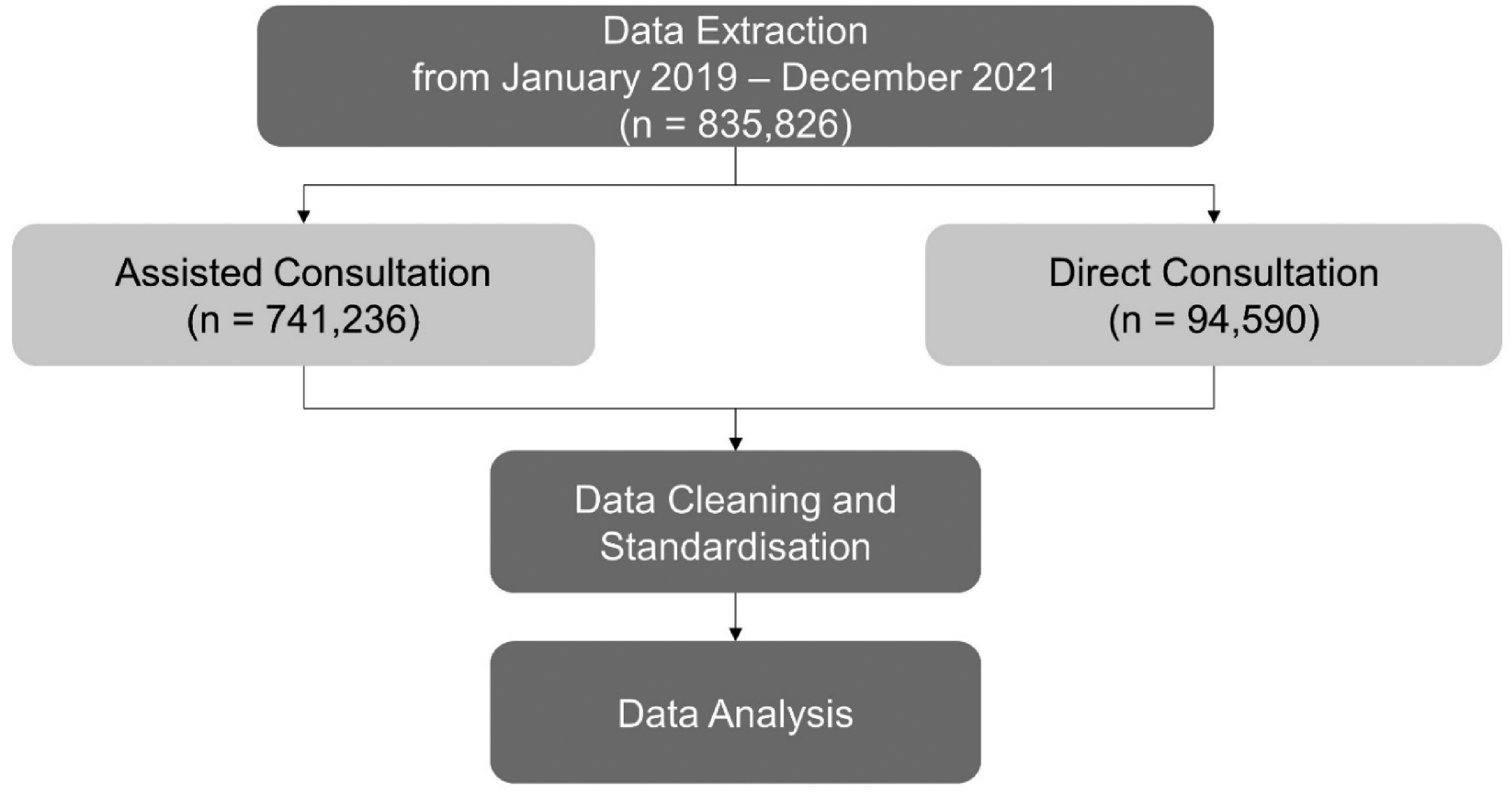
Data extracted for assisted consultation and direct consultation services between January 2019 and December 2021.
Data analysis was then performed using Python 3.11 with the Pandas and Matplotlib libraries.18,19 As the data included free text, there were significant variations in terminologies for diagnoses and medications, including abbreviations, brand names, and combination products. The data was therefore cleaned and standardised prior to analysis. Diagnoses were reclassified according to the closest International Classification of Diseases, 10th Revision (ICD-10) code, while drugs were reclassified using Anatomical Therapeutic Chemical (ATC) classification system.20,21 Assisted consultations with e-prescriptions and direct consultation services for specific medical complaints were analysed separately. The top diagnoses for both services were analysed, and the most common medication prescribed was reported for each diagnosis. Student's t-test was used to assess the difference in the mean age of the telehealth services users. Chi-squared (χ2) test was performed, respectively, to determine the association of telehealth usage between categorical variables, such as gender, age group and diagnosis. Pearson's correlation was used to measure the strength of the linear relationship between pairs of continuous variables. Multivariate logistic regression was used to study the probability of using direct consultations compared to assisted consultations based on patient demographics, comorbidities and medications. The p-values reported were two-tailed, with a value of <0.05 being statistically significant.
Results
A total of 835,826 records were extracted from 411 pharmacies across the states in Malaysia during the study period, consisting of 88.8% (n = 741,236) assisted consultations and 11.2% (n = 94,590) direct consultations. The demographic characteristics of telehealth users are shown in Table 1. Generally, the user population comprised of 58.7% female and 41.3% male, with a mean age of 50 ± 21 years, and were primarily Malaysians (96.9%) for both telehealth services. However, there were a significantly higher proportion of females using assisted consultations compared to those using direct consultation services (p < 0.001). On the other hand, the mean age of assisted consultation users was higher than that of direct consultation users (p < 0.001). In the multivariate analysis, users who were female and those with diabetes mellitus and hyperlipidaemia comorbidities were associated with a higher propensity in using assisted consultation services (p < 0.05) (Table 2), whereas non-Malaysians and those with asthma comorbidity were more likely to use direct consultation services (p < 0.05).
Demographic characteristics of telehealth users.
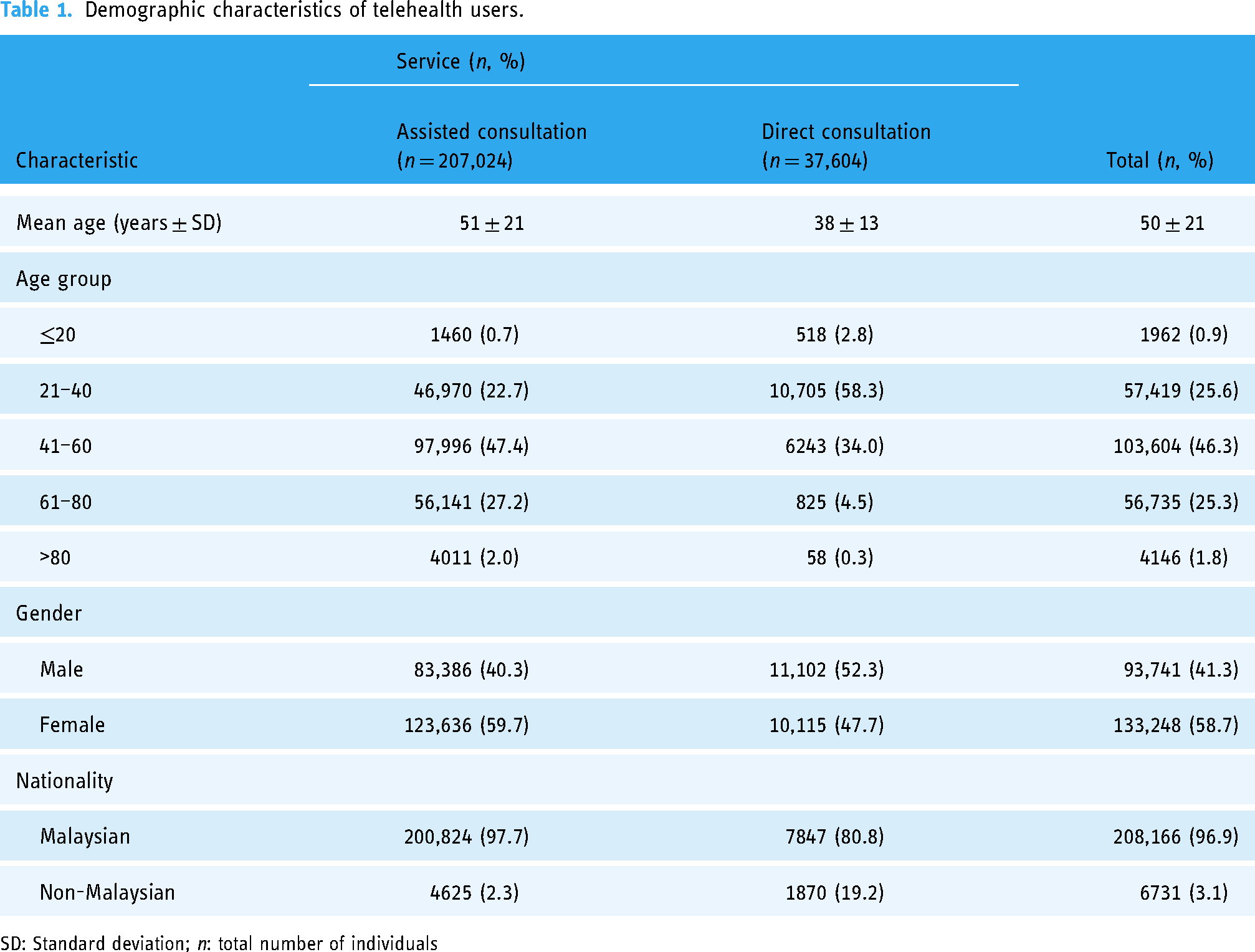
SD: Standard deviation; n: total number of individuals
Multivariate analysis of the usage of direct consultation services compared to assisted consultation services based on users’ characteristics.
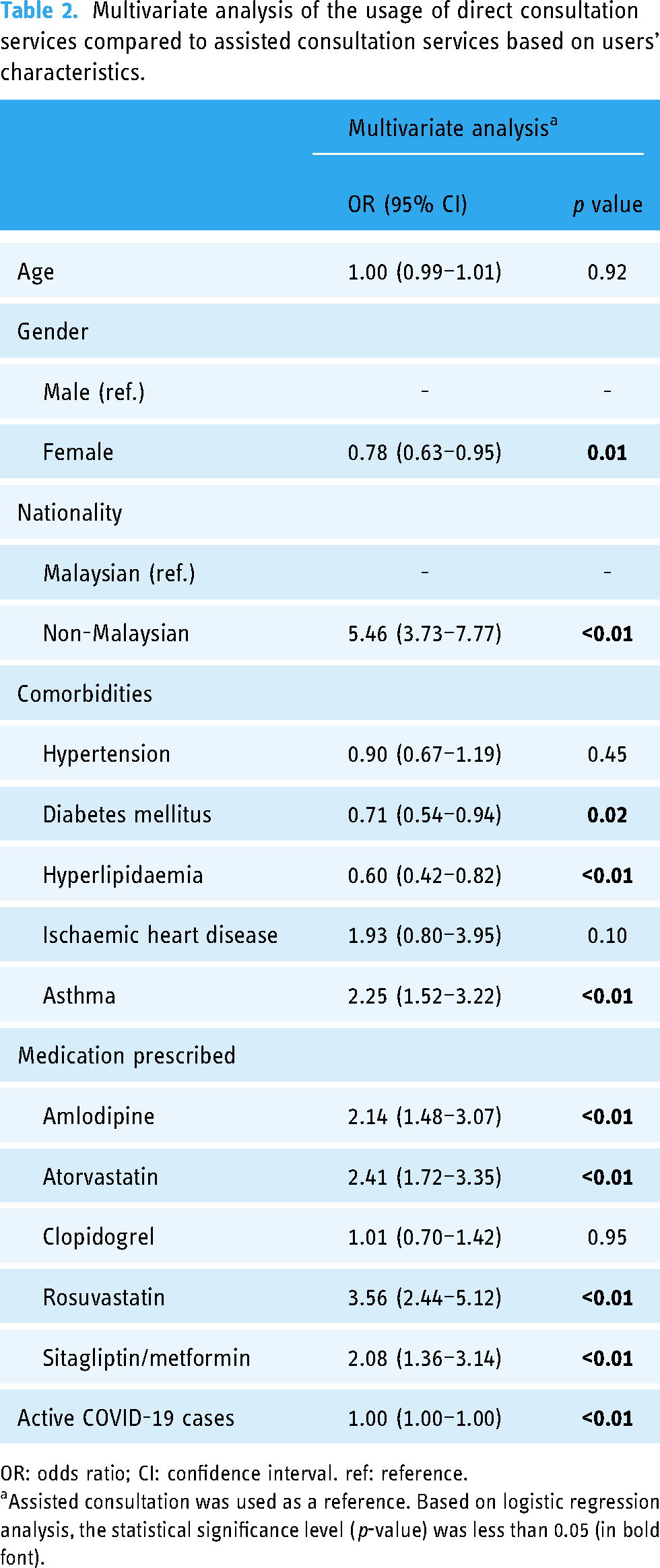
OR: odds ratio; CI: confidence interval. ref: reference.
Assisted consultation was used as a reference. Based on logistic regression analysis, the statistical significance level (p-value) was less than 0.05 (in bold font).
The trend of total unique patients per month utilising both services is shown in Figure 2. Throughout the study period, there was a steady increase in the number of unique users for both telehealth services. However, assisted consultation services were much more highly utilised compared to direct consultation services, reaching a peak of 29,081 unique users per month compared to only 5528 unique users per month for direct consultations. There appeared to be little correlation between the rates of increase in users with respect to the various Movement Control Orders (i.e. lockdowns) during the study period. Instead, it was observed that the rate of increase in the number of unique monthly users showed a moderate correlation to the number of active COVID-19 cases in the country, with R2 values of 0.587 and 0.540 between the number of active COVID-19 cases and the number of monthly users for assisted and direct consultations, respectively (p < 0.001, respectively). However, monthly users remained high even after active COVID-19 cases fell and movement restrictions were lifted.
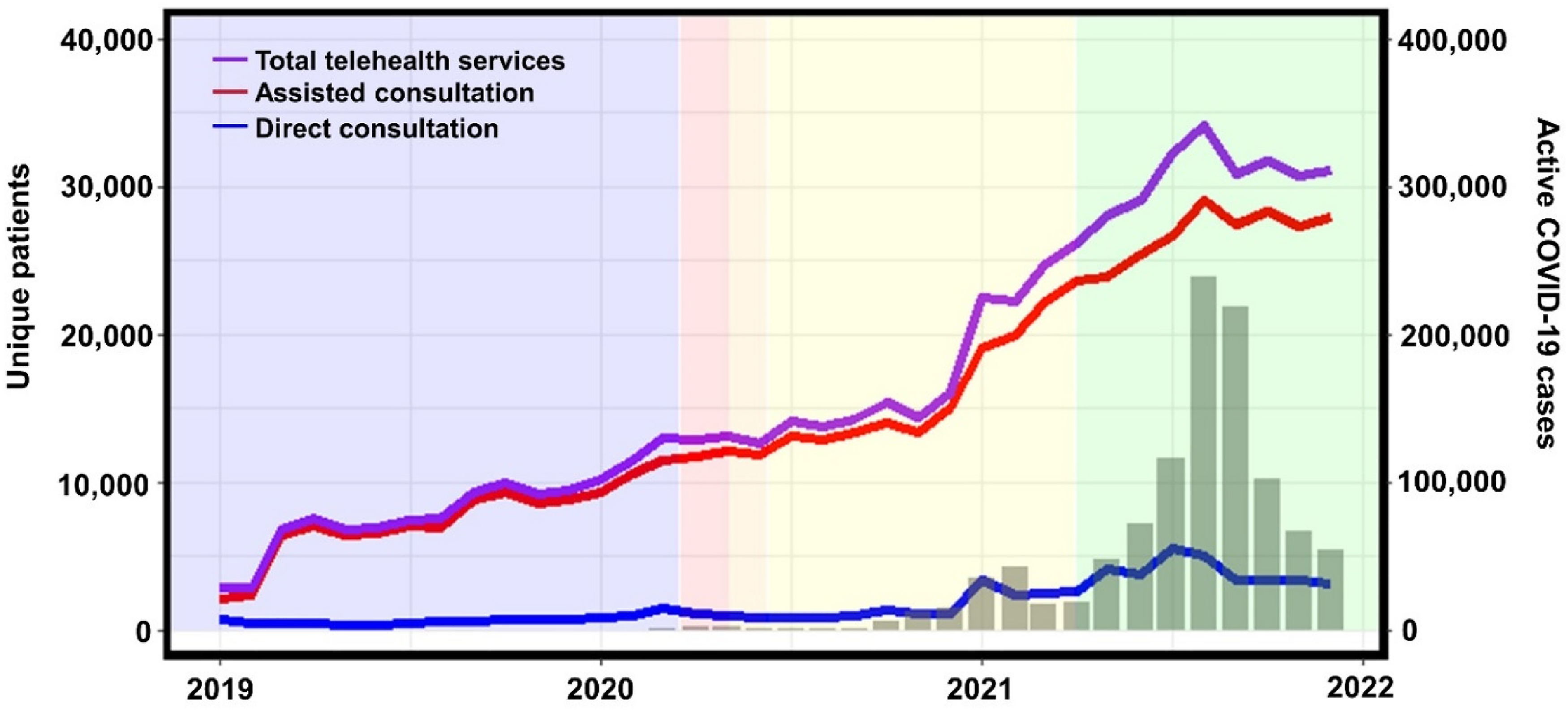
Number of unique patients per month utilising total telehealth services (purple), assisted consultation with e-prescriptions (red) and direct consultation (blue). The number of active COVID-19 cases (grey bars) is also shown, while the coloured backgrounds indicate various lockdown phases (blue = none, red = Movement Control Order, orange = Conditional Movement Control Order, yellow = Recovery Movement Control Order, green = endemic phase) during the corresponding period.
In terms of the duration of service being provided, notably, assisted consultation services required a much shorter average duration (80.0% required less than 5 minutes) than direct consultation services (71.6% required more than 2 hours). Generally, 97.6% of the assisted consultations resulted in e-prescriptions issued to the pharmacy. The remaining 2.4% of assisted consultations did not result in e-prescriptions issued due to incomplete patient details (40.7%), followed by out-of-scope requests (i.e. cases where the medical conditions or medications requested were not allowed according to the telehealth provider guidelines) (26.2%), incorrect drug indication (16.6%) and inappropriate medication dosage (16.4%). In contrast, 30.0% of direct consultations resulted in an e-prescription issued.
The most common diagnoses for both consultation services are shown in Table 3. Assisted consultation services with e-prescriptions were utilised primarily for common chronic diseases, particularly those related to cardiovascular diseases such as hypertension, ischaemic heart disease, arrhythmias and atherosclerosis, which made up 41.7% of all diagnoses. This was followed by diabetes mellitus and dyslipidaemia, accounting for 17.5% and 11.6% of all diagnoses, respectively. A similar trend was observed for direct consultations, with cardiovascular diseases accounting for 43.0% of all diagnoses, followed by diabetes and dyslipidaemia at 18.5% and 9.4%, respectively. Only one acute condition within the most common diagnoses consisted of various bacterial infections and accounted for 3.5% of all direct consultations. Consistently, the most common medications prescribed for both services corresponded with the respective top diagnoses (Table 4).
Most common diagnoses for telehealth services.

n: total number of consultations
Most common medications prescribed via telehealth services.

n: total number of consultations
Discussion
Over the past decade, telehealth services have seen continued growth and adoption globally. This growth has been fuelled by improving internet infrastructure and access worldwide and incentivised by governments seeking to leverage the benefits of digital health in their transition towards digital economies. 22 Malaysia has been a part of this transformative wave, as evidenced by the emergence of numerous health technology startups in recent years. In this study, we have analysed data from one of the largest telehealth services providers in the country, providing insights into the trends of digital health adoption, user demographics and the various conditions these services are utilised for.
The overall mean age of telehealth users was in the middle age range. Although younger adults aged <40 years old engaged most in direct consultation services compared to those who utilised assisted consultation services with e-prescriptions, this observation was not found to be significantly different in the multivariate analysis. A similar pattern was reported in nationally representative patients in the United States, where the users of teleconsultations were four times higher among younger users (i.e. 25–44 years old) than those aged 45 and above. Moreover, the younger group was more inclined to discuss their health concerns through teleconsultation than the older group. 23 This is likely due to higher digital literacy among younger adults, who may find it less challenging to utilise teleconsultation services in communicating with healthcare professionals regarding their illnesses. 24 This finding highlights that digital literacy could be one of the barriers to accessing telehealth services and poses a challenge in implementing telehealth among the older population. Furthermore, a qualitative study conducted among type 2 diabetes patients in Malaysia also revealed generational differences in the preference for telehealth. Specifically, older adults were found to be less inclined towards telehealth than younger adults. 25 On the other hand, there was a higher mean age among assisted consultation users compared to direct consultation users. This could be explained by the probability of having multiple chronic illnesses with increasing age, which requires a long-term prescription for these chronic conditions. 26 In contrast, younger patients are less likely to suffer from chronic conditions and are therefore more likely to utilise telehealth services for acute minor ailments, contributing further to their higher representation among users of direct consultation services. Notably, this study's findings support the notion that the most common diagnoses for e-prescription are the prevalent non-communicable diseases in the country, such as hypertension, diabetes and ischaemic heart disease.
This study yielded an interesting finding that a significantly higher proportion of females opted for e-prescriptions via assisted consultation services compared to direct consultation services. This finding contrasts with previous studies, which reported that female patients were more likely to use direct teleconsultation services (both via video and phone consultation) compared to in-person visits in an outpatient setting.27–29 In addition, a cross-sectional survey conducted in the United States found that female gender is one of the predictors of liking telehealth visits compared to traditional in-person visits. 30 Despite the growing prominence of telehealth services, there is still a notable lack of information regarding the satisfaction levels and preferences of female Malaysians specifically when it comes to utilising telehealth. Further investigation is required to reveal the possible factors contributing to this finding.
Our findings indicate a gradual rise in the acceptance and utilisation of telehealth services among the general public in recent years. These have at least been partially driven by the COVID-19 pandemic, as constraints on many regular physical activities acclimatised the general public towards the use of digital alternatives.31–33 Surprisingly, we observed that the lockdowns of various severities had less of an effect on adoption than the number of active COVID-19 cases, despite the former's more direct impact on physical restrictions. However, it should be noted that there exist various confounding factors in these observations, such as the number of participating healthcare providers, coverage of the services, marketing initiatives by the companies involved, the government's push towards a digital economy and diffusion time for public awareness of the availability of such services. Nonetheless, it is evident that recent events have helped improve public adoption of telehealth services, which traditionally have always shown inertia towards such voluntary changes.34,35
E-prescriptions via assisted consultation services were clearly more highly utilised than direct consultation services throughout the study period. Prior to the availability of e-prescriptions by telehealth services providers, the purchase of prescription medicines without a prescription from pharmacies did occur, with only a small number of medications dispensed with prescriptions. 36 The general public commonly cites factors such as inconvenience and increased cost in disfavouring dispensing separation and obtaining mandatory prescriptions. 37 The notable surge in demand for e-prescriptions, as observed in this study, is a testament to their valuable role in addressing a gap within the existing healthcare system. This growth is further encouraged by the active involvement and support of participating pharmacies. This represents a viable avenue to acclimate the general public towards the dispensing separation by diminishing the inconvenience associated with obtaining prescriptions. This was particularly true for medications for chronic conditions which required refills, as our findings also showed that the most common medications provided in conjunction with the e-prescriptions were for the chronic conditions with the highest prevalence in the country, such as hypertension, diabetes and hyperlipidaemia. 38 When coupled with recent amendments to national legislation defining the requirements for legally recognised e-prescriptions, 39 these findings provide an encouraging starting point for efforts to advocate the use of mandatory prescriptions to improve the medication supply process and promote the safe use of medications. In addition, this study also highlighted that when assisted by community pharmacists, the time required to issue an e-prescription was short, which could be a favourable feature in driving the adoption of e-prescriptions. While these telehealth services could undoubtedly spur the delivery of healthcare through community pharmacies, challenges remain in the context of the broader Malaysian healthcare system. Compared to other countries such as the United States, the United Kingdom and Australia, community pharmacies in Malaysia are not currently integrated with general practitioners as part of the broader primary care healthcare delivery system. 40 The lack of a central repository for medical information and a national healthcare insurance scheme makes information-sharing between different healthcare providers in the private sector difficult. This is further exacerbated by the disconnect with the federally managed public healthcare sector. Further integration, collaboration and coordination between these fragmented stakeholders under national initiatives would be required before the full potential of telehealth services in community pharmacies can be realised.
In contrast to e-prescriptions via assisted consultations, the adoption of direct consultation services, which allowed patients to consult with physicians via text chat or video calls for their medical complaints, was relatively weaker among the public. There could be multiple reasons for this lower uptake, including the inherent limitations associated with any consultation that cannot include a physical examination. Most patients would understandably prefer conventional face-to-face consultations, especially when their condition involves a degree of unfamiliarity or perceived severity that would outweigh the convenience afforded by an online consultation. 6 In addition, physicians were bound by guidelines issued by the telehealth services provider, which restricted the conditions they could treat and medications they could prescribe electronically. This approach ensures the delivery of quality healthcare while still allowing for physical consultations when necessary. As a result, the direct consultation services experienced a limitation in their overall coverage, potentially diminishing their utility. A study by Gilbert et al. shows that the tendency to seek treatment from the comfort of home is low as patients prefer to have some sort of physical interaction with a healthcare provider. 41 This observation was corroborated by the data showing the common conditions diagnosed. While one would assume direct consultation services would be well-suited for acute minor conditions requiring prompt medical attention, our findings indicate that the majority of diagnoses were for chronic conditions. Patients appeared to be using these services for routine follow-ups, potentially with self-monitoring data, rather than seeking initial diagnosis or treatment. Notably, the only prominent acute condition observed within the service was acute bacterial infections.
Furthermore, pharmacists are well-trained to manage minor ailments which can be managed by non-prescription medicines, and thus the need for direct consultation with physicians for minor ailments may not be required. These findings suggest that the role of teleconsultation in filling the gap within the healthcare system is relatively smaller when compared to the demand for e-prescriptions through assisted consultation services. The effectiveness of direct consultations within any healthcare system appears to be more suitable for routine follow-up of chronic conditions rather than addressing acute minor illnesses.
Overall, our study has shown that the adoption of telehealth services has grown significantly over the past several years, potentially accelerated by the COVID-19 pandemic. Obtaining e-prescriptions, in particular when assisted by pharmacists, appears to have the potential to fill a gap in the healthcare system, allowing for convenient access to prescriptions for regular follow-up medications. However, the findings of this study should be interpreted within the context of several inherent limitations. This study only included data from a single telehealth services provider in the country (albeit one of the largest), and therefore the types of services offered, scope, user experience, the growth rate in the number of participating healthcare partners, marketing initiatives and geographical coverage may limit the generalisability of the data and the conclusions made. Our study highlights the potential for telehealth and other digital health services to improve healthcare access and fill healthcare gaps. The challenge now is to ensure that these services are integrated into the broader healthcare system and made accessible to all patients, particularly those in the public healthcare sector who stand to benefit the most from digital transformation. Further research is needed to determine the most effective ways to integrate these digital health services into existing healthcare systems and to ensure equitable access to these technologies for all patients.
Conclusion
The utilisation of telehealth services in Malaysia has increased over the past several years and has been accelerated by the COVID-19 pandemic. Among the services provided, consultations associated with e-prescriptions issued following assistance from community pharmacists were significantly more utilised compared to direct consultations with physicians regarding specific medical complaints. These services are currently utilised primarily for the follow-up of chronic conditions, particularly cardiovascular diseases, and correspondingly the vast majority of e-prescriptions are for medications associated with these conditions. Taken together, these findings demonstrate that in the context of Malaysia's current healthcare system, e-prescriptions fill a significant gap in the management of chronic conditions. In order to fully leverage the potential of these services, a collaborative approach between all healthcare professionals, including physicians and community pharmacists, should be adopted to promote and assist patients in transitioning to these digital health services. By leveraging the expertise of various healthcare stakeholders, the potential of telehealth services can be fully realised in improving the management and outcomes of chronic conditions for patients in Malaysia.
Footnotes
Acknowledgements
The authors thank Dr Raymond Choy Wai Mun and Dr Shekhar BG Ramjutun from DOC2US Malaysia for their support in this project.
Data Availability
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Contributorship
JSEL, HYY, MHMMZ and NAR conceived the ideas to conduct this research and conducted the data collection. JSEL, HYY and NAR designed and planned the research and performed the literature search. YYT performed data extraction and analysis. The manuscript was drafted and edited by JSEL, HYY, YYT, KG, HCO and NAR and reviewed by all authors. All authors read and approved the final manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical approval
Ethics approval was obtained from the Universiti Malaya Research Ethics Committee (UM.TNC2/UMREC_2038, 28 July 2022). Informed consent was not necessary in this retrospective study as it was analysed using the existing records without direct subject recruitment. All data were collected with a unique study identity number, where there was no personal identifiable information within the records.
Funding
The authors disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This work was supported by DOC2US Malaysia.
Guarantor
NAR.