
Abstract
Aim
To systematically assess the quality, reliability, and content attributes of YouTube videos pertaining to transperineal prostate biopsy (TPB), an innovative method for diagnosing prostate cancer.
Materials and methods
A systematic search was performed on YouTube on May 18, 2025, using the terms “transperineal prostate biopsy,” “TP biopsy,” and “perineal prostate needle biopsy.” The search was conducted in incognito mode to reduce personalized bias. Videos in the English language uploaded from April 2019 to April 2025 were included. Videos that were duplicate, irrelevant, non-English, or lacking of sound were eliminated. Sixty movies, organized by relevance, were reviewed, resulting in 50 videos that satisfied the inclusion criteria for analysis. Two senior urologists independently evaluated each video using the Global Quality Scale (GQS) and the modified mDISCERN (mDISCERN) tool to measure reliability and quality. Video metadata, including time, views, likes, upload date, and creator category (academic professional, non-academic professional, patient, medical company, or others), was documented.
Results
The average duration of videos was nearly 7 min, with an average of 8950 views per video. Healthcare workers created 60% of the videos, whereas 10% included advertising material. The predominant subjects addressed were procedural methodologies, anesthesia, and a comparative analysis of infection risk associated with the transrectal technique. The average GQS score was 2.96 ± 0.77, indicating moderate quality, whereas the average mDISCERN score was 2.1 ± 0.9, suggesting low to moderate reliability. Several videos referenced peer-reviewed literature, while numerous others displayed commercial bias. Inter-rater reliability was significant, with intraclass correlation coefficients of 0.893 for GQS and 0.861 for mDISCERN.
Conclusion
YouTube videos related to TPB show significant range in quality and reliability. Despite being created by healthcare experts, the absence of peer-reviewed references and the prevalence of promotional bias reduce their educational value. There is an immediate necessity for standardized, evidence-based, and unbiased educational resources to enhance patient understanding and help with informed decision-making in prostate cancer diagnosis.
Keywords
Introduction
Prostate cancer is one of the most common cancers affecting men globally, and early detection is vital for enhancing prognoses. Prostate biopsy is the definitive standard for diagnosing prostate cancer, with transperineal biopsy (TPB) gaining popularity recently due to its lower infection risk and improved cancer detection rates compared to the conventional transrectal method.1,2 TPB is conducted through accessing the prostate via the perineal skin, frequently using ultrasound guidance, which avoids the rectal flora and reduces the likelihood of post-biopsy infections. 3 Although numerous professional guidelines support the use of TPB, particularly in patients with previous unfavorable transrectal biopsies or increased infection risk, the operation necessitates specialized training, equipment, and patient preparation.4,5 Consequently, patients frequently search online information to have a comprehensive understanding of the surgery, including its risks and advantages. YouTube is one of the most visited internet sites, providing a variety of health-related content. Nonetheless, due to YouTube's absence of editorial oversight or professional evaluation, the reliability and accuracy of medical content on the platform may differ significantly. 6 The aim of our study was to comprehensively assess the quality and reliability of YouTube videos about transperineal prostate biopsy (TPB). Previous research has assessed the quality of YouTube videos relating to various urological operations, including transrectal biopsy and prostatectomy.7,8 To our knowledge, no comprehensive study has specifically evaluated the quality and reliability of movies concerning TPB. We assessed video quality and reliability by analyzing duration, view count, likes, upload time, and the category of the video producer, utilizing the mDISCERN scale and The Global Quality Scale (GQS). This study aims to assist patients and professionals in obtaining accurate data concerning videos related to the TPB procedure.
Materials and methods
Study design
Our study has received approval from the Ethics Committee of the University of Health Sciences, Ankara Etlik City Hospital (AEŞH-BADEK2-2025-664-18/11/2025). A systematic search of YouTube was conducted on May 18, 2025 in English, using the keywords “transperineal prostate biopsy,” “TP biopsy,” and “perineal prostate needle biopsy.” This research was performed at the Ankara Etlik City Hospital, Department of Urology, University of Health Sciences. The project was completed within 2 months of initiating the YouTube video analysis. A study was performed on the videos chosen for May 18, 2025, because to their daily variability. During this timeframe, we finalized the video assessments, performed the statistical analysis of the manuscript, and composed the final English draft. The search was performed in incognito mode to avoid personalization bias. Due to the lack of a specific consensus regarding sample size, the sample sizes of the studies in the literature were considered. The first 60 videos sorted by relevance were screened, and 50 videos were ultimately selected for analysis, aligning with sample sizes used in previous video quality studies.9,10
Inclusion and exclusion criteria
Only English-language videos uploaded between April 2019 and April 2025 were included. Duplicate, unrelated, non-English, or soundless videos were excluded. Videos concerning transrectal prostate biopsy were excluded.
Evaluation of data
All videos were independently evaluated by two board-certified (Fellow of the European Board of Urology) urologists (Fatih Sandıkcı and Mehmet Altan), both experienced in prostate biopsy procedures. Reviewer calibration was ensured by referencing the latest EAU Guidelines on Prostate Cancer (2025) before video assessment. For each video, the following data were recorded: duration (in seconds), number of views, likes, upload date, and creator category (academic professional, non-academic professional, patient, medical company, or others).
The GQS is used to evaluate quality, with a range from 1 (poor) to 5 (excellent). GQS was created by A. Bernard and colleagues. It was designed as a 5-point measure to assess online information resources. The minimum score is 1, and the maximum score is 5. A rating of 4 or 5 indicates that the source is of superior quality. Although 3 points is deemed adequate, resources rated at 1 or 2 points are regarded as low quality. 11
Reliability was evaluated using the modified mDISCERN scale. This scale contains five yes/no questions. Each “yes” response is awarded 1 point. If not, it receives 0 points. This method allows for a maximum of 5 points for reliability. This evaluation system assesses the movie for bias and objectivity, reliability, clarity, citations, and additional resources. Videos rated 5 are deemed high-reliability, those rated 3 or 4 are classified as moderate-reliability, and videos rated 1 or 2 are categorized as low-reliability.12,13
Statistical analysis
All data were analyzed using SPSS Version 22.0 (SPSS Windows 22.0, IBM Corporation, USA). The data distribution was assessed using the Kolmogorov-Smirnov test. The data was determined to be regularly distributed. We applied the intraclass correlation coefficient test (Inter-rater reliability was assessed using a two-way random-effects, absolute-agreement, single-measures ICC(2,1)) to evaluate inter-observer agreement for mDISCERN and GQS values. Continuous variables are expressed as mean ± standard deviation and range (minimum–maximum). Numerical values and percentages were used for category variables. The standard deviation for statistical significance was established at p < .05, with results reported at a 95% confidence level (95% CI; “clearance 95%”). The Pearson correlation test was applied to assess the correlation between video resources and reliability and quality evaluation scales. Additionally, the Pearson Correlation test was used to examine the correlation between video resources and video parameters (duration, view count, like count). Statistical significance was evaluated as p < .01.
Results
All 50 analyzed videos related to TPB, with no exclusions beyond the preliminary screening. The mean video duration was 412 ± 175 s. The average number of views per video was 8950 ± 10,780, amounting to around 447,500 views in total across all videos. The mean number of likes per video was 63, with a range from 2 to 305. Regarding authorship, 60% (30/50) of the videos were generated by healthcare practitioners, whereas 30% (15/50) were produced by academic organizations. Commercial or institutional promotion appeared in 10% (5/50) of the videos. The predominant subjects addressed were procedural stages (68%), types and administration of anesthetic (52%), comparison of infection risk with transrectal biopsy (50%), cancer detection rates (46%), and patient comfort and pain control (40%). The video's information is summarized in Table 1. The mean GQS score was 2.96 ± 0.77. The GQS distribution was as follows: 10% (5/50) rated excellent (score 5), 34% (17/50) good (score 4), 38% (19/50) moderate (score 3), and 18% (9/50) poor or very poor (scores 1 or 2). The GQS scores are summarized in Table 2.
Statistical descriptive parameters related to videos.

The standard deviation for statistical significance was established at p < .05, with results reported at a 95% confidence level (95% CI; “clearance 95%”).
Global quality scale (GQS) scores.

*p < .05, with results reported at a 95% confidence level (95% CI; “clearance 95%”)
The mean mDISCERN score was 2.1 ± 0.9, with only 14% (7/50) of videos scoring 4 or higher, indicating moderate to high reliability. No videos cited peer-reviewed sources, and only 18% of the videos presented content free from promotional bias or subjective claims. The mDISCERN scores are summarized in Table 3. Inter-rater reliability was evaluated using a two-way random-effects, absolute-agreement, single-measures intraclass correlation coefficient (ICC(2,1)). The results demonstrated significant reliability for GQS, ICC(2,1) = 0.893, 95% CI [0.818–0.938], p < .05, and for mDISCERN, ICC(2,1) = 0,861 (95% CI: 0.795–0.898) indicating good-to-excellent coherence.
mDISCERN scores summary and inter-rater reliability.
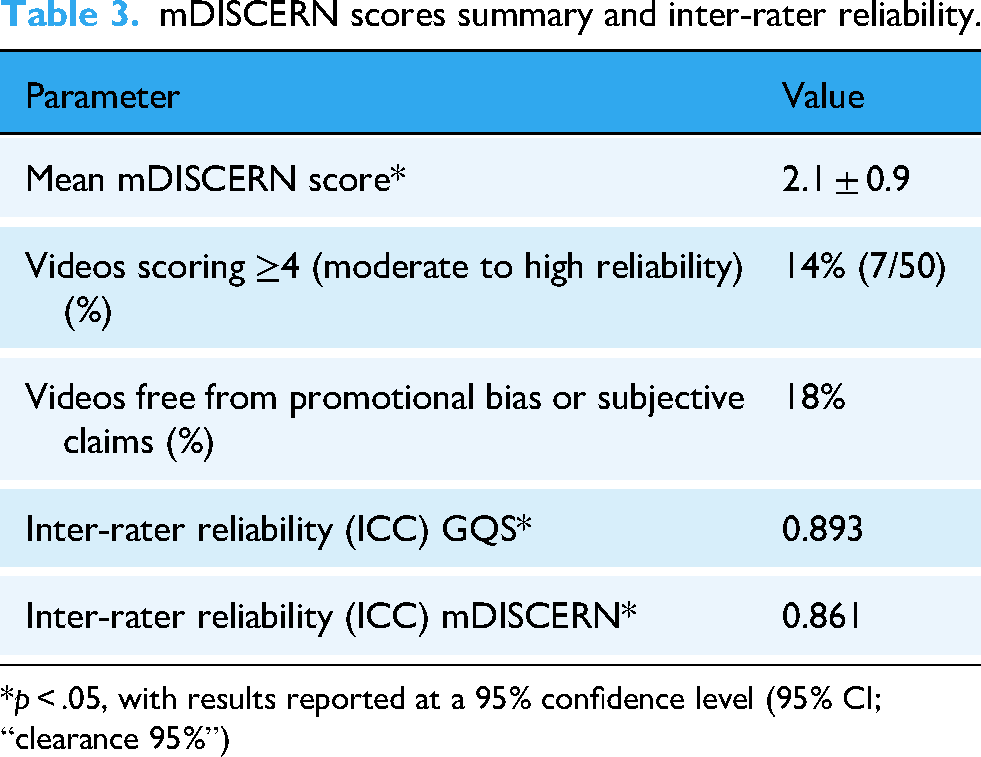
*p < .05, with results reported at a 95% confidence level (95% CI; “clearance 95%”)
The correlation between video resources and GQS scores was assessed. A positive correlation was observed (correlation coefficient [CC]: 0.831). A beneficial correlation was found between video resources and mDISCERN scores (CC: 0.613). The correlation between video sources and video parameters was evaluated as well. A beneficial correlation was found between video sources and the number of likes and views (CC: 0.645 and CC: 0.530, respectively). However, no correlation was detected between video durations and video sources (CC: 0.14).
Discussion
This study thoroughly evaluated 50 YouTube videos regarding TPB, an approach increasingly used for prostate cancer diagnosis. Our analysis offers significant insights on the quality, reliability, and content characteristics of publicly accessible videos, frequently used by clinicians, patients, and educators in search of knowledge. Our findings indicate that, while a minority of videos had excellent quality and reliability, the majority had no evidence of peer-reviewed references and exhibited moderate to low educational value.
The mean video duration was almost 7 min (412 ± 175 s), indicating a reasonable length that facilitates sufficient covering of procedural details while minimizing viewer fatigue. This duration correlates with prevalent instructional material trends on YouTube, which combine informational value with viewer involvement. Conversely, studies in the literature regarding video duration have also shown that longer video durations are more effective as educational material. In their study, Baturu et al. evaluated the contribution of laparoscopic radical nephrectomy videos on YouTube to education. The videos were divided into two groups based on duration. The average duration of the videos was 8.9 ± 4.3 min in Group 1 and 52.02 ± 31.09 min in Group 2 (p < .001). The number of views was 1029 (4–45,306) in Group 1 and 741 (2–12,202) in Group 2, indicating that short videos were viewed more frequently. However, when the videos were evaluated separately, it was concluded that the Video Power Index, calculated based on the view and like rates, was higher for longer videos, and these videos were watched more. It was concluded that the total GQS score was higher in Group 2 (long videos) and that long videos were more beneficial as educational material. 14
The number of views per video varied widely, averaging 8950 but ranging considerably, as indicated by the high standard deviation (±10,780). The total cumulative views of roughly 447,500 demonstrate significant public interest in the TPB procedure. However, this variation in viewership suggests that not all videos reach an equal audience size, which may be influenced by differences in content quality, presentation, search engine optimization, or uploader reputation. Videos with higher view counts inevitably have a greater impact on public understanding and perception, emphasizing the importance of ensuring that these widely viewed videos maintain a high standard of accuracy and comprehensiveness.
Engagement metrics such as likes also showed variability, with an average of 63 likes per video and a range from 2 to 305. Although these numbers suggest some degree of audience interaction and approval, the relatively low like counts for many videos may reflect passive consumption or the inherently informational nature of medical videos, which generally evoke less overt audience response than entertainment content.
Regarding the origin of these videos, 60% were created by healthcare professionals and 30% by academic institutions, which indicates positive in terms of content reliability. The inclusion of commercial or institutional promotion in 10% of videos, however, presents possible issues with bias. Although content from healthcare experts and academic institutions are frequently considered legitimate and evidence-based, promotional materials may occasionally favor marketing goals above objective teaching. This combination of sources emphasizes the necessity for viewers to correctly assess the information provided. Selvi et al. assessed the reliability of YouTube videos as a source for testicular self-examination. The authors categorized the 123 videos included in the study into two groups: useful data (n = 78, 63.4%) and misleading data (n = 45, 36.6%). The findings indicate significant inter-rater reliability across all evaluations. The group exhibited elevated rates regarding reliability, quality, and comprehensiveness, with a substantial amount of views, daily views, and likes. Dislike counts were assessed as elevated in Group 2. However, no difference was observed between the two groups for video duration, time allocated on YouTube, and comments. In the first group, the majority of the loading sources comprise universities, professional organizations, non-profit physicians, and physician groups, accounting for 23.1%. This circumstance enhances the reliability of the video. This rate is 3 times lower in the second group. Among the videos posted by individual users, 22 from the first group were contributed by individuals diagnosed with testicular cancer. Nevertheless, this number was discovered to be four members of the cohort of misinformation. 15 Rodriguez et al. assessed the quality of YouTube videos about incontinence post-cancer surgery. A strong association was identified among the five quality measures (mDISCERN, GQS, Journal of the American Medical Association, patient education materials assessment tool, and the medical quality video evaluation tool), demonstrating their efficacy in evaluating the quality of health information. The assessment of YouTube videos consistently indicated superior quality. The source is crucial for quality assessment, and the resources of health and academic institutions are rather secure. 16
The major subject matter was the procedural steps of the transperineal biopsy, included in 68% of the videos. This emphasis is acceptable as visual and extensive clarifications of the technique enhance the education of both patients and healthcare professionals. Types and administration of anesthesia were discussed in slightly more than half of the videos (52%), indicating prevalent concerns about patient comfort and procedural discomfort. Infection risk comparisons with the conventional transrectal biopsy method were discussed in 50% of the text, which is vital due to the clinical significance of infection prevention in prostate biopsy operations. Nevertheless, insufficient focus was allocated to cancer detection rates (46%) and patient comfort or pain management (40%), suggesting that critical clinical results and patient experience features may not be uniformly reported. Incorporating this information is essential for equipping patients with a thorough awareness of expectations and supporting joint decision-making. The quality of the videos, as assessed by the GQS, averaged 2.96 ± 0.77, suggesting moderate overall quality. The distribution of scores showed that only 10% of videos were rated excellent (score 5), with the majority falling into good (34%) or moderate (38%) categories. Alarmingly, 18% were rated as poor or very poor (scores 1 or 2). This variability indicates that while some videos provide clear, well-structured, and informative content, a considerable number lack depth, clarity, or production value. Poor-quality videos may present incomplete or confusing information, which could mislead viewers or result in misunderstanding the procedure's risks and benefits. Given the potential influence of such content on patient knowledge and decision-making, this is an important concern. Zaliznyak et al., in their study on newborn male circumcision videos on YouTube, reported similarly low overall quality scores (mDISCERN: 2.9 ± 0.7, GQS: 2.9 ± 1.1), consistent with our findings in TPB videos. Both studies highlight a concerning prevalence of low-quality content and potential bias on YouTube. 17 In a recent systematic review, it was reported that the majority of studies on YouTube urological content showed poor quality results, consistent with our findings of moderate to low quality in TPB videos. Both the review and our study emphasize the need for improved standards and guidelines to enhance the reliability of online urological educational materials. 18 Our results are consistent with the literature, confirming the generally moderate to low quality of urological videos on YouTube.
Assessment of reliability using the mDISCERN tool further highlighted limitations. The mean mDISCERN score was low at 2.1 ± 0.9, with only 14% of videos scoring 4 or higher, indicating moderate to high reliability. Notably, no videos referenced peer-reviewed scientific sources or clinical guidelines, which undermines their credibility and the trust that patients and clinicians can place in them. Moreover, only 18% of the videos were free from promotional bias or subjective claims, suggesting that a majority of content might contain elements that sway the viewer's perception, intentionally or unintentionally. This lack of rigorous referencing and potential bias raises concerns about misinformation or partial information, which could ultimately affect clinical outcomes and patient satisfaction. García-Cano-Fernández et al. reported that over 60% of Spanish-language bladder cancer videos on YouTube were of low quality according to mDISCERN scores, which aligns with our finding of predominantly moderate to low reliability videos. Both studies highlight the increased risk of misinformation due to insufficient content quality and underscore the urgent need for quality control and guidance in online urological educational materials. 19 Similar to the Fernández study and our findings, Di Bello et al. reported “fair” overall mDISCERN scores for YouTube videos on immunotherapy for urological tumors, highlighting significant misinformation and limited content reliability. This aligns with our findings of generally low to moderate mDISCERN scores in TPB videos, underscoring the widespread issue of inconsistent quality in urological video content. Both studies emphasize the urgent need for improved quality control to ensure accurate and trustworthy patient information online. 20
The high inter-rater reliability found in our assessments, with intraclass correlation coefficients of 0.893 for GQS and 0.861 for mDISCERN, strengthens the validity of our findings. These results confirm consistent evaluations across reviewers and support the use of these tools in analyzing online medical educational content.
The increasing dependence on internet platforms for health information, especially among patients who are newly diagnosed or planning prostate biopsy, emphasizes the importance of our findings. TPB is a more recent technique than the conventional transrectal method, prompting people to search for web videos to learn more about the surgery, its benefits, and associated difficulties. The poor quality and low reliability ratings of available videos show the potential for incomplete or misleading patient education from these sources. Healthcare professionals must acknowledge that patients may encounter various levels of information quality and may have misunderstandings that result from worse material. To deal with this, providers should take a proactive approach by promoting high-quality, approved videos or creating institutional training resources available to patients. Professional medical groups and academic institutions have to develop standardized, evidence-based video material that openly cites guidelines and scientific evidence. These efforts would guarantee that patients obtain clear, accurate, and unbiased information, thereby improving informed consent and minimizing anxiety related to the biopsy procedure. Our study has limitations that warrant consideration. We assessed videos at a single time point, while content on platforms like YouTube is dynamic, with new videos regularly uploaded and existing ones updated or removed. Thus, our findings represent a snapshot rather than a comprehensive or permanent picture of available information. Our study did not evaluate the influence of algorithmic bias potentially stemming from the platform's recommendation and ranking systems on the sample and results. Furthermore, it has not yet been subjected to independent peer review, and the methodological choices are available for external confirmation. We did not conduct a systematic analysis of audience responses; therefore, the aspects of reception and interaction were not specifically investigated. Additionally, while GQS and mDISCERN provide structured frameworks for evaluation, they cannot capture the nuances of viewer comprehension or the videos’ influence on patient behavior and decision-making. Future research should focus on how patients perceive and utilize these videos, their impact on knowledge and anxiety levels, and whether they alter treatment choices.
Further studies could also investigate interventions aimed at improving the quality and reliability of online medical videos, such as collaborations between clinicians, media experts, and patient advocates to produce and disseminate high-quality educational content. The potential establishment of certification systems or quality seals for medical videos could assist viewers in quickly identifying trustworthy sources, enhancing the overall standard of health information on public platforms.
Conclusion
Our evaluation of YouTube videos related to TPB reveals significant variability in content quality and reliability. Although most videos are produced by healthcare professionals, the absence of peer-reviewed references and the presence of promotional bias in many videos limit their educational value. There is a clear need for higher-quality, evidence-based, and unbiased video content to support patient education and facilitate shared decision-making in prostate cancer diagnostics. In accordance with the findings, rather than simply saying “the content is harmful,” specific measures should be done. Clinicians must guarantee the documentation of hazardous content and the formulation of secure content assessments. Content makers must guarantee transparency about identity and interests, use clear and comprehensible language, and focus on content development that corresponds to standards such as mDISCERN/GQS. Platforms, conversely, must emphasize verified sources and guarantee the regularity of resources together with the regulation of update dates. As digital platforms continue to shape health information dissemination, ensuring the accuracy and trustworthiness of online resources remains a critical priority for the medical community.
Footnotes
Author note
Since this study is based on online digital data, patients do not participate in the study either directly or indirectly. On the YouTube platform, all social media content is publicly accessible and free for data collection purposes. Furthermore, viewing the movies does not require individual consent. The relevant video content was accessed according to with the YouTube platform's terms of service.
Ethical approval
Ethics committee approval date and number: 18/11/2025-AEŞH-BADEK2-2025-664.
Patient consent statement
The consent statement form was obtained from all patients.
Author contributions
FS: Project development. FS and MA: Data collection (Transperineal prostate biopsy video search on YouTube). FS and MA: Data analysis (video evaluation). FS and MA: Manuscript writing and editing. All authors reviewed the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Available.
Clinical trial registration
The present study does not have a clinical trial registration number because it was a retrospective study nature.