
Abstract
Objective
Understanding the factors that shape public support for tobacco control policies is essential for effective legislation. This study aims to examine how online and offline health information seeking behaviors (HISB) among chronic disease patients influence their support for tobacco control policies.
Methods
Using data from a national survey in China (N = 745), this study developed and empirically tested a parallel mediation model examining the direct associations between online and offline HISB and support for tobacco control policies, as well as the indirect paths through perceived social disapprove of smoking and negative smoking outcome expectancies.
Results
Results indicated that online HISB was positively associated with support for tobacco control policies, both directly and indirectly through increased perceived social disapproval of smoking and negative smoking outcome expectancies. In contrast, offline HISB showed no direct association with policy support and exhibited an indirect negative pathway through reduced negative smoking outcome expectancies.
Conclusions
Findings highlight the positive role of online HISB, and the potential negative role of offline HISB, in shaping support for tobacco control policies. We therefore recommend promoting online channels for health information seeking, especially among adults aged 40 to 70 and those from lower socioeconomic backgrounds, who rely more on offline media and face higher chronic disease risk. Online campaigns should emphasize the social unacceptability of smoking and negative smoking outcome expectancies. In parallel, stricter regulation of pro-tobacco content in offline media, especially subtle promotional exposure, is needed, along with increased frequency and depth of antitobacco coverage in traditional media.
Keywords
Introduction
Tobacco is the leading preventable cause of death in China, claiming one million lives annually. 1 Without substantial improvements in smoking cessation efforts, tobacco-related deaths are projected to reach two million by 2030 and three million by 2050. 2 Moreover, an estimated 68.1% of nonsmokers in China are exposed to secondhand smoke, 3 which contributes to death, disease, and disability. 4 For every seven smokers who die from smoking, one nonsmoker dies as a result of secondhand smoke. 5
Tobacco control policies (e.g. requiring warning labels and raising tobacco taxes) have proven effective worldwide in reducing tobacco use, denormalizing smoking, encouraging cessation, and protecting nonsmokers from secondhand smoke.6,7 Since ratifying the World Health Organization (WHO) Framework Convention on Tobacco Control (FCTC) in 2005, China has made progress in both national and local tobacco control policies. However, obstacles posed by the tobacco industry and the government's ambiguous stance on the tobacco economy have hindered further advancement.2,3 To date, China still lacks comprehensive national legislation, and the enforcement of existing measures remains largely ineffective, as reflected in relatively low tobacco taxes and weak packaging warnings.2,8 In this context, promoting public support for tobacco control policies is essential because it influences political will, which is necessary for effective public health policy implementation. 9
Chronically ill patients, over 500 million in China in 2024, 10 stand to benefit most from tobacco control policies, as smoking and secondhand smoke are key risk factors for many chronic conditions, including hypertension, cardiovascular and pulmonary diseases, diabetes, infections, and cancer. 11 Understanding attitudes toward tobacco control policies among high-risk groups, and the factors that shape these attitudes, can help policymakers design targeted strategies to strengthen public support.
Literature on public health policy indicates that several factors, including media influence, personal values, smoking status, beliefs about substance use, and attitudes toward specific policies, can predict support for health policies.5,6,12–14 Media influence, in particular, plays a crucial role. High exposure to pro-tobacco content, such as price promotions on social media and newspaper coverage that negatively frames smoking bans (effectively pro-tobacco), increases tobacco use and reduces support for smoke-free policies.15–17 In contrast, repeatedly delivered antitobacco campaigns boost public support for restrictions on tobacco industry marketing.18,19 In addition, research also indicates that exposure to mixed messages, both positive and negative, about cigarettes may cause confusion, reduce perceived harms, and ultimately undermine support for cigarette regulation. 20
In recent years, health information seeking behaviors (HISB) have garnered significant attention from communication scholars, particularly regarding their influence on public health beliefs and behaviors.21–23 Chronic disease patients are particularly motivated to seek health information relevant to their personal experiences and chronic conditions.24–26 This often exposes them to antitobacco content such as tobacco and secondhand smoke risks, 24 which can influence their beliefs and behaviors. Empirical evidence shows a positive association between HISB and the intention to quit smoking, 27 reduced alcohol consumption, 28 and other preventive behaviors.22,29 Nevertheless, whether HISB can predict public support for tobacco control policies among chronic disease patients, as well as the psychological mechanisms through which HISB may shape such support, remains underexplored. Furthermore, chronic disease patients seek health information through diverse channels, including online platforms such as social media (e.g. engaging in online patient communities) and search engines (e.g. searching for tobacco-related health risks). 15 Offline sources such as newspapers and television are also commonly used, particularly among older adults and individuals with lower socioeconomic status. 17 Media selection (e.g. media features and individuals’ engagement patterns) may shape the communication process in different ways. 30 However, whether online and offline HISB produce similar or distinct effects on policy attitudes remains unclear. Therefore, this study aims to examine (1) the associations of online and offline HISB with support for tobacco control policies and (2) the psychological mechanisms underlying these associations.
Conceptual framework
The Stimulus–Organism–Response (S–O–R) framework 31 provides a structured and concise model for theorizing how HISB influences chronic disease patients’ support for tobacco control policies. This model posits that stimuli (S) originating from the external environment can activate internal organismic processes (O), including cognitive states, which in turn give rise to psychological or behavioral responses (R). Rooted in environmental psychology, the S–O–R model has been extensively applied in health communication research.32–34
In this study, support for tobacco control policies is conceptualized as the response (R), consistent with prior work that treats policy attitudes as outcomes shaped by cognitive processes.5,13,18–20 Social norms (e.g. perceived social disapproval of smoking) and outcome expectancies serve as the organism (O), reflecting the internal cognitive states through which external stimuli exert their influence. These two variables are commonly used as mediators to capture the psychological mechanisms examined in preventive health research. For example, Quick et al. 5 demonstrated that social norms and attitudes functioned as parallel mediators linking knowledge about the risks of environmental smoke to public support for clean-air policies.
HISB can be regarded as an environmental stimulus (S) as it exposes individuals to extensive health-related information that may initiate subsequent cognitive evaluations and attitudinal responses. 34 Notably, with the rise of new communication technologies such as the Internet, vertical offline media (e.g. television and newspapers), which deliver content through one-way, top-down communication, 35 are declining in influence, while horizontal online media (e.g. social media and search engines), serving diverse ideological and personal interests, are gaining prominence.36–38 Consequently, we separately examine the effects of online and offline HISB on the outcome variables (Figure 1).

Conceptual model.
Hypotheses and research question
HISB refer to the active acquisition of health-related information through various methods and channels across diverse health contexts. 39 Prior research has documented a positive association between HISB and support for public health policies. For example, Wang et al. 40 showed that HISB, as a common eHealth activity, can promote support for alcohol restriction policies. Similarly, Vázquez-Otero et al. 41 suggested that low support for tobacco control policies among individuals from lower socioeconomic backgrounds may result from limited access to health information.
HISB emphasizes individuals’ motivation and goal orientation in the process of acquiring information. 42 Online platforms support this process by enabling chronic disease patients to seek content aligned with their personal health concerns (e.g. tobacco and other risk factors). 43 As such, online channels are increasingly popular, with 79% of Chinese individuals frequently seeking health information online, 44 further amplifying their influence on public opinion.
In comparison, offline media disseminate standardized content through top-down communication, offering limited opportunities for audience-driven information selection. 45 Moreover, in China, offline media provide limited coverage of antitobacco information.8,46,47 For instance, an analysis of nearly 600 health-related articles from six major Chinese official newspapers found that smoking accounted for only 1.4% of the coverage. 47 In this context, whether offline HISB can enhance chronic disease patients’ support for tobacco control policies remains unclear. Literature on HISB focuses primarily on online platforms, with comparatively little attention given to offline HISB.
Given the distinct characteristics of online and offline HISB, we propose the following hypothesis and research question:
Online HISB is positively associated with support for tobacco control policies among chronic disease patients.
What is the association between offline HISB and support for tobacco control policies among chronic disease patients?
In the domain of risk communication, social norms and outcome expectancies are established predictors of risk behaviors, as highlighted by the Theory of Reasoned Action 48 and Social Cognitive Theory. 49 An increasing number of studies have examined these constructs as mediators linking exposure to risk-related information to behavioral outcomes.5,50,51
HISB may also indirectly impact policy support through attitudinal and normative psychological processes. Outcome expectancies denote individuals’ beliefs about the anticipated consequences, positive or negative, of engaging in a behavior. 52 Motivated chronically ill patients often search for risk-related factors relevant to chronic disease management and engage in deeper cognitive processing, which, in turn, facilitates the development of negative outcome expectancies regarding smoking. 53 Perceived injunctive norms of smoking reflect individuals’ beliefs about whether significant others approve or disapprove of smoking. 54 Exposure to health information has been associated with lower social acceptability of smoking, drinking, and other unhealthy behaviors.55,56 This is consistent with the Presumed Influence Hypothesis, 57 which posits that individuals tend to assume that others’ views will be shaped in accordance with the media messages they encounter. Previous studies further suggest that negative outcome expectancies and perceived social disapproval of smoking are positively associated with support for tobacco control policies. 58 We therefore propose the following hypothesis and research question:
Perceived social disapproval of smoking and negative smoking outcome expectancies mediate the relationship between online HISB and support for tobacco control policies.
Can perceived social disapproval of smoking and negative smoking outcome expectancies mediate the relationship between offline HISB and support for tobacco control policies?
Methods
Sample
Research ethics approval was obtained from the authors’ institution prior to data collection. This study followed the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) reporting guideline. From October 2024 to January 2025, we conducted an anonymous online survey to examine individuals’ health-related communication, attitudes, and behaviors. The survey was administered through Kantar (www.kantar.com), one of the world's largest market research and data analytics companies. Kantar operates a broad online survey panel that is widely used in academic and commercial research and can recruit large, diverse samples across China.
A total of 2000 respondents (≥18 years old) from all 31 provinces (or equivalent) in mainland China were recruited from Kantar's China panel to participate in this survey. Standard participation incentives were provided. Quota sampling was utilized, aligning with age and gender demographics from the Seventh National Population Census 59 conducted by the National Bureau of Statistics of China. Specifically, gender quotas followed the census distribution of 51.24% male and 48.76% female, and age quotas were set using the proportions of adults aged 15 to 59 (63.35%) and 60 years or above (18.70%) as benchmarks. Within each quota cell, random selection was applied to reduce sampling bias.
As the present study focused on adults with chronic diseases, respondents were subsequently filtered based on age (≥18 years) and self-reported medical conditions. This resulted in a final sample of 745 participants, each having at least one of the following chronic conditions: (1) diabetes or high blood sugar; (2) high blood pressure or hypertension; (3) heart conditions such as heart attack, angina, or congestive heart failure; and (4) chronic lung disease, asthma, emphysema, or chronic bronchitis. Cases with missing data (<1%) were excluded listwise in the regression analyses.
Measures
Support for tobacco control policies, was measured using five items assessing respondents’ level of support for specific tobacco control measures.6,60 Example items include: “Stores should be required to keep tobacco products out of sight at checkout counters” and “Just like violence and pornography, movies containing smoking scenes should also be regulated to prevent children and adolescents from being exposed to smoking imagery.” Responses were rated on a 5-point Likert scale ranging from 1 (strongly oppose) to 5 (strongly support), and a composite score was calculated by averaging the items (Cronbach's α = .746).
Online and offline HISB, were assessed by the frequency of seeking health information through various media channels in the past year. Online sources included (1) news apps, (2) health-related apps, (3) social media, and (4) search engines. 61 Offline sources included (1) newspapers, (2) radio, and (3) television. 62 Each item was rated on a 5-point scale from 1 (never) to 5 (often). Composite scores for online (Cronbach's α = .760) and offline (Cronbach's α = .743) HISB were computed by averaging the respective items.
Perceived social disapproval of smoking, was measured by the item: “Overall, do you think most people disapprove of smoking?”, 63 using a 5-point Likert scale from 1 (definitely not) to 5 (definitely yes).
Negative smoking outcome expectancies, was assessed by two items evaluating agreement with negative outcomes of smoking, including: “Smoking is as addictive as other drugs like heroin or cocaine” and “Inhaling secondhand smoke causes lung cancer.”64,65 Responses ranged from 1 (strongly disagree) to 5 (strongly agree), and a composite score was calculated by averaging the items (Cronbach's α = .713).
All focal variables were adapted from previously published studies and have demonstrated robust validity in prior research. The specific items used in this study are reported in the Supplemental materials.
Sociodemographic variables, past 30-day cigarette and alcohol use, and psychological distress were included as covariates due to their potential influence on support for tobacco control policies.6,13,20 Sociodemographic variables included gender (male = 0, female = 1), age (in years), and sexual orientation (heterosexual = 0, sexual minority = 1). Area of residence was classified as urban (including provincial capitals, prefecture-level cities, county-level cities, and counties = 0) or rural (including townships and villages = 1). Education was measured on a six-point scale (1 = primary school or below, 2 = junior high school, 3 = high school, 4 = vocational school, 5 = college, and 6 = master's degree or above). Employment status was coded as unemployed = 0 and employed = 1. Annual household income was reported in six categories (1 = ¥29,999 or less; 2 = ¥30,000–¥79,999; 3 = ¥80,000–¥149,999; 4 = ¥150,000–¥499,999; 5 = ¥500,000–¥999,999; 6 = ¥1,000,000 or more). Marital status was coded as divorced, widowed, separated, or single = 0 and married and living with a romantic partner = 1.
Psychological distress was assessed using the Patient Health Questionnaire-4 (PHQ-4), a reliable and valid scale for emotional health outcomes that has been widely used in prior research.66–68 Respondents were asked how often they had been bothered by four emotional problems over the past 2 weeks, with sample items including “felt down, depressed, or hopeless” and “felt nervous, anxious, or on edge.” Responses were recorded on a four-point Likert scale (1 = not at all, 2 = some of the days, 3 = several days, 4 = nearly every day) and averaged to create a composite scale (Cronbach's α = .771).
Past 30-day cigarette use was assessed by asking respondents how many days in the past 30 days they had smoked at least one cigarette, and past 30-day alcohol consumption was assessed by asking respondents how many days in the past 30 days they had consumed any alcoholic beverages. Responses for both variables were recorded as the number of days (0–30) and treated as continuous variables in the analysis.
Data analysis
Data analysis was performed by SPSS (v27). First, descriptive statistics were used to summarize sample characteristics, with means and standard deviations reported for continuous variables and frequencies and percentages reported for categorical variables. Second, Shapiro–Wilk tests were conducted to assess the normality of the focal variables, after which Spearman's rank-order correlations were used to examine associations among them. Based on our conceptual framework, which specifies two mediators operating in parallel rather than sequentially, we subsequently employed the PROCESS macro 69 (model 4) to test the parallel mediation effects of perceived social disapproval of smoking (mediator 1) and negative smoking outcome expectancies (mediator 2) on the relationship between online and offline HISB (independent variables) and support for tobacco control policies (dependent variable). Mediation effects were assessed using bootstrapping (5000 samples) with 95% confidence intervals (CIs). Finally, a post hoc power analysis was conducted using G*Power (version 3.1) to assess whether the final sample size provided sufficient statistical power for the regression models.
Results
Preliminary analysis
As presented in Table 1, the average age of participants is 42.75 years, with males comprising 47.1% of the sample. Over half of the participants have attained a college degree or higher, and more than 80% are currently employed. Regarding annual household income, approximately 50.2% fall within the ¥150,000 to ¥499,999 range (approximately $21,429 to $71,429). Additionally, the vast majority are in a partnership or marriage (93.4%), and reside in urban areas (96.2%).
Descriptive statistics (N = 745).

Past 30-day cigarette use and past 30-day alcohol consumption are reported as the number of days in the past 30 days (0–30). HISB; health information seeking behaviors; SD: standard deviation.
In terms of HISB, approximately 60% of participants reported frequently or very frequently searching for health information through online platforms. In contrast, only about 30% reported doing so via offline media.
Shapiro–Wilk tests indicated that the distributions of the key variables deviated from normality (all p < .001). Spearman's rank-order correlation analyses revealed that, as shown in Table 2, online HISB, perceived social disapproval of smoking, and negative smoking outcome expectancies were significantly and positively correlated with support for tobacco control policies, whereas offline HISB was not significantly correlated with any of these variables.
Spearman's rank-order correlation matrix.

*p < .05; **p < .01; ***p < .001.
HISB: health information seeking behaviors.
Based on the outcome regression (R2 = 0.246, 15 predictors, α = 0.05), the post hoc power analysis indicated very high statistical power (> 0.99), confirming that the sample was sufficient to detect the observed effects.
Mediation analysis
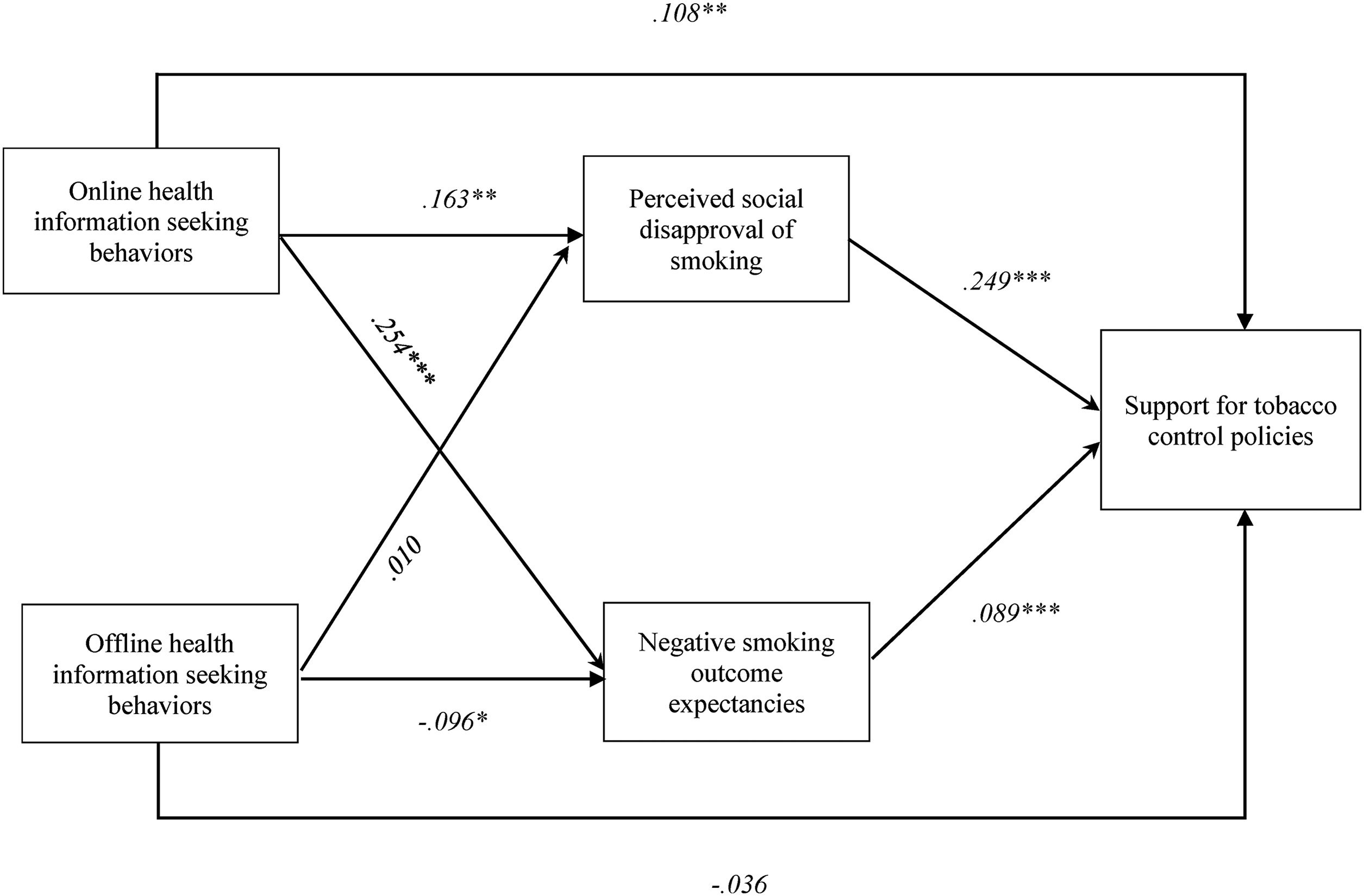
H1 predicted a positive direct association between online HISB and support for tobacco control policies. As shown in Table 3 and Figure 2, this direct relationship was statistically significant (b = 0.108, p < .01), indicating that chronic disease patients who engage more frequently in online HISB are more likely to support tobacco control policies. Therefore, H1 was supported.
Results of the mediation model.
Summary of mediation effects.

All model controlling for gender, age, sexual orientation, area of residence, education, employment status, annual household income, marital status, past 30-day cigarette use, past 30-day alcohol consumption, and psychological distress.
CI: confidence interval; HISB: health information seeking behaviors; STCP: support for tobacco control policies.
RQ1 examined the direct association between offline HISB and policy support. The results revealed no statistically significant relationship (b = –0.036, p > .05), suggesting that offline HISB alone does not predict support for tobacco control policies among chronic disease patients.
H2 was supported: both perceived social disapproval of smoking (b = 0.040, 95% CI [0.015, 0.068]) and negative smoking outcome expectancies (b = 0.014, 95% CI [0.007, 0.023]) significantly mediated the relationship between online HISB and policy support. Specifically, more frequent HISB was associated with stronger beliefs that significant others disapprove of smoking (b = 0.163, p < .01) and more negative smoking outcome expectancies (b = 0.254, p < .001), both of which, in turn, were related to greater support for tobacco control policies (b = 0.249, p < .001 and b = 0.089, p < .001, respectively).
RQ2 examined the mediating effects of perceived social disapproval of smoking and negative smoking outcome expectancies on the relationship between offline HISB and policy support. The analysis revealed a significant indirect effect via negative smoking outcome expectancies (b = –0.009, 95% CI [–0.019, −0.001]), whereas the path through social disapproval of smoking was not significant (b = 0.002, 95% CI [–0.016, 0.021]). This indicates that offline HISB may lower policy support primarily by reducing negative smoking outcome expectancies.
Discussion
Guided by the S–O–R framework and using survey data from 745 chronic disease patients in China, this study developed and tested a mediation model examining how online and offline HISB influence support for tobacco control policies. Results showed that, among chronic disease patient, online HISB effectively promotes support for tobacco control policies, both directly and indirectly by enhancing perceived social disapproval of smoking and negative smoking outcome expectancies. In contrast, offline HISB does not demonstrate a direct association with policy support and shows a negative indirect effect through weakened negative smoking outcome expectancies. These findings extend existing research by highlighting the distinct roles of online and offline information-seeking channels in shaping policy attitudes, and they offer practical implications for designing communication strategies to enhance public support for tobacco control.
Roles of online HISB in promoting policy support
The findings indicate that online HISB is directly associated with support for tobacco control policies among chronic disease patients in China. This is consistent with existing literature that highlights the constructive role of motivated, goal-oriented information seeking behaviors in preventive health.22,27,42 Previous research has primarily examined how HISB shapes individual-level health behaviors and outcomes, such as smoking cessation and reduced alcohol consumption. Our findings provide evidence that HISB can also predict positive attitudes toward tobacco control policies at the societal level.
Notably, our findings highlight the role of online HISB, which enable chronic disease patients to access health-related content aligned with their personal concerns. 43 Given that tobacco-related risks are highly relevant to various chronic conditions, 11 online HISB often exposes chronic disease patients to antitobacco information, thereby fostering their support for tobacco control policies.41,70
Furthermore, in line with the S–O–R framework, our findings indicate a normative and attitudinal psychological process underlying the association between online HISB and policy support. Specifically, health information obtained through personalized online platforms serves as the environmental stimulus (S) that enhances chronic disease patients’ understanding of health threats and their implications.28,71 This enhanced understanding triggers internal cognitive processes (O), namely, increased negative smoking outcome expectancies and reinforced perceived social disapproval of smoking,5,53which ultimately shape their attitudes toward tobacco control policies (R). 58
Roles of offline HISB in shaping policy support
In comparison to online seeking, offline HISB exhibits no direct effect on policy support. This discrepancy may be attributed to the characteristics of offline media and the ongoing transformation in media consumption patterns. Offline media disseminate standardized content through top-down communication, offering limited opportunities for audience-driven information selection. 45 Moreover, due to limited space and airtime, the amount of health-related information available in offline media is inherently constrained. 8 This issue is even more pronounced in China. Evidence46,47,72–74 shows that, compared to Western media, Chinese traditional offline media offers sparse and shallow tobacco control reporting, particularly after 2015 when such coverage significantly declined. 75
Furthermore, our findings indicate that approximately 60% of chronic disease patients reported frequently or very frequently searching for health information through online platforms, while only about 30% reported doing so via offline media. This result is consistent with the previous research,43,76 reflecting an ongoing shift in health information acquisition habits from traditional offline channels to online media platforms. As the reach of traditional media continues to decline, their capacity to shape health-related beliefs may be insufficient to produce measurable effects.
However, the results indicate a negative indirect pathway, whereby offline HISB reduces support for tobacco control policies through decreased negative smoking outcome expectancies. This negative indirect effect may also stem from the top-down, institution-driven communication structure of offline media, which allows the tobacco industry to subtly embed pro-tobacco messaging within traditional media content. Although tobacco control gains political support, the Chinese government faces, on this issue, potential conflicts of interest. The State Tobacco Monopoly Administration (STMA) and the China National Tobacco Corporation (CNTC) not only oversee the production and sale of tobacco products but also hold seats on China's FCTC implementation committee.2,3,8,77 This structural arrangement allows the tobacco industry to maintain its exposure in traditional media through relatively subtle means. For example, national awards such as the “Top Ten Trademarks in the Country” and the “National Quality Product—Gold Award” have been granted to cigarette brands, helping to foster a sense of official endorsement and legitimacy in their portrayal by traditional media. 2 Furthermore, A report by the China National Tobacco Control Association shows a 23.3% increase in smoking scenes across 30 popular TV shows in 2021 compared to 2020, with an average of 21 smoking scenes per show. 78 This rise in portrayals may enhance the cognitive accessibility of smoking-related cues among viewers, potentially leading to undesirable cognitive outcomes, such as the perception that smoking is appealing.
Theoretical and practical implications
Theoretically, this study extends research on media channel-specific effects in tobacco control. While the media's role in tobacco control is well-documented, far less attention has been given to comparing the effects of online versus offline HISB. By incorporating both channels into a single model, our findings demonstrate the constructive role of online HISB in promoting support for tobacco control policies, while also revealing the potential indirect negative influence of offline HISB. This offers theoretical insight into how media channel selection shapes the degree to which individuals are influenced by media coverage. 30 Building on this, future research could further compare how online and offline HISB predict other health behaviors and public policy attitudes in preventive health, as well as explore the potential mechanisms underlying these associations.
For practical implications, first, online media can serve as an important platform through which active HISB strengthens chronic disease patients’ support for tobacco control policies. Although online HISB has grown in popularity in recent years, certain groups, particularly adults aged 40 to 70 and individuals from lower socioeconomic backgrounds, still rely more heavily on traditional media than on digital sources.79,80 Given that these groups are also at higher risk for chronic conditions, it is imperative to actively promote the use of online channels, such as social media, health websites, and mobile health applications, for health information seeking among them. Doing so may not only enhance individual-level self-management but also contribute to a broader societal environment that is more supportive of tobacco control.
Second, online campaigns should prioritize strengthening the social unacceptability of smoking and enhancing negative smoking outcome expectancies. Prior research indicates that individuals in low-income countries and those from lower socioeconomic backgrounds in high-income countries tend to show lower support for tobacco control policies.6,41,81,82 This often stems from limited awareness of smoking-related risks and the high social acceptability of smoking. For example, many US adults, especially those with less formal education or more at-risk health behaviors, underestimate the harms of smoking. 81 In addition, in countries such as China and those in the South-East Asia Region, practices like gifting and sharing cigarettes remain widespread and socially accepted.83,84 These patterns underscore the need for online health communication that clearly conveys smoking risks and directly challenges the social acceptability of smoking.
Third, the findings reflect the ineffectiveness of tobacco control communication through offline channels. Given the top-down, one-way communication structure of offline media, stricter regulation of pro-tobacco content, particularly subtle promotional exposure such as smoking scenes in television dramas, is warranted. In addition, increasing both the frequency and depth of antitobacco coverage in offline media is essential. These measures are especially important for populations who depend more on offline media, such as older adults and individuals with fewer socioeconomic resources. Moreover, this offers valuable practical implications for countries with state-owned tobacco industries (e.g. Vietnam), 77 where governmental or economic interests may shape traditional media agendas. In such contexts, attention is needed to the subtle ways in which tobacco-related content in offline media may downplay health risks or implicitly normalize smoking.
Limitations
This study has several limitations that offer directions for future research. First, the use of a cross-sectional survey design limits the ability to establish causal relationships between key variables. Future research could address this issue by employing experimental or longitudinal designs. Second, the measurement of HISB primarily focused on general health content, rather than tobacco-specific information. Future studies may benefit from refining this measure to better examine the distinct impacts of online and offline tobacco-related information seeking behaviors on public opinion toward tobacco control in China.
Conclusions
By testing a parallel mediation model, this study demonstrates the distinct roles of online and offline HISB in shaping support for tobacco control policies among Chinese chronic disease patients. Online HISB promotes policy support both directly and indirectly by increasing perceived social disapproval of smoking and negative smoking outcome expectancies. In contrast, offline HISB does not enhance policy support and may even weaken it by reducing negative smoking outcome expectancies.
Based on these insights, we recommend actively promoting the use of online channels for health information seeking among adults aged 40 to 70 and individuals from lower socioeconomic backgrounds, who continue to rely more heavily on traditional media and are at higher risk for chronic conditions. Online campaigns should emphasize the social unacceptability of smoking and highlight negative smoking outcome expectancies to strengthen public support for tobacco control policies. At the same time, given the top-down and one-way nature of offline media, stricter regulation of pro-tobacco content, particularly subtle promotional exposure, is needed, along with efforts to increase the frequency and depth of antitobacco coverage in traditional media.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076261431847 - Supplemental material for Promoting support for tobacco control: The roles of online and offline health information seeking
Supplemental material, sj-docx-1-dhj-10.1177_20552076261431847 for Promoting support for tobacco control: The roles of online and offline health information seeking by Lunan Xu, Luxi Zhang, Yuzhou Duan, Xi Xia and Xinshu Zhao in DIGITAL HEALTH
Footnotes
Ethical consideration
The questionnaire and methodology for this study was approved by the Human Research Ethics committee of the University of Macau (Project number is SSHRE23-APP013-FSS).
Consent to participate
Informed consent was obtained from all participants prior to their completion of the survey for the data collection.
Consent for publication
Participants were informed that their data would be used for publication purposes, and they provided consent for the publication of the study results.
Author contributions
Guarantor
Xi Xia
Funding
This work was supported by the University of Macau under Grant [CRG2021-00002-ICI and ICI-RTO-0010-2021].
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Data will be made available on request to corresponding author.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.