
Abstract
Objective
The objective of this article is to describe the protocol for a non-randomized pilot study of a theory-driven mobile parenting intervention designed to enhance parental self-efficacy and reduce children's problem behaviors.
Methods
The intervention was developed using the analysis, design, development, implementation, and evaluation (ADDIE) instructional design model. The analysis phase involved a narrative review and application market research to inform the theoretical framework and benchmarking elements. Guided by these findings, the design phase applied Bandura's self-efficacy theory, with behavior change techniques mapped to the four sources of self-efficacy. A beta version will undergo expert validation and small-scale user testing, followed by a non-randomized pilot study with 30 caregivers. Feasibility and possible effectiveness will be evaluated using application usage data, questionnaires, and user interviews.
Results
The analysis phase reviewed 54 studies and 18 parenting-related mobile applications, identifying parental self-efficacy as a central intervention target and highlighting limitations in existing applications. In response, the proposed application was designed to address all four sources of self-efficacy through theory-aligned functions, including behavior tracking, peer support, positive feedback, and personalized education. The development phase is currently underway, and the pilot study is scheduled for May 2026.
Conclusion
This protocol outlines the systematic development of a theory-driven mobile parenting intervention and is expected to inform the feasibility of a self-efficacy–focused digital approach to supporting parents of children with behavioral problems.
Keywords
Introduction
Children undergo rapid developmental transitions that require them to adapt to new environments and adjust their behavior accordingly. These developmental changes often lead to behavioral problems during childhood. 1 Behavioral problems are defined as symptomatic expressions of maladjustment that are considered concerning or undesirable according to the norms of conventional society. 2 The worldwide pooled prevalence of disruptive behavior disorders has been estimated at 5.7% across 27 countries, representing every global region. 3 A study in Korea revealed that 7%–13% of children aged 3–5 years showed behavioral problems, and 3%–4% required professional intervention to manage their issues. 4 Moreover, behavioral problems are particularly prevalent in children with developmental disabilities, affecting 48%–60% of children with intellectual disabilities and 90% of children with autism spectrum disorder. 5
Behavioral problems may be a natural part of developmental changes; however, without proper management, they can have a serious negative impact on children, their families, and society. Children with behavioral problems often struggle to express themselves and understand others’ emotions, which can adversely affect their social adjustment and academic competence.1,6 Children's behavioral problems can also impose physical, psychological, and financial stress on family members, leading to a decline in their quality of life. 7 Furthermore, children's behavioral problems often continue as antisocial behaviors during adolescence, resulting in a substantial social burden. 8 Research conducted in 2004 has estimated that the minimum cost of adolescent problem behaviors amounted to ∼2.25 billion dollars (3 trillion KRW). 9 Therefore, it is essential to identify factors that influence children's behavioral problems and develop targeted interventions to manage them effectively.
Parenting is a key factor influencing children's development, and certain parenting behaviors are regarded as more favorable for addressing children's behavioral issues. Parenting styles are generally categorized as authoritative, authoritarian, permissive, or neglectful.10,11 Authoritarian, permissive, and neglectful parenting behaviors are related to higher levels of externalizing behavior. By contrast, an authoritative parenting style, characterized by warmth and behavioral control, is negatively associated with children's externalizing behaviors. 12
Positive parenting represents parenting skills that reflect authoritative parenting, defined as the ongoing relationship between a parent and a child, encompassing care, teaching, guidance, communication, and provision of a child's needs. 13 Numerous studies have demonstrated the efficacy of positive parenting in reducing children's behavioral problems, alleviating parental stress, and promoting children's successful development.14,15
Positive parenting is closely associated with parental self-efficacy (PSE). 16 PSE reflects caregivers’ beliefs about their capability to effectively manage parenting demands and influence their children's development.17,18 Bandura's theory suggests four core elements of self-efficacy: enactive mastery (success through direct experience that builds confidence in one's ability), vicarious experience (increasing confidence by observing others succeed), verbal persuasion (encouragement from others to strengthen belief in oneself), and physiological arousal (physical and emotional reactions influencing confidence). 19
Within the parenting context, PSE has been conceptualized as both an antecedent of parenting behavior and a key mechanism through which parenting practices influence child outcomes. 17 Parents with higher PSE are more likely to engage in positive, consistent, and responsive parenting behaviors, particularly when managing children's behavioral challenges. In contrast, lower PSE is associated with more coercive or avoidant parenting responses.18,20 Through these parenting behaviors, PSE shapes the quality and consistency of parent–child interactions, which subsequently influence children's behavioral adjustment.
Accordingly, PSE directly and indirectly affects children's outcomes via parenting practices, with lower levels of PSE being associated with a higher incidence of externalizing behavioral problems in children. 21 Moreover, positive parenting behaviors can reinforce parents’ mastery experiences and confidence, thereby strengthening PSE, which in turn helps stabilize adaptive parenting practices over time. This reciprocal process underscores the central role of PSE as a cognitive mechanism linking positive parenting practices to children's behavioral adjustment. 17
Various parent-involvement interventions that are evidence-based and cost-effective in addressing children's behavioral problems (e.g. Incredible Years, PCIT, and Triple P) have been developed to enhance PSE. 22 However, few families receive evidence-based interventions due to their low availability, accessibility, and fidelity. Many well-established parenting programs (e.g. Incredible Years, Triple P, PCIT, and PMT) require intensive time commitment, trained professionals, and in-person delivery formats, which limit their scalability and practicality for many caregivers. 23 To address these challenges, efforts have been made to transition to digital methods for delivering interventions aimed at managing behavioral problems. 24
Mobile health (mHealth) has emerged as a promising modality for delivering parenting interventions, particularly for families managing behavioral problems. 25 The proportion of the population that owns and regularly uses a smartphone in South Korea is ∼94.8%, which is significantly higher than the global average of 69% and is attributed mainly to the country's well-established IT infrastructure.26,27 Moreover, the integration of artificial intelligence (AI) into the healthcare field has enabled the exploration of personalized care approaches through big data analysis. 28 Such approaches can potentially improve outcomes and effectively deliver interventions. 29 Given these factors, delivering parenting interventions through mobile applications integrated with AI appears to be a highly feasible and effective solution. Therefore, we aim to develop a mobile application grounded in Bandura's self-efficacy theory to enhance PSE, foster positive parenting skills, and ultimately reduce behavioral problems in children (Figure 1).

Outline of the mobile application based on Bandura's self-efficacy theory.
The current mobile application is designed for parents of children aged 3–5 years who exhibit behavioral problems, and it is tailored to Korean-speaking caregivers within the Korean cultural context. The objective of this article is to describe the development process and study protocol for a non-randomized pilot study of a mobile application designed to enhance PSE and manage children's behavioral problems.
Methods
This article presents a protocol for a non-randomized pilot study describing the systematic development of a mobile parenting intervention using the analysis, design, development, implementation, and evaluation (ADDIE) model (Figure 2). 30 This instructional system design model is widely applied in educational programs and frequently employed in the development of academic and training programs in the healthcare field.31–33
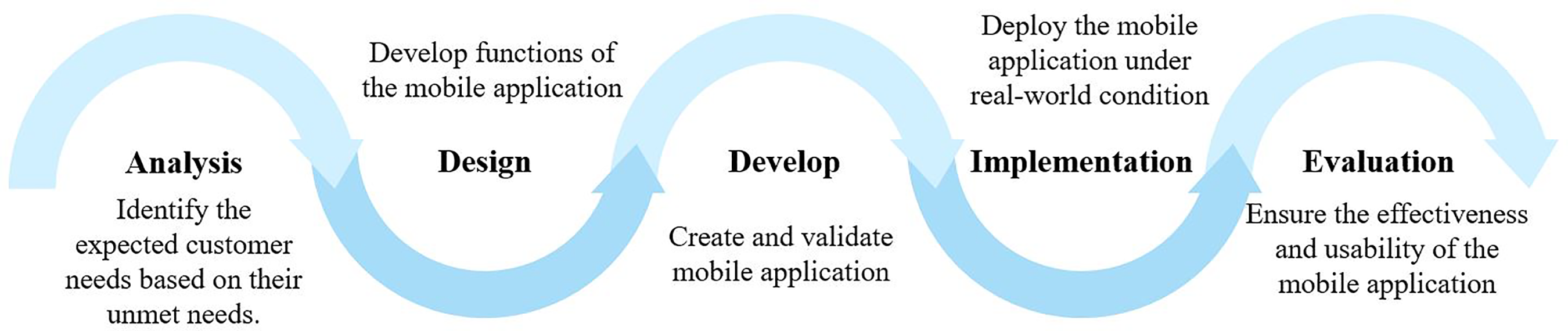
The analysis, design, development, implementation, and evaluation (ADDIE) model is based on the study objectives.
Table 1 provides a comprehensive overview of the implementation of the ADDIE model in the current mobile application development, outlining the key steps, methods, outputs, and completion status. Additionally, throughout the app development process, we will ensure adherence to the mobile health evidence reporting and assessment (mERA) checklist, a standardized framework designed to enhance transparency, comprehensiveness, and consistency in reporting mHealth research. 34
Overview of the analysis, design, development, implementation, and evaluation (ADDIE) model.

Analysis phase
Reviewing existing theories and intervention studies
The first key step involved a thorough narrative review to investigate current interventions and theoretical frameworks related to the management of children's behavioral problems. This review was conducted to examine what types of interventions are currently implemented, understand their effectiveness, and identify which evidence-based frameworks and intervention components could inform the development of our mobile application.
A comprehensive search was conducted on 23 December 2024, using two major academic databases—PubMed and CINAHL, which are widely used sources for nursing, behavioral health, and pediatric intervention research. The search strategy was structured around two thematic categories: (1) parenting interventions and (2) behavioral issues in children. Keywords used in the search included terms related to both parenting interventions (e.g. “parenting program,” “parent training,” “parent intervention,” and “Parenting guideline”) and children's behavioral problems (e.g. “behavioral problems,” “disruptive behavior,” and “externalizing behavior”). Studies were screened based on predefined criteria, which are presented in Table 2.
Inclusion and exclusion criteria for narrative review and application selection.

During data extraction, the included studies were coded according to intervention type, characteristics of the target population, theoretical foundations, core intervention components, delivery methods, and reported outcomes related to parenting practices or children's behavioral problems.
To derive the core benchmarking elements, we first summarized the core intervention components repeatedly reported across the included studies and compared these with the digital intervention elements suggested by Magnuson et al. 35 We identified intervention features that were repeatedly recommended or commonly present across studies, regardless of delivery format. This synthesis allowed us to consolidate recurring evidence-informed elements to guide the design of our mobile application.
Analyzing market needs and existing applications
In the market analysis, we reviewed related applications on platforms such as the Google Play Store and Apple App Store over a two-week period (15–29 January 2025). Search keywords included both English and Korean terms, such as “parenting” and “child behavior.” Applications were screened and selected based on predefined inclusion and exclusion criteria, which are presented in Table 2. Each application was then reviewed in terms of its core functions, usability features, and user feedback to inform benchmarking and differentiation strategies.
Each application was analyzed based on whether its features corresponded to the five core benchmarking elements identified from the narrative review. Because these benchmarking elements had been theoretically mapped to Bandura's four sources of self-efficacy, this approach allowed us to assess which sources of self-efficacy were addressed by each application. In addition, applications were reviewed in terms of their core functions, usability features, and user feedback to inform benchmarking and differentiation strategies.
Design phase
Developing primary functions
During the design phase, the findings from the analysis phase were systematically incorporated to guide the development of the mobile intervention. The theoretical framework identified in the analysis phase served as the overarching structure for functional design. Specifically, to enhance PSE, the intervention was designed to include application functions that address all four sources of self-efficacy proposed by Bandura. In this process, we aimed to construct a mobile intervention that integrates the previously identified benchmarking elements and differentiation strategies.
To translate the theoretical constructs and benchmarking elements into actionable intervention features, relevant behavior change techniques (BCTs) were selected from the BCT Taxonomy v1. 36 This theory- and evidence-based framework was used to ensure that each function is aligned with validated mechanisms of behavioral change. The identified BCTs were operationalized into specific application features to facilitate the intended user behaviors in real-world contexts.
Designing user-friendly UX/UI
To ensure a user-friendly interface design, we employed a UX/UI design tool to create wireframes that visualize the layout and structure of the application's core screens. Based on these wireframes, we developed the content flow from the perspective of end users, focusing on intuitive navigation, logical sequencing of features, and alignment with user needs. This approach will help create an application that effectively delivers its key functions and is easy for users to navigate.
Development phase
Developing a beta version
During the development phase, the research team is collaborating with a software company to ensure that the outputs from the previous analysis and design phases are accurately reflected in the beta version. The beta version will operate on both Android and iOS platforms, allowing it to be downloaded onto mobile devices.
In addition, we will ensure that server and data security are robustly established to protect users’ sensitive information. To minimize the risk of inadvertent disclosure of personal information, the application is designed according to data-minimization and privacy-by-design principles, employing predefined response options, character-limited and restricted free-text fields, and explicit in-application instructions prohibiting the entry of personally identifiable information. User access to the application is protected through secure authentication mechanisms (ID and password), and all data transmitted between the mobile device and the server will be encrypted using industry-standard secure communication protocols (e.g. TLS). Collected data are stored on a secure server infrastructure with role-based access control, and access is restricted to authorized research personnel only. For research purposes, all exported datasets will be de-identified using unique participant codes, and any linkage information, if required, will be stored separately under enhanced access restrictions.
Additionally, the community function of the application will be actively moderated by the research team and governed by explicit community guidelines prohibiting the disclosure of personal identifiers, the sharing of child images, and the use of abusive or inappropriate language. All posts will be subject to monitoring and removal when necessary, and community access will be restricted to enrolled caregivers only.
Conducting expert validity verification
Before conducting small-group user testing, the developed beta version will be distributed to experts for validity assessment. Experts will be purposively selected based on their relevant professional qualifications and experience in child behavioral health or parenting interventions, such as child and adolescent psychiatrists and parenting coaching specialists. All experts will receive detailed study information and provide informed consent prior to participation. They will assess the application's validity and usability using the specialist version of the Mobile Device Application Rating Scale (MARS), a reliable quality rating scale for mobile health applications. 37 In addition, feedback will be collected through interviews with the experts to help identify any necessary modifications and areas for improvement. The compiled revisions will then be communicated to the development team to ensure that the beta version is updated accordingly prior to its release to the user group for testing.
Testing a beta version with a small user group
The beta version will be distributed to two parents of children with behavioral problems to obtain user feedback. Participants will be recruited through convenience sampling from local child development and behavioral support centers and will participate voluntarily after receiving study information and providing informed consent. Users will receive standardized instructions on application navigation and core functions, use the beta version for one week, and subsequently provide feedback on technical performance and overall user experience.
The feedback obtained from the user interviews will be systematically analyzed to identify potential issues that require improvement within the application. Based on these insights, a user-centered beta version of the application will be developed for the implementation phase.
Implementation phase
Conducting a pilot study
Before initiating the study, Institutional Review Board (IRB) approval will be obtained from Yonsei University Healthcare System. After approval, the pilot study will be conducted and registered with the Clinical Research Information Service (CRIS) in Korea.
The pilot test will employ a one-group pretest–posttest quasi-experimental design to evaluate the feasibility and possible effectiveness of the application. The pilot group will comprise 30 Korean caregivers raising children aged 3–5 years with behavioral challenges, consistent with sample sizes used in similar studies.38,39 Behavioral problems will be defined using established cut-off scores on the Eyberg Child Behavior Inventory (K-ECBI) (Intensity ≥ 131 and Problem ≥ 15). 40
We will recruit participants through convenience sampling via multiple child development and behavioral enhancement centers in Korea. After receiving an explanation of the study and providing their informed consent, the caregivers will participate voluntarily in the pilot study. We will provide participants with a clear description of how to navigate the application and its primary functions.
The pilot test will be conducted over a three-month period, during which we will collect data on application usage and document any issues encountered by users. Outcome measures will be administered at baseline and post-intervention to evaluate changes in PSE, parenting behaviors, and children's behavioral problems.
Evaluation phase
Evaluating the possible effectiveness of the application
We will evaluate the possible effectiveness of the mobile application on PSE, parenting behaviors, and children's behavioral problems. Upon completion of the pilot test, the questionnaires will be readministered to facilitate comparison with the pre-test results. Statistical analyses will be performed using SPSS to examine changes in the study variables through paired t-tests.
PSE will be measured using the Korean version of the Parenting Sense of Competence scale (K-PSOC), a 22-item self-report measure assessing perceived parenting competence and satisfaction with the parenting role using a 5-point Likert scale. The scale demonstrated acceptable internal consistency, with Cronbach's α values of .76 for perceived competence, .75 for parenting satisfaction, and .79 for the total scale. 41 Parenting behaviors will be assessed using the Korean version of the Parents as Social Context Questionnaire (K-PSCQ), a 23-item scale measuring six dimensions of parenting behavior across supportive and controlling domains, with internal consistency coefficients ranging from .61 to .83. 42 Children's behavior problems will be assessed using the Korean version of the K-ECBI, a 36-item parent-report measure comprising Intensity and Problem scales, both of which showed excellent internal consistency (Cronbach's α = .93). 40
Evaluating the feasibility of the application
The feasibility of the application will be evaluated by assessing application usage metrics, including the frequency and duration of application use, which will be automatically captured through the application's manager-mode analytics system. In addition, after completing the pilot test, a user satisfaction survey will be conducted using the System Usability Scale, widely used for scaling user satisfaction. 43
Moreover, semi-structured user interviews will be conducted using an interview guide comprising open-ended questions developed a priori to elicit in-depth insights into participants’ experiences and perceptions of the mobile application, with a particular focus on feasibility-related objectives (e.g. usability, overall user experience, and barriers to engagement). All interviews will be audio-recorded and are expected to last ∼20–30 minutes. Interviews will be conducted by a trained research assistant with experience in qualitative data collection.
Interview transcripts will be analyzed using inductive content analysis to systematically identify themes related to user experience and perceptions of the intervention content. To enhance methodological rigor and transparency, the qualitative component of this study will be conducted and reported in accordance with the Consolidated Criteria for Reporting Qualitative Research. 44
Results
Analysis phase
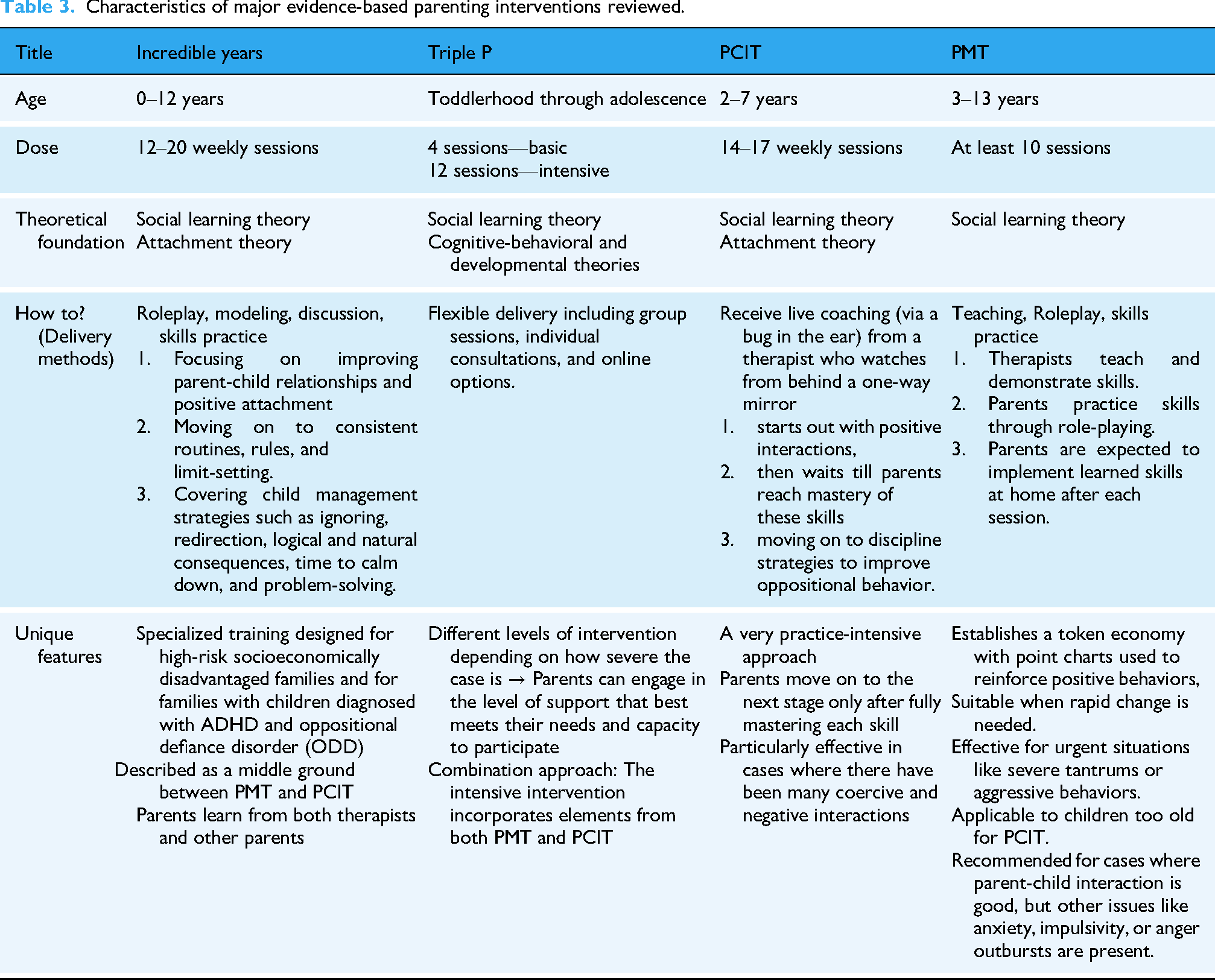
A systematic search identified 160 relevant studies, from which 54 met the inclusion criteria and were reviewed in detail. This narrative review highlighted the effectiveness of evidence-based parenting programs, specifically, Incredible Years, Triple P, Parent-Child Interaction Therapy (PCIT), and Parent Management Training (PMT), in reducing behavioral problems. These programs share a common theoretical foundation in social learning theory and consistently emphasize PSE as a core target for intervention. The key characteristics of these major parenting programs are summarized in Table 3 to provide a concise overview of their theoretical foundations and intervention components. Accordingly, Bandura's self-efficacy theory was adopted as the theoretical framework for application development. Additionally, national guidelines issued by the Korea National Center for Mental Health were reviewed to ensure that the application design aligns with standardized principles for managing children's behavioral problems in Korea. 45
Characteristics of major evidence-based parenting interventions reviewed.
Five core benchmarking elements were extracted from the literature review: (1) content customization, (2) push notifications, (3) behavior tracking, (4) skill modeling through video demonstrations, and (5) reward systems.35,46–48 These elements were mapped onto Bandura's four sources of self-efficacy to inform the application's design strategy.
The market analysis was conducted over a two-week period (15–29 January 2025), during which 18 parenting-related mobile applications were reviewed using Bandura's self-efficacy theory as an analytical framework. Each application was evaluated based on the extent to which it addressed the four sources of self-efficacy: enactive mastery, vicarious experience, verbal persuasion, and physiological arousal (see Table 4).
Comparison of parenting applications based on the four sources of Bandura's self-efficacy theory.

The comparative analysis revealed that only two applications incorporated all four components. For enactive mastery, five applications included behavior tracking features, and four provided diary functions. However, these tools primarily focused on general child activities (e.g. chores and reading), rather than specifically targeting problematic behaviors. Regarding vicarious experience, three applications offered peer community forums, while six featured role-modeling through video demonstrations. Verbal persuasion was the most commonly addressed component; 15 applications provided educational content, and seven delivered push notifications as a means of reinforcing parenting efforts. For physiological arousal, only a few apps integrated relevant strategies, such as reward systems (n = 4), relaxation guidance (n = 3), and content customization (n = 7).
These findings highlight a substantial gap in the current market. Most applications provide generic parenting guidance, and although many incorporate partial elements of self-efficacy, few offer a comprehensive, theory-based intervention specifically designed to enhance PSE in managing children's behavioral problems. To address this unmet need, our application was designed to incorporate all four sources of self-efficacy in an integrated manner. It distinguishes itself by focusing explicitly on problematic behaviors, applying behavior tracking to disruptive patterns, fostering peer learning through user communities, and enhancing emotional regulation via personalized support and rewards. This theory-driven differentiation positions the application as a unique and targeted digital intervention within the mHealth parenting landscape.
Design phase
The design phase focused on translating the outcomes of the analysis phase into concrete application features. This phase was guided by Bandura's self-efficacy theory, identified in the analysis phase as the core framework for intervention development. The primary objective of the mobile intervention was to reduce children's problem behaviors by enhancing PSE; accordingly, the application's functions were designed to support parents’ confidence in managing behavioral problems. Based on Bandura's theory, relevant BCTs were selected from the BCT Taxonomy (v1) and mapped onto the four sources of self-efficacy, considering the benchmarking elements and differentiation strategy. Figure 1 illustrates the overall structure of the application's primary functions grounded in Bandura's self-efficacy framework.
To support enactive mastery, the mobile application incorporated a “self-monitoring” technique by recording behavior, enabling users to track their parenting behaviors and their children's problem behaviors. “Self-monitoring” is widely regarded as an effective method for fostering a sense of accomplishment and success. 49 In this intervention, the self-monitoring function reflects the benchmarking element of behavior tracking. To differentiate the application from existing parenting tools, the tracking feature focuses exclusively on children's problem behaviors. This allows parents to monitor specific behavioral patterns and their corresponding responses rather than general activities.
To facilitate vicarious experiences, the mobile application implemented the “demonstration of behavior” technique through a user community. The “demonstration of behavior” method is effective for learning through observing others’ successes when executing tasks. 49 This feature allows users to observe success stories shared by other parents, operationalizing the benchmarking element of “skill modeling.” By observing how peers successfully apply behavioral management techniques, users can learn through social comparison and imitation, thereby strengthening their own perceived capability.
For verbal persuasion, the app incorporated a “verbal persuasion about capability” technique by providing users with positive feedback and push notifications. 48 These messages are designed to enhance users’ confidence in their parenting capabilities by providing personalized encouragement and reinforcement. Specifically, this component operationalized the benchmarking elements of push notifications and reward systems by delivering timely, tailored messages derived from the parents’ recorded behavioral data. By providing positive reinforcement that acknowledges effective parenting efforts and active application engagement, the intervention aims to sustain user motivation and instill confidence in the application of newly acquired parenting strategies.
To enhance physiological arousal, the mobile application introduced a “problem-solving” technique by offering personalized education to help users manage stressful situations. 48 These modules offer tailored content based on users’ behavioral data, including AI-driven tips based on user profiles and behavior patterns. This component integrated the benchmarking elements of content customization by delivering tailored educational modules based on users’ behavioral records when parents engaged with and applied the suggested strategies. The educational resources are developed based on empirical evidence from positive parenting research and established positive parenting guidelines. This design aims to support emotional regulation and stress management, specifically within the context of managing difficult behaviors.
In sum, during app-based intervention use, parents are prompted to record each occurrence of their child's problem behaviors, including the type of behavior, perceived triggers, duration, and intensity, as well as their own behavioral responses. Based on these records, the application delivers algorithm-driven feedback that provides personalized parenting coaching tailored to patterns of parent–child interaction. Parents may also engage in a community feature that facilitates experience sharing and observational learning by allowing users to view how other caregivers manage similar behavioral challenges. As behavioral data accumulate over time, the application generates periodic summaries that present analyzed patterns of both child and parent behaviors and provide ongoing positive feedback to support continued engagement. Through this integrated process of monitoring, feedback, peer-based learning, and reinforcement, the intervention aims to enhance PSE, promote effective responses to children's problem behaviors, and ultimately reduce child behavioral difficulties.
In addition, the UX/UI design was developed, ensuring that the application's layout, feature sequencing, and navigation align with end users’ needs (see Figure 3). The resulting application content flow reflects a logical progression from behavior tracking to feedback, personal education, and community, all of which are grounded in evidence-based behavior change techniques and aligned with the four self-efficacy components.

Example of content flow.
Development phase
The prototype was developed using a prototyping tool to simulate the application's core functionalities. Figure 4 presents several user interface designs of the application. Figure 4(a) shows the main login screens that users encounter upon launching the app. Figure 4(b) displays the primary dashboard screen, which summarizes daily behavior records. Figure 4(c) illustrates the behavior recording interface, where users are required to input the type of behavior, its duration, intensity, the antecedent situation, and its consequences. Figure 4(d) presents the app's analytic feature, which visualizes behavior trends and allows users to compare the frequency of occurrence over time easily.

Prototype of the app.
The development phase is currently underway in collaboration with a professional mobile application development company, reflecting the prototype. Upon completion of the beta version, the application will undergo the next planned steps: expert validity verification and testing with a small user group. These steps will provide essential feedback for refining the application before full-scale pilot implementation.
Implementation and evaluation phase
Once the beta version of the mobile application is fully developed, the implementation and evaluation phases will be conducted. A pilot study is scheduled to be initiated in May 2026 to assess the application's feasibility and preliminary effectiveness. Results from these phases will be reported following the completion of the pilot test and data analysis.
Discussion
Given the significant impact of children's behavioral problems on both themselves and their families, effective parenting interventions are essential. The mobile application that we aim to develop has the potential to serve as a valuable tool for enhancing PSE, thereby fostering positive parenting practices that can effectively manage children's behavioral issues.
The current mobile application exhibits strengths in its development, as it is grounded in robust theoretical evidence. For example, Altafim et al. 50 evaluated the Born Learning program, a WhatsApp-based content-delivery parenting intervention that demonstrated effectiveness in reducing coercive parenting and child behavioral problems; however, its theoretical framework primarily serves as a background rather than a systematically operationalized behavior change mechanism. In contrast, the present study develops a theory-driven mobile application grounded in Bandura's self-efficacy framework that explicitly embeds BCTs into application functions to enhance positive parenting practices.
Additionally, the present application offers a core functional strength through personalized content delivery, providing tailored modules and AI-driven feedback based on users’ behavioral data and profiles, an aspect frequently identified as lacking in prior parenting applications. 24
Once the application's effectiveness has been robustly established, its usage will be expanded to a broader audience, including families of children with behavioral problems, healthcare facilities, and community settings.
To promote clinical adoption, partnerships with pediatric and behavioral health clinics will facilitate integration into therapy programs. Community engagement will involve collaborations with parenting organizations, NGOs, and advocacy groups. Webinars will educate families on the app's benefits, while targeted social media campaigns will raise awareness among parents and healthcare professionals. These efforts will ensure the app's broad accessibility and practical application.
Future efforts include developing multilingual versions of the application and conducting follow-up studies to assess long-term outcomes, ensuring sustainability and scalability. To implement these dissemination plans, we plan to recruit additional personnel to promote the application, ensure effective service delivery, and develop new features.
Footnotes
Acknowledgements
This research was supported by the Brain Korea 21 FOUR Project funded by the National Research Foundation (NRF) of Korea, Yonsei University College of Nursing.
Ethical considerations
There are no human participants in this article, and informed consent is not required.
Consent to participate
Not applicable.
Consent for publication
Not applicable.
Authors’ contributions
AL conceived the app's development process and contributed to its conceptualization and functionality design. HL initiated the study design and drafted the initial research protocol. AL and HL critically reviewed and refined the protocol multiple times, providing critical revisions to ensure methodological rigor and coherence. All authors have read and approved the final version of the manuscript.
Funding
The authors received financial support for the research, authorship, and/or publication of this article. The current study was funded by the National Research Foundation of Korea (RS-2023-00212981).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Data sharing not applicable to this article as no datasets were generated or analyzed during the current study.
Declaration of generative AI use
AI-assisted tools were used only for language editing and grammatical refinement. The intellectual content, study design, analysis, and original writing were entirely generated by the authors without the use of AI tools.