
Abstract
Background
Hodgkin lymphoma (HL) is a malignant tumor of the lymphatic system. With the rapid expansion of short video platforms, the public increasingly relies on them for medical information, yet the scientific rigor and reliability of such content remain inconsistent. This study aimed to systematically evaluate the content and quality of HL-related videos on TikTok and Bilibili.
Methods
In August 2025, videos related to “Hodgkin lymphoma” were searched on TikTok and Bilibili. After applying predefined inclusion and exclusion criteria, video sources, engagement metrics, and content features were collected. Video quality and reliability were assessed using three validated tools: the Journal of the American Medical Association (JAMA) benchmarks, the Global Quality Score (GQS), and the modified DISCERN (mDISCERN) scale. Differences by uploader type, platform, and audience engagement were also analyzed.
Results
A total of 225 videos were included (155 from TikTok and 70 from Bilibili). TikTok videos were shorter but had significantly higher engagement (P < .05). Most TikTok videos were uploaded by professional doctors and had a higher GQS median score (3.0) than Bilibili (2.0). Both platforms had a median mDISCERN score of 3.0. Videos uploaded by professionals and institutions scored higher on GQS, mDISCERN, and JAMA compared with non-professional users. Bilibili had a larger share of videos from individual users, which were lower in quality and consistency. Across platforms, epidemiology and prevention were rarely covered, and overall content was fragmented. Spearman correlation analysis revealed strong associations among engagement metrics but no significant relationship with quality scores, suggesting that popularity is driven more by presentation and dissemination than by scientific quality.
Conclusion
TikTok and Bilibili differ significantly in the sources and quality of HL-related videos. Although high-quality short videos can improve public health literacy, their popularity depends more on style and reach than on scientific quality. Platforms should enhance professional certification and content review to promote the standardized dissemination of evidence-based medical knowledge.
Introduction
Hodgkin lymphoma (HL) is a malignant neoplasm of the lymphatic system characterized by Hodgkin/Reed–Sternberg cells.1,2 Despite major survival gains from contemporary chemotherapy, radiotherapy, and immunotherapies, HL remains clinically important because of its distinctive epidemiology and long-term survivorship needs.3–5 HL disproportionately affects adolescents and young adults, who are heavy users of social media and frequently seek health information online. Moreover, many patients achieve long-term survival yet still face relapse risk, treatment-related toxicities, and late complications, including cardiovascular disease and secondary malignancies. These issues necessitate sustained follow-up and informed self-management.6–8 In this setting, patient education is central to HL care and is associated with treatment adherence, symptom self-management, shared decision-making, and long-term psychosocial outcomes. Access to accurate, comprehensible, and actionable information helps patients engage with recommended therapies and survivorship plans. By contrast, misinformation can create unrealistic expectations, increase anxiety, encourage inappropriate self-management, delay appropriate medical evaluation, and ultimately undermine adherence and outcomes.9,10 As social media increasingly serves as a primary gateway for health information, systematically evaluating the quality and reliability of HL-related content is integral to patient-centered care.10,11 Notably, most evaluations of cancer-related social-media videos have focused on more prevalent malignancies (e.g., breast, lung, or prostate cancer), leaving HL-specific evidence limited. This gap is clinically important because HL patients’ information needs extend beyond initial treatment into survivorship, yet the quality of HL-related short-video content has not been systematically characterized.
With the rapid expansion of social media and short-video platforms, public access to medical and health information has undergone a profound transformation.12–14 In China, since the late 20th century, internet-based health education has developed rapidly, particularly among young and highly educated populations, with online platforms gradually becoming major sources of health information.15,16 High-quality medical short videos can present disease etiology, clinical manifestations, diagnosis, treatment processes, and follow-up considerations in an intuitive, vivid, and easily understandable manner, thereby enhancing public health literacy and treatment adherence. 17 However, videos containing errors, exaggerations, or biased interpretations may mislead viewers, resulting in inappropriate health decisions and potentially negatively affecting patients’ healthcare-seeking behaviors and psychological well-being. 18 Importantly, empirical oncology studies show that many patients and caregivers use social media to inform medical decisions, yet do not routinely verify such information with clinicians.11,19 In China, qualitative interviews and population-based surveys among patients and survivors further indicate that online health information seeking is common and closely tied to evolving information needs and self-management support across the cancer trajectory, reinforcing the clinical relevance of evaluating the quality of Chinese-language short-video content. 20
TikTok and Bilibili have emerged as important platforms for disseminating medical and health information in China.21,22 With their large user bases and diverse ecosystems, these platforms have exerted a notable impact on public health education. 23 TikTok is recognized for its short-video format and broad youth audience, whereas Bilibili attracts hundreds of millions of monthly active users through content diversity, interactive communities, and user-friendly interfaces.24,25 By contrast, platforms such as Facebook Reels and Instagram Reels are restricted in China and were excluded from this study. The quality of medical information on social media is highly variable 26 : videos uploaded by healthcare professionals generally demonstrate higher scientific reliability and credibility but have limited reach, whereas some creators without medical backgrounds achieve high engagement due to their large follower bases, even when their content is inaccurate or misleading.27,28 Furthermore, studies have reported that health-related videos produced by commercial organizations often contain a disproportionately high rate of erroneous information. 29 These observations highlight the need for systematic evaluation of video quality and enhanced regulatory oversight.
Recently, an increasing number of scholars have employed various assessment tools to systematically analyze the quality of medical videos on emerging platforms such as TikTok and Bilibili. 30 However, evidence specific to HL remains limited, despite the substantial overlap between HL-affected age groups and short-video users and the disease's distinct survivorship needs. In this context, a systematic assessment of the scientific reliability, completeness, and reliability of HL-related short videos on TikTok and Bilibili is clinically and publicly relevant. Accordingly, we aimed to evaluate the quality of HL-related short videos and examine their associations with audience engagement metrics (likes, comments, favorites, and shares), thereby informing strategies to improve public health information literacy and optimize cancer-related health communication.
Methods
Search strategy and data extraction
A search was conducted on August 26–28, 2025, using the keyword “Hodgkin lymphoma” (Chinese:“霍奇金淋巴瘤”) on TikTok and Bilibili, with the default ranking set to comprehensive order. This keyword was selected for its broad relevance in both clinical practice and public communication, ensuring retrieval of comprehensive and medically pertinent videos. To minimize bias, a newly registered account was used, and no filters were applied. Figure 1 presents the process from initial search to final video selection.

Flowchart of the research design, illustrating the video screening and analysis process.
Videos were screened using prespecified eligibility criteria. Inclusion criteria required that (1) the video was publicly accessible during the sampling period and (2) the content primarily focused on HL-related health education. “Health education–focused” content was defined as videos providing substantive medical information or patient education in at least one of the following domains: clinical manifestations/symptoms, treatment approaches, and general educational content (e.g., disease overview, care-seeking guidance, follow-up, or self-management advice).
Exclusion criteria were: (1) videos that were primarily advertisements or promotional material (e.g., marketing of products/services, promotion of clinics/hospitals, or solicitation of paid consultations without substantive educational content); (2) duplicate or near-duplicate videos (identical or substantially overlapping content; the earliest-posted version was retained to avoid double counting); (3) videos without audio, including silent videos even if subtitles or on-screen text were present; and (4) irrelevant content not addressing HL (e.g., general cancer content without HL-specific information). Videos that mentioned HL only in passing were excluded unless HL was the primary topic.
No restrictions were applied to the uploader type. All eligible videos were included regardless of whether they were uploaded by healthcare professionals, institutions, or individual users, to enhance sample representativeness. After eligibility screening, the uploader identity was recorded and classified based on publicly available account-level information (e.g., account name, profile description, verification status, and disclosed credentials or affiliations). Uploaders were classified into four categories: professional individuals (individual accounts explicitly indicating healthcare-related credentials and/or institutional affiliations), nonprofessional individuals (individual accounts without stated healthcare-related credentials), individuals (individual accounts with insufficient public information to determine professional status), and institutions (organizational accounts, including hospitals, universities/research institutes, professional associations, media or science communication organizations, government or public health agencies, and commercial entities such as pharmaceutical companies).
Data from all included videos were manually extracted by the research team and recorded in a standardized spreadsheet. Variables collected included video source, duration, number of likes, collections, comments, shares, content category, GQS, modified DISCERN, and JAMA scores. In addition, platform type and uploader identity were recorded as key variables, as these factors may influence video dissemination patterns and audience engagement (Supplementary Table S1).
Video content, quality, and reliability evaluation
Video quality was assessed using the Global Quality Score (GQS), which evaluates the overall utility, structure, and accessibility of online health resources. The GQS ranges from 1 to 5, with higher scores indicating better overall quality; scores of 3–5 are commonly interpreted as at least moderate quality (Table 1).13,31
The global quality score (GQS) quality criteria.

The modified DISCERN (mDISCERN) tool, originally developed by Charnock et al., was used to assess reliability. It consists of five items, with one point assigned for each affirmative response (total score range, 0–5). Higher scores indicate greater reliability; scores ≥3 are commonly interpreted as moderate-to-high reliability (Table 2). 32
The modified DISCERN (mDISCERN) reliability criteria.

The Journal of the American Medical Association (JAMA) benchmark criteria were also applied to evaluate the reliability and transparency of online resources across four domains: authorship, attribution, currency, and disclosure. Each domain scores 1 point, yielding a total score range of 0–4 (Table 3). 33
The Journal of the American Medical Association (JAMA) benchmark criteria.

Video evaluation was independently conducted by two medically trained researchers, with discrepancies resolved through discussion with the corresponding author to ensure standardized criteria and consistency. By integrating GQS, mDISCERN, and JAMA, the study systematically assessed the overall educational quality, completeness, and reliability of HL-related videos, thereby providing a quantitative basis for subsequent analyses. For inferential analyses, these scores were treated as ordinal/continuous measures rather than dichotomized categories.
Ethical approval
This study analyzed publicly accessible videos and did not involve human participants, clinical data, biological specimens, or animal experimentation. All videos included in the analysis were publicly available at the time of data collection. Data extraction was restricted to non-identifiable, video-level information and standardized reliability assessments based on the displayed content. No personally identifiable information was collected or reported, and no verbatim comments were analyzed or quoted. Based on these conditions, a formal institutional ethics review was not required.
Statistical analysis
Continuous variables were first tested for normality using the Shapiro–Wilk test. Normally distributed data were expressed as mean ± standard deviation; non-normal data were presented as medians with interquartile ranges (Q1, Q3). For group comparisons, the Mann–Whitney U test was used for two groups and the Kruskal–Walli's test for three or more groups. Categorical data were expressed as frequencies and percentages. Correlations between continuous variables were assessed using Spearman's rank correlation. A two-sided P-value <.05 was considered statistically significant. All statistical analyses and graphical visualizations were performed using R software (version 4.4.0).
Results
Video characteristics
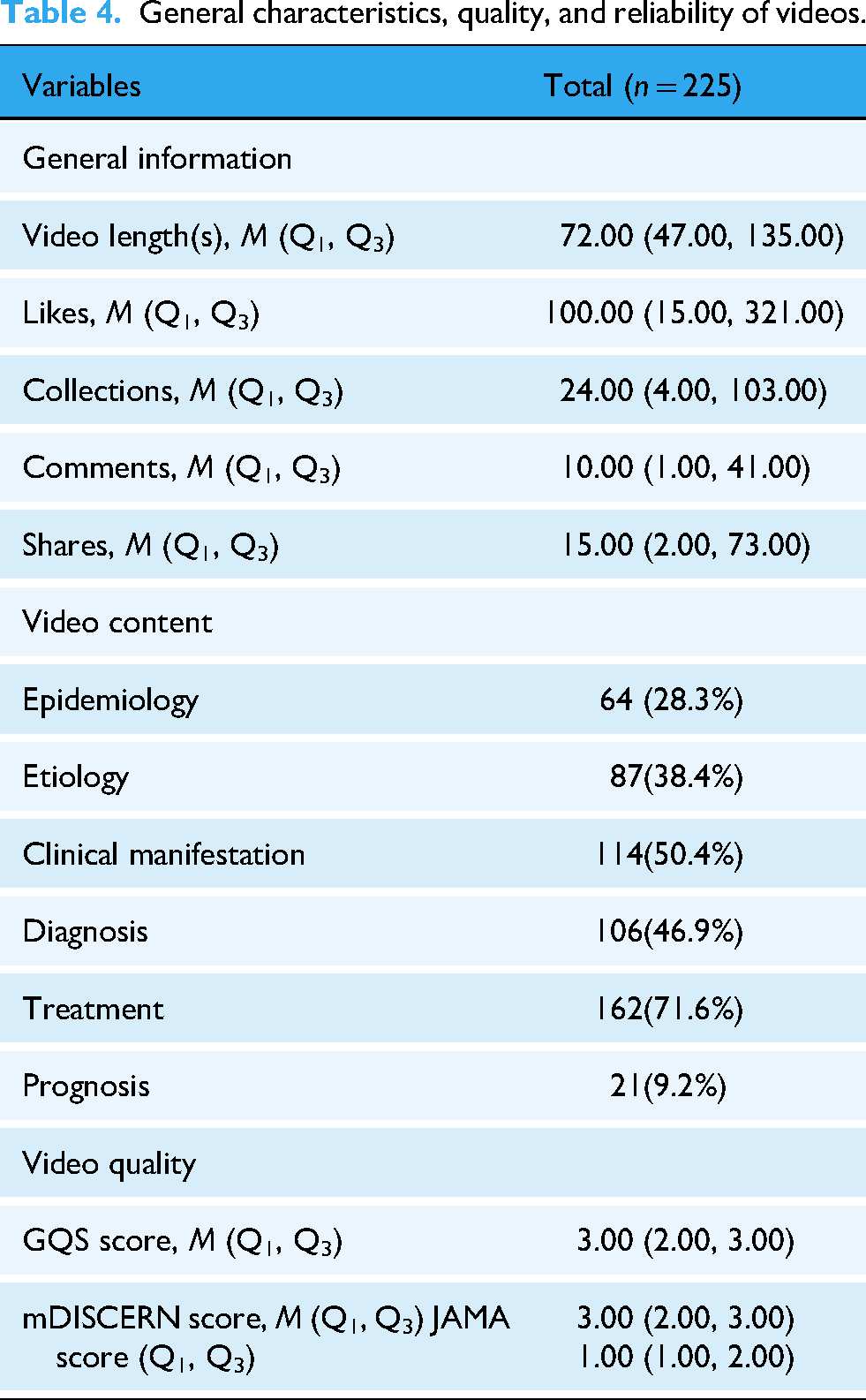
After exclusions, 225 HL-related videos were included, comprising 155 from TikTok and 70 from Bilibili (Figure 2(a), Table 4). TikTok videos were shorter in duration but demonstrated higher interaction rates. Median engagement for TikTok was likes 200 (IQR: 62.5–396.5), comments 24 (IQR: 5.5–61.0), collections 47 (IQR: 12–142), and shares 30 (IQR: 8.5–113.5). Significant differences were observed between platforms in audience engagement metrics (likes, comments, collections, and shares; P < .05). Bilibili videos consistently showed lower engagement across all metrics (Table 5). Notably, engagement metrics are influenced by platform-specific factors (e.g., user base size, recommendation mechanisms, and interaction affordances). Therefore, cross-platform differences in engagement (Table 5) are presented descriptively and should be interpreted with caution, rather than as direct proxies for information quality or reliability. Standardized quality and reliability scores (GQS, JAMA, and mDISCERN) were rated using the same procedures and are reported for cross-platform comparison (Table 5). Associations between engagement and quality are more interpretable within platforms, where the interaction environment is consistent.

Distribution of video uploaders on TikTok and Bilibili. (a) Overall proportion of videos on TikTok and Bilibili. (b) Distribution of all video uploaders. (c) Distribution of video uploaders on TikTok and Bilibili. (d) Distribution of professional versus non-professional uploaders on TikTok and Bilibili.
General characteristics, quality, and reliability of videos.
Characteristics of HL-related videos on TikTok and Bilibili.

Z: Mann–Whitney test.
M: Median, Q1: first quartile, Q3: third quartile.
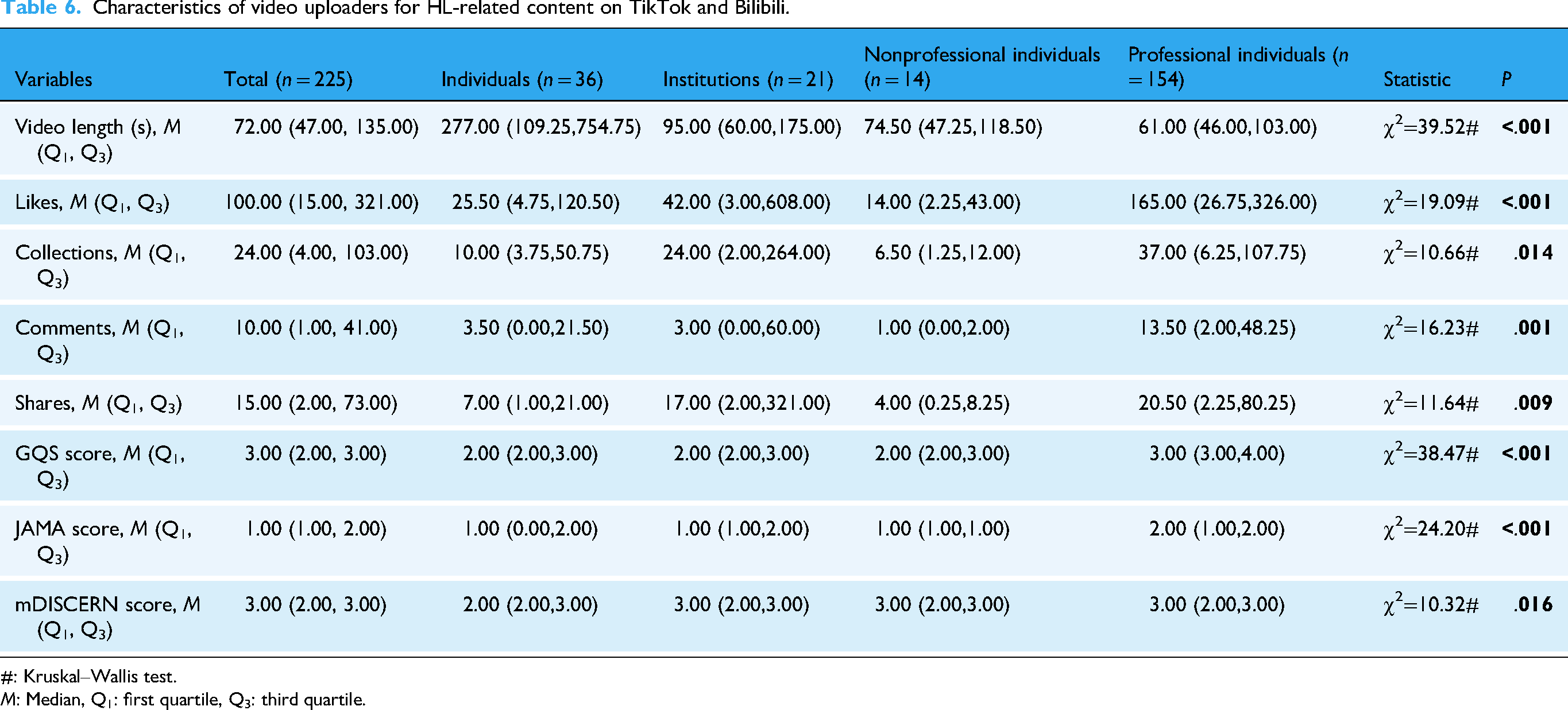
Stratified analysis by uploader identity revealed that videos from professional individuals generally received higher interaction, whereas individual users tended to upload longer videos (Table 6).
Characteristics of video uploaders for HL-related content on TikTok and Bilibili.
#: Kruskal–Wallis test.
M: Median, Q1: first quartile, Q3: third quartile.
Uploader characteristics
Video uploader distribution showed that professional individuals accounted for 69.2%, individual users 16.3%, institutions 8.6%, and nonprofessional individuals 5.9% (Table 6, Figure 2(b)). On TikTok, professional individuals contributed over 80% of uploads, whereas individual users dominated among nonprofessionals. On Bilibili, both professional individuals and individual users were primary contributors. Notably, 96% of TikTok videos were uploaded by professionals compared with 71% on Bilibili (Figure 2(c)–(d)). This indicates that professional individuals are the primary content providers on both platforms, particularly on TikTok.
Video content
Among the 225 videos, 15.7% addressed etiology, 20.6% clinical manifestations, and 19.1% diagnostics. Treatment was the most frequently discussed topic (29.2%). In contrast, epidemiology and prevention were covered less frequently, appearing in only 11.6% and 3.8% of videos, respectively. TikTok contained a broader range of content compared with Bilibili (Figure 3).

Comparison of HL video content across TikTok and Bilibili. (a) Pie chart of video content distribution. (b) Radar chart of video content coverage. (c) Bar chart of video content categories.
Video quality
On TikTok, the median GQS was 3.0 (IQR=3.0–4.0), while Bilibili's was 2.0 (IQR=2.0–3.0). For mDISCERN, both platforms had a median of 3.0 (IQR=2.0–3.0). Professional individuals and institutions scored higher on GQS, mDISCERN, and JAMA compared with individual users (Figures 4(a)–(c)). Significant platform differences in all three indices indicate that TikTok videos generally provided higher quality and reliability (Figures 4(d)–(f)).

Distribution of scores by uploader type and comparison of video quality and reliability on TikTok and bilibili. (a) GQS score. (b) mDISCERN score. (c) JAMA score. (d) GQS score by platform. (e) mDISCERN score by platform. (f) JAMA score by platform.
Correlation analysis
Spearman's correlation analysis demonstrated strong positive correlations among engagement metrics likes and comments (ρ = 0.93), collections and likes (ρ = 0.90), collections and comments (ρ = 0.93), shares and likes (ρ = 0.91), shares and comments (ρ = 0.85), and shares and collections (ρ = 0.83) (Figure 5). These results indicate synchronous increases in user engagement behaviors. In contrast, correlations between engagement metrics and quality scores were generally weak. Specifically, GQS was weakly correlated with likes (ρ = 0.24), comments (ρ = 0.17), collections (ρ = 0.30), and shares (ρ = 0.30), whereas mDISCERN showed near-zero correlations with all engagement metrics. Video length was weakly negatively correlated with engagement (ρ = −0.12 to −0.24) and moderately positively correlated with GQS (ρ = 0.37).

Correlation matrix of engagement metrics and video quality scores.
Discussion
The rapid development of short video platforms has profoundly reshaped the public's access to medical information.28,34 However, the open nature of these platforms and the absence of strict regulatory oversight raise concerns about the authenticity and scientific reliability of shared content.35,36 Given their broad influence on public health awareness, systematically evaluating the quality and reliability of medical information disseminated through short videos is essential. 37 While prior studies have examined cancer-related videos on TikTok and Bilibili, research specifically focusing on HL remains limited, particularly on China's mainstream platforms.
For patients and the public, the most pressing concerns typically center on disease diagnosis, treatment options, and daily management. In contrast, pathological mechanisms and molecular research are often too complex for non-medical audiences to readily comprehend. Consequently, ensuring the dissemination of accurate and accessible HL-related information via short video platforms carries important clinical and public health implications. Previous research indicates that improving disease awareness can reduce patient anxiety and enhance treatment adherence—both of which are critical in cancer management.38,39 Among HL patients, anxiety stems not only from treatment side effects and the risk of relapses but also from the lack of reliable information. Thus, high-quality, evidence-based medical short videos may enhance patient awareness and self-management, whereas misleading or exaggerated content may exacerbate anxiety and result in harmful health decisions. 40
This study is the first to systematically compare HL-related short videos on TikTok and BiliBili, revealing significant differences in both sources and quality of information. Using multiple validated tools, including mDISCERN, GQS, and JAMA scoring systems, we assessed the quality and reliability of the videos. Our findings show that TikTok videos, primarily produced by specialized doctors, achieved higher quality and reliability scores. In contrast, BiliBili contained a larger proportion of videos from non-professional individuals and individual users, leading to comparatively lower content quality and consistency. Furthermore, only a minority of videos explicitly addressed HL epidemiology and preventive management, indicating a gap in systematic and comprehensive disease education.
Platform characteristics strongly shaped dissemination patterns. TikTok's short, highly interactive video format facilitated rapid spread and audience engagement, whereas BiliBili's longer videos required greater commitment and therefore generated lower interaction rates.41,42 Videos uploaded by professional individuals consistently achieved higher GQS and mDISCERN scores, while those produced by non-professional individuals scored lower.38,43 These findings highlight the need for platforms to support a multidisciplinary, collaborative health communication approach. Because HL diagnosis and treatment involve multiple specialties, short-video platforms may provide a potential channel for interdisciplinary communication (e.g., coordinated, series-based content developed by multidisciplinary teams). However, in our sample, such structured, guideline-oriented multidisciplinary content was limited, and most videos offered fragmented rather than comprehensive perspectives. In addition, oncology care is inherently patient-centered and individualized; HL management typically requires multidisciplinary input and patient-specific diagnostic information. Therefore, generalized social-media content has limited utility for informing individualized clinical decision-making and should be viewed as supplementary for awareness and general education, rather than a substitute for professional consultation or personalized treatment planning.
Across platforms, several implications may generalize to video-based health communication beyond HL. First, platform affordances and uploader composition appear to shape both dissemination patterns and the information environment encountered by viewers. Second, consistently higher quality and reliability scores among professional uploaders suggest that credentialed participation may be a key lever for improving educational value in short-video settings. Third, the limited availability of structured, guideline-oriented, multidisciplinary content highlights an actionable gap: complex oncologic topics may be better addressed through coordinated, series-based communication that integrates complementary perspectives, rather than isolated single-topic clips.
Correlation analysis revealed strong associations among interaction metrics (likes, comments, collections, shares), but no significant relationship with GQS, mDISCERN, or JAMA scores. 44 These findings suggest that video popularity is largely driven by presentation style and emotional appeal rather than scientific rigor or quality.45,46 Accordingly, platform algorithms and moderation mechanisms should be improved to enhance the visibility of high-quality, evidence-based content. As reliance on social media platforms and AI-enabled tools for health information seeking increases, potential cognitive risks warrant consideration. One potential concern is “cognitive off-loading,” whereby rapid access to externally retrieved information may reduce deeper cognitive processing, leading to weaker retention and more superficial learning. In short-video environments, this dynamic may contribute to fragmented understanding and limit viewers’ ability to formulate nuanced questions for clinicians, even when the content appears credible. Taken together, these considerations underscore the importance of clinician-guided verification and the development of structured, evidence-based patient education resources.
From a social work perspective, this study provides systematic evidence on the dissemination of health information, offering healthcare professionals and researchers insights into current practices. It also highlights new digital tools for social workers engaged in patient education, psychological interventions, and social support. 47 By exposing the paradox between “information quality” and “popularity,” the study emphasizes the importance of strengthening interdisciplinary collaboration—including medicine, social work, and public health—to promote accessible, equitable, and scientifically sound medical knowledge. This is particularly valuable for improving the experiences of HL patients and their families, advancing social health equity, and informing health communication policy reform.
This study has several limitations. First, as a cross-sectional study, data collection was restricted to August 2025, limiting the ability to capture temporal changes in platform quality. An additional limitation is the dynamic and context-dependent nature of social media platforms; changes in recommendation algorithms, moderation policies, interface design, or user composition across time and geographic regions may alter content visibility and engagement patterns. Accordingly, our findings should be interpreted as a cross-sectional snapshot of the platforms during the sampling period and may not be fully replicable or generalizable to other time points, regions, or settings. Second, the evaluation tools employed (mDISCERN, GQS, JAMA) rely on manual scoring within the evidence-based medicine framework, which may introduce subjective bias. Future studies could incorporate AI-assisted evaluation methods to reduce subjectivity. Third, this study analyzed only Chinese-language videos, which restricts the generalizability of the findings to other linguistic and cultural contexts. Future research should conduct cross-platform and cross-language comparisons and further investigate the interactions among platform moderation mechanisms, patient education needs, and the quality of medical information.
Conclusion
This study systematically evaluated short videos on HL available on the TikTok and Bilibili platforms. The findings revealed that overall content completeness was limited, with only moderate quality, reliability, and transparency, whereas videos produced by professionals demonstrated substantially higher quality. Further analysis showed no significant relationship between engagement metrics and video quality. In the rapidly evolving digital media environment, short video platforms have become crucial channels for public access to cancer-related information; however, significant disparities persist in the scientific reliability of content. These results highlight the need to improve the quality and reliability of medical content in short videos, enabling patients to better understand their conditions, enhance treatment adherence, and reduce health risks associated with misinformation. Future efforts should involve medical institutions producing and disseminating guideline-based standardized content. Platforms should reinforce professional certification, implement AI-assisted content screening, and optimize recommendation algorithms to enhance the visibility of high-quality content. Simultaneously, the public should cultivate media literacy and prioritize content from professionals or authoritative organizations to ensure health information is communicated scientifically, accurately, and responsibly in the digital era.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076261430074 - Supplemental material for Science or hype? A cross-sectional analysis of the quality of Hodgkin lymphoma–related short videos
Supplemental material, sj-docx-1-dhj-10.1177_20552076261430074 for Science or hype? A cross-sectional analysis of the quality of Hodgkin lymphoma–related short videos by Hao Sha, Xiaoan Zhang, Lihai Wu, Dan Zhou, Daqing Dang, Haohao Yin, Tianxin Huang and Pengfei Zhang in DIGITAL HEALTH
Footnotes
Acknowledgments
The authors would like to express their gratitude to the video uploaders for their contributions to public health.
Ethical approval
The data used in this study were derived from publicly available videos on platforms such as Bilibili and TikTok. These videos are accessible to the public, and no personal or private information was involved during data collection. All analyses were conducted using publicly accessible content, and the study did not entail the collection or processing of users’ private information. In accordance with relevant ethical review guidelines, this study did not require formal ethical approval.
Contributorship
HS conceived and designed the study. XAZ, DZ, and HHY were responsible for reviewing and scoring the videos. LHW, QDD, and TXH collected and analyzed the data. HS wrote the original draft. XAZ reviewed and edited the manuscript. PFZ critically revised the manuscript for intellectual content. All the authors contributed to manuscript writing and editing and approved the final draft for submission.
Funding
This study did not receive external funding from any public, private, or nonprofit entities.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Derived data supporting the findings of this study are available from the corresponding authors upon request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.