
Abstract
Objective
This study examines how online appointment systems technology-based service encounters (OAS-TSE) relate to patient value co-creation behaviors through the mediating role of hospital image (HI) in Chinese healthcare settings.
Methods
This study surveyed 387 patients in China who had experienced OAS-TSE during their first hospital visit within the past 3 months. Using structural equation modeling in SmartPLS 4.0, this study tested relationships between OAS-TSE, HI, and four dimensions of value co-creation behaviors: Dialogue, Access, Risk Assessment, and Transparency (DART).
Results
Favorable OAS-TSE were associated with higher HI, which in turn was associated with all four DART dimensions. Direct associations between OAS-TSE and co-creation behaviors were significant for Dialogue, Access, and Transparency, but not for Risk Assessment. HI mediated all relationships, with full mediation observed only for Risk Assessment. The model explained substantially less variance in Risk Assessment compared to other dimensions.
Conclusion
This study reveals associations between OAS-TSE and patient participation through HI. Theoretically, HI emerges as a key psychological mechanism connecting digital touchpoints to patient co-creation, with boundaries identified for direct technology associations. Practically, findings suggest hospitals may benefit from recognizing digital touchpoints as image-building tools and adopting differentiated strategies for promoting patient participation based on behavior complexity.
This is a visual representation of the abstract.
Keywords
Introduction
Contemporary healthcare services are undergoing a profound paradigm shift.1,2 The traditional physician-centric model, where patients passively receive treatment, is being replaced by a new model of patient-physician relationship centered on the patient, emphasizing active participation and shared decision-making.3,4 As the World Health Organization clearly states, achieving true universal health coverage requires shifting from health systems designed around diseases and institutions to systems designed around people's needs. 5 At the core of this shift is the restructuring of the power dynamic between physicians and patients: patients are no longer merely passive recipients of medical services but are gradually becoming active participants with the right to know, decide, and express.6,7 The patient empowerment movement signals a transfer in the balance of power within healthcare, driving the formation of a more transparent and equitable medical system.8,9 Patient value co-creation, as an important manifestation of this transformation, refers to patients’ active participation behaviors in the healthcare process, through which they contribute to the quality and outcomes of their own care.10,11 Such behaviors can be captured through four dimensions: Dialogue, involving communication and knowledge sharing with providers; Access, referring to actively seeking health-related information and resources; Risk Assessment, encompassing evaluation of treatment options and responsibility for health decisions; and Transparency, involving truthful disclosure of health information.12,13
Simultaneously, the rapid development of digital technology has further accelerated this transformation.14,15 Digital touchpoints such as online appointment systems (OAS), mobile health applications, and remote monitoring devices are increasingly becoming the primary interface for patients to access healthcare services.16,17 These technological innovations not only enhance the accessibility and convenience of medical services but, more importantly, digital health technologies grant patients’ greater control over their own health and medical services, redefining the interaction between patients and providers.18–20 In this wave of digital transformation, the patient's experience with digital systems may not only relate to their service satisfaction but may also subsequently be linked to their willingness and behavior to participate in the medical process.21,22
In recent years, under the patient-centric healthcare paradigm, patient value co-creation has become a core issue and research hotspot in the field of healthcare service management, with scholars widely exploring its formation mechanisms and effects. 23 In this rich body of research, scholars have assigned diverse roles to value co-creation behavior within their models. Most scholars tend to view patient value co-creation behavior as a mediating process. For example, Mai et al. 13 confirmed that physicians’ interpersonal interaction behaviors enhance patient satisfaction by stimulating patients’ co-creation participation. Similarly, Tang et al. 24 also found that patients’ Self-efficacy indirectly relates to their perceived value through co-creation behavior. Furthermore, Fei et al. 25 positioned co-creation behavior as a mediating variable connecting platform quality and users’ continuous use intention. Other scholars, in their conceptual frameworks, regard patient value co-creation behavior as an antecedent. For instance, Dodds et al. 26 proposed that such behaviors influence mechanisms like Shared-control, ultimately leading to patient well-being.
Although these studies provide important insights into the mechanisms of patient value co-creation, there is still a lack of systematic exploration into how co-creation behavior itself is activated, especially its complete formation path in a digital context. Recent literature reviews also point out that the field urgently needs more research on the antecedents of value co-creation, particularly regarding how technological factors are associated with patient co-creation behaviors in a hybrid online-offline medical environment, where exploration remains insufficient.27,28 In the current era of rapid digital transformation, sufficient recent research has confirmed that customers’ digital touchpoint experiences have a significant association with their organizational image perception and subsequent behaviors.29–33 In the healthcare context, although the importance of digital technology touchpoints for patient experience and service quality has been widely recognized,34–36 this complete path from technology experience to organizational cognition and then to co-creation behavior has not yet received systematic theoretical elaboration and empirical testing.
To address the research gaps, this study proposes the following research question: In the digital healthcare context, how are patients’ experiences with OAS associated with their value co-creation behaviors through hospital image (HI)?
To answer this question, this study constructs a theoretical model based on the Stimulus-Organism-Response (SOR) framework,12,37,38 It positions the technological experience of the OAS as the stimulus, HI as the patient's internal cognitive state, and patient value co-creation behavior as the response, explaining the complete path by which technology experience, through shaping organizational cognition, is subsequently associated with the activation of co-creation behaviors. This study employs structural equation modeling using SmartPLS 4.0 to empirically test this theoretical framework.
Theoretically, this study integrates the SOR framework and the Service-Dominant Logic (SDL) perspective, positioning patient value co-creation behavior as the final response variable, and systematically traces its complete formation mechanism in a digital context, filling an important gap in existing research. The study identifies HI as a key psychological transmission mechanism linking technology experience and co-creation behavior, revealing the pathway by which digital touchpoints may require transformation through patients’ internal cognition to be associated with co-creation behaviors, and preliminarily identifying the boundaries of the direct associations of technology stimuli. Practically, this study provides a reference for medical institutions to reposition the strategic value of OAS, shape HI by optimizing digital touchpoints, and adopt differentiated management strategies for co-creation behaviors of varying complexity.
Theoretical background
Applying SOR to digital healthcare: integrating an SDL perspective
The SOR framework, proposed by Mehrabian and Russell 39 to explain how environmental stimuli influence behavioral responses through an individual's internal psychological mechanisms. The core logic of this framework is that external stimuli do not directly determine behavior, but rather indirectly lead to behavioral changes by activating an individual's internal states, including cognition, emotion, and attitudes. 40 Jacoby 37 pointed out that, compared to simple input-output models, the SOR framework can more accurately depict the psychological, fluid, dynamic, and recursive processes of consumer behavior.
The SOR framework was initially applied in consumer behavior and environmental psychology research, and in recent years has gradually expanded to service marketing, information systems, and healthcare services.41–43 In the current context of digital transformation in healthcare, the SOR framework is suitable for explaining how technology-based service encounters (TSE) influence patient behavior.34,44,45 With the rise of the patient-centric service philosophy, understanding how patients perceive technological systems, form evaluations of medical institutions, and adjust their participation behaviors accordingly has become an important research issue.46,47 The key value of the SOR framework lies in clarifying the mediating role of the organism: not all stimuli can be directly transformed into behavior; many stimuli must be processed and transformed by internal psychological states to produce meaningful behavioral responses.37,48
Although the SOR framework provides a concise and powerful theoretical lens for understanding customer behavior, it still presents a certain simplification of the complexity of the healthcare context. 40 For example, factors such as the patient's disease state, health literacy, and digital skills may moderate the transformation process from stimulus to response, and these boundary conditions are not fully considered in the classic SOR framework.49,50 However, as a classic theoretical framework that is both concise and highly explanatory, SOR continues to be applied and validated in recent patient behavior research, providing a robust theoretical foundation for understanding how technology encounters influence patient behavior through psychological mechanisms.43,51,52
In this study, the OAS-TSE is positioned as the stimulus (S). Research indicates that TSE are external environmental elements that patients encounter during the medical treatment process.53–55 Jacoby 37 categorized such factors into the first region, namely the environment an individual encounters at a specific moment. As the primary contact point for patients entering the healthcare system, the characteristics of the OAS, such as its usefulness, convenience, and ease of use, constitute a set of external stimuli. These stimuli trigger subsequent responses at the patient's psychological level.38,56
HI, as the organism (O), represents the patient's internal cognitive and emotional state toward the medical institution.57–59 Jacoby 37 noted that organism factors include an individual's long-term memory and current consciousness; these internal states are activated when receiving external stimuli and are responsible for interpreting and processing them. HI involves the patient's perception of the hospital's reputation, service quality, and overall status. Such perceptions originate from the accumulation of past experiences and are also activated and updated during current service encounters.60,61
Patient value co-creation behavior constitutes the response (R) in the SOR framework. Value co-creation behavior is essentially the patient's active participation and engagement in the medical service process, manifested as a series of actions where patients integrate their own knowledge, experience, and resources into the service process.10,12 SDL provides an important perspective for understanding value co-creation, emphasizing the central role of the patient as a resource integrator in value creation. Value is not unilaterally created by the service provider but is co-generated through the interaction between the patient and medical staff.62,63 However, existing SDL research mainly focuses on the outcomes and dimensions of value co-creation, with limited discussion on the psychological mechanisms of how TSE in a digital healthcare context trigger patient value co-creation behaviors.27,28 This study integrates the SOR framework with the SDL perspective to explore how technology stimuli trigger patient value co-creation behaviors through the psychological mechanism of HI. In the SOR framework, responses include all externally observable verbal, non-verbal, and behavioral expressions.64,65 Value co-creation behavior is externally observable and goal-oriented, fitting this definition.28,66 More importantly, value co-creation behavior is not an automatic stimulus reflex but a purposeful action requiring conscious patient participation. 67 Jacoby 37 emphasized that meaningful behavioral responses usually stem from cognitive processing and emotional evaluation of external stimuli, rather than simple conditioned reflexes. Value co-creation behavior is precisely this type of response that follows psychological processing. Its occurrence depends on the activation of the patient's internal motivation and their assessment of the benefits of participation, reflecting the complete transformation process from external stimulus to internal cognition and then to behavioral expression. 27
Hypothesis development
The relationship between OAS-TSE and HI
TSE, through characteristics such as perceived usefulness, convenience, and ease of use, directly influence the patient's overall evaluation of the medical institution.68,69 As the primary contact point for patients entering the healthcare system, the performance of the OAS-TSE will be generalized by patients to judge the hospital's overall service quality and professional capability.38,70,71 An efficient and convenient appointment experience reinforces positive patient perceptions of the hospital's modernization and service capabilities, whereas a poor technology experience may weaken patient trust and evaluation of the hospital.53,72,73 For the organization, this positive overall image is regarded as a critical intangible asset, which can significantly predict the subsequent participation willingness and co-creation behaviors of stakeholders.33,74,75
Therefore, this study proposes: H1: OAS-TSE has a significant positive association with HI.
The relationship between HI and patient value co-creation behaviors
HI, as the patient's internal cognitive and emotional state toward the medical institution, activates the patient's willingness and behavioral investment to participate actively in the medical service process.76,77 According to the SOR framework, organism factors trigger meaningful behavioral responses by interpreting and processing external stimuli. A positive HI enhances patient identification and psychological safety regarding the medical institution, which in turn encourages patients to be more willing to contribute their own knowledge, experience, and resources during the service process. 78
A good HI represents the patient's comprehensive cognition of the hospital's reputation, service quality, and professional competence.79,80 When patients hold a positive evaluation of the HI, this positive overall impression reduces the psychological distance and defensiveness in patient communication, making them more willing to express their needs, feedback, and doubts to medical staff, actively share symptom information, express treatment preferences, and cooperate with medical staff's advice.57,81
Therefore, this study proposes: H2a: HI has a significant positive association with Dialogue.
Therefore, this study proposes: H2b: HI has a significant positive association with Access.
Therefore, this study proposes: H2c: HI has a significant positive association with Risk Assessment.
Therefore, this study proposes: H2d: HI has a significant positive association with Transparency.
OAS-TSE and patient value co-creation behaviors: direct associations and mediation mechanisms
The SOR framework emphasizes that external stimuli primarily influence behavioral responses indirectly through internal psychological states. 37 However, in specific contexts, high-quality technology service encounters may also have certain direct effects on patient behavior.96,97 High-quality OAS-TSE, with premium features like usefulness, convenience, and ease of use, provide patients with a positive technology experience. This positive experience may directly lower the psychological barrier for patients to participate in the medical process and trigger more active participation behaviors.38,98 At the same time, the good technical performance of OAS-TSE also enhances the patient's cognitive evaluation of the hospital's overall capabilities, and indirectly influences patient participation willingness by shaping the psychological mechanism of HI.38,72,99 This study explores the direct associations of OAS-TSE on patient value co-creation behaviors and their indirect associations via HI.
High-quality OAS-TSE provide patients with a positive service experience, which may cultivate a tendency for active participation in medical services.100,101 When patients successfully complete registration through a convenient appointment system, this smooth interaction experience may extend to the subsequent medical process, making patients more willing to actively cooperate with medical staff's inquiries, discuss treatment or care plans, and share opinions on service improvement. 53
Therefore, this study proposes: H3a: OAS-TSE has a significant positive association with Dialogue. H4a: HI mediates the relationship between OAS-TSE and Dialogue.
Therefore, this study proposes: H3b: OAS-TSE has a significant positive association with Access. H4b: HI mediates the relationship between OAS-TSE and Access.
Therefore, this study proposes: H3c: OAS-TSE has a significant positive association with Risk Assessment. H4c: HI mediates the relationship between OAS-TSE and Risk Assessment.
Therefore, this study proposes: H3d: OAS-TSE has a significant positive association with Transparency. H4d: HI mediates the relationship between OAS-TSE and Transparency.

Conceptual framework.
Method
Questionnaire development
This study developed the questionnaire by adapting validated scales from existing literature. Both OAS-TSE and HI were measured using the scale from Wang et al. 38 The former includes four items, assessing patients’ perceived usefulness, timesaving, convenience, and ease of use of the hospital's OAS; the latter includes three items, capturing patients’ perceptions of the hospital's reputation, medical service quality, and overall status.
Patient value co-creation behavior was measured using the Dialogue, Access, Risk Assessment, and Transparency (DART) framework adapted by Mai et al. 12 This scale includes 23 items, covering four dimensions: Dialogue (six items, measuring active cooperation and communication with medical staff), Access (seven items, assessing behaviors of actively seeking and utilizing health-related information and resources), Risk Assessment (six items, evaluating the ability to inquire about potential risks and take responsibility for health decisions), and Transparency (four items, measuring the willingness to truthfully disclose health information and seek comprehensive information). Authorization was obtained from the original authors for the use of all scales.
A pre-test was conducted at Luoyang First People's Hospital to ensure item clarity and preliminary reliability. One item in the Risk Assessment dimension (“I will compare the benefits of different options before making a decision”) was deleted due to an insufficient factor loading. The final questionnaire contained 29 items, with the Risk Assessment dimension reduced to five items. All scales used a 5-point Likert scale (1 = strongly disagree, 5 = strongly agree). The complete list of measurement items is provided in the Appendix.
Study design and data collection
This study employed an online survey method. Respondents accessed the questionnaire via the Wenjuanxing website (https://www.wjx.cn/), a widely used online survey platform in China that provides professional respondent recruitment and targeted sampling services for academic research, including healthcare studies.113–115 The platform incorporates several quality control mechanisms, including response time verification, IP address tracking, and consistency checks, to ensure data reliability. 116 Before participating in the survey, respondents were informed of the research purpose, the ultimate use of the data, and the non-commercial nature of the data collection. The platform's built-in informed consent function required respondents to read and electronically agree to the informed consent form before proceeding; only those who provided consent were allowed to continue with the survey.117,118 The informed consent form explained respondents’ rights to participate and withdraw from the survey at any time. At this stage, all respondents were reminded that there are no right or wrong answers and were encouraged to provide truthful responses to minimize potential biases from data collection.
Participant inclusion criteria were: (1) adults aged 18 and above; (2) first-time visit to the hospital within the past 3 months; (3) used the hospital's OAS for booking; and (4) voluntary participation in the study. Only respondents who met all inclusion criteria were allowed to proceed with the survey.
A total of 408 questionnaires were collected. Following data cleaning, 21 responses were excluded due to incomplete data or response times shorter than 90 s, 119 resulting in 387 valid questionnaires for analysis. A priori power analysis using G*Power indicated that a minimum sample size of 68 was required to detect medium effect sizes (f2 = 0.15) with 80% power at α = 0.05 for two predictors; thus, the sample size was deemed adequate.120,121 Structural equation modeling analysis was performed using SmartPLS 4.0.
Ethical considerations
This study followed the Declaration of Helsinki and received ethical approval (Approval No. EC-2025-1001). Participants in the pre-test provided written informed consent before proceeding. For the main survey, participants provided electronic informed consent via the platform's built-in consent function. Personal information was anonymized, and data privacy was strictly protected. Participants could withdraw from the study at any stage without condition.
Sample characteristic
As shown in Table 1, Data were collected from 387 respondents who had used the hospital's OAS. The sample comprised slightly more females (52.71%) than males (47.29%). The majority of respondents were aged between 18–40 years (56.08%), reflecting the younger demographic more actively engaged with digital healthcare services.
Sample characteristic.

In terms of educational background, the sample was relatively well-educated, with bachelor's degree holders representing the largest group (35.66%), followed closely by college diploma holders (34.88%). Approximately one-tenth of respondents held master's degrees or above (9.82%), while 19.64% had high school education or below.
Regarding monthly income, the sample showed a typical middle-income distribution pattern. The largest proportion earned between RMB 2500–4000 (28.42%) and RMB 4001–6000 (26.61%), with fewer respondents in the lower income bracket below RMB 2500 (15.76%) and higher income brackets above RMB 8000 (11.63%).
In terms of healthcare utilization, most respondents had visited hospitals 2–3 times annually (41.60%), followed by single-visit patients (27.39%). Approximately one-third of the sample (31.01%) reported four or more hospital visits per year, indicating diverse healthcare needs within the sample.
Results
Common method bias assessment
To ensure data quality, this study assessed common method bias (CMB) using multiple methods. First, Variance Inflation Factors (VIF) were used to evaluate multicollinearity. The results showed that VIF values for all paths ranged from 1.000 to 1.391, well below the critical standard of 5.0.122,123 This indicates that no severe multicollinearity issues exist among the model variables, and each predictor variable maintains a relatively independent explanatory role for the dependent variables.
Furthermore, Harman's single-factor test was employed to assess potential CMB. The results indicated that the first principal component explained 33.2% of the variance, which is below the 50% critical threshold. 124 Based on these test results, the CMB in this study's data is within an acceptable range.
Measurement model assessment
This study assessed the reliability of the measurement model using Cronbach's α and Composite Reliability (CR). As shown in Table 2, all constructs’ Cronbach's α values ranged from 0.812 to 0.915, and CR values ranged from 0.876 to 0.932, both exceeding the recommended standard of 0.70. 122 These results demonstrate that the measurement tools in this study possess good internal consistency reliability.
Reliability and convergent validity.
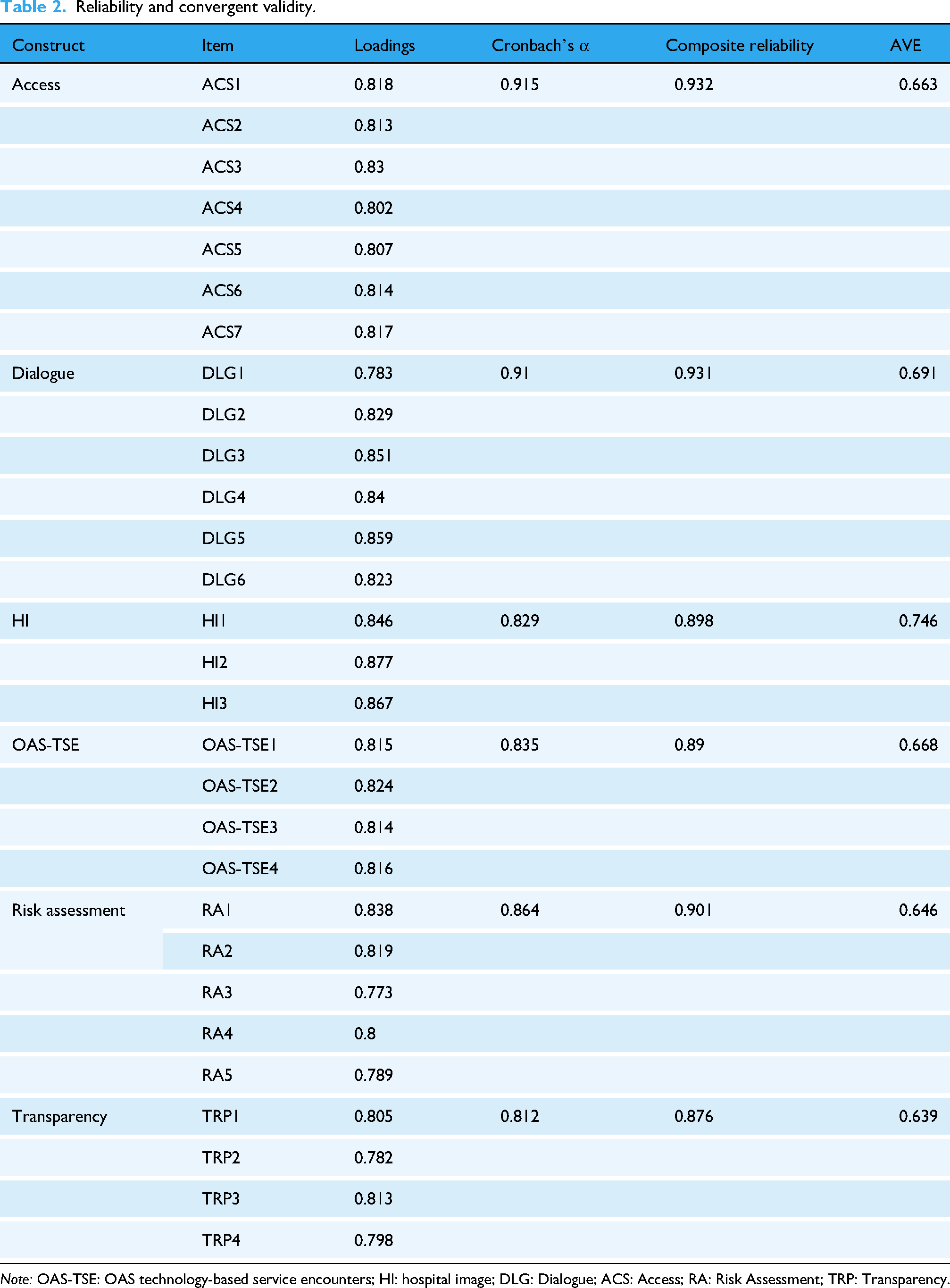
Note: OAS-TSE: OAS technology-based service encounters; HI: hospital image; DLG: Dialogue; ACS: Access; RA: Risk Assessment; TRP: Transparency.
To examine the convergent validity of the measurement model, the factor loadings of each item and the Average Variance Extracted (AVE) were further tested. The AVE values for all constructs ranged from 0.639 to 0.746, all exceeding the recommended standard of 0.50. 125 The vast majority of item factor loadings surpassed the recommended threshold of 0.70.126–128
Discriminant validity
The Fornell-Larcker criterion and the Heterotrait-Monotrait Ratio (HTMT) were adopted, as shown in Table 3. According to the Fornell-Larcker criterion analysis, the square root of the AVE for each construct (bold values on the diagonal in Table 3) was greater than the correlation coefficients between that construct and others, meeting the discriminant validity standard proposed by Fornell and Larcker. 125
Discriminant validity assessment.
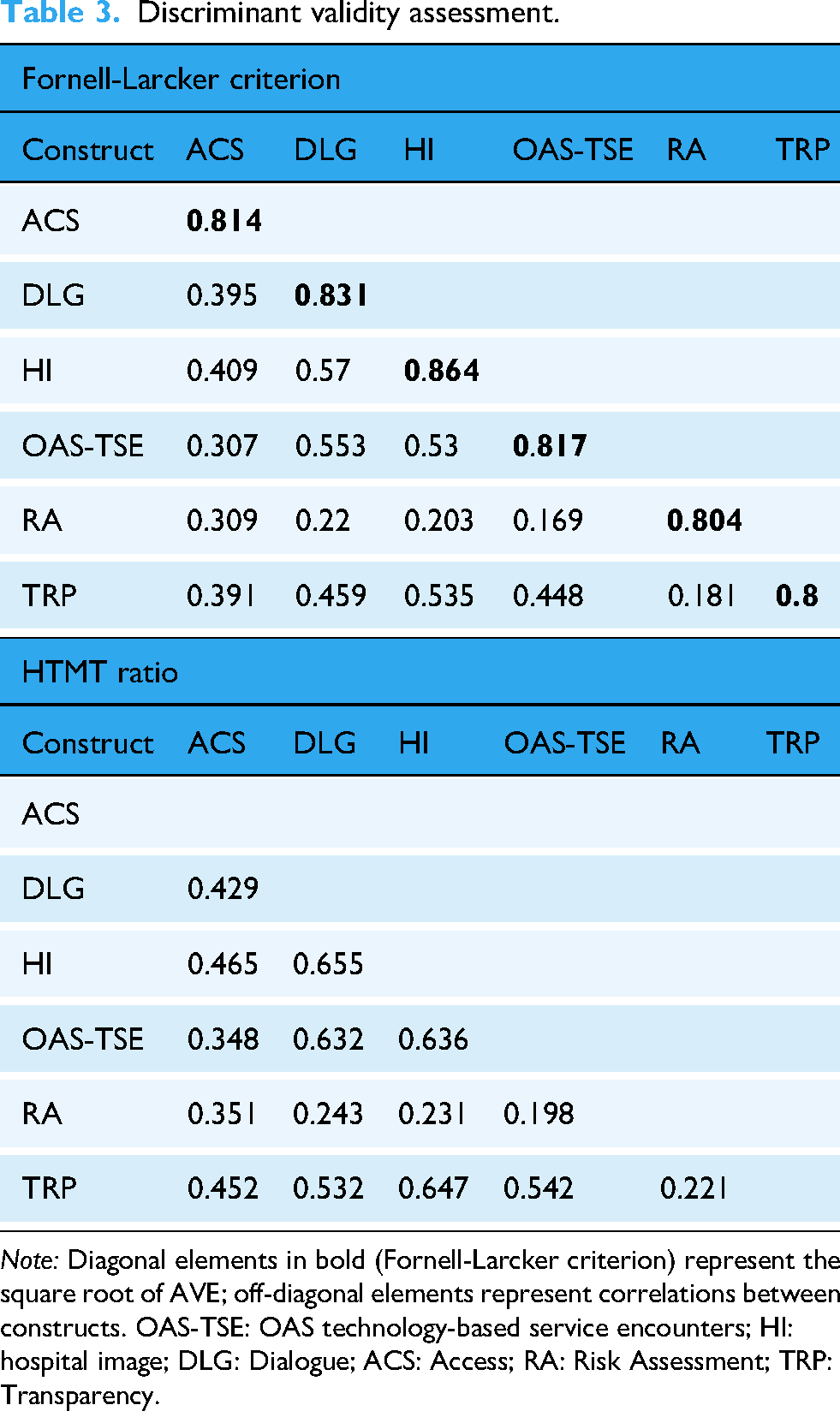
Note: Diagonal elements in bold (Fornell-Larcker criterion) represent the square root of AVE; off-diagonal elements represent correlations between constructs. OAS-TSE: OAS technology-based service encounters; HI: hospital image; DLG: Dialogue; ACS: Access; RA: Risk Assessment; TRP: Transparency.
The HTMT ratio analysis showed that all HTMT values between construct pairs ranged from 0.169 to 0.655, far below the recommended threshold limit of 0.90. 129 This further confirms good discriminant validity among the constructs, indicating that the constructs in this study are conceptually distinct.
Hypothesis testing
As shown in Table 4, all hypotheses except H3c were statistically supported. The direct association analysis showed that OAS-TSE had a significant positive association with HI (β = 0.530, t = 11.385, p < 0.001), supporting H1. HI had significant positive associations with Dialogue (β = 0.385, t = 6.647, p < 0.001), Access (β = 0.342, t = 5.841, p < 0.001), Risk Assessment (β = 0.157, t = 2.407, p < 0.05), and Transparency (β = 0.414, t = 7.514, p < 0.001), supporting H2a, H2b, H2c, and H2d.
Hypothesis testing results.

Note: OAS-TSE: OAS technology-based service encounters; HI: hospital image; DLG: Dialogue; ACS: Access; RA: Risk Assessment; TRP: Transparency; CI: confidence interval.
*p < 0.05, **p < 0.01, ***p < 0.001.
OAS-TSE also exhibited direct associations with patient co-creation behaviors. OAS-TSE had significant positive associations with Dialogue (β = 0.349, t = 5.795, p < 0.001), Access (β = 0.125, t = 2.176, p < 0.05), and Transparency (β = 0.228, t = 4.045, p < 0.001), supporting H3a, H3b, and H3d. However, the direct association between OAS-TSE and Risk Assessment was not significant (β = 0.086, t = 1.385, p = 0.166), thus H3c was not supported.
Regarding mediation, HI significantly mediated the relationship between OAS-TSE and Dialogue (β = 0.204, t = 5.541, p < 0.001), Access (β = 0.182, t = 5.229, p < 0.001), Risk Assessment (β = 0.083, t = 2.342, p < 0.05), and Transparency (β = 0.220, t = 6.274, p < 0.001), supporting H4a, H4b, H4c, and H4d.
The R2 values for the endogenous constructs showed varying explanatory power. Dialogue (R2 = 0.412) and Transparency (R2 = 0.324) demonstrated acceptable explained variance. The explained variance for HI (R2 = 0.281) and Access (R2 = 0.178) was relatively low, while the explained variance for Risk Assessment (R2 = 0.046) was markedly low. 121 These results will be explored further in the Discussion section.
Discussion
Based on the SOR framework, this study explored the associations among OAS-TSE, HI, and patient value co-creation behaviors. The findings largely support and extend the theoretical model, while also revealing the complexities of different behavioral dimensions.
First, a core finding of this study is the significant, strong positive correlation between OAS-TSE and HI. This result suggests that in the digital healthcare context, OAS is no longer just an efficiency tool but has become a digital forefront for HI. The technical experience patients gain at the very beginning of the medical process, such as convenience and ease of use, appears to be associated with their cognitive and emotional evaluations of the medical institution's overall image, including reputation and service quality. This finding is consistent with existing research, which posits that touchpoint experiences are generalized into users’ overall perception of the organization.38,70,71 This highlights the strategic value of TSE in organizational image management, a finding that is particularly important as digitalization becomes more prevalent among patients. 130
Second, the results strongly support the core psychological transmission role of HI within the model. HI was not only significantly positively associated with all four dimensions of value co-creation, but it also demonstrated a significant mediating effect in the relationships between OAS-TSE and these four dimensions. This indicates that the association between the external stimulus (OAS) and patient participation behavior is largely transmitted through the mechanism of the patient's internal psychological state. When patients hold a positive overall impression of the hospital, they tend to show greater activation, leading to a higher willingness to invest their own knowledge and resources in the healthcare service process. This finding also confirms the view in the healthcare context that organizational image is a key psychological antecedent that activates customer participation and co-creation behaviors. 32
However, this study also reveals differences across behavioral dimensions. Notably, the direct association between OAS-TSE and Risk Assessment was not significant. Interestingly, Lee 131 previously found in research on healthcare technology encounters that technology-mediated contact could not even directly improve patient satisfaction. In contrast, this study did observe significant direct associations between OAS-TSE and the other three value co-creation behaviors (Dialogue, Access, and Transparency). This perhaps reflects the increasing direct role of technology touchpoints in the patient journey as digital healthcare becomes more pervasive and advanced. 47
Nonetheless, the absence of a direct association between OAS-TSE and Risk Assessment clearly marks a boundary for the direct associations of technology. This seems to suggest that even as technology becomes more important, for complex behaviors like Risk Assessment that require higher-order cognitive engagement, a foundation of trust, and responsibility for decisions, technological convenience alone is insufficient to form a direct association. The activation of such behaviors appears to be more reliant on an indirect relationship, where the technology encounter first enhances the patient's overall perception of the institution.
This boundary of technology's direct association might be further understood by the differences between the functional characteristics of OAS and the demands of Risk Assessment behavior. The core function of an OAS is to optimize processes and provide convenience. 132 This convenience may be sufficient to be directly associated with some behaviors with relatively low participation barriers, such as Dialogue or Access.133,134 However, Risk Assessment is a complex, judgment-based behavior highly dependent on patient expertise, cognitive engagement, and decisional responsibility. 135 A smooth appointment system experience alone seems insufficient to directly predict whether patients will engage in such a difficult cognitive task. 136 Given that Risk Assessment behavior involves shared responsibility for treatment and risk, and this study shows HI plays a key transmission role, this implies that healthcare providers should perhaps focus on optimizing the digital touchpoint experience to build a positive organizational image, which may be critical for promoting patient participation in such high-order co-creation behaviors. 47
Interestingly, this lack of a direct association between technology use and specific subsequent behaviors is also reflected in another research. For example, Silver et al. 137 found that actual portal usage frequency itself did not significantly predict health-seeking behaviors. This is similar to the finding of this study regarding OAS-TSE and Risk Assessment, and together these findings suggest that technology use may function more as a foundational condition or source of experience. To effectively translate this user experience into more complex or proactive patient health behaviors, a key psychological transformation process seems to be required. The results of this study indicate that the patient's overall perception of the medical institution plays precisely such an important mediating role.
The unique nature of the Risk Assessment dimension is also reflected in its model's overall explanatory power. The markedly low R2 value for Risk Assessment reflects the multi-factorial nature of this behavior. While our model focuses on OAS-TSE and HI and reveals a key pathway, Risk Assessment, as a high-order cognitive behavior, is influenced by multiple factors such as health literacy, digital literacy, disease severity, physician-patient communication quality, and healthcare accessibility.138–141 Although Hair Jr et al. 121 noted that low R2 values are considered acceptable in some disciplines, the low explanatory power for the Risk Assessment dimension does indicate the influence of unmeasured factors. This also highlights the complexity of digital health research, and future studies should pay closer attention to the factors influencing treatment in a digital environment.117,142
In summary, this study reveals that OAS, as a digital forefront for the hospital, is indirectly associated with patient value co-creation through the psychological mechanism of HI. Although technology may not be directly associated with all types of behavior, especially complex ones such as Risk Assessment, it plays a vital role in shaping patients’ internal perceptions. This positive organizational image, transformed from the technology experience, serves as a valuable psychological resource for activating subsequent patient participation in the medical process.
Theoretical contributions
First, this study contributes by identifying a specific digital touchpoint as a key antecedent (S) to active patient value co-creation (R) in the healthcare SOR framework. While extensive research has called for studies on the antecedents of value co-creation, especially regarding technology's influence,27,28 previous patient value co-creation research has often focused on outcomes or used co-creation as a mediator.13,26 Our study responds by providing direct empirical evidence of the association between the OAS-TSE (S) and the active, in-service process of patient value co-creation (R).
Second, beyond establishing this antecedent link, this study explores how this association occurs by providing preliminary evidence for the role of HI (O) as a key psychological transmission mechanism. Our exploratory findings suggest that HI is a critical mediator. This finding contributes by extending the understanding of the pathway from organism to response in this context. While the link between organizational image and customer co-creation has been explored in general consumer or business contexts,32,143 this association remains underdeveloped in the unique healthcare environment, which is characterized by high professionalism, risk, and information asymmetry.144,145
Third, by deconstructing behavior using the DART multidimensional framework, this study preliminarily identifies the potential boundaries of the direct OAS-TSE to co-creation association. This finding offers certain implications for technology acceptance research, suggesting that different types of patient participation behaviors may have differentiated response patterns to technology stimuli. For participation behaviors with relatively low cognitive load, the technology convenience stimulus may have a more direct association. Conversely, for complex behaviors involving high-order cognitive judgment, risk trade-offs, and decisional responsibility, the technology stimulus appears to need transformation through the patient's internal psychological state into a cognition of the medical institution's capability and trustworthiness, to be indirectly associated with patient participation. This observation enriches the theoretical understanding of the mechanisms of digital health technology's influence and provides preliminary empirical evidence for future research to consider the potential role of behavioral complexity in the technology acceptance process.
Practical implications
This study, by exploring the associations among OAS, HI, and patient value co-creation, offers several practical implications for digital transformation and patient participation management in healthcare institutions.
This study suggests that OAS platforms are not merely instrumental tools for improving service efficiency but are also important channels for shaping the overall HI. Hospital managers may need to reassess the strategic positioning of OAS, elevating them from simple booking tools to integral components of hospital brand building and image management.
Specifically, hospitals could consider integrating OAS into their overall brand-building framework. For example, they might add assessment items to patient satisfaction surveys about how the appointment system experience is associated with the hospital's overall impression, and include patient experience indicators such as the system's usefulness, convenience, and ease of use within the key performance indicators for brand management.137,146 Furthermore, hospitals could also strengthen the communication of brand elements and values in the system's interface design, for instance, by incorporating hospital logos, service philosophies, or expert team introductions into the appointment interface. This would allow patients to more intuitively perceive the hospital's professionalism and service commitment while using the system.147–149
Further, hospitals could consider establishing a tracking and evaluation mechanism for the pathway from technology experience to HI and then to patient participation. By regularly monitoring the system's technical performance indicators, such as response speed, failure rates, and user task success rates, and by analyzing how these technical issues are associated with patients’ HI evaluations, 150 hospitals could more precisely identify which technical problems are most likely to damage the overall HI and thus prioritize resources for improvement. Such a systematic tracking mechanism would not only help to continuously optimize the technical system itself but also aid in maintaining and enhancing the hospital's overall image in patients’ minds, thereby promoting active patient participation behaviors.151,152
This study suggests that when promoting patient participation in the healthcare service process, hospital managers may need to adopt differentiated management strategies for co-creation behaviors of varying complexity. For participation behaviors such as Dialogue, Access, and Transparency, hospitals could continuously optimize the OAS's user interface and interaction flow to reduce operational difficulty for patients. 153 For example, providing clear instructions on the visit process, FAQs, and convenient online consultation access within the system could help patients more easily obtain needed information and actively communicate with medical staff.154,155 These measures might help encourage these types of participation behaviors by improving the technology experience.
However, for complex participation behaviors like Risk Assessment, which involve high-order cognitive judgment and decisional responsibility, promoting patient participation may require hospitals not only to provide a high-quality technology experience to enhance the overall HI, but also to continuously reinforce the hospital's professionalism, reliability, and compassion throughout all stages of the patient-provider interaction.156,157 For example, by fostering deep patient trust through sufficient communication from medical staff, personalized treatment plan explanations, and patient education, hospitals might encourage greater participation in complex co-creation behaviors such as treatment decisions. 158 This differentiated management strategy may help hospitals more effectively activate various types of patient participation behavior, enhancing the overall quality of medical services. 159
Conclusion
This study explored the association mechanisms between OAS and patient value co-creation behaviors in the digital healthcare context. The findings suggest that HI plays a key psychological transmission role in the link between technology touchpoints and patient co-creation behaviors. This indicates that patients’ experiences with OAS may be associated with their participation in medical services by shaping their overall cognition of the medical institution. This finding reveals the role of digital touchpoints in patient cognitive formation; the performance of technology systems may become one of the important bases for patients to evaluate medical institutions. Notably, co-creation behaviors of different complexities respond differently to technology experiences; the activation of high-order cognitive behaviors, such as Risk Assessment, appears to be more dependent on the transmission role of HI. This study provides a theoretical perspective for understanding patient participation mechanisms in the digital healthcare context and offers practical references for medical institutions to optimize digital touchpoints to promote patient participation. Future research could further verify the causal nature of these associations through experimental or longitudinal designs and explore other potential factors associated with patient co-creation behaviors.
Limitations and future recommendations
This study has several methodological and contextual limitations. First, the sampling method may introduce systematic bias. The online questionnaire distribution method is more likely to reach patients familiar with digital technology, potentially excluding groups with lower digital literacy. This implies that patients who experience significant difficulties with or resistance to using digital technology may be underrepresented in the sample. This group's experience with OAS and their perception of HI may differ significantly from those of proficient users, thereby weakening the representativeness of the findings. Second, the cross-sectional design and complete reliance on self-reports limit the strength of causal inference. Although CMB was tested, social desirability bias and recall bias may still exist, and the lack of validation with objective behavioral data further weakens the causal claims. Third, the model's explanatory power is limited, particularly for the Risk Assessment dimension, which showed markedly low explained variance. This indicates the presence of important unmeasured factors, suggesting that patient participation in complex decision-making behaviors may be activated by a more diverse set of factors.
Despite these limitations, this study still reveals the important role of digital touchpoints in the activation process of patient value co-creation behaviors, particularly identifying the value of HI as a key psychological transmission mechanism. Future research can further deepen and expand upon these findings in several ways.
First, to address the limitations of causal inference, future studies could employ experimental designs or longitudinal tracking to strengthen the verification of causal relationships. For example, a quasi-experimental design could compare changes in patients’ HI and co-creation behaviors before and after the optimization of an OAS. Alternatively, a short-term longitudinal design could conduct two follow-up surveys within the same medical institution, tracking the dynamic changes in HI perception and participation behaviors from the patient's initial use of the system to repeated use, while controlling for baseline characteristics to enhance the reliability of causal inferences.
Second, sampling strategies should be improved to enhance sample representativeness. Future research could combine online and offline survey methods, for instance, by using on-site paper questionnaires or telephone interviews to cover patient groups with lower digital literacy. Collaborating with community medical institutions could also help reach a broader range of patient types, allowing for comparisons of trust formation and participation behaviors across different digital proficiency groups. Additionally, future studies could compare patients who use OAS with those who use traditional appointment methods (e.g. walk-in or telephone booking) to examine whether different appointment channels are associated with distinct patterns of HI perception and value co-creation behaviors. Furthermore, incorporating qualitative methods such as semi-structured interviews or focus groups could provide a richer, deeper understanding of how technology experiences are transformed into HI perceptions and patient participation motives, offering explanatory evidence for quantitative models.
Third, to address the issue of low explanatory power for the Risk Assessment dimension, future studies could explore other key factors influencing patient participation in Risk Assessment. For example, variables such as patients’ health literacy, disease severity, prior medical experiences, and the quality of physician-patient communication could be included to more comprehensively understand the diverse mechanisms driving patient participation in complex decision-making behaviors in the digital healthcare context and to identify the relative importance of different factors.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076261420892 - Supplemental material for The digital front door: How online appointment systems build hospital image and activate patient value co-creation
Supplemental material, sj-docx-1-dhj-10.1177_20552076261420892 for The digital front door: How online appointment systems build hospital image and activate patient value co-creation by Luxin Zhang and Zenglin Wu in DIGITAL HEALTH
Footnotes
Acknowledgments
The authors would like to thank the healthcare professionals at Luoyang First People's Hospital and its affiliated hospitals for their support in data collection. We also extend our gratitude to all participants who voluntarily completed the questionnaire and made this research possible.
Author contributions
Luxin Zhang was responsible for conceptualization, data collection, data analysis, and manuscript drafting.
Zenglin Wu provided supervision, theoretical guidance, methodological validation, and critical revisions of the manuscript. All authors reviewed and approved the final manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the Nanfang College, Guangzhou Doctoral Research Fund Project (Grant Number 2025BQ060).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.