
Abstract
Objectives
This study aimed to systematically characterize the landscape of artificial intelligence (AI) applications in gynecologic cancers, offering a comprehensive overview of current research trends, influential publications, key contributors, and future research directions. The focus of this study was to provide a quantitative overview of the field's development and trends.
Materials and Methods
A structured search was performed in the Web of Science Core Collection to identify original articles on AI use in gynecologic oncology. Two independent reviewers screened and selected studies based on predefined inclusion criteria. Extracted data—including publication trends, author and institutional collaborations, keyword co-occurrence, and citation networks—were analyzed using CiteSpace 6.2.R6 and VOSviewer software.
Results
A total of 2544 articles were included for analysis. Research activity showed a notable acceleration after 2019, reaching its highest output in 2024. China and the United States emerged as dominant contributors, with the Chinese Academy of Sciences and Fudan University leading among institutions. Influential authors such as Sala Evis, Tian Jie, and Scambia Giovanni were identified. Major research themes focused on “Radiomics,” “Deep Learning,” “Radiotherapy,” and cancers including cervical, ovarian, and endometrial. Recent emerging topics included “Digital Pathology,” “Personalized Medicine,” and “Tumor Heterogeneity,” signaling a shift toward precision oncology.
Conclusions
This bibliometric study delineated the evolving field of AI in gynecologic oncology, highlighting dynamic research fronts and gaps.
Introduction
Gynecological cancers, including ovarian cancer, cervical cancer, and endometrial cancer, have become an important global public health issue, primarily due to their rising incidences and the significant burden on women's health worldwide. For instance, ovarian cancer is usually detected at advanced stages, as subtle early symptoms often present with a poorer prognosis. 1 Endometrial cancer, which is generally associated with obesity and metabolic syndrome, has shown a concerning trend toward younger age at diagnosis. 2 Similarly, cervical cancer remains highly prevalent in low-resource settings, especially in low-resource settings. 3 While advancements in imaging and molecular analysis have improved the accuracy of early detection for these malignancies, many challenges remain, such as resolving tumor heterogeneity, enhancing prognostic accuracy, and predicting treatment response.4,5
Artificial intelligence (AI), particularly machine learning and deep learning, has emerged as a powerful tool to address these challenges. Artificial intelligence systems are capable of processing and interpreting large-scale clinical, radiologic, and genomic data, thereby offering opportunities to enhance diagnostic accuracy, guide personalized treatment, and refine prognostic modeling. 6 In gynecologic oncology, AI applications already encompass imaging-assisted diagnosis, pathology, and molecular profiling, and their impact on clinical decision-making is expanding rapidly. 7 Nevertheless, the intellectual structure, developmental trajectory, and global dissemination of research in this field have not yet been systematically characterized. To address this gap, the present study employs bibliometric methods to provide a comprehensive overview of AI-related research in gynecologic oncology.
The application of AI in gynecologic oncology differs from that in other cancers. Unlike breast or lung cancer, which benefit from established screening programs and large public datasets, ovarian and cervical cancers present unique diagnostic difficulty due to subtle early symptoms and the lack of reliable early biomarkers. The complex anatomy of the female pelvis further necessitates multimodal integration of ultrasound, computed tomography (CT), magnetic resonance imaging (MRI), and histopathology, making this field particularly amenable for AI-driven multimodal approaches. These distinctions are highlighted in the International Federation of Gynecology and Obstetrics Cancer Report 2025, 8 which underscores AI's capacity to improve early detection and treatment planning while also cautioning that issues such as algorithmic bias, data privacy, and the need for rigorous validation must be addressed before routine clinical adoption. Taken together, these features underscore the rationale for a domain-specific bibliometric analysis: AI in gynecologic oncology follows distinct research trajectories and translational priorities compared with broader oncology fields, offering both opportunities and challenges for equitable clinical implementation.
Bibliometric analysis serves as an established quantitative method for visualizing knowledge landscapes and identifying research hotspots across disciplines. 9 By systematically retrieving and analyzing literature using statistical and computational techniques, bibliometric studies offer valuable insights into publication trends, major contributors, landmark publications, and patterns of scientific collaboration. 10 Such analyses are instrumental in shaping future research priorities, promoting interdisciplinary and international cooperation, and informing evidence-based policy development in AI-driven healthcare for gynecologic malignancies. This study aims to contribute to the understanding of AI's growing role in this field, providing a foundation for future research and clinical application.
This study has examined publication trends, identified major contributors, explored collaborative networks, and analyzed research hotspots by reviewing data sourced from the Web of Science Core Collection (WoSCC). The focus of this study is not to review AI algorithms or clinical applications in depth, but to offer a quantitative overview of the field's development and trends. It presents an overview of AI applications in gynecologic cancers from a global perspective, which may help inform future research directions and facilitate collaboration across disciplines, advancing the clinical integration of AI in gynecologic oncology.
Materials and methods
Data sources and search strategy
Bibliographic records were sourced exclusively from the WoSCC, which provided comprehensive coverage of peer-reviewed publications in a wide array of disciplines. We conducted a detailed search using a combination of keywords associated with AI and gynecologic malignancies. The search query was constructed as follows: TS = (“artificial intelligence” OR “machine learning” OR “deep learning” OR “neural network” OR “natural language processing” OR “radiomics” OR “convolutional neural network” OR “computer-aided diagnosis”) AND TS = (“gynecologic cancer” OR “gynecologic oncology” OR “ovarian cancer” OR “cervical cancer” OR “endometrial cancer” OR “uterine cancer” OR “vaginal cancer” OR “vulvar cancer”). This initial query returned 2903 records. Applying a publication date filter from 1 January 2005 to 28 March 2025 reduced the dataset to 2849 entries. Further refinement was carried out by restricting document types to articles and reviews (n = 2557) and limiting the language to English, resulting in a final dataset of 2544 publications used for analysis (see Figure 1). Given the focus of this study, only articles published in English were included to avoid potential bias introduced by language barriers.
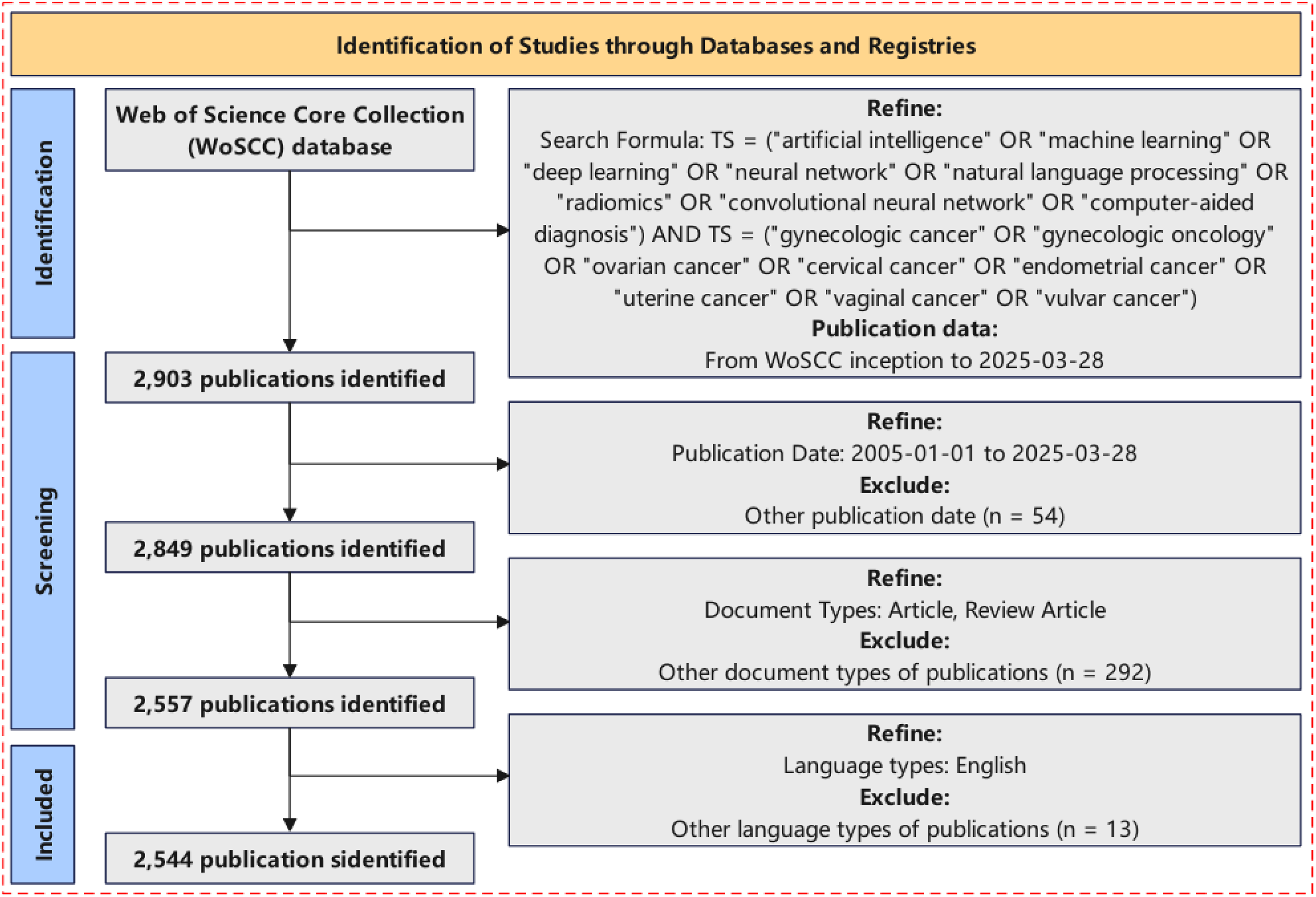
Study selection flowchart. The final dataset comprised 2544 publications sourced from the Web of Science Core Collection database, covering the years 2005 to 2025.
The WoSCC served as the primary bibliometric data source for this study, largely due to its ability to provide comprehensive and trusted data for analyzing trends in AI research in gynecologic oncology. First, WoSCC offered comprehensive coverage of highly cited journals across multiple disciplines, ensuring the retrieval of influential publications and thereby providing a standardized, high-quality dataset for bibliometric analysis. 11 Moreover, the comparison of many alternatives has shown that WoSCC provides more reliable citation links and backward/forward citation coverage than many others. This was illustrated by a recent analysis, which recommended WoSCC over Scopus for its accuracy in backward citation searching. 12 Secondly, WoSCC was recognized for its selectivity and indexing rigor, suggesting that although it indexed fewer journals in total compared to Scopus or other larger databases, the journals it did index typically had higher standards of peer review and citation reliability. 13 This selectivity supported the integrity of bibliometric metrics derived from its data by providing for higher standards of peer review and citation reliability. Additionally, the widespread use of WoSCC in bibliometric studies has established its export formats, metadata schemas, and compatibility with tools like VOSviewer and CiteSpace, facilitating robust tracking of citation networks and research trends. 11 Since our study aimed to map global trends in AI research in gynecologic oncology rather than to include every article, WoSCC was favored for its balance of breadth and depth, ensuring consistent and reproducible results in meaningful literature.
Although other databases such as PubMed, Scopus, and Embase might contain more documents, their inclusion would lead to inconsistencies in indexing criteria, metadata formats, and citation records, complicating data cleaning, deduplication, and analysis. Indeed, several bibliometric studies warned not to make use of multiple databases without extensive deduplication and cross-normalization, which further justified the decision to use WoSCC exclusively.14,15 Therefore, to ensure methodological consistency and analytical feasibility, a single database format applied with WoSCC was chosen for our study.
In summary, WoSCC was appropriate for this study since it combined high journal-quality standards, robust and reproducible citation data, and practical compatibility for large-scale bibliometric mapping, with consistent and operational use and ease, and represented the current development trends of research to be available in AI for gynecologic oncology.
Bibliometric analysis and visualization
All bibliometric analyses were performed using CiteSpace (version 6.3.R1). 16 The analysis parameters were configured with a time span from 2005 to 2025, using one-year intervals, and selecting the top 50% most cited or frequently occurring items in each time slice. Key analyses included annual trends in publication output, collaboration networks among countries and institutions, author coauthorship and co-citation patterns, journal co-citation mapping, reference co-citation and clustering, as well as keyword co-occurrence, burst term detection, and temporal visualizations including timeline and time zone mapping.
For the timeline analysis, clustering was performed using CiteSpace's built-in algorithms to examine the temporal evolution of research themes. Cosine similarity was applied to calculate link strength, and the network was pruned using the minimum spanning tree algorithm to reduce complexity. Cluster labeling employed the log-likelihood ratio method, which identifies representative terms by comparing their within- and between-cluster frequencies. This parametric approach has been widely adopted in bibliometric research due to its ability to generate distinctive and interpretable labels. Cluster quality was assessed using the modularity Q and weighted mean silhouette score. All parameter settings and procedures followed standard bibliometric practices and CiteSpace methodological guidelines to ensure reproducibility.
Results
Literature identification
A total of 2903 publications were initially retrieved from the WoSCC. After applying inclusion criteria—publication years (2005–2025), English language, and article/review type—2544 documents were selected for bibliometric analysis (Figure 1).
Annual publication trends
Figure 2 showed the publication trends over the past two decades. Annual publications remained low until 2019, when a noticeable increase occurred, peaking at 634 publications in 2024. This growth coincided with rapid advances in machine learning and deep learning, suggesting increasing interdisciplinary integration between AI and gynecologic oncology.7,17 The trend indicated continued expansion through 2025.
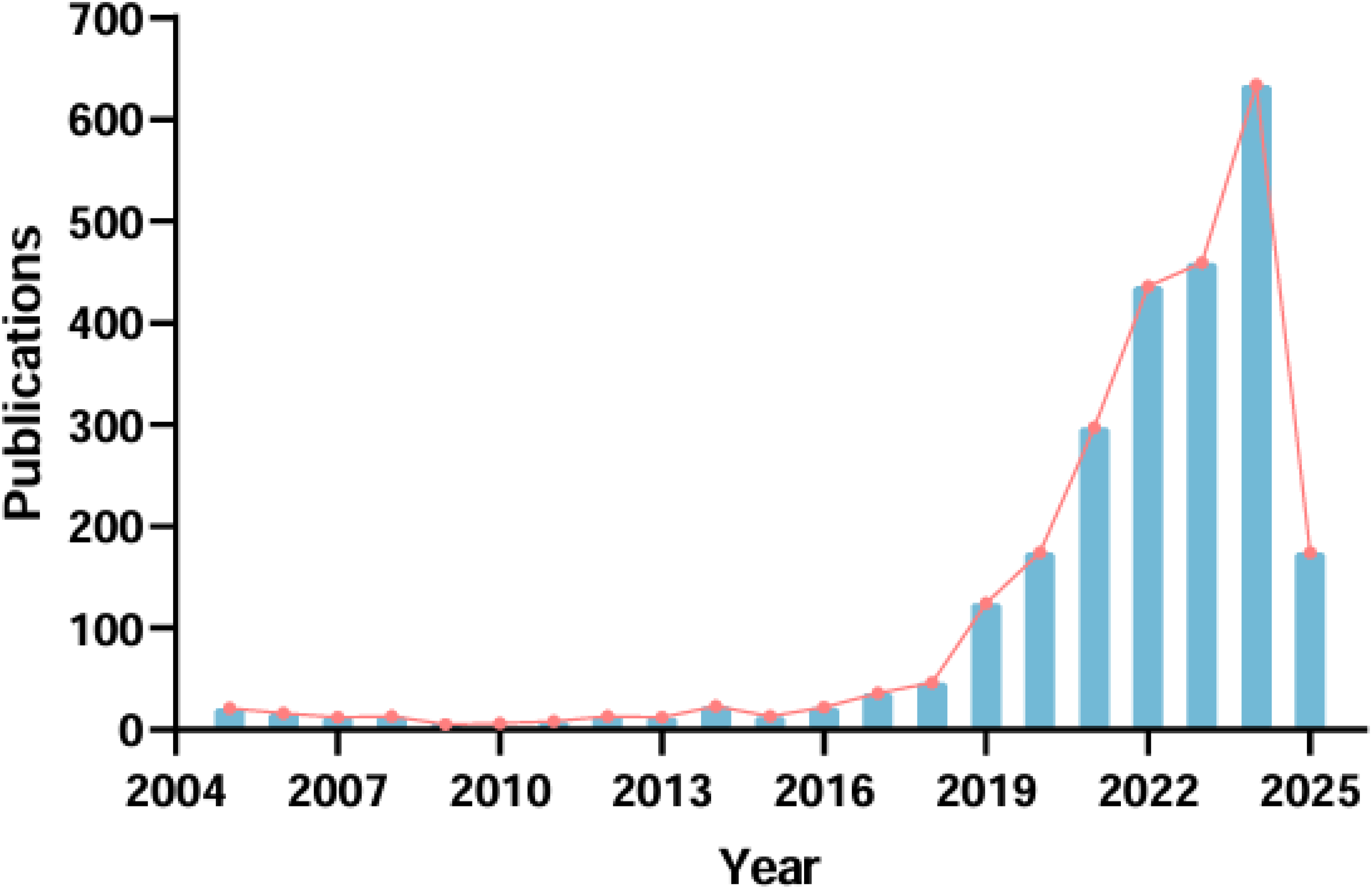
Trends in annual publications on artificial intelligence and gynecologic cancers. The consistent increase in publications highlighted a growing interest, especially in recent years.
Geographical distribution and country/institution contributions
The global landscape of research in this field demonstrated widespread international involvement, as shown in Figure 3A. Researchers from across the globe, especially from China, the United States, and India, have made significant contributions. These countries have established collaborative links with institutions across Europe, Asia, Africa, and the America.

Global and institutional collaboration in artificial intelligence and gynecologic cancers research. (A) A global collaboration map depicting international collaborations, with China, the United States, and India as pivotal contributors. (B) Annual publication trends of the top 10 countries/regions showed significant contributions from China, the United States, and India, with notable growth post-2019. (C) Global co-occurrence network illustrating the international collaboration intensity. (D) Institutional co-occurrence network pinpointing the major contributing organizations.
Annual publication data from the top 10 most productive countries (Figure 3B) indicated that China, the United States, and India have consistently led in output, particularly since 2019. Other notable contributors with rising trends included the United Kingdom, Italy, and South Korea.
Using VOS viewer software, a detailed visualization of international collaboration networks was generated (Figure 3C), encompassing 112 participating countries. The map underscored the central roles of China and the United States in terms of publication volume. India, England, and Italy also emerged as key facilitators of transnational knowledge exchange. Countries with purple rings in the network diagram exhibited centrality scores above 0.1, highlighting their strategic importance within the collaborative framework.
At the institutional level (Figure 3D), several universities and research organizations distinguished themselves through high publication counts and central roles in collaborative networks. Leading institutions included the Chinese Academy of Sciences, Fudan University, China Medical University, Huazhong University of Science and Technology, and Wenzhou Medical University. Particularly in China, the prominence of the Chinese Academy of Sciences and Fudan University reflected substantial national investment in the convergence of AI and gynecologic oncology. A detailed listing of the top 10 most prolific countries and institutions was provided in Table S1.
It should be noted that the “influential authors” and “influential institutions” were identified based on publication output and citation frequency. However, the field size and collaboration intensity should be considered when evaluating these entities. For example, institutions such as the University of California System and the Chinese Academy of Sciences contributed significantly to AI research in gynecologic oncology, which might be explained by these institutions’ larger size and higher collaboration rates.
Author collaboration and influence
Author coauthorship mapping (Figure 4A) revealed several active collaborative clusters. Influential contributors include Sala Evis, Tian Jie, and Scambia Giovanni, who exhibited strong interconnectivity and high centrality, indicative of leadership in multi-institutional studies. Co-citation analysis (Figure 4B) highlighted foundational scholars such as Sung et al., Siegel, Lambin et al., and He et al., whose works provided the conceptual basis for AI applications in gynecologic oncology. Table S2 listed the top-cited and most collaborative authors.

The collaboration and co-citation analysis of authors in artificial intelligence and gynecologic cancers research. (A) Author co-occurrence network highlighting collaborative relationships among researchers in the domain, indicating central figures such as Sala Evis, Tian Jie, and Scambia Giovanni as major influencers with frequent collaborations. (B) Author co-citation network indicating leading figures with high influence, including Sung et al., Siegel, Lambin et al., and He et al.
Journal influence and interdisciplinarity
High-volume journals include Frontiers in Oncology, Scientific Reports, and Cancers. Co-citation analysis (Figure 5) identified Gynecologic Oncology, Radiology, and European Radiology as core knowledge sources. These journals reflected a concentration of scholarly output at the intersection of clinical oncology and imaging science. Table S3 listed the most cited and co-cited journals. A dual-map overlay (Figure S1) confirmed interdisciplinary citation flows from medicine, molecular biology, and clinical science (citing journals) to domains such as genetics, imaging, and materials science (cited journals), underscoring the cross-disciplinary nature of the field.
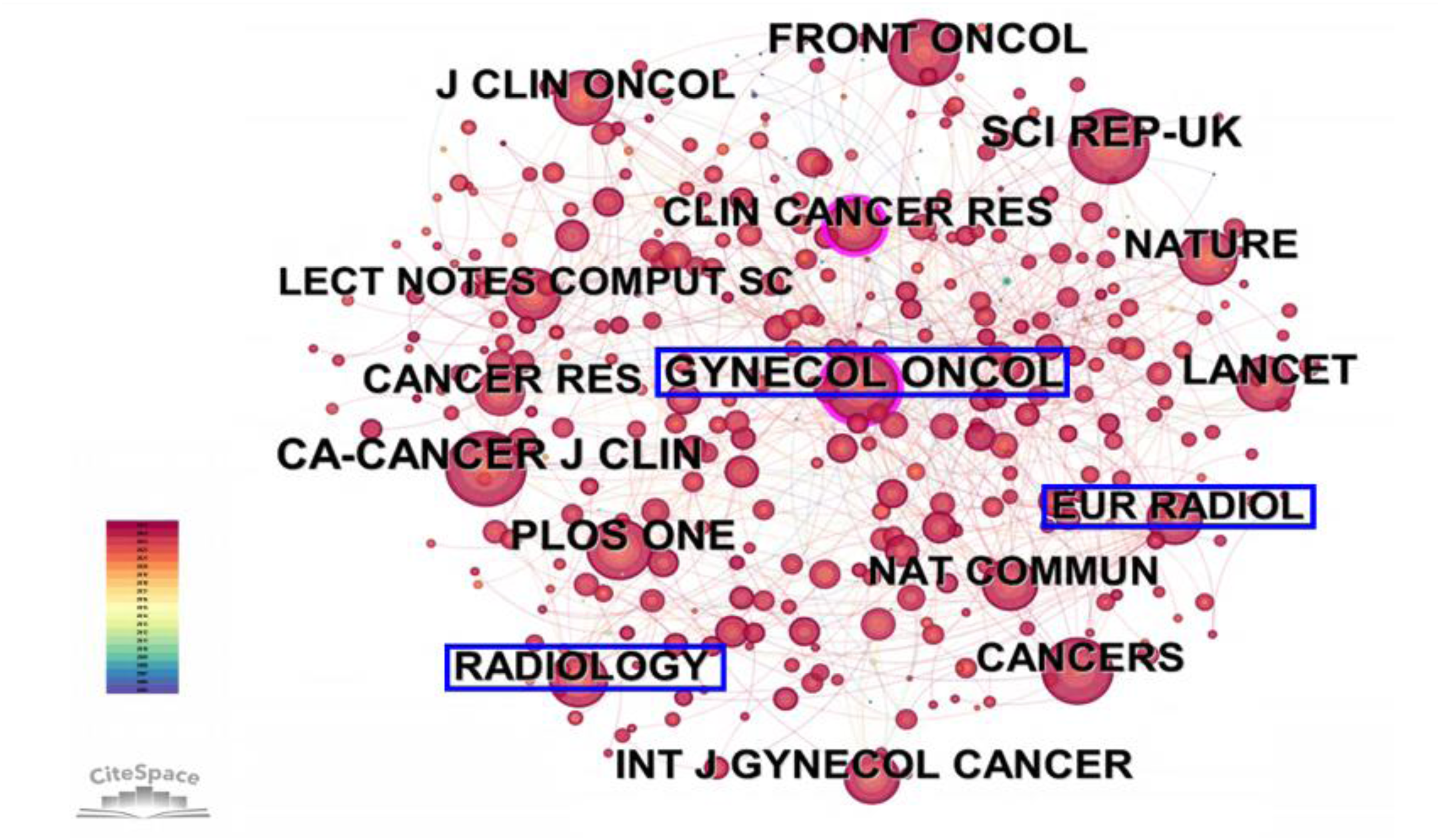
The co-citation network of journals identified frequently cited journals in the field.
Reference co-citation and cluster analysis
To uncover key literature and thematic directions within the field, we performed a reference co-citation analysis. The resulting co-citation network (Figure 6A) highlighted several seminal works that have fundamentally shaped research at the intersection of AI and gynecologic oncology. References by Sung et al., 18 Gillies et al., 19 Arbyn et al., 3 Bray et al., 20 He et al., 21 Ronneberger et al., 22 Lambin et al., 23 and Lambin et al. 24 demonstrated notably high co-citation frequencies and strong centrality measures, reflecting their critical influence on advancing the field. The top 10 most highly co-cited references were presented in Table S4. Among these influential works, three references Sung et al., 18 Bray et al., 20 He et al. 21 mainly addressed epidemiological aspects of tumor incidence and mortality. The remaining highly co-cited studies primarily concentrated on the integration of AI in cancer imaging, with a particular emphasis on cervical cancer. The article by Gillies et al. 19 introduced the concept of radiomics, describing the high-throughput extraction of quantitative imaging features that converted medical images into rich datasets for mining and clinical decision support, especially in oncology. Similarly, two studies authored by Lambin et al.23,24 elaborated on the application of radiomics in personalized medicine, while also emphasizing the current lack of standardized methodologies to ensure the scientific and clinical reliability of radiomics research. In addition, Zhang et al. 25 developed a segmentation-free method for cervical cell classification using deep features from convolutional neural networks (ConvNets). After pretraining on natural images and fine-tuning on cervical cytology datasets, classification was achieved by aggregating patch-level predictions. Experiments on Pap smear and liquid-based cytology datasets showed improved accuracy and specificity over previous methods, demonstrating strong potential for clinical cervical cancer screening.

Reference co-citation analysis and citation burst detection. (A) Co-citation network of references identifying foundational studies with high co-citation frequencies. (B) Clustering analysis of co-cited references. (C) Top 25 references with significant citation bursts, indicating literature that gained rapid attention during specific periods from 2005 to 2025.
The clustering analysis of references (Figure 6B) further depicted the thematic progression within the field. Ten major clusters were identified, among which the most significant thematic groups included #1 endometrial cancer, #2 ovarian cancer, and #3 cervical cancer, reflecting a focus on the predominant types of gynecologic malignancies. Additional important clusters such as #0 radiomics, #4 magnetic resonance imaging, #5 colposcopy, #6 tissue characterization, #7 biomarker discovery, #8 mass spectrometry, and #9 deep learning revealed the major technical and scientific areas where AI was being actively applied in the study and management of gynecologic cancers.
References with strongest citation bursts
A citation burst analysis identified 25 key references with notable citation surges between 2005 and 2025, indicating significant impact on the field (Figure 6C). The study by Gillies et al. (2016, Radiology) 19 showed the strongest burst (30.57), underscoring radiomics’ central role in oncologic imaging and AI. Other influential works included Esteva et al., 6 Zhang et al., 25 and Krizhevsky et al., 26 highlighting the growing influence of deep learning in medical imaging.
Two main periods of heightened attention were noted: an early phase (2005–2007) marked by foundational studies like Petricoin et al., 27 and a sustained phase from 2017 onward, aligning with AI advancements. Recent bursts (2023–2025) in studies by Crosbie et al., 28 Sung et al., 18 and Gao et al. 29 pointed to emerging interest in AI applications in gynecologic oncology and cancer epidemiology.
This trend illustrated a shift from early biomarker research to AI-driven diagnostic models, reflecting the field's evolution toward precision medicine and digital health.
Besides, the mean citation burst strength of AI-related research in gynecologic oncology was approximately 2.4 (Figure 7C), indicating a moderate but sustained growth in scholarly attention. When compared with AI-focused bibliometric analyses in colorectal cancer, 30 the relative intensity in gynecologic oncology appeared slightly lower. This difference suggested that, while AI integration in gynecologic oncology was still emerging, it was following a similar developmental trajectory to that observed in other mature oncologic subfields. The pattern reflected a transition from methodological exploration to translational application, with accelerating interest in radiomics-based prognostic modeling and pathology-driven deep learning.

Keyword co-occurrence and clustering analysis. (A) Network depicting keyword co-occurrence. (B) Visualization of clustered keywords into thematic areas. (C) Top 25 keywords with significant citation bursts, highlighting emerging research trends throughout the study period.
Keyword analysis
To investigate core research themes, a keyword co-occurrence analysis using CiteSpace was conducted. The resulting network (Figure 7A) showed high-frequency terms such as “cervical cancer,” “ovarian cancer,” “machine learning,” “deep learning,” “artificial intelligence,” “classification,” and “prediction,” reflecting a dominant focus on applying AI to major gynecologic cancers.
Keyword clustering (Figure 7B) revealed eight distinct clusters. The largest, Cluster #0, labeled “deep learning,” underscored its centrality in AI-based gynecologic oncology research. Other key clusters included “radiotherapy” (#1), “ovarian cancer” (#2), “machine learning” (#3), and “endometrial cancer” (#4), highlighting AI's growing role in both diagnosis and treatment. Additional clusters, such as “artificial neural network” (#5), “digital pathology” (#6), and “cervical cancer” (#7), pointed to specialized areas where AI is transforming screening and decision-making.
The quality of the clusters was evaluated using modularity Q and the silhouette coefficient. The overall modularity Q score of the network was 0.4736, indicating a high degree of modularity in the clustering solution. Additionally, a silhouette score was calculated for each cluster to assess cluster robustness (Table S5). All clusters had silhouette scores greater than 0.65, which was considered acceptable for cluster reliability. Notably, some clusters demonstrated particularly high silhouette scores, such as Cluster #4 (“Endometrial Cancer”) with a score of 0.869 and Cluster #6 (“Digital Pathology”) with a score of 0.873, indicating the strength and coherence of these thematic areas (Table S5). Besides, sensitivity analysis of time-slicing parameters confirmed the robustness of the clustering results (Table S6). The 1-year method produced eight distinct clusters; however, expanding to 2-year time-slicing parameters revealed eleven clusters. Core thematic areas, including cervical cancer, radiomics, deep learning, and endometrial cancer, were retained, while new areas of exploration emerged, such as biomarkers and cancer antigen 125. The changes were modest: modularity Q improved from 0.4736 to 0.789, and silhouette scores increased from 0.7664 to 1.000, supporting the stability and coherence of the findings (Table S6).
Citation burst analysis (Figure 7C) revealed evolving research trends. Early bursts (2005–2012) focused on “biomarker discovery,” with keywords such as “serum,” “proteomic patterns,” and “identification.” The term “artificial neural network” has been found with an early surge starting in 2006, marking the initial application of AI in diagnostics.
From 2017 onward, the focus shifted to advanced imaging and deep learning, with terms such as “segmentation,” “images,” and “neural networks” gaining prominence. Between 2020 and 2025, emerging bursts included “tumor heterogeneity,” “object detection,” “prognostic factors,” and “mortality,” indicating a growing emphasis on clinical outcomes. Recent terms such as “ensemble learning,” “personalized medicine,” “lymphovascular space invasion,” and “immunotherapy” reflected rising interest in precision oncology and predictive modeling.
In summary, the evolution of keyword trends illustrated a clear shift from early molecular diagnostics to advanced, AI-driven clinical strategies, highlighting the field's growing complexity and translational impact.
Temporal evolution of research themes: timeline and time zone analyses
During the early stage (2005–2015), research focused on foundational AI techniques such as support vector machines, neural networks, and classification, primarily applied to cervical and ovarian cancer for diagnostic modeling and biomarker identification (Figure 8A and B).

Evolution of research hotspots over time. (A) Timeline view of major keyword clusters showing the development and persistence of research topics across different periods. (B) Timezone view of keywords from 2005 to 2025, describing the emergence of key terms.
Between 2015 and 2020, deep learning gained traction, with increased use of convolutional neural networks, segmentation, and feature extraction for advanced image analysis (Figure 8A and B). Radiotherapy became a key focus, particularly in treatment planning and texture analysis. Simultaneously, studies on endometrial cancer expanded, emphasizing MRI-based prediction of lymph node involvement.
From 2020 to 2025, deep learning applications intensified in medical imaging, cancer screening, and digital pathology (Figure 8A and B). The “Digital Pathology” cluster advanced rapidly, leveraging AI for whole-slide image analysis and tumor recognition. Artificial intelligence integration in cervical cancer screening also progressed, particularly in human papillomavirus testing and Pap smear interpretation.
Overall, the timeline revealed a shift from classical machine learning in early diagnostic studies to sophisticated, interdisciplinary deep learning applications across radiology and pathology, supporting comprehensive disease characterization and precision oncology.
Discussion
General data
This bibliometric analysis reviewed the research on application of AI in gynecologic cancers between 2005 and 2025. The number of publications per year grew slowly and never rose above 50 but began to grow significantly since 2019, indicating that this research has ushered in a new era. This growth reflected advancements in deep learning and machine learning technologies, which had significantly improved diagnostic and prognostic capabilities. China published the highest number of publications, followed by the USA, indirectly reflecting both nations’ robust investment in AI research and technological infrastructure. However, the USA collaborated most frequently with other countries (regions). The top three authors were Sala Evis, Tian Jie, and Scambia Giovanni, with the highest number of publications. Gynecologic Oncology, Scientific Reports, and European Radiology were central sources of scholarly knowledge within this interdisciplinary field.
Current research application areas
The introduction of AI has transformed various aspects of modern medicine, particularly in analytical, decision-support, and predictive functions. In gynecologic oncology, AI-based technologies, including machine learning, deep learning, and natural language processing, have been increasingly being incorporated into clinical practice. Artificial intelligence has shown significant potential to improve decision-making processes, especially with regard to early detection and the formulation of treatment plans. For instance, AI-based imaging analysis has demonstrated improved sensitivity in the early detection and diagnosis of cervical and ovarian cancers. Xu et al. conducted a meta-analysis involving 34 studies showing that the AI model had a pooled sensitivity of 88% and a specificity of 85% as well as an overall area under the curve (AUC) of 0.93 for identification of image-based ovarian cancer. 31 Given that cervical, ovarian, endometrial, vaginal, and vulvar cancers continued to contribute substantially to global morbidity and mortality, AI technologies have presented a data-driven opportunity to advance and optimize care for patients with gynecologic cancer diagnoses. 7
Imaging-assisted diagnosis
Medical imaging was a cornerstone in the management of gynecologic cancers, and AI has significantly augmented its utility. Deep learning algorithms have been applied to interpret ultrasound, MRI, and CT images with remarkable accuracy.32,33 These models could automate tumor detection, assess tumor stage, and differentiate between benign and malignant lesions. For example, AI-assisted cervical cancer screening using digitized cytology images has demonstrated superior sensitivity compared to traditional methods.25,34,35 Radiomics, the extraction of quantitative features from medical images, when combined with machine learning classifiers, has shown potential in predicting treatment responses and survival outcomes in ovarian cancer patients.36–38
Pathology and molecular diagnostics
Digital pathology with AI support enabled fast and reproducible histopathological assessments. Deep learning-based models could classify histological subtypes, quantify tumor-infiltrating lymphocytes, and analyze tumor heterogeneity accurately.39,40 At the molecular level, multi-omics data integration—comprising genomic, transcriptomic, and proteomic information—enabled differentiation of gynecologic tumors into molecular subtypes. 41 Artificial intelligence models could predict biomarkers such as BRCA mutations or mismatch repair deficiency and inform targeted therapy selection. 42 Furthermore, computational pathology was increasingly being used to infer molecular alterations directly from histological images without the need for additional assays. 43 Of note, AI-assisted pathology has progressed rapidly in endometrial cancer. Sheakh et al. reported the ECgMLP model, achieving a near-perfect 99.26% accuracy in multiclass histopathological classification—far outperformed the ∼79% in earlier systems. 44 Similarly, the EndoNet framework integrated convolutional and transformer architectures, and achieved F1 scores of 0.91 (internal) and 0.86 (external) in carcinoma grading. 45 These advances demonstrated AI's potential to address interobserver variability and improve the reproducibility of pathology. Molecular applications remained nascent, but the promise of using multiomics data was growing as it was increasingly integrated into diagnostic pathways.
Personalized treatment decision support
Artificial intelligence has shown significant promise for personalized treatment plans by utilizing clinical, pathological, and imaging data. It has been proven that machine learning models trained on this type of data could predict optimal treatment strategies tailored to individual patients, minimizing unnecessary toxicity and maximizing therapeutic benefit. For instance, a 2024 multicenter Chinese cohort study of ovarian cancer, including more than 10,000 patients, developed an ensemble AI model based on routine laboratory tests for ovarian cancer diagnosis, achieving an AUC of 0.95 in internal validation and 0.88 in external validation—outperforming cancer antigen 125. 46 Similarly, predictive models for lymph node metastasis in early-stage cervical cancer could help surgeons to choose between radical surgical intervention and conservative management.47,48 Artificial intelligence algorithms have also been used to predict chemoresistance in ovarian cancer, allowing clinicians to adjust treatment plans earlier in the course of care. 49 These AI-driven tools contributed to more precise, accessible, and cost-effective personalized interventions. Additionally, AI-based decisional support systems were being piloted in the optimization of chemotherapy decision-making and surgical planning, although widespread clinical adoption remains limited due to the lack of prospective validation.
Prognosis assessment and recurrence prediction
The accurate prediction of disease recurrence and survival outcomes was essential for the effective management of patients. Artificial intelligence-based prognostic models, using features derived from imaging, pathology, and clinical data, have been developed to classify patients based on their risk for recurrence and survival.50,51 Based on this, time-series approaches incorporating sequential follow-up data provided dynamic risk estimates over the disease course. In gynecologic oncology, such dynamic systems could be utilized in order to personalize surveillance strategies over time and to guide decisions on adjuvant treatment and monitoring frequencies. A 2023 systematic review evaluated 45 studies and 80 AI models for ovarian cancer prognosis, which included recurrence and chemotherapy response. 52 It also reported a promising performance, however, there was an overall risk of bias and limited external validation. 52 Similar gaps existed in studies on cervical and endometrial cancer prognosis, underscoring the need for robust and prospective multicenter trials. Nevertheless, the early findings indicated that AI had the potential to improve risk stratification and guide long-term follow-up strategies.
Clinical trial design and patient recruitment
Natural Language Processing technologies were increasingly applied to facilitate clinical research. By extracting structured data from unstructured clinical notes, AI systems could automatically identify patients who meet complex eligibility criteria for clinical trials, greatly accelerating recruitment processes.53,54 Moreover, AI could optimize clinical trial design by identifying patient subgroups most likely to benefit from investigational therapies, thus enhancing trial efficiency and success rates. 55
Factors driving research trends
The rapid growth of AI research in gynecologic oncology might be attributed to several factors, among which the availability of extensive high-quality datasets, particularly in medical imaging and genomics, played a critical role. 56 Additionally, advances in computational power and the development of sophisticated deep learning algorithms facilitated the analysis and interpretation of large and complex medical datasets. 56 For instance, Kawakami et al. reported that a random forest algorithm achieved 92.4% accuracy (AUC with Random Forest = 0.968) in distinguishing epithelial ovarian cancer from benign tumors by analyzing 32 peripheral blood biomarkers. 57 As the field of precision medicine progressed, AI's ability to tailor treatments to individual patients was becoming increasingly important. Despite these advancements, AI tools had yet to achieve widespread implementation in clinical practice, largely due to the “black-box” nature of many models, which limits their interpretability. 58 Furthermore, challenges such as regulatory approval processes, safeguarding patient privacy, and the need for large-scale validation studies exacerbated the difficulties associated with adopting AI-driven solutions. 8 Although these challenges reflected broader issues in AI implementation, they underscored specific barriers in gynecologic oncology that hindered the seamless integration of AI into practice. Addressing these obstacles required the development of AI models that provided transparent and interpretable reasoning, in addition to leveraging technological capability. 59
Quality assessment of cited literature
This bibliometric analysis revealed both the opportunities and limitations associated with the application of AI in gynecologic oncology. The cited studies provided a multilayered foundation3,18–24: large-scale epidemiological investigations delivered robust population-level evidence yet remained primarily descriptive; seminal radiomics studies emphasized methodological rigor but highlighted the pressing need for prospective validation; and algorithmic innovations such as ResNet, U-Net, and DeepPap demonstrated high technical accuracy but were constrained by retrospective designs, single-center datasets, and limited external validation. Collectively, these studies highlighted the transformative potential of AI while underscoring the persistent absence of multicenter, prospective validation and standardized datasets. To achieve clinical application, future research needed to prioritize rigorous validation frameworks, multimodal data integration, and international collaboration to ensure that AI-driven tools achieved both methodological robustness and equitable clinical applicability in gynecologic oncology.
Future directions and challenges
Artificial intelligence was finding a steadily expanding role in gynecologic oncology, and several areas appear particularly promising at this stage. Among these, multimodal AI models, federated learning, explainable AI, and the newer field of generative AI were attracting growing attention. Multimodal models brought together information from imaging, histopathology, genomics, and routine clinical data. By linking these pieces, the models could capture a more realistic picture of tumor biology and patient behavior, which in turn improved diagnostic and prognostic accuracy. 36 Federated learning made it possible for hospitals to build joint models without actually sharing their data, a design that widened the diversity of training sets while keeping privacy intact.60,61 Explainable AI, though technically demanding, tried to make the system's reasoning visible—something clinicians often needed in order to trust its outputs. 62 Generative AI has only recently entered this field, yet early work suggested that it might be used to create simulated patient datasets or design individualized treatment plans, ideas that could change how clinical trials are organized.63,64
Our bibliometric analysis also showed that radiomics and digital pathology were gaining momentum within gynecologic oncology. These tools were now being used to turn images and tissue slides into measurable data. Maiorano and colleagues, for instance, showed that radiomics-based AI models can predict treatment response in ovarian cancer, pointing to the clinical promise of data-driven phenotyping. 65
Nevertheless, the field still faced several persistent problems. Data from different centers often varied in quality and structure, and the total number of available cases remained small, especially for rare cancers. 7 Without large, standardized, and multi-institutional datasets, reproducibility and external validation were difficult to achieve. 7 Compared with other cancer domains, gynecologic oncology still lacked comprehensive collections that combine imaging, clinical, and genomic data.52,66,67 The biological variation across ovarian, endometrial, and cervical cancers added another layer of complexity, making model transfer and validation harder.66,67 In addition, ethical and legal frameworks had not kept pace with technical progress. Many AI systems still functioned as “black boxes,” leaving unclear who was accountable for errors. Concerns about bias, patient privacy, and informed consent remained unresolved.68–70 These issues were particularly relevant in low-resource regions, where AI might otherwise help reduce inequality in access to care. 8
Future progress will depend on a few practical steps: building large, curated datasets that are shared responsibly; developing AI systems that clinicians can interpret and verify; and testing them through prospective, real-world studies. It will also be essential to establish international guidelines and ethical standards so that the adoption of AI in gynecologic oncology proceeds in a safe and transparent way.71–73
Limitations
This study has several limitations. First, the search strategy was restricted to publications available up to 28 March 2025, which might have excluded more recent research. And default CiteSpace settings were used for cluster resolution and cosine similarity thresholds; additional sensitivity analyses—such as systematically varying these parameters—were not performed due to limited time and research resources. Also, the inclusion of data up to March 2025 might have introduced potential biases related to partial-year publication trends. While this approach allowed us to capture the most up-to-date patterns, we acknowledged that no sensitivity analysis was performed to evaluate the effect of excluding partial-year data, which might limit the robustness of conclusions regarding recent surges. Besides, regression analyses to statistically evaluate keyword growth trends (e.g., “personalized medicine” vs. “radiotherapy”) were not performed because most keywords did not meet the minimum frequency threshold for robust modeling. This limitation reflected the temporal sparsity of certain terms and highlighted a future direction for methodological refinement. Moreover, although the selected keywords reflected dominant themes, the omission of more granular or emerging terminology might have reduced retrieval sensitivity. Future work will incorporate controlled vocabularies and a broader set of domain-specific terms to improve precision and coverage as indexing practices evolve.
Second, the analysis included only English-language publications, which might miss significant studies from non-English-speaking regions (e.g., East Asia and Latin America), where AI research in gynecologic oncology was progressing but often remained underrepresented in the global literature. This language restriction could bias the results toward English-speaking countries, notably major contributors to AI-related research such as the United States and England. Although many Chinese publications were available in English, studies published exclusively in Chinese were not included due to our limited database resources and fundings.
Additionally, this study relied on a single database, the WoSCC, thereby excluding literature from other databases, such as PubMed, Scopus, and Embase. This choice might have resulted in the omission of relevant studies. Consequently, the representation of global AI-related research in gynecologic oncology might have unintentionally bias.
Moreover, bibliometric analyses carried inherent limitations, including citation lag, keyword ambiguity, and delayed in database indexing. Furthermore, citation analysis tools such as CiteSpace and VOSviewer were sensitive to parameter settings, which could result in differing outcomes. Issues such as author name ambiguity and coauthorship difficulties also introduced methodological challenges. Besides, although country-level centrality analysis was performed, we did not extend the analysis to the institutional level using advanced social network analysis metrics (e.g., betweenness centrality). Institutional-level analysis would have allowed us to pinpoint key bridging institutions that facilitate cross-border knowledge transfer, offering a more granular understanding of global research dynamics. This remained an important direction for future research. Additionally, the identification of leading authors and institutions was not normalized by field size or collaboration intensity, potentially biasing influence estimations. Citation counts and total link strength were reported in Tables S1 to S4.
Furthermore, our study relied on CiteSpace for visualization, which has not yet supported subject-level filtering or quantitative examination of interdisciplinary citation patterns. Consequently, the proportion and impact of cross-disciplinary research (e.g., AI combined with radiology vs. AI combined with genomics) could not be systematically quantified in this analysis. To address this limitation, future studies should incorporate external subject classification systems or apply manual classification approaches to systematically evaluate interdisciplinary trends and their citation impacts.
Future research should address these methodological limitations and expand the scope of inquiry to improve the accuracy and comprehensiveness of bibliometric analyses in gynecologic oncology.
Conclusion
In the field of AI-related research in gynecologic oncology, China and the United States have emerged as leading contributors, producing a substantial volume of high-quality, influential work. Artificial intelligence has the potential to transform gynecologic oncology by facilitating early diagnosis, enabling personalized treatment planning, and improving patient outcomes. However, the successful integration of AI into clinical practice remains contingent upon overcoming several critical challenges, including regulatory approval, data security, and the establishment of AI models reliability through rigorous validation studies. Future research should focus on addressing these barriers while enhancing model performance and narrowing the gap between research innovation and clinical application. In particular, the incorporation of multimodal data, the development of prospective datasets, and an emphasis on model transparency and interpretability represent essential directions for advancing the clinical utility of AI in gynecologic oncology.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076261416708 - Supplemental material for Application of artificial intelligence in gynecologic cancers: A bibliometric analysis
Supplemental material, sj-docx-1-dhj-10.1177_20552076261416708 for Application of artificial intelligence in gynecologic cancers: A bibliometric analysis by Nan Liu, Feng Jiang, Yaochen Lou and Jun Guan in DIGITAL HEALTH
Supplemental Material
sj-docx-2-dhj-10.1177_20552076261416708 - Supplemental material for Application of artificial intelligence in gynecologic cancers: A bibliometric analysis
Supplemental material, sj-docx-2-dhj-10.1177_20552076261416708 for Application of artificial intelligence in gynecologic cancers: A bibliometric analysis by Nan Liu, Feng Jiang, Yaochen Lou and Jun Guan in DIGITAL HEALTH
Supplemental Material
sj-docx-3-dhj-10.1177_20552076261416708 - Supplemental material for Application of artificial intelligence in gynecologic cancers: A bibliometric analysis
Supplemental material, sj-docx-3-dhj-10.1177_20552076261416708 for Application of artificial intelligence in gynecologic cancers: A bibliometric analysis by Nan Liu, Feng Jiang, Yaochen Lou and Jun Guan in DIGITAL HEALTH
Supplemental Material
sj-docx-4-dhj-10.1177_20552076261416708 - Supplemental material for Application of artificial intelligence in gynecologic cancers: A bibliometric analysis
Supplemental material, sj-docx-4-dhj-10.1177_20552076261416708 for Application of artificial intelligence in gynecologic cancers: A bibliometric analysis by Nan Liu, Feng Jiang, Yaochen Lou and Jun Guan in DIGITAL HEALTH
Supplemental Material
sj-docx-5-dhj-10.1177_20552076261416708 - Supplemental material for Application of artificial intelligence in gynecologic cancers: A bibliometric analysis
Supplemental material, sj-docx-5-dhj-10.1177_20552076261416708 for Application of artificial intelligence in gynecologic cancers: A bibliometric analysis by Nan Liu, Feng Jiang, Yaochen Lou and Jun Guan in DIGITAL HEALTH
Supplemental Material
sj-docx-6-dhj-10.1177_20552076261416708 - Supplemental material for Application of artificial intelligence in gynecologic cancers: A bibliometric analysis
Supplemental material, sj-docx-6-dhj-10.1177_20552076261416708 for Application of artificial intelligence in gynecologic cancers: A bibliometric analysis by Nan Liu, Feng Jiang, Yaochen Lou and Jun Guan in DIGITAL HEALTH
Supplemental Material
sj-docx-7-dhj-10.1177_20552076261416708 - Supplemental material for Application of artificial intelligence in gynecologic cancers: A bibliometric analysis
Supplemental material, sj-docx-7-dhj-10.1177_20552076261416708 for Application of artificial intelligence in gynecologic cancers: A bibliometric analysis by Nan Liu, Feng Jiang, Yaochen Lou and Jun Guan in DIGITAL HEALTH
Footnotes
Acknowledgements
During the preparation of this work the authors applied a GPT-4.0 model in order to improve the readability and polish language in the manuscript. After that, the authors reviewed and edited the content as needed and took full responsibility for the content of the published article.
Contributorship
NL: manuscript writing and revising. FJ: data curation, methodology, and visualization. YL: literature investigation, methodology, and manuscript revising. JG: Conceptualization, methodology, formal analysis, manuscript revising, funding acquisition, and supervision. All authors agreed to the published version of the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by NSFC82171633 and the Natural Science Cultivation Program of Obstetrics & Gynecology Hospital of Fudan University, Shanghai, China (grant number No. GZRPY202315).
Declaration of conflicting interests
The authors declared that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.