
Abstract
Background
Cervical cancer remains a leading cause of cancer morbidity and mortality among women worldwide, with an estimated 661,021 new cases and 348,189 deaths in 2022. In China's health-resource-limited areas, a substantial share of the population remains hard to reach, and the effectiveness of data-driven identification and digital outreach for this hard-to-reach population is uncertain.
Objective
This study aims to (a) use ID-card-based record linkage to identify women who have never undergone cervical cancer screening and (b) evaluate whether the integrated digital intervention reduces redundant repeat screening while improving women's knowledge, attitudes and practices (KAP) in health-resource-limited areas.
Methods
We will conduct a quasi-experimental controlled trial including an external historical control cohort and two individually randomised digital intervention arms in 11 sites. Women will be identified by matching unique ID-card numbers across the national screening registry and local household records. Newly screened eligible women will be randomly allocated to one of two intervention arms: (a) tailored digital interventions and (b) generic digital interventions, while an external historical cohort (January 2022–December 2023) from the same sites, before implementation of the digital platform, will serve as the control arm.
Results
Recruitment began on 15 April 2025. The trial plans to recruit 142,417 participants (122,817 in the historical control cohort and 9800 in each intervention arm). Baseline surveys commenced on 15 April 2025 and will continue until December 2026.
Conclusions
If effective, this study will be among the first to evaluate a full-process digital health intervention that combines algorithm-based identification with a web-plus-WeChat platform for cervical-cancer screening in resource-limited areas of China. The findings could inform programme development and benefit hard-to-reach populations.
Keywords
Introduction
Cervical cancer remains a major public health challenge worldwide. It is one of the most common cancers among women and a leading cause of cancer-related death, particularly in low-and medium-Human Development Index (HDI) countries.1,2 In China alone, the National Cancer Registry reported 150,700 new cases and 55,700 deaths in 2022, 3 accounting for 22.8% and 16.0% of the world, respectively. Since 2009, the Chinese government has funded population-based screening for women aged 35–64 years across 30 provinces (cities).4,5 However, over the past 20 years, both the incidence and mortality of cervical cancer in China have continued to increase and tend to be younger, with persistent gaps in both under-screening and over-screening.6,7 Low awareness of HPV and cervical cancer and delays in care can worsen disease progression or lead to overtreatment, increasing the economic burden. 8
Outcomes and statistical analysis.

*Primary outcome.
The proportion of women reading examination results, health education materials and professional screening recommendations among those who are screened and have received digital health interventions.
From the latest report updated to colposcopy.
From the latest report updated to therapy.
Internationally, culturally tailored educational videos for Hispanic and Moroccan-Dutch women, web-based decision aids, and interactive tools have been used to address informational and psychosocial barriers to screening.9,10 Interventions that combine home-based HPV self-sampling kits with educational materials, 11 as well as Short Messaging Service (SMS) reminders for HPV-positive women, 12 aim not only to promote screening uptake but also to enhance knowledge, informed decision-making, sample-return rates and adherence to recommended follow-up. Studies in China are also actively carrying out health education on the prevention and treatment of cervical cancer. Information is disseminated through various channels, including community outreach, media reports and health lectures in health care institutions. These initiatives help improve women's self-care awareness and participation in screening.13–17
However, few studies have systematically leveraged China's unique ID-card-based health-information infrastructure to identify never-screened women, quantify redundant repeat screening and deliver personalised digital interventions. In this protocol, we define ‘hard-to-reach women’ as those who remain unscreened or inconsistently screened despite eligibility, often living in health-resource-limited counties or facing socioeconomic, geographic or informational barriers to care. We use the term ‘digital population-management platform’ to refer to an integrated, ID-card-linked system that connects population registers, screening test results, risk stratification, digital notification of results and follow-up management tools for both women and providers. By embedding targeted, WeChat-based digital health interventions within this platform, our study aims to address under-screening, reduce redundant repeat screening and support guideline-consistent follow-up for hard-to-reach women in China's health-resource-limited areas.
Method
Study design
We will conduct a pragmatic, quasi-experimental controlled trial in 11 sites of China's health-resource-limited areas (April 2025–December 2026), including an external historical cohort without exposure to digital health interventions and a contemporaneous two-arm individual randomised digital intervention component. A concurrent non-digital control arm was not feasible because the digital platform is being implemented as part of routine services in the participating counties and local health authorities considered it unacceptable to withhold the platform once introduced; to mitigate potential temporal biases, we restrict the historical control period to the two years immediately preceding implementation, apply identical eligibility criteria and data sources across periods, and will adjust for site, calendar time and key baseline characteristics in the analyses. If women are identified as eligible according to the ID-card record linkage, they will be randomised in a 1:1 ratio within each site to Arm1 (tailored digital health interventions for women with screening and digital health interventions for screening doctors) or Arm 2 (generic digital health interventions for women with screening and digital health interventions for screening doctors), both delivered on top of the traditional notification method. An external historical cohort from the same sites (January 2022–December 2023), which had no exposure to digital interventions, will serve as the control arm.
Digital health interventions will be based on personal computer (PC) webpage of a digital platform and WeChat, an all-in-one app that combines instant messaging (text and voice/video calls), WeChat Pay (which allows users to link bank accounts for safe and convenient payments), and service notifications (which provide real-time notifications), with more than 1.38 billion monthly active users. 18 And WeChat has been demonstrated to be an effective and more cost-efficient technological tool for chronic disease management. 19 As for mini programs, they are like small, lightweight apps that can be used in WeChat without downloading. 20 And data of the PC webpage and Wechat mini program is interconnected through the digital platform.
Study objectives
Our objectives are to evaluate whether integrated digital interventions reduce over-screening, improve colposcopy completion and guideline-concordant treatment, and enhance KAP among participants. Specifically, we hypothesise that:
Compared with routine care (paper-based archival and telephone notification), integrated digital interventions will significantly reduce over-screening rates, improve completion of colposcopy and receipt of guideline-concordant treatment, shorten referral-to-treatment intervals, and improve participants’ KAP scores; Tailored digital messages, compared with generic messages, will be more effective in improving KAP, shortening follow-up intervals, and increasing colposcopy completion and adherence to treatment guidelines; Digital interventions targeting screening providers will offer additional benefits beyond patient-only interventions, particularly in enhancing timeliness of follow-up and appropriate management of abnormal results.
Sites
The study will be conducted in 11 county-level sites across Shanxi, Sichuan, Yunnan and Gansu Provinces (e.g., Zezhou, Wuxiang, Xiangyuan, Mangshi, Heqing, Xinping Yi and Dai Autonomous County, Yanting, Songpan, Shimian, Jingtai and Yangcheng; see Figure 1).

Distribution map of the 11 study sites.
Map showing the 11 county-level sites across four provinces in China (Shanxi, Sichuan, Yunnan, Gansu): Zezhou, Wuxiang, Xiangyuan, Yangcheng, Yanting, Songpan, Shimian, Jingtai, Mangshi, Heqing, and Xinping Yi and Dai Autonomous County. Red markers indicate participating counties.
Randomization
Eligible women in each site were randomly allocated at the individual level by the digital platform's built-in algorithm. Randomisation will be stratified by site and screening strategy to ensure balance, and will use a concealed, computer-generated 1:1 sequence assigning participants to Arm 1 and Arm 2 (Figure 2). Allocation is concealed within the platform until after enrolment; blinding of participants (women) and providers (screening doctors) is not feasible due to the nature of the interventions; data analysts are blinded to allocation using de-identified group codes. Only certain researchers with permission were able to obtain data of what specific intervention type women received through ID numbers.

Study flow diagram of the digitally-enabled trial.
Overview of the controlled trial with an external historical cohort and two individually randomised intervention arms. Steps include ID-card-linked e-registration, questionnaire, specimen collection, digital result notification, randomisation to tailored vs generic messages for screen-positive/negative women, referral for colposcopy, and follow-up or treatment; knowledge/attitudes/practices (KAP) surveys are administered in predefined subsamples.
Participants
This study is based on National Cervical Cancer Screening Program in China, which provided the sampling frame and registry data for ID-card linkage.
In the National Cervical Cancer Screening Programme (NCCSP) registry, the investigators (village doctors or nurses) who had undergone unified standardized training conducted face-to-face interviews, and used the method of double entry and double checking to enter the data. After the on-site investigation, they checked whether the information was standardized and logical. After confirming that it was correct, the woman was told to leave. Additionally, among women who are identified as eligible through the NCCSP but do not enrol in the digital services, we will document their characteristics. De-identified information such as age, county of residence, ethnicity and previous screening history will be extracted from the routine registry. Investigators will also record the primary reason for non-participation (e.g., no smartphone access, not using WeChat or other digital tools, or a preference for non-digital contact) using a brief standardised form. These data will allow us to quantify potential selection bias introduced by the digital intervention. And doctors of higher-level units in the 11 sites regularly extracted data related to screening and intervention for review and quality control.
Interventions
Control arm (routine care)
The control arm adopted the traditional notification method. All women received HPV DNA testing, and women with negative results of the primary screening were not notified, while women were reminded to complete colposcopy one by one by the hospital staff on the phone if (a) women were positive for HPV-16 / 18 and (b) women were positive for any other high-risk types, and their cytology or visual inspection with acetic acid/Lugol's iodine (VIA/VILI) findings showed abnormal. And women who were diagnosed as cervical intraepithelial neoplasia grade 2 or worse and cervical cancer (CIN2+) were also called in the same way.
Intervention arms
Eligible women will enrol by scanning a QR code, providing electronic consent and completing real-name authentication to link their 18-digit ID to the mini-program. When laboratory result reports are updated, the WeChat mini-program automatically notifies the women through WeChat service notifications, from which women can view their reports, learn the meaning of the examination results, and take professional recommendations (Figure 3). For women whose screening results are negative, the digital messages will focus on explaining that no immediate further tests are needed, providing general cervical cancer and women's health education, and reinforcing the guideline-recommended interval for their next screen, in order to discourage redundant repeat screening while maintaining engagement with the program. During the intervention period, newly screened eligible women will be individually randomised in a 1:1 ratio to the tailored or generic digital intervention arm using a computer-generated allocation sequence embedded in the digital platform (see Figure 2 for the study flow diagram). Randomisation will be stratified by site and screening strategy, with allocation concealed within the platform until after enrolment. Blinding of participants and providers to allocation is not feasible due to the nature of the interventions, but data analysts will work with de-identified allocation codes. In Arm 1, women received tailored intervention materials matched to their screening results, whereas participants in Arm 2 received a uniform generic intervention delivered via the WeChat mini-program. Digital-service acceptance (i.e., the click-through time, click-through rate and reading time among women with screening) was continuously logged by the mini program, and for women who are referred but have not completed colposcopy within 2 weeks of the initial digital notification of an abnormal screening result, the system will automatically trigger supplementary text messages and follow-up phone calls by local healthcare workers. Upon availability of colposcopy and pathology reports, the system pushed a second result-linked notification, following the same Tailored or Generic logic.
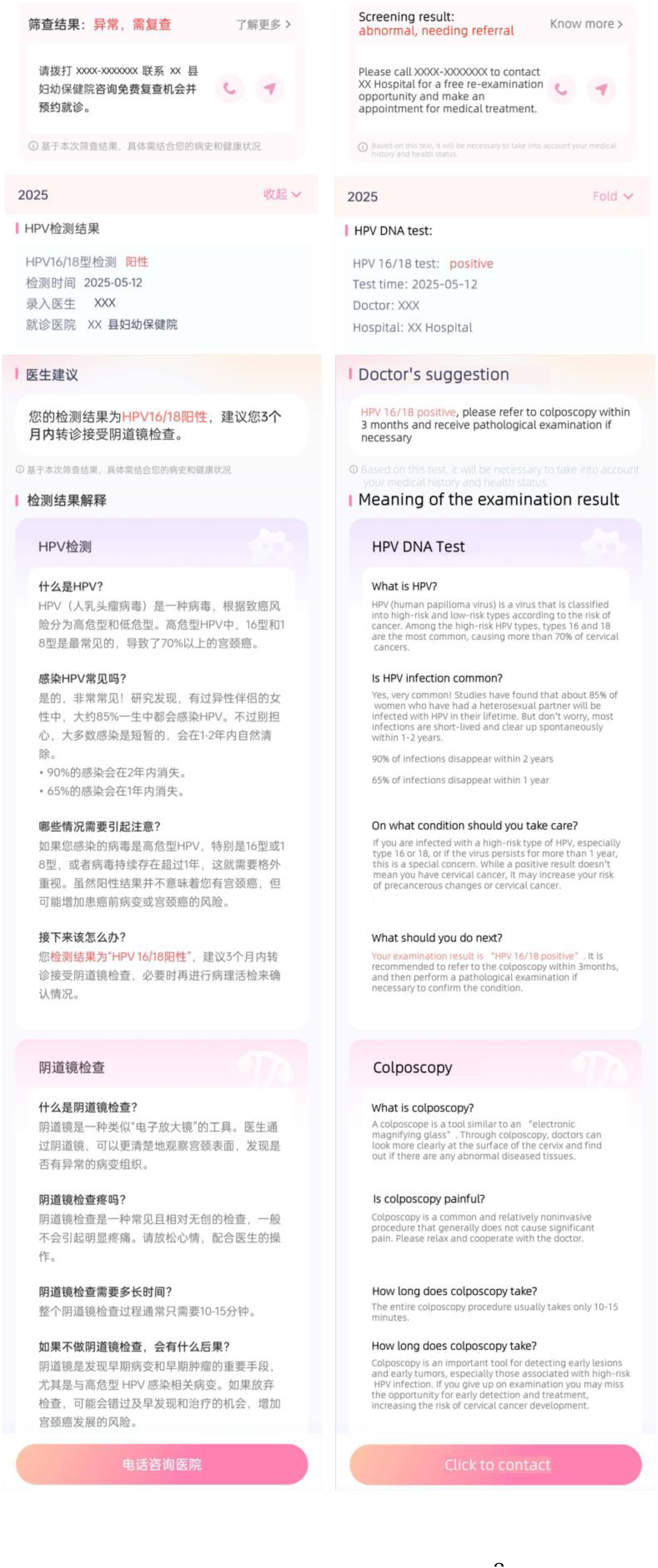
Patient-facing digital messages (WeChat mini-program). Examples of result-linked notifications and plain-language education shown to women (Chinese and English versions): HPV DNA test results, doctor's suggestions, explanations of human papillomavirus (HPV) and colposcopy, and a ‘click to contact’ option for referral support.
As for doctors, the provider dashboard (PC webpage + mini program) displayed a real-time list of women pending colposcopy, sorted by days remaining within the 90-day guideline window, and generated automated reminders. Doctors could record contact attempts and schedule follow-up directly in the system (Figures 4 and 5).

Provider dashboard on the PC webpage.

Provider dashboard in the WeChat mini-program.
Provider-facing interface displaying de-identified lists of women pending colposcopy, latest follow-up type, and a countdown to the 90-day guideline window, with buttons to review records and log contacts. Designed to support timely referral management and documentation.
Mobile interface for screening doctors showing the same follow-up list, status labels, next follow-up date and one-click outbound call, enabling real-time tracking and action during routine work. Chinese and English versions are shown.
Sample size calculation
Referral interval (time from result notification to colposcopy) was selected as the behavioural outcome for sample-size estimation. The previous study had shown that the referral interval for colposcopy was approximately 49 days (median) for patients not reminded and was shortened to about 15.5 days (median) for those who were reminded. 21 PASS 15 was used for the sample size calculation, assuming a statistical power of 80% (α = 0.05, bilateral), taking into account 10% (due to visits to other hospitals, etc.) not available data and 10% loss to follow-up rate. Such calculation indicated a required target sample size of 392 women who need to be referred for colposcopy in each intervention arm. Based on historical statistics in the control arm, about 4% of women with screening required colposcopy. Thus, 9800 women with screening should be included in each intervention arm, and a total of 19,600 women with screening should be included in two intervention arms.
We chose KAP score as a cognitive outcome for sample size calculation
The previous study had shown that an awareness score of approximately 8.2 (SD = 1.0) in the intervention group and 7.6 (SD = 1.2) in the control group. 10 According to PASS 15, assuming a statistical power of 90% (α = 0.05, bilateral), 88 women should be screened, taking into account the 20% loss to follow-up rate. A total of at least 176 screened women should be randomly selected from the tailored digital health intervention arm and generic digital health intervention arm to conduct questionnaires related to awareness and attitude.
Outcomes and statistical methods
Acceptance and use of the platform were among the primary outcomes
The click-through of the PC webpage or WeChat mini program of the digital platform can be recorded through the data platform connected with it. The use of the digital platform's PC webpage or WeChat mini program can be measured by a usability scale (Appendix) which was developed with reference to System Usability Scale (SUS), 22 and recorded on an online questionnaire platform called SoJump. For women with screening, trained healthcare workers will administer the usability scale by telephone and enter the responses directly into SoJump, whereas screening doctors will self-complete the corresponding usability questionnaire online via SoJump. And interviews can be conducted with various field staff in accordance with the Consolidated Framework for Implementation Research (CFIR 2022) to gather feedback on the strengths and weaknesses of digital health interventions. 23 For this trial, the primary process outcomes are defined operationally as follows (Table 1). Digital-service acceptance is defined as at least one click on the WeChat mini-program result page or any linked educational message during the follow-up period, with the number and timing of clicks recorded by the platform. Colposcopy completion is defined as completion of a recommended colposcopy examination within 90 days of the referral date among all women who receive a colposcopy recommendation. Guideline-consistent treatment is defined as receipt of treatment that is consistent with national or WHO recommendations given the woman's worst histopathology result and age group. A key secondary outcome is redundant repeat screening, defined as any screening test repeated within three years of a negative cytology result or within five years of a negative HPV result, in accordance with guideline-recommended screening intervals. KAP outcomes include knowledge and attitude scores derived from the structured questionnaire in the Appendix, which will be calculated as continuous scale scores and, where appropriate, categorised for descriptive purposes.
Knowledge, attitude and practice (KAP) scores were also a primary outcome
Baseline and follow-up demographic data, test dates, and inspection results can be recorded through the PC webpage or WeChat mini program of the digital platform. KAP scores related to knowledge and attitude will be assessed using the structured questionnaire in the Appendix, which was developed based on the study of Jo Waller and Daisy Le.10,24 At the time of screening registration, before test results or digital health education are delivered, trained healthcare workers will administer the baseline KAP questionnaire face to face and record the responses in the structured form. After test results have been pushed through the digital platform and women have had the opportunity to view the educational materials, the same KAP questionnaire will be administered by telephone by healthcare workers, who will enter the responses directly into the SoJump electronic questionnaire system. For binary outcomes such as digital-service acceptance, colposcopy completion and guideline-consistent treatment, we will use modified Poisson regression with robust standard errors to estimate risk ratios and 95% confidence intervals, adjusting for site and key baseline covariates (for example, age and baseline screening history). For time-to-event outcomes such as referral interval and time to treatment, we will construct Kaplan–Meier curves and use Cox proportional hazards models to estimate hazard ratios. Each digital intervention arm will be compared with the historical control cohort, and the two intervention arms will be compared with each other. Models will account for clustering by site where appropriate. We will explore the impact of potential confounders and conduct sensitivity analyses, including alternative model specifications and approaches to handling missing data (e.g., complete-case analysis and, where feasible, multiple imputation).
Baseline characteristics will be summarized as mean ± SD (or median, IQR) for continuous variables and number (percentage) for categorical variables. Balance across the two intervention arms will be assessed with chi-square tests for categorical variables and t-tests for continuous variables.
We will perform missing value identification on the dataset, using statistical methods to determine the missing status of each variable. For variables with a high proportion of missing, we will assess their impact on the study results and decide whether to include them in subsequent analyses.
Categorical outcomes, including redundant repeat screening, digital-service acceptance, click-through action, completion of colposcopy and guideline-concordant treatment, will be analysed using the pre-specified modified Poisson regression with robust standard errors to estimate risk ratios (RR) and 95% confidence intervals (CI). Time-to-event outcomes (referral interval and time-to-treatment) will be compared with Kaplan-Meier curves and log-rank tests. Cox proportional-hazards models will then estimate hazard ratios (HR), with Schoenfeld residuals used to verify the proportional-hazards assumption. Continuous outcomes, including message-reading time and scores will be analyzed with t-test / Welch's t-test.
All analyses will be performed in R (v 4.3). Results will be considered statistically significant at P < 0.05.
Ethics and registration
The study protocol and all related materials for this study were reviewed and approved for use by the Ethics Committee for Biomedical Research Involving Humans, Chinese Academy of Medical Sciences & Peking Union Medical College (Approved No. of ethic committee: CAMS&PUMC-IEC-2025-043; CAMS&PUMC-IEC-2025-060). In the event of a protocol change, the Ethics Committee for Biomedical Research Involving Humans, Chinese Academy of Medical Sciences & Peking Union Medical College and the Chinese Clinical Trial Registry will be informed. After receiving a full explanation face-to-face, participants will be asked to sign an informed consent form.
Electronic files containing participant information will be password-protected and encrypted. In addition, the data of this study will be accessible only to members of the research team under strict confidentiality requirements. The results of this study will be published in a peer-reviewed international scientific journal.
The study was registered with the Chinese Clinical Trial Registry (ChiCTR2500100545). A national coordinating centre will oversee trial implementation, including training of local staff, monitoring of protocol adherence and supervision of data quality across all sites. Each participating county will designate a local coordinator responsible for day-to-day implementation, liaison with village doctors and screening staff, and timely reporting of operational issues. The digital population-management platform will be managed by a dedicated data management team, which will ensure secure data storage, role-based access control, routine data checks and audit trails.
Harms monitoring and data security. Given the minimal-risk nature of the digital messaging intervention, anticipated risks include psychological distress following abnormal results and data-security incidents. All adverse events (AEs) and serious adverse events (SAEs) considered related to study procedures will be recorded by site staff in the platform within 24 h; SAEs will be reported to the ethics committee within 72 h. Any data-security incident will be escalated immediately to the data management and institutional information-security teams in accordance with institutional policy. A national coordinating centre will review safety logs and protocol deviations at regular intervals.
Results
In accordance with this protocol, the recruitment of participants started on 15 April 2025. A total of 142,417 participants will be allocated, with 122,817 in the historical control arm and 9800 in each intervention arm. The baseline survey began on 15 April 2025, and is currently ongoing as of the end of December 2026.
Discussion
Expected findings
We anticipate that implementing a digital push service for cervical cancer screening education will generate measurable benefits, if the intervention is effective in this low-resource setting. With mobile-internet penetration exceeding 90% in China, 25 and WeChat dominating daily communication, smartphone delivery is likely to secure high user engagement. We anticipate improvements in participants’ KAP regarding cervical cancer prevention. Evidence from systematic reviews confirms that tailored health education increases KAP and screening uptake. 26 By delivering accurate, result-tailored messages in the Tailored arm versus generic messages in the Generic arm, the platform can empower women to interpret results and take appropriate follow-up action. In turn, better-informed participants may mitigate post-result anxiety and reduce overtreatment of transient lesions. Higher HPV knowledge has been linked to lower anxiety after positive results. Overall, we expect the digital push to be acceptable and to have the potential to reduce redundant repeat screening.
Comparison with prior work
Traditional health-education initiatives in China have largely relied on one-size-fits-all methods such as community lectures, mass media campaigns, brochures, and clinic seminars. Although they transiently raise awareness, they seldom integrate with individual health management or sustain behavior change over time. For example, community health workers (CHWs) routinely deliver cancer awareness talks to the general public, and such face-to-face education is an established strategy to promote screening adherence by increasing knowledge. 27 However, these programs are typically delivered as standalone sessions and are not tailored to each person's health status or connected to a continuous follow-up system. Participants may receive information passively (e.g., listening to a lecture or reading a pamphlet), without interactive features or personalized reinforcement over time. As a result, once the initial intervention ends, the gains in knowledge or screening behavior often diminish, and there is a paucity of data on enduring real-world impacts. In fact, in-depth evaluations of cancer-related health education programs have rarely been reported in China, underscoring a gap in evidence on long-term outcomes. Moreover, the broader cervical cancer control system has suffered from a lack of ‘closed-loop’ management. Screening, follow-up, and treatment are not tightly coordinated, leading to issues like loss to follow-up. 28 Prior educational campaigns did not typically link to individuals’ medical records or provide ongoing reminders, meaning opportunities were missed to integrate education with actual screening appointments and follow-up care.
Our study embeds education in an ID-card-linked digital platform that couples health messages with each woman's real-time screening status. Result-tailored pushes trigger at key milestones, such as booking, result release, and referral, rather than general broadcasts. These help close the loop between education and action, in line with recent age-specific outreach recommendations. 27 By leveraging digital technology, our program not only disseminates information but also ties into each participant's health actions (like scheduling screening or seeking referral), which earlier methods did not achieve. We believe this integrated model has the potential to produce more sustained improvements in KAP and actual screening behaviors. Furthermore, our trial will collect real-world longitudinal data on these outcomes, helping to fill the evidence gap left by previous short-term studies. In summary, whereas previous work in China often showed only transient KAP improvements after one-off public health messages, our digitally enhanced intervention aims to provide a sustained, interactive education that is woven into individuals’ health management routines, potentially leading to more durable behavior change and better documentation of long-term effectiveness.
Limitations
This protocol has several main limitations. Foremost, the digital nature of the intervention may limit its accessibility for women without smartphones or internet literacy. Individuals who are illiterate in internet use or who only have basic mobile phones (a group typically consisting of some elderly or very low-income residents) may be unable or unwilling to engage with the app-based education content. 27 Their limited exposure could reduce intervention reach and limit the generalizability of our findings to the offline minority. Fortunately, this subset is rapidly shrinking in China. Smartphone and mobile internet penetration have grown enormously in recent years—by mid-2024 China had approximately 1.1 billion internet users (about 78% of the population), 99.7% of whom access the internet via mobile phones. 29 Thus, the vast majority of women in even low-resource communities are now reachable through digital channels. Nonetheless, women who lack smartphones or are uncomfortable with technology may not benefit directly. Additional measures (such as providing parallel offline educational materials or having community health workers assist non-smartphone users) may be needed to ensure these individuals are not left behind. In parallel, we will document women who are identified as eligible in the screening registry but do not enrol in the digital services, extract their available baseline characteristics, and record the primary reasons for non-participation. These data will allow us to quantify the extent of the digital divide and to interpret our findings in light of who was and was not reached by the intervention. Second, KAP outcomes rely on self-reported data and may be subject to reporting bias. We will seek to reduce this risk with validated questionnaires and confidential data collection. In addition, log-based measures of digital engagement may not fully capture informal information sharing or offline learning, and some aspects of equity in access to digital tools may be difficult to measure directly. To address these issues, we will use stratified analyses (e.g., by age group and county), usability scores and qualitative interviews based on the CFIR framework to explore differential reach, implementation fidelity and equity in who benefits from the programme. Third, the inclusion of an external historical control cohort rather than a concurrent non-digital control arm introduces the possibility of temporal confounding and unmeasured changes in policy or service delivery. We will mitigate this risk by restricting the historical period to the two years immediately preceding implementation, using the same eligibility criteria and data sources across periods, and adjusting for site, calendar time and key baseline characteristics in the analyses, but residual confounding cannot be excluded. Finally, as with any community-based intervention, variations in local engagement or healthcare infrastructure could influence outcomes in each site. We will document and analyse these contextual factors when interpreting the results.
Despite these limitations, the intervention's broad compatibility with the current digital landscape in China gives us cautious optimism that it can reach and positively impact the target population in meaningful numbers, if it is successfully implemented at scale.
Conclusion
This protocol describes a pragmatic, quasi-experimental controlled trial that combines an external historical cohort with two individually randomised WeChat-based digital intervention arms in health-resource-limited counties in China. The study is designed to assess whether an ID-card-linked digital population-management platform can improve colposcopy completion, guideline-concordant treatment, and knowledge, attitudes and practices, while reducing redundant repeat screening among hard-to-reach women. If effective, this approach may offer a scalable way to strengthen cervical cancer screening programmes in similar low-resource settings.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076261416317 - Supplemental material for Digital health interventions for cervical cancer screening among hard-to-reach women in health-resource-limited areas: Protocol for a controlled trial with historical controls and two randomised intervention arms
Supplemental material, sj-docx-1-dhj-10.1177_20552076261416317 for Digital health interventions for cervical cancer screening among hard-to-reach women in health-resource-limited areas: Protocol for a controlled trial with historical controls and two randomised intervention arms by Xinhua Jia, Xi’ao Da, Jingyi Shi, Yuting Wang, Mingyang Chen, Yao Yang, Chen Gao, Jiahuan Zhai, Hanyue Ding and Youlin Qiao in DIGITAL HEALTH
Supplemental Material
sj-docx-2-dhj-10.1177_20552076261416317 - Supplemental material for Digital health interventions for cervical cancer screening among hard-to-reach women in health-resource-limited areas: Protocol for a controlled trial with historical controls and two randomised intervention arms
Supplemental material, sj-docx-2-dhj-10.1177_20552076261416317 for Digital health interventions for cervical cancer screening among hard-to-reach women in health-resource-limited areas: Protocol for a controlled trial with historical controls and two randomised intervention arms by Xinhua Jia, Xi’ao Da, Jingyi Shi, Yuting Wang, Mingyang Chen, Yao Yang, Chen Gao, Jiahuan Zhai, Hanyue Ding and Youlin Qiao in DIGITAL HEALTH
Footnotes
Abbreviations
ORCID iDs
Ethical approval
The Institutional Review Board of the Chinese Academy of Medical Sciences and Peking Union Medical College (CAMS&PUMC-IEC-2025-043;CAMS&PUMC-IEC-2025-060).
Contributorship
Study conception, design and overall coordination: Xinhua Jia, Chen Gao, Jiahuan Zhai, Youlin Qiao. Protocol development, gained IRB approval: Xi’ao Da, Jingyi Shi. Manuscript drafting and coordination: Xinhua Jia, Xi’ao Da. Critical revision of the manuscript: Yuting Wang, Mingyang Chen, Yao Yang, Hanyue Ding. Study supervision and corresponding author: Youlin Qiao.
Funding
This study has been supported by the Tencent Sustainable Social Value Inclusive Health Lab and through the ChongQing Tencent Sustainable Development Foundation ‘Comprehensive Prevention and Control Demonstration Project for Eliminating Cervical Cancer and Breast Cancer in Low Health Resource Areas of China’ (Project No.:SD20240904145730), and by medical institutions including Zezhou County Maternal and Child Health Hospital, Wuxiang County Maternal and Child Health Hospital, Xiangyuan County Maternal and Child Health Family Planning Service Center, Mangshi Maternal and Child Health Hospital, Heqing County Maternal and Child Health Hospital, Xinping Yi and Dai Autonomous County Maternal and Child Health Hospital, Yanting County Maternal and Child Health Hospital, Songpan County Maternal and Child Health Hospital, Shimian County Maternal and Child Health Family Planning Service Center, Jingtai County Maternal and Child Health Hospital and Yangcheng County Maternal and Child Health and Family Planning Service Center. The Tencent Sustainable Social Value Inclusive Health Lab and through the ChongQing Tencent Sustainable Development Foundation (Grant No. SD20240904145730).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Guarantor
Xinhua Jia and Youlin Qiao.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.