
Abstract
Introduction
The development of digital health technologies has had a positive impact on the management of comorbidity in the elderly. At the same time, it also sets certain requirements for the digital health literacy of older adults. To effectively implement interventions that improve digital health literacy among older adults with multimorbidity, it is essential to involve patients in decision-making processes and to develop interventions that align with their preferences.
Methods and analysis
This study will use Discrete choice experiment to investigate the needs and preferences of older adults with multimorbidity for digital health literacy intervention. Attributes were identified through a literature review, in-depth interviews, and expert consultation. The attributes are intervention provider, content, type, frequency, material, learning mode, supplementary services, and cost. According to the identified attributes and levels, the choice set questionnaires were generated using Stata software. Furthermore, the study will assess the impact of demographic factors, social support, self-efficacy, levels of digital health literacy, and technology anxiety on the selection of preferences. A mixed logic model will analyze respondents’preferences for different intervention attributes and levels. A latent class model will identify heterogeneous group preferences.
Results
We anticipate a minimum of 300 older adults with multimorbidity in community enrolling and completing data collection. Study results will be published in peer-reviewed scientific journals.
Conclusions
The collection and analysis of patient preference information will greatly improve the accuracy and effectiveness of digital health literacy interventions in the development, adoption, and economic evaluation.
Introduction
Non-communicable chronic diseases are the leading cause of death in the world, according to the World Health Organization, which constitutes 74% of all death. 1 Chronic diseases have become significant public health problems that seriously endanger public health and affects the quality of life of individuals. Meanwhile, with the acceleration of the global aging process, the phenomenon of multiple chronic conditions has become prominent among the elderly. Multiple chronic conditions, also known as comorbidity, refer to two or more concurrent chronic physical, mental, or behavioral health problems in an individual. 2 In recent years, the incidence of multimorbidity in older adults has been on an upward trend. 3 Among Americans aged 65 or older, more than 68% have multimorbidity. 4 In China, about 180 million older adults suffer from chronic diseases, and the prevalence of multimorbidity is 54.4%. 5 Having multimorbidity can have a detrimental impact on an individual's health. Multimorbidity results in reduced physical capabilities, frequent in-person doctor consultations, and higher costs and time investments in utilizing healthcare services among older adults. 6
Effective self-management is crucial for optimizing health outcomes in patients with multimorbidity. The use of digital health technology to seek health information and communicate with doctors on the Internet has become an important avenue of health management for older adults with multimorbidity.7,8 Advances in digital technology have positively impacted the shared use of online healthcare resources and increased access to healthcare services for older adults. For example, the emergence and use of digital health technologies or tools such as telemedicine, 9 smartphone health applications, 10 and wearable devices have become increasingly prevalent. 11 Digital health tools are accessible, affordable, reliable, and effective to facilitate disease prediction, diagnosis, monitoring, management, and personalized treatment.12,13 However, the successful use of digital health tools to access medical information requires digital health literacy (DHL). 14
DHL refers to the ability to address health issues by accessing, understanding, and evaluating health information from electronic resources or digital environments.15,16 DHL has been identified as an important driver of health technology usage. 17 When older adults possess high DHL, their correct perceptions and positive beliefs about health management and health promotion influence health-related decisions, thereby promoting healthy lifestyles and ultimately improving health outcomes. 18 Put simply, a higher level of DHL is associated with better health, more positive health behaviors, and greater health knowledge. Improving DHLs increases likelihood of older adults searching for and finding health information online, which can encourage better health behaviors. 19 However, the level of DHL among older adults with multimorbidity is generally low, 20 which is mainly manifested as the lack of ability to efficiently acquire health information, the lack of ability to scientifically interpret and evaluate health information, and the lack of motivation to effectively use and participate in health management. 21 These problems not only increase the distress and anxiety of multimorbidity in the process of health management, but also cause physical harm and social risks due to false health information. In addition, a scoping review shows that more education to understand their disease and training on how to use technology are existing health needs for older adults with multimorbidity. 22
DHL is not static, it is a capability that can be enhanced through education and training. 23 Previous research has established that interventions can effectively improve the level of DHL among the elderly.24–27 Intervention content typically includes the following main areas: computer basics, 28 major search engines, 29 official patient portals. 30 Yet, few studies have included interventions that take into account the needs of groups of older adults with different online experiences. 29 In terms of intervention methods are traditional classroom, training based on digital technology,31,32 and intergenerational mentors. 24 Intervention periods range from 2 to 8 weeks or even longer. 21 However, due to the different content, methods, and duration of intervention, the current DHL intervention measures and effectiveness vary widely. The effectiveness of DHL interventions needs to be further explored. Additionally, although DHL interventions are short-term, compliance with the intervention is poor and the interventions withdrawal rate is high, particularly for the web-based intervention. 30 A review suggests that intervention plans should be designed to assess the needs of older adults for interventions and to tailor interventions to individual preferences. 33 The American Geriatrics Society Guiding Principles for Care of Older Adults with Multimorbidity recommend eliciting and incorporating patient preferences into medical decision making. 34 Understanding patient preferences for interventions and groups of patients with similar preferences can help to design targeted interventions. Thus, to design acceptable and effective interventions, willingness of older adults with multimorbidity to comply with the DHL interventions must be considered, that is, their preferences for interventions and the contextual factors influencing the preferences. 35 The study aimed to explore the needs and preferences of DHL interventions from a digital empowerment perspective to increase older adults’enthusiasm for utilizing digital health resources and to make digital devices and software easier to use.
Discrete choice experiment (DCE) is a method for eliciting individual preferences
36
and is increasingly being used to elicit preferences for healthcare interventions and services.
37
It can be used in hypothetical situations, allowing preferences to be measured prior to the implementation of potential policy changes or changes in the digital health system.
36
The DCE was carried out as a preparatory part of an intervention trial and was also considered to be an appropriate approach for investigating new interventions.
38
To our knowledge, there are currently few studies on intervention preferences for DHL in older adults. Therefore, we used the DCE method to explore the needs and preferences of older adults with multimorbidity for DHL intervention design prior to intervention implementation. Objectives of this study are as follows:
To identify and explore which components of DHL intervention programs are essential for older adults with multimorbidity. To measure the preferences of older adults for DHL interventions at the individual level, and to understand the importance and heterogeneity of patients’preference for interventions. Understand the preference heterogeneity among different categories of older adults at the group level, thereby explaining the selection preference of each category. Analyze the change in the probability of respondents choosing an intervention when the level of a particular attribute changes, to understand the extent of the impact on preference.
Methods
This study used a cross-sectional DCE within a mixed-methods design. 39 The objective was to elucidate the needs and preferences of the older adults for digital empowerment intervention services. Qualitative data, garnered from in-depth interviews, facilitated the identification of key attributes for the intervention services, 40 ensuring that the attributes and levels incorporated into the experiment were a true reflection of the actual needs of this demographic. Subsequently, a factorial design was utilized to present participants with a series of hypothetical scenarios (choice sets).41,42 Data quantifying participants’preferences were collected through the process of making trade-offs between each choice set, known as the choice experiment phase.
In DCE, attributes reflect the characteristics of a good or service and are a key to understanding consumer preferences. 43 Each attribute has several levels that detail the range of properties between the different options, providing a more nuanced baseline for comparison for each property. Choice sets encompass various attributes and level combinations. Responses to multiple choice sets enabled the researchers to estimate the relative importance of different attributes of the scenario and understand participants’ preferences for intervention services. 44 The development process of the DCE is shown in Figure 1.

The development process of the discrete choice experiment.
Step 1: identifying and defining attributes and levels
Literatures review
We conducted a comprehensive literature review on DHL interventions for older adults with multimorbidity, utilizing databases such as Web of Science, EMBASE, PubMed, China National Knowledge Infrastructure (CNKI), and WANFANG DATA. To ensure thorough search, we employed a strategy that combined medical subject headings with text words. The search strategy exemplified on PubMed is as follows: ((Geriatric OR senior* OR Aged OR old OR “old people” OR “older people” OR “older adult” OR “elder*” OR “elder people” OR “elderly people” OR “elder adults” OR “aged people” OR “aged person” OR aging OR “baby boomer” OR retiree*) AND (“ehealth literacy” OR “e-health literacy” OR “digital health literacy” OR “digital literacy program” OR “online health literacy” OR “online health information” OR “web-based health information” OR “electronic health literacy” OR “electronic health information” OR “mhealth literacy” OR “telehealth literacy” OR “health information literacy” OR “information literacy” OR “computer literacy” OR “basic computer training” OR “computer literacy program” OR “ICT training”)). After retrieval, the facilitators, and barriers to DHL intervention in the elderly were analyzed and summarized. The needs for DHL intervention in the elderly with chronic complications and the potential attributes and levels were identified.
In-depth interviews
After a comprehensive review of the existing literature and the identification of a range of potential attributes and levels, in-depth interviews were conducted. This approach aimed to further refine the attributes and levels, ensuring they more closely aligned with the actual needs of older adults with multimorbidity. 45 We posted recruitment posters in community health services centers to attract potential participants. The posters provided information about the study, including its purpose, the nature of the interviews, and how to express interest in participating. For older adults who expressed interest, our researchers accessed their electronic medical records at the community health centers to check for a diagnosis of chronic diseases. After identifying eligible seniors based on their medical records, we contacted them to collect basic demographic information and further confirm their eligibility to ensure compliance with the maximization of sampling principle.
Maximal difference sampling is a sampling strategy used in qualitative research. This approach emphasizes finding and exploiting significant differences between respondents in sample selection to ensure that the results reflect the opinions and feelings of different populations as fully as possible. 46 We applied the difference maximization principle on key features to enrich the content of the interview. In our study, these characteristics included demographic information, chronic disease status, and digital device usage (Supplemental material 2). However, the interviews do not pursue the size of the sample but depend on the principle of data saturation. 47 As interviews are conducted, the researcher needs to assess whether enough information has been obtained from the different groups. When information from a new interview begins to repeat itself and no longer provides new insights, information saturation is considered to have been reached. 48 This is also a key criterion for determining the adequacy of sample size in qualitative research. 49 A systematic review shows that studies with relatively uniform study groups and narrow target definitions usually reach saturation in the range of 9–17 interviews. 50 Our study's population, consisting of community-dwelling older adults with multimorbidity, is relatively homogeneous, and objectives are specifically focused on DHL intervention preferences. After each interview with respondents, two researchers independently conducted iterative analysis of the interview content to increase the depth of analysis. Finally, 15 older adults with multimorbidity in the community completed in-depth interviews. (November 2023 and January 2024).
The interviews primarily focused on the experiences of older adults using digital devices to access health information and medical services, the difficulties they encountered, what kind of support services they would like to receive, and how such services should be delivered. Throughout the interview process, researchers posed relevant questions and asked follow-ups based on the participants’ responses. Interviews lasted 30–50 min (average 40 min). All interviews were recorded for subsequent transcription and coding. The interviews were conducted by a researcher who was trained and experienced in qualitative interviewing techniques.
Interviews occurred in the Health Education Clinic of the Community Health Service Centre, a location that ensured a quiet and private environment. At the end of the interview, participants received a 5 yuan compensation gift. Then, we transcribed, coded, and analyzed recordings of in-depth interviews. Directed content analysis, often used in needs assessment, project review, and intervention development, involves a direct description of experiences or events. 51 During the analysis, two researchers independently coded the interview content using NVivo 12 software, focusing on respondents’ needs for learning to use digital health technologies and services.
Expert consultation
Policy determines resource allocation and support, while the medical context determines the specific needs and application scenarios for digital empowerment intervention. To ensure that the potential attributes and corresponding levels were appropriate in the current political and medical context, we consulted with experts in the field of chronic disease management in the community (February 2024 and April 2024). These experts were asked to rate the importance of potential attributes and levels on a scale from 1 (unimportant) to 5 (important). In addition, the description of the attributes and levels were reviewed by experts to ensure linguistic accuracy and comprehensibility.
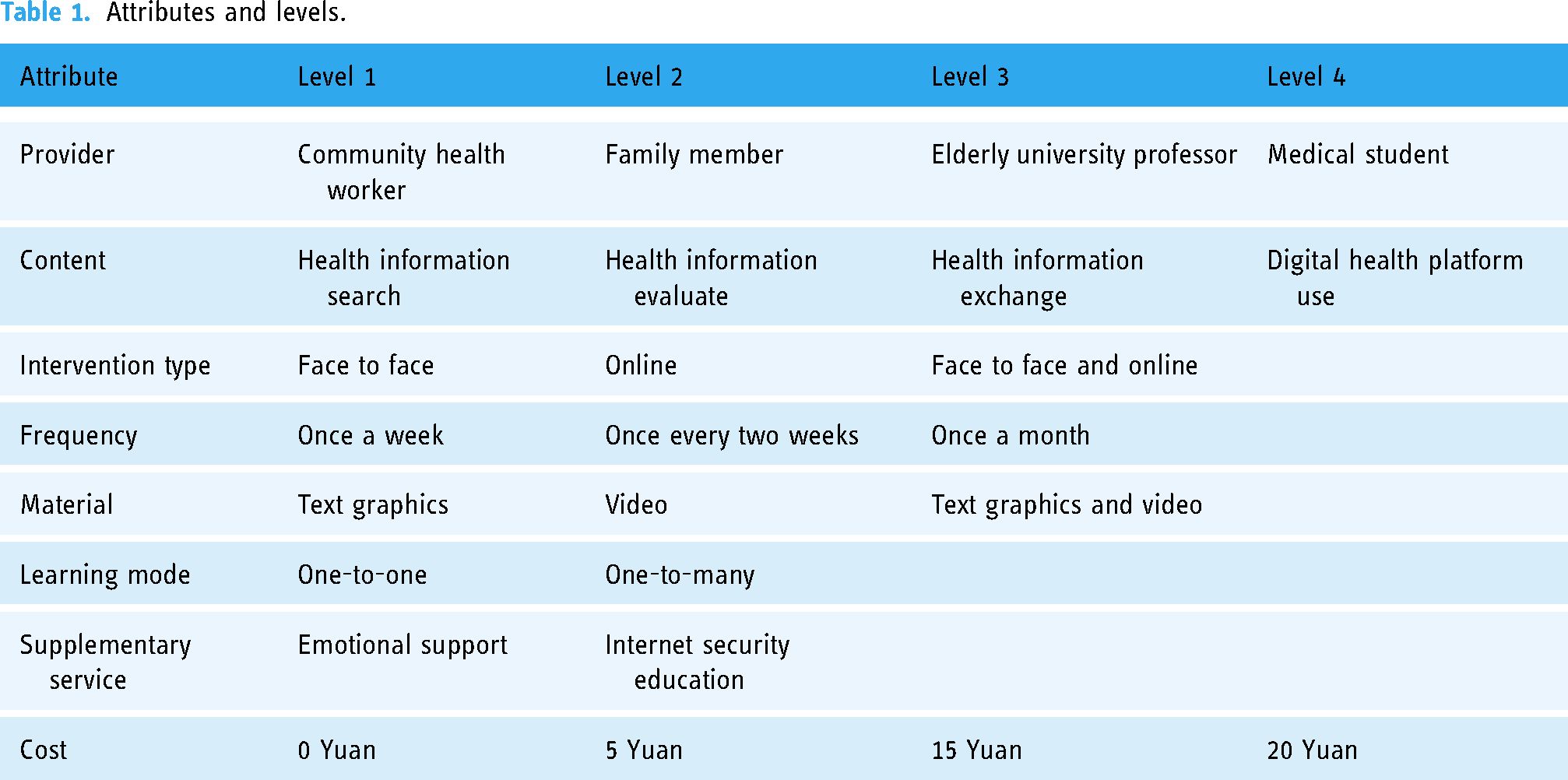
The selection of experts was based on the following criteria: they had to have been engaged in research or work related to chronic diseases in the elderly within the community for at least 5 years, hold a bachelor's degree or higher, and possess an intermediate or higher professional title. Ultimately, 16 medical professionals, including three public health physicians, four community physicians, and nine nurses, completed two rounds of correspondence. Table 1 shows the attributes and levels of digital empowerment interventions.
Attributes and levels.
Step 2: generate choice sets and questionnaire designs
Choice task questionnaire
The number of choice sets depends on the attributes included in the study and the number of their corresponding levels. 52 In the design of a selection questionnaire for DCE, it is important to minimize the correlation between attribute levels, balance the number of occurrence levels, and minimize the overlap of attribute levels between systems. 53 Full factorial design synthesizes all possible combinations. However, this is difficult to implement in practice. Therefore, this study adopted fractional factorial designs to optimize the choice sets and reduce the cognitive burden on participants. 54 Additionally, we included an opt-out option to more accurately reflect the behavior of respondents in the real world, who often have the choice not to select any option. The D-efficient design in Stata 17.0 was utilized to generate the choice sets for the choice task questionnaires. Finally, we created 27 choice sets and divided them into three versions of the questionnaire. Respondents were asked to complete only one version of the questionnaire. An example of the choice task is shown in Figure 2.

An example of the choice task.
Administration of the questionnaire
The questionnaire is organized into two distinct sections. The initial section provides a comprehensive explanation of the attributes and levels, followed by choice sets. Before conducting the choice experiment, we provided textual descriptions of the specific meanings of each attribute and level to enhance participants’comprehension and ensure a uniform interpretation (Supplemental material 1). To further aid understanding, especially for those with low digital literacy, we incorporated visual aids when presenting the choice set. Each level is illustrated with images to help participants understand the meaning (Figure 2). Images also can help older adults better recall the details of what they had previously seen in words that detailed descriptions of attributes and levels.
The second section gathers general information about the participants, encompassing demographic information, chronic disease status, and digital device usage. To understand respondents’representation in the DCE and to conduct subgroup analyses to explore the impact of other factors on preferences, additional information needs to be collected. We also used the Digital Health Literacy Assessment Scale For Community-dwelling Older Adults to measure the level of DHL, the Technophobia Scale to measure the degree of technical anxiety in older adults, the Social Support Rating Scale to measure the degree of social support older adults received, and the General Self-efficacy Scale to measure an individual's self-confidence in the face of new things.55–58 The higher the score on the scale, the higher the corresponding literacy or degree of the individual. This will help to analyze how these factors influence their preferences for choosing intervention services.
Pilot study
Whether respondents understand the definition of attributes and levels, whether they understand the choice task, and whether they can make a trade-off between the two intervention options requires pilot studies. The DCE User Guide specifies that at a minimum of 30 respondents is required for the pilot study. 59 Consequently, a pilot study was conducted to ensure the questionnaire's comprehensibility prior to the formal survey. Electronic medical records of patients attending community health centers were retrieved and people over the age of 60 who had been diagnosed with two or more chronic conditions were identified as potential participants. For potential participants, researcher further asked patients for information on inclusion criteria to determine eligibility for participation in the pilot study. Researcher then distributed the questionnaires face-to-face to those who agreed to participate and informed them of the instructions for completing the questionnaire. Participants filled out questionnaires in the field and collected them immediately. The researchers recorded how long they spent filling out the questionnaires and participants’feedback on it. Ultimately, 32 older adults who met the study criteria completed the pilot study at a community health service center.
Recruitment and sample size
Inclusion criteria were as follows: (1) individuals aged 60 and above, (2) diagnosed with two or more chronic diseases, (3) community-dwelling (not in long-term care) at the time of recruitment, (4) ownership of at least one smart device, and (5) able to provide written consent to participate in this study. Participants with cognitive impairments or communication deficits were excluded.
The sample size for the choice questionnaire is contingent upon the structure of the DCE questions, the desired precision of the outcomes, and the degree of preference heterogeneity within the population.
60
An excessively large sample size can lead to a needless expenditure of manpower, financial resources, and other assets. An insufficiently small sample size, typically considered to be less than 30, may preclude meaningful statistical analysis.
59
In the context of DCE, an adequately large sample size is essential for capturing significant preference variations across the observed population and for discerning differential preferences among various subgroups. Currently, there are multiple methodologies for ascertaining the appropriate sample size for choice set questionnaires. Research indicated that each questionnaire version with 20–30 participants can yield accurate parameter assessments.
61
Pearmain et al. showed that a sample size of 100 or more can provide a reliable preference gauge.
62
Research by Johnson and Orme indicated that a sample size of approximately 150 achieves the highest level of precision, with a decline in accuracy observed when the sample size exceeds 300.
63
Johnson and Orme's thumb formula offered a means of calculating the minimum sample size. However, the choice of sample size is largely dependent on budget and available resources. Therefore, based on the previous research experience and the limited resources of this study, we adopted the thumb formula to calculate the sample size.64,65
The survey will be conducted in five community health service centers. Prior to the recruitment, we conducted comprehensive training for the researchers involved in the study. The training content had the purpose of research, the meaning of selecting the set, the precautions to fill out the questionnaire, and the communication skills with the elderly. One researcher is responsible for screening potential participants to ensure they meet the inclusion criteria. This researcher also obtains written consent from eligible participants and provides them with a small gift as a token of appreciation. The paper questionnaires are distributed face-to-face to participants who meet the inclusion criteria. Participants are randomly received one of three versions of the questionnaire. Another researcher helps the participants with any questions they may have while filling out the questionnaire. Questionnaires data will be double-checked by two researchers with input analysis software.
Step 3: modeling analyzed preference heterogeneity
Ethics and institutional review board
The study has been reviewed and approved by the Ethics Institutional Review Committee of Qingdao University (reference number: QDU-HEC-2023228). In the data collection section, we will obtain a paper informed consent form signed by the respondents for the data collection. The data collected will be anonymized and used only for this study. Participants who complete the questionnaires will receive compensation in the form of a gift (5 yuan).
Data analysis plan
Quantitative data from the DCE is analyzed using random utility theory. Random utility theory is an economic theory that assumes that individual preferences are random and can be quantified as utility functions. 41 Data is analyzed using random-effects binary probits and logits, conditional logits, and mixed logits for estimating participants’ preferences for different intervention attributes. 52 Compared to other models, the mixed logit model is a more flexible model that allows the parameters of the utility function to vary randomly between individuals and captures heterogeneity and dynamic changes in respondents’ preferences.66,67 This model generates two main parameters, the mean coefficient and the standard deviation. The mean coefficient represents the average degree of respondents’ preference for the level of the intervention attribute. The higher the coefficient, the stronger the influence on the decision to choose. The standard deviation represents the heterogeneity of respondents’ preference for the same attribute.
Mixed logit model analyses individual preferences for different intervention attributes and levels, while the latent class model (LCM) can be used to identify heterogeneous group preferences. 68 Respondents are categorized based on their choice preferences, allowing for an understanding of the choice preferences within each group. Understanding the preferences of different sub-groups will help design more personalized interventions to meet the needs of different groups.
In addition, this study analyses willingness to pay (WTP) to measure the strength of an individual's preference for and valuation of intervention service attributes. WTP can be calculated as the ratio of the coefficient value of the attribute level to the coefficient of the consumption attribute. 69 A positive WTP value indicates that a participant is willing to pay an additional cost to obtain a higher level of an attribute. Uptake rates are calculated by simulating changes in probability of receiving an intervention from baseline after a change in the level of one or more attributes. 59 For example, when the providers of intervention services shift from community health workers to medical students, the probability of older adults accepting intervention programs may increase or decrease.
Discussion
With the extension of average life expectancy and the development of medical technology, the elderly's requirements for medical and health services have evolved to encompass comprehensive health management. Digital health information has become an essential resource for older adults with multimorbidity to manage their health and make informed decisions. Better access to, understanding, and application of digital health information to manage one's health more effectively requires DHL. Understanding the needs and preferences of older adults with multimorbidity for improving DHL has important implications for tailoring and adapting digital empowerment intervention services.
The study found that older adults need different types of digital empowerment intervention providers. Fully mobilizing social resources to expand digital skills education resources and access channels is the way to improve the DHL of the elderly. In the context of digital healthcare, the elderly often have specific needs when they use digital devices to obtain health information and medical services, such as how to consult their medical conditions online. 70 Community health workers may have more specialized medical knowledge and be able to provide precise guidance to older adults around specific needs. However, for remote areas not covered by community health service centers, intergenerational support is more critical to improving DHL among older adults. 71 In China, family support is still the main mode of support, and children are the main caregivers of the elderly. Under such a social background, the younger generation's familiarity with digital tools and flexibility in their time schedules can help older people search for health information and use digital platforms faster, improving DHL. However, interviews found that some elderly people do not want family members to provide intervention, but prefer other types of personnel, such as senior college teachers and medical students. This may be related to the fact that older people usually have strong independence and self-esteem, and they are reluctant to ask their children for help frequently, fearing that it is a burden on their children.
In terms of intervention content, the elderly wanted to choose content modules they were not familiar with to receive intervention. This is different from Mitsuhashi's intervention. 32 Many intervention contents may increase the learning burden and psychological pressure of the elderly and have a negative impact on the compliance of intervention services. When the elderly learn and use digital platforms, they often face the challenge of physical function and memory decline, which makes them only gradually learn the content they need most in the face of many intervention contents. This study set up separate modules in the intervention content, such as health information assessment and health information exchange. The elderly pay more attention to practicability, which makes them choose the content module they need most to receive intervention. Additionally, the elderly's anxiety about the use of technology and their concern about privacy and security have attracted our attention. This is consistent with previous research. 72 In the intervention to improve the DHL of the elderly, some patients raised concerns about the security of their medical information, which might lead them to give up using certain services when necessary. Anxiety regarding digital technology utilization hampers acceptance and learning of intervention services and fosters resistance to digital devices. The provision of supplementary services can help older adults increase their personal self-confidence, make them more willing to experiment with and use digital technologies, and be more receptive to digital empowerment intervention services.
DCE are used to elicit participants’ preferences for digital empowerment intervention services. However, there are some limitations to be acknowledged. DCE data is collected at only one point in time, so it is not possible to measure changes in people's willingness to receive intervention services over time. Additionally, DCE contains a limited number of attributes and levels in the choice set. We used literature reviews, qualitative interviews, and expert consultations to comprehensively identify the critical attributes and levels for inclusion. However, as participants struggled to understand more than six to eight attributes, it was difficult for studies to represent all the potentially important features of complex health care systems in the DCE choice sets.
Conclusion
Chronic disease management within the digital realm is inherently constrained by the DHL levels of patients, particularly among the elderly suffering from chronic conditions. Our study employs a DCE to ascertain the preferences of older adults for DHL intervention services and to pinpoint the most significant intervention attributes. Insights culled from patient preference data are invaluable to healthcare providers and policymakers, facilitating the provision of digital health management solutions tailored to the specific needs of older adults and the formulation of effective interventions to achieve digital empowerment.
Supplemental Material
sj-doc-1-dhj-10.1177_20552076251319662 - Supplemental material for Preferences of community-dwelling older adults with multimorbidity for digital empowerment interventions: Protocol for a discrete choice experiment study
Supplemental material, sj-doc-1-dhj-10.1177_20552076251319662 for Preferences of community-dwelling older adults with multimorbidity for digital empowerment interventions: Protocol for a discrete choice experiment study by Yawen Ren, Li Yang, Wenguang Wang, Runtian Lv, Xiuqing Fang, Yueling Wang and Jiayi Zhong in DIGITAL HEALTH
Footnotes
Acknowledgements
We appreciate the support of the medical staff at the Community Health Service centers in recruiting patients. We are also grateful to the 16 medical experts who completed the survey for their suggestions on modifying the DCE attributes and levels.
Contributorship
Yawen Ren: writing—review and editing, writing—original draft, validation, methodology, data curation, investigation, conceptualization, formal analysis. Li Yang: writing—review and editing, writing—original draft, validation, supervision, project administration, methodology, formal analysis, conceptualization. Wenguang Wang: validation, methodology, data curation, investigation, formal analysis, software. Runtian Lv, Xiuqing Fang, Yueling Wang, Jiayi Zhong: data curation, methodology, formal analysis, writing – review and editing, software.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval
The study has been reviewed by the Ethics Institutional Review Committee of Qingdao University (reference number: QDU-HEC-2023228). Literature review, in-depth interviews, expert consultation, and pilot study were completed in May 2024. Patient recruitment will start in June 2024 and is expected to end in May 2025. In the in-depth interview, all respondents signed an informed consent form. In the data collection part, we will also obtain informed consent for data collection from the respondents. The data collected will be anonymized and used only for this study.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Natural Science Foundation of Shandong Province (grant number No. ZR2023MG071).
Guarantor
Li Yang.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.