
Abstract
Background
Mental health conditions commonly co-occur with chronic diseases, yet few evidence-based interventions are designed for rural populations or scalable within primary care. This study evaluated the mental health impact, clinical significance, and usability of a digitally delivered Personal Empowerment Program (PEP).
Methods
This single-arm prospective interventional trial (October 2023−August 2025) enrolled 182 community-dwelling adults with ≥1 physician-diagnosed chronic condition in Pictou County, Nova Scotia. The six-month PEP program delivered daily digital modules via email and YouTube covering physical fitness, nutrition, mindfulness, sleep, and social connection, with weekly self-monitoring and monthly videoconferencing, optimized for low-bandwidth mobile access. The primary outcome was psychological distress (Kessler Psychological Distress Scale (K10); secondary outcomes included anxiety (GAD-7) and depression (CES-D). Generalized estimated equations assessed changes (baseline, 6, and 12 months).
Results
A total of 115 participants (63.2%) completed 6- and 12-month K10 follow-up assessments. K10 scores declined by 3.00 points (95% CI:−4.05,−1.95) at 6 months and 3.60 (95% CI:−4.84,−2.36) at 12 months (both P < 0.001). GAD-7 scores declined by 1.36 points (95% CI:−2.28,−0.45) at 6 months and 2.11 points (95% CI:−3.03,−1.20) at 12 months, while CES-D scores declined by 2.43 points (95% CI:−4.65,−0.21) at 6 months and 4.31 points (95% CI:−6.84,−1.78) at 12 months. Clinically meaningful improvement at 12 months was observed in 23% (K10), 23% (GAD-7), and 38% (CES-D) of participants. Usability ratings were high.
Conclusions
PEP demonstrates sustained mental health benefits and high usability within a scalable, low-bandwidth digital model, supporting equitable mental health care for rural adults with chronic conditions.
Keywords
Introduction
Chronic conditions affect nearly half of Canadian adults, contributing to psychological distress, diminished quality of life, and escalating healthcare costs.1,2 According to the Public Health Agency of Canada, 45.1% of adults over age 20 have at least one chronic condition, and nearly one-third experience multimorbidity.1,3 Comorbid anxiety and depression, present in up to 40% of patients, are associated with poorer treatment adherence, increased healthcare utilization, and worse outcomes. 4 Despite the proliferation of digital tools in healthcare, most models continue to prioritize physical symptoms, overlooking scalable, digital approaches to psychosocial care, particularly in rural and underserved settings. 5
Rural communities face disproportionately high rates of chronic disease and limited access to mental health services, exacerbated by geographic isolation, specialist shortages, and transportation barriers.5–7 In Pictou County, Nova Scotia (∼44,000 residents), approximately one-quarter of adults lack a family physician, and rates of obesity (33.7%) and diabetes/prediabetes (33%) exceed national averages.1,8–10 Recent national surveillance data show that nearly one-third of Canadian adults live with obesity, which substantially increases the risk of multiple chronic conditions and adverse health outcomes. 11 Obesity and diabetes are also closely linked with psychological distress and depression. Canadian and international studies show that adults with diabetes have nearly twice the odds of major depressive disorder, while obesity is associated with higher rates of mood and anxiety disorders.5,11,12 These intersecting physical and mental health burdens are further intensified in rural Nova Scotia, where persistent provider shortages, digital inequities, and social isolation leave residents vulnerable to delayed or fragmented mental healthcare. 13
Multicomponent, home-based interventions that enhance patient activation and support self-management show strong potential for improving mental health and quality of life among individuals with chronic conditions.14–17 A recent systematic review and meta-analysis of 43 randomized controlled trials involving over 10,000 participants by Silva et al. reported that multicomponent lifestyle interventions targeting two or more health behaviors, such as structured exercise, dietary modification, behavioral self-management support, and mindfulness, produce small to large improvements in key health behaviors and significant positive effects on health outcomes among adults with chronic conditions. 18 Many digital interventions remain short in duration (typically fewer than 8 to 12 weeks) and focus narrowly on a single behavioral domain, such as exercise or diet, limiting their ability to sustain behavioral and psychological change.16–20 Programs that simultaneously address physical activity, nutrition, mindfulness, and stress management have shown stronger and more durable effects, yet these multicomponent approaches are rarely adapted for rural populations facing multimorbidity, unreliable broadband access, and limited health-service infrastructure.21,22
The Pictou County-Patient Empowerment Program (PEP) was developed to overcome these limitations by providing a 6-month, multicomponent intervention that integrates daily behavioral prompts, nutritional guidance, exercise videos, mindfulness and stress-management training, and peer support. Delivered asynchronously via daily emails and short, low-bandwidth videos accessible on any device, PEP is specifically designed for rural adults with chronic conditions. By extending duration, broadening content, and optimizing accessibility, PEP addresses key shortcomings of prior digital and home-based programs.
The Prostate Cancer Patient Empowerment Program (PC-PEP), a 6-month digital intervention integrating physical activity, nutrition, mindfulness, sleep hygiene, and social connection, demonstrated significant reductions in psychological distress and was cost-effective, improving quality-adjusted life years.23,24 Building on this success, the program was expanded into the Cancer Patient Empowerment Program (CancerPEP) to serve individuals diagnosed with diverse forms of cancer.25 Adaptations in CancerPEP included removing modules specific to prostate cancer (e.g. pelvic floor and Kegel training), adopting gender-neutral language and imagery, and incorporating 26 weeks of cooking videos featuring affordable, nutritious, plant-based recipes tailored for rural accessibility and food security. The program also introduced 26 weeks of attitudinal healing teachings; secular, evidence-informed lessons on forgiveness, compassion, and reconciliation, drawing inspiration from Indigenous Canadian healing traditions such as the Medicine Wheel, as well as from Māori and Hawaiian concepts of health, all of which emphasize balance and the interconnectedness of physical, emotional, mental, and spiritual well-being. Additional modules addressed fatigue, sleep, multimorbidity, and goal-setting relevant to diverse cancer survivorship contexts. In a phase 2 interventional trial, CancerPEP significantly reduced psychological distress among patients with various cancer types (excluding prostate cancer); a subanalysis among breast cancer participants demonstrated similar benefits. 25
Building on this foundation, the Pictou County PEP was developed to extend PC-PEP and CancerPEP frameworks to a broader rural population living with chronic conditions. PEP was nearly identical in structure and delivery but replaced cancer-specific education with chronic-disease self-management content and goal setting applicable to multiple health conditions. The delivery model was optimized for rural feasibility through low-bandwidth, asynchronous formats (daily emails and short videos accessible on any device). These adaptations preserved PC-PEP's evidence-based multicomponent framework while enhancing inclusivity, accessibility, and cultural resonance for rural adults with chronic diseases.
This single-arm prospective interventional trial evaluated Pictou County PEP's impact on psychological distress (primary outcome), anxiety, and depression over 12 months. We hypothesized that this low-bandwidth, digitally delivered program would yield sustained improvements in mental health outcomes, specifically reductions in psychological distress, anxiety, and depression, based on both theoretical and empirical evidence supporting its design. Frequent, brief, self-directed behavioral engagement fosters habit formation, self-efficacy, and perceived control, key mechanisms that buffer psychological distress.14,23,25–28 Daily micro-interventions integrating mindfulness, exercise, nutrition, gratitude, and attitudinal healing have been shown to strengthen emotion regulation and resilience even when delivered asynchronously.16,29,30 Moreover, low-bandwidth asynchronous formats improve accessibility and adherence in rural populations where broadband limitations and variable schedules hinder synchronous participation.19,20,23,25
Evidence from prior PEP trials supports the proposed mechanisms of action. In a phase 3 PC-PEP randomized clinical trial, a 6-month digital intervention significantly reduced psychological distress compared with standard care among men with prostate cancer. Mechanistic analyses from the same trial showed that improvements in self-efficacy and illness perceptions explained nearly 50% of the variance in distress reduction among participants who received the intervention. 14 Similarly, the CancerPEP trial demonstrated significant and sustained reductions in Kessler Psychological Distress Scale (K10)-measured psychological distress over 12 months among individuals with diverse cancer types (excluding prostate cancer). 25 Together, these findings indicate that multicomponent, digitally delivered empowerment interventions can durably improve mental health by enhancing behavioral activation, strengthening self-efficacy, and increasing accessibility. Building on this theoretical and empirical foundation, we hypothesized that the low-bandwidth, multicomponent PEP program would yield meaningful and sustained reductions in psychological distress among rural adults with chronic conditions. By targeting the urgent need for accessible mental health interventions in underserved settings, this study seeks to provide a practical and scalable model to help close persistent gaps in chronic disease care.
Methods
Study design and participants
This single-arm, prospective interventional trial (October 2023–August 2025) was conducted in Pictou County, Nova Scotia, a rural region with ∼44,000 residents and limited access to specialty care. Adults aged ≥18 years with ≥1 chronic condition (e.g. diabetes, obesity, hypertension; excluding cancer within 5 years) were recruited via community flyers, media, and social media outreach. Eligibility required safety for low-to-moderate exercise (Physical Activity Readiness Questionnaire), English proficiency, and internet access. Individuals with a current or past cancer diagnosis within the preceding 5 years were excluded because the intervention has already been evaluated extensively in cancer populations through PC-PEP and CancerPEP trials. The present study sought to assess the feasibility and mental-health impact of the adapted PEP model in adults living with chronic conditions other than cancer. While this exclusion may limit generalizability to cancer survivors with concurrent chronic illness, it ensured that findings specifically reflected the program's performance within a noncancer chronic-disease context.
Participants provided electronic informed consent through REDCap's e-Consent platform, which also enabled secure online survey administration hosted by Nova Scotia Health. 31 All participants were enrolled consecutively and completed online surveys at baseline, 6 months, and 12 months. All procedures complied with Nova Scotia Health privacy and data security policies and Canadian PIPEDA standards. The study was approved by the Nova Scotia Health Research Ethics Board (1029744) on October 19, 2023, prior to participant recruitment. The study was registered as a single-arm prospective interventional trial with ClinicalTrials.gov (NCT06064110). All 182 participants who consented completed baseline assessments and were included in intention-to-treat (ITT) analyses. Figure 1 presents the participants flow diagram illustrating recruitment, enrollment, and follow-up. Exclusion reasons are provided in eTable 1 in the Supplemental materials.

Flow diagram of participant recruitment, allocation, follow-up, and analysis. Flow of participants through the Pictou County personal empowerment program (PEP) single-arm prospective interventional trial (nonrandomized). Of 236 individuals assessed for eligibility, 182 were enrolled and received access to the 6-month home-based digital lifestyle intervention. Reasons for nonenrollment included not meeting inclusion criteria (n = 54), declining to participate (n = 50), and other reasons (n = 4). All 182 participants were included in the intention-to-treat (ITT) analysis. Follow-up assessments were completed by 115 participants at both 6 and 12 months. The remaining 67 were lost to follow-up. CONSORT 2010 extension for nonrandomized trials. Trial registered at ClinicalTrials.gov: NCT06064110.
Intervention
The Pictou County PEP was a 6-month, home-based program that delivered daily emails with 4–6-min YouTube videos guiding participants through six behavioral domains: (1) aerobic exercise (150–300 min/week), (2) strength training or yoga (30 min twice weekly, moderate-to-intense), (3) relaxation techniques (≥10 min/day), (4) dietary advice (mostly plant-based, limiting ultra-processed foods, per Canada's Food Guide), 32 (5) habit formation, and (6) relationship training.
Content was optimized for low-bandwidth and mobile accessibility, ensuring reach in rural and underserved settings without requiring high-speed internet or specialized apps. Optional components included a peer “buddy” system, monthly live videoconference sessions (via Zoom), and occasional in-person events to foster community connection and accountability.
Adherence and feedback monitoring
Adherence was assessed weekly using self-reported frequency measures indicating the number of days per week participants engaged in each coreprogram component (e.g. exercise, mindfulness, nutrition), typically on a 0–7 days/week scale (eTables 2 and 3 in the Supplemental materials). Although REDCap did not track email open rates, participants reported viewing daily emails and videos an average of 5.4 days per week. Their perceived usefulness of key components, which included daily educational videos, nutrition modules, buddy pairing, and monthly videoconferences, is summarized in eTable 4 (Supplemental materials). These self-reports closely aligned with weekly compliance data (eTable 3 in the Supplemental materials), supporting the reliability of engagement measures.
Participants received automated weekly reminders to complete compliance surveys, which included open-ended feedback used to refine engagement strategies. Nonresponders were contacted by phone to address technical or motivational barriers, enhancing retention.
Open-ended feedback was reviewed biweekly by the research team to identify common issues and improvement opportunities. Suggestions informed implementation refinements. For example, clarifying exercise video instructions, simplifying email formatting for mobile access, and adjusting reminder timing to align with participant routines. These usability enhancements improved engagement but did not alter the program's core content or duration.
Adaptation for chronic conditions
The Pictou County PEP retained the multicomponent structure of CancerPEP but removed all cancer-specific education. Exercise and nutrition modules were grounded in national, evidence-based guidelines and designed to be safely adaptable across chronic conditions (e.g. diabetes, hypertension, arthritis). Videos and written guidance provided examples and cautions relevant to these conditions. For example, pacing and exertion monitoring for cardiovascular disease or blood-sugar awareness for diabetes, while encouraging participants to tailor intensity and diet in consultation with their healthcare providers.
Outcomes and measures
The primary outcome was psychological distress, measured by the K10 (range, 10–50; higher scores indicate greater distress). 33 The continuous K10 sum score was prespecified as the primary analysis for hypothesis testing, assessing mean change in psychological distress over time. K10 was also analyzed in binary form (K10 ≥ 20, indicating significant distress) and as a responder variable (≥7-point reduction from baseline), both considered secondary analyses to aid interpretation of clinical significance. 33 Secondary outcomes also included anxiety (Generalized Anxiety Disorder 7-item (GAD-7); range, 0–21) and depression (Center for Epidemiologic Studies Depression Scale (CES-D); range, 0–60).34,35 Responder status was defined as a reduction of ≥7 points in sum K10 scores, ≥4 points in sum GAD-7 scores, and ≥5 points in sum CES-D scores, based on established minimal clinically important differences (MCIDs).36–38 Sensitivity analyses used higher MCIDs of ≥10 points for K10 and ≥9 points for CES-D to assess robustness in more severe cases (Supplemental materials). 39 For the K10, a ≥7-point reduction has been associated with reliable change in psychological distress in community and clinical populations. 36 For the GAD-7, an MCID of ≥4 points was established in clinical settings. 37 For the CES-D, a ≥5-point reduction was considered clinically meaningful in community-based populations, with ≥9 points used for chronic disease populations.38,39 Covariates included age, sex (assigned at birth), relationship status, Charlson comorbidity index, and baseline anxiety/depression medication use.40–43 These covariates were selected a priori based on theoretical relevance and prior evidence from the PC-PEP and CancerPEP trials, which identified these factors as potential confounders or modifiers of mental health outcomes.23,25 Specifically, sociodemographic variables (age, sex, relationship status) have been associated with psychological distress and program adherence, while comorbidity burden and baseline psychotropic medication use may influence both baseline distress and response to behavioral interventions.40–43
Sample size
This phase 2 interventional feasibility study enrolled 182 participants to evaluate feasibility, adherence, and preliminary effectiveness. The target sample size was determined pragmatically based on projected recruitment capacity within the study timeframe rather than a formal a priori power calculation.
Statistical analysis
All analyses followed the ITT principle, including all participants with baseline data regardless of program adherence or follow-up completion. Primary and secondary outcomes were analyzed using generalized estimating equations (GEEs) to model repeated measures across three time points (baseline, 6 months, 12 months).
Continuous outcomes (K10, GAD-7, CES-D) were modeled assuming a Gaussian distribution with an identity link function, while binary outcomes (e.g. K10 ≥ 20, responder status) used a binomial distribution with a logit link. An exchangeable working correlation structure was selected because correlations among repeated measures were expected to be similar across time points, providing efficient and robust estimates under a missing-at-random (MAR) assumption for moderately correlated longitudinal data. Robust (Huber–White) standard errors were used to account for potential model misspecification. All models were adjusted for prespecified covariates: age, sex, relationship status, Charlson comorbidity index, and baseline anxiety/depression medication use. Estimated marginal means and pair-wise time-point comparisons were computed using the emmeans package in R (version 4.4.1).44,45 Tukey-adjusted tests were used to control the family-wise error rate across posthoc pair-wise comparisons, while the primary contrast (baseline vs. 6-month K10 change) was tested at a two-sided α = 0.05 without adjustment.
Missing data were evaluated using logistic regression, modeling the probability of missingness as a function of baseline age, sex, relationship status, comorbidity index, baseline K10 score, and medication use. No baseline variable significantly predicted missingness (all P > 0.10), supporting the MAR assumption. Under this assumption, GEEs incorporate all available data at each time point without imputation, yielding unbiased population-averaged estimates. Therefore, a GEE-based ITT analysis was performed rather than a strict complete-case analysis.
Responder analyses were conducted for each outcome using binary logistic regression, comparing the proportion of participants achieving the predefined MCIDs (≥7 points for K10, ≥4 for GAD-7, ≥5 for CES-D). Changes in responder proportions from baseline to follow-up were assessed using McNemar's test, and 95% confidence intervals (CIs) for responder rates were calculated using exact binomial methods.
Sensitivity analyses using higher MCID thresholds were conducted to assess robustness. All tests were two-sided with α = 0.05.
Attrition and missing data handling
Analyses followed an ITT-consistent approach, including all participants with baseline data regardless of program adherence or follow-up completion. Outcomes were analyzed using GEE models, which incorporate all available observations from each participant under an MAR assumption. This approach allows participants with partial follow-up data to contribute to estimates without list-wise deletion or imputation. Attrition (36.8%) was primarily due to disengagement or loss of contact rather than withdrawal or adverse events. Baseline characteristics did not differ significantly between completers (n = 115) and noncompleters (n = 67) across age, sex, comorbidity index, baseline psychological distress, or medication use (all P > 0.10). Sensitivity analyses restricted to completers yielded consistent results.
Results
Of 182 participants enrolled in the Pictou County PEP single-arm prospective interventional trial (median age, 60 years (interquartile range (IQR), 51–68); 85.2% female), all reported ≥1 chronic condition at baseline (Table 1). The most common were overweight/obesity (25.3%), type 2 diabetes (12.6%), hypertension (9.3%), arthritis (7.7%), and depression (4.4%). The median number of chronic conditions was 3 (IQR, 1–3); the median Charlson comorbidity index was 2 (IQR, 1–3). Most participants identified as white (96.2%) and heterosexual (92.3%); 60.4% had not completed university. Participants represented a range of socioeconomic backgrounds, with 20.9% reporting annual household incomes below CAD$50,000, 39% between CAD$50,000–99,999, and 30.2% ≥CAD$100,000; approximately half (49.5%) were employed, and half were retired or not working. Socioeconomic status, race, or sexual orientation were not inclusion or exclusion criteria, and no significant differences in engagement or adherence were observed across education, income, or employment categories (all P > 0.10). Median baseline body mass index was 32 (IQR, 27–38), with self-reported weight gain of ∼24 lb over 2 years. Follow-up assessments for the primary outcome (K10) were completed by 115 participants (63.2%) at both 6 and 12 months. Follow-up rates for secondary outcomes varied by time point (eTable 5 in the Supplemental materials). No serious adverse events occurred; six participants (3.3%) reported mild injuries (e.g. muscle strain or soreness).
Sample characteristics at baseline among 182 participants in the Pictou County PEP phase 2 trial who reported having at least one diagnosed chronic condition, from Pictou County, Nova Scotia, Canada.

PEP: personal empowerment program; IQR: interquartile range; BMI: body mass index; COPD: chronic obstructive pulmonary disease.
Primary outcome
Psychological distress, measured by the K10, decreased by 3.00 points (95% CI, −4.05 to −1.95; P < 0.001) at 6 months and by 3.60 points (95% CI, −4.84 to −2.36; P < 0.001) at 12 months, based on GEEs (Table 2). The model-estimated probability of screening positive for clinically significant distress (K10 ≥ 20) was 48% (95% CI, 36% to 60%) at baseline, 25% (95% CI, 16% to 38%) at 6 months, and 17% (95% CI, 10% to 28%) at 12 months. Sensitivity analyses using a ≥10-point threshold identified 5.2% responders at 6 months and 7.8% at 12 months (eTable 6 in the Supplemental materials). Using the predefined MCID of ≥7 points, responder rates were 18% (95% CI, 11% to 25%) at 6 months and 23% (95% CI, 15% to 30%) at 12 months. Responder status was not significantly associated with age, sex, baseline psychological distress, number of chronic conditions, or comorbidity index (all P > 0.10). Self-reported barriers to engagement included fluctuating physical health, competing life demands, and limited internet access (eTable 4 in the Supplemental materials), which may have contributed to variation in response magnitude.
Longitudinal changes in psychological distress (Kessler-10 scale) among 182 adults with chronic conditions in the Pictou County PEP trial at 6 and 12 months using generalized estimating equations.
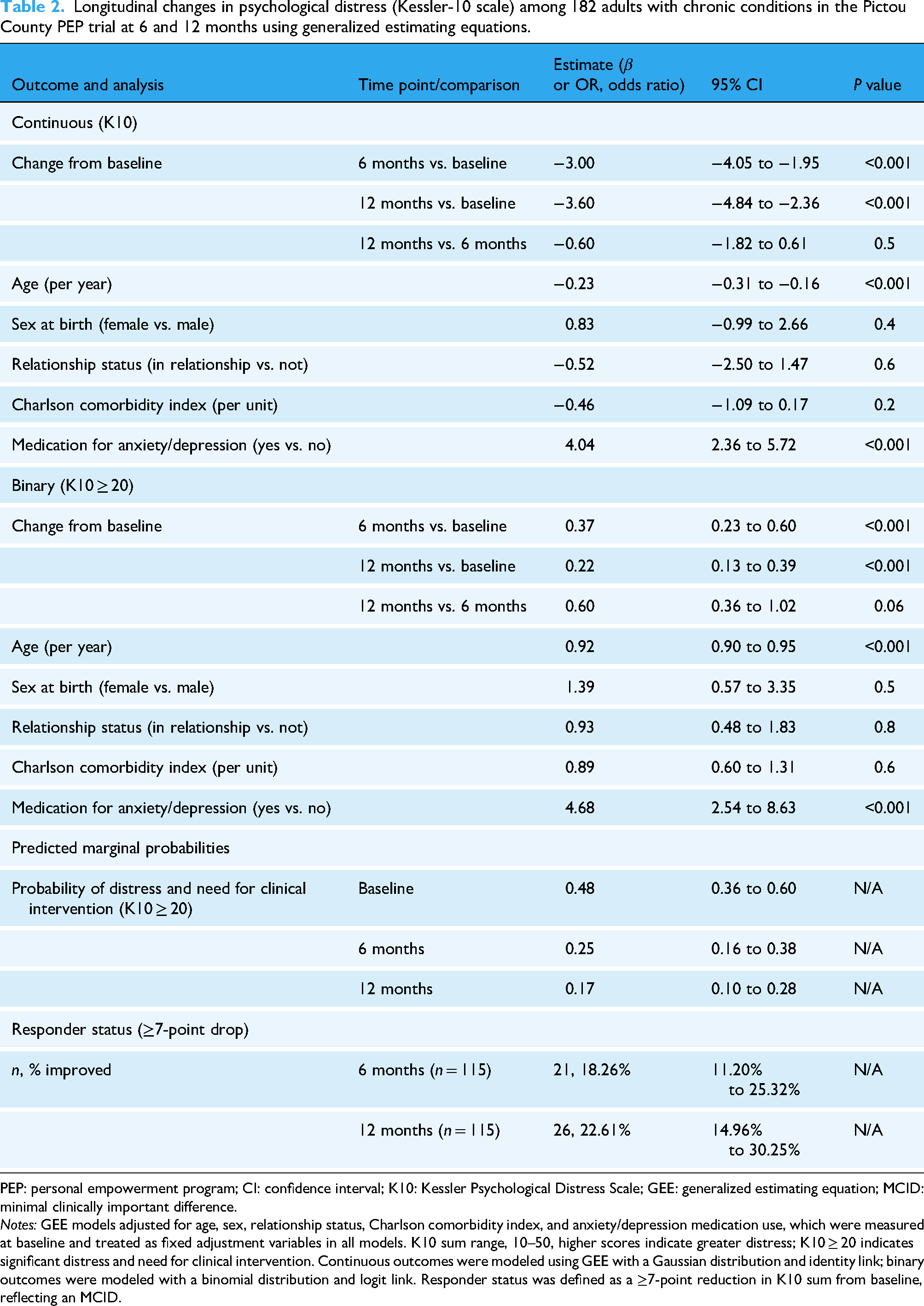
PEP: personal empowerment program; CI: confidence interval; K10: Kessler Psychological Distress Scale; GEE: generalized estimating equation; MCID: minimal clinically important difference.
Notes: GEE models adjusted for age, sex, relationship status, Charlson comorbidity index, and anxiety/depression medication use, which were measured at baseline and treated as fixed adjustment variables in all models. K10 sum range, 10–50, higher scores indicate greater distress; K10 ≥ 20 indicates significant distress and need for clinical intervention. Continuous outcomes were modeled using GEE with a Gaussian distribution and identity link; binary outcomes were modeled with a binomial distribution and logit link. Responder status was defined as a ≥7-point reduction in K10 sum from baseline, reflecting an MCID.
Secondary outcomes
GEEs showed reductions in anxiety (GAD-7) scores of 1.36 points (95% CI, −2.28 to −0.45; P = 0.001) at 6 months and 2.11 points (95% CI, −3.03 to −1.20; P < 0.001) at 12 months (Table 3). Predicted marginal means decreased from 6.1 (95% CI, 5.1 to 7.1) at baseline to 4.8 (95% CI, 3.7 to 5.8) at 6 months and 4.0 (95% CI, 2.9 to 5.1) at 12 months. GAD-7 responder rates (≥4-point reduction) were 22.8% (95% CI, 15.1% to 30.5%) at 6 months and 23.2% (95% CI, 15.4% to 31.0%) at 12 months.
Longitudinal changes in anxiety (GAD-7 scale) among 182 adults with chronic conditions in the Pictou County PEP trial at 6 and 12 months using generalized estimating equations.

GAD-7: Generalized Anxiety Disorder 7-item; PEP: personal empowerment program; CI: confidence interval; GEE: generalized estimating equation; MCID: minimal clinically important difference.
Notes: GEE models adjusted for age, sex, relationship status, Charlson comorbidity index, and anxiety/depression medication use, which were measured at baseline and treated as fixed adjustment variables in all models. GAD-7 sum range, 0–21, higher scores indicate greater anxiety symptoms. Results were modeled using GEE with a Gaussian distribution and identity link. Responder status was defined as a ≥4-point reduction in GAD-7 sum from baseline, reflecting an MCID.
Depressive symptoms, measured by the CES-D, decreased by 2.43 points (95% CI, −4.65 to −0.21; P = 0.028) at 6 months and by 4.31 points (95% CI, −6.84 to −1.78; P < 0.001) at 12 months (Table 4). Predicted marginal means declined from 15.3 (95% CI, 13.2 to 17.5) at baseline to 12.9 (95% CI, 10.6 to 15.2) at 6 months and 11.0 (95% CI, 8.7 to 13.3) at 12 months. CES-D responder rates (≥5-point reduction) were 31.8% (95% CI, 23.1% to 40.5%) at 6 months and 38.2% (95% CI, 29.1% to 47.3%) at 12 months. In sensitivity analyses using a ≥9-point threshold, 21.8% and 25.5% of participants were classified as responders at 6 and 12 months, respectively (eTable 6 in the Supplemental materials).
Longitudinal changes in depression (CES-D 20 scale) among 182 adults with chronic conditions in the Pictou County PEP trial at 6 and 12 months using generalized estimating equations.

CES-D: Center for Epidemiologic Studies Depression scale; PEP: personal empowerment program; CI: confidence interval; GEE: generalized estimating equation; MCID: minimal clinically important difference.
Notes: GEE models adjusted for age, sex, relationship status, Charlson comorbidity index, and anxiety/depression medication use, which were measured at baseline and treated as fixed adjustment variables in all models. CES-D range, 0–60, higher scores indicate greater depressive symptoms. Results were modeled using GEE with a Gaussian distribution and identity link. Responder status was defined as a ≥5-point reduction in CES-D sum from baseline, reflecting an MCID.
Program adherence and program ratings
Over the 26-week program, the mean number of submitted weekly adherence surveys per participant was 15.2 of 26 possible (58.3%). Participants viewed daily PEP videos or emails an average of 5.36 days per week (SD, 2.30), with weekly engagement meeting the compliance threshold (≥5 days/week) 74.4% of the time (SD, 34.4%) (eTable 3 in the Supplemental materials).
Among the program's core behavioral targets, mean weekly compliance was highest for intimacy-related behaviors (58.6%; SD, 38.3%), followed by strength training and/or yoga (48.2%; SD, 37.1%), aerobic activity (42.8%; SD, 36.4%), and healthy sleep practices (51.9%; SD, 37.9%). Meditation or relaxation techniques had the lowest adherence (29.0%; SD, 33.9%). Within the intimacy domain, physical intimacy showed the highest engagement (54.6%; SD, 41.0%), and recreational intimacy the lowest (28.8%; SD, 33.3%). Dietary behavior, assessed using the Starting the Conversation scale (range 0–16), had a mean score of 4.83 (SD, 1.96), indicating moderately healthy eating patterns.
At 6 months, the program's overall usefulness was rated 7.88 of 10 (SD, 2.32), and the likelihood of recommendation 8.52 (SD, 2.27). The perceived importance of PEP as a component of standard chronic care was rated 8.21 (SD, 2.21), and perceived lifestyle improvement was rated 7.23 (SD, 2.19). Among core content, dietary guidance (7.84; SD, 2.49), habit formation (7.65; SD, 2.50), and meditation (7.57; SD, 2.73) received the highest usefulness ratings, while intimacy content (6.90; SD, 2.62) and physical activity videos (6.98; SD, 2.75) were rated somewhat lower. Optional components such as yoga/Qi Gong (7.43; SD, 2.46; n = 56), monthly videoconferences (6.46; SD, 2.68; n = 57), and the private Facebook group (7.22; SD, 2.42; n = 95) were positively evaluated among those who engaged. The research team's competence was rated 9.18 (SD, 1.41), and responsiveness 7.89 (SD, 2.40). Interest in program continuation was expressed by 53.7% of respondents, and 3.3% reported mild injuries (eTable 4 in the Supplemental materials).
Qualitative feedback further contextualized these findings. Among the 45 participants who used the optional peer accountability feature, most described engaging in weekly motivational check-ins and sharing progress with their program partners. Participants cited enhanced commitment and reduced feelings of isolation as primary benefits of this feature (eTable 4 in the Supplemental materials). The 57 participants who attended monthly live video sessions engaged primarily in discussions about exercise technique, adapting routines to comorbidities, and maintaining motivation. Many used these sessions to connect socially with peers and program leads, reinforcing a sense of community and accountability. Together, these results support the feasibility, high digital engagement, and potential scalability of a low-bandwidth, multicomponent intervention for improving mental health outcomes among rural adults with chronic conditions.
Exploratory posthoc power analysis
To contextualize the achieved sample size in this feasibility trial, we conducted an exploratory posthoc power analysis based on the observed magnitude of change in psychological distress. Assuming a mean reduction in K10 scores of approximately 3 points, a standard deviation of 8, and modest within-participant correlation (ρ = 0.02), the enrolled sample (n = 182) provided approximately 98% power to detect this change at a two-sided α = 0.05. 46 Accounting for attrition, the retained sample with complete 6- and 12-month follow-ups (n = 115) provided approximately 89% power to detect the observed effect under the same assumptions.
For responder outcomes, the achieved sample size provided adequate power to detect the observed 12-month K10 responder rate of approximately 23% relative to a low baseline responder rate, although these analyses are presented descriptively. All power estimates are exploratory and posthoc and should be interpreted cautiously, as the study was not prospectively powered for hypothesis testing and these analyses were not prespecified in the study protocol.
Discussion
This study shows that a digitally delivered, home-based empowerment program can reduce psychological distress, anxiety, and depression in rural adults with chronic conditions. Clinically meaningful improvements were observed at 6 months for 18% (K10), 23% (GAD-7), and 32% (CES-D) of participants, with responder rates sustained or increasing at 12 months (23%, 23%, and 38%, respectively).36–39 These findings extend prior PC-PEP efficacy in prostate cancer to a multimorbid rural cohort. 23 The mean K10 reduction of 3.60 points at 12 months indicates durable benefit, an important outcome given the risk of worsening mental health with chronic disease. 6 Effects were statistically significant and exceeded accepted thresholds for clinical relevance.34–37 Recent meta-analyses (e.g. Silva et al., Snoswell et al.) similarly support moderate effects of multicomponent, digitally delivered interventions.16,19
The proportion of participants achieving clinically meaningful reductions in psychological distress (18% at 6 months; 23% at 12 months) compares favorably with responder rates of 15–25% reported in meta-analyses of digital interventions for chronic disease populations, where clinician support is often required for higher effects.16,19,34 The moderate responder rate observed here likely reflects contextual barriers rather than participant characteristics; exploratory analyses found no significant associations between responder status and age, sex, baseline distress, or comorbidity burden. However, qualitative feedback highlighted fluctuating health, caregiving demands, and intermittent internet access as common barriers to sustained engagement, underscoring the need for adaptive support mechanisms and digital equity strategies. The mean GAD-7 reduction of 1.36 points at 6 months and 2.11 points at 12 months, while below the individual-level MCID of ≥4 points, aligns with population-level mean changes typically observed in digital and community-based anxiety interventions for adults with chronic conditions.18,34,37 These sustained effects over 12 months (e.g. achieved without clinician-led therapy) suggest that even modest symptom reductions can be clinically meaningful when delivered at scale to populations with limited access to mental healthcare.
Digital design and accessibility
Designed for rural digital access, PEP integrates physical activity, nutrition, mindfulness, sleep, and social connection in a modular, asynchronous format consistent with chronic-disease self-management principles. The use of low-bandwidth video and email delivery targeted known access barriers in telehealth.21,22 The use of low-bandwidth-optimized videos and email-delivered content ensured accessibility regardless of internet quality, a critical barrier noted in telehealth literature.21,22 In settings where access to primary care is limited and emergency department use for mental health is elevated, PEP's remote, self-directed model offers a means of reducing reliance on in-person care and addressing gaps in rural mental health access.6,9,13 The observed reductions in psychological distress, anxiety, and depression reinforce the growing evidence that scalable, digital-first interventions can close access gaps while maintaining clinical impact, provided they are designed with digital equity in mind. 22 As Snoswell et al. noted in a systematic review of 38 meta-analyses, telehealth interventions are most effective when they incorporate structured, multidomain content and frequent patient engagement, elements which are central to the PEP design. 21
Practical measures were taken to mitigate common digital barriers in rural settings. All PEP videos were rendered in low-resolution formats to minimize buffering and data use, enabling smooth playback on older smartphones and low-speed internet connections. Content was hosted on YouTube and distributed via plain-text email links, ensuring universal accessibility without requiring specialized software or large file downloads. Participants could view materials asynchronously and replay them as needed, a feature frequently cited in feedback as essential for ease of use and engagement. For those with limited digital literacy, the research team provided individualized phone support to resolve access or navigation issues. Weekly surveys also included a space for reporting technical problems, which informed iterative refinements during implementation. These strategies helped bridge the digital divide, ensuring that even participants with minimal technological experience or unstable internet access could fully engage with the program.
Acceptability, engagement, and adherence in digital interventions
The high program ratings (usefulness: 7.88/10; likelihood of recommendation: 8.52/10) and a 53.7% interest in continuation underscore the acceptability of this digital approach. Follow-up attrition (37–39% across outcomes) is comparable to rates in long-duration digital behavioral trials without incentives. 47 Across the 26-week program, participants completed adherence surveys in 58.3% of weeks, with 74.4% meeting the compliance threshold for weekly video engagement. The program's integration into participants’ daily routines, even with variable internet access and without synchronous clinician support, supports its feasibility as a digital health model for chronic care management.
Adherence patterns (eTable 3 in the Supplemental materials) did not differ by age, education, or baseline health status. Meditation showed the lowest adherence (29.0%) yet high perceived usefulness (7.57/10), suggesting practical barriers despite perceived value. Participants commonly cited limited time, environmental distractions, or fatigue as reasons for incomplete engagement. These findings highlight the need for flexible delivery options and lighter-touch interventions within digital self-management programs. Future iterations of PEP will pilot shorter guided mindfulness sessions, optional reminders, and micro-practices embedded in daily routines to help participants sustain engagement with relaxation and stress-management content.
Digital prescription and value-based care
These findings suggest that digital programs like PEP could complement existing primary care by acting as “digital prescriptions” for patients with chronic disease and comorbid distress. Clinicians could recommend structured digital routines (e.g. ≥150 min/week aerobic activity and daily stress-reduction practices) within a digital prescription model to support incremental symptom reduction consistent with PEP outcomes. The scalability and asynchronous nature of the program also alleviate the need for costly digital peripherals or synchronous care, making it a cost-sensitive option for expanding access. This aligns with international recommendations to leverage patient activation and digitally enabled care to promote self-management and reduce healthcare utilization. 14
Beyond trial evaluation, the broader PEP ecosystem demonstrates feasibility for large-scale, value-based digital care. CancerPEP has transitioned from research to delivery as a nonprofit service, making the program accessible to patients across North America and New Zealand. PC-PEP has been adopted across Nova Scotia and internationally (pcpep.org). Building on these models, ongoing collaborations are underway with the Province of Nova Scotia to integrate the chronic-disease PEP into the provincial healthcare system as a free, publicly accessible digital service. This initiative, currently under development, aims to leverage existing commercialization infrastructure to sustain long-term delivery and growth. Together, these efforts underscore the potential for PEP to evolve from a clinical research intervention into a community-anchored, globally scalable model for equitable, digital-first chronic disease management.
Health economics and system integration potential
System-level adoption of PEP could yield substantial cost savings while improving outcomes. PC-PEP, a related intervention for men with prostate cancer, demonstrated healthcare savings of CAD$411.53 per participant at 6 months and CAD$660.89 at 12 months, while preventing approximately 30–31% of new cases of clinically significant psychological distress. 24 These results positioned PC-PEP as a dominant strategy in health economics, achieving superior clinical outcomes at reduced cost, which is an ideal outcome in cost-effectiveness modeling. If effects comparable to PC-PEP were realized, scaling to 1000 participants would imply direct savings on the order of CAD$0.4–0.7 million over 12 months, based on PC-PEP trial estimates and local service-use profiles. 24
A formal cost-effectiveness analysis of Pictou County PEP is now underway, adopting a public-payer perspective with linked administrative billing and hospital discharge data over a 12-month analytic horizon, with sensitivity analyses extending to 24 months. The analysis will estimate incremental cost-effectiveness ratios (cost per quality-adjusted life year gained, derived from validated health-related quality-of-life measures) and quantify changes in healthcare utilization, including primary-care, emergency, and inpatient services, as well as medication expenditures. Bootstrapped uncertainty analyses and subgroup evaluations will assess robustness and equity-adjusted cost-effectiveness across rural and lower-income populations.
These results will inform policymakers on the fiscal and population-health impact of scaling digital mental-health interventions within value-based care frameworks. This aligns with federal and provincial mandates for equitable, cost-effective, digitally enabled care.5–7,10 Moreover, the PEP's modular structure, asynchronous delivery, and independence from costly digital peripherals (e.g. heart rate variability monitors) enhance its scalability and feasibility across geographic and demographic groups with diverse chronic disease burdens. Snoswell et al. emphasized that digital programs embedded into broader health systems and supported by self-monitoring infrastructure produce the greatest returns on investment, a design principle we adopted in this trial. 21 Digital interventions like PEP not only address treatment gaps but also advance equity by delivering accessible, affordable care to patients in low-resource, high-need areas.19–22
Patterns of engagement and digital optimization
Program adherence patterns offer further insight into participant engagement and potential areas for refinement. Participants engaged most consistently with connection-focused (intimacy, 58.6%), strength and yoga (48.2%), and aerobic activity (42.8%) components. Despite relatively low adherence to meditation (29.0%), it was among the highest-rated components (7.57/10), suggesting a perceived benefit but possible barriers to implementation. These findings underscore the importance of tailoring interventions to participant preferences and exploring strategies (e.g. enhanced guidance, personalization, or integration into existing routines) to improve engagement with lower-adherence components. Engagement with dietary and sleep practices was moderate. However, the 74.4% average engagement with daily video and email content indicates that the delivery format was well-suited to rural adults with chronic conditions. Future digital refinements may include optional push notifications, micro-learning modules, or artificial intelligence-driven personalization to enhance engagement in lower-uptake areas. Such adaptivity aligns with recent best practices in digital health usability, especially in rural or aging populations with limited digital literacy. Future refinements may include optional reminders, micro-learning modules, and personalization to bolster engagement in lower-uptake areas, implemented within robust privacy and data-governance frameworks.
Lower usefulness ratings for physical activity and intimacy modules point to targets for optimization. As indicated in eTable 4 in the Supplemental materials and accompanying qualitative feedback, participants reported fluctuating physical health, fatigue, physical limitations, and limited home exercise space as barriers to exercise videos. Similarly, some participants reported discomfort or limited perceived relevance of intimacy-focused content, particularly those living alone or not in active relationships. These findings suggest that tailoring future iterations of PEP to include graded physical activity options, adaptive intensity levels, and opt-in intimacy modules with broader relational framing may enhance inclusivity and perceived usefulness. Usefulness ratings likely capture perceived value rather than the frequency of engagement. High ratings for meditation despite lower adherence may indicate that participants recognized its benefit even if they practiced it less often. Future evaluation tools will separate perceived usefulness from enjoyment to clarify motivational versus experiential responses. As in other domains of behavior change, effortful practices may yield deeper benefit despite initial discomfort.26–28 Communicating this to participants with empathy and clarity, emphasizing that improvement often involves challenge, will be central to future program refinement.
Although the present trial was not powered to isolate the relative contribution of each behavioral domain, qualitative feedback from this and prior PEP cohorts suggests that participants valued the program's multifaceted design as central to sustaining engagement. 48 Many reported that single-domain interventions (e.g. exercise or diet alone) had been difficult to maintain in the past, whereas PEP's combination of daily activities across movement, nutrition, mindfulness, and connection allowed them to choose and prioritize what best fit their needs. This theme has been repeatedly documented in qualitative evaluations of PEP programs and echoed in prior qualitative evaluations. 48
Positioning within the digital health landscape
To our knowledge, PEP is among the longest-duration, home-based, multifaceted digital interventions evaluated for adults with chronic conditions, combining scope, intensity, and sustainability. Unlike conventional chronic disease self-management programs, which frequently target a single health behavior (e.g. physical activity, nutrition), this 6-month program concurrently addresses five key domains essential to chronic disease management: physical activity, whole-food nutrition, stress reduction, sleep hygiene, and social connection with daily digital touchpoints. Delivered daily and supported by weekly monitoring, peer accountability and optional monthly live video conferences (which continued beyond the formal intervention period and remain ongoing), PEP was designed to foster sustainable behavior change across interrelated health domains. Clinically, this whole-person approach aligns with the growing recognition that multimodal interventions are essential to meaningfully impact the physical and mental health burden experienced by patients with multiple chronic conditions, particularly in rural settings where access to care is limited.6–7,10,49
Compared with other long-duration digital interventions such as Silva et al., which reported moderate psychological improvements in multibehavioral programs averaging 8–12 weeks, and Snoswell et al., which reviewed 38 meta-analyses of telehealth programs rarely exceeding 3 months, PEP stands out for its 6-month continuous engagement and multidomain behavioral scope.18,21 The program's integration of daily physical activity, mindfulness, nutrition, sleep, and connection content surpasses the typical single-domain focus of most digital chronic disease interventions. Its combination of asynchronous and live elements provides a replicable blueprint for other chronic conditions, allowing modular adaptation as for example, substituting cancer-specific content or cardiovascular risk modules within the same behavioral framework. This high-frequency delivery exceeds the minimum contact standards recommended in digital self-management interventions and reflects best practice for behavior change reinforcement.50,51 Recent systematic reviews consistently identify the lack of integrated, long-duration, and engagement-rich digital tools for chronic conditions which is a gap PEP directly addresses.13,51
Findings from recent systematic reviews and meta-analyses reinforce the rarity and potential significance of such comprehensive approaches. Allegrante et al. found that most behavioral self-management interventions lacked sustained delivery and typically addressed only one or two health behaviors. 50 Silva et al. conducted a systematic review of multibehavior change programs, reporting moderate effect sizes. However, they noted that most trials lacked long-term follow-up or ongoing post-intervention support, were brief, focused on single behaviors, and were poorly integrated into broader care systems. 18 Similarly, Farris et al. reported limited psychological impact and duration in chronic disease interventions, particularly among dialysis patients, with the majority lasting fewer than 3 months, with no daily continuous engagement component. 51 One 6-month program cited in the review did not entail daily contact; it provided periodic peer group sessions and education, and was considered an outlier in duration. PEP addresses these critical gaps by combining extended duration, breadth of behavioral targets, continuous engagement tools, and post-intervention support infrastructure. This modular architecture facilitates adaptation for various chronic diseases and healthcare settings, enabling integration into existing digital care platforms while maintaining fidelity to core behavioral and psychological components.
Clinical implications
The Pictou County PEP represents an innovative model for addressing mental health in adults with chronic conditions, particularly those in rural and underserved settings. Its daily, home-based digital format delivered over 6 months is, to our knowledge, without precedent in the chronic disease literature. Recent reviews consistently identify the absence of long-duration, high-frequency behavioral interventions as a critical gap in current practice. This delivery model is especially well-suited to individuals with limited access to in-person care, whether due to geography, transportation, or mobility limitations, thereby advancing equity in mental healthcare access. 9
Sustained improvements at 12 months likely reflect the program's design features that promote ongoing engagement, social reinforcement, and community ownership. Many participants reported continuing to use PEP videos, mindfulness practices, and daily behavioral routines after completing the 6-month intervention. Monthly live videoconference sessions have been maintained and are expected to continue indefinitely, providing a stable forum for connection, accountability, and shared learning. The platform remains open to allow the program to grow organically within the community, with early participants increasingly taking on peer-mentor roles for new enrollees. This continuity of support, combined with the program's emphasis on habit formation, attitudinal healing, and intrinsic motivation, likely underpins the sustained psychological benefits observed at 1 year, a rare outcome among digital self-management interventions for chronic disease populations.
Although this sample was predominantly female, prior PC-PEP and CancerPEP trials demonstrated comparable responder rates among men, suggesting that engagement rather than sex-linked responsiveness may drive outcomes. Recruitment of male participants in community-based behavioral trials remains challenging due to cultural norms around help-seeking and self-care. Future PEP implementations will use tailored recruitment strategies, peer mentorship, and gender-specific framing to enhance male participation and ensure balanced representation.
For primary care physicians, the integration of PEP or similar programs into routine practice offers a pragmatic, evidence-informed strategy to support behavioral health. Structured behavioral prescriptions, such as 150 min of weekly aerobic activity, as modeled in PEP, may reduce psychological distress by 20% to 30%, based on our findings. At the system level, PEP has potential as a population health intervention, with implications for reducing mental health-related emergency department visits and inpatient utilization in patients with chronic disease.6,7
Preliminary economic data from the related PC-PEP trial demonstrated significant healthcare savings (up to CAD$660.89 per participant over 12 months) alongside improvements in psychological distress. 24 If replicated in broader populations, such outcomes could translate into millions of dollars in cost savings annually. A formal cost-effectiveness analysis of the Pictou County PEP is underway and will provide additional guidance for policymakers and payers. The program's modular structure, asynchronous delivery, and emphasis on patient activation align with federal and provincial priorities for value-based, digitally enabled, and scalable chronic disease care. Early economic modeling suggests that widespread implementation of digital mental health interventions could reduce system-wide mental health-related healthcare costs by 10% to 15% annually, although further evaluation is needed. 24
Implementation and policy implications
The Pictou County PEP provides a compelling model for policy and digital health integration. Its asynchronous, modular structure supports embedding into virtual care ecosystems, patient portals, or provincial telehealth infrastructure. It is device-agnostic, requires no specialist personnel for delivery, and uses freely available platforms (e.g. YouTube, email), enhancing scalability. Integration with existing provincial and federal digital health strategies aligns with ongoing initiatives such as Canada's Framework for Digital Health Equity and Nova Scotia's VirtualCareNS expansion. PEP's asynchronous and low-bandwidth format makes it compatible with these systems, allowing delivery through patient portals or telehealth infrastructure without additional hardware or proprietary software. However, challenges remain, particularly in regions with limited broadband connectivity or low digital literacy. Addressing these barriers may involve partnerships with public libraries, community health centers, and primary-care networks to facilitate onboarding and provide optional digital literacy support. Lessons from successful telehealth programs in other provinces suggest that sustained mentorship, local champions, and integration into primary-care workflows are key to equitable implementation and uptake. These considerations will guide the program's next phase of provincial integration and national scale-up planning. As digital therapeutics grow in acceptance globally, models like PEP offer low-cost, high-reach solutions aligned with provincial and federal strategies for mental health equity and chronic disease care. This program also exemplifies how low-tech digital tools can yield high-impact outcomes, which is an insight increasingly valuable in global digital health planning.
Limitations
This single-arm prospective interventional trial limits causal inference. Although attrition was comparable to similar interventions, 49 differential dropout could bias results. The sample was predominantly white and female, which may limit generalizability. Engagement measures were self-reported and susceptible to social desirability bias; however, validated instruments and ITT-consistent modeling mitigate some concerns. Future studies should aim to improve representativeness by recruiting from more diverse geographic and demographic populations, including urban, Indigenous, Black, and immigrant communities. Oversampling from underrepresented groups and collaborating with community-based organizations may enhance reach and cultural relevance. Additionally, targeted retention strategies, such as proactive check-ins, flexible survey completion options (e.g. phone or paper-based), and enhanced digital support, could reduce attrition among participants with higher baseline distress or lower digital literacy. These adaptations will strengthen generalizability and minimize potential attrition bias in subsequent trials.
Future directions
Randomized trials are needed to confirm efficacy and explore mechanisms of action. Cost-effectiveness analyses using linked billing data are ongoing. Adapting PEP for cultural and linguistic diversity will enhance equity and reach. Integration with electronic health records (EHRs) or virtual care platforms could facilitate clinical implementation. Future studies should evaluate implementation in diverse populations and health systems. Ongoing cost-effectiveness evaluation and integration into EHRs will support scalability. Longitudinal studies beyond 12 months will help quantify sustained impact on healthcare utilization and mental health burden.
Priority adaptations now underway include French-language and Mi’kmaw versions for Atlantic Canada and versions codeveloped with Indigenous, Black, and immigrant communities across Canada. We are actively engaging with Nova Scotia Health's VirtualCareNS and Digital Health Strategy teams to explore secure integration with EHRs and provincial virtual care platforms through application programming interfaces, data-sharing agreements, and alignment with existing privacy frameworks. Such interoperability would enable clinicians to refer patients directly into PEP and view progress metrics within EHRs. Future iterations of the program will be delivered through PEPLife, a digital platform currently under development to support sustained, scalable, and equitable implementation across diverse healthcare settings. Longitudinal follow-up beyond 12 months will assess the sustainability of mental health improvements, long-term healthcare utilization trends, and factors influencing continued engagement, including motivation, digital access, and evolving health needs. These data will inform scalable models for sustained digital health engagement and population-level impact.
Conclusions
The Pictou County Patient Empowerment Program (PEP) significantly reduced psychological distress, anxiety, and depression in rural adults with chronic conditions, with effects sustained or improved at 12 months. These clinically meaningful improvements, including reliable change in distress for 18% of participants and in depressive symptoms for up to 38%, highlight the program's potential to address persistent mental health disparities in rural and underserved populations.
PEP's digitally delivered, home-based format offers a scalable model for integrating behavioral health into chronic disease care. By combining daily engagement in physical activity, nutrition, stress reduction, sleep, and connection, PEP supports patient activation and self-management, principles central to value-based care. PEP's combination of daily engagement, multicomponent behavioral targets, and asynchronous digital delivery supports its promise as a model for digitally integrated chronic disease care. Its alignment with healthcare priorities and demonstrated acceptability position it as a promising strategy to extend mental health support beyond clinical settings.
Further validation through randomized trials and health economic evaluation is warranted. Adaptation for culturally and linguistically diverse populations, along with integration into digital health infrastructure, could enhance reach and equity. PEP offers a sustainable, evidence-informed solution to the growing mental health burden among individuals with chronic disease, particularly in settings where access remains limited.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076251413351 - Supplemental material for Digital delivery of a 6-month home-based empowerment program improves mental health in rural adults with chronic conditions: A single-arm prospective interventional trial
Supplemental material, sj-docx-1-dhj-10.1177_20552076251413351 for Digital delivery of a 6-month home-based empowerment program improves mental health in rural adults with chronic conditions: A single-arm prospective interventional trial by Gabriela Ilie, Stuart Murphy, Cody MacDonald and Robert David Harold Rutledge in DIGITAL HEALTH
Supplemental Material
sj-pdf-2-dhj-10.1177_20552076251413351 - Supplemental material for Digital delivery of a 6-month home-based empowerment program improves mental health in rural adults with chronic conditions: A single-arm prospective interventional trial
Supplemental material, sj-pdf-2-dhj-10.1177_20552076251413351 for Digital delivery of a 6-month home-based empowerment program improves mental health in rural adults with chronic conditions: A single-arm prospective interventional trial by Gabriela Ilie, Stuart Murphy, Cody MacDonald and Robert David Harold Rutledge in DIGITAL HEALTH
Footnotes
Acknowledgments
This study was funded by the Aberdeen Health Foundation. The authors gratefully acknowledge all members of the Foundation's Board, as well as Ms Michelle Ferris, Executive Director, for their support to this work. The authors also acknowledge the support of Mr and Mrs Frank and Debbi Sobey, whose generosity supports the endowed academic position that enabled the broader development of this research. The study was conducted with the support of Dalhousie University and the Faculty of Medicine, which provided the academic and research environment for this work. The authors also thank the Pictou County community, local clinicians, and all program participants for their engagement, time, and commitment.
Ethical considerations
Ethical approval was obtained from the Nova Scotia Health Authority Research Ethics Board (NSHA REB), reference number: 1029744.
Author contributions
GI: conceptualization, data curation, formal analysis, funding acquisition, investigation, methodology, project administration, resources, software, supervision, validation, visualization, writing—original draft, and writing—review and editing.
SM: validation, visualization, formal analysis, writing—original draft, and writing—review and editing.
CM: methodology, data curation, formal analysis, investigation, project administration, software, validation, and writing—review and editing.
RDHR: conceptualization, funding acquisition, investigation, methodology, project administration, resources, supervision, validation, and writing—review and editing.
All authors had full access to all the data in the study and had final responsibility for the decision to submit for publication.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Aberdeen Health Foundation and the Dalhousie University Faculty of Medicine.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
Deidentified data are available upon request to the corresponding author, subject to institutional policies and a data access process in compliance with patient privacy and research protection regulations (NSHA Research Ethics Board).
Guarantor
Gabriela Ilie.
Role of funder/sponsor
The funders had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; or decision to submit the manuscript for publication.
Trial registration
ClinicalTrials.gov identifier: NCT06064110.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.