
Abstract
Objective
To develop a clinical nursing decision support system for pressure injury and explore its application in managing pressure injury in postoperative cardiac surgery patients.
Methods
A multidisciplinary research team was formed to develop a clinical nursing decision support system. Key indicators, including wound assessment accuracy, wound treatment accuracy, pressure injury healing rate, pressure injury incidence, and defect rates in nursing records, were compared before and after the clinical nursing decision support system utilization. Count data were described using frequency and composition ratio (%), and comparisons were made using the chi-square test or Fisher's exact probability method. Measurement data following a normal distribution were described by mean and standard deviation, while non-normally distributed data were described by median and interquartile range. Independent sample t-tests and rank-sum tests were used for between-group comparisons. A significance level of α = 0.05 was set, with results considered statistically significant if P < 0.05.
Results
The clinical nursing decision support system implements an intelligent decision-making engine and interactive dashboard for human–computer interaction, enabling intelligent assessment and decision-making, re-evaluation reminders, interactive modules, intelligent auditing, and a three-level quality control system for pressure injury. After applying the clinical nursing decision support system, the pressure injury incidence in postoperative cardiac surgery patients decreased from 14.8% to 12.8%, with no statistically significant difference (P > 0.05). The pressure injury healing rate increased from 89.1% to 97.2%, wound assessment accuracy improved from 90.8% to 97.2%, and wound treatment accuracy increased from 88.3% to 96.5%. The defect rate in nursing records decreased from 15.3% to 7.7%, with all differences being statistically significant (P < 0.05).
Conclusion
This study successfully developed and implemented a clinical nursing decision support system for pressure injury management in postoperative cardiac surgery patients. These results confirm the system's clinical utility in standardizing pressure injury care, optimizing nursing workflows, and elevating documentation quality. The clinical nursing decision support system provides an effective tool for enabling evidence-based, personalized interventions and strengthening closed-loop quality control in pressure injury management.
Keywords
Introduction
Pressure injury: The hidden crisis in global healthcare systems
Pressure injury (PI) refers to localized skin and/or underlying tissue damage caused by pressure or pressure combined with shear forces, typically occurring over bony prominences and sometimes associated with medical devices or other objects. 1 PI is a global health issue faced by healthcare systems worldwide. The results of an epidemiological survey that collected data on 13,254 patients in 1117 ICUs in 90 countries showed an overall prevalence of ICU stress injuries of 26.6% and an ICU-acquired prevalence of 16.2%. 2 Additionally, there were significant differences between the hospital-acquired PI prevalence of intensive care versus non-intensive care patients. 3 Large-scale, multicenter cross-sectional studies in China have shown that the prevalence of PI among hospitalized patients ranges from 1.67% to 1.79%.4,5 In China, the incidence of hospital-acquired PI has become a key indicator for evaluating nursing quality. 6 In addition to the burden of pain, infection, and death, it is estimated that hospital-acquired PI costs the health system $26.8 billion annually, with over 50% of the cost attributed to treating Stages 3 and 4 pressure injuries. 7 Therefore, the effective prevention of this complication has become an urgent challenge for the global medical community to solve.
Cardiovascular disease and PI: A serious challenge under a double burden
The 2019 Global Burden of Disease Study revealed that there were 523 million cardiovascular patients worldwide, with cardiovascular disease being the leading cause of death globally, accounting for 32.92% of all deaths. 8 In China, from 2009 to 2019, the mortality rate of cardiovascular disease among residents showed an overall upward trend, indicating that cardiovascular disease remains a major public health issue threatening the health of the Chinese population. 9 Surgical intervention is a critical treatment for complex cardiovascular diseases. The long duration of cardiac surgery, the large fluctuation of intraoperative temperature, the use of vasoactive drugs, and the need for extracorporeal circulation, coupled with the perioperative routine clinical pathway of cardiac surgery patients for the ward-operating room-cardiac surgery intensive care unit (CSICU)-ward, the route involves two high-risk departments, so PI is a common perioperative complication in cardiovascular surgery patients. A meta-analysis has shown that the incidence of intraoperative acquired pressure injuries in open-heart surgical patients can reach 25%. 10 This complication seriously hampers post-operative recovery and even triggers a chain of medical risks. However, the current PI prevention for this high-risk group has certain deficiencies. Routine care relies on generic assessment tools such as the Braden Scale, which fail to incorporate risk parameters specific to cardiac surgery; moreover, the psychometric properties of the Braden Scale prove inconsistent in intensive care unit settings. 11 Concurrently, there exists no specialized nursing decision support system that provides real-time early warning and intervention guidelines based on factors exclusive to cardiac surgery. Therefore, the development of PI decision support tools adapted to the pathophysiological characteristics of cardiac surgery patients has become an urgent need for the realization of precision care.
Enabling precision care: Clinical nursing decision support systems
The prevention of PI and the quality of care depend on nurses’ experience and accurate knowledge. 12 However, studies have shown that gaps in nurses’ knowledge and skills related to identification and staging of PI, heavy nursing workload and inadequate staffing levels, prevent nurses from making decisions to prevent nosocomial PI in accordance with the recommendations of PI management guidelines and clinical judgment. 13 Healthcare information technology integrated into clinical workflows—clinical nursing decision support systems (CNDSS)—can guide nurses in decision-making and adherence to recommended guidelines. CNDSS are based on evidence-based nursing practices, collecting and analyzing patient information, integrating it with a clinical decision knowledge base, and clearly defining nursing goals and interventions. This enables the development of scientific, individualized care plans and assists nurses, especially less experienced ones, in making quick, accurate, and effective decisions during the nursing process. 14
Diogo et al. 15 developed the PROCEnf-USP Clinical Decision Support System, which supports decision-making and enables nurses with varying educational backgrounds and professional experience to make clinical decisions with medium to high accuracy. This demonstrates that CNDSS serve as a strategy to bridge gaps in clinical decision-making abilities arising from differences in cognitive skills and professional expertise. In the field of cardiovascular disease, CNDSS can provide effective support from early warning, diagnosis, treatment decision-making, to risk assessment and pharmacological management. 16 In specific nursing domains, the development and application of CNDSS in intensive care units have primarily focused on clinical nursing issues such as critical value management, nursing risk management, airway management, and nurse handover management. 17
However, there are limitations of the existing CNDSS in PI management after cardiac surgery. At the present time, the generalized CNDSS does not integrate cardiac surgery-specific risk parameters and is unable to accurately warn of PI. The early system fails to achieve structured and intelligent assessment of PI staging and relies on manual descriptions of wound characteristics. Additionally, decision support in CSICU scenarios mostly focuses on a single link, such as critical value management, and lacks a full-process management covering PI risk prediction → graded intervention → healing tracking in cardiac surgery patients.
Chinese research and development on CNDSS: emerging explorations and applications
In 2020, Xia et al. utilized CNDSS to assess PI's staging, achieving dynamic evaluation alerts, intelligent interpretation recommendations, and real-time monitoring and analysis, providing nurses with accurate and objective decision support. This improved the quality of care and management efficiency. 18 However, this study did not achieve structured or intelligent staging assessments for PI. In 2022, Zhou et al. 19 developed an automated, intelligent, and information-based PI decision-making platform, incorporating risk management and wound management for PI. This platform employs a structured assessment model to evaluate wound location, size, color, exudate, and staging in detail, supplemented by intelligent decision-making to provide personalized nursing interventions. However, research on CNDSS in China is still in the initial stages of exploration—whether addressing a single problem or integrating multiple domains. However, the potential for its application in critical care is beginning to emerge.
This study addresses the unique needs of PI management for cardiac surgery patients and builds a specialized decision support system. Exclusive prediction model for cardiac surgery: based on 12 cardiac surgery variables such as intraoperative mean arterial pressure, duration of mechanical ventilation, and epinephrine dosage; Structured-intelligent full-process management: to achieve closed-loop management from risk prediction (immediate postoperative) → graded intervention → tertiary quality control → healing tracking; Human–computer interaction optimization: to dynamically push warnings of high-risk patients to the nursing terminals through an intelligent dashboard.
We seek to answer the following questions:
How can a CNDSS be specifically developed to support the prevention and management of pressure injuries (PI) in postoperative cardiac surgery patients? What is the impact of implementing this PI-specific CNDSS on key nursing and patient outcomes related to PI care in postoperative cardiac surgery patients?
Method
Study design and setting
A randomized controlled trial was not feasible due to the institutional policy of implementing the new decision support system as a quality improvement initiative. Therefore, a quasi-experimental before-after design was adopted to evaluate the system's impact. The reporting of this quasi-experimental study follows the Transparent Reporting of Evaluations with Nonrandomized Designs statement. Furthermore, to ensure complete transparency of the artificial intelligence (AI) component of the clinical decision support system, relevant items from the CONSORT-AI extension have been incorporated into the methodology and results reporting. This study was conducted at a tertiary specialized hospital in Tianjin, China, which admits nearly 60,000 patients and performs nearly 7000 surgical procedures throughout the year.
System development process
A multidisciplinary research team was established, comprising 10 members from various fields. The team included two nursing management personnel (associate senior titles), four wound care team nurses (two with associate senior titles), one network management center staff member (senior engineer), and two software engineers, all team members are from the hospital. The CNDSS for PI is a knowledge-based network architecture. Its framework consists of three main components: a knowledge base, an inference engine, and a human–computer interaction module. The system development consists of three stages (Figure 1).

The study process of the CNDSS for PI in postoperative cardiac surgery patients.
In the early stages of this study, an evidence-based nursing approach was adopted to conduct a comprehensive search of expert consensus, guidelines, journal articles, relevant documents, materials, and research reports on PI nursing care both domestically and internationally. Evidence assessment sessions and analysis of user needs were conducted using a focus group discussion format with 12 panelists, including two nursing management specialists, two CSICU nurse managers, four CSICU clinical nurses, and four wound care team nurses. The panelists comprehensively assessed the feasibility, appropriateness, clinical significance, and effectiveness of evidence translation and identified system functionality, taking into account the clinical situation of CSICU, existing departmental conditions, and the preferences of patients and their families. Using hospital data, a risk prediction model for postoperative PI in CSICU patients undergoing cardiac surgery was constructed, leading to the preliminary development of the clinical nursing decision support knowledge base for postoperative PI. The Delphi expert questionnaire was employed, involving two rounds of questionnaires, feedback, and revisions. Ultimately, this process resulted in forming the clinical nursing decision support knowledge base for PI in postoperative cardiac surgery patients.
The risk prediction model
The risk prediction model was developed using retrospective data from 2580 cardiac surgery patients admitted to our CSICU in 2022. Initially, 27 potential predictor variables were considered based on clinical relevance and literature review. These variables underwent univariate analysis, and those with a p < 0.1 were included in the multivariable logistic regression analysis using a stepwise selection method. The final model included 11 variables, as presented in Table 1. The model's performance was evaluated on a hold-out validation set (30% of the data). Discrimination was assessed by the area under the receiver operating characteristic curve (AUC), which was 0.735 (95% confidence interval (CI) [0.692, 0.779]). Calibration was assessed using the Hosmer–Lemeshow goodness-of-fit test (χ2 = 11.804, p = 0.160), indicating no significant deviation between predicted and observed probabilities. The risk stratification thresholds (green: <1%, yellow: 1–2%, orange: 2–5%, red: ≥5%) were determined by balancing clinical utility and the model's predicted probabilities using Youden's index.
Definition of variables.

CSICU: cardiac surgery intensive care unit.
In this case, the formula of the predictive model for the risk of postoperative PI in CSICU patients undergoing cardiac surgery was: ln(p/1 − p) = −6.210 + 3.865 × X1 + 0.701 × X2 + 0.010 × X3 − 0.007 × X4 − 0.038 × X5 + 0.037 × X6 + 0.032 × X7 + 0.012 × X8 − 0.043 × X9 − 0.104 × X10 + 0.036 × X11. The definition of variables is shown in Table 1.
The patients’ risk class was determined according to the risk value of PI: no risk (green), 0 ≤ risk value <1%; low risk (yellow), 1% ≤ risk value <2%; medium risk (orange), 2% ≤ risk value <5%; high risk (red), risk value ≥5%; and occurred (purple).
Patients were matched with appropriate nursing measures according to their PI risk level: 0 ≤ risk value < 2%, basic management strategy; 2% ≤ risk value < 5%, primary management strategy; risk value ≥5%, secondary management strategy.
The frequency of assessment is judged according to the patient's risk level of PI: when the PI is high risk or has occurred, it is assessed every 12 h; when the PI is medium-risk or less, it is assessed every 3 days; patients who are newly admitted to the department or who have a change in their condition need to be assessed immediately.
If PI has occurred, it will be treated according to the treatment measures established by the Tianjin Nursing Quality Control Center, which is shown in Table 2.
Measures for the treatment of stages of pressure injuries.

PI: pressure injury.
System architecture and function
System architecture
The CNDSS system developed in this research adopts server/customer service (Client/Server, C/S) mode as its operating environment, C# as its development language, Oracle19c as its database, domain-driven design as its guiding ideology, micro-services as its technical means, DevOps as its delivery guarantee to realize the loose coupling between modules, and based on the ESB (Enterprise Service Bus), it realizes standard exchanges between heterogeneous business systems. The engineers first use data warehouse technology (Extract-Transform-Load) to extract patient medical information from the hospital clinical data center, transform it into the data structure of this system, and store it in the database, embed the logistic regression model into the system through Predictive Model Markup Language (PMML), and construct the clinical auxiliary decision support system based on the Drools rule engine. All data is analyzed, filtered, cleansed, and integrated, enabling intuitive, clear, and dynamic human–computer interaction through an intelligent dashboard display. Additionally, the system can issue nursing task assignments and generate task lists to assist nurses in executing clinical nursing duties effectively.
The system is embedded within the electronic nursing documentation system. The framework of the CNDSS is shown in Figure 2, and the CNDSS module is shown in Figure 3.
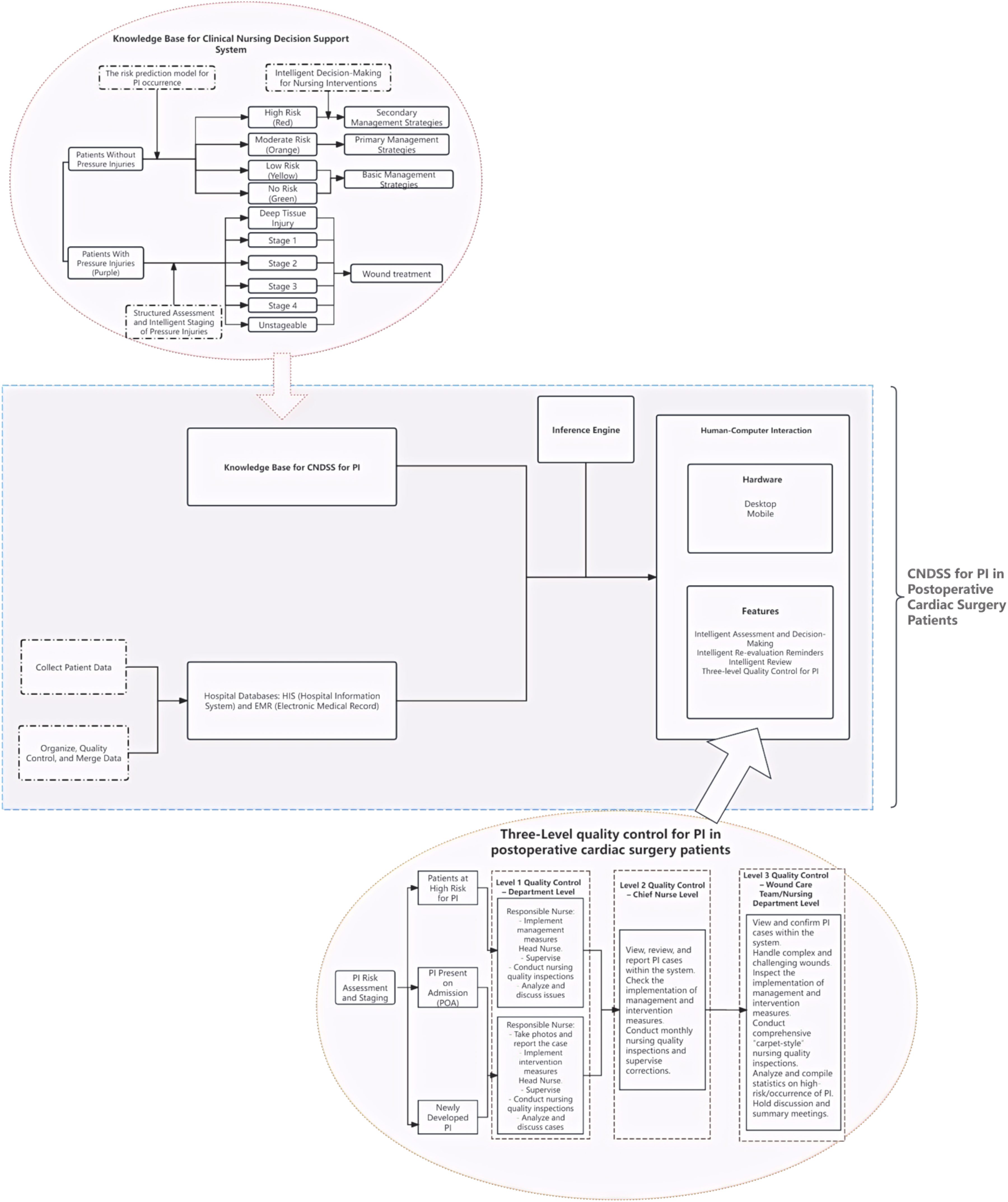
Framework of the CNDSS for PI in postoperative cardiac surgery patients.

The CNDSS module for PI in postoperative cardiac surgery patients.
System function
Intelligent assessment and decision-making
The system automatically retrieves data to assess patients who have not yet developed PI. A postoperative PI risk prediction model for cardiac surgery patients determines the risk of developing PI. Based on the risk level, the system automatically recommends preventive management strategies for PI. For patients who develop PI during hospitalization, the system automatically matches the appropriate level of intervention measures. The department can request a nursing consultation after discussion for complex and challenging wounds, such as Stage 3, Stage 4, or unstageable injuries. An electronic nursing consultation form is submitted to the hospital's wound care team.
Intelligent re-evaluation reminders
After nurses conduct PI risk predictions or staging assessments for patients, the system integrates an evaluation reminder function based on the timing requirements, evaluation frequency, and stratification of PI risk levels. The system automatically generates pending evaluation time points displayed on the nursing assessment interface to remind nursing staff to conduct timely evaluations.
Intelligent human–computer interaction module: Designed based on the intelligent dashboard concept
The system's human–computer interaction interface has two components: real-time static electronic dashboard interaction and dynamic rule-based reminders and alerts. The static electronic dashboard interaction consists of two dimensions: Ward Level: Patient information is presented in summary card format. By logging into the ward overview interface, nurses can clearly view key information about the entire ward from a nursing perspective, facilitating efficient access to valuable real-time data. More detailed information can be accessed by drilling down or hovering the mouse over a specific patient's card. Individual patient level: Key patient information is visually displayed, allowing nurses to immediately grasp critical details when providing care. The reminder and alert interaction is primarily driven by the system's knowledge base, which generates judgments and pushes the results to relevant medical staff's computers or personal digital assistants (PDAs) according to preset rules. Different alert or reminder methods are used to facilitate interaction.
Intelligent review
The system incorporates an image upload function, allowing for a multi-level review process involving individual reporting, department head nurse review, and specialist group/nursing department verification. When an individual reports a PI, they can upload images via PDA or personal computer. During the review process by the department head nurse or members of the wound care group/nursing department, the system supports one-click access to nursing records and the patient's PI history and images. This enables reviewers to examine comprehensive patient records, ensuring accurate and efficient review.
Three-level quality control for PI
The system facilitates a three-level quality control process for PI, consisting of ward-level, head nurse-level, and wound care group/nursing department oversight, as shown in Figure 2.
For high-risk patients and those with hospital-acquired or pre-existing PI reported by the responsible nurse, the ward head nurse promptly conducts bedside assessments of the patient's skin condition, takes photographs, and reports the case to the head nurse via the information system. The ward head nurse monitors daily evaluations of high-risk patients and uses the system to track the implementation rate of preventive measures for hospitalized patients at risk of PI. Additionally, the ward head nurse conducts random monthly nursing quality inspections. Based on data generated by the system, key issues are analyzed and discussed with the entire nursing team to develop and implement improvement measures.
The head nurse reviews and verifies reported high-risk patients and those with hospital-acquired or pre-existing PI before final approval. The healing process of reported cases is tracked and recorded in the information system. Each month, the head nurse organizes quality inspections of high-risk patients in the wards under their supervision, using the PI quality management module. Identified issues are addressed by guiding the ward head nurse to implement corrective actions.
Members of the wound care group and the nursing department's quality control committee review and verify the skin condition images submitted via the PI risk management module. Cases involving pigmentation or fecal dermatitis are rejected within the system. For complex wounds, the wound care group conducts an on-site evaluation within 24 h and verifies the case through the system. The nursing department conducts regular comprehensive “blanket-style” quality checks for PI nursing care across all patients in the hospital. Any identified problems are corrected and recorded in the system, where data is automatically analyzed and summarized. The nursing department holds quarterly meetings to discuss frequent issues and weaknesses, providing feedback, training, and follow-up to ensure continuous quality improvement.
Technical validation
The system was first tested internally by two software engineers, including the executive unit, integration, and system-level testing. Subsequently, usability testing was conducted by two other software engineers with 30 nurses (including intensive care unit nurses, wound care specialists and nurse managers) through simulated scenarios, examining the system modules (risk assessment, decision prompts, alerts, and picture uploads) against the preset clinical rules, and evaluating the system's usability using the task completion rate (Nurses completed standardized scenarios of risk assessment, wound staging, and intervention selection) and the System Usability Scale (SUS) for evaluation.
The system was first tested in-house by two software engineers, including performing unit, integration, and system-level testing. Subsequently, usability testing was conducted by two other software engineers with 30 nurses (including intensive care unit nurses, wound care specialists, and nurse managers) through a simulation scenario and checked that the system modules (risk assessment, decision prompts, alerts, and picture uploads) conformed to predefined clinical rules. The system was assessed by task completion rates (nurses completed standardized risk assessment, wound staging, and intervention selection tasks), and the SUS were assessed.
The PI risk prediction model was retrospectively validated based on historical data from 50 cardiac surgery patients, and an additional 20 assessments generated by the system were independently reviewed by a wound care expert, and all adverse events (e.g., missed alarms and staging errors) were recorded. The system's clinical accuracy and safety were validated through the AUC value of the risk model and the consistency between the system's assessments and those of experts.
Clinical evaluation
This study is a quasi-experimental study.
Research subjects
Patients admitted to our hospital's CSICU from April 2023 to September 2023 were selected as the control group, while patients admitted from October 2023 to March 2024 were designated as the intervention group. Inclusion Criteria: ICU inpatients undergoing cardiac valve replacement, coronary artery bypass grafting, congenital heart defect repair, etc.; Aged ≥18 years; Informed consent from patients or their families regarding the study. Exclusion Criteria: Patients with severe comorbid primary diseases, such as malignant tumors, severe liver or kidney dysfunction, cerebrovascular diseases, etc.; Patients who died during surgery; Patients with existing PI prior to cardiac surgery. This study was reviewed and approved by the hospital's Ethics Committee (2023YS-031-01). Written informed consent was obtained from all participants or their legally authorized representatives prior to their enrollment in the study.
Sample size calculation

Based on previous studies, 20 the incidence of PI in the control group is 1.63%, while in the intervention group it is 0.75%. Using the formula (1) to estimate the required sample size and accounting for a 20% loss to follow-up, the total sample size for this study is approximately 2234 cases. The estimated sample size required for both the intervention and control groups is 1117 cases each (Zα/2 = 1.96 for a two-tailed probability at α = 0.05, Zβ = 1.28 for a one-tailed probability at β = 0.10. p1 and p2 represent the PI incidence rates in the two groups, and P0 = (P1 + P2)/2).
Research methods
Control group: The traditional management model was adopted. During the patients’ stay in the CSICU, the responsible nurse monitored their vital signs and recorded any changes in PI. In case of abnormalities, the attending physician was promptly informed of the intervention.
Intervention group: Risk assessment: Patients were assessed for existing PI immediately after surgery and upon transfer to the CSICU. If no injuries were present, the postoperative PI prediction model was used to evaluate the risk. Numeric assessment items were automatically retrieved from the electronic medical record system, while the nursing staff manually selected the history of PI. The form could only be saved once all items were completed. The system calculated the patient's PI risk score based on their basic information, disease characteristics, and classification data. Risk identification: Upon completing the PI risk assessment, the system determined the patient's risk level based on the calculated risk score. If the patient was identified as high risk, the assessment result was automatically pushed to the nursing and physician interfaces, accompanied by a flashing pop-up box to prompt immediate attention. Intelligent decision-making: The system automatically matched corresponding nursing interventions from the knowledge base based on the patient's risk level. Nurses could select appropriate interventions for the patient's condition and develop personalized nursing plans. Evaluation: The system automatically determined the frequency of evaluations based on the patient's risk level, generating tasks and issuing real-time reminders. When patients were discharged or transferred, the system prompted nurses to assess the effectiveness of PI management, ensuring a closed-loop process and the completeness of management records. All interventions were automatically saved in the system, generating nursing records simultaneously.
Outcome
Wound assessment accuracy, wound treatment accuracy, PI healing rate, PI incidence rate, and PI nursing record defect rate were used as observational indicators in this study, and each indicator was calculated as follows: wound assessment accuracy = (number of accurate wound assessments/total number of assessments) × 100%, wound treatment accuracy = (number of correctly treated wounds/total number of wounds requiring treatment) × 100%, PI healing rate = (number of healed PI/total number of PI) × 100%, PI incidence rate = (number of Inpatients with hospital-acquired pressure injuries/total number of inpatients) × 1000%, PI nursing record defect rate = (number of defective nursing record entries/total number of nursing record entries during the same period)
Data collection and analysis
For the control group, wound care team members compiled paper-based high-risk PI assessment forms from April 2023 to September 2023. Two individuals double-checked these forms for accuracy before entering them into the computer. Data from October 2023 to March 2024 for the intervention group was automatically extracted from the computer system's backend and exported into Excel spreadsheets.
A descriptive analysis of general data was conducted. Count data were described using frequency and composition ratio (%), and comparisons were made using the chi-square test or Fisher's exact probability method. Measurement data following a normal distribution were described by mean and standard deviation, while non-normally distributed data were described by median and interquartile range. Independent sample t-tests and rank-sum tests were used for between-group comparisons. A significance level of α = 0.05 was set, with results considered statistically significant if P < 0.05.
Quality control
Trained research team members conducted baseline assessments of enrolled patients to ensure that patients met the inclusion criteria and did not fall under the exclusion criteria.
Before the study commenced, the head of the hospital's network management center provided training to study implementers on the use and standards of the CNDSS. Implementers were allowed to ask questions and demonstrate their understanding on-site after the training.
During the patients’ hospitalization in the CSICU, the responsible nurses conducted digital monitoring and nursing care, guiding and assisting patients in preventing and treating PI. The study lead followed up with patients in both groups via phone, WeChat, or ward visits to track and record their PI conditions.
Results
Results of system development and technical validation
Usability testing with 30 nurses yielded a high SUS score of 82 (out of 100) and a task completion rate of 94%. Retrospective validation of the embedded risk prediction model on an independent cohort of 50 patients demonstrated an AUC of 0.87 (95% CI [0.82, 0.91]). A blinded review by a wound care expert showed 97.7% agreement with the system's assessments on a subset of 20 cases, with no safety events recorded.
Results of clinical evaluation
A total of 2592 patients were included in the clinical evaluation (Figure 4), with 1302 in the control group and 1290 in the intervention group. Although group allocation was not randomized, the socio-demographic and clinical characteristics of the two groups were comparable, as shown in Table 3 (all p > 0.05), suggesting that the groups were well-balanced and reducing the potential for confounding. The impact of the CNDSS on key outcomes is presented in Table 4.

Study participants flowchart.
Socio-demographic data comparison between two groups.

Monitoring results before and after the implementation of the CNDSS for PI.

CNDSS: clinical nursing decision support systems; PI: pressure injury; CI: confidence interval.
Discussion
CNDSS improves the accuracy of wound assessment and treatment and promotes wound healing
Related studies have shown that in PI's prevention and nursing care, nurses must make decisions by integrating patient information with standard nursing workflows and protocols. 21 However, factors such as increasing patient volumes, the complexity of medical conditions, and the introduction of new medical and nursing technologies greatly affect the accuracy and continuity of clinical decisions. In clinical practice, nurses process information through four stages: information analysis, decision-making, information acquisition, and action execution. The CNDSS can automate the stages of information analysis and decision-making. 22 Reports suggest that with the increasing volume of stored patient data, digital nursing documentation systems assist nurses in making informed clinical decisions. 23 Ho et al. constructed psychiatric knowledge-based clinical decision support system based on nursing standards and norms and designed the operational process of the information system according to clinical nursing practice. Results showed that the system helped nurses make accurate nursing diagnoses and execute correct nursing procedures. 24
A systematic review of clinical decision support systems for stroke prevention has demonstrated that applying such systems may significantly benefit patient outcomes. These benefits include improved accuracy and efficiency in identifying high-risk patients, better adherence to evidence-based stroke prevention guidelines, and the facilitation of early diagnosis and intervention. 25 The CNDSS assist nurses in making timely decisions and providing patients with accurate, effective, and personalized care. 26 In this study, PI's wound assessment and treatment accuracy significantly improved. The reason for these improvements may be attributed to the system's four modules: risk assessment, risk identification, intelligent decision-making, and evaluation. These modules incorporate the principles of early warning management and visual management to establish a comprehensive, multi-perspective early warning and pre-control system. Combining the CNDSS with nursing knowledge bases and reasoning engine decision rules enhances nurses’ ability to make nursing diagnoses and decisions. 24 This approach addresses common challenges in clinical nursing, such as inadequate PI risk prediction, insufficient wound observation, unprofessional wound descriptions, and improper treatment. Consequently, the system enables precise PI assessment, real-time alerts, and effective interventions, reducing the workload of nursing staff, optimizing the management process for PI, and maximizing the application of information technology in nursing. This reflects the intelligent and accurate nature of clinical nursing.
While the CNDSS demonstrated significant improvements in process outcomes such as wound assessment accuracy and documentation quality, the observed reduction in the incidence of PI (from 14.8% to 12.8%) was not statistically significant (P = 0.35). This finding warrants a critical appraisal. Several factors may explain this result. First, the study duration might have been insufficient to detect a significant change in a relatively low-incidence outcome. PI development is multifactorial, and a longer follow-up period with a larger sample size would provide greater statistical power. Second, the Hawthorne Effect might have played a role; nurses in the intervention group, aware of being studied, might have heightened their vigilance regardless of the system's prompts, thereby reducing the observable difference between groups. Third, and most importantly, the primary value of the CNDSS in this context may lie in standardizing care processes and enhancing early detection and documentation, rather than solely in preventing entirely new cases. Many “prevented” PIs might have been very early-stage (e.g., Stage 1) that were accurately identified and managed promptly, thus not progressing to a reportable injury. This is reflected in the significantly improved healing rate. This interpretation is supported by literature suggesting that decision support systems often yield more immediate and pronounced effects on the quality and reliability of clinical processes than on ultimate patient outcomes. 27 Future studies with longer durations and cluster-randomized designs are needed to definitively establish the system's impact on PI incidence.
CNDSS can optimize the quality of nursing paperwork records and improve the quality of nursing management
After implementing the CNDSS for PI, standardized and structured specialized nursing documentation provides nurses with accurate definition instructions, facilitating the querying, analysis, and statistical evaluation of patient data. This, in turn, helps standardize nursing practices. 28 A study by Oliveira et al. demonstrated that applying a well-developed and fully functional CNDSS and enhanced team training improves the quality of nursing documentation. 29 Additionally, standardized nursing procedures help integrate and organize information, promote communication among interdisciplinary team members, and contribute to improved nursing quality and patient safety. 30 In this study, the quality of nursing documentation improved compared to previous levels, aligning with the findings of Zhao et al.. 30 Their research team developed PedN-Clinical Decision Support Systems, which can automatically extract each nursing process step and populate standardized, structured, and formatted nursing records. This effectively prevents omissions in documentation and enhances the overall quality of nursing records.
This study developed a knowledge base for PI in postoperative cardiac surgery patients by integrating guidelines, professional (industry) standards, expert consensus, systematic reviews, evidence summaries, and clinical practice literature related to PI. By importing relevant data sources and text, the system enables real-time sharing of similar data and information across various nursing records, reducing the time nurses spend on repetitive data entry and minimizing errors, thereby increasing the time available for direct patient care. A study that embedded standardized nursing language and clinical decision support into nursing information systems showed that introducing record templates based on standardized nursing language reduced variability in manual data entry, promoted data integration, and improved the quality of nursing documentation. 31 Additionally, nursing managers can access the system's backend at any time to review reported PI cases, ensuring the quality of nursing records. Risk assessments for PI are monitored and reviewed by head nurses in real-time, ensuring the accuracy and comprehensiveness of nursing documentation. High-risk patients are displayed in the head nurse's management system, allowing managers to supervise the overall department's PI risk assessments and preventive care in real-time, ensuring consistent quality in PI management across the unit. This demonstrates that using the system to manage PI effectively prevents irregularities often found in paper-based nursing documentation, ensures the quality of nursing records, and enhances the comprehensiveness of PI risk assessments and reporting. The system's practicality is evident, supporting its clinical use and further promotion.
The CNDSS for PI developed in this study optimizes the management process and achieves closed-loop management of pressure injuries. In the quality control process of PI management, it is essential to implement layered monitoring and ensure that every step is executed, thus achieving comprehensive quality management. 32 A study by Sharkey et al. demonstrated that integrating health information technology with quality control and improvement can continuously enhance clinical processes and outcomes. 33 At this hospital, the system facilitates three-level quality control of PI. After reporting high-risk or confirmed PI cases, reviews by head nurses and specialized teams are required to ensure dual-level quality control at the hospital and department levels. The system provides quality PI nursing practices among nurses and enables managers to monitor the overall status of PI in the department in real-time. This aids nurses and nursing managers in improving the quality of PI nursing care. Furthermore, the intelligent presentation of the system contributes to the scientific management of PI. Key nursing processes become measurable by allowing nursing managers to collect, store, process, and retrieve data on PI. Statistical analyses can be conducted based on data sources and calculation methods to evaluate nursing outcomes, estimate workloads, identify key areas for clinical improvement, and accurately analyze quality indicators related to PI. The system supports systematic tracking, failure mode, effect analysis, and other quality improvement activities. This aids clinical decision-making for nursing staff, enhancing the quality and efficiency of nursing management. 19
Strengths and limitations of this study
Although CNDSS improve decision-making efficiency, its adoption relies on nurses’ trust in the system's output. Our design employs explainable artificial intelligence (XAI) techniques [e.g., shapley additive explanations, local interpretable model-agnostic explanations, attentional mechanisms], such as (1) visual risk stratification: risk levels are color-coded (green/yellow/orange/red/purple) and mapped to specific management strategies (basic/primary/secondary). This provides immediate, visual understanding of patient risk status. (2) Structured rule-based logic: interventions are triggered by predefined rules (e.g., “if risk ≥5% → secondary management”). These explicit, clinically validated rules make the system's reasoning process transparent. (3) Dashboard-driven interactions: the “Intelligent Dashboard” shows: real-time patient risk summary (ward/individual level). Automated alerts with explicit task assignments (e.g., “Reassess in 12 h”). The system incorporates intuitive visualizations and explicit rule-based logic to reveal the rationale behind AI-driven recommendations. These methods conform to interpretable AI by making risk stratification and intervention triggers clinically interpretable. A computerized nursing information system provides decision support for nurses, enhancing their ability to make nursing diagnoses. However, the recommendations provided by CNDSS are intended to complement, not replace, the professional judgment of nurses in clinical practice. Previous studies 34 have shown that nurses rarely make decisions based solely on CNDSS recommendations. Instead, they integrate subjective and objective patient information to assess the accuracy of the CNDSS and make more precise and comprehensive decisions. Nurses’ clinical experience is crucial in determining whether CNDSS can benefit clinical work. Experienced nurses are better equipped to grasp patients’ overall condition, identify accurate diagnoses related to their clinical status, 35 and internalize nursing processes in their practice. Rigid adherence to clinical practice recommendations may reduce their autonomy. 36 Therefore, while benefiting from the convenience brought by CNDSS, nurses must continue to develop problem-solving skills and translate knowledge into improved nursing quality and patient outcomes. 37
However, due to the limited duration of the study, the current system still has certain structural and functional limitations. Some modules, such as the nursing record management and PI-related test indicator association modules, have not yet been activated. These issues will be addressed in the next phase of development planning. Additionally, system instability has been observed during operation. Tasks like uploading images increase workload, leading to resistance among nursing staff and low compliance in using the system. This aligns with existing literature on the implementation of health information technologies, which often highlights the challenge of workflow integration and user acceptance. 38 This highlights the potential influence of organizational and human factors, such as institutional culture and differences in nurses’ readiness for change and proficiency with health information technology, which may have modulated the system's effectiveness and the observed outcomes. Therefore, it is essential to conduct relevant training for nursing staff to enhance the system's intelligence and user-friendliness, maximizing its value in nursing practice. Moreover, the data collected in this study were obtained immediately after the system was implemented. As a result, the long-term impact of the system on the prevention and nursing care of PI may not have been fully captured. And the quasi-experimental design, while pragmatic, limits our ability to establish causality definitively due to the potential for unmeasured confounding factors.
Reflections on future development
While the present study offers valuable empirical evidence supporting the implementation and benefits of a CNDSS for PI management in cardiac surgery patients, several avenues for future research hold significant promise for strengthening the evidence base and optimizing system utility:
Cross-Setting Validation and Adaptability: Future research should actively evaluate the effectiveness, generalizability, and adaptability of the CNDSS across a broader spectrum of clinical environments. This includes rigorous testing in diverse settings such as intensive care units (beyond cardiac-specific ICUs), geriatric wards, long-term care facilities, rehabilitation centers, and among patients with complex comorbidities (e.g., diabetes, chronic kidney disease, spinal cord injury). Understanding how the system performs and integrates into varying workflows, patient populations, and resource constraints is crucial for demonstrating its broader applicability and identifying necessary contextual adaptations. Robust Comparative Effectiveness Research: To establish a higher level of evidence for the CNDSS's clinical impact and value, well-designed randomized controlled trials (RCTs) are recommended. These trials should compare patient outcomes (e.g., PI incidence, healing rates, complications, and length of stay), process indicators (e.g., adherence to guidelines and documentation quality), and potentially economic outcomes (cost-effectiveness) between care delivered with the support of the CNDSS and conventional, non-system-supported care practices. Such trials would provide more definitive proof of the system's causal contribution to improved outcomes. Comprehensive User Experience and Implementation Science: A deeper understanding of end-user (nurses and managers) acceptance, satisfaction, and experience is essential for sustainable implementation and optimization. Future studies should employ mixed-methods approaches, combining quantitative surveys (measuring usability, perceived usefulness, satisfaction, workload impact) with qualitative methods (e.g., interviews and focus groups) to explore facilitators, barriers, perceived value, workflow integration challenges, and unintended consequences. This user-centered research can inform critical refinements to the system's design, functionality, training programs, and implementation strategies to maximize adoption and effectiveness. Longitudinal Impact and Sustainability: Investigating the long-term effects of CNDSS implementation is vital. Research should track outcomes over extended periods to assess the sustainability of observed improvements in PI rates, healing, documentation, and nursing efficiency. This includes monitoring potential changes in user engagement, system utilization patterns, and the maintenance of quality gains over time.
Conclusion
This study successfully developed and implemented a CNDSS for PI management in postoperative cardiac surgery patients. Key outcomes demonstrate that the CNDSS significantly improved clinical practice: Enhanced PI healing rates (89.1–97.2%, P < 0.05), increased accuracy in wound assessment (90.8–97.2%, P < 0.05) and treatment (88.3–96.5%, P < 0.05), reduced defects in nursing documentation (15.3–7.7%, P < 0.001). These results confirm the system's clinical utility in standardizing PI care, optimizing nursing workflows, and elevating documentation quality. The CNDSS provides an effective tool for enabling evidence-based, personalized interventions and strengthening closed-loop quality control in PI management. To further advance this field, future research should prioritize: evaluating CNDSS effectiveness in diverse clinical settings (e.g., geriatric, neurology, or general ICU wards), conducting randomized controlled trials to quantify its impact on patient outcomes and healthcare costs, assessing nurse acceptance and satisfaction to refine usability and implementation strategies, and exploring the vertical impact and sustainability of the system.
Footnotes
Ethical approval
This study was reviewed and approved by the hospital's Ethics Committee (2023YS-031-01). Written informed consent was obtained from all participants or their legally authorized representatives prior to their enrollment in the study.
Author contributions
All authors contributed to the study's conception and design. Meng Zexuan performed material preparation, data collection, and analysis. Zhang Yan wrote the first draft of the manuscript. Zhang Nan and Fa Tian’e commented on previous versions of the manuscript. Xu Lina and Wu Zhenhua are responsible for funding acquisition and project supervising. All the authors read and approved the final manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Tianjin Nursing Society 2023 Research Project, Tianjin Municipal Education Commission Scientific Research Programme Project (Natural Science), Tianjin Key Medical Discipline Construction Project (Grant Number tjhlky2023QN07, 2022YGYB10, TJYXZDXK-3-030C).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
The data sets used and/or analyzed during the current study are available from the corresponding author on reasonable request.