
Abstract
Background
Chatbots have been extensively utilized in chronic disease management to collect real-time health data, deliver personalized educational content, and guide self-management. Nevertheless, critical research gaps persist regarding their differential implementation across specific contexts and quantified comparative effectiveness.
Objective
To synthesize existing research on the application of chatbots in chronic disease management, providing evidence-based insights to inform future clinical practice.
Methods
Following Arksey and O’Malley's framework, we systematically searched eight databases from their inception until October 20, 2024. Relevant data were extracted from eligible studies, with a focus on disease areas, application platforms, interaction methods, technical architectures, implementation elements, and evaluation indicators. The findings were then synthesized and analyzed to identify key trends and gaps in the literature.
Results
A total of 19 studies were included in this review, comprising 10 randomized controlled trials (RCTs) and 9 quasi-experimental studies. The investigated chronic conditions encompassed cancer, diabetes, hypertension, and other prevalent chronic diseases. Chatbot deployment platforms primarily included mobile applications, web-based platforms, and instant messaging software. The underlying technical architectures consisted of artificial intelligence-driven systems, rule-based systems, and hybrid models. The implementation strategies were categorized into night key dimensions. The predominant interaction modality was hybrid, with communication content focusing on self-management education, emotional support, and related domains. Outcome measures evaluated health-related indicators and user adherence indicators.
Conclusions
Chatbots hold considerable clinical application value in chronic disease management. However, current research has some limitations. Future research should further optimize interaction design, refine system functionalities, and fortify privacy protection measures to better facilitate the integration of chatbots into chronic disease management.
Introduction
Noncommunicable diseases (NCDs), encompassing cardiovascular diseases, malignancies, chronic respiratory diseases, diabetes, hypertension, and related conditions, represent a critical global public health challenge. 1 Characterized by multifactorial etiology, prolonged disease duration, refractory nature to complete cure, and high rates of disability and mortality, NCDs exhibit persistently increasing prevalence and mortality rates. This trend imposes substantial disease burden and socioeconomic costs worldwide.1,2 According to the World Health Organization (WHO) reports, NCDs account for approximately 41 million annual deaths globally, representing 74% of total mortality worldwide. 3 This challenge is particularly acute in China, where epidemiological data reveal a substantial and growing chronic disease burden. Notably, over 85% of all deaths in China are attributable to NCDs, with these conditions contributing to more than 70% of the nation's total disease burden,3,4 which significantly exceeds global averages. Health management serves as a pivotal strategy for chronic disease prevention and control, demonstrating efficacy in reducing disease burden and extending healthy life expectancy. However, persistent challenges in chronic disease management include inadequate patient self-management capacity, poor long-term adherence to follow-up protocols, and the need for personalized interventions. 5
To address the challenges in chronic disease management, WHO has strongly advocated for digital health interventions as a strategic approach to enhance healthcare capacity, expand service coverage, and improve intervention efficiency, ultimately advancing universal health coverage goals. 6 In recent years, the digital health landscape has undergone a paradigm shift, evolving from traditional domains such as eHealth and mHealth to cutting-edge interdisciplinary frontiers integrating advanced computational sciences, particularly big data analytics, genomics, and artificial intelligence (AI). 7 The rapid advancement of AI, particularly machine learning (ML), deep learning (DL), and natural language processing (NLP) technologies, 8 is transforming healthcare interventions in unprecedented ways. AI applications have demonstrated significant potential across critical clinical domains, including disease diagnosis, risk prediction, prognostic evaluation, and patient follow-up management. Against this technological backdrop, AI-powered chatbots have emerged as innovative solutions. Chatbots are computer systems designed to simulate human conversation through multimodal interfaces, including text, voice, and visual interactions. These systems are broadly categorized into two distinct architectures: artificial intelligence-based chatbots and rule-based conversational agents. 9
The clinical applications of chatbots have expanded beyond basic health inquiries to encompass diverse domains, including disease screening, chronic condition management, psychological support, and clinical training. Given the characteristics of chronic diseases, including relatively stable disease status, insidious symptoms, protracted disease course, propensity for recurrence, and difficulty in achieving a complete cure, patients require long-term self-management and medical supervision. However, traditional follow-up models frequently encounter challenges such as limited resources, temporal and spatial constraints, and inadequate dynamic monitoring. A growing evidence suggests that chatbots can play a pivotal role in chronic disease management by assisting patients with disease monitoring, facilitating healthy behavior change, delivering disease-specific knowledge and skills education, enhancing adherence, and providing psychosocial support, thereby improving clinical outcomes, enhancing quality of life, and reducing healthcare costs.10,11 Furthermore, chatbot systems demonstrate significant utility in automating the collection of patient-reported outcomes (PROs), 12 thereby providing clinicians with comprehensive, longitudinal health data that enhances clinical decision making during both consultations and follow-up care. An online survey found that doctors generally believe that healthcare chatbots have a positive effect on patients’ health self-management behaviors, which can improve patients’ disease symptoms, mental health, and health behaviors. 13 Therefore, chatbots provide an efficient, personalized, and cost-effective digital health intervention for chronic disease management, demonstrating significant potential to delay disease progression and reduce all-cause mortality rates in chronic disease populations.
In recent years, the design of medical chatbot systems has largely shifted from traditional rule-based frameworks to sophisticated generative models powered by large language models (LLMs). 14 Conventional systems rely on static decision trees and keyword matching, which, while demonstrating a certain capacity to mimic medical interactions through scripted dialogs, inherently constrain their flexibility, contextual understanding, and ability to handle diverse patient inputs. In contrast, LLMs such as GPT and Deepseek employ transformer-based architectures to comprehend and generate natural language in a dynamic and context-sensitive manner. 15 This transition enables more fluid, context-aware, and linguistically complex interactions, allowing such systems to adapt to varied user needs and expand their functional scope. 16 For instance, Zhang Sainan et al. 17 developed a chatbot named Chat Ella using Generative Pre-trained Transformer 2 (GPT-2) to assist in diagnosing 24 chronic diseases. Their results indicated a diagnostic accuracy of 97.50%, and the system received positive feedback from 68.7% of participants. Similarly, Kim et al. (2024) developed an AI-based chatbot to support self-management in gastric cancer patients, reporting an accuracy of 85.2% and a precision of 87.6%. Despite the considerable potential of LLMs in building more intelligent and personalized chatbots for chronic disease management, their integration requires careful consideration of multiple challenges, including accuracy, fairness, and ethical and privacy concerns, to ensure safe and effective clinical application.15,16
Nevertheless, current research exhibits substantial heterogeneity in chatbot design elements, including interaction modalities, functional capabilities, and evaluation indicators, which compromises the comparability of study outcomes and hinders the development of standardized practice guidelines.11,18 Consequently, this study employs a scoping review methodology to systematically examine the existing literature on chatbot applications in chronic disease management. Through comprehensive analysis of relevant research, we aim to identify current research gaps and methodological limitations. This study aims to provide a foundational basis for formulating standardized clinical intervention strategies and developing clinically demand-driven chatbots.
Objectives
This scoping review aims to synthesize existing research on the application of chatbots in chronic disease management, with particular focus on technical architectures, implementation characteristics, and evaluation indicators. By identifying current research limitations and knowledge gaps, the study provides an evidence-based foundation for optimizing clinical decisions and intervention strategies in digital health.
Methods
Study design
This scoping review was conducted following the five-stage methodological framework established by Arksey and O'Malley 19 : (1) identifying the research question, (2) determining relevant research, (3) selecting research, (4) charting the extracted data, and (5) collating, summarizing, and reporting the results. This scoping review adhered to the PRISMA-ScR (Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews) statement, 20 as detailed in Supplementary File 1. This review is not registered as PROSPERO does not accept scoping reviews.
Identifying the research question
Following preliminary literature screening and analysis of current chatbot applications in chronic disease management, we formulated four key research questions: (1) What platforms and techniques support chatbot implementation in chronic disease management? (2) What implementation characterize these interventions? (3) How are chatbot-based interventions evaluated?
Determining relevant research
This scoping review conducted a systematic search of PubMed, the Cochrane Library, Web of Science, Embase, CINAHL, the China National Knowledge Infrastructure (CNKI), Wanfang Database, and the Chinese Biomedical Literature Database (CBM), covering all available records from inception through October 20, 2024. Search terms including keywords and subject headings were related to chatbot technologies (e.g. “conversational agent,” “chatbot,” “smartbot,” “dialog system,” and “dialog agent”) and chronic diseases (e.g. “chronic kidney disease,” “chronic disease,” “cardiovascular diseases,” “stroke,” “neoplasms,” “hypertension,” “diabetes mellitus,” and “dementia”). The search strategy of all databases used is presented in Supplementary File 2.
Selecting research
All records retrieved from database searches were imported into EndNote Reference Manager for deduplication. Two independent reviewers (JH and SL) conducted the screening process following a standardized protocol: initial title and abstract screening followed by full-text assessment of potentially eligible studies. Any discrepancies were resolved through consensus discussion. Inclusion criteria comprised: (1) Studies involving adult patients with chronic conditions; (2) Interventions utilizing chatbots with automated response algorithms for chronic disease management (excluding human-operated systems); (3) Study designs including randomized controlled trials, quasi-experimental studies, observational studies, or systematic reviews; and (4) Clearly defined interventions with measurable outcomes. Exclusion criteria included: (1) Unavailable full-text articles; (2) Duplicate publications; and (3) Non-English or Non-Chinese language publications.
Charting the extracted data
Information extraction was performed on the included literature, with extracted content encompassing author(s), year of publication, country, study type, type of chronic disease, sample size, application objectives, application platforms, interaction methods, implementation elements, intervention duration, and evaluation indicators. All data were entered into an Excel spreadsheet for aggregation and analysis.
Data synthesis and analysis
Through a comprehensive synthesis of the included studies, we identified and descriptively analyzed the core characteristics of chatbot interventions in chronic disease management. Given the substantial heterogeneity in interventions, outcome measures, and reporting formats among the included studies, a meta-analysis was not deemed appropriate or feasible. The findings are therefore synthesized narratively and presented in a summary table of key outcomes.
Results
Study selection
A total of 1079 studies were retrieved. After eliminating duplicates, 673 remained, of which 567 were excluded following a review of titles and abstracts. A full-text review was conducted on the remaining 106 studies, and ultimately 19 studies were included (see Figure 1).

Flowchart of literature screening.
General characteristics of the included studies
Among the included studies, RCTs represented the majority (n = 10)21–30 followed by quasi-experimental studies (n = 9).31–39 These studies encompassed a broad area of chronic diseases, with cancer being the most frequently investigated condition (n = 6),28,29,33,35,36,38 followed by diabetes (n = 5).24,27,30,37,39 Other disease areas included mental and neurological disorders (n = 3),22,23,25 hypertension (n = 2),26,34 kidney diseases (n = 2),21,32 and orthopedic conditions (n = 1). 31 Intervention durations ranged from 1 week to 2 years, except for one study that did not report this information. 36 One study focusing on task completion time reported an average duration of 18 min. 34 The chatbot-delivered interventions served distinct clinical purposes across studies. Self-management was the primary objective (n = 11),21,22,26,29–31,33,35,37–39 while other applications included supervision (n = 3),23,25,34 education (n = 3),28,32,36 and emotional support (n = 2).24,27 Most studies account for patients’ varied disease characteristics and demographic profiles, while also requiring device support. Specifically, some research incorporates diverse racial backgrounds (n = 3),34,37,38 smartphone usage capabilities (n = 3),23,24,28,31 and language diversity support (n = 2)32,39 to alleviate the digital divide. The two reviewers maintained agreement throughout all phases of the systematic review process. The general characteristics of the included studies are summarized in Table 1.
General characteristics of the included studies (N = 19).

Platforms and technical architectures of chatbots
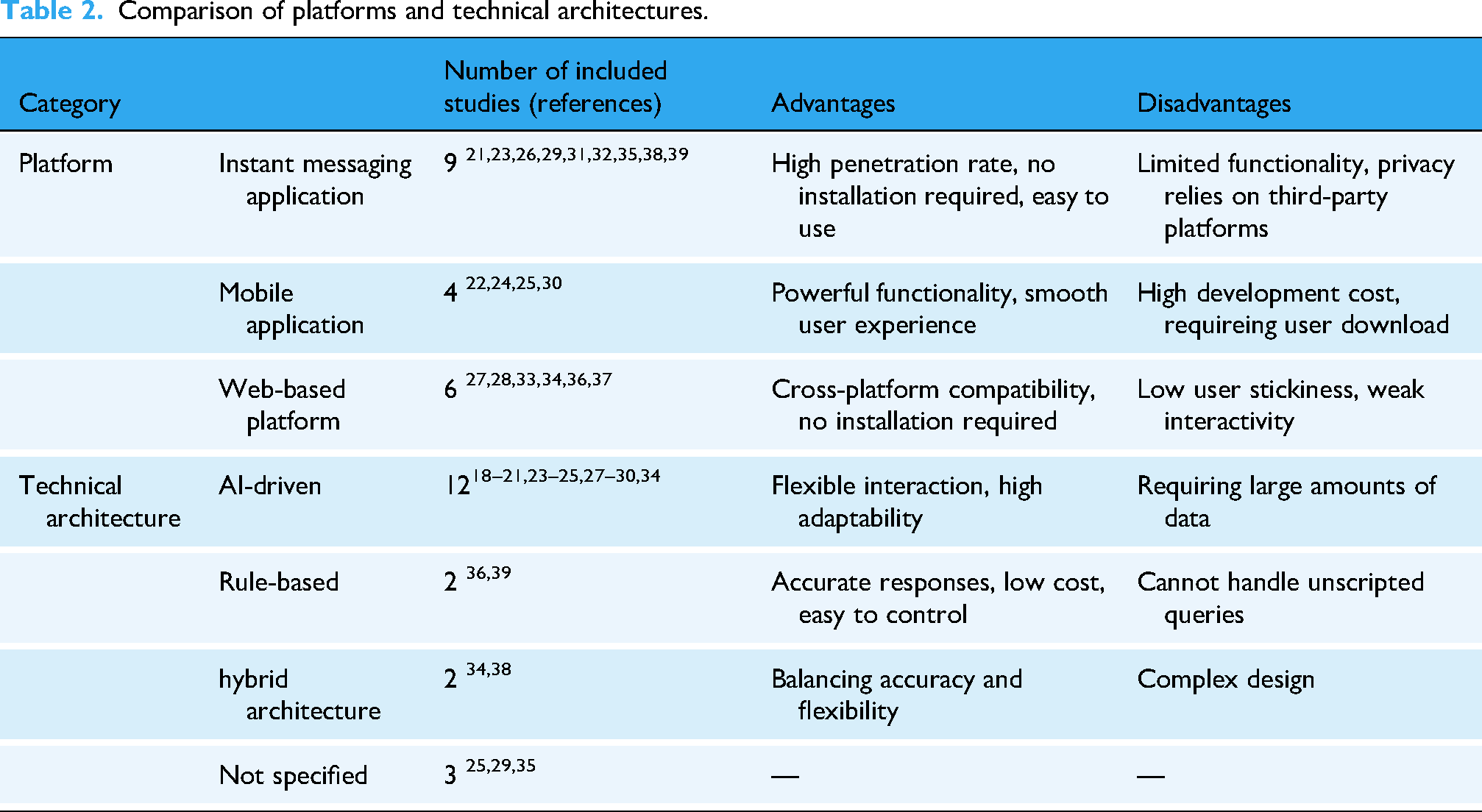
The included studies deployed chatbots across three primary platforms. Instant messaging applications (e.g. WeChat, WhatsApp, LINE, Telegram) were the most ubiquitous (n = 9) due to their widespread adoption and low operational complexity.21,23,26,29,31,32,35,38,39 Mobile applications enabled more sophisticated and integrated self-management functionalities (n = 4).22,24,25,30 Web-based platforms served well for information education and retrieval (n = 6).27,28,33,34,36,37
Regarding technical architectures, artificial intelligence (AI) systems were employed in 12 studies to develop chatbots capable of personalized and conversational interactions,21–24,26–28,30–33,37 while rule-based systems were used in two studies for managing structured tasks.36,39 Furthermore, two studies adopted hybrid architectures to balance flexibility with control, with one integrating rule-based grammatical matching with ML, 34 and the other combining rule-based scripted dialog content with artificial intelligence technologies designed to enhance question comprehension. 38 The technical architectures were not explicitly specified in three studies.25,29,35 See Table 2 for details.
Comparison of platforms and technical architectures.
Interaction methods of chatbots
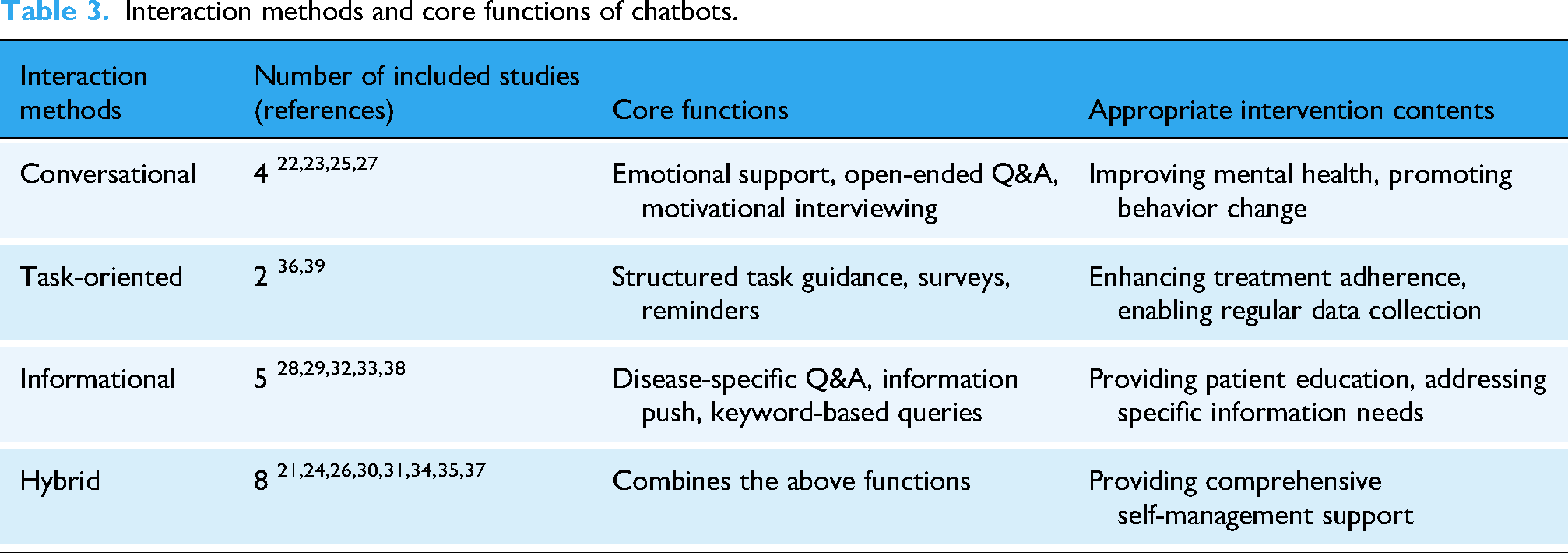
Among the 19 included studies, hybrid interaction modes dominated chatbot designs. With advancing technologies and evolving patient needs, chatbots relying on a single interaction mode have shown limited effectiveness in clinical management. Conversational chatbots (n = 4)22,23,25,27 provide personalized emotional support and open-ended Q&A through bidirectional, open dialog with patients, which is conducive to improving users’ mental health and facilitating behavioral change. Task-oriented chatbots (n = 2)36,39 guide patients through self-management tasks via structured steps, significantly improving treatment adherence. These studies utilized pre-visit surveys for symptom monitoring, requiring patients to submit health data regularly and receive strategy feedback, which led to marked improvements in self-management compliance. Informational chatbots (n = 5)28,29,32,33,38 depend on the accuracy and accessibility of knowledge bases. The studies built specialized knowledge bases as information sources, allowing patients to query symptoms and self-management issues via inputting questions or keywords, and receiving standardized information in return. The remaining eight studies featured hybrid chatbots,21,24,26,30,31,34,35,37 integrating the strengths of different interaction modes. Three studies combined informational and task-oriented features,34,35,37 four studies merged conversational and informational functions,21,24,26,31 and one study integrated all three modes. 40 See Table 3 for details.
Interaction methods and core functions of chatbots.
Implementation elements of chatbots
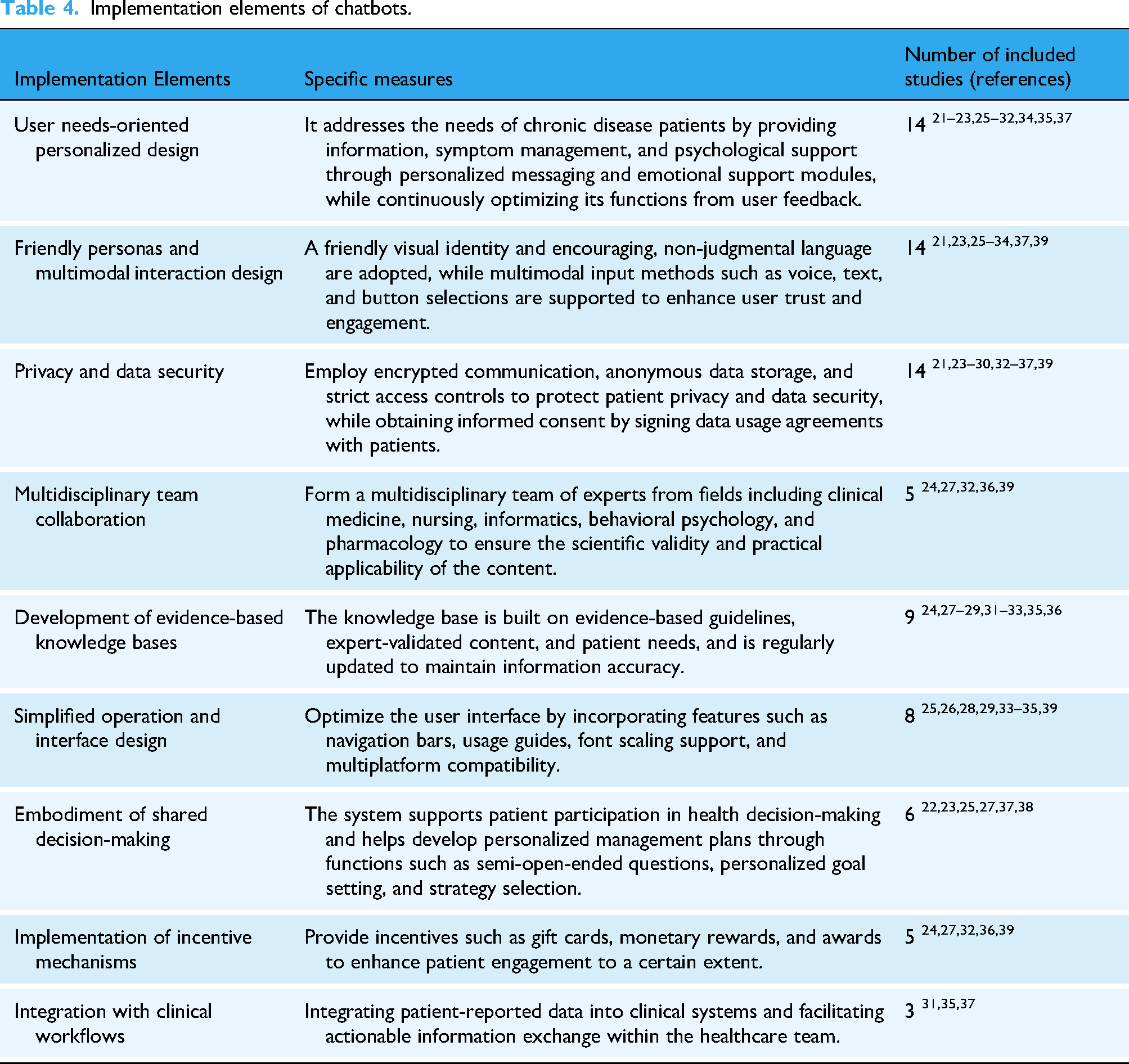
Effective chatbot implementation strategies should be multifaceted, encompassing: user needs-oriented personalized design, multidisciplinary team collaboration, development of evidence-based knowledge bases, friendly personas and multimodal interaction design, embodiment of shared decision-making, privacy and data security, implementation of incentive mechanisms, simplified operation and interface design, and integration with clinical workflows. As detailed in Table 1 and Table 4, the most emphasized implementation elements were a user needs-oriented personalized design (n = 14),21–23,25–32,34,35,37 privacy and data security (n = 14)21,23–30,32–37,39 and friendly personas with multimodal interaction design (n = 14).21,23,25–34,37,39 Furthermore, multidisciplinary team collaboration27,29,33,34,37 and evidence-based knowledge bases24,27–29,31–33,35,36 were identified as foundational to maintaining scientific rigor and content accuracy in chatbot development. Notably, eight studies25,26,28,29,33–35,39 point out that simplifying the operation interface (e.g. by adding navigation bars or supporting font scaling) can significantly lower the usage barriers for elderly patients or digitally disadvantaged groups. Six studies22,23,25,27,37,38 mentioned that chatbots should support patient participation in health decision-making. Five studies24,27,32,36,39 suggested that providing incentives such as gift cards, monetary rewards, and awards can improve patient engagement to a certain extent. By integrating chatbots with clinical information systems (e.g. electronic medical record, clinical decision support system), three studies31,35,37 demonstrated that this approach supported real-time clinician review of electronic patient-reported information and enhanced proactive follow-up care. Other details are provided in Table 1.
Implementation elements of chatbots.
Evaluation indicators for chatbots
Given the heterogeneity of the included studies, a meta-analysis was not performed. Instead, a narrative synthesis was conducted, with outcomes quantified in Table 1. Chatbot interventions were evaluated across four domains: health outcomes, user engagement, self-management ability, system usability and user satisfaction. Fifteen studies21–27,29,30,35,37,38 indicated that chatbots could improve health-related outcomes, including health-related quality of life22,30,35 mental health,21,23–25,27,30 disease-specific indicators,21,22,25,26,29–31,35,37,38 and social function indicators.23,25,35 Ten studies26,28,30,33–39 assessed user engagement through analysis of usage data, including frequency of use, task completion rates, and interaction duration. However, a decline in usage over time was observed in two studies.30,38 Eleven studies21,23,25,26,28–30,32,35,37,39 addressed the impact of chatbots on self-management indicators, such as self-management capabilities,29,31,37 treatment adherence,21,23,26,39 self-efficacy,25,35,39 knowledge or skill acquisition,23,26,30,32 information needs, 28 and treatment readiness. 35 Seven studies27–29,32,34,36,38 evaluated system usability and feasibility using tools including the System Usability Scale (SUS),27,32,34 the Chatbot Usability Questionnaire (CUQ), 29 self-developed usability questionnaires,28,36,38 and system performance metrics (e.g. accuracy, specificity, FI score). 33 Overall, usability ratings were high. User satisfaction was investigated in seven studies24,25,33,35–37 via self-developed questionnaires and the Client Satisfaction Questionnaire-8 (CSQ-8). 27 Additionly, six studies employed interviews to gain deeper insights.24,26,27,34,35,39
Discussion
This scoping review synthesized evidence from 19 studies to map the current landscape of chatbot applications in chronic disease management. The analysis revealed diverse application platforms, technical architectures, and implementation strategies, while also identifying significant trends and gaps in the critical, cross-cutting themes of equity, privacy, and clinical integration. The clinical value of this study lies in providing a theoretical foundation and practical guidance for optimizing chatbot technology, formulating standardized clinical implementation pathways, and promoting the sustainable development of chatbots in chronic disease management.
This review found that instant messaging applications were the most widely used platforms among the included studies, followed by web-based platforms and mobile applications. Instant messaging applications benefit from their extensive user base and high penetration rate.21,23,26,29,31,32,38,39 Since patients can utilize chatbot features without learning new operations, these platforms enhance participation rates while significantly lowering the usage barrier for older adults. Mobile applications offer comprehensive functionalities, supporting complex monitoring and management features, but incur higher development and maintenance costs. Web-based platforms facilitate centralized information display and retrieval, yet their limited adaptability to mobile devices poses operational inconveniences for patients. These differences suggest that platform selection should be based on a comprehensive consideration of specific clinical contexts, target population characteristics, and intervention complexity.
In terms of technical architecture, this study confirms that artificial intelligence (AI) systems represent the predominant framework,21–24,26–28,30–33,37 demonstrating advantages in natural language interaction and personalized feedback. 41 With ongoing advances in natural language generation and emotion recognition technologies, chatbots are progressively achieving more natural and empathetic interactions.42,43 Nevertheless, AI systems still carry potential risks, such as output uncertainty and lack of transparency in decision-making logic. 15 In contrast, rule-based systems offer greater controllability and safety in handling structured tasks such as medication reminders and risk assessments. To balance usability and safety, future systems should adopt layered architectures and modular designs tailored to the characteristics and needs of different chronic disease patient groups, so as to better support their self-management behaviors.
Current research has accumulated significant experience in user-centered design, interdisciplinary collaboration, and evidence-based knowledge base construction. However, to achieve the scalability and sustainable application of chatbots in chronic disease management, it is still necessary to develop a multidimensional integration strategy while balancing technical feasibility and clinical practicality. First, at the user level, an equity-oriented design philosophy should be advocated. Users of different ages, digital literacy levels, racial and ethnic backgrounds, socioeconomic statuses, and language preferences should be included in the evaluation and testing phases during the early development stages to lower the barrier to technology use and avoid exacerbating health inequities due to the digital divide. Some studies have begun to address these aspects, but these efforts are often isolated and not systematically integrated. In the short term, measures such as incentive mechanisms and interface simplification can effectively enhance user engagement. In the short term, measures such as incentive mechanisms and interface simplification can effectively enhance user engagement.24,27,32,36,39 However, long-term engagement still depends on patients’ intrinsic motivation, the functional design of the chatbot, and its clinical value. Second, at the system functionality level, multidisciplinary teams and evidence-based knowledge bases are the foundation for ensuring information accuracy.44,45 However, predefined scripts often lack flexibility when dealing with complex symptoms. Therefore, technologies such as NLP need to be introduced to enhance semantic understanding and interactive capabilities. 43 The current hybrid interaction model, which integrates informational, task-based, and conversational elements, has become the most widely adopted approach. It covers the workflow of screening, education, implementation, and feedback, thereby improving adherence and clinical utility. 46 Future research should prioritize the systematic integration of equity principles by ensuring that chatbots are rigorously tested and optimized with diverse user groups during the design phase to mitigate the digital divide. It is also essential to establish interdisciplinary teams throughout the development process, fostering the creation of hybrid interaction modes tailored to user needs. Such an approach will enhance the reliability of knowledge bases and improve the overall technical adaptability of chatbot systems.
The application of chatbots may raise ethical problems, primarily related to patient data security and privacy. As chatbots collect and store substantial amounts of personal and medical information (e.g. voice recordings and geolocation data), the highly sensitive nature of healthcare data poses significant risks. Unauthorized disclosure of such information could lead to stigmatization or discrimination against participants, thereby amplifying their concerns regarding data privacy and security.14–16 Consequently, it is essential to strengthen privacy safeguards in digital health through measures such as data encryption and anonymization to establish and maintain patient trust. Regarding clinical integration, current progress remains limited. True integration should enable data sharing between patients and providers, supporting real-time monitoring and proactive interventions. Future research should strengthen privacy protection technologies, including measures such as communication encryption and data anonymization, to ensure the security of chatbots; secondly, a clinical integration framework should be established. Since chatbots collect extensive management data from cancer patients, including medication, symptoms, psychology, and information, the use of chatbots can be integrated into hospital electronic medical record systems to enable data sharing. Additionally, an ethical protection mechanism should be established, with transparent informed consent processes developed to ensure fairness and transparency.
Chatbot-mediated interventions demonstrate potential in enhancing chronic disease management, yet their effectiveness is closely tied to alignment with patient-specific needs and clinical contexts. Evidence confirms benefits across several domains, particularly in mental health, symptom control, social functioning, and self-management ability. Improvements were observed in psychological indicators and selected clinical outcomes such as complication and fracture rates. However, benefits in areas including cognitive function, pain management, and psychosocial support remained limited or inconsistent. Furthermore, some benefits, such as reductions in anxiety, were not sustained in the long term, as evidenced by non-significant differences at the 12-month follow-up in one study. 30 In the management of breast cancer chemotherapy side effects, Tawfik et al.reported that the ChemoFreeBot intervention led to significant reductions in the frequency, severity, and distress of physical and psychological symptoms, with self-care behavior effectiveness scores significantly higher than in the nurse-led education group. 29 However, it is crucial to note that this finding is not universally generalizable. Notably, studies by Gong et al. 30 and Ma et al. 38 observed declining usage frequency over time, potentially attributed to misalignment between interaction design and patients’ health literacy or usage preferences, declining long-term needs, and insufficient intrinsic motivation. While usability and information utility receive high patient ratings.28,29 These findings highlight a need for more adaptive and person-centered interaction strategies to sustain participation. User satisfaction was generally high, often attributed to perceived information value, interface usability, and clear visual design.24,34 Nevertheless, limitations in conversational naturalness and technical reliability were consistently identified as barriers to a positive user experience.24,27 System usability assessments reveal critical gaps. Only one study employed the chatbot-specific CUQ scale, 29 while others relied on SUS or custom questionnaires, overlooking core conversational competencies like dialog fluency, affective interaction naturalness, and clinical semantic precision.17,47 Current research suffers from fragmented metrics, lack of safety assessments, absence of standardized tools, and insufficient long-term verification, hindering effective comparison of results across studies. 46 Thus, future research should establish standardized, multidimensional evaluation systems, verify chatbots’ long-term efficacy in chronic disease management via high-quality studies, use mixed methods to reveal feasibility-influencing mechanisms, clarify ethical guidelines, and conduct safety assessments, ultimately enhancing the comparability of intervention effects and the clinical translational value of chatbots in chronic disease management.
Implications for future research
Future research should concentrate on four priorities: First, establishing interdisciplinary collaborative teams that integrate expertise from clinical medicine, informatics, and psychology throughout the chatbot design, development, and evaluation process to enable data-driven precision management. Second, advancing AI-driven optimization by leveraging LLMs for complex query processing, developing personalized multimodal chatbots integrated with electronic health records, and implementing senior-friendly designs (e.g. simplified user interface, gamification) with cross-device compatibility. Third, conducting RCTs to establish core outcome measures and validate long-term effectiveness through multicenter studies. Finally, strengthening regulatory and privacy protection frameworks by implementing rigorous privacy-preserving protocols and robust data security mechanisms to build patient trust.
Strengths and limitations
The innovation of this review lies in being the first to systematically extract and construct an night-dimensional implementation strategy framework for the use of chatbots in chronic disease management, along with an analysis of their characteristics, thereby providing a critical theoretical foundation for establishing standardized clinical intervention pathways in the future. Another advantage is reflected in the methodological rigor. By integrating evidence from multiple countries through a scoping review approach and addressing the current challenges of high heterogeneity among studies, it offers a practice-oriented direction for developing standardized solutions driven by clinical needs.
A potential limitation of the current study is the small sample sizes of the included studies and the limited number of studies on the same diseases, coupled with significant variations (e.g. in disease types and outcome measures), which precluded a meta-analysis of effects across studies. Secondly, the single-center study designs limit the generalizability of the findings. Future research should involve multicenter, large-sample randomized controlled trials, and meta-analyses are necessary. Finally, Most prior studies were conducted as short-term pilot investigations; future research should adopt longitudinal designs, and qualitative methods could be employed to explore potential barriers and facilitators during implementation.
Conclusion
Chatbots hold considerable clinical value in chronic disease management, yielding positive effects on health outcomes, self-management, and other domains. However, current research has some limitations. Moving forward, it will be necessary to further optimize interaction design, enhance system functionality, and strengthen privacy protection to better facilitate the application of chatbots in chronic disease management.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076251411287 - Supplemental material for Application of chatbots in chronic disease management: A scoping review
Supplemental material, sj-docx-1-dhj-10.1177_20552076251411287 for Application of chatbots in chronic disease management: A scoping review by Jiayi Hou, Shineng Lin, Peimeng Teng, Yuyuan Han, Yijia Luo and Guijuan He in DIGITAL HEALTH
Footnotes
Acknowledgments
We would like to acknowledge all of the participants and all of the researchers in this study.
Ethical considerations
Not applicable.
Consent to participate
Not applicable.
Contributorship
J. Hou and S. Lin: conceptualization, methodology, investigation, data curation, formal analysis, writing—original draft, writing—review & editing. P. Teng, Y. Han, and Y. Luo: investigation, data curation, writing—review & editing. G. He: conceptualization, methodology, resources, supervision, project administration, funding acquisition, writing—review & editing.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by Zhejiang Provincial Natural Science Foundation of China under Grant No.LTGY23H250001.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
The datasets generated during and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.