
Abstract
Objective
With the increasing global burden of chronic diseases, there is the potential for conversational agents (CAs) to assist people in actively managing their conditions. This paper reviews different types of CAs used for chronic condition management, delving into their characteristics and the chosen study designs. This paper also discusses the potential of these CAs to enhance the health and well-being of people with chronic conditions.
Methods
A search was performed in February 2023 on PubMed, ACM Digital Library, Scopus, and IEEE Xplore. Studies were included if they focused on chronic disease management or prevention and if systems were evaluated on target user groups.
Results
The 42 selected studies explored diverse types of CAs across 11 health conditions. Personalization varied, with 25 CAs not adapting message content, while others incorporated user characteristics and real-time context. Only 12 studies used medical records in conjunction with CAs for conditions like diabetes, mental health, cardiovascular issues, and cancer. Despite measurement method variations, the studies predominantly emphasized improved health outcomes and positive user attitudes toward CAs.
Conclusions
The results underscore the need for CAs to adapt to evolving patient needs, customize interventions, and incorporate human support and medical records for more effective care. It also highlights the potential of CAs to play a more active role in helping individuals manage their conditions and notes the value of linguistic data generated during user interactions. The analysis acknowledges its limitations and encourages further research into the use and potential of CAs in disease-specific contexts.
Introduction
In recent years, there has been a significant rise in the prevalence of chronic diseases, resulting in a growing number of individuals living with at least one chronic health condition. 1 Chronic conditions have enduring and persistent effects, necessitating patients and healthcare professionals to navigate complex lifestyle and behavioral adjustments and engage in long-term management. 2 Moreover, these conditions reduce quality of life and life expectancy and can escalate personal healthcare expenses due to disability, frequent hospitalizations, and the need for multiple treatment procedures.
In healthcare, the continuum of care 3 is the concept of an integrated care system that guides and tracks patients over time through every subsequent step of health services. The care system contains a range of healthcare and social services, from preventive care to acute treatment, rehabilitation, and long-term care. Over time, the patient goes through various parts of the system, depending on the stage of the treatment or the need for care. The continuum of care aims to provide patients with the right care at the right time and in the most appropriate setting (e.g., home, rehabilitation centers, or hospitals), promoting better health outcomes and patient satisfaction.
Alongside work performed by healthcare professionals, there are often health-related activities that patients and their informal caregivers undertake in managing their health conditions, sometimes referred to patient work. 4 The activities include various processes, from cognitive to physical, performed individually or collaboratively with others, including family and community members, and can be classified as visible when they are acknowledged and valued by others or invisible when they are taken for granted by others and consequently undervalued. 5
Digital technologies have the potential to empower people, giving them a sense of agency and control, allowing them to extend their skills and knowledge and giving them access to experiences and functions that people did not have before. 6 Technologies can reduce the burden of patient work or self-management of health conditions and serve as accessible alternatives to in-person support and supervision. One such technology is conversational agents (CAs), computer systems that imitate human-like conversations using natural language user interfaces involving images, text, and voice. 7 CAs potentially offer the advantages of scalability, reduced costs, lowered stigma, and personalized health support available at any time.8,9 CAs can be delivered through text or speech, making them versatile for different target groups, including children and older individuals. CAs can address various healthcare needs, such as mental health management support, 10 aid in chronic disease self-management, 11 and lifestyle change facilitation, e.g., physical activity and dietary modifications. 12
However, existing digital technologies designed for patients with chronic conditions face challenges adapting to changing health needs and goals. Specific subgroups significantly differ in healthcare preferences and goals and require different information and recommendations. 13 Moreover, patients evolve and change the apps they use throughout the trajectory of their condition, from diagnosis to long-term care, as their health goals change over the course of their disease. 13 The chronic illness trajectory model 14 describes how the course of illness varies for each patient and changes over time. Patients may shift between different illness phases repeatedly in unpredictable and inconsistent ways, as their conditions fluctuate.
Digital systems that are not only focused on one specific stage of the disease but also adapt to the changing needs of users can enable sustained app usage by reducing the necessity to search for more appropriate apps. Such systems would facilitate continuous tracking of healthcare data over time, supporting individuals in effectively managing their health and reducing the disruption caused by switching between different apps.
Despite the extensive research on the application of CAs in healthcare, to our knowledge, there has been no scoping review of different types of CAs in chronic disease management with no constraints on demographics. Existing reviews often restricted their focus to specific health areas, such as mental health,15–17 smoking cessation, 18 physical activity 19 or body weight management20,21; population, e.g., young (25 years and younger), 17 or adults (18 years and older) 22 ; or agent types, e.g., embodied,23,24 voice-based, 25 artificial intelligence-based2,21,26,27 CAs or CAs with unconstrained natural language input, 28 e.g., free text or speech. Other reviews report solely on the evaluation outcomes, e.g., effectiveness and acceptability,18,27,29 or on one of the CAs’ aspects, e.g., personalization 30 or design features. 24
This paper provides the results of a literature analysis aimed at addressing several research questions related to the use of CAs in the context of chronic disease management. The research questions explored in this article are:
What are the health domains, and the characteristics of the end users, targeted for CA interventions? What are the characteristics of the CA studies? Do CAs address continuum of care and patient work concepts for self-management? Do CAs adapt to the changing needs of users? What are the CAs’ characteristics? How do different types of CAs map with patients’ profiles and health domains?
By addressing these research questions, this study aims to contribute valuable insights into the design, implementation, and optimization of CAs, as supportive tools in managing chronic health conditions. The findings presented in this paper seek to inform healthcare professionals and technology developers about the potential of these digital solutions to empower patients, improve health outcomes, and enhance the overall quality of life for different groups of people living with chronic diseases.
Methods
This study employs a scoping review approach, 31 which provides a comprehensive overview of the evidence on the chosen research topic. Our approach, therefore, is to give a relative breadth in our review rather than to focus on evidence around a single clinical or systematic question.
Search strategy
The review followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) guidelines 32 with the PRISMA-ScR checklist available as a Supplemental Material. We conducted a search of the literature using the electronic databases PubMed, ACM Digital Library, Scopus, and IEEE Xplore. These databases were chosen as they cover relevant aspects of health, technology, and interdisciplinary research and have also been used in other reviews covering similar topics. The main keywords used were “conversational agent” and “health” which were searched in titles and abstracts (Table 1).
Search terms.

Study selection criteria
The review is based on literature dated between the beginning of January 2018 and the end of January 2023 published in English with full text available. We included articles on chronic disease management (e.g., treatment or monitoring) and prevention of specific chronic diseases. Articles that addressed general well-being were not included. Articles must provide some description of the theoretical basis, choice of the intervention components, or CA development process. We included both quantitative and qualitative studies, without any constraints on approach. Studies employing experimental designs that involve group comparisons must include details about the comparators used. Studies focusing only on technical aspects and design features of CAs (e.g., language models, systems, chatbot's personality) and studies using the Wizard of Oz method weren’t included.
Conversational agents
The review considers studies that involve interventions provided by a CA. This review does not include studies where CA focuses on video- and image-based diagnosis (e.g., skin cancer, gait, correct execution of exercises) and whose aim is screening before appointments, filling hospital forms, checking doctors’ availability, and giving diagnoses from the symptoms provided by the user.
Intervention
This review considers studies that evaluate intervention programs that include strategies to provide educational materials, help achieve health goals, and monitor health conditions. Interventions must not be intended for a hospital setting but can be tested in a laboratory environment. The intervention must be directly targeted toward the patients (e.g., not for emergency medical services, clinicians, or medical students).
Validity
This review considers studies that were tested on targeted user groups and have a report on the interventions’ impact on participants and/or participants’ experiences with the CA. Additionally, articles must have evaluation or validation of outcomes (e.g., acceptability, effectiveness) measured by reliable tools.
Results
The literature search process from the four databases resulted in a total of 3151 research papers. The steps of the screening methodology are presented in Figure 1, along with the number of studies that were excluded in each step. The first step consisted of removing duplicate records of common studies that were found across all databases using the reference manager Zotero, which resulted in 2406 unique articles. All remaining unique studies were then considered in the initial title- and abstract-based screening. Following the proposed exclusion criteria described above, 409 articles remained. Full-text assessment of the remaining papers was then performed, resulting in a final list of 42 articles. The most relevant exclusion factor was validity, as many studies included only preliminary methods and results or presented CAs without any evaluation results (e.g., studies at the pre-pilot stage), or CAs that were evaluated with subjects different to the intended population.
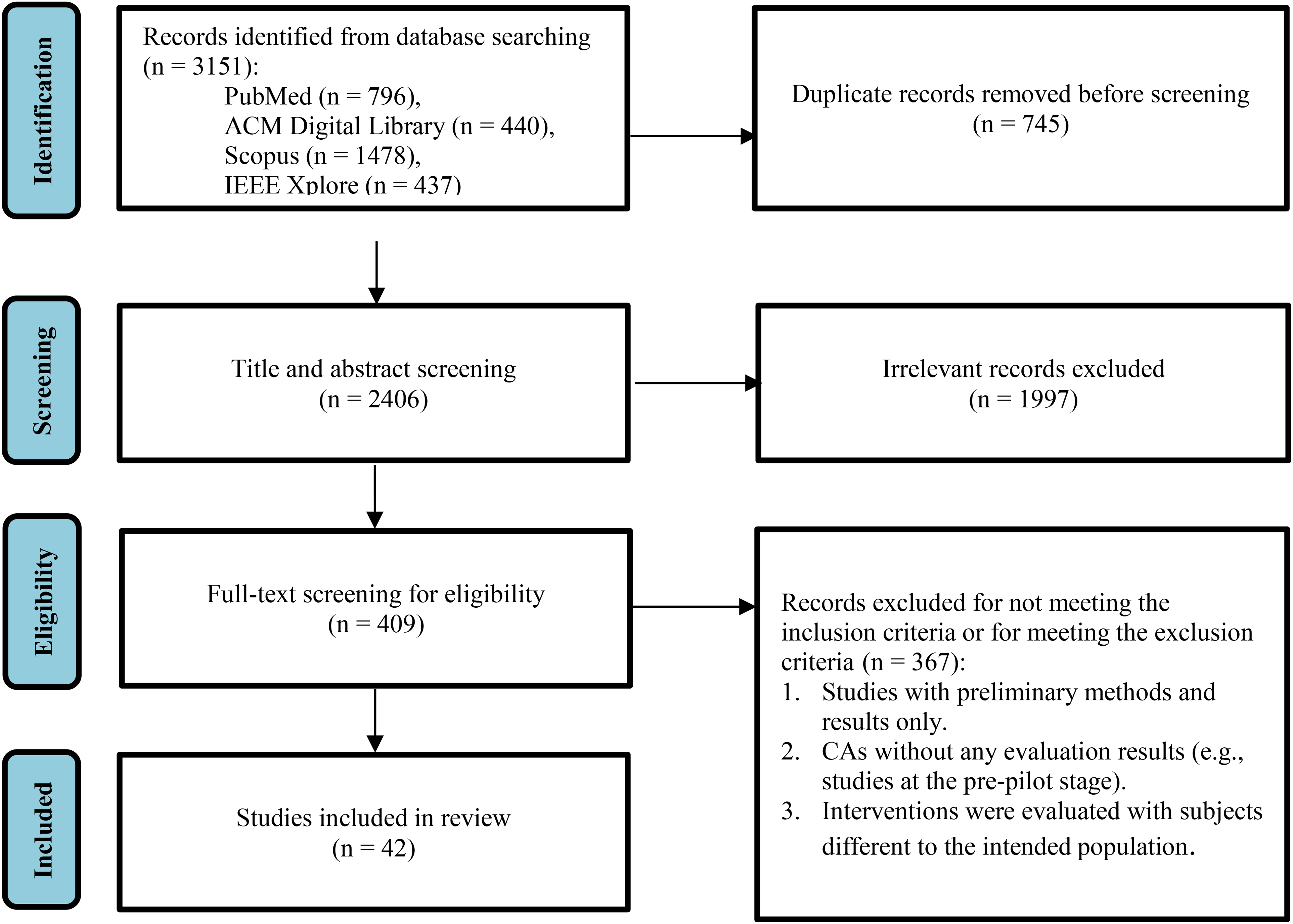
PRISMA-ScR 32 flow diagram of included studies.
Characteristics of included studies
The full list of included studies is provided in Tables 2–7. Article publication dates ranged from 2018 to 2023. Eighteen studies were conducted in the USA,8,10,33–48 three each in Switzerland49–51 and China,52–54 two each in Australia,55,56 France,57,58 and the UK,59,60 and one each in Canada, 61 Japan, 62 Singapore, 63 Saudi Arabia, 64 South Africa, 65 India, 66 Germany, 67 Italy, 68 Norway, 69 Spain, 70 the Netherlands, 71 and across Europe. 72 The total number of participants ranged from 6 to 4737 and one study 69 didn’t provide information on participant numbers. Participants aged between 5 and 86 years but not all articles provided information on age ranges.
Health domains and targeted users’ characteristics.

PHQ-9 score equal to or greater than nine was decided according to the average inclusion PHQ-9 score in previous depression trials. 54
Studies’ characteristics.

Note. N/R: not reported; BMI: body mass index; HCP: healthcare professionals; SCD: patients with sickle cell disease; T1D: type 1 diabetes; T2D: type 2 diabetes; AA: African American; ECA: embodied conversational agents. AEC: association between program engagement and the change in HbA1c, FBG, and PPBG levels; AEI: adherence, engagement, and interaction; CCP: comparison of the average scores obtained by the chatbot and by the physicians for each individual; EIQOL: efficacy of the intervention with regard to the participants’ quality of life; FDBT: frequency of coping via dialectical behavior therapy skills; HL: health literacy; HO: health outcomes; HRQOL: health-related quality of life; IHR: impact on healthcare resources (number of medical appointments per month for each patient); IMCB: intention and motivation to change behavior; MA: medication adherence; SS: social support; SP: self-perception on the importance of drug abstinence and confidence in stopping the drug use; TA: therapeutic alliance; UIN: users’ informational needs; UX: user experience.
A cut-point of >1 on the CAGE-AID (cut down, annoyed, guilty, eye opener-adapted to include drugs) has a sensitivity of 70% and specificity of 85% for identifying individuals with substance use disorders. 33
BMI between 25 and 29.9 kg/m2 falls within the overweight range, and BMI 30 kg/m2 or higher falls within the obese range. For the Asian and South Asian populations, overweight is when BMI is between 23 and 24.9 kg/m2, and obesity is when BMI is greater than 25 kg/m2. 73
Parents were requested to provide information on any instances of their child being hospitalized or seeking medical attention for depression or anxiety-related issues in the preceding 2 weeks up to 1 month.
PHQ-9 assesses depression symptoms; scores of 5–9 predominantly represented patients with either no depression or subthreshold depression; patients with scores of 10 and higher are more likely to be diagnosed with depression. 74
Number of people accessing the service and their demographic characteristics (age, gender, and language preferences).
CAs’ purposes in the selected studies.

Factors impacting CA’s role in self-management.

Note. The table includes only studies that contain at least one of the discussed components. N/R: not reported; T1D: type 2 diabetes; HCP: healthcare professionals.
Underpinning frameworks in the selected studies.

Note. N/R: not reported.
CAs’ technical characteristics in the selected studies.

Note. ECA: embodied conversational agents; RA: relational agent; VA: voice assistant; UC: unidirectional coach.
What are the health domains and the characteristics of the users, targeted for CA interventions?
When creating technology for a specific health domain, it is essential to consider symptoms, treatment requirements, and challenges associated with that domain that people may encounter at different stages. Moreover, understanding users’ characteristics, such as demographics, medical history, cultural background, goals, and preferences, allows the content and interaction strategies to be tailored. This enhances engagement, adherence, and overall health outcomes.75,76 Table 2 shows information about the health domains addressed by the CAs in the selected articles, providing the context of the disease, including phase, e.g., prevention, after-care or during (between onset and end of the disease), as well as information about the target users.
Health domains
Among the various types of chronic conditions, different types of diabetes (type 1, type 2, gestational diabetes, and prediabetes)47,55,56,63,65,66,68,69,71 and mental health issues (depression, depressive symptoms, anxiety, bipolar disorder, and other complex, difficult-to-treat mental disorders)38,45,46,53,54,60 received the most attention. Other types of chronic conditions included six studies on cancer (multiple myeloma, breast cancer, cancer genetic evaluation, and after cancer treatment),37,39,48,57,58,67 four studies on addictions and substance abuse (smoking cessation, alcohol and methamphetamine use disorder, and substance misuse),33,34,36,52 four studies on cardiovascular disease (heart failure and atrial fibrillation),8,35,40,61 three studies on obesity,44,51,59 two studies on chronic pain,49,62 and one study each on asthma, 50 autoimmune (celiac disease), 64 genetic condition (sickle cell disease), 72 and functional bowel disorder (irritable bowel syndrome). 42 Additionally, there were four studies focused on comorbid diseases: two on musculoskeletal conditions and mental health,10,43 one on type 2 diabetes and depressive disorder, 70 and another one on obesity and cancer. 40
Most of the systems were aimed at supporting people who already have chronic diseases (37 studies). There were only three studies that highlighted their focus on prevention: one study focused on patients without cancer who were eligible for cancer genetic evaluation, 37 one on communicating breast cancer risk and the recommended medical guidelines to healthy women, 48 and another on promoting healthy lifestyle behavior changes with the focus on diabetes and prediabetes knowledge in the general population. 63 Two studies focused on after-disease care: one study concentrated on overweight or obese cancer survivors 41 and another on young people after cancer treatment. 39
Targeted users’ characteristics
In the selected studies, people with chronic conditions, or the risk of acquiring one were the most common final targeted interaction recipients. Only three studies targeted the interaction of patient–parent dyads.47,50,59
The age groups of target users varied. There were six studies focused on children and teenagers.45,47,50,51,59,71 Four studies targeted young adults.38,39,53,54 The remaining 32 studies were for different groups of adults.
There was no information about the duration of illness, medication usage, number and type of comorbidities, employment and marital status or any other socio-demographic information of target users that might be important for intervention development. Only a few studies were targeted recipients additionally specified; two studies targeted university students,38,54 one study focused on veterans, 34 one specifically targeted African American/Black women, 44 and one had a focus on workers. 62
What are the characteristics of the CA studies?
When conducting studies, it can be meaningful to test interventions with multiple study arms to compare them, evaluate their efficacy and inform decision-making. Conducting studies with participants representative of the target group enhances applicability and generalizability that improves the validity and relevance of findings for the interventions’ intended users. Knowing the intervention duration can be important for the understanding of the impact and effectiveness of the interventions. Moreover, chosen measure types guide the evaluation of health apps, ensuring evidence-based interventions and objective outcome assessment. Thus, effectiveness, a fundamental aspect of intervention assessment, can be measured through various outcome indicators chosen by researchers, such as symptom reduction, changes in health behavior and health indicators (e.g., blood pressure, glucose levels), improvements in quality of life, and others. These measures serve as quantifiable evidence of an intervention's success in achieving its intended goals. The characteristics of the studies are summarized in Table 3. If there were multiple race groups participating in the study, we mention only those above 20%. We reported gender and sex as explicitly stated in the studies. If the totals do not add up to 100, it means this information was not provided in the studies.
Participants
The age of the research participants corresponded to the targeted users’ descriptions since this was a criteria for inclusion in the review. There were six studies focused on children and teenagers aged from 5 years to 18 years old.45,47,50,51,59,71 Four studies targeted young adults, 17–29 years old.38,39,53,54 One study had a wide range age of targeted users and participants from 13 to 65+ years old. 58 The remaining 31 studies involved different groups of adults. Three studies didn’t provide any information about participants,64,67,69 except that they corresponded to the target users, e.g., already had the health condition or risk of acquiring the disease. Moreover, one of these studies, Baertsch et al., 67 besides patients, had healthcare professionals and caregivers among the users since the program was advertised and had open access.
Apart from age, gender, or sex was frequently mentioned in the articles as a demographic characteristic of the participants. There were 17 articles that used the term “gender,” 12 that used the term “sex,” 2 that used both terms, and 11 did not specify. Unfortunately, it is often impossible to determine exactly what researchers meant when they used a particular term. Furthermore, some of the articles provided additional information on specific health indicators, such as body mass index (BMI) or disease duration, employment and marital statuses, race, and ethnicity. Having a more detailed description provides valuable insights for understanding the diverse demographics and health profiles of the participants, allowing conducting in-depth analysis of the interventions’ effectiveness and relevance across different populations.
Duration
There were two studies with unspecified duration.67,68 Of those with specified domains, there was one study 69 that collected data over 20 weeks (there were two periods: 8 and 12 weeks), though it is not clear for how long and how many times each user engaged with the chatbot since the data were anonymous and the identification of users was not permitted. Five studies took only 1 day to finish the planned intervention.37,48,52,57,72 Two studies each were for 1 week and 2 weeks, nine studies were about 1 month long, seven studies had a 2 month duration, and eight studies had a 3 month duration. Several studies lasted more than 3 months: two studies for about 4 months,54,66 one study for 5.5 months, 51 one study for 9 months, 70 and 3 studies for 1 year.55,56,58
Study arms
Most of the studies were single-armed (22/42). There were 15 two-arm studies, 11 of which compared intervention and control groups (see Table 3), including five that compared intervention and usual care,40,44,51,56,62 four that compared immediate intervention and waitlist control groups,33,39,42,45 and two compared intervention and control groups with no treatment.59,64 Another setup encountered is a comparison of two alternative interventions: responses from chatbot versus responses from physicians, 57 interaction with a chatbot concerning pain management versus reception motivational messages unrelated to chronic pain, 49 bibliotherapy versus chatbot interaction, 54 and smart speaker versus visually animated and voice-enabled avatar interaction. 35 There were also five three-arm studies, that compared an e-book, a general chatbot, and mental health chatbot 53 ; control group that only received a link to a book, 2 and 4 weeks intervention groups 38 ; control version, adaptive, and non-adaptive embodied conversational agent (ECA) 48 ; control group that received printed written information, smart speaker, and text-based intervention 41 ; and usual orthopedic care without any specific mental health intervention, usual orthopedic care with in-person psychological counseling and usual orthopedic care with digital mental health intervention. 43
Measures
A diverse range of measures was used to assess the interventions in the selected studies. One of the most common measures were health outcomes (23/42) which were measured by physical assessments like BMI, glycated hemoglobin level, blood pressure, and heart rate,44,51,56,59,66,70 and questionnaires, such as Generalized Anxiety Disorder-7, Patient Health Questionnaire-9, International Physical Activity Questionnaire, Pittsburgh Sleep Quality Index, and Perceived Stress Scale.33,38,39,42–46,49,51–54,56,59,60,62,63,65,68,70–72 All the studies demonstrated improvement, but not always statistically significant.
The same metrics are often used to evaluate engagement, adherence, and interaction with apps and CAs, e.g., number, lengths and context of messages sent, and this can create challenges in distinguishing the specific aspect being assessed. Among the selected studies, 26 evaluated chats with CAs and activity in the apps (we called this measure Adherence, Engagement, and Interaction in Table 3), which was measured by a variety of methods, including analysis of interview transcripts, 8 chat transcripts and metrics, e.g., number and length of messages,35,37–40,45,49,51,53,56,58,60,62–64,69,70 app usage, e.g., number of accesses to the app and videos watched,42,44,45,56,70 different questionnaires, e.g., Godspeed for assessing human-like traits of CA, 36 the Usefulness Scale for Patient Information Material for evaluating perceived usefulness 72 and the User Engagement Scale–Short Form questionnaire for measuring self-reported user engagement, 68 and other surveys to evaluate various aspects, e.g., the level of confidence, attitude, and perceived quality of the answers.39,47,54,57,58 Many metrics based on chat and app usage provided quantitative values that were evaluated relative to each other, such as the number of messages sent weekly. The results indicated that participants found the CAs to be useful, reported overall positive attitudes, and showed high engagement and adherence rates. All other 26 measurements identified were used in fewer than 13 articles.
Effectiveness
Most of the studies didn’t talk explicitly about the effectiveness. It can be assumed that effectiveness of the intervention is determined by the results of the selected measures, as noted in the previous paragraph, such as health outcomes, usability, and engagement. However, there are several articles that mentioned why they didn’t provide information about effectiveness; some of the studies weren’t designed to test the effectiveness, 63 other couldn’t establish it for different reasons, e.g., the small sample size and/or insufficient intervention duration.45,46,51,59,60
Do CAs address continuum of care and patient work concepts for self-management? Do CAs adapt to the changing needs of users?
CAs play a multifaceted role in chronic disease management, addressing the continuum of care by providing, for example, education, remote monitoring, and seamless health records integration that can enable access to comprehensive patient data that contributes to creating personalized and tailored interventions. CAs contribute to patient work through symptom tracking and coaching, empowering patients and caregivers to self-manage their health. Moreover, human involvement, e.g., relatives, peers, and healthcare professionals, in chronic condition management can provide social support and motivation for patients, enhancing adherence to the interventions and overall well-being.77,78 Furthermore, the inclusion of medical records in health applications can facilitate the development of personalized interventions, resulting in enhanced health outcomes, greater user engagement, and heightened satisfaction.
The purpose of the reviewed CAs are presented in Table 4 and the factors impacting CA's role in self-management are shown in Table 5 for any study that mentioned the CA's factors.
CA purposes
In the selected studies, CAs had a diverse range of purposes. The most common ones were providing information and education (33/42), delivering cognitive therapy (12), and providing mental health and emotional support (11) (see Table 4). All other purposes, such as providing feedback, collecting data, sending reminders, and motivational messages and monitoring symptoms, were mentioned fewer than six times.
CA personalization
Twenty-five CAs didn’t adopt message content to users’ characteristics at all (see Table 5). Five studies mentioned that CAs sent “personalized text messages” and “tailored replies depending on users’ responses” without further explanation.49,56–58,62 In one study participants can choose to receive more or less details on the topics based on their preferences. 37 Based on participants’ goals, habits, and data entered during a conversation with CA, four CAs provided personalized feedback,36,44,50,71 and four CAs sent personalized educational, motivational, and coaching messages.41,55,61,66 One CA tailored the conversation to the user's present situation and to the reported need at that moment, 45 one CA referred to earlier data entered, tasks, or activities performed and added user's name 72 and another CA added user's name and appropriate time context to the messages, e.g., “Good Afternoon John.” 40
Medical records
We have only considered the usage of medical records in conjunction with the CAs. For example, cases when medical records were used for recruiting participants are not demonstrated in Table 5. Thirty studies didn’t mention any connection to patients’ medical records (see Table 5). Nine studies used medical records data for the studies.10,35,37,40,41,43,56,61,66 One study recorded information after the study to participants’ electronic health record (EHR) 37 and one study used participants’ medical charts to confirm any additional mental health diagnoses and record their initial treatment plan. 45 Moreover, one study aimed to integrate the findings in existing patient web portals that support the care of patients with type 1 diabetes, 71 and one study noted the possibility of integrating the chatbot's administration panel into the existing EHR system. 38 One study collected medical history and stored it in the app when the patient was onboarded to the program 61 and one study stored personal health record files with additional diabetes-related information (e.g., laboratory reports and details of treating physician) that users logged in the mobile application. 66 Among these 12 studies, there were three on diabetes,56,66,71 three on cardiovascular conditions,35,40,61 two on mental health,38,45 two on comorbid chronic pain and mental health,10,43 one on cancer, 37 and one on comorbid cancer and obesity. 41
Human involvement
Despite the evidence that human involvement, e.g., family members, peers, and healthcare professionals, in the management of chronic conditions can offer patients social support and motivation,77,78 in 31 studies there was no human involvement in the intervention groups (see Table 5). Four studies allowed the participants to communicate with health experts, two studies only through chat,10,43 one through chat and face-to-face interaction 50 and one through chat and voice calls. 66 In three studies, healthcare professionals monitor participants’ engagement and results.35,52,70 In one study, healthcare professionals could intervene by telephone (Mental Assistance Hotline) when the participants reported that they needed emergency psychological assistance 54 and in another study, the app alerted healthcare professionals in case of a lack of chat interaction during more than 2 days and four standardized counseling on-site visits, two via phone and 10 minutes of interaction through chat app was included. 51 Family members were included in one study by Kowatsch et al., 50 CA could send SMS text messages to them, and healthcare professionals had a possibility to communicate with family members through the app. In Stasinaki et al. 51 patients were able to chat with each other and in Klaassen et al. 71 there was a message exchange between patients, their peers, and their caregivers. In two of the studies without human involvement the CA motivated users to join online peer-support patient communities or request health coaching from a human 72 or search for local support groups. 67
The targeted health domains for the studies with human involvement were diabetes,66,71 comorbid chronic pain and mental health,10,43 mental health, 54 comorbid diabetes and mental health, 70 asthma, 50 cardiovascular conditions, 35 addictions and substance abuse, 52 cancer, 67 and obesity. 51
What are the CAs’ characteristics? How do different types of CAs map with patients’ profiles and health domains?
Choosing or designing CAs suitable to target users requires an understanding of their characteristics, such as type of CA, input and output modalities, as these influence the user experience and engagement. The input modality refers to how users interact with the CA, such as through text, speech, or by choosing from the responses menu, while the output modality relates to the CA's responses, whether in text, speech, or visual forms. Moreover, different types of CAs have unique capabilities and advantages. For instance, relational agents focus on building and maintaining long-term, social–emotional relationships with users, fostering a sense of trust and empathy 79 ; ECAs have the same properties as humans in face-to-face conversation, including producing and responding to verbal and nonverbal communication 80 ; and task-oriented dialogue agents are designed to perform a specific function or deliver a particular service, such as providing educational tutorials. These agents are different from general-purpose CAs, which are more versatile and capable of handling a wide range of tasks and conversations. 81
Theoretical frameworks are essential when developing health interventions and applications as they provide a structured and evidence-based foundation, guiding the design, implementation, and evaluation process to ensure effectiveness and alignment with established health behavior principles.
Underpinning frameworks are presented in Table 6 and CAs’ technical characteristics are in Table 7.
Theoretical frameworks
One-third of all the studies (14/42) did not mention any theoretical base on which the interventions and the application design were based (see Table 6). The rest of the studies had a lot of variety in the theories, therapies, techniques, and frameworks that were considered when developing the studies. A total of 40 different theories were mentioned, with cognitive behavioral therapy, mindfulness (includes training and all mindfulness-based therapy and techniques), motivational interviewing (includes brief motivational interviewing), dialectical behavior therapy, behavior change techniques, and self-determination theory being referenced most frequently (10, 6, 5, 4, 3, and 3 times, respectively), with the remaining 33 theories having no more than two mentions each. All the frameworks can be categorized into several domains: psychotherapy and counseling theories (acceptance and commitment therapy, cognitive behavioral therapy, dialectical behavior therapy, emotionally focused therapy, interpersonal psychotherapy, motivational enhancement therapy, solution-focused brief therapy), health behavior change theories (behavior change techniques, goal setting theory, self-determination theory, social cognitive theory, stress and coping theory, theory of planned behavior, transtheoretical model), educational and learning theories (adult learning theory, cognitive theory of multimedia learning, experiential learning theory), healthcare models and guidelines (American Association of Diabetes Educators (AADE) framework, chronic care model, chronic-disease extended model, obesity-related behavioral intervention trials framework, US Clinical Practice Guidelines, World Health Organization's handbooks on how to implement text-based mHealth interventions), mind-body techniques (mindfulness techniques, sleep meditations, deep breathing techniques), technology and digital health frameworks (digital persuasion model, persuasive system design model, technology acceptance model).
CAs’ characteristics
The majority of CAs in the reviewed studies were text-based (28 out of 42) (see Table 7). Seven CAs only allowed users to choose an answer from the options provided46,51,62,63,65,70,72 and three CAs had several free text questions, e.g., provide the user's name.37,49,50 Among these CAs, four sent media, like audio lessons and pictures with exercises, to users.49,62,63,65 In three studies, participants could type their responses freely39,57,60 and, in Liu et al., 54 participants could also send voice messages to the chatbot. In six CAs, users could both choose responses from a menu and send free text messages or choose from the responses menu.10,38,43,58,68,69 Six studies didn’t specify users’ input format.33,42,45,53,64,66 There were three studies with unidirectional coaches where the CAs sent messages to the participant, but the participant could not communicate with the agent.41,44,71 Four studies based their intervention on Amazon's Alexa,35,59,61,67 including one that compared Amazon's Alexa with a visually animated and voice-enabled avatar. 35 Additionally, one study compared unidirectional coach with Amazon voice assistant. 41 Ten studies used an ECA to provide interventions,8,34–36,40,47,48,52,55,56 the users’ input modes varied: most systems allowed interaction with the ECA only with predefined answer options,8,48,52 while others allowed voice and/or free text messages.36,55,56
Among the selected studies, there were five with relational agents designed to build and maintain long-term emotional relationships with their users.33,40,45,47,60 Three of them were text-based for mental health and addictions and substance abuse33,45,60 and two were ECA targeting diabetes and cardiovascular issues.40,47
Discussion
Advancements in technologies have facilitated a plethora of mobile apps specifically designed to support and improve health habits that give patients more control and a sense of agency, empowering them to take charge of their health. 82 Existing digital technologies for patients with chronic conditions face challenges in adapting to changing health needs and goals, requiring diverse information and recommendations for specific subgroups. 13 Implementing adaptable digital systems can enable sustained app usage, supporting individuals in effectively managing their health and reducing disruption caused by switching between different apps.
Relevant studies were obtained from the PubMed, ACM Digital Library, Scopus, and IEEE Xplore databases. The methodology adopted in this review aligned well with the PRISMA-ScR guidelines and checklist 32 process, see the Supplemental Material for further details. The review included 42 studies reporting interventions delivered by CAs, targeting chronic diseases. Diabetes, mental health, and cancer are the diseases most commonly targeted by CA interventions, as opposed to other chronic conditions, such as autoimmune, genetic conditions, functional bowel disorders, and asthma. The review shows that current CAs address a wide variety of chronic diseases. Although it provides valuable insights, the extensive range of conditions complicates the ability to compare them within and between conditions. To address this, future research should focus on evaluating CAs specifically tailored to particular chronic diseases.
The overall trends can be summarized as follows:
Focus on stable chronic condition management
The analysis reveals that the majority of studies have primarily targeted individuals who already have chronic diseases. There seems to be a disproportionate emphasis on stable chronic condition management rather than on other stages of the disease where people might have other needs, for example, newly diagnosed patients or patients after crises. Only one study mentioned it was designed to address current and future patients’ needs. 58 This finding highlights a potential gap in leveraging digital interventions that adapt to the changing needs of people with chronic diseases, which could significantly impact the overall burden of these conditions on healthcare systems.
Limited representation of specific demographics
The research highlights the lack of studies focusing on certain demographic groups, including children/teenagers and older adults, which aligns with previous reviews. 22 While interventions for adults aged 18 and above are relatively abundant, there is a noticeable gap in providing support for younger and older populations. Understanding the specific challenges and requirements of these groups is crucial for designing age-appropriate and inclusive digital health solutions.
Incomplete participant information
For this review, we selected studies featuring participants who matched the targeted user group. Yet, there is often limited information about the participants beyond basic demographics such as age and gender or sex. Since studies sometimes did not explicitly report all values beyond the primary gender or sex and the terms “gender” and “sex” can be used interchangeably, with “gender” increasingly used to describe biological variations traditionally assigned to “sex,” 83 comparing these studies becomes challenging. Marital status, ethnicity, and other socio-economic features are often missing. Moreover, studies failed to provide a thorough comprehension of participants’ needs, aligning with the previous reviews.22,28 This lack of comprehensive participant information might hinder a thorough understanding of the interventions’ applicability and effectiveness across diverse populations.
Importance of human involvement
While CAs offer promising directions, the limited provision for human interaction within these systems is identified as a potential drawback. Human support from healthcare professionals, family members, and peers with similar health problems can provide emotional encouragement, motivation, and vital insights that are essential for successful long-term management of chronic conditions.77,78
Limited integration of medical records
The review indicates that limited use of medical records by the CAs potentially hinder smooth communication and collaboration between individuals and healthcare professionals. Moreover, medical records in health apps can enable the creation of personalized and tailored interventions that lead to improved health outcomes and increased user engagement and satisfaction.
Insufficient information on theoretical framework
Several studies didn’t provide information about the theoretical framework guiding the design and implementation of interventions. This omission raises concerns about the basis for the interventions and highlights the importance of incorporating robust theoretical foundations in future research and development.
Lack of unified evaluation measures
In accordance with prior reviews, we also found that the evaluation measures used to assess the effectiveness of the interventions and their impact on chronic conditions varied widely across studies.15,28 This lack of standardization makes it challenging to compare and generalize findings.
Limited use of technologies and user information
There is potential for CAs to assist people in actively managing their conditions instead of passively consuming information. However, most current CAs have dialogue management systems that do not consider user preferences, goals, or history of interaction with the system. To better serve user needs, the design of these agents should evolve. The linguistic data generated by users during interaction with CAs holds the capacity to provide insights into users’ emotional and physical states. These data can help people with self-management and provide valuable information for the patients’ support team. A scoping review on psychology-oriented ECAs revealed that most agents were still in their initial phases of development and evaluation, 23 aligning with our results. A systematic review on health-related CAs with unconstrained language input capabilities found limited use of agent-based systems capable of handling complex dialogues and allowing users to lead conversation. 28 The review found only one study evaluated such systems in health contexts, but agents weren't designed for health-related queries. The authors indicated the requirement for large training datasets as a major drawback, potentially slowing their adoption in health applications.
Another factor to consider is that, at the time of writing, advances in the application of large language models offer significant opportunities in various fields, including healthcare. However, this has not yet been reflected in the available literature. It will be interesting to observe how this technological progress could potentially address the highlighted issues.
Strengths and limitations
The main strength of this review is its novelty. To the best of our knowledge, this is the first scoping review addressing different types of CAs in chronic disease management with no constraints on demographics. Nevertheless, it is essential to acknowledge that this analysis has its limitations. First, given that the research question is very broad, a detailed review of the use of CAs in different chronic diseases was not possible. Second, the review was exclusively focused on text and voice CAs, omitting those utilizing images and video. Third, we included articles in English with full text available only and the search in other databases, such as CINAHL and Web of Science, was not conducted. Fourth, our analysis only incorporated features, e.g., theoretical frameworks, explicitly mentioned in the articles. Therefore, certain characteristics may not be fully represented in our review, potentially limiting the generalizability of the conclusions due to potential bias.
Conclusions
This paper highlights the current state of CAs for chronic condition management and raises important considerations for future research and development in this field. The findings emphasize the health application requirements to adapt to the changing needs during the course of illness that varies for each patient and changes over time, customize interventions based on specific user subgroups, and improve the reporting of study participant characteristics to enhance the applicability of the findings. It also underscores the importance of incorporating human support and medical records integration within digital health solutions to provide more effective care for individuals living with chronic conditions. Additionally, studies should clearly articulate the theoretical frameworks guiding their interventions, and efforts should be made to standardize evaluation measures to facilitate meaningful comparisons between studies. Future research could more closely explore studies on each particular disease to gain a deeper understanding of CAs’ use and potential in disease management.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076241277693 - Supplemental material for Exploring the characteristics of conversational agents in chronic disease management interventions: A scoping review
Supplemental material, sj-docx-1-dhj-10.1177_20552076241277693 for Exploring the characteristics of conversational agents in chronic disease management interventions: A scoping review by Ekaterina Uetova, Lucy Hederman, Robert Ross and Dympna O’Sullivan in DIGITAL HEALTH
Footnotes
Acknowledgments
We would like to thank Róisín Guilfoyle, research support librarian at Technological University Dublin, for her assistance and guidance in this research.
Contributorship
Ekaterina Uetova researched literature and wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This work was conducted with the financial support of the Science Foundation Ireland Centre for Research Training in Digitally Enhanced Reality (d-real) under Grant No. 18/CRT/6224 and the ADAPT SFI Research Centre for AI-Driven Digital Content Technology under Grant No. 13/RC/2106_P2. For the purpose of Open Access, the author has applied a CC BY public copyright license to any Author Accepted Manuscript version arising from this submission.
Ethical approval
Ethical approval was not required as this is a review paper.
Guarantor
Ekaterina Uetova.
Reporting guidelines
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.