
Abstract
Objective
To evaluate the immediate learning outcomes of an AI- and sensor-integrated cardiopulmonary resuscitation (CPR) retraining system (Intelligent Practical Training System, IPTS) with conventional face-to-face retraining in healthcare professionals.
Methods
We conducted a randomized trial of 136 healthcare professionals, allocated 1:1 to a 30-minute IPTS or face-to-face groups. IPTS integrates AI and sensors to enable instructor-free learning and examiner-free assessment. Learning outcomes were measured objectively using the manikin, without providing any feedback or assessment results to participants. Primary outcomes were chest compression depth (CC) accuracy and CC rate. Secondary outcomes included tidal volumes of the two rescue breaths and CPR self-efficacy.
Results
No evidence supports the superiority of IPTS in CC depth accuracy (P_adj = .878) or CC rate (P_adj = .729). However, the IPTS group achieved significantly superior rescue breath quality (first: rank-biserial r = −.585, 95% CI [−0.737, −0.416], P_adj < .006, large; second: rank-biserial r = −.512, 95% CI [−0.687, −0.323], P_adj < .006, large), with median values falling within the American Heart Association recommended range (first: 548.99 mL, second: 542.68 mL), whereas the face-to-face group's values were excessively high (first: 806.97 mL, second: 800.23 mL). Both groups showed significant and similar improvements in CPR self-efficacy, indicating comparable psychological benefits.
Conclusion
Under controlled conditions, IPTS did not demonstrate superiority in immediate outcomes for CC quality and CPR self-efficacy compared to sensor-free face-to-face instruction, but achieved superior immediate outcomes for rescue breaths. These results demonstrate the feasibility of a novel integration of AI and sensors in medical education.
Keywords
Introduction
The integration of artificial intelligence (AI) and sensor data enables potential solutions in complex environments. 1 Multisensor systems generate large volumes of heterogeneous data, 2 while transformer architectures have fundamentally reshaped cross-modal tasks in language and vision. 3 The interdisciplinary AI–sensor approach has been widely applied in fields such as autonomous driving, 4 the Internet of Things, 5 and infrastructure monitoring, 6 delivering improvements in closed-loop feedback, precise prediction, and performance assessment. In healthcare, sensors are extensively used for physiological signal acquisition, and integrating AI algorithms translates these signals into quantifiable features while reducing reliance on expert human intervention. Ansari et al. 7 systematically reviewed the applications of transformers and large language models based on multimodal data in electrocardiogram diagnosis, providing evidence of this approach's feasibility.
Although the value of this approach is evident, its feasibility in medical education—especially for sensor-assisted yet instructor-dependent retraining contexts—requires further validation, with cardiopulmonary resuscitation (CPR) serving as a prototypical case. Cardiac arrest remains a substantial public health problem. 8 Successful resuscitation following cardiac arrest requires an integrated set of coordinated actions, and early CPR serves as a critical link in the Cardiac Arrest Chain of Survival. 9 As a technical skill, however, CPR knowledge deteriorates rapidly after training. 10 Periodic retraining is widely acknowledged to improve knowledge retention,11–13 and accredited CPR retraining enhances key metrics—such as chest compression (CC) depth, CC rate, and ventilation quality.12,14,15 The American Heart Association (AHA) has promoted resuscitation quality improvement initiatives emphasizing shorter retraining intervals and spaced learning strategies for healthcare professionals. 12 Although the importance of reinforcing CPR knowledge and practice has been formally recognized, 16 many healthcare professionals lack access to quality learning opportunities once they enter work practice. 17
To enhance learning outcomes and reduce training burdens, a variety of digital educational tools have been used. Studies and guidelines underscore the value of real-time feedback during retraining, 12 with manikins equipped with integrated sensor-based feedback now an established component of CPR retraining. In addition to sensor-based feedback, some studies18,19 involve examiners using scoring scales to assess overall CPR performance, capturing multiple performance domains. 20 Smart devices like smartphones 21 and virtual reality headsets 22 have been employed to develop online CPR teaching tools. However, these alternative methods each present distinct limitations: in-person instructional formats remain reliant on instructors and examiners; purely online applications find it difficult to provide authentic physical feedback; and resource-intensive setups exhibit limited flexibility in special scenarios (e.g., the COVID-19 pandemic).
Recent evidence suggests that applying AI to basic life support (BLS) instruction enhances assessment objectivity and produces standardized, quantitative feedback from both video and audio signals. On the video side, Constable et al. 23 highlighted the need for a data-sharing culture in healthcare professional education and demonstrated the possibility of an automatic clinical assessment tool for BLS based on computer vision and machine learning. Li et al. 24 deployed posture-estimation and object-detection algorithms on automated external defibrillators (AEDs) to assist with real-time standardization of CPR actions. Liu et al. 25 designed a prompt-enhanced hierarchical transformer—comprising a video feature extractor, an action segmentation executor, and a prediction refinement calibrator—specifically for CPR action segmentation. Huang et al. 26 developed SmartCPR, a smartphone-based training system that integrates AI frameworks and trainers to provide training and guidance for high-quality CPR maneuvers. On the audio side, Choi et al. 27 developed Beep-CPR, a novel device that enables a sound recognition-based CPR training system. Nevertheless, the strength of AI lies in its ability to quantify indicators that are difficult to measure directly—such as motion continuity, positional accuracy, and completeness of verbal calls—whereas for core metrics like CC depth and rate, sensor-based measurements remain more robust and reliable than AI.
Integrating sensors embedded in CPR manikins with video- and audio-based AI algorithms—achieving multimodal sensor integration, real-time algorithmic feedback, and automated performance assessment under practical constraints—aligns with the advantages of the interdisciplinary AI–sensor approach introduced earlier. Sensor-based data collection enables the objective measurement of CPR-specific metrics, while AI algorithms can process multimodal data and provide an examiner-free evaluation of overall CPR performance. However, current research primarily focuses on algorithm development and the application of digital educational tools; the effectiveness of this AI- and sensor-integrated format, as well as the differences in learning outcomes compared to traditional face-to-face retraining, remains underexplored.
To address this gap, we conducted a randomized trial in Wuhan, China, to evaluate the effectiveness of the Intelligent Practical Training System (IPTS) in learning outcomes among healthcare professionals. The IPTS is an AI-powered instructional system with manikin-embedded sensors, and it integrates two automated functions: instructor-free learning (including instruction, practice, and feedback) and examiner-free assessment. Its workflow and learning outcome metrics were designed in accordance with the 2020 AHA Guidelines for CPR and Emergency Cardiovascular Care (ECC). 9 In this study, “retraining” refers to enhancing CPR skills and confidence through structured coursework and simulation, rather than time-scheduled refresher training, and the IPTS focused exclusively on CPR retraining rather than broader resuscitation modalities (e.g., defibrillation, advanced resuscitation). We hypothesized that the IPTS, as a digital health innovation, would enhance healthcare professionals’ adherence to CPR guidelines and lead to superior immediate learning outcomes relative to conventional face-to-face retraining.
Materials and methods
Study design and participants
All participants provided written informed consent prior to study initiation. Participants included physicians, nurses, and medical technicians recruited from three tertiary hospitals in Wuhan: Union Hospital, People's Hospital of Dongxihu District, and the Eighth Hospital of Wuhan. In addition, healthcare professionals from community healthcare centers were also invited. All participants were recruited via the messaging and social media application WeChat (Tencent, Guangzhou) and were allocated in a 1:1 ratio between June 6 and June 14, 2024.
The inclusion criteria were as follows: (1) last received CPR training six or more months prior, and (2) did not hold a currently valid CPR certification. Exclusion criteria were: (1) any ICU work experience within the preceding six months; (2) any physical condition that would preclude the ability to perform CPR (e.g., pregnancy, recent fractures); and (3) self-reported inability to use smart devices independently.
Randomization and masking
A random allocation sequence was generated using an online tool (www.randomizer.org). To ensure allocation concealment, the sequence was enclosed in sequentially numbered, opaque, sealed envelopes (SNOSE). Participants were assigned to either the intervention group (IPTS) or the control group (face-to-face) in a 1:1 ratio upon selecting an envelope. Blinding of participants and retraining personnel was not feasible due to the inherently distinguishable nature of the interventions. Outcome assessments were automated and standardized, functionally serving as blinded endpoints.
Intervention
The IPTS comprises an online platform, a Hikvision 6-channel Network Video Recorder, a display screen, a computer, and a manikin integrated with multiple sensors (see Figure 1). The sensors embedded in the manikin are primarily used to collect CPR performance data (e.g., CC depth and rate, ventilation volume, and head-turning actions). AI algorithms—based on human behavior analysis, speech recognition, spectrum analysis, and object recognition (see Appendix A for technical details)—are applied to provide feedback for scene assessment, patient assessment, and effectiveness assessment. In addition, the AI modules analyze the standardization of CPR performance actions such as CC and head-turning, thereby working in conjunction with sensor data to generate more comprehensive feedback items.

Components of the IPTS. (A) Devices included in the IPTS. (B) Manikin with multiple sensors of the IPTS. (C) The workflow and functions of the IPTS.
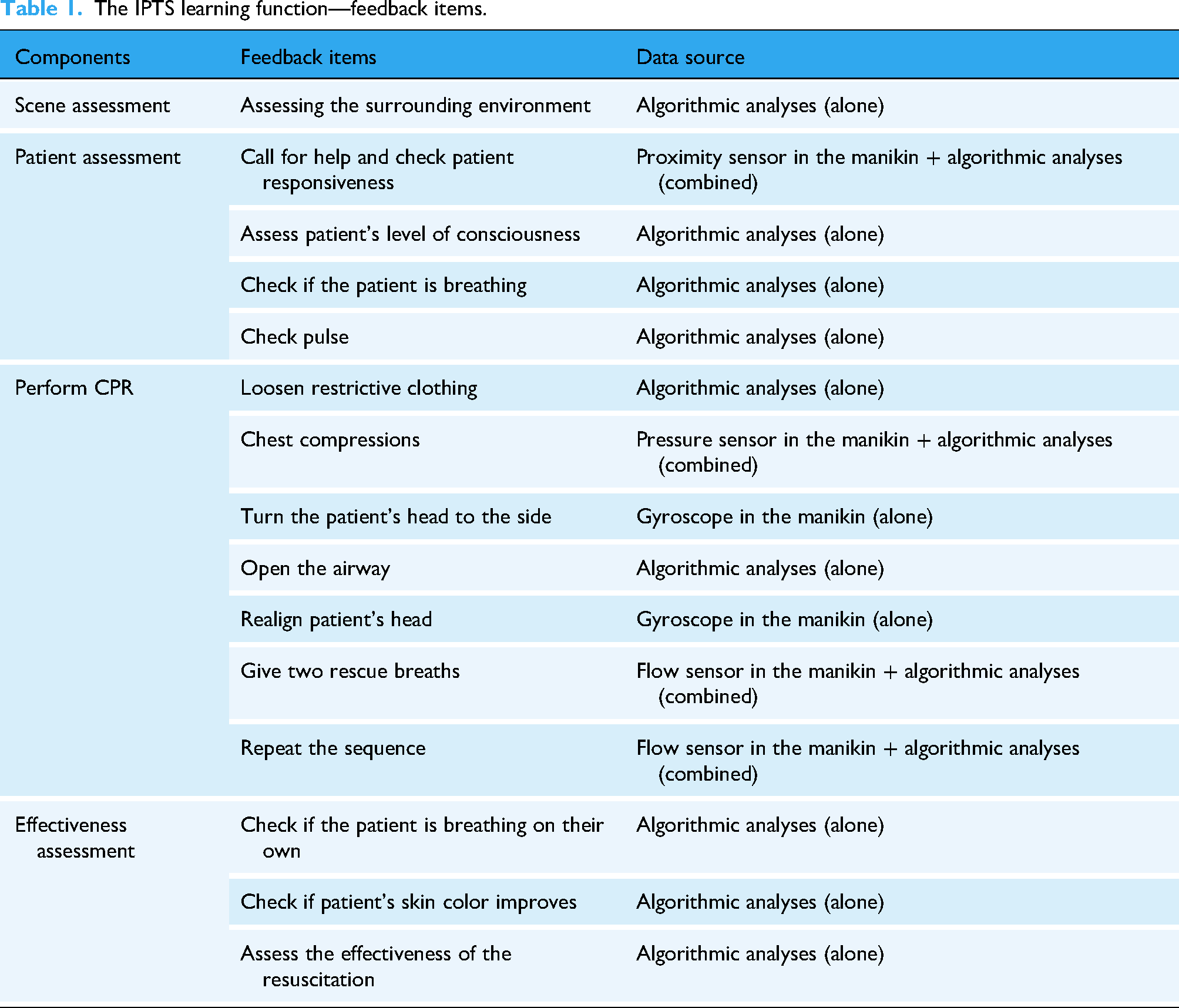
Participants in the IPTS group underwent unsupervised CPR instruction, practice, and feedback via the system's learning function. During retraining, the IPTS delivered step-by-step instructions through sequential videos and voice prompts. Trainees practiced CPR on the manikin while the system automatically generated feedback, displayed it on the screen, and provided video replays of critical actions to facilitate self-review and improvement. The “Feedback items” column in Table 1 presents the indicators, and these are displayed as real-time operational readouts in the learning function (see Appendix B-Figure A1-A,B for the feedback screens).
The IPTS learning function—feedback items.
Study procedure
Baseline assessment and retraining preparation
Following randomization, all participants completed a paper-based baseline questionnaire to collect demographic data (e.g., gender, age) and assess their initial CPR self-efficacy. Subsequently, each participant performed a baseline CPR test on the IPTS manikin without receiving any feedback. The IPTS's assessment function automatically generated item scores as shown in Table 2 and recorded the raw values of indicators such as CC depth accuracy, CC rate, and tidal volume (the assessment screen is presented in Appendix B-Figure A1-C, which was not shown to the participants). Finally, all participants underwent a standardized theoretical course to ensure a consistent knowledge base. This course involved viewing an instructional video provided by the Red Cross Society of China and reading a handbook adapted from the 2020 AHA Guidelines for CPR and ECC. 9
The IPTS assessment function—weighted scoring framework (overall 0–100).

It should be noted that “Overall CPR performance” in Table 2 is defined as an integrated score automatically generated by the IPTS's assessment function. Its data source is consistent with the feedback items in Table 1, but it is calculated as a weighted score. The development of this weighted framework was guided by expert consensus and drew upon established standards, including the AHA's adult CPR skills testing checklist and the 2018 National Consensus on CPR Training in China. A pilot study was conducted (see Appendix C for detailed procedures) involving 112 medical students and four experts, using the average of the experts’ scores as the consensus reference for validating the IPTS assessment function. Key results were as follows: (1) the IPTS showed high assessment consistency across three repeated measurements (one-way repeated measures ANOVA, all P > .05) (Appendix C-Table A2), indicating that the IPTS assessment function was stable and reproducible; (2) the intraclass correlation coefficient (ICC) for overall CPR performance scores among four experts was 0.391 (Appendix C-Table A3), suggesting the subjectivity of scores from different experts and reflecting the inherent limitations of human judgement; and (3) the Pearson correlation coefficient between IPTS and the average of the four experts’ scores was 0.920 (P < .01) (Appendix C-Table A4), indicating that the IPTS closely approximated the consensus component of experts’ scores, whereas its low correlation with Expert 2 (r = .318) suggests that this expert's scores deviated from those of the other experts.
Retraining procedure
In the IPTS group, participants first received a brief orientation on the system's operation and feedback items interpretation. They then practiced CPR independently for a maximum of 30 minutes using the system's learning function. In the face-to-face group, participants received conventional CPR retraining from an AHA-certified instructor (an experienced head cardiology nurse) for no more than 30 minutes. They practiced on the same model of manikin as the IPTS group, but with the learning and assessment functions deactivated. The instructor followed the AHA's Adult CPR Skills Testing Checklist and Skills Descriptors. 28 The retraining comprised a 15-minute demonstration of correct CPR techniques, followed by 15 minutes of supervised practice with verbal feedback and manual correction based on direct observation and stopwatch timing.
Final assessment
Thirty minutes after the intervention, all participants performed a final CPR test under the same conditions as the baseline assessment. They also completed the same questionnaire again to reassess their post-intervention CPR self-efficacy.
Procedure standardization
The following measures were implemented to maintain the quality and objectivity of the study: (1) all participants received an identical theoretical course prior to intervention; (2) each participant completed only one practical retraining encounter, capped at 30 minutes; (3) the face-to-face group was divided into subgroups of no more than six participants, in accordance with the recommended 1:6 instructor-to-trainee ratio 29 ; to align throughput and control the overall study timeline, the IPTS group was also divided into subgroups of up to six participants and deployed seven devices—six for parallel intervention and one as a backup to avoid downtime from equipment failure; (4) the same model of manikin was used for all learning and testing across both groups, with one manikin allocated per participant in both groups; (5) during the baseline and final CPR tests, no feedback or assessment results were displayed to participants.
Outcome measures
The IPTS's assessment function served as the objective data collection instrument for all participants in both groups during the baseline and final CPR tests. To avoid “teaching-to-the-test bias” of the IPTS group, we did not use the score as the outcome. Instead, we prespecified objective, sensor-derived physical metrics and questionnaire data as outcomes.
Primary outcome
CC quality was assessed using data from the IPTS manikin's pressure sensor, with two metrics: (1) CC depth accuracy, with a target range of 5–6 cm—specifically, this refers to the proportion of total CCs that fall within target range, and (2) CC rate, with a target range of 100–120 compressions per minute (min−1). These metrics are recognized as key metrics of CPR performance,18,30 and were assessed in this study following the AHA guidelines.
Secondary outcomes
Rescue breath quality
The quality of rescue breaths, captured by the IPTS manikin's flow sensor, was assessed based on the tidal volume of the two mouth-to-mouth ventilations. In line with AHA recommendations, the target tidal volume was 500–600 mL per ventilation. Previous studies have suggested that ventilation quality during CC is an important component of CPR performance,
31
thus it was included as a key metric in this study.
CPR Self-efficacy
CPR self-efficacy was measured using a nine-item, 7-point Likert scale questionnaire (see Appendix D-Table A5). The instrument assesses two main constructs: (1) recognition and alertness, and (2) CPR performance confidence. CPR self-efficacy refers to an individual's belief in their ability to effectively perform CPR,32–34 and prior research has well supported the significant positive correlation between CPR training and self-efficacy levels.35,36 The CPR self-efficacy scale employed in this study was originally developed by Hernández-Padilla et al. 37 and subsequently revised and validated by Lee et al., 38 who demonstrated its robust validity (0.90) and reliability (Cronbach's α = .85).
Sample size
Previous CPR feedback trials in healthcare professionals have shown substantial improvements in CC depth, including an approximately 20%-point advantage with real-time visual feedback. 38 Because detailed post-training means and standard deviations were not available, a precise standardized effect size could not be calculated from that study. Therefore, we conservatively assumed a moderate effect size of d = 0.5 for sample size determination. Using G*Power software (version 3.1.9.2), we calculated a required sample size of 64 per group, with a two-sided significance level (α) of .05 and a statistical power (1−β) of 0.8. Due to the absence of follow-up stages in our study, we conservatively set the dropout rate at 5% rather than the commonly used 10%. Consequently, to account for this potential dropout, we adjusted the targeted sample size to approximately 68 participants per group (64÷0.95). No separate a priori power calculation was performed for secondary outcomes; the sample size was primarily determined based on the expected between-group difference in CC depth accuracy.
Statistical analysis
All statistical analyses were performed using IBM SPSS Statistics (version 26), after double data entry and validation in EpiData (version 3.0). The normality of distribution for continuous variables was checked using the Shapiro-Wilk test. If normality was confirmed, these variables were presented as means ± standard deviations (SD), and differences were assessed using the independent samples t-test (for between-group comparisons) and the paired samples t-test (for within-group comparisons), with Cohen's d as the effect size measure (95% confidence intervals [CIs] reported). Conversely, non-normally distributed variables were reported as medians [interquartile ranges (IQRs)]. The Mann-Whitney U test was used to examine between-group differences (effect size: rank-biserial r, 95% CIs reported), and the Wilcoxon signed-rank test was used to analyze within-group differences before and after the intervention (effect size: paired rank-biserial r, 95% CIs reported). Categorical variables were expressed as frequencies and percentages [n (%)]. All P-values were adjusted for multiple comparisons using both the Bonferroni and Holm-Bonferroni methods to control for type I error inflation.
Results
Participant flow and baseline characteristics
A total of 164 individuals were assessed for eligibility, of whom 136 were enrolled and randomized in a 1:1 ratio to either the IPTS group or the face-to-face group (n = 68 per group) (Figure 2). Following randomization, 7 participants (5.1%—5 from the IPTS group and 2 from the face-to-face group) were excluded, primarily due to scheduling conflicts. Thus, the final analysis included 129 participants (94.9%): 63 in the IPTS group and 66 in the face-to-face group.
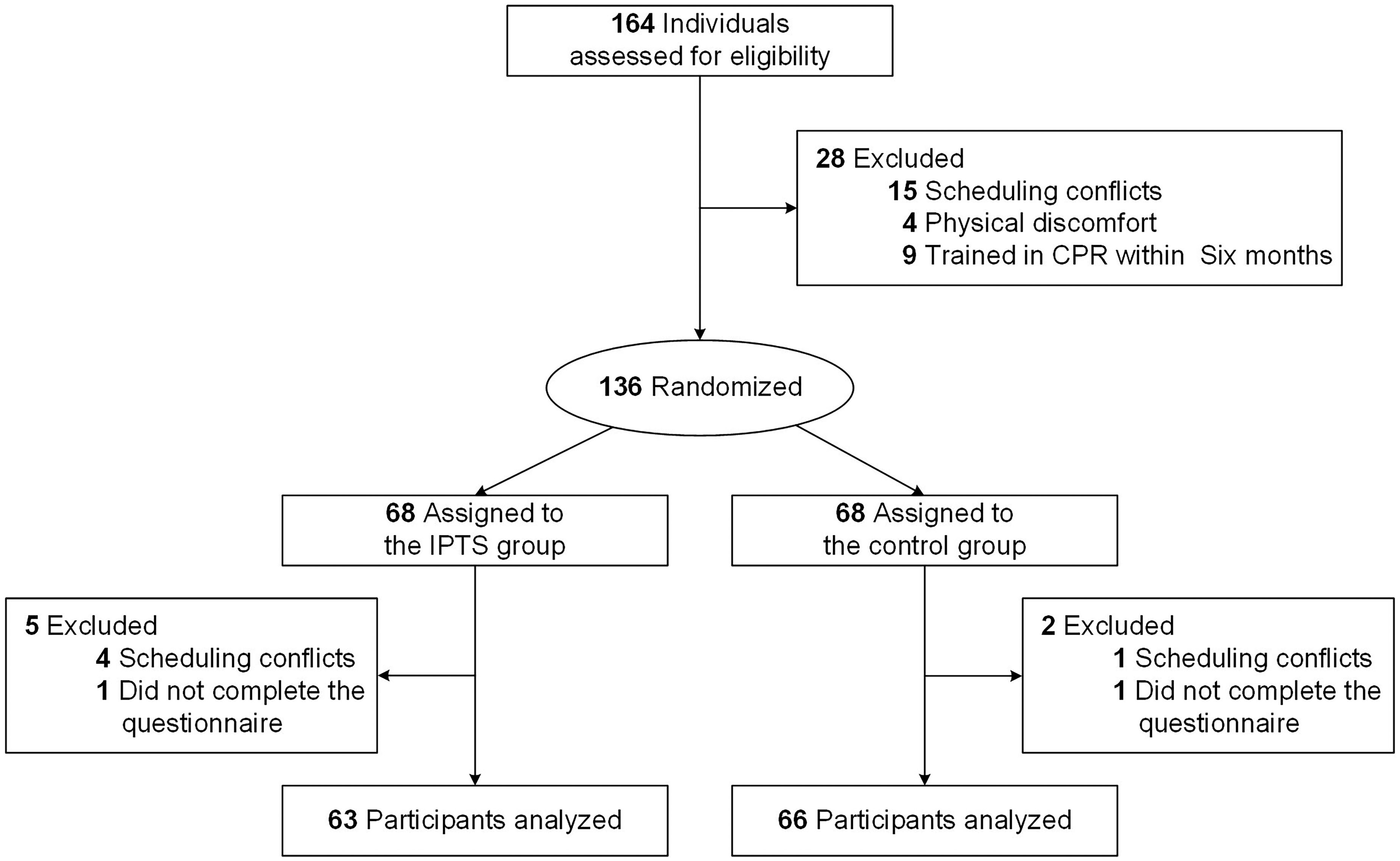
Participant recruitment flowchart.
The baseline characteristics of the 129 participants are presented in Table 3. Overall, the cohort was predominantly female (81, 62.8%), included a high proportion of nurses (62, 48.1%), and the majority had received a higher education (126, 96.9%). The median age of the cohort was 25 years [IQR, 23–30]. Additionally, all participants had previously received CPR training, with 115 (89.1%) having received CPR training within the previous 6 months to 2 years.
Baseline characteristics of the total analysis population.
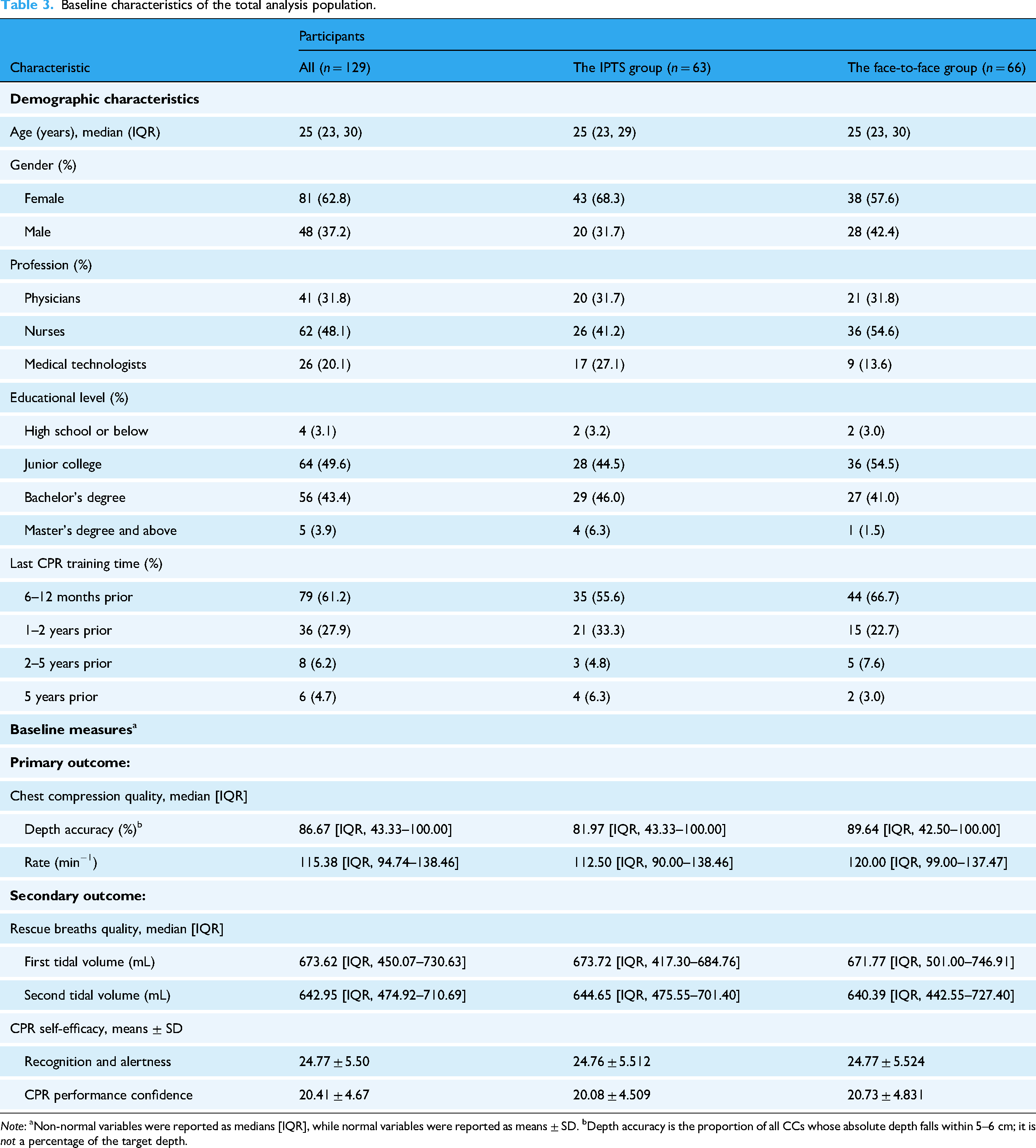
Note: aNon-normal variables were reported as medians [IQR], while normal variables were reported as means ± SD. bDepth accuracy is the proportion of all CCs whose absolute depth falls within 5–6 cm; it is not a percentage of the target depth.
Baseline assessment revealed widespread deficiencies in CPR quality across the entire cohort. Although both groups met standards for CC rate, none achieved the target for CC depth. Regarding the secondary outcomes, the tidal volume of the two mouth-to-mouth ventilations in both groups exceeded the AHA standard. Table 3 further presents baseline measures of CPR self-efficacy.
Effects of the intervention
Effects on primary outcome
There was no significant difference between the IPTS and face-to-face groups in the primary outcome of post-intervention CC quality (Table 4, Figure 3(A), (B)). Specifically, the groups did not differ in CC depth accuracy (P_adj = .878) or CC rate (P_adj =.729) Table 5. A within-group analysis showed that both groups demonstrated significant improvements in CC depth accuracy from baseline (IPTS group: from 81.97% [IQR, 43.33–100.00] to 100.00% [IQR, 73.33–100.00], paired rank-biserial r = .473, 95% CI [0.177, 0.731], P_adj = .010, moderate-to-large; face-to-face group: from 89.64% [IQR, 42.50–100.00] to 100.00% [IQR, 80.00–100.00], paired rank-biserial r = .511, 95% CI [0.202, 0.788], P_adj = .004, large). No significant changes in CC rate were observed within either group post-intervention. Because this study was designed as a superiority trial, the absence of statistical significance should not be interpreted as evidence of equivalence.

Effect of intervention with the IPTS vs. face-to-face methods on chest compression, rescue breaths, and CPR self-efficacy. (A) CC depth accuracy (AHA guideline range: 5z6 cm). (B) CC rate (AHA guideline range: 100–120 min−1). (C) and (D) The tidal volume of the two mouth-to-mouth ventilations (AHA guideline range: 500–600 mL). (E) The total point of recognition and alertness component is 5 * 7 = 35, and the total point of CPR performance confidence component is 4 * 7 = 28. (F) The total point of overall CPR self-efficacy is (5 + 4) * 7 = 63. For (E) and (F), all items were measured on a 7-point Likert scale where “1 = strongly disagree” and “7 = strongly agree,” and the error bars indicate the SD.
Between-group and before vs. after intervention differences in measurements.

Note: aNon-normal variables were reported as medians [IQR], while normal variables were reported as means ± SD. bBased on normality used independent samples t-test (effect size: Cohen's d) or the Mann–Whitney U tests (effect size: rank-biserial r). cp_adj denotes the Holm–Bonferroni-adjusted P-value, and the unadjusted P-values are available in Table 5. dBased on normality used a paired samples t-test (effect size: Cohen's d) or the Wilcoxon signed-rank test (effect size: paired rank-biserial r). eDepth accuracy is the proportion of all CCs whose absolute depth falls within 5–6 cm; it is not a percentage of the target depth.
Unadjusted P-values, Bonferroni-adjusted P-values, and Holm–Bonferroni-adjusted P-values.
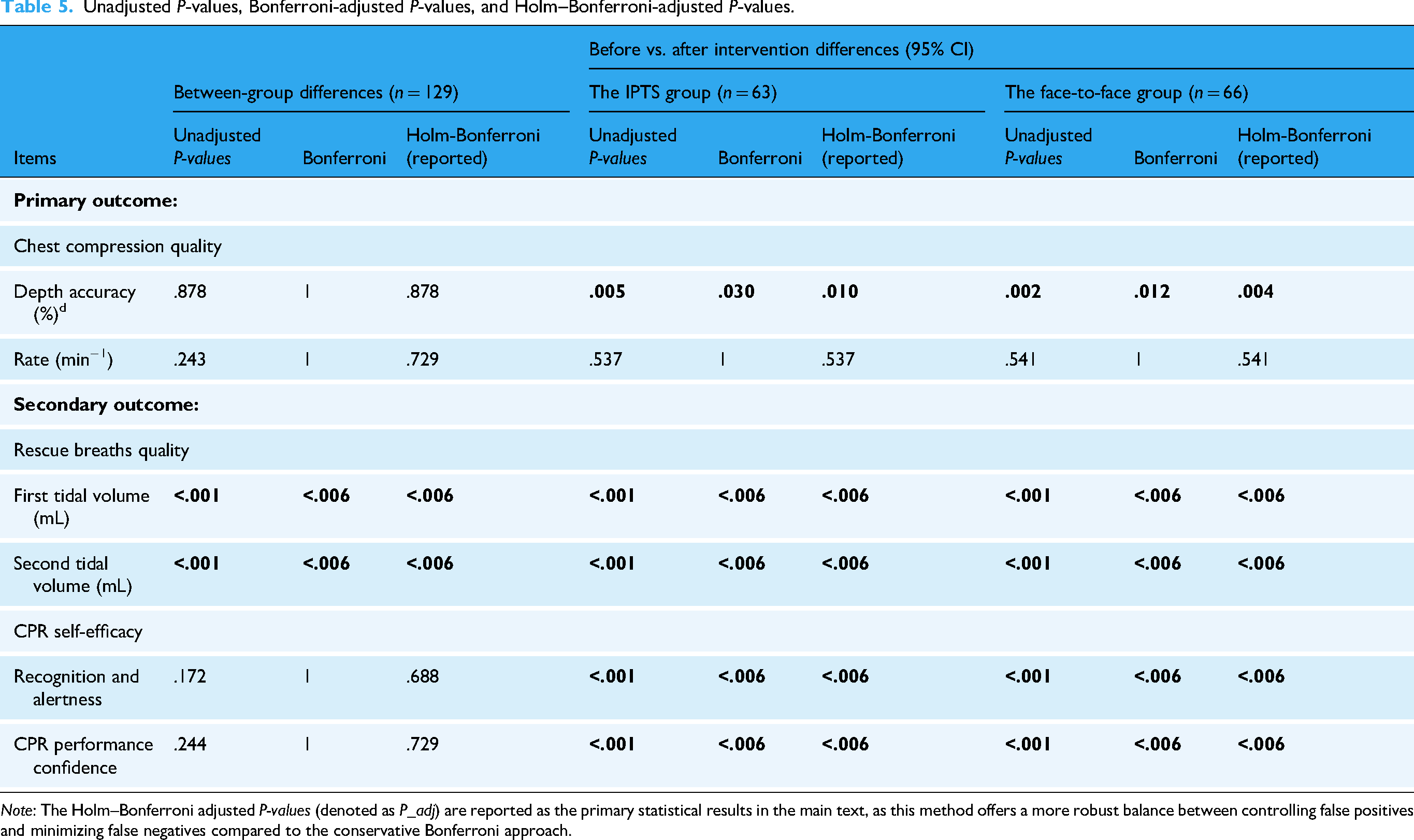
Note: The Holm–Bonferroni adjusted P-values (denoted as P_adj) are reported as the primary statistical results in the main text, as this method offers a more robust balance between controlling false positives and minimizing false negatives compared to the conservative Bonferroni approach.
Effects on secondary outcomes
Significant between-group differences were observed in rescue breath quality. First, the IPTS group achieved a higher proportion of guideline-range rescue breath volumes than the face-to-face group (first: rank-biserial r = –.585, 95% CI [−0.737, −0.416], P_adj < .006, large; second: rank-biserial r = –.512, 95% CI [–0.687, −0.323], P_adj < .006, large). Post-intervention, there was a highly significant difference in tidal volume between the groups for both ventilations (P_adj < .006 for both, and the effect size was large for both) (Figure 3(C) and (D)). Notably, the median tidal volumes in the IPTS group fell squarely within the AHA recommended range (first: 548.99 mL [IQR, 384.10–657.58], second: 542.68 mL [IQR, 437.54–624.22]), while the control group did not (first: 806.97 [IQR, 583.67–868.63], second: 800.23 [IQR, 533.57–842.18]).
There were no significant between-group differences in post-intervention self-efficacy scores for either the “recognition and awareness” component (P_adj = .688) or the “CPR performance confidence” component (P_adj = .729) (Figure 3(E), (F)). Within-group comparisons, however, showed that both retraining methods were effective at improving participants’ self-efficacy. In the “recognition and alertness” component (maximum of 35 points), the IPTS group showed a mean improvement of 5.794 [4.762, 6.825] points (Cohen's d = 1.414, 95% CI [1.061, 1.762], P_adj < .006, large), while the face-to-face group improved by 6.121 [5.148, 7.095] points (Cohen's d = 1.546, 95% CI [1.185, 1.902], P_adj < .006, large). In the “CPR performance confidence” component (with a maximum of 28 points), the IPTS group achieved a mean increase of 4.778 [3.864, 5.710] points (Cohen's d = 1.291, 95% CI [0.953, 1.624], P_adj < .006, large), and the face-to-face group showed an improvement of 4.152 [3.313, 4.990] points (Cohen's d = 1.217, 95% CI [0.895, 1.533], P_adj < .006, large).
Discussion
This study evaluated an AI- and sensor-integrated instructional system for CPR retraining among healthcare professionals. The principal finding was that no statistically significant between-group differences were observed in the prespecified primary outcomes and CPR self-efficacy. However, for secondary outcomes, the IPTS led to significantly superior learning outcomes in rescue breath quality. Overall, the findings support the hypothesis that the IPTS enhances healthcare professionals’ adherence to CPR guidelines, while the hypothesis that it delivers superior immediate learning outcomes relative to conventional face-to-face retraining is not supported—with superiority demonstrated only in certain secondary outcome measures.
We affirm that a digital retraining method, incorporating AI and sensor-based feedback, can effectively improve participants’ learning outcomes in CC depth accuracy. Although a prior review suggests that effective CPR quality still largely depends on some form of in-person training, with the adequacy of CC being higher in instructor-led groups, 39 our study indicates that the integration of AI and sensors may approach expert-level performance in certain metrics. This suggests that step-by-step instruction, hands-on practice, and real-time feedback provide an effective teaching format for healthcare professionals. Additionally, both groups demonstrated adequate CC rates at baseline, and this outcome probably reflects the relative stability of CC rate over time, as it shows less pronounced decay compared to CC depth and remains consistent for up to 12 months post-training, 40 particularly in our cohort, where 61.2% had training within 6–12 months. The lack of significant between- or within-group changes in CC rate post-intervention is primarily attributable to a ceiling effect—participants already possessed solid pre-existing competence in CC rate control, leaving little room for further improvement via either intervention.
This study found that the learning outcomes of tidal volumes in the IPTS group were significantly superior to those in the face-to-face group. A particularly striking finding was that participants in the face-to-face group not only failed to achieve the recommended tidal volume but also performed worse than their own baseline. Previous studies have attributed suboptimal tidal volumes after face-to-face CPR training—excessively low or excessively high—to several factors: (1) reliance on visible chest rise alone makes it difficult to control ventilation volume accurately,41,42 even for certified instructors 43 ; (2) insufficient training duration36,42,44; (3) ventilation skills being more difficult to acquire and retain than CC skills 45 ; (4) guidelines place greater emphasis on high-quality CCs and minimizing hands-off time, leaving ventilation performance relatively neglected 45 ; and (5) trainees’ limited effort and perfunctory attitude.44,45 In our study, although the instructor in the face-to-face group adhered to the AHA guidelines, she and trainees relied on observing “visible chest rise with each breath” to judge tidal volumes, lacking quantitative feedback. This limitation is also corroborated by the pilot study: among all assessed indicators, the “give two rescue breaths” item showed the lowest ICC across four experts (Appendix C-Table A3). The face-to-face group's ventilation results and the pilot study findings point to a shared structural issue: without quantitative monitoring tools, it is often challenging to judge tidal volume with precision. This is an inherent challenge of sensor-free, face-to-face methods rather than a shortcoming of individual instructors, trainees, or experts. At the same time, this phenomenon underscores the practical necessity of developing standardized and quantifiable tools such as the IPTS.
Moreover, the study shows that CPR retraining can improve participants’ self-efficacy, but it did not demonstrate the superiority of IPTS over face-to-face on this outcome. Following the intervention, the IPTS group improved by 5.794 points on “Recognition and alertness” and by 4.778 points on “CPR performance confidence,” indicating that, in the short term, healthcare professionals strengthened their psychological preparedness for emergencies and gained confidence to analyze, decide, and perform CPR correctly. These findings speak to a key question in digital medical education: an automated, integrated system can produce substantial gains at the psychological level, providing empirical support for the practical value of technology-driven method. This has also been validated in other CPR retraining methods such as blended learning 46 and hands-on practice or simulation training. 35 Notably, the present statistical results did not establish superiority or inferiority of IPTS versus face-to-face instruction on CPR self-efficacy; future studies should predefine equivalence or non-inferiority margins and employ appropriate trial designs to more clearly determine their relative value.
Furthermore, this study methodologically demonstrated the feasibility of an interdisciplinary AI–sensor integration approach for enabling both instructor-free learning and comprehensive performance assessment in medical education. Although existing feedback devices, as well as virtual reality and mobile applications, have been shown to improve the quality of CPR training through audiovisual cues,22,47,48 they often either overlook comprehensive performance indicators 49 or continue to rely on human examiners for final assessment.18,19 Our innovation lies in the full automation of the learning-assessment workflow through the digital integration of established algorithms and sensors. In practice, the effectiveness of using AI for quantitative prediction and modeling based on measurement data has been well demonstrated. 50 Beyond that, in resource-constrained scenarios, lightweight and deployable AI algorithm designs have also been implemented in several non-medical domains, such as FluidNet-Lite 51 in fluid mechanics and MicroCrystalNet 52 in geosciences. Similar to these studies, the value of the IPTS lies in its interdisciplinary design approach for real-world scenarios, leveraging technology to enhance practical performance. More specifically, because early CPR is a critical link in the Cardiac Arrest Chain of Survival, our findings demonstrated the potential of applying an AI–sensor approach within a resuscitation skills quality improvement system.
Limitations
This study has several limitations. At the sample level, first, all participants were healthcare professionals who had previously received CPR training, with educational backgrounds concentrated at the junior college and bachelor's degree levels; bystanders or novice learners were not included. Second, our recruitment strategy, which relied on an online social media platform, led to a sample skewed towards younger healthcare professionals, limiting age representativeness. Finally, all participants were recruited from Wuhan, China, without multicenter data from other regions or countries. Therefore, these sample characteristics may restrict the generalizability of the study findings to broader populations and settings.
In terms of study design, first, we assessed only the immediate learning outcomes after a 30-minute rest period. In the absence of follow-up assessment, we cannot determine the effect of IPTS retraining on long-term retention. Secondly, the study could not fully avoid a teaching-to-the-test bias: during retraining, the IPTS group received feedback from AI and sensors, learning the specific thresholds and calibration characteristics of the device, which was not provided to the control group. This introduced an inherent bias favoring the IPTS group. Finally, we did not collect data on the instructors in the face-to-face group: the face-to-face group was designed as a sensor-free face-to-face method, and quantitative data on instructors’ demonstrations and corrective actions were not recorded. This limits the extent to which the face-to-face method can serve as an ideal comparator and reduces the internal validity of the between-group comparison. Taken together, these design-related limitations may, to some extent, affect the robustness of the study's conclusions.
From a broader application perspective, the effectiveness of the IPTS was evaluated in a controlled simulated environment, and all outcome measures were derived from questionnaires and manikins. However, clinical practice scenarios are more complex, and CPR is only one link in the Cardiac Arrest Chain of Survival; improvements in CPR retraining cannot be directly equated with improved patient survival. Furthermore, this study has not evaluated the cost-effectiveness, scalability, scheduling flexibility, or other practical considerations associated with adopting the IPTS, and thus, the overall evaluation of its value remains incomplete.
Conclusions
Under controlled conditions, the IPTS did not differ significantly from sensor-free, face-to-face retraining in immediate learning outcomes related to CC quality or CPR self-efficacy; however, it showed superior immediate rescue breath quality. These outcomes indicate that our hypothesis that IPTS enhances healthcare professionals’ adherence to CPR guidelines is supported, whereas the prespecified hypothesis of overall superiority in immediate learning outcomes is not supported, with superiority observed only on selected secondary outcomes. By providing step-by-step instruction, hands-on practice, and quantitative feedback, an AI- and sensor-integrated instructional system can improve guideline adherence without a human instructor or examiner, supporting the feasibility of an interdisciplinary AI–sensor integration approach in medical education.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076251411030 - Supplemental material for Immediate learning outcomes of AI- and sensor-integrated versus face-to-face CPR retraining for chest compression quality: A randomized trial
Supplemental material, sj-docx-1-dhj-10.1177_20552076251411030 for Immediate learning outcomes of AI- and sensor-integrated versus face-to-face CPR retraining for chest compression quality: A randomized trial by Jingdong Ma, Wei Dai, Xiaoge Yuan, Xingce Zhu, Guo Ding, Yang Song, Hong Wu, Yan Zhang, Yuran Zhou, Wen Chen and Jinghui Nan in DIGITAL HEALTH
Supplemental Material
sj-docx-2-dhj-10.1177_20552076251411030 - Supplemental material for Immediate learning outcomes of AI- and sensor-integrated versus face-to-face CPR retraining for chest compression quality: A randomized trial
Supplemental material, sj-docx-2-dhj-10.1177_20552076251411030 for Immediate learning outcomes of AI- and sensor-integrated versus face-to-face CPR retraining for chest compression quality: A randomized trial by Jingdong Ma, Wei Dai, Xiaoge Yuan, Xingce Zhu, Guo Ding, Yang Song, Hong Wu, Yan Zhang, Yuran Zhou, Wen Chen and Jinghui Nan in DIGITAL HEALTH
Footnotes
Abbreviations
Acknowledgments
We thank all the healthcare professionals for their participation and the investigators for their hard work.
Ethical approval and consent to participate
This study was approved by the Ethics Committee of Huazhong University of Science and Technology Tongji Medical College Union Hospital (approval number: UHCTIEC-SOP-016–03–01; approval date: June 4, 2024). Informed consent was obtained from all subjects involved in the study.
Contributorship
Conceptualization, Jingdong Ma, Guo Ding, Yuran Zhou and Jinghui Nan; Data curation, Wei Dai and Xiaoge Yuan; Formal analysis, Wei Dai, Xiaoge Yuan and Xingce Zhu; Funding acquisition, Jingdong Ma and Jinghui Nan; Investigation, Guo Ding and Wen Chen; Methodology, Wei Dai; Project administration, Jingdong Ma and Jinghui Nan; Resources, Guo Ding; Software, Wei Dai and Xiaoge Yuan; Supervision, Jinghui Nan; Writing—original draft, Jingdong Ma, Wei Dai and Xingce Zhu; Writing—review and editing, Yang Song, Hong Wu, Yan Zang and Jinghui Nan.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Funding for Scientific Research Projects from Wuhan Municipal Health Commission (grant number WY22M03), The Program of Health Human Resources Exchange and Development Center of Hubei Province.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data presented in this study are available on request from the corresponding author due to ethical reasons.
Guarantor
The corresponding author is the guarantor of this article and accepts full responsibility for the integrity of the work as a whole.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.