
Abstract
Introduction
Frailty is defined as a clinically recognised state of increased vulnerability, reflecting a decline in an individual's psychological and physical reserves. Digitally-enabled interventions are increasingly utilised to monitor and support the health of older adults. Evidence on the effectiveness of digitally-enabled interventions in reducing frailty is limited. This systematic review aimed to investigate the types of digitally-enabled interventions tested, with what goals with respect to frailty, and the resulting outcomes.
Method
Medline, CINAHL, Scopus, PsychInfo and Embase were searched from time of origin until July 2024. Peer-reviewed RCTs assessing the impact of digitally-enabled interventions on older adults were included. Outcome measures explored were frailty, cognitive status, mental health, quality of life, adherence and usability. Data was extracted independently by two people using Covidence platform. Narrative synthesis was performed for all studies and meta-analysis was performed for outcomes reported in four or more studies.
Results
From 4476 titles and abstracts screened, 17 studies were included following full text review. Overall, 12 studies included exercises as a component or the sole form of intervention. The mean duration of intervention was 4.04(SD2.56) months. Mean adherence to the intervention was 59% which was lower in exercise-based intervention. The most and least reported frailty-specific outcome was walking speed (n = 8) and self-reported exhaustion level (n = 2). Meta-analysis showed non-exercise-based interventions showed significant improvements in SPPB. There was no statistically significant change in Timed-up and Go and handgrip strength. Narrative synthesis indicates there was insufficient evidence to evaluate the impact of digital interventions on frailty, frailty-specific outcomes, mental health, activities of daily living, health-related quality of life, sleep and cognition.
Conclusion
The findings suggest low technological readiness and adherence among digitally-enabled interventions for older adults. Narrative synthesis of overall frailty and outcome measures showed mixed results and limited evidence on the impact of digital interventions on frailty and outcomes.
Introduction
Older adults, defined as individuals aged 65 years or older, constitute one-tenth of the global population.1,2 While ageing does not inherently equate to ill health, it is frequently accompanied by increased medical issues and greater use of healthcare resources. 3 The English Longitudinal Study of Ageing (ELSA) highlights that only 26% of individuals aged over 65 and 14% aged over 85 years old in England are free from any long-term health condition. 4
A major contributor to ill health in older adults is frailty which is a clinical state marked by reduced capacity to manage physiological stressors. 5 The phenotype model identifies five key measurable characteristics of frailty: exhaustion, weight loss, low activity levels, slow walking speed, and weak grip strength. 5 Frailty has widespread implications. This is associated with poor outcomes including increased length of hospital admissions, acute emergency attendances to hospital, general practice visits, specialist outpatient clinic appointments, and reduced quality of life.3,6,7 Moreover, frailty is associated with a reduction in one's quality of life, ability to self-care and to live independently. 6 Population studies have shown increased formal and informal healthcare costs as individuals become more frail.8,9 Beyond the personal impact, frailty imposes financial and emotional burdens on both an individual and their family.8–10 As such, addressing frailty not only mitigates individual harm, but can also reduce the burden on wider society and healthcare infrastructure.8–10
Digital sensors are electronic devices capable of capturing various data and converting it into actionable information. 11 Within the context of frailty, sensors serve diverse roles. 11 For example, a sensor worn by the user (like a smartwatch, pedometer or accelerometer) can monitor users’ active behaviours using step count and walking speed. 12 Another example is a motion sensor which tracks the users’ activity without requiring a high level of user interaction.12,13 These tools have been employed to detect changes in markers of frailty, such as reduced walking speed, and support interventions aimed at reducing frailty in older adults. 14 Combined interventions delivered digitally, such as exercise programmes, with sensors to monitor participants’ activity levels have demonstrated effectiveness in improving frailty status among older adults. 15
However, a systematic review of randomised controlled trials (RCTs) in 2016 on the digital sensors tested to reverse frailty identified an absence of well-developed and thoroughly tested technologies for older adults. 16 Most studies investigating the impact of digital technology on frailty to date are proof-of-concept or feasibility studies, reflecting low technology readiness – defined as the developmental maturity of a technology. 16 There has been a rapid development of consumer-grade wearables and smart-home sensor technologies have been created since this paper was published in 2016. As such, this evidence gap underscores the need for robust research to evaluate the effectiveness of digital sensors in the measurement of frailty and related outcomes.
To address this gap in evidence, the current systematic review and meta-analysis aims to address the following question: What is the evidence for the impact of digital interventions on frailty in older adults?
The objectives of the review were to:
Explore and categorise which types of digitally-enabled interventions have been tested in older adults, including but not limited to home sensors, wearable devices, telehealth and telemedicine technologies. Evaluate the engagement with digitally-enabled interventions through metrics of adherence, usability and acceptability. Evaluate the impact of digitally-enabled interventions on frailty and associated outcomes in older adults, including walking speed, grip strength, self-reported exhaustion level, weight loss, physical activity level, cognition, quality of life, wellbeing and mental health.
Methods
In order to answer the objectives, the primary outcome of this study was to identify and categorise the types of digitally-enabled interventions used among older adults, such as telehealth platforms, sensor-enabled exercise programmes, and wearable technologies.
The secondary outcomes were to:
assess the measurable impact on engagement with digitally-enabled interventions through metrics of adherence, usability and acceptability. evaluate the measurable impact of these interventions on
frailty phenotype components according to Fried's criteria which include weight loss, reduced grip strength, walking speed, increased self-reported exhaustion level and low physical activity levels. associated or secondary age-related outcomes including mental health, quality of life, activities of daily living, cognition and sleep.
This systematic review and meta-analysis was registered with Prospero (CRD42023472317) 17 and was reported according to the Preferred Reporting Items for Systematic Reviews and Meta-analysis (PRISMA 2020) statement guidelines (Appendix 1). 18
Search strategy
The search strategy was designed to identify all randomised controlled trials (RCTs) that investigated the use of digitally-enabled interventions in older adults, with a focus on frailty. Referring to Appendix 1, the search terms were designed with the support of an Imperial College London Department of Medicine Librarian, building on terms utilised in similar studies on frailty and digitally-enabled interventions. 15 18–20 The initial search was conducted on 30 November 2023. With expert review, this search was updated on 11 July 2024 with additional keywords ‘Accelerometer’, ‘Pedometer’ and ‘Activity tracker’. These keywords are devices which could be used in digitally-enabled interventions to monitor activity levels among older adults. The full search strategy and explosion terms developed in line with the PICO approach are available in the Appendix 1. Reference lists of included studies were also reviewed.
Databases
Databases searched were Medline, CINAHL, Scopus, PsychINFO and Embase from origin to 11 July 2024.
Inclusion and exclusion criteria
Studies were included within the systematic review if they met the following criteria: any adult aged greater than or equal to 65 because this is the definition of older adult used by the Office for National Statistics and NHS England.1,19 The studies evaluated the effectiveness of community-based digitally-enabled interventions – including home sensors, wearables, telehealth, and telemedicine. Additionally, these were RCTs that were published in English.
The exclusion criteria were: unavailable full text; laboratory-based, cohort or cross-sectional studies; commentary articles; dissertations; full text which were not published in English; did not assess the outcome measurements of interest.
The outcomes measured include frailty and related outcomes (exhaustion, involuntary weight loss, slow walking speed, weak handgrip strength, low physical activity levels), activities of daily living, cognitive frailty, sleep, mental health, changes in quality of life, adherence, acceptability, usability, and cost of intervention.
The inclusion and exclusion criteria for this systematic review were designed to ensure the selection of studies that are most relevant and rigorous to address the research objectives. The list of community-based digitally-enabled interventions was selected to reflect the study's aims and following discussions with an expert panel of researchers and the Department of Medicine librarian. Only RCTs were included because they provide the most robust evidence in evaluating the impact of a new intervention. 20
Data extraction
Two reviewers independently identified the eligible studies according to the inclusion and exclusion criteria. Titles, abstracts and full-text reviews were reviewed according to the inclusion and exclusion criteria by two authors (TT and one other independent reviewer: FC, HA or BM. Any differences in opinion were resolved through discussion and when necessary, with support from a third reviewer. This process was completed on Covidence platform. 21
Risk of bias and quality assessment
Quality assessment of the studies included in the systematic review was carried out using the revised Cochrane Risk of Bias tool for randomised trials (ROB-2). 22 This was independently completed by TT and one other reviewer (FC or BM). Differences in opinions were resolved through consensus, and when necessary with support from a third reviewer.
Data synthesis
Objective 1: Explore and categorise types of digitally-enabled interventions tested in older adults
Given heterogeneity in interventions and outcomes, narrative synthesis was conducted across all objectives. Where at least four studies reported the same outcome using a comparable measurement tool, meta-analysis was performed. This synthesis method enabled a description of the landscape of digitally-enabled interventions and outcomes of interest reported in these studies.
23
Studies were summarised with respect to their total number of participants, digitally-enabled intervention and control groups, duration of intervention and follow-up. Objective 2: Evaluate the engagement with digitally-enabled interventions through metrics of adherence, usability and acceptability
Narrative synthesis was conducted for the objectives in all studies. The papers were further stratified according to outcomes of interest. Studies were summarised regarding their adherence, usability and acceptability levels. Objective 3: Evaluate the impact of digitally-enabled interventions on frailty and associated outcomes in older adults
The five characteristics of the frailty phenotype can be measured using methods including walking speed, grip strength, weight, physical activity levels, self-reported exhaustion level. Across literature, these methods are not standardised in the reporting of frailty phenotype. Additional tools are Timed-up and Go (TUG) and Short Physical Performance Battery (SPPB). Five age-related health outcomes were explored, including mental health, quality of life, independence level and activities of daily living, cognition and sleep. Narrative synthesis was conducted for this objective in all studies. The papers were further stratified according to the outcomes of interest.
Studies were assessed for their suitability for meta-analysis, according to the measurement tool used to evaluate the outcomes of digitally-enabled interventions with respect to frailty. If the same measurement tool was used in four or more studies, they were then included for meta-analysis. Examples of different measurement tools in an outcome is walking speed where studies have measured this using time to complete three metres, or duration walked in six minutes. Four or more studies were chosen to reduce heterogeneity. 24
Heterogeneity between eligible studies was assessed with Cochrane's Q and Higgins I2 test, with an I2 greater than 50% considered significant heterogeneity. A random effect model was used for these outcomes. A confidence interval (CI) of 95% was calculated for each outcome variable. Odds ratio for binary categorical variables and Standardised mean difference (SMD) were calculated for continuous variables. Egger's test was performed to assess for publication bias. All tests were calculated as 2-tailed. A p-value of less than 0.05 was considered statistically significant. Data analysis was completed using Microsoft Excel and IBM SPSS version 29. 25
Results
The updated search in July 2024 identified 4476 studies. Following title and abstract screening, 55 full-texts were assessed for eligibility. Of these, 17 were included in the review. The PRISMA flowchart for study selection can be viewed in Figure 1.

PRISMA flowchart of study selection.
Study characteristics
The characteristics of the studies are presented in Table 1. Out of the 17 studies, six studies were pilot RCTs
16
26–30 and the remaining studies were RCTs.31–41 Nine studies were published in Europe, five in Asia, two from North America and one from South America. There were 1759 participants across all studies. One study focused on older adults undergoing total hip replacement and another study focused on older adults with type two diabetes mellitus.26,36 The outcomes assessed were changes in overall frailty level27,29,31,3239–41 (7/17) or changes in an aspect of frailty such as low muscle strength26,3032–34,38,40 (7/17), physical activity levels26,33,37,40,42 (5/17), nutrition37,40 (2/17) and cognitive levels35,38 (2/17). Research Objective 1: Explore and categorise which types of digitally-enabled interventions have been tested in older adults, including but not limited to home sensors, wearable devices, telehealth and telemedicine technologies
Summary of included studies.
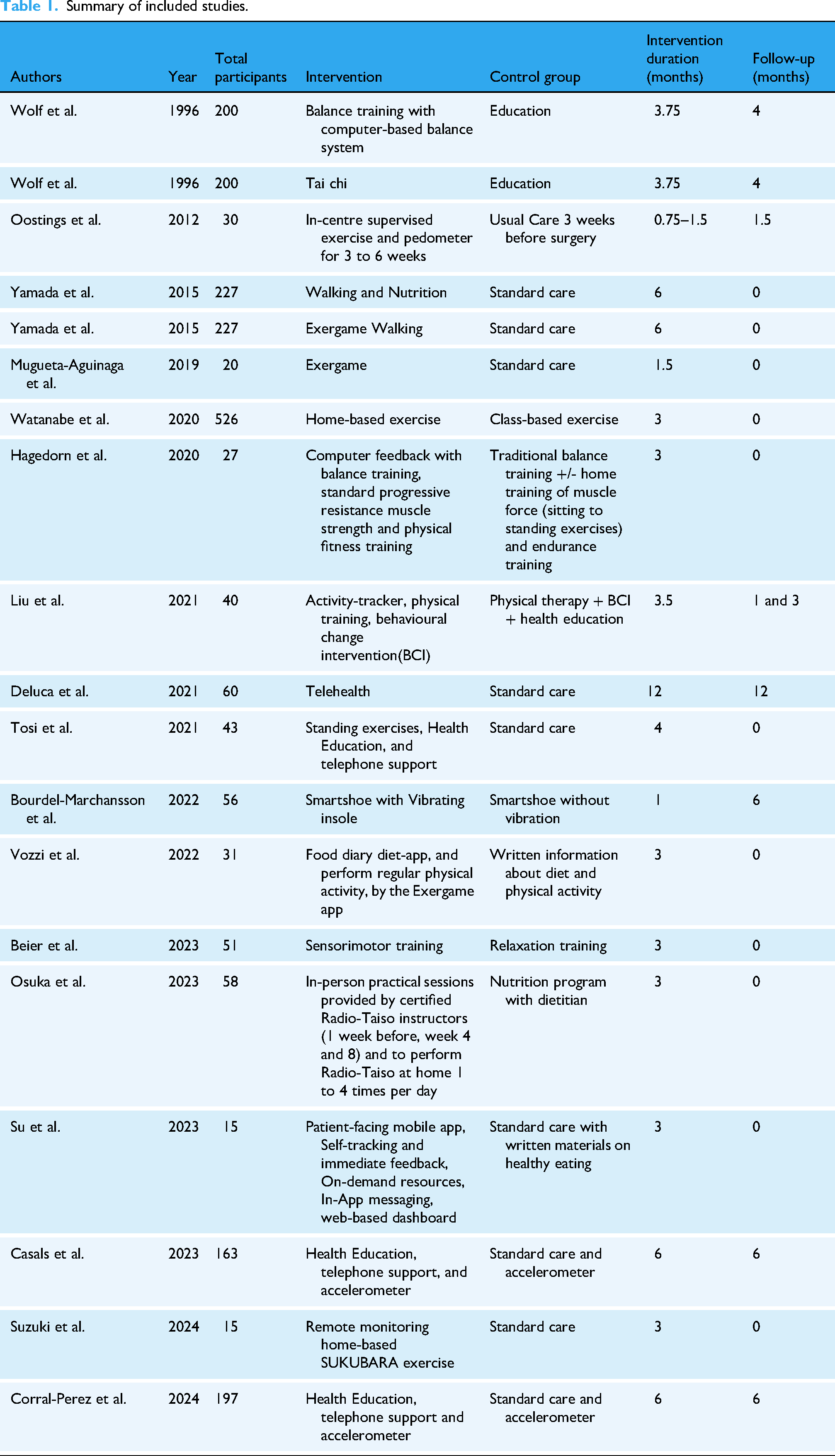
Overall, 12 (70.6%) studies included exercises using technology as a component or the sole form of intervention. Three studies incorporated the use of a mobile application which delivered exercises through a gamified approach27,30,32 or an in-app dashboard for activity tracking and messaging
29
or tracking participants’ diet.
37
Three studies utilised accelerometers for measuring the activity levels of their participants.26,40,41 None of the studies utilised home sensors. Three studies incorporated health education as a part of their intervention28,40,41 and four studies as part of their control arm.29,31,37,42 The mean duration of intervention was 4.04 (SD 2.56) months. Seven studies followed their participants after the end of the intervention.26,31,35,3640–42 The mean duration of follow-up was 5.5 (SD 3.3) months. Research Objective 2: Evaluate the engagement with digitally-enabled interventions through metrics of adherence, usability and acceptability
Adherence
Adherence was reported in eight studies 28 31–33,36,38,39,42 with a non-weighted mean of 59.5%, ranging between 26.7% and 100% in the intervention group. Among five studies suitable for meta-analysis,28,31,36,39,42 there was non-significant lower adherence rates for exercise-based interventions than non-exercise interventions (OR 0.21, 95%CI [0.05, 0.84], p = 0.43 vs OR 0.33, 95%CI [0.14, 1.17], p = 0.35) (Figure 2).

Forest plot of adherence of in experimental and control groups subclassified by exercise vs non-exercise groups.
Usability
Two studies evaluated usability of their intervention using the Systems Usability Scale (SUS).27,35 Mugueta-Aguinaga et al. reported a higher SUS of 95.26 (SD 4.56) for their intervention than De Luca et al. which was 66.17 (SD 12.63).27,35
Acceptability
Two studies assessed the acceptability of the intervention. Liu et al. used self-reported acceptability through a feedback questionnaire, while Su et al. used the Mobile Application Rating Scale which looked at engagement, functionality, information and aesthetic of the application.29,42 Liu et al. had 90.9% acceptability of the intervention. This rate was not reported by Su et al.
29
Research objective 3: Evaluate the impact of digitally-enabled interventions on frailty and associated outcomes in older adults, including walking speed, grip strength, self-reported exhaustion level, weight loss, low physical activity levels, cognition, quality of life, wellbeing and mental health.
Overall frailty as a composite measure using fried
Out of the 17 included studies, overall frailty was measured in five studies.16,27,38,40,41 Three of these calculated mean changes in the Fried Frailty score which reduced in all three intervention40–42 and two control groups at the end of the intervention.38,41 Two studies showed a statistically significant change, where p < 0.05.42,43 However, this was not statistically significant by Beier et al. 38 Meta-analysis was not conducted for overall frailty due to the heterogeneity of the outcome measure.
Specific measures of frailty
The most reported frailty outcome was walking speed (n = 8, 47.1%),26,31,33,3436–38,40 while the least reported outcome was self-reported exhaustion level (n = 2, 11.8%).38,40 Frailty outcomes suitable for meta-analysis were Short Physical Performance Battery (SPPB), Timed-Up and Go (TUG) and grip strength. Due to the heterogeneity of the measurement tools used in various studies and a small number of studies, narrative synthesis was conducted for overall frailty, walking speed, unintentional weight loss, physical activity and self-reported exhaustion levels.
Seven studies evaluated the effect of their intervention in the form of SPPB.27,2936–40 Using Cohen's D, two studies reported statistically significant improvements in the standardised mean difference (p < 0.05)27,37 and two studies reported non-significant improvement in standardised mean difference (SMD) of SPPB scores.29,36 Three studies reported statistical significant worsened SPPB scores in their intervention group.37,38,40 Meta-analysis of all seven studies revealed a non-significant effect size for any intervention on SPPB (SMD = 0.28, 95% CI [-0.16, 0.71], p = 0.21). Looking at intervention categories, exercise-based interventions had a negligible impact on SPPB (SMD = -0.07, 95%CI [-0.40, 0.26], p = 0.68) and non-exercise-based interventions demonstrated significant improvements (SMD = 0.72, 95%CI [0.41, 1.02], p < 0.05) (Figures 3 and 4).

Graph of mean changes in short physical performance battery score.

Plot of mean change in short physical performance battery (SPPB).
Five studies assessed changes in TUG as a result of their intervention.26,33,34,36,42 All five studies incorporated exercise as a form of intervention and reported reduced time taken to complete the task in the intervention groups26,33,34,36,42 and in three in their control groups.33,34,42 Reduced time in TUG was statistically significant in the intervention group in the study by Liu et al. and the control group in the study by Watanabe et al.33,42 Meta-analysis for TUG of the four studies included showed no significant change (SMD = -0.01, 95% CI [-0.29, 0.27], p = 0.96). There is no effect of exercise on TUG (Figure 5).

Forest plot of timed up and go (TUG).
Walking speed
The most commonly evaluated frailty-specific measure was changes in walking speed, which was measured in eight studies.26,31,33,3436–38,40 This was measured in varied formats, including the time taken to walk a fixed distance,36,38,40 total distance walked in 6 minutes26,34,37 or 12 minutes. 31 Six studies incorporated exercise as part of the intervention,26,31,33,34,37,38 one study used a Smartshoe sensor with a vibrating insole, 36 and one study delivered health education and telemedicine in the intervention group. 40 Three studies reported reduced walking speed at the end of the intervention, with only one (Casals et al., p < 0.001) showing a significant difference between intervention and control groups; the remaining two did not reach significance (p > 0.05).36,37,44 Three studies reported non-significant reduction in walking speed in the control group (p > 0.05).34,36,45
Handgrip strength
Five studies evaluated changes in handgrip strength.30,31,33,38,40 Four studies included exercise as a component of the intervention.30,31,33,38 Three studies reported non-significant increase in mean grip strength in the intervention group (p > 0.05).33,38,40 Meta-analysis of these five studies30,31,33,38,40 revealed a non-significant increase in grip strength (SMD = 0.10, 95% CI [-0.07, 0.26], p = 0.24) (Figures 6 and 7).
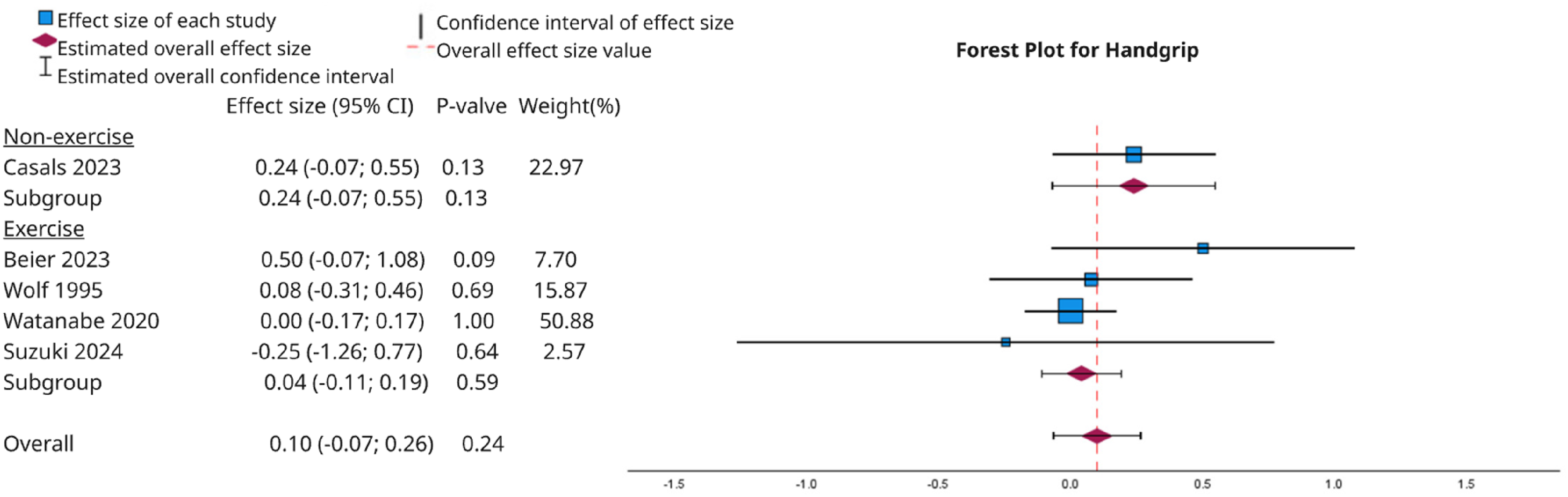
Forest plot of changes in handgrip strength.

Histogram of mean changes in handgrip strength.
Weight loss
Six studies reported changes in participants’ weight using measurement methods including body mass index29,32,37,38,40 and body mass. 30 Four studies incorporated exercise as one or the only intervention.32,37,38,40 As described earlier, one characteristic of the frailty phenotype is unintentional weight loss. 5 Two studies measured unintentional weight loss over the course of the study.38,44 Casals et al. 44 reported statistically significant reduction in the number of participants with unintentional weight loss in the intervention group (p < 0.05) while it was non-significant (p > 0.05) in the study by Beier et al. 38 In both studies, the reduction in unintentional weight loss was non-significant between intervention and control groups.38,44
Physical activity
Seven studies assessed changes in physical activity level.26,28,33,38,40,42 Physical activity level was measured through various measurement methods - Moderate to vigorous physical activity (MVPA) per valid day or week,33,40,42 self-reported activities,26,38 and total sedentary time on the accelerometer. 28 Both Liu and Watanabe incorporated exercise-based interventions.33,42 There was increased activity levels in four of the intervention groups28,33,38,42 and four of the control groups.28,33,38,40
Self-reported exhaustion
Two studies reported changes in self-reported exhaustion level.38,40 Both reported a reduced number of participants with self-reported exhaustion levels that met Fried criteria. This was statistically significant in the study by Casals et al. (p < 0.05) but not in the study by Beier et al. (p = 0.13).
Age-related outcome measures
Five age-related outcomes were explored including mental health, quality of life, independence level and activities of daily living, cognition frailty and sleep. Narrative synthesis was conducted for these five age-related measures due to the heterogeneity of the measurement tools used in various studies and the small number of studies in each outcome.
Mental health
Out of the 17 included studies, two studies reported the impact of digital intervention(s) on mental health.35,38 This was measured using the Centre for Epidemiologic Studies Depression Scale (CES-D) 38 and Geriatric Depression Scale.35,38 De Luca et al. showed a significant reduction in depression scores (p = 0.03) while Beier et al. reported no difference in depression scores (p = 0.99).35,38
Health-related quality of life
Four studies26,27,38,39 reported health-related quality of life using EQ-5D-5L,27,38 Short-form 36 (SF-36)38,39 and Hip-related QoL. 26 EQ-5D-5L is an overall score which combines both physical and mental quality of life. Narrative synthesis revealed mixed findings for the intervention group. The study by Mugueta-Aguinaga reported statistically improved EQ-5D-5L scores between the groups (p = 0.039) 27 while it showed non-significant reduction (p = 0.82) in the study by Beier et al. 38
SF-36 is normally divided into Physical Component Score (PCS) and Mental Component Score (MCS). 46 As such, the analysis was further divided into these domains. Beier et al. reported an increase in the mean PCS score of the intervention arm, while Osuka et al. reported worsening of the mean PCS.38,39 MCS improved in both studies in the intervention arm, the control arm in Beier et al. reported improvement in MCS score, 36 while it worsened in the study by Osuka et al. 39
Independence level and activities of daily living (ADL)
Two studies measured activities of daily living (ADL) outcomes using Barthel's ADL, 27 Katz 35 and Lawton-Brody Instrumental ADL. 35 Both studies showed statistically significant improvement in ADL (p < 0.05) among the intervention group and reduced ADL in the control group.
Cognitive frailty
Cognitive frailty was measured in two studies in the form of the Mini-Mental State Examination (MMSE) 35 and computerised multidimensional neurocognitive task battery. 39 Osuka et al. showed non-statistically significant improvement in cognitive score after intervention (p > 0.05), while De Luca et al. reported reduced MMSE score after intervention (p-value not reported).35,39
Sleep
Sleep was investigated in three studies using a self-reported sleep question “How often do you have trouble falling asleep?”, 31 Pittsburgh Sleep Quality Index and efficiency.40,41 However, Wolf et al. did not report whether this had changed at the end of the study. Both Casals et al. and Corral-Perez et al. were from the same patient cohort and reported significantly improved PSQI scores at 12 months (p = 0.03). 41
Adverse events
Out of 17 studies, five studies reported their adverse events.28,3234–36,39 In studies where the intervention involved exercises, the most common adverse event were muscle aches and pain.32,36,39 Bourdel-Marchasson et al. also reported three falls in the intervention group. 36
Risk of bias assessment
The quality of evidence for digital interventions used with respect to frailty was assessed using the Cochrane Risk of Bias (ROB-2) assessment. The majority of the studies were identified as having a high risk of bias (9 out of 17), and six had some concerns. The primary issue stemmed from the selective reporting of significant results (column D5, Figure 8). In these cases, multiple tests were conducted and the most significant results were presented in the paper (7 out of 17). Figure 8 illustrates the Risk of Bias table.

Risk of bias analysis. 47
Discussion
This study represents a comprehensive review of the impact of digitally-enabled interventions on frailty and related outcomes among older adults. This review found that although digitally-enabled interventions were associated with improvements in physical frailty measures such as SPPB and grip strength in some studies, these changes were not statistically significant in pooled analysis. Meta-analysis demonstrated that digitally-enabled interventions had a non-significant effect on these outcomes. In addition, this is a first-of-its-kind detailed narrative synthesis of various frailty-specific and related outcomes including unintentional weight loss, walking speed, reduced physical activity levels, self-reported exhaustion, mental health, health-related quality of life, activities of daily living, cognitive frailty, sleep, acceptability, acceptability, adverse events, and usability.
What this study found in comparison with literature
The most common digitally-enabled intervention reported in the literature was exercise using technologies such as accelerometers and mobile application-based user interfaces. The findings of this study align largely with existing literature where exercise-based intervention was the most commonly investigated digitally-enabled intervention. 15
Numerous studies included in this review were underpowered and pilot studies. This could be due to limitations in funding for the study. Additionally, early digitally-enabled interventions are likely uncontrolled pilot and feasibility studies potentially due to regulatory and culture reasons. 48 It may suggest low technological readiness in the field of digitally-enabled intervention for older adults. A review on technology readiness of studies measuring activities of daily living by Gadey et al. demonstrated moderate technology readiness among technology-based interventions for older adults, and there is a lack of evidence for home monitoring technologies. 49 Gadey et al. reported most studies used accelerometers to measure changes in ADLs. 49 These findings suggest more high-quality, robust studies are required in evaluating the impact of digital technologies.
Narrative synthesis on engagement, adherence, acceptability and usability has highlighted variability in outcome measurement tools used and a limited number of studies for each outcome. Firstly, there was great variability in usability scores reported in the studies. This reflects variability in user experience, specifically how well the digitally-enabled intervention was designed to meet the needs of older adults. Only Liu et al. study reported the self-reported acceptability of their intervention. 16 Adherence levels were lower in the exercise group, which reflects difficulty in following digitally delivered exercise interventions. This differs from earlier meta-analyses which showed higher adherence to technology-based exercise programmes than traditional (91.25% vs 83.58%). 50 Adherence to traditional unsupervised home-based interventions was lower than supervised interventions. This is supported by literature which highlighted reasons such as low motivation, loss of interest, and inability to use the technology.50,51 Additionally, evidence has shown exercise is more effective when performed in groups rather than individually. 52 Yet, digitally-enabled interventions were created for individual use. This may influence the adherence and effectiveness of digitally-enabled intervention.
The findings of this systematic review reinforce the growing consensus on the potential of digitally-enabled interventions to improve both frailty and age-related health outcomes. Narrative synthesis revealed some improvements in Fried Frailty scores and related metrics in individual studies. However, overall evidence remains inconclusive due to small sample sizes and heterogeneity. Two studies showed a reduction in Fried Frailty score. This means participants have a reduced number of the five frailty characteristics. It also suggests improved grip strength, walking speed, reduced self-reported exhaustion levels, reduced physical activity level and/or reduced unintentional weight loss. In addition, frailty-specific outcomes like grip strength, TUG and weight loss showed non-significant effects. These findings are mirrored by a meta-analysis by Cieslik et al. which reported non-significant improvement in TUG measurements, muscle strength, functional mobility and balance among older adults which underwent technology-assisted exercise rehabilitation programmes. 15 Our findings are supported by a systematic review on in-centre compared to home-based exercise programme which reported no significant difference between-group differences in walking speed and physical activity levels. 53 However, systematic reviews of conventional exercise programmes have demonstrated greater improvements in strength and balance than technology-assisted programmes.54,55
This systematic review showed non-exercise intervention had a significant improvement in SPPB scores, but no overall impact for exercise-based intervention. This novel insight has not been reported in literature and contributes new evidence on the use of digitally delivered intervention using app-based health education. This suggests alternative approaches may complement or outperform traditional exercise-based digitally-enabled interventions for older adults.
Narrative synthesis of mental health, health-related quality of life (HR-QoL), sleep and cognitive outcomes showed mixed results. De Luca et al. reported significant reduction in depression scores while Beier et al. observed worsening of symptoms. 35 Similarly, a meta-analysis of telehealth interventions showed significant improvements in the mental components of SF-36 but a non-significant effect of telehealth interventions on the physical component of SF-36. 56 The mixed findings on cognitive outcomes contrasts with various systematic reviews of digitally delivered cognitive training and exercise with games which showed improved cognitive performance in older adults.15,57,58 In addition, the mixed findings of the impact of digitally-enabled intervention of sleep differs from scoping review of five mobile health studies which had reported improvements in self-reported sleep quality. 59 This review did not show quantitative differences in sleep outcomes. 59 Thus, there is mixed results on the impact of digitally-enabled interventions on mental health, HR-QoL, sleep and cognitive outcomes.
Strengths and limitations
The strength of this systematic review is its rigorous methodological approach, combining qualitative narrative synthesis and quantitative meta-analysis. The categorisation of outcomes into frailty and age-related outcomes is a holistic approach of the impact of digitally-enabled interventions on older adults. Additionally, this study offers practical insights into implementation by evaluating adherence, usability and acceptability of digitally-enabled interventions.
In contrast, the limitations of this systematic review are the heterogeneity of measurement tools, a small number of studies for certain outcomes, and high risk of bias among the included studies. Given the short duration of intervention and lack of significant effects on the meta-analysis, the inclusion of observational service evaluation and pilot studies can potentially increase the scope of evidence. The rapidly evolving landscape of digital health research, business models, use of personal records, community research and use of artificial intelligence have created new ways of implementing and assessing the effectiveness of these interventions.
Opportunities for future work
Future research should focus on standardising the measurement tools used in frailty research and outcome reporting guidelines to enable robust comparisons across studies. Additionally, cost-effectiveness and scalability of digitally-enabled interventions should be evaluated across diverse populations. A large, well-designed randomised controlled trial is required to establish a strong evidence base on the impact of digitally-enabled intervention for managing frailty among older adults – including pre-frail, technologically literate older adults. As none of the studies included investigated the use of home sensors as a digitally-enabled intervention, the findings also suggest that the design of digitally-enabled interventions for older adults requires a holistic approach using physical, social, and cognitive elements.
Conclusion
In summary, this systematic review and meta-analysis indicate that overall frailty is commonly measured using physical frailty in the form of SPPB and TUG. A variety of digitally-enabled interventions tested in the included literature are exercise using games, mobile applications and accelerometers. A meta-analysis of the effect size of non-exercise-based digitally-enabled interventions showed significant improvement in SPPB. There were no statistically significant changes in TUG, low handgrip strength, and weight loss. Due to the heterogeneity of measurement tools, narrative synthesis was conducted for overall frailty, walking speed, physical activity levels, self-reported exhaustion, mental health, health-related quality of life, activities of daily living, cognitive frailty, sleep, acceptability, acceptability, adverse events and usability.
In the future, better reporting guidelines and high-quality randomised controlled trials are required to evaluate the impact of digitally-enabled interventions on older adults with and without frailty. The findings also suggest the design of digitally-enabled interventions for older adults requires a holistic approach using physical, social, and cognitive elements.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076251410997 - Supplemental material for The impact of digitally-enabled interventions on frailty and other age-related outcomes – Systematic review and meta-analysis
Supplemental material, sj-docx-1-dhj-10.1177_20552076251410997 for The impact of digitally-enabled interventions on frailty and other age-related outcomes – Systematic review and meta-analysis by Tricia Tay, Kate Grailey, Fangyue Chen, Hamzah Amin, Balraj Maan, Simon Dryden, Leila Shepherd, Michael Fertleman and Ara Darzi in DIGITAL HEALTH
Supplemental Material
sj-docx-2-dhj-10.1177_20552076251410997 - Supplemental material for The impact of digitally-enabled interventions on frailty and other age-related outcomes – Systematic review and meta-analysis
Supplemental material, sj-docx-2-dhj-10.1177_20552076251410997 for The impact of digitally-enabled interventions on frailty and other age-related outcomes – Systematic review and meta-analysis by Tricia Tay, Kate Grailey, Fangyue Chen, Hamzah Amin, Balraj Maan, Simon Dryden, Leila Shepherd, Michael Fertleman and Ara Darzi in DIGITAL HEALTH
Footnotes
Contributorship
TT, KG, LS conceived the study and advised TT on the activities. TT searched the literature, undertook extraction, analysis and drafted the paper. FC, HA, BM undertook extraction. KG and SD reviewed versions of the paper. All authors reviewed and approved the final version of the manuscript. TT is the guarantor.
ORCID iDs
Ethical approval
Not required because all data were extracted from previously published studies with appropriate ethical approvals.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
All data can be requested from the corresponding author.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.