
Abstract
Objective
This study systematically measures the coupling coordination between China's digital economy and healthcare service resources, reveals their spatiotemporal evolution, and identifies key driving factors.
Methods
Using panel data from 31 Chinese provinces (2012–2023), we constructed a comprehensive evaluation system. The entropy weight method determined indicator weights, the coupling coordination degree model assessed coordinated development levels, kernel density estimation analyzed dynamic trends, spatial autocorrelation examined agglomeration characteristics, and the spatial Durbin model explored regional driving mechanisms.
Results
The coupling coordination degree increased continuously from initial to medium-high coordination, with significant regional disparities: “high-stable coordination in the east, improvement in the center, and catch-up growth in the west.” Spatial analysis revealed significant negative dependence with clustered low-value areas. Economic development, education, population aging, urbanization, and government digitalization significantly influenced coordination with regional heterogeneity: the east showed synergistic effects, the center relied on factor inputs, and the west faced resource diffusion constraints.
Conclusion
While coordination levels are improving, regional imbalances persist. Promoting balanced digital infrastructure, optimizing resource mobility, and improving digital governance are essential for synergistic development.
Keywords
Introduction
At present, China is confronted with profound structural challenges, including the accelerated aging of its population and the frequent occurrence of major public health emergencies. 1 The traditional healthcare system, constrained by limited service capacity and inefficient resource allocation, can no longer meet the increasingly diverse and multi-level health demands of the public. Meanwhile, the digital economy has emerged as a key engine driving China's high-quality socioeconomic development. As an integral component of public services, the digital transformation of the healthcare system not only enhances resource allocation efficiency and reduces service costs but also generates new avenues for economic growth. In this context, the Chinese government has attached great importance to the coordinated development of the digital economy and the public service system. A series of national strategic documents—including the 14th Five-Year Plan for Digital Economy Development, the Healthy China 2030 Blueprint, and the Medium- and Long-Term Plan for Actively Responding to Population Aging—explicitly emphasize the need to accelerate the deep integration of digital technologies into the healthcare sector, thereby building an efficient, equitable, and sustainable smart healthcare system. From a theoretical perspective, the interaction between the digital economy and healthcare service resources can be viewed as a relationship between two highly interrelated subsystems. The digital economy provides technological empowerment and data support for resource allocation, while the healthcare system, through demand feedback, promotes improvements in digital infrastructure and institutional frameworks. The coupling and coordination process between the two not only reflects the technological diffusion and industrial linkage effects of the digital economy but also demonstrates the adaptation and restructuring of the healthcare system within a digitalized environment.
The digital economy refers to economic activities in which digital knowledge and information serve as key production factors and modern information networks act as the principal carrier. 2 Through digital infrastructure construction, industrial digitalization, and technological innovation, it facilitates the reallocation of resources, thereby improving economic efficiency and governance capacity. Healthcare service resources, encompassing medical institutions, equipment, personnel, technologies, and information systems, constitute an organic whole that underpins the operation of the public health system and the improvement of population health. 3 From the perspective of coupling coordination theory, the digital economy and healthcare service resources function as two closely interlinked subsystems that form a dynamic coupling relationship through a bidirectional mechanism of “technological driving” and “feedback guidance” (see Figure 1). Specifically, the digital economy exerts its driving influence on healthcare service resources in four dimensions. First, digital infrastructure development reshapes the spatial structure of healthcare services by breaking temporal and spatial constraints, promoting cross-regional resource flows, and reducing information asymmetry. Second, technological innovation empowerment—through telemedicine, optimized resource allocation, and personalized treatment—improves the precision and efficiency of healthcare delivery. Third, industrial integration stimulates market vitality by generating new business models, expanding digital finance tools, and diversifying funding channels. Fourth, digital governance enhancement improves decision-making transparency, strengthens regulatory effectiveness, and refines institutional safeguards, thereby optimizing the governance environment for healthcare services. Conversely, the feedback effects of healthcare service resources on the digital economy manifest in four aspects. First, human capital improvement strengthens the foundation of digital economy development by enhancing population health, boosting labor productivity, and supplying a high-quality workforce. Second, industrial linkage expands application scenarios of the digital economy through the development of medical equipment, pharmaceutical R&D, and health management industries. Third, market demand stimulation fosters digital innovation by enriching application scenarios, accumulating data resources, and driving technological iteration and platform integration. Fourth, innovation-driven demand promotes algorithm optimization, product iteration, and service model innovation, thereby accelerating the digital economy's transformation and upgrading. This two-way interactive process embodies the technological diffusion and industrial spillover effects of the digital economy and reflects the healthcare system's adaptive reconstruction under digital transformation.

Coupling coordination theory model.
The integration of the digital economy and healthcare services has become a pivotal topic in global health policy and innovation research. Digital transformation is widely recognized as a crucial driver for addressing inefficiencies in healthcare systems, expanding service accessibility, and improving health outcomes. 4 Early studies primarily focused on the micro level, examining how digital tools such as electronic health records (EHRs), telemedicine, and mobile health (mHealth) enhance healthcare efficiency and reduce administrative costs.5,6 With the advancement of national strategies such as “Internet Plus Healthcare,” research perspectives have gradually shifted from internal technological adoption within medical institutions to macro-level concerns regarding system performance, regional coordination, and governance effectiveness. Aishan et al. empirically examined the significant impact of informatization on healthcare service levels using a provincial dynamic spatial panel model, highlighting the importance of balanced regional digital infrastructure development. 7 Walter et al. argued that digital transformation should extend beyond the technical dimension to focus on institutional design and performance evaluation systems, thus establishing a scientific and dynamic regulatory mechanism guided by healthcare system objectives. 8 In terms of spatial heterogeneity, numerous studies have revealed regional disparities in digital–healthcare integration. Hao and Yu found that the development of the digital economy exerts a significant spatial spillover effect on public health performance, though with pronounced regional differences. 9 Deng et al. constructed a composite digital economy index and demonstrated that its influence on public health service efficiency operates mainly through social media use and urban–rural healthcare disparities, exhibiting significant regional variation. 10 Yuwen et al. measured the digital economy development level and public health service efficiency across 31 Chinese provinces from 2009 to 2018 and found that the positive effects of the digital economy were significantly stronger in eastern regions compared to central and western areas. 11
Despite these valuable contributions, several research gaps remain. First, most existing studies rely on single indicators or subjective weighting methods, limiting their ability to objectively and comprehensively assess the development levels of the digital economy and healthcare resources, particularly their coupling coordination relationship. Second, in-depth exploration of regional disparities and spatiotemporal evolution is insufficient, as most studies employ cross-sectional data for static comparisons, failing to capture dynamic evolution trajectories and distributional shifts. Third, research on spatial spillover effects and regional coordination mechanisms remains relatively weak. Although some scholars have identified spatial correlations in the digital economy, quantitative evidence on spatial dependence and heterogeneity in the coordinated development of digital infrastructure and healthcare resources is still lacking. To address these gaps, this study employs an integrated framework combining the entropy weight method, the coupling coordination degree model, and the spatial Durbin model (SDM) to systematically evaluate the integration level, spatiotemporal evolution pattern, and driving mechanisms of China's digital economy and healthcare service resources from 2012 to 2023. By emphasizing both the direct promoting effects of the digital economy on the healthcare system and the quantitative identification of spatial heterogeneity and spillover effects, this research decomposes regional disparities and underlying mechanisms. The findings provide quantitative evidence for optimizing the allocation of digital healthcare resources, narrowing regional health gaps, and improving multi-level governance systems, as well as empirical and policy insights for constructing a China-specific digital health governance model.
Methodology
Indicator system
Selection of indicators for the digital economy and healthcare service resources
Drawing on existing literature,12–23 the developmental characteristics of China's healthcare service system, and the National Plan for Digital Economy Development issued by government authorities, 24 this study constructs a comprehensive evaluation indicator system for both the digital economy and healthcare services (see Table 1), in alignment with the actual conditions of regional development.
Digital economy and healthcare service resource indicator system.
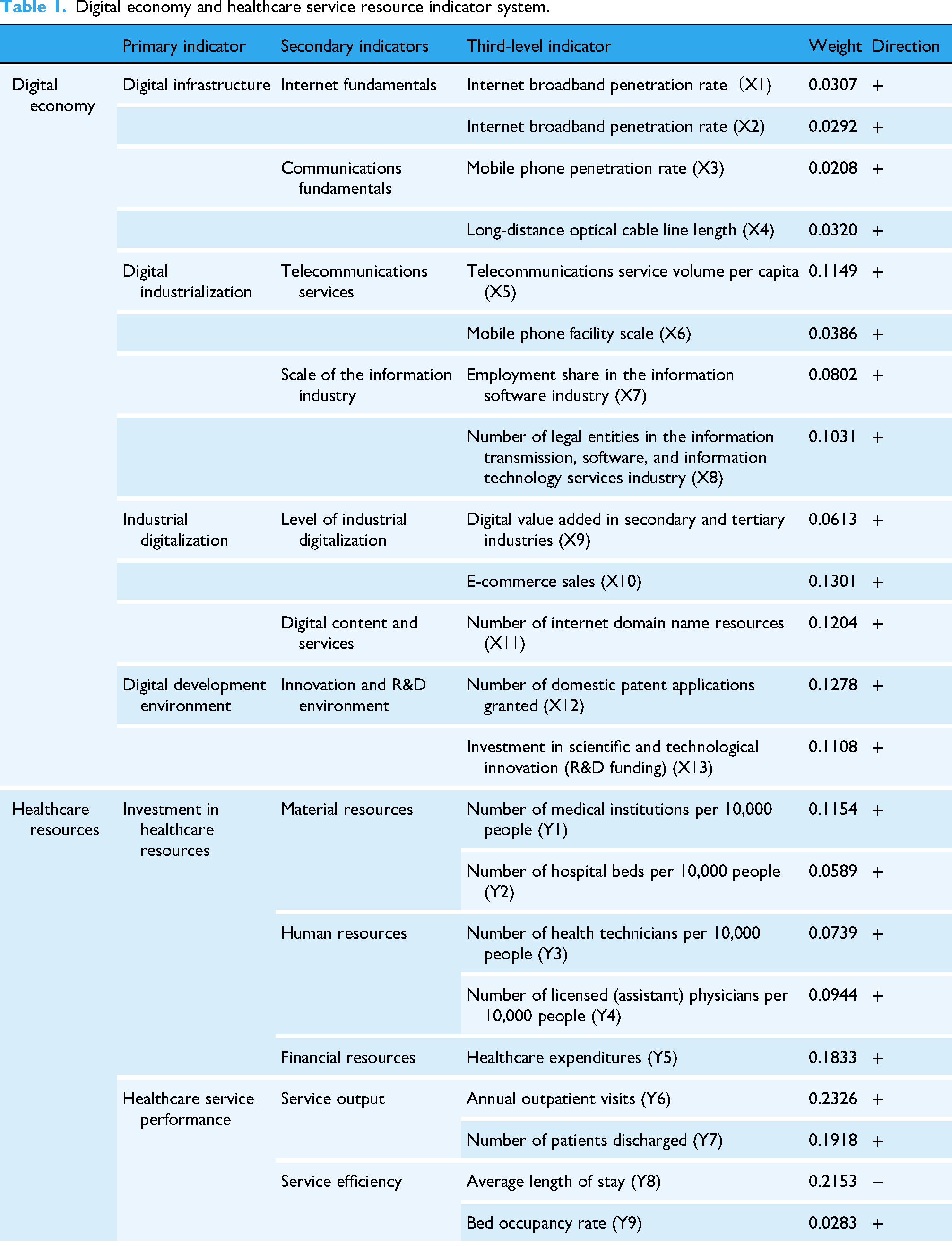
First, the digital economy serves as a crucial engine driving socioeconomic growth. Based on four dimensions—digital infrastructure, digital industrialization, industrial digitalization, and digital development environment—a total of 11 quantitative indicators were selected for measurement. Among these, digital infrastructure represents the material foundation and technological backbone of digital economic development. Through key components such as network facilities, computing power, and data infrastructure, it provides robust hardware support for the widespread application of digital technologies and the inclusive delivery of digital services. On this foundation, digital industrialization reflects the degree to which digital technologies have become industrialized, indicating the scale effect and technological innovation capacity of core digital industries—an endogenous driving force for the expansion of the digital economy. Industrial digitalization, in turn, measures the depth of integration between digital technologies and traditional industries, highlighting the penetration and transformative effects of digitalization on the real economy; it serves as a vital indicator of the overall level of digital economic development. Lastly, the digital development environment, as the institutional and external guarantee of digital progress, encompasses elements such as policy environment, talent support, and innovation ecology, providing the necessary institutional safeguards and environmental conditions for the sustainable development of the digital economy.
Second, healthcare services constitute a vital component of public welfare and directly concern people's well-being. The evaluation of healthcare service quality aims to scientifically assess the supply capacity and service efficiency of the healthcare system. Given the public and social nature of healthcare, its efficiency and quality largely depend on the rational allocation of resources and the effectiveness of service delivery. Accordingly, this study defines healthcare resource inputs from three dimensions: material resources, human resources, and financial resources, which collectively represent the foundational support capacity of the healthcare system. Simultaneously, healthcare service performance is characterized from two dimensions—service output and service efficiency—to capture the actual operational outcomes and quality levels of healthcare provision. The indicators across these dimensions are interrelated and jointly constitute a systematic logical framework of “resource input–service output.”
In recent years, the Chinese government has successively issued a series of key policy documents, including the 14th Five-Year Plan for Digital Economy Development, the Healthy China 2030 Blueprint, and the Medium- and Long-Term Plan for Actively Responding to Population Aging. These documents provide clear policy guidance and institutional guarantees for the coordinated development of the digital economy and healthcare services. They emphasize that several critical factors—such as the level of economic development, talent cultivation, demographic changes, urban–rural integration, and government leadership—play essential roles in promoting the advancement of both the digital economy and the healthcare service system.
Building upon this policy background and existing research,25–28 and guided by relevant theories and practical considerations, this study selects influencing indicators across six dimensions: economic foundation, human capital, demographic structure, spatial pattern, development stage, and policy orientation (see Table 2). Specifically, regional GDP per capita reflects the level of economic development and the capacity for capital investment; the proportion of the population with tertiary education or above represents the stock of human capital and innovation capability; the proportion of the population aged 65 and above captures demographic characteristics and changing service demands; urban population density and the urbanization rate indicate spatial structure and development stage; and provincial government attention to digitalization reflects the intensity of policy support and the institutional environment.
Factors influencing the coupling of China's digital economy and healthcare resources.

Data sources
Data on digital economy indicators were primarily obtained from the China Statistical Yearbook, the Statistical Report on China's Internet Development released by the China Internet Network Information Center (CNNIC), statistical data published by the Ministry of Industry and Information Technology (MIIT), and the statistical yearbooks of various provinces (municipalities and autonomous regions). Data on healthcare service indicators were mainly sourced from the China Health and Family Planning Statistical Yearbook, the China Statistical Yearbook, statistical bulletins on the development of health services issued by the National Health Commission, and provincial (municipal and autonomous regional) health statistical yearbooks.
Due to data availability constraints, this study excludes Hong Kong, Macao, and Taiwan. The dataset covers 31 provincial-level administrative regions in mainland China (including provinces, municipalities, and autonomous regions) from 2012 to 2023. Affected by the epidemic, the data on the number of outpatient and emergency visits and the number of discharged patients in hospitals in Hubei Province in 2020 were missing, and the linear interpolation method was used for supplementation.
Research method
Entropy weight method
The entropy weight method is an objective weighting approach based on information entropy theory, which determines the weight of each indicator by measuring the degree of data dispersion.
First, this method can objectively handle complex multi-level indicator systems. The evaluation system of the digital economy and healthcare service resources constructed in this study involves multiple layers of indicators with significant differences in information content and importance. The entropy weight method effectively avoids subjective bias in the weighting process. 29 Second, it is well suited for large-scale panel data. This study utilizes panel data from 31 provinces in China covering the period 2012–2023, characterized by a sufficient sample size and broad spatiotemporal coverage. The entropy weight method can fully exploit the temporal and spatial variations in the data, ensuring the stability and scientific validity of the weight assignment while retaining as much original information as possible. Third, it demonstrates a strong capacity to handle indicator heterogeneity. The indicators of the digital economy and healthcare service resources differ fundamentally in numerical characteristics and fluctuation ranges. The entropy weight method allocates weights according to the actual information content of each indicator, effectively avoiding bias arising from differences in units of measurement or numerical magnitudes. Although the entropy weight method has certain limitations—such as sensitivity to extreme values and potential neglect of policy orientation—these effects are relatively minor in the context of large-sample panel data. Therefore, considering the characteristics of the dataset and the research objectives, this study adopts the entropy weight method to determine the weights of all indicators.
To eliminate the influence of differing measurement units, the original data are standardized. For positive and negative indicators, the following formulas are applied, respectively:

Here, (1) Calculate the weight of each indicator (2) Calculate the information entropy of each indicator (3) Calculate the weights for each indicator (4) Calculate the composite score




Here,
Coupling coordination degree model
The coupling degree reflects the closeness of the association between two systems, while the coordination degree measures the harmony of their joint development. In line with the research objectives, this study constructs the following model based on the digital economy development level index and the healthcare resource allocation index:
1. Coupling coordination degree calculation

Here, 2. Calculation of the comprehensive development index 3. Coupling coordination degree calculation


The coupling coordination degree
Classification criteria and types of coupling coordination degree.

Kernel density estimation
Kernel density estimation (KDE) is a non-parametric statistical method commonly used to estimate the probability density function of a random variable. This method offers several advantages—it does not require any prior assumptions about the data distribution, provides strong adaptability, and yields intuitive visual results. KDE can effectively reveal the distribution characteristics of variables across different value ranges and is widely applied in studies of regional disparities and dynamic evolution. Following the approach of Changsong et al., 31 this study applies kernel density estimation to panel data across regions and years, including the digital economy development level, healthcare service development level, and coupling coordination degree index. This method allows for the identification of the temporal evolution of these indicators, thereby revealing the dynamic patterns of interaction between the digital economy and healthcare services. Specifically, the shift in the peak position of the kernel density curve reflects the overall upward or downward trend of the indicators, while the change in the curve's shape indicates whether regional development disparities are narrowing or widening—further revealing whether the relationship between the digital economy and healthcare services tends toward convergence or divergence.
The specific kernel density estimation formula is expressed as follows:
Here, 

Here,
Spatial autocorrelation analysis
Spatial autocorrelation analysis is employed to examine whether the distribution of a particular attribute across geographical units exhibits spatial dependence and clustering characteristics. In this study, both the Global Moran's I and Local Moran's I indices are used to measure the overall spatial association and local spatial clustering patterns of the coupling coordination degree between the digital economy and healthcare services.
The Global Moran's I index is used to evaluate the degree of spatial autocorrelation of the study variables across the entire spatial domain. The calculation formula is as follows:
where n denotes the number of spatial units;
The local Moran's I index is used to identify the local spatial association patterns between a specific spatial unit and its neighboring units, thereby revealing the precise locations and types of spatial clusters. Its calculation formula is as follows:
where
Spatial Durbin model
The spatial Durbin model (SDM) simultaneously accounts for the spatial lag effects of both the dependent and independent variables, providing a comprehensive framework to characterize the spatial interaction mechanisms among variables. In this study, a two-way fixed-effects SDM is constructed to investigate the key factors influencing the coupling coordination degree between the digital economy and healthcare services, as well as their spatial spillover effects. The general form of the spatial Durbin model is as follows:
where
Results
Analysis of coupling coordination degree between digital economy and medical resources
The measurement results of coupling coordination degree between China's digital economy and medical resources from 2012 to 2023 (see Table 4) reveal that at the national level, the coupling coordination level between the two exhibited a significant upward trend in the temporal dimension and pronounced spatial differentiation characteristics. From the temporal dimension, the coupling coordination levels of all provinces (autonomous regions and municipalities) demonstrated a sustained upward trajectory. In 2012, the coordination degrees of provinces generally ranged within the low-to-moderate coordination interval of 0.3–0.6, which gradually elevated to the 0.4–0.9 interval by 2023, achieving an overall transition from primary coordination to medium-to-high coordination. From the perspective of development stages: The period of 2016–2019 constituted an accelerated improvement phase, during which coordination degrees exhibited a rapid ascending trend, and inter-regional disparities began to emerge, with the eastern region taking the lead in surpassing the coordination degree threshold of 0.6, followed closely by the central and western regions. The period of 2020–2023 represented a deep integration phase, during which coordination degrees in all regions achieved substantial leaps, with the overall national coordination level advancing into the medium-to-high coordination stage, though inter-regional development gaps further widened.
Coupling coordination degree between China's digital economy and healthcare resources, 2012–2023.
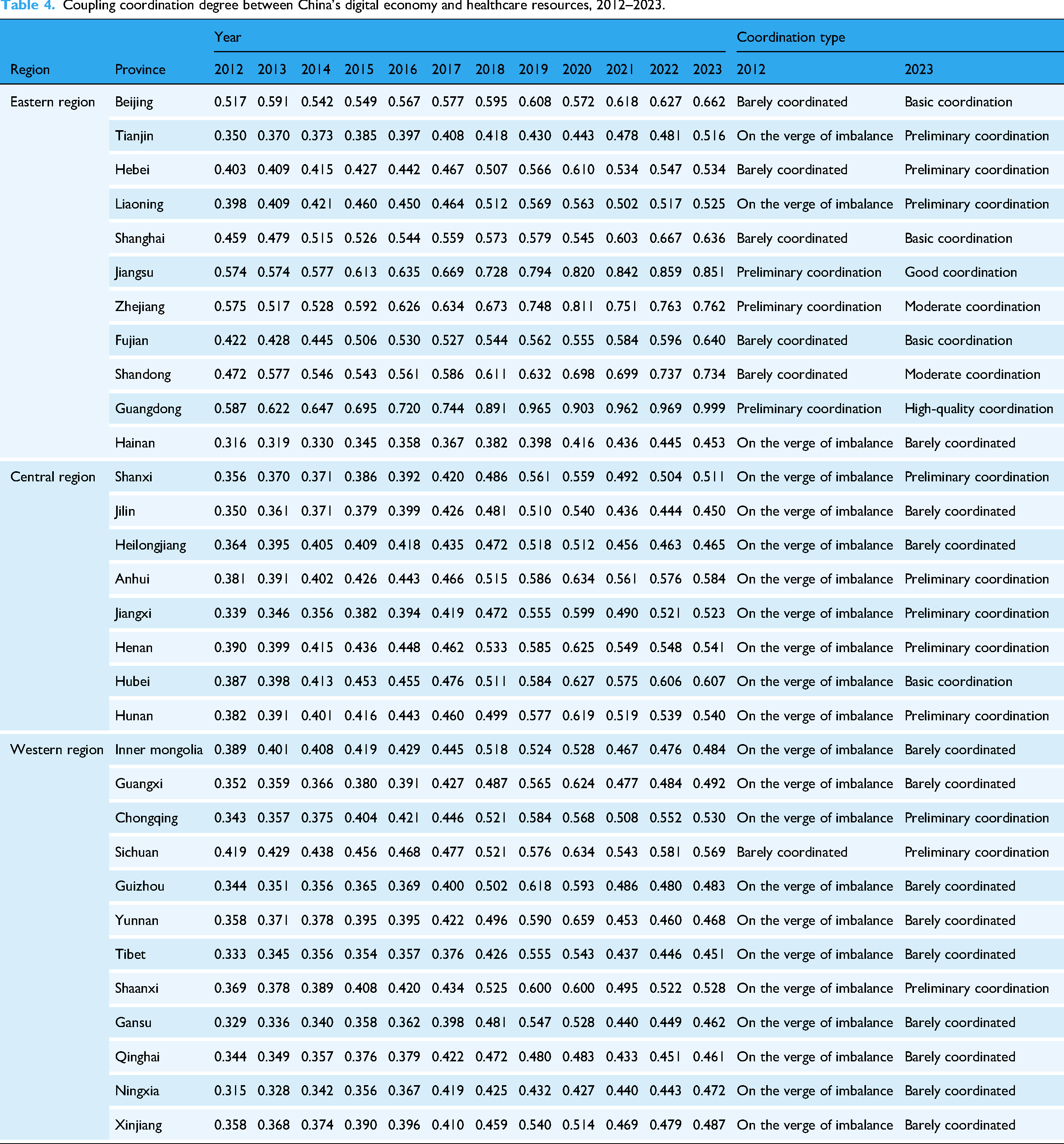
From the spatial dimension, the integration of digital economy and medical resources across China's eastern, central, and western regions presented a distinct pattern characterized by “high stability in the east and catch-up in the west.” The eastern region consistently maintained a high coupling coordination level, with the integration indices of most provinces ranging between 0.6 and 0.9, reflecting a medium-to-strong coordination state. This advantage stemmed from the region's robust economic foundation, advanced digital infrastructure, and high-quality medical resources. Among these, provinces with developed digital economies such as Guangdong, Jiangsu, and Zhejiang maintained coordination degrees consistently ranking at the national forefront. Taking Guangdong Province as an example, its coordination index climbed from 0.587 in 2012 to 0.999 in 2023, approaching a state of complete coordination. The central region demonstrated steady advancement, with provincial coordination degrees gradually rising from the 0.3–0.4 interval in 2012 to the 0.4–0.6 interval in 2023, achieving an overall transition from low coordination to moderate coordination, with Hubei, Hunan, and Anhui provinces exhibiting relatively outstanding performance. Although the western region started relatively late, it displayed significant catch-up development characteristics, with coordination degrees in most provinces substantially increasing from below 0.3 in 2012 to the 0.4–0.5 interval in 2023. Core western provinces and municipalities such as Sichuan and Chongqing played pivotal roles as regional growth poles, with their coordination levels significantly exceeding those of other western provinces. This phenomenon indicates that central cities play a crucial leading role in driving the coordinated development of regional digital healthcare.
From 2012 to 2023, the spatial distribution of coupling coordination degree between China's digital economy and medical services exhibited significant geographical agglomeration characteristics and gradient diffusion effects (see Figure 2).

Spatial distribution of coupling coordination degree across China's regions.
In terms of spatial distribution patterns, high coordination regions were primarily distributed in belt-shaped and block-shaped configurations. National strategic regions such as the Yangtze River Economic Belt, the Beijing-Tianjin-Hebei urban agglomeration, and the Guangdong-Hong Kong-Macao Greater Bay Area formed distinct high-value clusters. Meanwhile, interprovincial boundary effects were prominently manifested, with coordination degrees among adjacent provinces demonstrating strong spatial correlation and spillover effects. This characteristic was particularly pronounced in the Yangtze River Delta integration region and the Pearl River Delta urban agglomeration, where coordination degrees within these regions formed contiguous high-value distribution patterns. From the perspective of diffusion pathways, high coordination regions presented a radiation diffusion pattern characterized by “point-to-area expansion.” Growth poles centered on first-tier cities and provincial capitals exerted significant influence, with their effects gradually transmitting to surrounding prefecture-level cities, thereby forming a spatial development model featuring “core cities as centers radiating and driving surrounding regions”. Furthermore, topography and geomorphology exerted substantial influence on coordination degree distribution, with plains and coastal areas generally exhibiting higher coordination degrees, while mountainous areas and frontier regions remained relatively lagging.
Dynamic evolution of coupling coordination between digital economy and medical resources
At the national level, the coupling coordination between China's digital economy and medical service resources exhibits a dynamic evolutionary characteristic transitioning from fluctuation to convergence (see Figure 3). The national coupling coordination degree displays a multi-peak distribution pattern, with kernel density values fluctuating between 0 and 10. From the temporal dimension, the coupling coordination level is primarily concentrated within the 0.2–0.8 interval, presenting a clear trajectory of dynamic changes. The kernel density distribution gradually evolves from relatively dispersed to concentrated convergence, indicating that the coordinated development between China's digital economy and medical resources is progressively stabilizing. During the study period, the peak distribution of the kernel density function exhibits phased variation characteristics, reflecting the fluctuation patterns of coupling coordination levels across different periods.

Dynamic evolution of coupling coordination levels across the nation and three major regions.
At the regional level, the coordinated development between digital economy and medical resources in China's eastern, central, and western regions demonstrates differentiated evolutionary pathways. The eastern region exhibits a dispersed distribution pattern with the lowest kernel density peak (0–4), and its coupling coordination level is mainly concentrated in the medium-to-high coordination interval of 0.4–0.8, suggesting that overall development in this region is relatively balanced, although internal regional disparities persist. The central region displays a highly concentrated distribution pattern with the highest kernel density peak (exceeding 30), and its coupling coordination level primarily clusters within the 0.4–0.6 interval, forming a distinct “single-peak” agglomeration pattern that reflects the region's high development homogeneity and relatively concentrated development level. In contrast, the western region exhibits moderate concentration characteristics, with kernel density peaks at intermediate levels (0–20), and its coupling coordination level is relatively evenly distributed within the 0.3–0.7 interval, reflecting internal regional development differentiation and insufficient equilibrium.
Spatial correlation analysis
Global autocorrelation
The calculation results of the global Moran's I index for coupling coordination degree based on the geographical adjacency matrix are presented in Table 5. Overall, except for 2019, the global Moran's I indices during 2012–2023 were significantly negative, exhibiting pronounced spatial negative correlation. This indicated that the coupling coordination degree between the digital economy and healthcare services displayed a discrete spatial distribution pattern, where high-value regions were often surrounded by low-value areas, or low-value regions were encircled by high-value areas, with evident disparities in coupling coordination levels between adjacent provinces.
Global Moran's I Index of coupling coordination degree based on the spatial adjacency matrix, 2012–2023.

*** P<0.01, ** P<0.05, * P<0.1
From the temporal evolution perspective, the global Moran's I index of coupling coordination degree exhibited phased fluctuation characteristics. During 2012–2016, the Moran's I index decreased from −0.0815 to −0.0942, with spatial negative correlation continuously intensifying. During 2017–2019, the index rebounded to −0.0555 and became insignificant in 2019, indicating some alleviation of the spatial dispersion trend. During 2020–2022, the index declined again to approximately −0.09 and remained highly significant, with spatial negative correlation re-intensifying. In 2023, the index slightly increased to −0.0898 but remained significantly negative.
Local autocorrelation
The local spatial autocorrelation cluster maps revealed the spatial heterogeneity characteristics of the coupling coordination degree between the digital economy and healthcare services (see Figure 4). From the perspective of spatial distribution types, all three periods exhibited significant local clustering effects, primarily manifested as two spatial heterogeneity patterns: “High-Low” clusters and “Low-High” clusters, where high-value regions were surrounded by low-value areas or vice versa. This corroborated the findings of significantly negative global Moran's I indices. In contrast, homogeneous spatial clustering patterns of “High-High” clusters and “Low-Low” clusters were relatively rare, indicating substantial disparities in coupling coordination levels between adjacent provinces and the absence of a spatial pattern conducive to regional coordinated development.

Spatial distribution of local spatial agglomeration types of coupling coordination degree across provinces based on geographic adjacency matrix in 2012, 2017, and 2023.
From the temporal evolution perspective, the local spatial clustering pattern remained relatively stable overall but underwent localized adjustments, exhibiting a pronounced spatial lock-in effect. During 2012–2017, the number and distribution scope of spatial heterogeneous clustering areas expanded, consistent with the declining trend of the global Moran's I index, reflecting the intensification of inter-regional development imbalances. During 2017–2023, although the global negative spatial correlation experienced fluctuations of initial weakening followed by strengthening, the local clustering pattern did not undergo fundamental changes, with spatial heterogeneous clustering remaining dominant.
Analysis of regression results
Selection of spatial econometric model
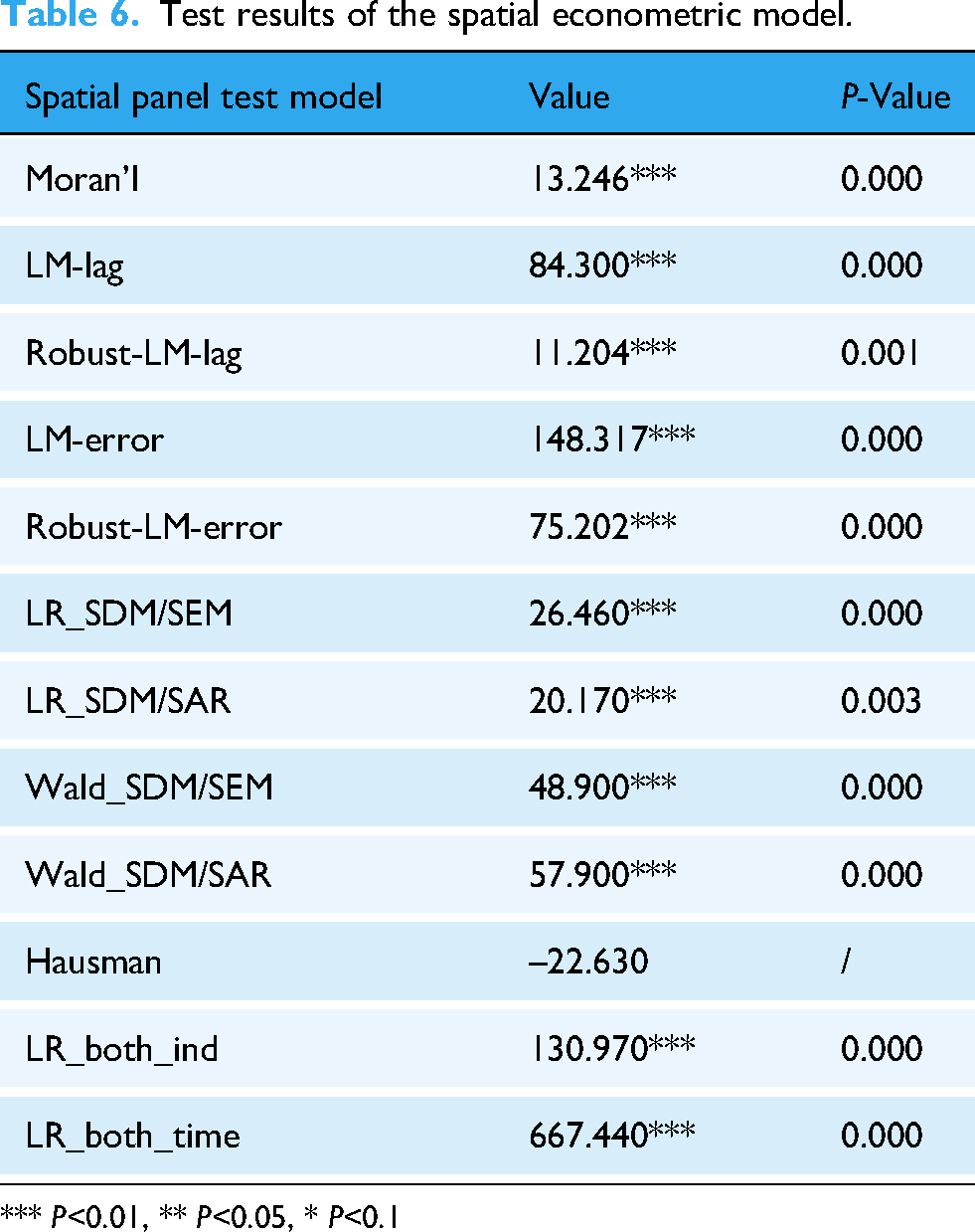
To ensure the scientific validity of the model specification, this study conducted a series of diagnostic tests on the spatial econometric model to determine the final estimation model (see Table 6). First, the global Moran's I index was 13.246, which was significant at the 1% level, indicating significant spatial dependence in the coupling coordination degree between the digital economy and medical services. This suggests that traditional panel models are no longer appropriate, and a spatial econometric model needs to be constructed. Second, the LM test results showed that the LM-lag and LM-error test statistics were 84.300 and 148.317, respectively, both significant at the 1% level. In the robustness tests, the Robust-LM-lag and Robust-LM-error statistics were 11.204 and 75.202, respectively, also significant at the 1% level, indicating the simultaneous presence of spatial lag effects and spatial error effects in the model. This preliminarily suggests that the spatial Durbin model (SDM) should be selected. Furthermore, both the LR and Wald tests were significant at the 1% level, with LR_SDM/SEM and LR_SDM/SAR test statistics of 26.460 and 20.170, respectively, and Wald_SDM/SEM and Wald_SDM/SAR test statistics of 48.900 and 57.900, respectively. These results rejected the null hypothesis that the SDM would degenerate into either a spatial lag model (SAR) or spatial error model (SEM), confirming that the SDM should be selected for regression estimation. Finally, LR tests were employed to compare the goodness-of-fit of different fixed effects models. The LR_both_ind and LR_both_time test statistics were 130.970 and 667.440, respectively, both significant at the 1% level, indicating that the model should simultaneously control for individual fixed effects and time fixed effects. In summary, this study ultimately selected the SDM with two-way fixed effects for the analysis of influencing factors.
Test results of the spatial econometric model.
*** P<0.01, ** P<0.05, * P<0.1
Regression results of the spatial Durbin model
The spatial Durbin model (SDM) results for the coupling coordination degree between the digital economy and medical service resources (see Table 7) show that the spatial autoregressive coefficient (ρ=−1.521, P < .01) is significantly negative, indicating significant spatial correlation in the model and demonstrating that the coupling coordination level across regions exhibits spatial linkage characteristics.
Regression results of the spatial Durbin model.

Standard errors in parentheses.
*** P<0.01, ** P<0.05, * P<0.1
From the effect decomposition results, the total effect of per capita regional GDP (lnx1) is significantly negative (−0.416, P < .01), showing negative and significant effects in both direct and indirect effects. The proportion of population with college education or above (lnx2) shows a significantly positive direct effect (0.108, P < .05), while its indirect and total effects are not significant. The proportion of population aged 65 and above (lnx3) demonstrates significantly negative effects in both the indirect effect (−0.925, P < .05) and total effect (−0.923, P < .05). Urban population density (lnx4) shows negative coefficients across all effects, but none reach statistical significance. The urbanization rate (lnx5) is significantly positive in the direct effect (0.211, P < .05), indirect effect (0.545, P < .1), and total effect (0.757, P < .05). Provincial government's digital attention (lnx6) shows positive and statistically significant effects in both the indirect effect (0.291, P < .1) and total effect (0.296, P < .1). The sign directions and significance levels of the explanatory variables are generally consistent, indicating high stability of the model estimation results.
Regional heterogeneity test based on spatial Durbin model
The sub-sample spatial Durbin model (SDM) regression results (Table 8) reveal significant regional heterogeneity in economic development and educational factors. The impact of per capita regional GDP on the coupling of digital economy and healthcare services exhibits notable differences across the three major regions. In the eastern region, both the indirect effect (0.133*) and total effect (0.139*) are significantly positive, while the direct effect is insignificant. In the central region, the direct effect is significantly positive (0.056***), whereas the indirect and total effects are insignificant. In the western region, the direct effect is insignificant, but both the indirect effect (–0.672**) and total effect (–0.638**) are significantly negative. The influence of educational attainment also demonstrates substantial differentiation: in the eastern region, the direct effect of the proportion of population with college education or above is insignificant, while the indirect effect (–0.270***) and total effect (–0.205**) are significantly negative; in the central region, all three types of effects are insignificant; in the western region, the direct effect is significantly positive (0.179*), while the indirect and total effects are insignificant.
Regression results of the spatial Durbin model (SDM) by subsamples.

The mechanisms of demographic structure and urbanization factors also exhibit pronounced spatial differentiation. The degree of population aging shows opposite effects across different regions. For the proportion of population aged 65 and above in the eastern region, the direct effect is insignificant, while the indirect effect (0.015**) and total effect (0.013*) are significantly positive. In the central region, the direct effect is insignificant, but the indirect effect (–0.435*) and total effect (–0.428*) are significantly negative. In the western region, the direct effect (–0.103**), indirect effect (–0.635*), and total effect (–0.738*) are all significantly negative. The impact of urbanization rate varies across regions: in the eastern region, the direct effect (0.004**), indirect effect (0.012**), and total effect (0.016**) are all significantly positive but with relatively small coefficients; in the central region, all three effects are insignificant; in the western region, the direct effect is insignificant, but the indirect effect (1.084***) and total effect (0.999**) are significantly positive with the largest coefficients. Regarding urban population density, all three effects are insignificant in the eastern region; in the central region, the direct effect is significantly negative (−0.015*), while the indirect and total effects are insignificant; in the western region, the direct effect is insignificant, but the indirect effect (0.264**) and total effect (0.274*) are significantly positive.
The impact of government digital attention demonstrates a gradient decline from eastern to central to western regions. For provincial government digital attention in the eastern region, both the direct and indirect effects are insignificant, while the total effect is significantly positive (0.010*). In the central region, the direct and indirect effects are insignificant, but the total effect is significantly positive (0.057*) with a higher coefficient than the eastern region. In the western region, all three types of effects are insignificant.
Discussion
Addressing regional economic development differentiation and establishing a differentiated allocation system
The empirical results indicate that the total effect of per capita regional GDP on the coupling coordination between digital economy and healthcare services at the national level is significantly negative (–0.416), revealing deep-seated contradictions in regional development: economically developed regions may fall into “path dependence” in resource allocation, while regional heterogeneity tests further confirm this differentiation—the eastern region generates significantly positive effects through spatial spillover effects (indirect effect 0.133), the central region relies on direct investment to enhance local coordination levels (direct effect 0.056), whereas the western region exhibits significantly negative effects due to resource siphon effects (total effect −0.638). This divergence in mechanisms stems from the resource allocation logic at different development stages: the eastern region has entered a technology-driven stage, where economic growth drives digital healthcare development in neighboring provinces through industrial spillover; the central region remains in the factor input stage, where economic resources are directly transformed into local healthcare informatization infrastructure; the western region, however, faces a situation where its limited economic resources tend to flow preferentially to central cities rather than being invested in the digitalization of healthcare services. In response to this regional differentiation pattern, differentiated resource allocation mechanisms should be established: the eastern region should function as a “spillover engine” —for instance, Jiangsu Province exports its smart hospital construction experience to provinces such as Anhui and Jiangxi through the establishment of the Yangtze River Delta Digital Healthcare Collaborative Innovation Alliance; the central region needs to strengthen its undertaking and transformation function by establishing demonstration zones for digital healthcare industry transfer and prioritizing the deployment of regional medical centers and internet hospitals; the western region must break the “center dependence” by establishing east-west digital healthcare collaboration networks through counterpart assistance mechanisms, promoting the downward delivery of quality medical resources to grassroots levels.
The impact of educational attainment (proportion of population with college education or above) also demonstrates significant regional heterogeneity: at the national level, the direct effect is positive (0.108) but the spatial spillover effect is insignificant, while sub-regional tests reveal different mechanisms of educational factors—the eastern region's highly concentrated educational resources paradoxically generate negative spatial spillover (indirect effect −0.270), the central region shows insignificant effects, and the western region exhibits a significant local promoting effect (direct effect 0.179). This differentiated impact pathway reflects the mobility patterns of talent across different regions: the eastern region is rich in higher education resources but experiences the “peacock flying southeast” phenomenon, where highly educated talent concentrates in core cities, exacerbating intra-regional imbalances; the central region maintains relatively balanced talent mobility with educational resources matching healthcare demands; in the western region, each 1% increase in population with college education or above can significantly boost the local reserve of digital healthcare talents. Therefore, targeted talent cultivation and recruitment strategies should be implemented: the eastern region should promote rational mobility of high-level talent—Zhejiang Province, through its “Medical Talent County Plan,” provides targeted training for grassroots medical institutions in digital healthcare technology while establishing talent-sharing mechanisms to facilitate the downward flow of expert resources; the central region should establish a collaborative “medical-educational-research” training system, conducting digital healthcare skills training through regional medical centers; the western region should implement a “talent multiplication plan,” introducing digital healthcare professionals through east-west collaboration with preferential policies such as housing subsidies and professional title advantages, ensuring that talent can be “attracted, retained, and effectively utilized.”
Addressing population aging density challenges and optimizing age-friendly spatial layout
The impact of population aging (proportion of population aged 65 and above) on the coupling coordination between digital economy and healthcare services demonstrates a distinct regional differentiation pattern: at the national level, both the indirect effect and total effect are significantly negative (–0.925, −0.923), but regional heterogeneity tests reveal that aging in the eastern region paradoxically generates positive effects (indirect effect 0.015, total effect 0.013), while the central and western regions exhibit significantly negative impacts (central region total effect −0.428, western region total effect −0.738). This “positive in the east, negative in the central and western regions” differentiation pattern reveals the dual mechanism of aging factors: in the developed eastern region, the growth of the elderly population has generated strong demand for digital healthcare services, driving the development of new business models such as telemedicine and smart elderly care, achieving positive incentives through “demand-driven supply”; whereas in the central and western regions, aging has become a constraining factor due to insufficient medical resources and the digital divide, as elderly groups struggle to adapt to digital healthcare services, creating a “supply-demand mismatch” dilemma. In response to this differentiated impact pathway, a stratified and categorized age-friendly digital healthcare service system should be established: the eastern region should consolidate its “demand-led” advantage by accelerating the development of the smart elderly care industry—Guangdong Province, through its “Internet + Nursing Services” platform, provides home-based medical services to elderly residents at home, transforming aging pressure into industrial development momentum; the central region needs to strengthen age-friendly transformation by simplifying digital healthcare service interfaces, conducting smart technology training for the elderly, and deploying intelligent assistive equipment in community health service centers; the western region should establish an “intergenerational collaboration” mechanism, through family doctor contract services, enabling younger family members to assist elderly individuals in using telemedicine while maintaining traditional service channels to ensure that elderly groups are not marginalized by the digitalization process.
The impact of urban population density is insignificant at the national level, but regional heterogeneity analysis reveals the complexity of its spatial effects: in the central region, increased population density generates a negative direct effect on coupling coordination (–0.015), while in the western region, it produces significantly positive effects through spatial spillover (indirect effect 0.264, total effect 0.274). This contrast stems from the different roles population density plays in various regions: in the central region, excessive urban population concentration leads to strained medical resources, where digitalization efforts cannot keep pace with demand growth, creating a “congestion effect”; in the western region, with relatively dispersed population, moderate population concentration facilitates the co-construction and sharing of digital healthcare infrastructure, generating economies of scale. Differentiated population spatial optimization strategies should be further implemented: the central region needs to relieve medical pressure in central cities by establishing urban medical groups to extend quality resources to new districts and satellite cities, utilizing 5G telemedicine to alleviate congestion in core areas; the western region should strengthen the “point-axis development” model, using urban agglomerations such as Chengdu-Chongqing and Lanzhou-Xining as pivots, deploying digital healthcare service nodes along transportation corridors, improving service efficiency through moderate concentration while establishing mobile medical service stations to cover remote areas, achieving a spatial pattern of “dispersion within concentration, and security within dispersion.”
Releasing urbanization gradient dividends and advancing collaborative radiation pathways
The urbanization rate demonstrates comprehensive positive effects on the coupling coordination between digital economy and healthcare services. At the national level, the direct effect (0.211), indirect effect (0.545), and total effect (0.757) are all significantly positive, indicating that urbanization not only enhances coordination levels through local infrastructure improvement but also drives development in surrounding regions through spatial spillover effects. Regional heterogeneity tests further reveal gradient differences in the effects of urbanization: the eastern region shows significant but smaller effect coefficients (total effect 0.016), reflecting its entry into a mature urbanization stage with diminishing marginal effects; the central region shows insignificant effects, being in the urbanization transition period; the western region exhibits the strongest promoting effects (indirect effect 1.084, total effect 0.999), highlighting that it remains in the urbanization dividend release period. This regional differentiation in impact pathways stems from three mechanisms through which urbanization promotes digital healthcare development: first, the demand agglomeration mechanism, where population urbanization expands the potential market scale for digital healthcare services and reduces unit service costs; second, the infrastructure leap mechanism, where infrastructure construction such as communication networks and data centers brought by urbanization provides hardware support for digital healthcare; and third, the spatial spillover mechanism, where digital healthcare services in central cities radiate to surrounding counties and rural areas through telemedicine and internet hospitals. In response to this gradient advancement trend, differentiated pathways for coordinated development of urbanization and digital healthcare should be established: the eastern region should focus on integrating urban renewal with smart healthcare, embedding intelligent health monitoring facilities in the renovation of old communities to create “15-minute digital healthcare service circles”; the central region should synchronously plan digital healthcare facilities during new urbanization processes to avoid the path dependence of “construction first, renovation later”; the western region should fully release its latecomer advantage by deploying digital infrastructure such as 5G networks and cloud computing platforms during urbanization, achieving simultaneous advancement of physical space urbanization and digital space medicalization, while strengthening the radiation and driving effect of central cities on surrounding regions by extending quality urban medical resources to township health centers through county-level medical community construction.
Strengthening government-guided spillover and improving cross-regional coordination mechanisms
The impact of provincial government digital attention on coupling coordination primarily operates through spatial spillover channels. At the national level, the indirect effect (0.291) and total effect (0.296) are significantly positive, while the direct effect is insignificant, indicating that government digitalization policies generate cross-regional impacts more through demonstration leadership and standard-setting rather than direct investment in local projects. Regional heterogeneity tests show that the effect of government digital attention demonstrates a “gradient decline from east to central to west” characteristic: the total effect is 0.010 in the eastern region, increases to 0.057 in the central region, and is insignificant in the western region. This regional difference in impact pathways reflects the stage-specific characteristics of government roles: in the eastern region, with mature market mechanisms, the government primarily plays the role of “rule-maker,” generating spillover effects through institutional innovation and policy pilots; in the central region, the government functions as an “organizational coordinator,” with the largest coefficient indicating that government promotion is most critical in this region; in the western region, insufficient market development means that policy attention alone is difficult to translate into actual effectiveness, requiring more direct resource investment. A multi-tiered government guidance mechanism should be established: governments in the eastern region should strengthen institutional supply functions, taking the lead in exploring innovative systems such as digital healthcare regulatory sandboxes and data security protection, providing replicable experiences for the nation through pilot programs; Central region governments should actively promote resource integration, establish provincial-level special funds for digital healthcare development, coordinate and align efforts among medical insurance, health commissions, big data and other departments to form policy synergy; governments in the western region should increase fiscal investment, building regional digital healthcare platforms and cultivating local digital healthcare service enterprises through government procurement. Meanwhile, cross-regional government coordination mechanisms should be established, promoting policy experience exchange through platforms such as the Digital China Construction Summit, facilitating the promotion of mature practices from the eastern region to the central and western regions, forming a gradient advancement pattern of “eastern innovation, central undertaking, and western follow-up,” ultimately achieving balanced development of coupling coordination between digital economy and healthcare services nationwide.
Conclusion
This study systematically investigated the spatiotemporal evolution patterns and driving mechanisms of the coupling coordination between China's digital economy and healthcare service resources from 2012 to 2023. The findings reveal that the national coupling coordination level exhibited a significant upward trend in the temporal dimension, achieving an overall transition from primary coordination to medium-high coordination. However, distinct spatial differentiation characteristics emerged, forming a pronounced pattern of “high stability in the east and catch-up in the west.” Spatial correlation analysis unveiled a significant negative correlation in the spatial distribution of coupling coordination degrees, where high-value regions were often surrounded by low-value areas, reflecting substantial inter-regional development disparities and spatial heterogeneity clustering patterns.
The driving mechanism analysis demonstrated that the pathways through which influencing factors operate exhibited significant regional heterogeneity characteristics. Economic development level exerted positive impacts on eastern regions through spatial spillover effects drove coordination level improvement in central regions via direct investment, while manifesting negative effects on western regions due to resource siphoning effects. Factors including education level, population aging, urban population density, urbanization rate, and government digital attention displayed differentiated influence mechanisms across regions, reflecting the complex regional development environment and diversified influence pathways confronting China's digital healthcare development.
This study yields important policy implications. First, a differentiated resource allocation mechanism should be established, with eastern regions serving as “spillover engines,” central regions strengthening “undertaking and transformation” functions, and western regions breaking free from “center dependency” predicaments. Second, precise talent cultivation and recruitment strategies should be implemented, along with the establishment of a hierarchical and categorized age-friendly digital healthcare service system and differentiated population spatial optimization strategies. Finally, tiered government guidance mechanisms and cross-regional coordination mechanisms should be constructed to form a gradient advancement pattern characterized by “eastern innovation, central undertaking, and western follow-up.”
Research limitations
This study explores the degree of coordinated development, dynamic evolution process, and regionally heterogeneous driving factors of China's digital economy and healthcare service resources based on panel data from 31 provinces and municipalities from 2012 to 2023. However, several limitations remain. First, variable measurement relies on proxy indicators, making it difficult to fully capture the complexity and multidimensionality of core concepts. Digital economy and healthcare service development possess complex and multidimensional characteristics, yet the measurement of certain variables in this study relies on proxy indicators that may not comprehensively reflect their connotations. For instance, the study employs indicators such as internet penetration rate and telecommunications service volume to represent the development level of digital infrastructure, which may inadequately capture the quality and accessibility of grassroots-level digital services. Similarly, healthcare service-related indicators primarily focus on quantitative metrics of resource allocation, potentially overlooking the significance of qualitative dimensions such as service quality, patient satisfaction, and treatment outcomes. Second, the analysis is based on provincial-level data, which masks within-province heterogeneity. The study conducts analysis using provincial-level data, a spatial scale that inevitably conceals significant heterogeneity within provinces. Provincial administrative boundaries aggregate regions with markedly different geographic, economic, and institutional characteristics into single analytical units, thereby obscuring refined spatial patterns and localized dynamic changes in coupling coordination relationships. This data aggregation may overlook variations among prefecture-level cities and counties, as well as urban-rural disparities, limiting the identification of micro-level mechanisms and hindering precise targeting of policy intervention points. Finally, this study places greater emphasis on the enabling role of the digital economy in enhancing healthcare services, with insufficient attention to reverse feedback mechanisms. The research primarily analyzes how the digital economy enhances healthcare service capacity, while relatively attention is devoted to the reverse feedback mechanisms whereby improvements in healthcare services stimulate digital economy development. The study does not systematically examine how factors such as improved healthcare infrastructure, enhanced population health levels, and expanded healthcare market scale provide feedback effects on digital economy growth.
In future research, consideration should be given to adopting prefecture-level or county-level data to conduct more refined spatial analysis. Subsequent studies could employ prefecture-level or county-level data to more accurately capture within-province heterogeneity characteristics. Municipal-level data can more clearly identify local factors influencing coupling coordination relationships, facilitate analysis of city-specific policy intervention effects, and reveal urban–rural disparities that remain invisible at the provincial scale. A finer spatial resolution would also enhance the assessment accuracy of spatial spillover effects and clustering patterns, providing support for formulating more targeted policies. Meanwhile, establishing a comprehensive bidirectional analytical framework to systematically investigate the interactive mechanisms between digital economy and healthcare services is essential. Specifically, emphasis should be placed on analyzing how improvements in healthcare service quality and population health levels generate demand for digital technologies, drive innovation in medical technology industries, provide valuable data resources for digital economy development, and catalyze novel business models in the healthcare sector. Through panel vector autoregression (PVAR) models or dynamic simultaneous equation systems, the bidirectional causal relationships between the two can be clarified, and the feedback effects of healthcare service development on digital economy growth can be quantified. Such analysis would more comprehensively reveal the co-evolutionary processes underlying digital health transformation and provide more balanced policy insights for promoting synergistic development of these two critical sectors.
Footnotes
Acknowledgements
We would like to thank all participants who provided assistance for this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: All funding sources related to this study have been fully and accurately listed in the manuscript, with no omission or misstatement of any research funding projects.
Declaration of conflicting interests
The authors declare that there are no potential conflicts of interest (financial or non-financial) that could inappropriately influence the content or conclusions of this article. All authors have no relevant affiliations or involvement with any organization or entity with a financial interest or non-financial interest in the subject matter or materials discussed in the manuscript.