
Abstract
Background
Delays in transporting sputum samples and medicines from peripheral health centers to diagnostic laboratories are a persistent barrier to timely tuberculosis (TB) diagnosis in rural India. Conventional transport methods are often constrained by poor road connectivity, long travel times, and logistical inefficiencies. Unmanned aerial vehicles/drones have shown promise in bridging such gaps in other low-resource and rural areas, yet there is limited evidence on their feasibility, acceptability, and integration within India's National TB Elimination Programme.
Methods
In the present qualitative study, 28 in-depth interviews and 12 focus group discussions with 101 purposively selected stakeholders were conducted to understand the feasibility across the five components: acceptability, demand, practicality, implementation, and integration. Data were thematically analyzed using a feasibility framework. Ethical approval was obtained from the Institutional Ethics Committee (IEC No: AIIMS/BBN/IEC/JULY/2022/164), and written and verbal informed consent was obtained from all participants.
Results
Participants highlighted that drones improved acceptability, demand, and integration by reducing travel, enabling timely sputum and medicine delivery, and building community trust. Practicality and implementation were supported by coordination and district authority support, and while stigma, limited payload, weather disruptions, and training gaps were noted, they were viewed as improvable. Peripheral workers were central to community uptake and routine adoption.
Conclusion
Drone-based sputum and medicine transport is operationally feasible and acceptable in rural Indian settings, and participants viewed drones as a promising way to reduce sample transport times and improve access to diagnostics, particularly in hard-to-reach areas. Addressing awareness gaps, stigma, operational barriers, and regulatory delays, while embedding drones into existing health systems, could enable sustainable scale-up and strengthen rural diagnostic networks.
Keywords
Introduction
Delays in sputum transport and inadequate access to diagnostic facilities remain key challenges across the globe, 1 and in response to this, there has been an increase in the adoption of newer technology like unmanned aerial vehicles (UAVs)/drones to bridge these gaps. 2
The earliest use of drones was documented in South Africa in 2007 for transporting HIV samples from rural clinics to central labs. 3 Since then, Rwanda and Ghana have reportedly developed national drone delivery systems to transport medical supplies like blood, diagnostics, and even vaccines, cutting the delivery time substantially. 4 Also, during the COVID-19 pandemic, drones were used for contactless delivery of essential items to public surveillance. 4 In recent years, India has begun to integrate drones into its public health efforts. The ICMR's i-DRONE (Drone Response and Outreach in North East) initiative demonstrated successful vaccine delivery to remote northeastern states of India using indigenously developed drones, 5 and their evidence suggests strong optimism among the healthcare workers. Apart from this, drones have also been used in disaster management and emergency settings. In Vietnam, the United Nations Development Programme (UNDP) deployed drones for the damage assessment caused by floods, and drones have been reportedly used for glacier bursts surveillance in Uttarakhand, India, and for locust control in Rajasthan, India. 6 Drones have also been used for epidemiological surveillance and vector control by deploying larvicides and sterile insects in malaria-endemic regions. 7 All these examples of the evolving role of drones to help strengthen the health systems emphasize the importance of scaling such technological innovations to improve health care delivery, especially in regions that are inaccessible to proper healthcare.
Conducting drone operations formed an integral part of this study, undertaken under the National TB Elimination Programme (NTEP) to assess the operational feasibility of drone-based sputum and medicine transport in remote and tribal areas of Yadadri-Bhuvanagiri. Using in-depth interviews and focus group discussions with the frontline healthcare workers, this study explores their perceptions regarding the use of drone-assisted services across the five feasibility components of acceptability, practicality, demand, integration, and implementation. The findings from this study can be used to provide scalable approaches for the integration of drone-assisted services in the NTEP, while also identifying the gaps in tuberculosis (TB) services.
Methodology
Study design and setting
Using a thematic analysis approach, this qualitative study was conducted in the Yadadri-Bhuvanagiri district of Telangana, India, a region characterized by remote rural villages with limited access to healthcare services. The study employed a hub-and-spoke model of drone-based sample transportation implemented to support active case-finding activities in the community, wherein tuberculosis units (TUs) served as logistical hubs, and 11 primary health centres (PHCs) and 60 sub-centres (SCs) acted as spokes (Figure 1). Drones transported sputum samples and medicines between these points from February 2024 to February 2025. This district was selected based on its geographic challenges and TB burden, making it a meaningful setting for evaluating early stage implementation of drone-assisted health service delivery. The present study explores the operational feasibility and ground-level acceptability of this intervention in the context of the NTEP.

Administrative map of Yadadri-Bhuvanagiri district of Telangana, showing the 28 IDIs and 12 FGD sites where drone operations were also conducted. IDIs: in-depth interviews; FGD: focus group discussion.
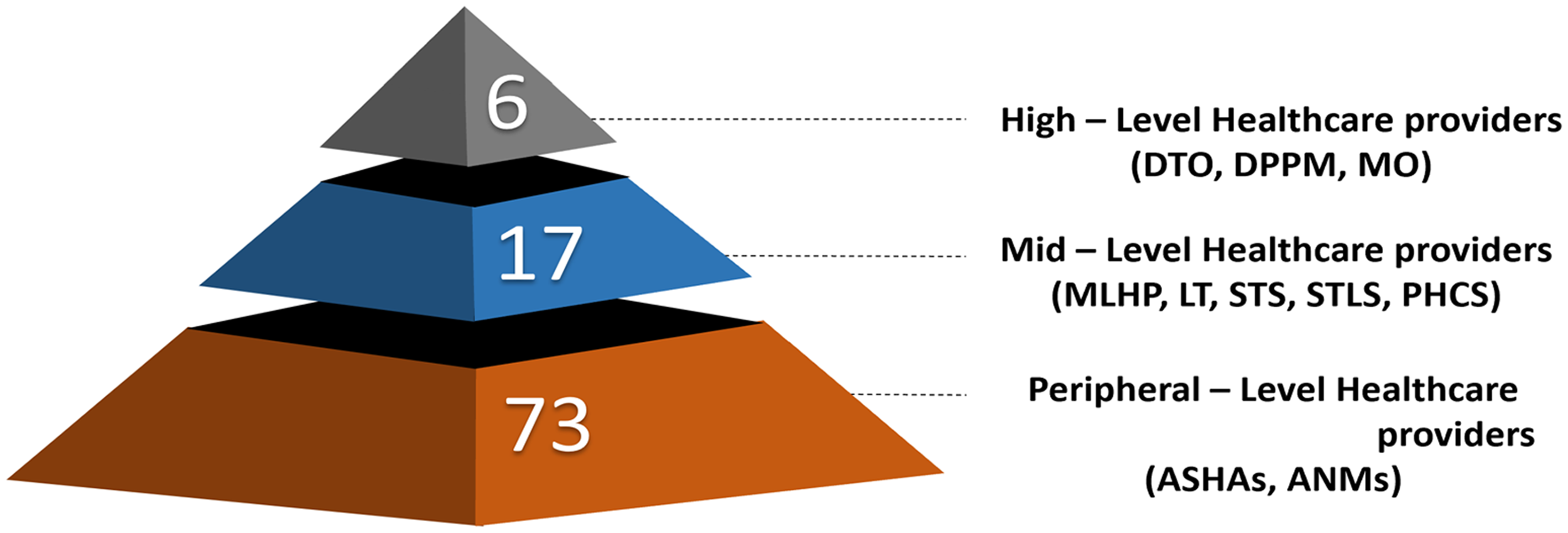
A hierarchical pyramid showing the number of healthcare workers (n = 101) interviewed across three levels of the health system.
Participant recruitment and sampling
To ensure maximum variation, purposive sampling was used. Participants were selected from different health system roles with different levels of exposure or involvement in the drone operations (Figure 2). Data was collected from a total of 28 individuals for in-depth interviews (IDIs), including the district TB officer, district TB program manager, medical officers, and so on (Table 1), and 73 individuals, including 41 Accredited Social Health Activists (ASHAs) and 32 Auxiliary Nurse Midwives (ANMs) (Table 1). All participants had a minimum of 2 years of professional experience with TB-related services. Sampling continued until no new codes or concepts emerged, and this data saturation was tracked using review discussions among the research team after every IDI/focus group discussion (FGD). All sputum samples were collected at PHCs or SCs, and no home collection was conducted, thereby ensuring patient confidentiality. Patients were not directly enrolled as participants to preserve confidentiality; however, random patient exit interviews were conducted to assess perceptions regarding the drone service.
Characteristics of study participants involved in the in-depth interviews (IDI) and focus group discussions (FGDs).

DTO: District TB Officer; DPPM: District TB Program Manager; STS: Senior Treatment Supervisor; STLS: Senior TB Lab Supervisor; MO: Medical Officer; MLHP: Mid-level Health Providers; LT: Lab Technician; PHCS: PHC Supervisor; DO: Drone Operators; ASHA: Accredited Social Health Activist; ANM: Auxiliary Nurse Midwife.
Data collection procedures
Data were collected between February and May 2025 using a combination of in-person IDIs and FGDs. Interviews were conducted in Telugu, English, or Hindi, depending on the participant's preference, using a semi-structured interview guide developed around five feasibility domains. Tools were piloted and customized for each cadre. All interviews and discussions were conducted in private to ensure comfort and confidentiality. Informed written consent was obtained for audio and video (for FGDs) recording, and no non-participants were present. Each IDI lasted ∼15–40 minutes, while FGDs ranged from 20 to 40 minutes. A trained qualitative researcher (BDS and MPH), working as a scientist, led all sessions with the support of a note-taker who documented non-verbal cues and contextual details. During sample collection, persons with presumptive TB were additionally asked an open-ended question to obtain feedback and better understand patient-level responses to the intervention.
Ethics and consent
The study protocol received ethical clearance from the Institutional Ethics Committee (IEC No: AIIMS/BBN/IEC/JULY/2022/164) and the District Medical and Health Officer (DHMO) of Yadadri-Bhuvanagiri. Necessary permissions were also obtained from regulatory bodies such as the Directorate General of Civil Aviation (DGCA) and the Commissionerate of Police to ensure the safe and ethical use of drones. Participants were provided with comprehensive information about the study's purpose, voluntary nature, and confidentiality protocols. Written and verbal informed consent was secured before data collection. All participants agreed to participate, and none withdrew during the course of the study.
Data management
All audio recordings were transcribed verbatim in Telugu/Hindi and then translated into English by trained personnel familiar with local dialects and healthcare terminology. The translated transcripts were anonymized to protect participant identity and stored securely on encrypted devices accessible only to the core research team. A quality assurance process, including random transcript checks by the Principal Investigator, ensured translation and transcription accuracy. Field notes were also digitized and compiled alongside transcripts to enrich contextual understanding. This article adheres to the Consolidated Criteria for Reporting Qualitative Research (COREQ) guidelines.
Trustworthiness and rigor
To ensure rigor, credibility was enhanced through member-checking, and triangulation was employed across methods (IDIs and FGDs) and cadres. Reflexivity was maintained through regular journaling and team debriefs, where potential biases were discussed. These practices helped ensure participant voices remained central to interpretation. Dependability was supported by meticulous use of field notes and reflective memos that captured team deliberations throughout the research process.
Analytical approach
Thematic analysis was conducted using licensed ATLAS.ti (Version 25.01.32924) software. Coding followed a hybrid approach; deductively structured around the feasibility components – acceptability, demand, practicality, implementation, and integration – and inductively driven by participant narratives. The research team collaboratively developed a thematic analysis that captured sub-themes and categories, and descriptions aligned with representative codes, and the discrepancies in coding were resolved through discussion and peer debriefing. The finalized themes reflected facilitators and barriers, and broader applications supporting the feasibility framework. These themes structured the final interpretation of the feasibility and scalability of drone-assisted sputum and medicines transport in rural TB care delivery. Figure 3 illustrates the distribution of perspectives across different healthcare cadres and has been referenced within this section for clarity.

Matrix: Sankey diagrams showing stakeholders’ perspective. (a) High-level healthcare providers and their perspectives. (b) Mid-level healthcare providers and their perspectives. (c) Peripheral-level healthcare providers and their perspectives.

Network framework illustrating how facilitators and barriers influence the feasibility of drone-based sputum transport, as well as their interrelationships.

Results-discussion framework linking key findings from feasibility components to corresponding programmatic implications for drone-based sputum and medicines transport in tuberculosis (TB) care.
Results
Participant characteristics
The study included 101 participants across 28 in-depth interviews and 12 focus group discussions. Participants were purposively selected from various cadres involved in this drone-based transport system (Table 2).
Demographic distribution of participants.

MBBS: Bachelor of Medicine, Bachelor of Surgery; DGO: Diploma in Gynaecology and Obstetrics; MSW: Master of Social Work; BAMS: Bachelor of Ayurvedic Medicine and Surgery; BHMS: Bachelor of Homeopathic Medicine and Surgery; DMLT: Diploma in Medical Laboratory Technology; DGCA: Directorate General of Civil Aviation.
Overview of themes
Three overarching themes emerged from the analysis: Facilitators and Barriers, and Broader Applications of drone-based sputum and anti-TB medicines transport. Each theme captures the social, logistical, and systemic dynamics affecting implementation; sub-themes were structured using the feasibility framework and supported by participant narratives and codes (Table 3).
Distribution of identified sub-themes and categories.

TU: tuberculosis unit; PHC: Primary Health Centre; SC: sub-center; TB: tuberculosis, SOP: Standard Operating Procedure; NCD: non-communicable disease; ANC: antenatal care, ASHA: Accredited Social Health Activist; ANM: auxiliary nurse midwife; DTO: District TB Officer; DPPM: District Public-Private Mix Coordinator; STS: Senior Treatment Supervisor; STLS: Senior TB Laboratory Supervisor; MO: Medical Officer; MLHP: Mid-Level Health Provider; LT: Lab Technician; DO: Drone Operator; NTEP: National TB Elimination Programme; UAV: unmanned aerial vehicle; IEC: Institutional Ethics Committee; DGCA: Directorate General of Civil Aviation.
Thematic presentation
A. Facilitators and barriers supporting the feasibility framework for drone-based sputum and medicines transport
Acceptability
In assessing acceptability, we aimed to understand how well drone-assisted sputum and medicine transport was received by both healthcare providers and communities, recognizing that acceptance would facilitate uptake, while rejection or fear could hinder feasibility.
Fear of New Technology: Initially, drones were often perceived with anxiety and scepticism, particularly regarding safety and confidentiality. Some questioned whether drones could securely transport infectious sputum samples. “Initially, there was hesitation; people were asking, will it really carry the sputum safely?” (MLHP5) “Some were curious but also worried … they had never seen something like this in our village.” (PHCS1) Community Hesitancy and Stigma: In villages with low digital literacy, drones triggered doubt or mistrust. The stigma of TB also intersected, as patients feared being recognized when drones were sent to their homes. “Giving prior information, community meetings, etc., helps … otherwise people are doubtful.” (PHCS3) “Many local workers live five in a room … if one is diagnosed, others get scared.” (MO1) Staff Enthusiasm and Community Trust: Over time, frontline workers played a critical role in shifting perceptions. ASHAs and ANMs leveraged their established rapport to reassure communities and normalize drone operations. “After the first few flights, everyone wanted to be part of it … they would call to check if the drone was coming.” (ASHA2) “Because ASHAs explained it, people didn’t feel scared, and they saw it was for their benefit.” (ANM4) Visible Benefits: Concrete improvements, such as faster testing and reduced travel, reinforced acceptance and encouraged broader participation. In addition to sputum, the delivery of medicines by drone further strengthened acceptability, as staff recognized its direct utility for patient care. “Samples went faster with minimal travel … that made people believe it works.” (MO2) “We got medicines as well through drone, and it was a good experience as we did not have to travel to the PHC for medicines…” (ASHA19)
Demand
In examining demand, we sought to assess whether patients and providers perceived drones as a service worth engaging with. High demand would indicate feasibility for scale-up, while low uptake or preference for conventional methods would signal barriers.
Lack of Awareness and Underuse: At the start, limited awareness about drones restricted their use. Patients were often unaware of their role in sputum transport, leading to hesitancy. “Patients would ask why the drone was here, they had no idea it was for TB samples.” (PHCS2) “Even though drones were coming, in the beginning, very few samples were sent … people were watching first.” (MLHP4) High Patient Interest: As patients began to observe drones, they expressed satisfaction and eagerness to participate, especially due to reduced time and wage loss. “When patients saw the drone land, they asked if their sample could go immediately.” (PHCS1) “I am happy I do not have to lose an entire day of work…” (Person with presumptive TB feedback) Ease of Access: By overcoming geographical barriers, drones improved accessibility for remote communities. “For villages far away, this saved a lot of travel time.” (ANM7) “Yes, it helped them a lot, they were so happy.” (ANM6) Stigma Reduction: In some facilities, drones helped normalize sputum collection and reduced embarrassment linked to TB. “People were ready to give their samples and did not protest as they usually do, and it helped us also.” (ASHA10)
Practicality
Our focus on practicality was to evaluate whether drones were operationally viable in real-world settings, addressing issues of capacity, timeliness, reliability, and external constraints such as weather. If drones proved practical, they could enhance system efficiency; if not, they risked being unsustainable.
Storage Limits: Drone payload capacity was restricted to 8–10 samples per sortie, necessitating multiple trips on busy days. “If there are more than 8–10 samples, we have to wait for the next trip.” (MO3) “We had to ensure samples are transported before 2 PM…” (DO2) Weather Dependency: Flights were often disrupted by heavy rains or winds, compelling workers to revert to road transport. “During the rainy days, the drone couldn’t come … we had to send samples by road.” (MO4) Drone Malfunctions: Occasional technical issues like signal loss or battery drainage created delays and uncertainty. “One day, there was a signal problem and the schedule changed suddenly.” (MLHP2) Timely Delivery, Pilot Support, and Smooth Operations: When operational, drones consistently accelerated delivery of both sputum and medicines, reassuring staff through coordinated support from pilots and research teams. ASHAs and ANMs valued this particularly, as it reduced the need for separate visits to collect drugs for patients. “People were hesitant to get tested as it used to take up their entire day, now it is a matter of minutes.” (MO2) “Pilots, research team, and our team all coordinated well with each other, and the pilots explained the process initially so we remain confident.” (MO3) “Instead of a week, our work was getting done in one day … so we worked a little extra on one day, and it encouraged us.” (ASHA14) “Medicines also came on time through drone, and it helped us give them to patients quickly.” (ANM6)
Implementation
In the domain of implementation, we aimed to understand how drones could be embedded within the TB program, focusing on regulatory approvals, staff preparedness, and stakeholder coordination. Smooth implementation was a key determinant of feasibility, while delays or gaps posed barriers.
Delayed Permissions and Training Issues: Administrative clearances slowed the early roll-out. In addition, frontline workers felt underprepared due to insufficient training. “The issue is with planning and coordination; sometimes the schedule is not followed exactly.” (STS5) Good Coordination and District Authority Support: Once approvals were secured, strong coordination between drone operators, research teams, and PHC staff facilitated smooth operations. District leadership added legitimacy and encouraged staff compliance. “They worked with us to fix the timings so we could prepare samples on time.” (PHCS2) “Because the DTO supported it, staff took it seriously.” (STS2)
Integration
In exploring integration, our aim was to determine whether drones could align with existing TB workflows and be sustained within daily health system operations. Integration was seen as a marker of long-term feasibility.
Reporting Delays and Miscommunication: Although drones sped up physical delivery, lapses in communication between PHCs and TUs, or delays in laboratory reporting, reduced perceived benefits. “The issue is with planning and coordination; sometimes the schedule is not followed exactly.” (STS5) Alignment with Workflows and Routine Adoption: Despite initial hiccups, drones were eventually embedded into routine TB services without major disruptions. The inclusion of medicines along with sputum reinforced continuity of care and was widely appreciated by ASHAs, ANMs, and PHC staff. “We got medicines as well through drone, and it was a good experience as we did not have to travel to the PHC for medicines…” (ASHA19)
B. Broader applications of drone technology in rural health systems
Beyond TB sputum and medicines transport, participants envisioned wider uses of drone technology in addressing public health challenges in remote regions.
Community participation in newer technology
Motivation to Reduce Patient Burden: Many health workers viewed drone use as a meaningful innovation that reduced delays and lessened patient travel needs. The possibility of delivering results or medicines closer to patients was seen as a valuable way to improve access and continuity of care. “Patients don’t have to come all the way to the hospital now … it saves their strength and money.” (ASHA) Perspectives of Healthcare workers: Several staff members expressed personal satisfaction in being part of a pilot that served hard-to-reach populations. Their active involvement was framed as a form of public service and innovation-driven motivation. “It feels good to be part of something new that helps people here.” (MO1) Community Perspective: Individuals with presumptive TB also shared positive feedback about the intervention, noting that drone-based transport eased their logistical and financial burden. They appreciated that they no longer needed to spend on transport or lose wages while travelling to distant facilities for sample submission or results. “Before, we had to take a day off and go far to give samples … now we can do it nearby and don’t lose money or work.” (Person with presumptive TB feedback)
Scope for expansion
Drones for Vaccines: There was strong support for using drones beyond TB, especially for transporting vaccines, blood samples, and even organs to outreach sessions in difficult terrains or during emergencies. Drones were seen as promising for ensuring cold chain temperatures and reaching underserved areas.
“It can help during monsoons to use drones for dengue testing.” (MO4).
“We can use it to send organs, blood samples, so many things … I have worked with organ transporting using drones, so I know it can be a game changer.” (DO2)
Diagnostics, NCDs, and ANC Services: Respondents suggested extending drone-based transport to other diagnostic services, including blood and urine samples for non-communicable diseases (NCDs), antenatal care (ANC), and so on. Such expansions were seen as logical and highly beneficial in difficult settings.
“It can carry blood samples, medicines for BP or sugar, even ANC reports.” (ANM17)
C. Perspectives of stakeholders on the various aspects of drone feasibility
Figure 3 matrix highlights how perspectives on drone feasibility varied across different cadres of healthcare providers. High-level staff (Matrix A), such as medical officers, DTOs, and DPPMs, most often discussed barriers and acceptability, reflecting their focus on stigma, safety, and the administrative processes required to legitimize drone operations. Mid-level providers (Matrix B), including MLHPs, STS, PHC supervisors, LTs, and STLS, emphasized both barriers and demand, underscoring practical constraints such as sample capacity, weather dependence, and laboratory coordination, alongside growing patient interest and uptake. In contrast, peripheral-level providers (Matrix C) ASHA workers’ and ANMs’ narratives concentrated around community response, acceptability, and implementation. Positioned as trusted intermediaries, they played a pivotal role in reducing stigma, encouraging patient participation, and embedding drones into routine sputum and medicine transport. Together, these perspectives illustrate that while higher-level staff frame feasibility in terms of systemic enablers and constraints, mid-level staff focus on operational realities, and peripheral staff drive community trust and day-to-day integration, demonstrating the need to engage all cadres for effective scale-up of drone-assisted health services.
Discussion
This section discusses the five key feasibility components identified in this analysis—acceptability, demand, practicality, implementation, and integration—and reflects on the potential broader application of drone technology in rural health systems. Healthcare workers expressed optimism, viewing the intervention as a potential solution to logistical gaps in TB diagnostics.
Findings from 28 IDIs and 12 FGDs reported that drones could expedite diagnosis by cutting down the sample transport, enabling earlier treatment initiation. Similar benefits have been seen in Rwanda's “Uber for blood” program, where drone delivery reduced transport time to < 45 minutes. 8 The time savings, in addition to community trust in the healthcare system, were seen as major facilitators in this study. Despite this, many barriers were also highlighted. Low awareness of drone technology among both community members and some staff members, combined with TB-related stigma, created concerns that drone use could inadvertently reveal a patient's TB status. These concerns mirror those observed in a study in Nepal found that successful implementation required community engagement. 9 Before scale-up, it might be beneficial to sensitize the community about both TB and drone technology. Also, leveraging the influence of trusted local figures like ASHAs or ANMs as drone ambassadors can enhance acceptance. 10 These experiences highlight that early investment in awareness campaigns and meaningful engagement with community stakeholders may greatly improve acceptability and help reduce stigma in future drone-enabled TB programs.
In terms of demand and practicality, many said that it was a much-needed intervention, especially in villages with disconnected transport, old people who have no support, and patients who are not able to travel due to financial instability. They also saw value beyond TB samples, indicating latent demand to integrate the drones into broader health services like vaccines, blood samples, dengue tests, and so on, as seen in Malawi 11 and Guinea, 12 where drones were used for HIV testing of infants, but turning this demand into sustained use will require addressing operational challenges. Adverse weather conditions, such as heavy gusts and rain, were frequently cited as hindering operations, while hilly terrain caused minor navigation and landing issues. Similar challenges were observed in the drone trials in the Himalayas of Himachal Pradesh. 13 Having risk mitigation frameworks for prolonged bad weather, as highlighted in a study by Kumbhani et al., 14 and investing in drones equipped to handle local environmental conditions may help overcome these issues.
Implementation and integration of drone operations with existing NTEP workflows were seen as essential for sustainability and smooth adoption. Participants felt that when the timings matched the routine schedule and there was support from district authorities, the process was smoother and easier to conduct. Regulatory hurdles were also observed during this study, causing delays in operations. Similar challenges were reported in Nepal, and in contrast, supportive regulations in Rwanda and Ghana enabled rapid scale-up of services. 10
In our study, stakeholders were positive but questioned who would fund and maintain operations after the pilot phase. Similar concerns were raised in Nepal, where communities asked whether the investment was “worth it” without continued support. 9
While drones require upfront and operational costs, participants have said that they reduced patient out-of-pocket expenses by reducing travel expenses, etc. It was observed that drones slightly outperformed motorbikes in cost per sample in difficult terrain in Himachal Pradesh. 2 Nevertheless, if drones continue to prove their ability to save time and improve health outcomes, they may attract funding from TB programs aiming to reach national targets. Integration into the government health budget or public–private partnerships, for example, contracting drone logistics firms, could provide stable financing beyond the pilot stage. Importantly, scale-up should also explore leveraging drones for other healthcare deliveries—medicines, vaccines, lab samples for other diseases—as participants suggested, to maximize utilization and impact across the health system.
To our knowledge, this is one of the first in-depth qualitative investigations into drone-based TB specimen transport in the Indian context. By including a wide range of health personnel, from ASHA workers to district TB officer, and structuring analysis around a multi-component feasibility framework (Figure 4), this study gained a holistic understanding of the facilitators and barriers. The use of FGDs alongside interviews enriched the data by capturing collective viewpoints and debates among frontline workers; these strengths add credibility and relevance to the findings.
However, we acknowledge several limitations. First, the study was conducted in a single district, and perceptions in other regions might diverge. Second, this being at a pilot stage during data collection, participants’ opinions were largely based on a few drone operations, and real-world implementation might reveal unforeseen challenges. Third, we did not quantitatively evaluate economic feasibility, which remains a key concern for scalability. Future research should incorporate cost assessments to validate the feasibility insights reported here. Despite these limitations, this study provides timely qualitative evidence that can guide context-appropriate strategies for introducing drones into TB care.
In conclusion, drone-based sputum transport was seen as acceptable and feasible in rural settings, provided there is successful community engagement, adequate training, and preparedness for risk management (Figure 5). Many studies show that with preparation and support, drones can overcome geographic barriers to strengthen service delivery.8,9
By situating drone networks within existing TB control efforts and the broader health delivery ecosystem, India and similar high-TB-burden countries can move closer to closing the access gap and delivering equitable care, even in the most remote corners.
Conclusion
This study demonstrates that drone-assisted sputum and medicine transport is feasible in remote rural settings, with strong acceptability among healthcare workers once initial hesitations are addressed. While drones offered clear benefits in reducing transport time and improving access to diagnostics, their sustained use will require community engagement, staff training, streamlined regulatory processes, and integration into existing TB workflows. This study successfully implemented a drone-based sample and medicine transport system under routine programmatic conditions; however, addressing operational challenges such as weather disruptions and limited payload capacity will be essential. With these measures in place, drones could become a reliable component of rural health logistics, contributing to earlier TB diagnosis and improved health system reach, which will ultimately be helpful to achieve the Sustainable Developmental Goals of TB elimination in India.
Footnotes
Acknowledgements
We extend our sincere gratitude to the district administration and the Health Department, particularly the DTO, DPPM, Medical Officers, MLHPs, LTs/STLS, ASHAs, ANMs, PHC supervisors, and drone operators, for their timely participation in the IDIs and FGDs and for providing valuable insights. We also acknowledge the dedicated efforts of our research staff, Mr S Vidyasagar and Mr K Nandhakishore, whose meticulous note-taking and support were instrumental during the data collection phase. Minor editorial assistance using AI tools was employed only for language refinement wherever deemed necessary. ![]() matrix is made with sankeymatic.com.
matrix is made with sankeymatic.com.
Author contributions
All authors contributed to conceptualizing the study. Data collection, including conducting the IDIs and FGDs, was carried out by Dr Bhushan and Dr Gayatri. Data analysis and interpretation were primarily undertaken by Dr Bhushan, Dr Meely, and Dr Gayatri, with additional contributions from Dr Sumit, Dr Kuldeep, Dr Vidya, Dr Rashmi, and Dr Neeraj. Technical inputs on drone logistics and health system integration were provided by Dr Bhushan, Dr Sumit, Dr Vikas Bhatia, and Dr Kuldeep. All authors participated in regular discussions and cross-verification after each IDI and FGD as part of the triangulation process. The manuscript was drafted by Dr Gayatri with critical revisions from all co-authors. All authors reviewed and approved the final version of the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was funded by the Indian Council of Medical Research (ICMR) Extramural Grant with a sanction order: HIV/STI/11/02/2022-ECD-II.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Guarantor
Dr Sumit and Dr Bhushan are the guarantors of the work.