
Abstract
Background
Many seniors need to increase their physical activity (PA) and participation in fall prevention exercise. Therefore, digital systems have been developed to support fall-preventive PA. Most of them lack video coaching and PA monitoring, two functionalities that may be relevant for increasing PA.
Objective
To develop a prototype of a system to support seniors’ fall-preventive PA, which includes also video coaching and PA monitoring, and to evaluate its feasibility and user experience.
Methods
A system prototype was conceived by integrating applications for step-monitoring, behavioural change support, personal calendar, video-coaching and a cloud service for data management and co-ordination. Its feasibility and user experience were evaluated in three consecutive test periods combined with technical development. In total, 11 seniors tested the system at home for four weeks with video coaching from health care professionals.
Results
Initially, the system's feasibility was non-satisfactory due to insufficient stability and usability. However, most problems could be addressed and amended. In the third (last) test period, both seniors and coaches experienced the system prototype to be fun, flexible and awareness-raising. Interestingly, the video coaching which made the system unique compared to similar systems was highly appreciated. Nonetheless, even the users in the last test period highlighted issues due to insufficient usability, stability and flexibility. Further improvements in these areas are needed.
Conclusions
Video coaching in fall-preventive PA can be valuable for both seniors and health care professionals. High reliability, usability and flexibility of systems supporting seniors are essential.
Introduction
Falls are a major global health problem, especially among adults over the age of 60 years. 1 The risk of falls is particularly severe in older adults developing frailty (a vulnerable state characterized by reduced homeostatic reserves) 2 and sarcopenia (a disorder involving progressive loss of muscle mass), 3 two states characterized by physical function impairment. 4
Physical activity (PA) has several positive health effects for the older population including physical abilities and cognitive outcomes and is a cost-efficient strategy to prevent falls and fall-related injuries.5,6 PA also plays an important role in treatment of frailty and sarcopenia.7,8 Global recommendations on PA for health for adults aged 65 years and older are the same as for adults in general with the addition to: ‘as part of their weekly PA, older adults should do varied multicomponent PA that emphasizes functional balance and strength training at moderate or greater intensity on 3 or more days a week, to enhance functional capacity and to prevent falls’. 6 However, adults aged 65 years and older (hereafter called seniors) represent one of several groups where insufficient PA is particularly severe. 9 Moreover, seniors’ uptake and adherence to fall prevention exercise programs are low.10,11
E-health interventions, interventions delivered by digital means, are effective in increasing seniors’ PA performance and have been recommended for inclusion in guidelines to enhance PA in seniors. 12 Also, technology-based exercise interventions can increase seniors' adherence to exercise programs and may provide a sustainable means of promoting PA and preventing falls in seniors. 13 Moreover, the incidence of mobility disability in older adults with physical frailty and sarcopenia can be reduced by a multicomponent intervention based on PA with technological support and nutrition counselling. 14 Also there exists promising research on using virtual reality (VR) as a tool for promoting PA in seniors; however, the effects on the involved subjects are still missing solid validation. Even more important, there exist relevant doubts about a number of factors such as frailty, usability and acceptability of these VR interventions for seniors and knowledge on cost-effectiveness of immersive VR. 15
Digital behaviour change interventions refer to technology designed to promote and maintain health 16 and that includes behavioural change techniques (BCTs). 17 A rapid review of publicly available apps and websites supporting seniors in strength and balance training independently identified no sources or sites evaluated in randomized controlled trials (RCTs) but recommended four apps and six websites based on evidence-base, quality and BCT scores. 18 One of the apps 18 was later reported to have significantly reduced rate of falls and number of injurious falls over two years in an RCT including 503 seniors. 19 Research-based apps combining home-based balance- and strength training with motivational instruments include ActiveLifestyle, 20 Safe Step 21 and M-OTAGO. 22 ActiveLifestyle has shown to significantly improve single- and dual-task walking compared to brochure guided training 23 and seniors using Safe Step have shown similar adherence to a four-month intervention as paper booklet guidance and has been indicated to facilitate long-term maintenance in regular exercise. 24
The apps presented above are used independently by seniors. A previous study performed by the authors of this article designed a system based on needs and preferences from seniors, health care professionals (HCPs) and key stakeholders in health care organizations.25,26 Compared to the apps and webpages described above, this system contains a combination of the features present in the existing digital resources (i.e., behaviour change support and exercise programs) and new functionalities (i.e., video coaching and step counting). In this respect, several studies have suggested that video coaching may improve adherence and effectiveness of digital health interventions for PA, 27 and that step counting may increase PA participation. 28 Adding these two functionalities to digital support for seniors’ PA might create new, effective ways to boost seniors’ motivation for PA. However, the complexity of the system increases with the number of functionalities included, both technically and for the user. It is, therefore, essential to evaluate the drawbacks and benefits of the different integrations at early development stages. In fact, the need for pragmatic approaches to evaluate digital health solutions has been identified. 29 Although early feasibility studies can be of high value as guidance for further research, lessons learnt from pilot and feasibility studies are often not published. 30
The aim of this study was to develop a prototype of a system to support seniors’ fall-preventive PA, which includes also video coaching and PA monitoring (setup in Figure 1), and to evaluate its feasibility and user experience.
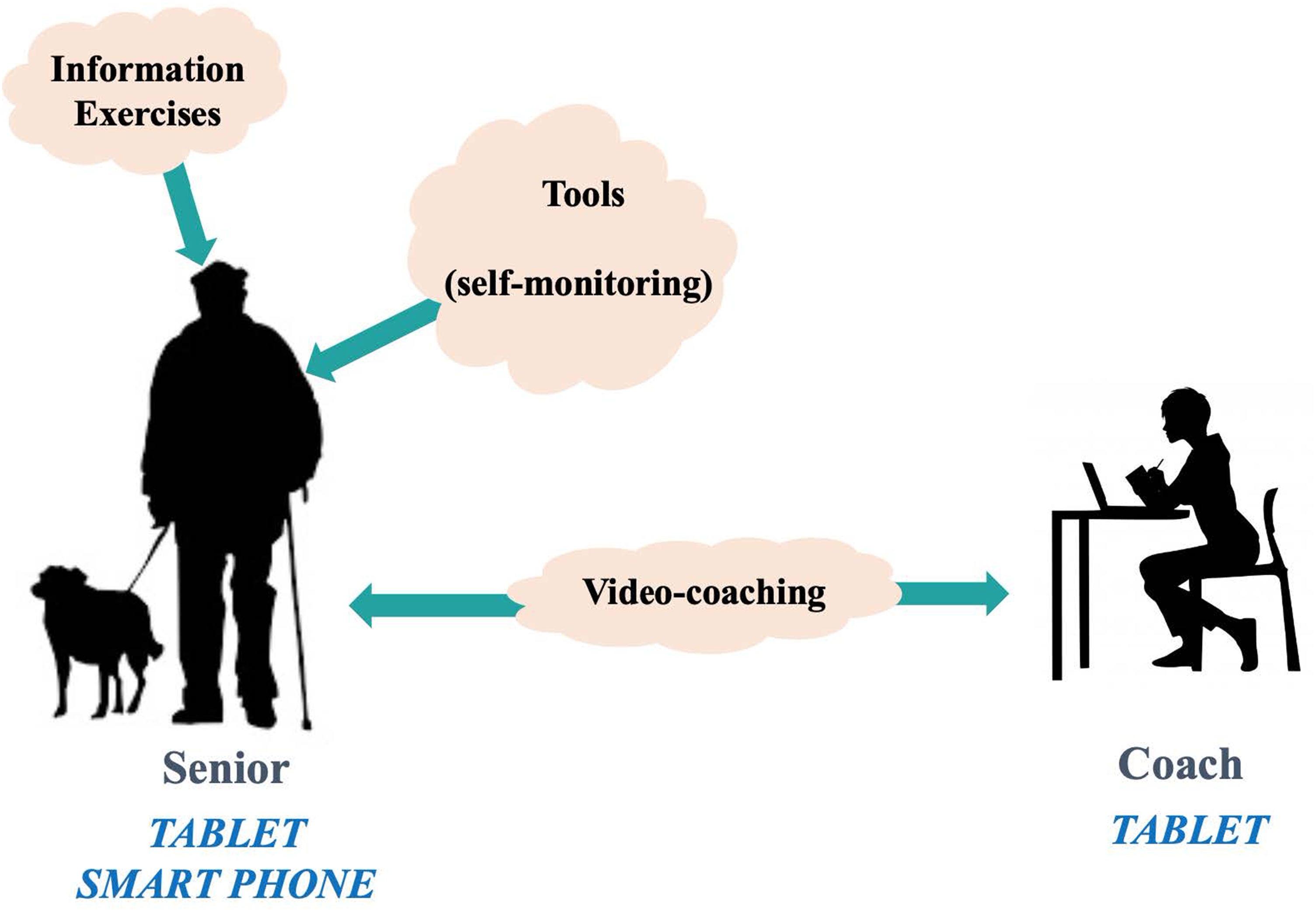
System setup.
This article presents the system prototype and its development together with the results from the evaluation. Based on the study results, we elaborate on the advantages and drawbacks of the strategy to integrate existing applications, as well as summarize lessons learnt from the work. We believe that the described experiences can be of benefit to future research on e-health for seniors, especially related to interventions to support PA and fall-preventive exercise.
Method
System architecture and development
The system was developed in a project aiming at promoting PA in seniors to reduce their fall risks. In this respect, an information system (IS) was designed based on requirements from seniors, HCPs and health care organizations. 26
The system provided the seniors with information, exercises to strengthen balance, self-monitoring tools (goal setting, planning, activity monitoring including a step counter, self-evaluation and feedback) and regular coaching via video from an HCP. Therefore, the integrated system (overview in Figure 2) included the following user applications: (i) a mobile phone–based step counter application; (ii) a motivation support application with features to set goals for steps and other PAs, scheduling PAs, self-evaluations of performed PAs, visualizing levels of goal achievement and setting new goals, etc.; (iii) a video communication application integrated with a video-client application, to enhance the communication between seniors and HCPs. The IS was co-ordinated by a cloud service to create and store the system users and to store their step data over time.

Overview of the system.
Given the feasibility boundaries due to the time frame of the project (two years) and aiming at implementing a system prototype and evaluating its feasibility in a real-world setting, the system was conceived as an integration of existing applications that had been identified from user requirements 26 and were delivered by four technology providers (three small and medium-sized enterprises (SMEs)and one university). The integrated system included both digital services developed or customized for the project (Revenäs et al., 2023, Towards digital inclusion of older adults in e-health: A case study on support for PA, submitted to Universal Access in the Information Society) and existing ones. Hence, the system integration in this study had a bottom-up perspective and thereby differ from recommendations for the development of Smart Home Technology Innovation for People With Physical and Mental Health Problems. 31 Therefore, the principles that drove the selection of the components to be integrated and thereby gave place to a target system architecture in this study, are discussed in “Discussion” section of this article. Nonetheless, in the remainder of the article, we illustrate concrete implementations of the components that, in some cases, diverged from the original plans as side effects of user evaluations and feedback, as well as constraints and limitations of available technologies.
Mobile app for step counting: Data acquisition and communication
Recommendations on PA for adults aged 65 years and above include both general PA and PA emphasizing functional balance and strength training. 32 Therefore, measuring the level of seniors’ general PA represented a critical aspect of the system. A preliminary internal survey excluded specific solutions like the development of on-purpose sensors and suggested to opt for activity monitors widely available on the market. Moreover, devices simple to use and easy to integrate with the other components (notably, allowing the automated sharing of recorded activity data) were needed.
Motivation support: User interaction and communication
Livanda 33 is a Swedish SME that develops digital solutions for the treatment of health problems (e.g., stress, anxiety, depression and insomnia) based on cognitive behavioural therapy. Among these, it provides a web-based application for self-support in behavioural therapies. For the system used in this study, Livanda's web-app played the role of motivation support. The application was meant to provide seniors with a dashboard on their PA achievements, instruments to set goals for upcoming weeks, PA planning in a calendar and illustrative pages explaining the need for PA in fall prevention and corresponding exercises to be done at home.
Video-application: User interaction and communication
Abilia 34 is a Swedish SME that develops equipment to support people with cognitive disorders. For the system used in this study, Abilia delivered a medical device in the form of an Android tablet characterized by an accessible interface and including specific apps, for example, to make video calls (e.g., to meet a HCP) to specific established contacts (i.e., video clients). Moreover, the device included a browser-app intended to run Livanda's motivation support web application.
Cloud service: Data processing and co-ordination
A cloud service component had been planned for coordinating all the pieces of the IS. More specifically, this component was intended to create and store the system users and to store their step data over time. It included a web page (MS Azure App Service, Microsoft), used by administrators to create user accounts and to initiate the connection of users to the step counter application, and a secure storage of user-id and step data (MS SQL Azure, Microsoft).
Integrated system
The system resulting from the integration of the components described so far was planned to work as follows: users’ accounts are created by means of the cloud service and thanks to it they are identified across the other applications (namely the mobile app for step count, the Livanda web application and the Abilia tablet and its apps). Users are identified by an alias linked to a globally unique identifier (GUID) which is generated on the web page by system administrators (the technical support person). User accounts utilizing the same alias-GUID are also generated on Livanda's and Abilia's cloud servers. In this way, data pertaining to a certain user could be accessed in a consistent way from all the different parts of the system. Moreover, no personal information other than the users step data and the alias-GUID was stored in the system. By going into more details, the tablet played the role of the access device to the system, as it included the video-call and the -client apps, as well as the browser to access Livanda's motivation support application. In turn, thanks to the cloud coordination, it could be possible to access PA data (retrieved from the step counter app), etc. to both show progress and set new goals.
System security
To ensure secure handling of user data in accordance with the General Data Protection Regulation (GDPR), a risk analysis was performed a prior to the system evaluation. It included a workshop to identify potential risks as well as structured work to analyze risks and to generate a plan for how to manage the most severe risks. The process was organized, led and documented by a specialist in cyber security and GDPR who received input from the project partners. The outcome was a risk management plan including approximately 14 relevant actions, related to needed technical implementations and practicalities (routines, information) in the execution of the study. The risk management plan was implemented prior to the study.
System evaluation
Study design
The study had an exploratory, iterative, mixed-method design (Figure 3). It consisted of three test periods (TPs), where groups of seniors tested the system during four weeks in their home. The first TP was a pilot TP informing on the feasibility, developmental areas and potential consequences of the system, as well as on qualitative data on user experience. The following TP1 and TP2 explored the system's feasibility, developmental areas, potential consequences as well as both quantitative and qualitative data on use, usability and user experience.

Overview of study design of system evaluation.
Research questions
The study explored the potential of the system prototype to support seniors PA with coaching from HCPs by addressing eight research questions covering five different areas (Textbox 1).
Research questions addressed in the study exploring five areas.

Participants and recruitment
Seniors: Eleven seniors were recruited from the workplaces of the participating coaches. Inclusion criteria: 65 years and older, independent living or living in block of service flats, able to move independently outdoors and indoors with or without walking aids, having wireless internet (Wi-Fi) at home, having home insurance including accident insurance. Exclusion criteria: Vision and hearing impairments that cannot be compensated by technical aids, unable to understand oral and written Swedish, no previous experience of computer, tablet or mobile phone.
Coaches: Two HCPs from a primary care unit and three health professionals from a municipal support unit for senior citizens were recruited. Inclusion criteria: Previous professional experience from supporting and promoting seniors’ health and PA.
Recruitment: Coaches were recruited via their employer: municipal and regional contact persons in the project identified suitable operational units in their home organization and received approval from the operations managers to involve unit staff. A researcher contacted suitable persons and informed them about the study. Seniors were recruited from the units where the recruited coaches worked. Here, coaches identified suitable seniors based on the eligibility criteria. Persons who showed interest in participating and gave consent to be contacted received a phone call from one of the researchers who gave additional information about the study and participation. The process aimed to recruit a group of seniors with equal gender distribution, varied previous experience with digital technologies, varied function and varied activity levels. Persons who had given consent to participate received written information about the study with an invitation to an information meeting with the researcher and the technical support persons. Meeting for coaches were held at work, and meeting for seniors were held in their homes. In the meetings, participants gave written consent to participate and the devices (tablet, and for seniors’ mobile phone with step counter app) were installed and tested.
Intervention
One week before the start of each TP, participants were introduced to the intervention and the system in an information meeting (see above). Here, the participants received oral and written instructions on intervention procedures and how to use the technical equipment. The technical support person helped participants to connect devices (Figure 1) to the local Wi-Fi (which was password protected) and instructed them on how to handle those. The users borrowed the devices from the university during the TP. The users tested the applications with support from the researcher and were instructed to call the technical support person in case of problems with the system.
The intervention was performed according to the following outline:
The video coaching meetings were held twice a week according to a predefined plan. The coaches had written instructions for the meetings including questions to follow-up performed PA in the past week in relation to set goals and difficulties experienced when initiating and performing PA. Coaches were instructed to individualize the coaching according to the seniors’ needs. The seniors prepared the sessions by reflecting with support from questions on PA performed, if set goals had been reached, and difficulties experienced.
Collection and analysis of data
To overcome the potential weaknesses of single methods, methodological triangulation was used.
Background characteristics questionnaires: At the information meeting, the senior was asked to complete a study-specific questionnaire on personal background characteristics (e.g., PA behaviour/level, previous experience of digital technologies and perceived health), and the coaches were asked to complete a similar questionnaire on professional characteristics and experience. All questionnaires were analyzed by descriptive statistics.
Seniors’ diaries: During the intervention, the seniors were asked to report daily in a structured dairy on whether the system had worked as expected (yes/no), and any problems experienced. Similarly, the coaches were asked to report after each coaching session if the system had worked as expected (yes/no), problems experienced, and how the coaching-meeting had worked out. For each senior, the number of days the user had reported that the system had worked as expected (i.e., yes/no to the question ‘Has the system worked satisfactory today?’) was summarized and the proportion (%) of satisfactory days compared to the number of total test days was calculated. The groups’ average and range of satisfactory days were calculated per TP. Descriptions of problems experienced by seniors and coaches were searched in the diaries. The plan was to compile problems for each user group and merge similar problems. In addition, the coaches’ notes on how the system and the meeting had worked out were compiled, with similar experiences merged.
Technical support persons’ logbook: The technical support persons documented, in a structured logbook, all calls from the participants to report problems and deficiencies of the system, as well as the measures taken to amend the problem. The logbook was handed into the researchers after each finalized TP. The total number of calls from the users was calculated, both per week and per TP. Notes on experienced difficulties or deficiencies experienced were compiled and similar experiences were merged.
Focus group interviews: After each TP, focus group interviews, one with seniors and one with coaches, were held in a meeting room at the university. The interview sessions were moderated by a researcher and lasted 45–60 min. The sessions started with the participants returning the technical devices and the participants completing a questionnaire on user experiences (described below). The focus group interviews followed semi-structured interview guides and explored the users’ experiences of the system and coaching including its usability, feasibility, perceived benefits and deficiencies, the views of their close persons and areas in need of further development. The interviews were documented through minutes written by the researcher, and/or a moderator (also a researcher) and audio recorded. The minutes were condensed and words or sentences describing the users’ experiences were identified and sorted into categories reflecting the research questions. Similar experiences were merged. The analysis followed the principles of a thematic analysis. 35 Audio recordings were listened to validate that the identified experiences of the categories reflected user experiences expressed in the interviews.
System logs: During TPs 1 and 2, data on the seniors’ use of the applications’ functions and on the senior's self-monitoring of steps and PA was collected from the respective sub-systems. Numbers and lengths of performed video calls were logged for all TPs. The responsible parties (university or companies) summarized the data from all participants per TP. Due to the technical instability of the system in the pilot TP, data on system use was not perceived to reflect appropriate use. Therefore, this data was not analyzed during the pilot TP.
Questionnaire on user experience: The questionnaire contained eight multiple-choice rating questions, with possible answers ‘Fully agree’ (Score 5), ‘Partly agree’ (Score 4), ‘Neutral’ (Score 3), ‘Partly disagree’ (Score 2) and ‘Fully disagree’ (Score 1). The questions related to use/feasibility, usability/learnability, user experience/ perceived values, perceived difficulties/problems and areas for further development. The participants had the possibility to add free-text answers after each question. Seniors and coaches had slightly different versions. For both seniors and coaches, responses ‘Do not know’ and scores given under the condition that the system was improved were omitted from the analysis. Proportions (%) of responses per possible answer were calculated per question for all seniors and all coaches participating in TPs 1 and 2.
System improvements
The system was gradually improved between TPs, each iteration targeted different aspects of the system. Particularly, the improvements proceeded in a bottom-up way with respect to the system architecture, that is, from single components of the solution towards the whole integrated system. After each test iteration, all the elicited problems were collected and discussed, both possible causes and corresponding needed system improvements. Problems were also classified based on their criticality with respect to the effective use of the system in order to adopt an appropriate prioritization of the required fixes. Eventually, each issue selected to be fixed for the next iteration came along with a corresponding set of tests to verify the successful resolution or possibly elicit further modifications. Improvements performed after the respective TPs are described in the results section.
Result
System evaluation
Participants
In the pilot TP, 1/4 seniors recruited dropped out since the technology had not functioned satisfactorily. Two men and one female (80–83 years old) fulfilled the pilot TP. One of them used walking aids. All were physically active on a lower level. Two had higher self-rated internet experience and one lower. In TP1 and TP2, all seven recruited users (four women/three men, 75–83 years old) fulfilled their TP. All of them were physically active, four on a higher level and three on a lower level. None of them used mobility aids and 6/7 had a higher self-rated internet experience. Five coaches (all women, 28–51 years old) were recruited, two worked in primary care (one nurse and one physiotherapist) and three worked in a municipal unit as senior guides supporting seniors’ health and independent living. More detailed background information of seniors and coaches is presented in Online Appendix 1.
Feasibility
Quantitative data from the seniors’ diaries and the technical support logbook demonstrated that the system's feasibility was insufficient in the pilot TP and increased importantly between the TPs (Table 1). Diaries showed that 80% (28/35) of the planned coaching sessions in TPs 1–2 were performed in the video app and 20% (7/35) over telephone or email without video. In several cases, the users were unable to initiate video calls or experienced poor video quality due to limited network capacity and, therefore, used phone instead. Some users experienced sound problems with the app on the tablet or with the external speakers that were provided to overcome problems with the tablets’ sound. Therefore, 18% (5/28) performed video sessions using simultaneous voice conversation over phone.
Quantitative data describing overall system feasibility per test period (TP) as reported in seniors’ diaries and the technical support persons’ logbook.

To identify factors limiting the system's feasibility and usability, complementary data collection methods were used. As no factors were identified from diaries, logbooks and focus group interviews were data sources (Table 2). In all TPs, seniors experienced difficulties with motivation support. Many users were confused after having been automatically logged out after 48 h and needed help to restart the web browser and login again. Another problem in the pilot TP and the beginning of TP 1 was that the automatic transmission of step data from the smart phone app to the motivation support webserver was inhibited. This limited the system's feasibility importantly and reduced the users’ motivation to use the system considerably. Several underlying reasons for the server communication problems were identified and handled. Moreover, several seniors and coaches were unable to initiate video calls in the pilot- and TP 1. The underlying reason was insufficient local Wi-Fi connections in senior's home or at the coach's workplace. Complementary strategies were used to handle this. When this problem still occurred, coach meetings were held over phone instead.
Problems experienced by seniors (s) and coaches (c) per TP categorized by the sub-system they related to. Data was collected by technical support persons’ logbook (L) and focus group interview (F) with seniors and health care professionals.

Use (of motivation support in TP1 and TP2)
System logs from TP 1 and TP 2 showed that all seniors had visited the pages of all main functions in the motivation support (Table 3). The logs from the motivation support application also showed that the numbers of logins, visits on the home page and on the main functions’ pages varied widely between users (Table 3).
Numbers of events per senior in test periods (TPs) 1 and 2 (n = 7).

System logs from the motivation support application also showed that the mean number of visits on specific pages per user was slightly higher for men than for women (Table 4). Pages for planning and evaluating PA had the highest (mean) number of visits for both men and women.
Numbers of visits on pages in motivation support per seniors in TP 1 and 2.

Most of the seniors used the goal-setting features in the motivation support during TP 1 and 2: 6/7 seniors set goals for daily steps and 3/7 modified their step goal once or twice. In addition, all seniors set at least one goal for another weekly PA. In most cases, the PA goals were modified at least once or twice. The goals were categorized as strength-, balance-, endurance- or everyday activities. Balance activities were the most common category in goal setting, used by 6/7 seniors.
Usability and user experience (in TP1 and TP2)
The questionnaire ratings from TPs 1 and 2 indicated that, in general, the seniors perceived the digital applications to be usable and create a positive experience (Figure 4). The coaches’ ratings indicated that their experience of the digital applications was less positive than seniors’ (Figure 5). However, they all agreed, strongly or partly, that distance coaching was fun.
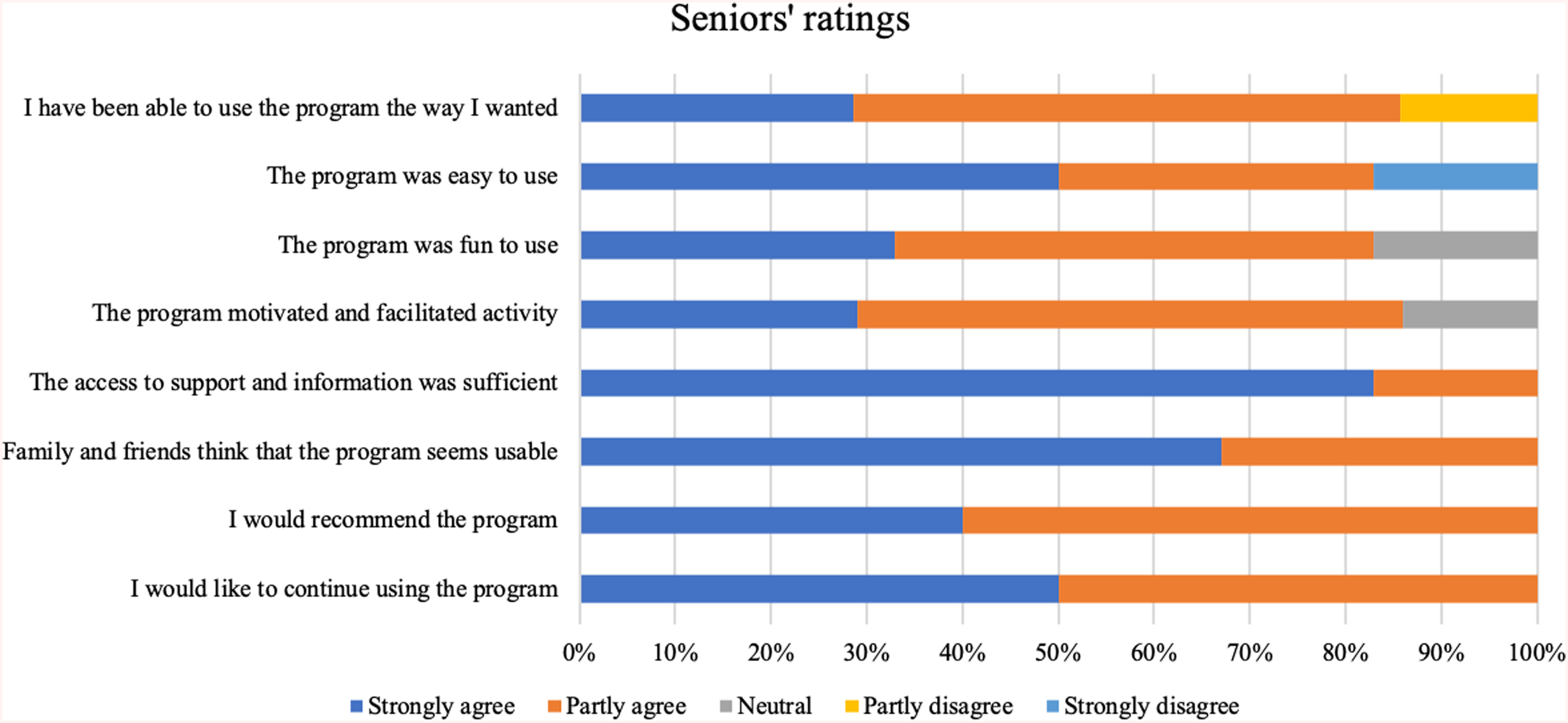
Proportion of responses per score and question given by seniors participating in tps 1 and 2 (N = 7). Number of responses included in analysis per question presented to the right followed by numbers in parenthesis representing numbers of responses ‘Do not know’ and ‘If the program worked more stably and was easier to use’, respectively.

Proportion of responses per score and question given by coaches participating in tps 1 and 2 (N = 7). Number of responses included in analysis per question presented to the right followed by numbers in parenthesis representing numbers of responses ‘Do not know’ and ‘If the program worked more stably and was easier to use’, respectively.
Benefits and potential consequences
Both seniors and coaches described in the focus groups that they had experienced benefits from the system. For example, both groups described that the system was a fun and flexible way to support and stimulate PA. They also saw that the system could raise seniors’ awareness of their activity levels in everyday life and thought that goal achievement as well as feedback on results could be encouraging for seniors. Moreover, the seniors experienced the system to be interesting and to stimulate PA. They liked the idea of having their own personal coach who supported them to be more active. They expressed interest in continuing using the program after the TP. Furthermore, the coaches stated that they liked the way that the system enabled them to support seniors PA at a distance. They believed that distance coaching supported the seniors to take own responsibility for PA and described that video coaching was helping to build relationships with the senior. They saw that the system was useful and complementary to traditional care (See Table A2, Appendix 2 in Online, for more details).
The users also identified factors limiting the system benefits. After the pilot TP and TP 1, both seniors and coaches described that the technical problems had created a barrier for them to use the system. Especially in the pilot TP, the instable and difficult technology caused stress and disappointment. The coaches experienced at that time that the coaching sessions had focused more on technical problems than on PA. In TP1 and TP2, some of the coaches expressed that they lacked expertise in supporting PA behaviour change and maintenance. Although the system's usability and stability were gradually improved between TPs, seniors and coaches from all TPs expressed that the motivation support program was difficult to manage and took time to learn. They also saw that the scheduled tablet-based video coaching limited the seniors’ personal freedom. In addition, the seniors perceived that the mobile phone for step counting was too large to carry around in daily life. The users’ descriptions of how their close persons experienced the systems were brief: one senior expressed that his/her spouse had helped him/her with technical problems. Some coaches stated both lack of time to show the system to colleagues and that colleagues had shown interest in the system (See Table A2, Appendix 2 in Online, for more details).
Seniors and coaches described possible consequences of the system in the focus groups. For example, both groups foresaw that video-coaching may stimulate PA long term. The seniors also saw that the videos with exercise programs could improve/facilitate PA since the exercises could be performed at home at any time. The videos were also expressed to be encouraging. Moreover, the coaches anticipated the system to be cost-effective, flexible and a fun way to support long-term PA. They envisioned the system to provide them with an opportunity to offer their patients and clients alternative supporting methods. However, both seniors and coaches expressed concerns about that system would increase inequality since only computer-literate persons would be able to use the system. They saw that it was important to reach out to lonely, inactive persons in greater need of support than active people. Also, they saw that, with the current prototype's tablet and Wi-Fi requirements, video coaching might make the seniors more bound at home. It was also stated among seniors that persons were afraid of technology and preferred using pen and paper instead. The coaches expressed that technical instability might cause waste of time and limit the system's flexibility. Moreover, they pointed out that the system needs to be secure and safely store personal information and envisioned that coaching a group of seniors simultaneously may be difficult (See Table A3, Appendix 3 in Online, för more details).
Developmental areas
The focus groups explored which areas the users perceived as the most important developmental areas; different areas were identified in different TPs (Table A4, Appendix 4 in Online).
Initially, coaches and seniors perceived that the reliability and usability of the system were insufficient and that the hardware devices needed to be neater and simpler.
Over the TPs, both system reliability and instructions to users on how to handle potential problems were improved. This increased the feasibility of the system and enabled the users to identify other types of problems. For example, both seniors and coaches stated the need to improve the system to enable individualized and flexible coaching, to enable the use of own technical equipment, for example, their own mobile phone, and coaching-media of choice and at times when needed. Moreover, the coaches got more time to reflect on their role as a coach and how coaching should be structured to give optimal support to the senior. The seniors identified that concepts in the motivation support needed to be clearly defined. For example, it was not obvious to everyone what activities to be counted as PA or what endurance training meant. The seniors appreciated the video exercise program and wanted them to be further developed. Moreover, already in the pilot, seniors also expressed that they would prefer automatic monitoring of general PA that was not limited to only step count.
System improvements made between TPs and resulting prototype version
The system prototype was improved between the TPs in a bottom-up approach, starting from single apps (the step counter, the motivation support, the video client- and call supports), and then extending the tests and improvements to the integration (data retrieval and exchange between apps, and so forth). In the remainder of this section, we describe relevant issues and corresponding fixes adopted for the next phase in the three test iterations and present the resulting version of the system prototype.
In the pilot TP, both seniors and coaches reported severe problems with the system's stability. For example, the automatic transfer of steps from the smart phone to the motivation support app did not work stably. After analysis of underlying reasons from system logs and internal tests, the step counter app was improved. As a backup solution for upcoming TPs, seniors got the opportunity to manually report steps (monitored by their own activity tracking device or a manual step counter provided by the project). Moreover, the video calls, which generated a lot of interest as a nice coaching possibility, were in several cases limited by network resources. This was addressed by improving the network for one coach, finding optimal locations for video calls in the seniors’ homes and developing a new version of the video app containing an indicator of current network quality detected by the tablet. For the following test sessions (TP1–2), the users were recommended to check the internet access in the video app before initiating a call and in cases of limited resources move to a spot in their home with better capacity. To improve the sound quality of the video calls, the seniors were provided with external speakers. Also, some features in the motivation support app were simplified and clarified, for example, to facilitate login, navigation and planning activities. Finally, the calendar function on the tablet was turned off to cancel reminders.
In TP 1, the users showed appreciation for the system improvements. Especially the added exercise videos were perceived to be useful, and the PA reporting was experienced as more flexible although the need to manually write in numbers of taken steps was perceived as tedious. Although some of the video calls were successful, users still experienced problems with the video app. In preparation for the next testing phase, the following improvements were planned: further refinement and simplification of certain texts as well as the addition of new exercise videos in the motivation support; further improvements in the step counter app to ensure that the automatic upload of step data in the cloud and automatic retrieval of step data into the motivation web application would work more stably; modification of settings used in the connection quality indicator of bandwidth to warn the users about potential issues during video calls, and prolonging the maximum time for video calls from 20 to 60 min.
Eventually, in TP 2, the system was validated as a whole (Figure 2). Here, both seniors and coaches could focus mainly on the system's approach to PA and support for motivation. To summarize, the final version of the system prototype, used as a concept for boosting seniors’ motivation for PA, was composed of:
A cloud service used as entry and coordination point. This service was developed by MDU and managed users, login and step data. An Android app to be installed on any compatible phone to automatically detect number of steps taken. This app was developed in collaboration between MDU and the company RealTest. A web application, developed by the company Livanda, including information on PA, excersies videos and features for goal setting, planning, monitoring and evaluation of PA. For example, through (possibly automatically retrieved) step data. A video call app integrated with a client management tool developed by the company Abilia, used as coaching/communication tool between seniors and coaches.
Discussion
The aim of this study was to integrate as well as to evaluate the feasibility and user experience of a system prototype to support seniors’ fall-preventive PA. The system was designed in a user-centered requirements engineering study 26 and, therefore, included a broader repertoire of functionalities compared to other digital supports for seniors fall prevention exercises (such as Apps and websites in McGarrigle et al., 18 Silveira et al., 20 Sandlund et al., 21 Arkkukangas et al., 22 van Het Reve et al., 23 Mansson et al., 24 Pettersson et al., 36 and Mixed Reality Technologies in Nishchyk et al. 37 ). Particularly, the studied system prototype included not only self-monitoring and behavioural support but also digital support for video coaching and step counting as well as an Internet-of-Things (IoT)-based architecture utilizing a cloud-based service for co-ordination and data management. 38 The evaluation used an iterative approach with three sequential TPs intervened by structured work to improve the prototype based on results from the previous TP. Ten seniors fulfilled the intervention (three in the pilot TP and seven in TP 1 and TP2). They had an equal gender distribution, were 75–83 years old, as well as rather active and used to digital technologies. In the study, the seniors received regular video coaching from an HCP. Five HCP participated, all females and employed in municipal and regional organizations with university degrees in health sciences and behavioural medicine education or equivalent.
Main study results in relation to other empirical studies and theory
This section discusses the study's main results in terms of the areas and research questions stated in Text Box 1.
Feasibility
The evaluation results indicate that the system prototype version used in the pilot TP had insufficient feasibility: the seniors became stressed by the technical problems and reported that the system had functioned satisfactory approximately half of the test days. Their negative experiences of the system created a barrier towards using it, a reaction in accordance with the Unified Theory of Acceptance and Use of Technology 39 and a secondary study of seniors’ adoption of health information technologies. 40 As usability- and user experience rating scores from the pilot TP only reflected the use of a prototype version with poor technical stability, these scores were omitted from the evaluation analysis of usability and user experience. However, by presenting the pilot TP's feasibility results together with encountered problems and strategies to address them, we hope to contribute to future related research. Other authors have highlighted the need to increase the publication of lessons learnt from early feasibility studies to guide further research. 30 The results also show that the development efforts performed between TPs were effective in improving the system's technical feasibility: especially the prototype version used in TP 2 but also that used in TP 1, worked more stably.
Use
In TP 1 and TP 2, all seniors used the motivation support applications’ main functionalities and had scheduled video-coaching sessions with the HCPs. On several occasions, the users were unable to initiate video calls or experienced poor video quality, problems also identified in a study by Shaw et al. 41 and in line with a secondary study concluding the major problem with video conference in care still is the technology itself. 42 However, the seniors and HCPs overcame this problem by talking over phone instead, a strategy also seen in a study by Shaw et al. 41 The project team also made efforts to support the users in how to achieve the best possible network quality. One improvement with a high impact on the system's technical feasibility and the users’ motivation to use the system was the reliability of the step counting and the automatic transfer of the step data to the motivation support.
Usability and user experience
The user ratings from TP 1 and TP2 indicated that seniors and coaches generally saw the system as valuable but that the insufficient stability and usability limited their experience and that the access to help and information had been sufficient. As the system prototype was a proof-of-concept displaying main functionalities, several parts of it had not been optimized with regards to usability and user experience. This was reflected in the evaluation results which showed that the seniors found the hardware non-optimal and the motivation support too extensive and rather difficult to grasp. These usability problems are related to several of the eight main categories of usability problems (basic system performance, task-technology fit, accessibility, interface design, navigation and structure, information and terminology, guidance and support and satisfaction) identified by Broekhuis et al. to be relevant for e-health applications, with patients as primary users. 43
Benefits and potential consequences
Experienced and foreseen benefits of the system included enjoyment, flexibility, awareness raising, interest and stimulation. Particularly, the video-coaching was appreciated, an interesting result since this study was performed before the Covid-19 pandemic which significantly increased the clinical use of video consultation. 44 The seniors found the video coaching interesting and stimulating while the HCPs considered it a nice complement to ordinary care since it made the senior take responsibility for PA and helped to build relationship. Supporting relatedness and autonomy is important for long-term motivation according to the Self-Determination Theory, 45 which has been suggested as a theoretical basis of health coaching. 46 The change of roles and responsibilities when using video visits has been identified in outpatient care of patients with obesity. 47 Previous research has also identified the potential for additional coaching via video or phone to improve adherence and effectiveness of digital behaviour interventions for behaviour modification in adults.27,48 The users in this study foresaw that video coaching could make seniors increasingly bound at home and suggested that the coaching should be more flexible and individualizable in how and when it was performed. This is relevant since the combination of activity tracker use and regular support from health professional via texting also can assist older adults to maintain their activity levels. 49
The seniors also suggested that the system support activity monitoring based on other types of PA data than step count, different options for this exist. 50 It is likely that the more personalized support services suggested by the seniors in this study also should be adaptable over time, something identified as a need in a study on design and development of e-health for collaborative self-management among older adults with chronic diseases. 51
The users in this study described that their experiences of system benefits had been limited by the technically instable prototype versions as well as by the fact that it took some time to learn how to use the system. Poor and complex functionality as well as overwhelming and difficult-to-understand content are included among the previously identified barriers to the use of e-health by older adults. 52 In fact, the users in this study foreseen that the system could increase inequity due to discrimination of persons with low digital literacy and lacking local Wi-Fi at home. The risk of digital technology to increase health inequities associated with digital literacy and infrastructure has been identified as pitfalls in the digital transformation of health and medical care. 53 Moreover, cost of internet service has been identified as a barrier for seniors’ use of e-health. 52
Developmental areas
Improving the system's technical stability and the applications’ usability was identified as crucial for wider implementation of the system. Improved usability of digital applications is crucial since seniors adopt health information technologies perceived to be useful and requiring low effort commitment. 40 Hardware interoperability was another important developmental area since some of the seniors wanted to use the applications on their own devices and suggested that the system should integrate also activity data other than steps taken. Increasing the flexibility and possibility to adapt the system to the users’ personal needs and preferences was also identified as important in further development of the system. Personalized content is a facilitator of older adults’ use of e-health. 52
Another area for development is to further study the implementation of the system into clinical practice and identify for which patients digital PA support may be most cost-effective and provide the most health benefits. Notably, one area of interest is seniors with sarcopenia and fraility since increased PA may prevent or delay the onset of adverse outcomes such as disability, falls and lower quality of life.2,4 Recent research have presented promising results on screening tools to detect frailty in primary care setting.54,55 This allows health care to be proactive by starting adequate treatments earlier and hence prevent or delay the onset of adverse outcomes. Digital behaviour changes interventions to support PA adapted to seniors specific needs may be an important tool to deliver timely and flexible treatment for the increasing population of older adults worldwide.
Benefits and costs related to integrating existing applications
Creating a system by integrating several existing applications provided by different organizations comes both with benefits and costs. A substantial benefit of this strategy was the mobilisation of resources and complementary expertise from all the partners. By involving companies who had previously developed own products for other user groups, the project was able to rapidly produce a system prototype including digital applications on a high technology readiness level. 56 This proof-of-concept prototype enabled feasibility and user experience-evaluation helpful for identifying core functionalities of a future product. Other approaches for the rapid development of usable e-health systems exist, as noted by Daraghmi et al. 57
The strategy used in this project enabled user testing of new functionalities, that is, video coaching and step counting, that is not present in other digital supports for seniors’ PA (e.g., Silveira et al., 20 Sandlund et al., 21 Arkkukangas et al., 22 van Het Reve et al., 23 Mansson et al. 24 and Pettersson et al. 36 ). However, integrating different applications from several providers and for different purposes creates a technically complex system, also referred to as IoT, which may be difficult to set-up and to use in health care settings. 58 For instance, the applications in this system had been included based on functional user requirements and the partners’ interests to participate in the collaboration. Considering also interoperability in the selection of applications is likely to lead to smoother integration and more stable systems. The consortium collaborated successfully to develop a common login system for all applications (the GUIDs) and to ensure secure data handling. However, the created solutions required extensive manual resources in the set up and regeneration of devices between TPs. Moreover, the trouble-shooting work to solve technical problems had to be distributed between several organizations and required substantial co-ordination efforts. Consequently, carefully considering interoperability in the selection of applications and planning in advance for their interconnection is likely to prevent many integration challenges and to lead to more stable systems. In fact, setting up a digital infrastructure and ensuring the components of the system communicate are the first two key steps in recommendations on how to develop a successful smart home innovation for people with mental and physical health conditions. 31
Strengths, weaknesses and limitations
Several strengths can be identified related to the testing methodology. Firstly, the study design with the three iterations showed to be important for repeated and gradual improvements of the system as well as to gain a deeper understanding of the value of the system components. Secondly, the reasonable size and equal gender distribution in the group of senior participants. Thirdly, the use of multiple methods to collect data on the users’ experiences and system use. Fourthly, the broad range of competences represented in the multidisciplinary project team which enabled integrating complementary perspectives in the integration and evaluation of the system.
Weaknesses of the study include the insufficient stability of the system prototype, especially in the pilot TC. Most importantly since it caused stress among the seniors who encountered a lot of problems with the system and the well-being of research persons is of the highest priority. However, the support and information to users was extensive and rated sufficient by the participants. Future related studies are recommended to, before testing feasibility during weeks, include shorter pre-tests in real-world environments to detect problems that are difficult to detect in laboratory tests.
Limitations of the study include the bias in the group of senior participants who were mainly physically active and experienced in digital technologies. Future research on systems that are feasible in real-world settings should also include inactive seniors and explore their experienced and preferences for digital PA support. Moreover, the study was limited to female HCPs from two health organizations, one municipal and one regional.
Conclusions and lessons learnt
The main conclusion of this study is that video coaching seems to have a great potential in PA coaching among seniors, particularly in building relation between senior and coach, as well as in making the senior taking responsibility for his/her PA. The study experienced that the local WiFi access is crucial for stable, high-quality video meetings. Therefore, we recommend the use of video applications that are as flexible as possible to bandwidth. Moreover, we conclude that although setting and following up PA goals is motivating for seniors, activity monitoring should be based on other types of data than steps counted.
This study learnt that integrating applications from different providers in a common system prototype can be efficient for rapid production of a proof-of-concept. However, the system complexity might become high, and this may cause technical challenges. We, therefore, recommend considering also interoperability in the development of a system specification.
Another lesson learnt from the study is that iterative study design can be of value also in feasibility- and user experience studies. In this study, the TPs were very useful for improving the system based on real-world experiences. However, we recommend more extensive functional testing in real-world setting before involving real users in the testing. We see it as highly important that users are only involved when the technical concept is reasonably stable. Early tests with a technically stable system can yield valuable insights into the potential of the respective components for the users.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076231180973 - Supplemental material for Towards multimodal boosting of motivation for fall-preventive physical activity in seniors: An iterative development evaluation study
Supplemental material, sj-docx-1-dhj-10.1177_20552076231180973 for Towards multimodal boosting of motivation for fall-preventive physical activity in seniors: An iterative development evaluation study by Å. Revenäs, L. Ström, A. Cicchetti and M. Ehn in DIGITAL HEALTH
Supplemental Material
sj-docx-2-dhj-10.1177_20552076231180973 - Supplemental material for Towards multimodal boosting of motivation for fall-preventive physical activity in seniors: An iterative development evaluation study
Supplemental material, sj-docx-2-dhj-10.1177_20552076231180973 for Towards multimodal boosting of motivation for fall-preventive physical activity in seniors: An iterative development evaluation study by Å. Revenäs, L. Ström, A. Cicchetti and M. Ehn in DIGITAL HEALTH
Supplemental Material
sj-docx-3-dhj-10.1177_20552076231180973 - Supplemental material for Towards multimodal boosting of motivation for fall-preventive physical activity in seniors: An iterative development evaluation study
Supplemental material, sj-docx-3-dhj-10.1177_20552076231180973 for Towards multimodal boosting of motivation for fall-preventive physical activity in seniors: An iterative development evaluation study by Å. Revenäs, L. Ström, A. Cicchetti and M. Ehn in DIGITAL HEALTH
Supplemental Material
sj-docx-4-dhj-10.1177_20552076231180973 - Supplemental material for Towards multimodal boosting of motivation for fall-preventive physical activity in seniors: An iterative development evaluation study
Supplemental material, sj-docx-4-dhj-10.1177_20552076231180973 for Towards multimodal boosting of motivation for fall-preventive physical activity in seniors: An iterative development evaluation study by Å. Revenäs, L. Ström, A. Cicchetti and M. Ehn in DIGITAL HEALTH
Supplemental Material
sj-docx-5-dhj-10.1177_20552076231180973 - Supplemental material for Towards multimodal boosting of motivation for fall-preventive physical activity in seniors: An iterative development evaluation study
Supplemental material, sj-docx-5-dhj-10.1177_20552076231180973 for Towards multimodal boosting of motivation for fall-preventive physical activity in seniors: An iterative development evaluation study by Å. Revenäs, L. Ström, A. Cicchetti and M. Ehn in DIGITAL HEALTH
Footnotes
Acknowledgements
The authors would like to thank all seniors and coaches who participated in the study. The authors also want to thank all persons involved in the system development at Abilia, Livanda-Internetkliniken, Real-Test and Mälardalen University for their contributions. Moreover, the authors are grateful to Pär Hellström, Niklas Persson and Jonas Larsson who were responsible for preparation and installation of the systems in the seniors’ homes and for giving technical support to the seniors.
Contributorship
ÅR and ME researched literature and conceived the study, were involved in protocol development, gaining ethical approval, patient recruitment and data analysis. AC was responsible for coordinating the technical development of the system. LS was responsible for the technical development and of the motivation support application and for summarizing its data acquired in the study. ME wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
The ethics review authority in Uppsala, Sweden, approved the study (Dnr: 2019-00818).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Swedish innovation agency under Grant Dnr: 2017-0317 and the project partners (Abilia, Livanda Internetkliniken AB, Mälardalen University, Real-Test, Region Västmanland, Vital Integration of Scandinavia, Västerås Municipality).
Guarantor
ÅR
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.