
Abstract
Objective
This study aims to advance the On Scene Injury Severity Prediction (OSISP), an Artificial Intelligence (AI)-based model, as a Clinical Decision Support System (CDSS) that supports Emergency Medical Service (EMS) personnel during on-scene assessment of adult trauma patients. The objectives are to explore the integration of OSISP with the prehospital trauma workflow and to refine the User Interface (UI) that communicates the predictions.
Methods
Workflow integration was studied in a workshop by analysis of a customer journey map created by personnel with experience of working in the EMS setting (n = 8). Literature reviews were conducted to identify key factors enabling efficient human–AI collaboration and implementation options. Identified UI components derived from workshop and literature review findings were then evaluated and selected to refine the OSISP UI.
Results
The workshop derived that OSISP is a service to be used on portable IT platforms as a second opinion, support for prioritization, and support during patient assessment. The literature reviews identified key content, characteristics, and goals of communicating predictions to users. The refined UI consisted of eight information components (prediction, entered predictors, missing predictors, and model details), and four functions (notification, exploration mode, and filtering of top three entered and missing predictors), to communicate the OSISP prediction.
Conclusions
The refined OSISP UI has potential to integrate well into the clinical workflow during patient assessment, as well as enhance human–AI collaboration through customizable information when communicating predictions. However, usability testing of the OSISP UI is needed to ensure clinical utility.
Keywords
Introduction
In medical emergencies, such as trauma, minimizing time for providing optimal individual patient care is essential to increase the chance of survival and reduce the risk of disabilities. 1 Trauma is the most common reason of death for young adults worldwide. 2 For severely injured trauma patients, the nearest acute care hospital may not always be the adequate destination, and instead a more distant trauma center may be the preference for providing optimal care. 3 It is therefore crucial for Emergency Medical Service (EMS) personnel to quickly decide on both initial care 1 and appropriate transport destination.1,3
To make these critical decisions the EMS team must assess safety, scene situation, injury mechanisms, injury severity, care need, traffic situation and transportation time, as well as providing immediate care. 1 All in all, the decision-making process is a difficult and time-pressuring task. The challenge is reflected in the literature, where a high proportion of patients are transported to care facilities with resources that do not match the actual care need.4–6 This may lead to a delay to optimal care, in particular for severely injured patients, increasing the risk of morbidity and mortality. 3 Furthermore, excessive use of care resources for noncritical patients may impact care for critical patients. 3
Artificial Intelligence (AI) has potential to help improve trauma care. In research studying epidemiological changes due to the COVID-19 pandemic, like reduced trauma volumes and specific injuries, 7 AI has been used to explore impact of variables like age and place of residence on trauma types. 8 Multiple studies demonstrate the ability to support management of traumatic hemorrhage by predicting mortality, need of transfusion, and injury severity. 9 Furthermore, AI can predict the need for lifesaving interventions, 10 and the risk of severely injured patients who can benefit from care at trauma centers. 11 Integrating AI in Clinical Decision Support Systems (CDSS) therefore has potential to improve support given to EMS teams during assessment of trauma.
The prehospital challenges of assessing care needs and optimal transport destinations have previously been addressed by our research group, where digital technology is used to support the EMS personnel during the decision-making process. One example is the concept On Scene Injury Severity Prediction (OSISP). OSISP describes a CDSS to be used as a supporting tool by EMS personnel during the on-scene assessment of trauma patients. Based on mathematical models such as AI methods, OSISP uses patient information to predict the risk that the patient is severely injured. Initially, the concept was tested on retrospective motor vehicle crash data, indicating improved triage performance.12–14 Next, the OSISP scope was expanded to include all trauma incidents, using the Swedish Trauma Registry (SweTrau) 15 as base, which shows promise for enhanced field triage. 16
To advance OSISP toward clinical implementation, efforts are needed to develop a high-fidelity prototype and study usability in clinical practice. The Verified Innovation Process for Healthcare Solutions (VIPHS), 17 a stepwise framework for the design, testing, utilization, and implementation of digital health tools and innovations, may be used as a guide. Building on previous work, documentation of the care process and design of the User Interface (UI) system remain to complete VIPHS step 1. These activities were initiated by Wallstén et al., 18 where a tablet-based UI prototype that incorporated eXplainable AI (XAI) features was proposed, including a prediction information page for communicating model predictions. When tested by six user participants, the prototype received high usability scores. For future research, the authors suggested focusing on enhancing specific aspects of communicating the OSISP predictions, for example, by providing explanations of feature importance to the user and when to notify the user.
The next step is to refine the care process and UI prototype by considering previous limitations, suggested future research, state of the art, and user feedback. 18 The refinement of documenting the care process may be based on service design, a human-centered, collaborative, iterative, and sequential design approach to create holistic services that meets the need of reality. 19 Customer journey mapping is a popular service design method used in healthcare, 20 and visualizes how a customer experiences a service. 19 By adopting customer journey mapping for the analysis of the care process, a deeper understanding of how to integrate the CDSS into the EMS personnel's workflow can be obtained.
Furthermore, XAI is important to consider for successful implementation of AI in healthcare. 21 The refinement of the UI prototype will therefore focus on the prediction information page and be based on user feedback presented in reference 18 and state of the art in human–AI communication. Examples of such communication items that have received attention are systematic model descriptions intended for clinical users, 22 and incorporation of warning alerts when the model input does not match the model's intended use. 23 There are several suggestions on how to communicate AI-based predictions to users, but it is also recognized that the design of an explainable interface needs to be customized for the task at hand. 24 Instead of being used as general solutions, suggestions in the literature should therefore be evaluated on a case-by-case basis.
OSISP has not yet been designed as a CDSS to enable effective use in prehospital settings. This study bridges that gap by co-designing an interpretable, user-centred interface that supports EMS personnel in real-time decision making. The purpose of this paper is to further develop OSISP as a CDSS with emphasis on human–AI collaboration. The objectives are: (1) to identify critical information and decision points and explore the use of OSISP in the prehospital trauma workflow using customer journey mapping, and (2) to refine the prediction information page by suggesting an updated set of XAI features based on user feedback and current best practices. By completing VIPHS step 1, the ambition is to advance the OSISP concept and provide inspiration on how to address human–AI collaboration in emergency care.
Methods
Study design
This study was conducted in Sweden through a collaboration between Chalmers University of Technology, the University of Borås, the University of Gothenburg, Dedalus Sweden AB and an ambulance organization in the region of Västra Götaland. Information about the projects is given in the funding statement. The members had either research experience in digital health, technical experience in developing CDSS for the prehospital sector and in AI-based models, or clinical experience of working with trauma patients in Swedish prehospital settings or at trauma hospitals.
The study design was guided by the VIPHS framework. 17 Because the development of OSISP is in an early design phase, the first step of VIPHS was targeted, which results in a blueprint describing the care process, technology proposal, system design proposal and theoretical testing and evaluations. Workflow integration and UI design proposal was the target for the presented study, complementing earlier studies.16,18 The method was divided into three parts (Figure 1). Part 1 explored the workflow integration. Part 2 reviewed XAI approaches in general and in healthcare. Part 3 refined the OSISP UI with an updated set of XAI features in the prediction information page, with suggestions on how to realize their functionality. This study focused on designing the OSISP as a CDSS, whereas empirical evaluation of the design proposal will be conducted in future work.

Overview of the method. The workflow integration was studied by creating and analyzing a customer journey map. State of the art for communicating predictions was studied by reviewing current XAI approaches and UI components. The findings were used to identify options of UI components to refine the OSISP prototype. OSISP: On Scene Injury Severity Prediction; UI: User Interface; XAI: eXplainable AI.
Previous work and scope of study
The work in this study was based on previous results. Firstly, the technology proposal presented by Bakidou et al. 16 was used to define the scope of the prototype. Secondly, the set of UI components, limitations, and suggestions for future research presented by Wallstén et al. 18 were used as a foundation for refining the journey map and OSISP prototype. This study focused on identifying key information and features for effective human–AI collaboration. It did not address fundamental UI design elements, such as UI component shapes or placement.
Part 1: Workflow integration
Customer journey mapping was used to analyze how to integrate OSISP with the users’ workflow. The map was co-created with intended end users in a full day (7 hours) workshop following the method outlined by Stickdorn et al., 25 with modifications (Table 1). The moderator (author AB) facilitated the workshop by providing instructions throughout the workshop. Critical information and decision points, and factors impacting decision making were concluded by participants during discussion of the customer journey map. The findings were used to identify appropriate workflow integration by an inductive thematic analysis of the transcribed discussions, conducted by a single researcher (author AB). To enrich the reporting of the workshop, quotations were translated to English and added.
Details of the method used to study workflow integration, based on a modified method by Stickdorn et al. 25 .

EMS: Emergency Medical Service; OSISP: On Scene Injury Severity Prediction.
Part 2: XAI approaches
To obtain an understanding of key factors that enable efficient human–AI collaboration, a literature review was conducted to find an overview of state of the art and recommendations on XAI in general and in healthcare in particular. The purpose of the review was to inform the design refinement of the OSISP UI. The methodology followed selected parts of full systematic/scoping reviews, as deemed appropriate for its purpose. The review was conducted by a single researcher (author AB) and the electronic databases used were PubMed, Scopus, ACM, and Web of Science. Snowballing was not conducted. The screening process was facilitated using the web application Rayyan (Rayyan Systems Inc). 27
The review process was conducted as follows. First, relevant studies were identified by searching the selected databases. The search string “(artificial intelligence OR machine learning) AND (interfac* OR interact* OR explain* OR interpret* OR design* OR transpar*)” was applied on titles in the electronic databases. The search string used an asterisk (*) to capture variants of the words interface, interaction, explanation, interpretation, design, and transparency. Inclusion criteria were systematic and scoping review articles in English language. Because XAI is a rapidly evolving field, the search was limited to publications in 2024 to capture the most current XAI approaches. Second, the built-in function for detecting duplications in Rayyan was used to remove duplications. Third, abstracts were screened in Rayyan. Studies were included if the content described XAI approaches in general or applied in the healthcare sector. Papers related to drug development were excluded. Fourth, studies with full text access were included. Fifth, eligibility criteria were applied. Sixth, included studies were divided in two categories: general XAI approaches and XAI in healthcare. Lastly, for included studies, the following information items were charted in Microsoft Excel: XAI terminology, XAI taxonomy, and XAI techniques mentioned in more than one study. Additional aspects considered relevant for describing the state of the art were also documented, on which an inductive thematic analysis was conducted. The review did not consider data protection or integrity aspects. Based on the review findings, key contents and characteristics of prediction communication were identified.
Part 3: Prototype refinement
A refined UI of the prediction information page that enhances human–AI collaboration was proposed based on the findings from parts 1 and 2 (Figure 1) and previous work on OSISP's UI. 18 A complementary literature search was conducted to identify complementary implementation aspects for the OSISP UI. The search was conducted by a single researcher (author AB). The electronic databases were PubMed, Scopus, ACM, and Web of Science. E-journals that Chalmers University of Technology had access to through their digital database were also considered. Next, implementation options were evaluated, and a refined set of UI components were selected. Lastly, the updated set of UI components and identified key characteristics were used to refine the prediction information page in Microsoft PowerPoint.
Ethical considerations
The study was conducted in accordance with the Declaration of Helsinki. Under the Swedish Ethical Review Act (SFS 2003:460), ethical approval was not required as no sensitive personal data or data about legal violations were processed. The data were managed in accordance with Chalmers University of Technology's policies and underwent a review by Chalmers Data Office. Written informed consent was obtained from all participants prior to participation in the workshop.
The workshop participants were employed by a project member organization and the time spent in workshops was part of their ordinary work time, and no additional incentive was used. Any sensitive personal data inadvertently collected from the workshop were excluded from the research material.
Results
Part 1: Workflow integration
This section presents findings from the workshop, where a customer journey map was created and analyzed.
Description of the workshop participants
The workshop was conducted by the moderator (author AB) and eight participants (involving authors MAH, ECC, and BAS). Participants had experience of working as EMS personnel (n = 3), EMS medical doctor (n = 2), trauma surgeon (n = 1), and industry representatives (n = 2). The majority of the participants were men (n = 6), the average age was 51 years, the clinical prehospital experience ranged from 8 to 17 years, and the experience of prehospital technology development ranged from 15 to 32 years. The participants had experience of working in various locations and the most common place was the Swedish region of Västra Götaland.
Customer journey map: Patient scenario 1
The participants assessed the journey maps of the workshop's two groups to be similar, with complementary aspects. The maps were therefore merged without modifications. The final customer journey map, accompanied by descriptions of each phase, is presented in a supplemental file (Table S2, Appendix B). Below follows extracted results connected to integrating OSISP into the workflow.
“… or maybe you need AI the most, those are the cases when you don't know if the patient is actually healthy or sick… will they get sick… so those who are very traumatized, it's quite easy, or you know what to do, but those who are on the borderline…” “… and here is just… for example, is this a medical case or a traumatic case… you don't usually know that…”
Summary of critical points and availability of OSISP predictors throughout each phase of the prehospital trauma workflow.

Critical information points = lacking or attention competing information. Critical decision points = when the user must make an important decision. OSISP predictors are listed where they are likely to be collectable at first, and the number of available predictors in each phase.
*Predictors where first occurrence is uncertain.
OSISP: On Scene Injury Severity Prediction.
“I think, it's valuable when it thinks something different than what you yourself thought… then I think, okay, I've missed something here… because now I got a reservation here, I think this is trauma alert level one, and then I have to think about it a bit more… if it thinks the same as me, then it's just driving, then I don't focus on it any more…” “… it would be a bit nice to say, yes but look, I think he's completely unharmed and this AI support also says he should be triaged as…”
Part 2: Prediction communication
About 16,800 papers were identified in the initial search. After applying eligibility criteria, including filtering out nonreview papers and papers not published in 2024, nine unique reviews were included, where 6 reviews focused on XAI approaches in general28–33 and 3 reviews focused on XAI approaches applied in the healthcare sector.34–36 Figure 2 presents the selection flowchart, and charted information is presented in a supplemental file (Tables S3 and S4, Appendix C). XAI considerations identified as important for prediction communication are summarized in Table 3.
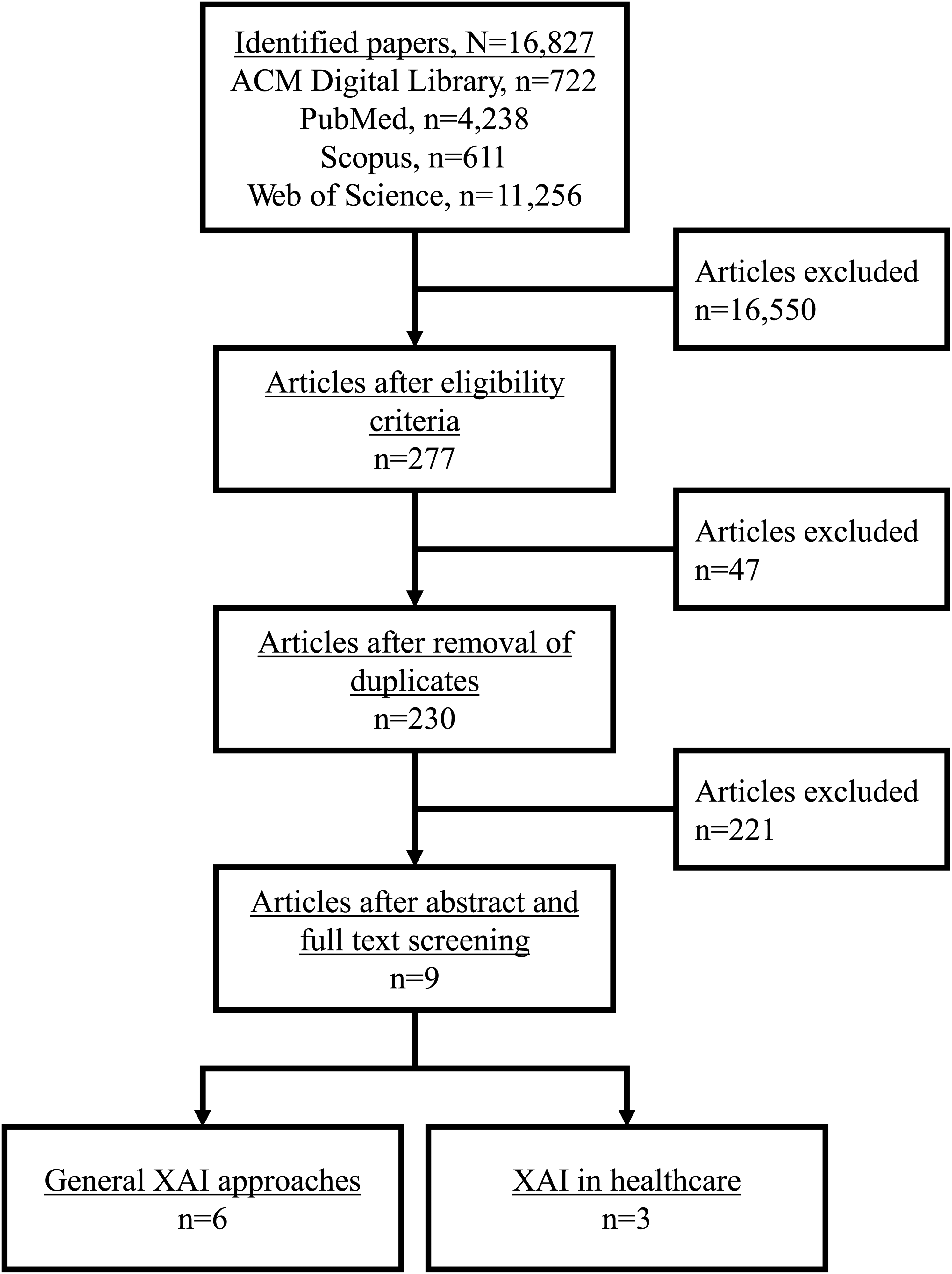
Review selection flowchart.
Key findings on prediction communication based on literature review of eXplainable AI (XAI) approaches.

Findings on general XAI approaches
Findings on XAI approaches in healthcare
Part 3: Prototype refinement
In this section, considerations and design options of the OSISP UI components are explored, evaluated and selected.
Complementary literature search
Evaluation and selection of UI components
The design should adapt to users utilizing both system 1 and 2 processing. To achieve this, the interface was designed with interactive cards that by default displays initial (system 1) information, with the option to access extended (system 2) information. Evaluation and selection of UI components are presented in Table 4, with indications of inclusion, modification and exclusion of previous OSISP UI components. 18 A summary of all UI component and functions is presented in Table 5.
Selection of new UI components.

Components from the first version of the OSISP UI presented in reference 18 .
Future work suggested for the OSISP UI presented in reference 18 .
New components suggestions.
CX/FX: component/function number; OSISP: On Scene Injury Severity Prediction; SHAP: Shapley Additive Explanations; UI: User Interface.
Summary of UI components and functions.

AI: Artificial Intelligence; UI: User Interface.
Prediction information page refinement
The included UI components were used to refine the prediction information page of the OSISP UI into four sections: prediction, entered predictors, missing predictors, and model details. The prediction information page with initial information is shown in Figure 3 and additional design details are presented in a supplemental file (Appendix D).

Refined OSISP prediction information page (initial information). The circles on the sides represent the UI component number: C1 = Risk prediction, C2 = Summary, C3 = Entered predictors for serious condition, C4 = Entered predictors against serious condition, C5 = Missing predictors, C6 = Model name, C7 = Model outcome, C8 = Use cases, F1 = Exploration mode, F2 = Filter for top 3 predictors for and against serious condition, F3 = Filter for top 3 missing predictors. OSISP: On Scene Injury Severity Prediction; UI: User Interface; M. Vehicle: Motor Vehicle; Inj. Mech: Injury Mechanism; Up. Extrm: Upper Extremity; AIS: Abbreviated Injury Scale; GCS: Glasgow Coma Scale; Sys-BP: Systolic Blood Pressure; Resp. Rate: Respiratory Rate; Dom. Type: Dominating Type of Injury; Resp. Time: Response Time; Card. Arrest: Cardiac Arrest.
Discussion
This study has conducted customer journey mapping and literature reviews to explore considerations of integrating OSISP in the clinical workflow and communicating OSISP's prediction to end users, as well as proposed a refined UI. The results showed critical information and decision points, predictor collection points, use cases, common XAI approaches in general and in healthcare, and options of UI components. Reflection of the results is important to understand how OSISP may support the EMS personnel.
Interpretation and implications of workflow integration
OSISP is intended to be used by any EMS personnel, from novices to experts, with varying education level and experience of working with AI or prehospital IT systems. Because novices may be defined as having less than a year of experience, 63 the workshop participants represent experts, since the clinical experience was at least 8 years. Compared to experts, novices tend to use guidelines and system 2 thinking more 37 and may therefore produce other use cases and design preferences. However, the critical information and decision points, and predictor collection points are considered independent of this factor as these were derived from standardized procedures. The workshop participants had mostly experience of working in a region where no digital platforms are yet available during prehospital patient assessment. In that regard, the participants are considered novices, which may cause their input to focus on usability rather than more detailed input on functionality and accuracy. 64 Nevertheless, obtaining input primarily on usability was deemed appropriate during early phases of product design.
Running OSISP as a dynamic service, i.e., the prediction updates as new data are entered, was appreciated. This is in line with recent research on using AI-based CDSS in all steps leading to a diagnosis of sepsis. 65 Practically, this would imply that OSISP can be used in all phases of the workflow, where early predictions (before reaching the patient) are based on alarm information. Notably, alarm information may be lacking or incorrect, 66 causing two conflicting cases where OSISP may on one hand support mental preparation by complementing with an early prediction on the patient's condition, on the other hand add information that is based on less reliable data and in worst case be misleading. Another implication of early predictions is that a prediction will only be shown when the confidence is as high as safely required by the healthcare organization, therefore predictions may not be triggered early in the workflow due to too low confidence (e.g. due to fewer predictors available, Table 2). This may result in unavailable predictions from receiving the call until conducting the first on scene assessment. Moreover, the current OSISP model uses some predictors that cannot be unknown. 16 Hence, if enabling early use of OSISP, the technology solution should be revised, and a warning of incorrect input data should be provided. As a result, when determining the confidence threshold for displaying predictions, healthcare organizations should consider the potential effects on both the model's performance (ratio of correct and incorrect predictions) and the availability of early predictions.
The current outcome of OSISP is a prediction whether the patient is severely injured or not. In a recent study, it has been proposed that the model outcome should be adaptable and recommend actions matching the steps leading to a diagnosis for successful human–AI collaboration. 65 In view of this proposal, it could be argued that the current OSISP outcome does not adapt to the clinical decision-making steps of the workflow (Supplemental file, Appendix A). Also, the outcome is not explicitly stated in the assessment or treatment protocols used today, which may reduce the user's autonomy of following standardized procedures and thereby increase the user's dependence on the AI support. Consideration of alternative outcomes is therefore valuable and could be inspired by the critical decision points (Table 2) and use cases. Actionable outcomes supporting these activities could be obtained by mapping the prediction of severely injured or not to assessment and treatment policies, for instance recommending transport of predicted severely injured patients to trauma centers. 11 However, recommendations on where to transport a patient often depends on carefully developed policies that consider the healthcare organization's resources. Because resources often differ between regions and nations, it is believed that an outcome on the patient's condition is more useful, as each healthcare organization can adapt it to their setting. Other more detailed alternatives of actionable outcomes could be recommended assessments, decisions and treatments, however, matching such outcomes would require extensive reviews by local clinical experts.
Comparison of refined prediction information page with existing solutions
The refined prediction information page (Figure 3 and Supplemental file, Appendix D) is largely based on knowledge from scientific publications. Yet, the novelty of the field and rapid development of new methods may put stakeholders in industry as suitable representatives of state of the art. Since the literature review performed in the present study did not consider gray literature, such information could be overlooked. Dialogs with industry representatives indicate implementation challenges with best practices for regulatory compliance. A brief search of AI solutions at websites belonging to prominent companies delivering IT-solutions for EMS, for example, MobiMed by Ortivus AB (Stockholm, Sweden), amPHI by Dedalus (Milan, Italy), Paratus by OMDA (Oslo, Norway), EWA by Bliksund (Grimstad, Norway), and ZOLL emsCharts by ZOLL Data Systems (Broomfield, Colorado, US), did not result in any new insights about AI-based CDSS.
Most of the current field triage tools are rule based, i.e., the patient's priority is determined by checking if one or more criteria are fulfilled, typically predefined vital signs, injury type, and mechanisms of injury. 6 There is an increasing body of literature presenting the potential benefit of using AI for predicting various trauma outcomes.8–10 However, to the authors’ knowledge, the literature on advancing these AI-models as CDSS is scarce and only one group from the Netherlands has been found to design their solution as a CDSS and advanced to prospective evaluations.11,45 That model classifies a patient as being severely injured or not, and was implemented as an application for smartphones and tablets named the trauma triage (TT) app. 45 Predictors were managed page-by-page by either entering an integer (continuous predictors), selecting between yes and no (dichotomous predictors), or marking regions on a figure (injury predictors), with a resulting recommendation on transport destination. 45
Comparison of current triage tools and the TT app with the refined OSISP UI presented here shows several differences. The OSISP UI is designed for tablets and does not provide an actionable outcome such as recommendation on transport destination. Information is not divided on separate pages, as entered input is displayed in the prediction information page, enabling the user to maintain a holistic picture of the situation without the need for information recall. The prediction information page was designed with intended end user and XAI in focus, resulting in extended information items (prediction, entered predictors, missing predictors, and model details) and functionalities for customization.
Interpretation and implications of refined prediction information page
The scope of the prediction information page is interesting to reflect on. If considering the most basic format, AI-based CDSS could be formatted and viewed as advanced checklists to enable close comparison with current rule-based protocols. Yet, findings from the literature review suggest that additional information is needed to make AI predictions clinically useful (Table 3). A more advanced interface than a checklist is therefore deemed needed to enable efficient XAI communication. An example of such interface is the TT app. 45 Although the work on the TT app has not addressed or evaluated XAI specifically, the interface presents a new approach for communicating predictors to users. When comparing the solution in the TT app with the proposed OSISP prediction information page, it is natural to question the scope of prediction communication. What is a reasonable scope? The question may be answered by reflecting on OSISP's position in the scientific debate on XAI and healthcare. It has been argued that black box models should not be used in a high stake domain like healthcare and that attempting to explain such models is misleading. 67 Instead, inherently interpretable models are recommended since they produce faithful explanations and can achieve high predictive performance. 67 By contrast, several of the reviewed XAI references point to the trade-off between interpretability and the predictive ability, list several examples of black box models with improved predictive performance, and emphasize the need of explanations when deploying AI in healthcare.
In light of this debate, the prediction information page may be considered a bridge. In the present study, the work was based on the proof-of-concept study, where models of varying complexity were tested and no significant difference in predictive ability was found. 16 This could motivate the selection of the logistic regression model as it is inherently interpretable. However, besides conveying trust it is also important to not increase the cognitive load as end users already have multiple factors to consider during the decision making. 68 With these aspects in mind, we believe the most important design principle is for the system to contain a uniform prediction information page applicable to any type of model, rather than focusing on whether the model is inherently interpretable or not. For instance, in the case of multiple CDSSs running in parallel, end users only need to learn how to use the prediction information page once to utilize any of the CDSSs. Employing a unified approach independent of model type is also in line with other XAI proposals, for instance systematic descriptions of models.22,54,55 To that end, the scope of the prediction information page is deemed appropriate.
A risk with the proposed OSISP UI may be increased cognitive load, as it consists of more information items and increased requirements for interaction compared to current field triage tools. Because novices tend to follow protocols strictly, 37 the UI may cause novices to spend additional time navigating the UI compared to current checklists. This may increase the perceived task complexity, possibly causing automation bias, i.e., over-reliance on the system. In critical situations, an increased cognitive load may risk patient safety. At the same time, XAI is deemed needed for successful adoption in healthcare. 21 A balance is therefore needed in our opinion, with a simple and intuitive design that minimizes the set of communication items and interactions, while providing understandable support that EMS personnel can use to make informed decisions. As no work studying XAI for prehospital use has been identified, finding a minimum set of UI components requires an iterative design process with intended end users involved.
Lastly, equal care should be provided to all. The refined OSISP UI has an increased possibility for customization. Users may then use OSISP with varying degree of efficiency, which raises the concern of its potential impact on the care provided. For instance, the extended information is a new proposal that intends to support novices, but may instead cause increased processing time if information is considered overwhelming. An alternative could be to remove customization functionalities so that only one navigation route results in the intended use. What is an appropriate level of design freedom remains to be answered as current findings on successful human–AI collaboration have not specifically targeted the prehospital setting. Verification and validation of OSISP and its UI with end users are therefore important to understand the potential impact of the proposed design on patient assessment and outcomes as well as clinical utility. This may be done using common design principles, for instance Nielsen's design principles. 69
Limitations
The customer journey map was generated based on the first patient scenario (traffic accident), with complementary discussions on potential changes in case of the second patient scenario (fall accident), making it possible that some aspects were missed when not constructing a separate customer journey map for the latter scenario. The workshop focused on ground ambulances, but OSISP may also be used in air and water ambulances. It is unclear how well the knowledge customer journey map may be transferred to these additional EMS services due to their different conditions. For instance, to the authors’ knowledge, air ambulances are usually staffed with a clinician with higher medical competence and have the option to transport patients over longer distances compared to ground ambulances. Water ambulances, on the other hand, are often staffed with people with lower levels of medical competence. Consequently, the generated customer journey map may lack perspectives to properly represent their workflow.
The literature review did not adapt the full methodology used for systematic or scoping reviews. This may impede the reproducibility of the findings. The review and search were also performed by a single author (author AB), which may cause biased results. However, the identified reviews largely overlapped, indicating that the most relevant content had been found. The terminology in XAI varies and may have caused some relevant literature to be missed. Only considering reviews during 2024 was decided to find current best practices, but may risk missing earlier XAI approaches. The explorative search to find inspiration for refining the UI may have missed important articles. None of the included literature on XAI targeted the prehospital setting specifically, therefore not all findings may be transferable.
The usability of the prediction information page was not tested in this study, which limits conclusions on how it will impact the EMS team's decision making during field triage. Furthermore, the flexible design allows EMS personnel to use the UI in a variety of ways, which may make conclusions on usability in future work challenging. The prediction information page was designed based on recommendations for successful human–AI collaboration based on findings from the workflow integration workshop and XAI review. Because the workshop was limited to ground ambulance teams and mainly included experienced participants from one region in Sweden, while the XAI literature did not address the prehospital setting, the prediction information page may need further refinement to enable efficient usage by all EMS teams. In addition, we acknowledge that technical barriers may impede implementation in current IT-platforms, but examining this in detail was beyond the scope of this study.
Future work
The proposed workflow integration and prediction information page hold promise to support EMS personnel as a CDSS, but its potential must be validated in collaboration with EMS personnel to ensure that the functionalities support decision making during field triage as intended. Future work should therefore focus on conducting usability tests, where VIPHS 17 should guide future activities. The findings from this study and previous OSISP activities resulted in a system design proposal, a first blueprint of step 1 of VIPHS. In the second step of VIPHS, the system design is tested in simulations with increased complexity. Thereby, future work should initiate the second step of VIPHS and conduct simplified simulations with EMS personnel, refine the system proposal if needed, and iteratively advance the complexity in the simulations until operational realism is reached. To ensure that all intended uses for OSISP have been identified and can be validated, it is important that future usability testing also involves participants with complementary experiences, i.e., EMS personnel with few years of experience and EMS personnel with experience of using IT platforms.
There are several functionalities that can be added to create a more holistic solution. First, the customer journey map should be expanded to cover perspectives of air and water ambulances. Next, EMS personnel may care for multiple patients at once. For such cases, ideally multiple CDSS for different conditions and outcomes could run simultaneously. An overarching model could be created to prioritize patients when resources are restrained based on predicted level of severity for individual patients, for example, for mass casualty incidents and military settings. Additional cognitive aspects may be interesting to study, for instance the perception of what is going on and higher system level impact from organizational and political-societal system levels. Adding these functionalities and aspects will make OSISP a more complete concept. For each refinement of OSISP, testing with end users, in controlled simulations with increasing complexity, is recommended to ensure usability.
To further advance OSISP, regulations, ethics and technical implementation are next to study. OSISP is considered to be an active medical device software since it is a service that analyses patient data and will be deployed on a digital platform. Special legal requirements need to be fulfilled for such device. To demonstrate that OSISP fulfills MDR, the process to obtain the CE-marking must be conducted, including the assessment of the risk class, product development, safety and performance evaluation, technical documentation, conformity assessment, and a plan for postmarket surveillance. Ensuring privacy and responsibility will be important ethical questions to address. As EMS personnel are responsible for their decisions when using current tools, a similar responsibility role is expected when OSISP is implemented. While the suppliers of OSISP must ensure good performance and patient safety according to regulations such as the AI Act in EU, the healthcare organizations implementing the CDSS must ensure that usage aligns with the supplier's documentation. The responsibility is therefore expected to be distributed across suppliers, EMS personnel, and healthcare organizations. Lastly, consulting suppliers of EMS IT systems on what UI components can be implemented is needed, for example, if the interactive functionalities are reasonable, and if standardized resources for exchanging healthcare information, such as Fast Health Interoperability Resources, exists to capture the extended information at the prediction information page.
Conclusion
In this study, OSISP has been advanced as an AI-based CDSS by studying workflow integration, UI design and communication of predictions to end users. The customer journey map analysis found critical information and decision points throughout the prehospital workflow, which led to identification of several use cases for OSISP such as supporting assessment and prioritization of trauma patients, as well as being a second opinion. Workshop participants recommended OSISP to continuously update when new data are entered, and a complete set of predictors was found available from on scene assessment and treatment and forward in the workflow. Based on the literature reviews, key considerations for human–AI collaboration were identified, including recommended communication content, characteristics and goals, as well as implementation options. The findings were used to refine the UI page that communicates OSISP's predictions to end users, resulting in eight UI components and four UI functions with information on the prediction, entered predictors, missing predictors, and model details. The prediction information was divided into two layers: default information supporting experts, and extended information supporting novices or unsure users. Future work includes usability testing of the OSISP UI to ensure clinical utility. Further development of OSISP may be beneficial to support end users already when receiving the call. Lastly, this work has derived five design principles that may inspire development of other AI-based CDSS for healthcare in general, and prehospital settings in particular: (1) user-centered development (base design-phase on feedback from end users and workflow); (2) consistent UI (modular design usable by a variety of models); (3) contextual communication (holistic description with continuously updated information and adaptable notifications); (4) informed safety-nets against uncertainty (prediction explained and only communicated if above threshold and for intended use cases); and (5) flexible interaction (intuitive, customized, and actionable design).
Supplemental Material
sj-docx-1-dhj-10.1177_20552076251403207 - Supplemental material for Human–AI collaboration for prehospital trauma triage: Designing the On Scene Injury Severity Prediction (OSISP) model as a clinical decision support system
Supplemental material, sj-docx-1-dhj-10.1177_20552076251403207 for Human–AI collaboration for prehospital trauma triage: Designing the On Scene Injury Severity Prediction (OSISP) model as a clinical decision support system by Anna Bakidou, Magnus Andersson Hagiwara, Eunji Lee, Eva-Corina Caragounis, Bengt Arne Sjöqvist, Mattias Seth, Anders Jonsson and Stefan Candefjord in DIGITAL HEALTH
Supplemental Material
sj-pdf-2-dhj-10.1177_20552076251403207 - Supplemental material for Human–AI collaboration for prehospital trauma triage: Designing the On Scene Injury Severity Prediction (OSISP) model as a clinical decision support system
Supplemental material, sj-pdf-2-dhj-10.1177_20552076251403207 for Human–AI collaboration for prehospital trauma triage: Designing the On Scene Injury Severity Prediction (OSISP) model as a clinical decision support system by Anna Bakidou, Magnus Andersson Hagiwara, Eunji Lee, Eva-Corina Caragounis, Bengt Arne Sjöqvist, Mattias Seth, Anders Jonsson and Stefan Candefjord in DIGITAL HEALTH
Supplemental Material
sj-pdf-3-dhj-10.1177_20552076251403207 - Supplemental material for Human–AI collaboration for prehospital trauma triage: Designing the On Scene Injury Severity Prediction (OSISP) model as a clinical decision support system
Supplemental material, sj-pdf-3-dhj-10.1177_20552076251403207 for Human–AI collaboration for prehospital trauma triage: Designing the On Scene Injury Severity Prediction (OSISP) model as a clinical decision support system by Anna Bakidou, Magnus Andersson Hagiwara, Eunji Lee, Eva-Corina Caragounis, Bengt Arne Sjöqvist, Mattias Seth, Anders Jonsson and Stefan Candefjord in DIGITAL HEALTH
Supplemental Material
sj-pdf-4-dhj-10.1177_20552076251403207 - Supplemental material for Human–AI collaboration for prehospital trauma triage: Designing the On Scene Injury Severity Prediction (OSISP) model as a clinical decision support system
Supplemental material, sj-pdf-4-dhj-10.1177_20552076251403207 for Human–AI collaboration for prehospital trauma triage: Designing the On Scene Injury Severity Prediction (OSISP) model as a clinical decision support system by Anna Bakidou, Magnus Andersson Hagiwara, Eunji Lee, Eva-Corina Caragounis, Bengt Arne Sjöqvist, Mattias Seth, Anders Jonsson and Stefan Candefjord in DIGITAL HEALTH
Supplemental Material
sj-pdf-5-dhj-10.1177_20552076251403207 - Supplemental material for Human–AI collaboration for prehospital trauma triage: Designing the On Scene Injury Severity Prediction (OSISP) model as a clinical decision support system
Supplemental material, sj-pdf-5-dhj-10.1177_20552076251403207 for Human–AI collaboration for prehospital trauma triage: Designing the On Scene Injury Severity Prediction (OSISP) model as a clinical decision support system by Anna Bakidou, Magnus Andersson Hagiwara, Eunji Lee, Eva-Corina Caragounis, Bengt Arne Sjöqvist, Mattias Seth, Anders Jonsson and Stefan Candefjord in DIGITAL HEALTH
Footnotes
Acknowledgements
The authors wish to extend their sincere appreciation to all participants who shared their expertise and experience during the workshop. Special thanks go to EMS personnel Elisabeth Tejlin for the support in workshop recruitment. Finally, the authors gratefully acknowledge the financial support provided by the funding bodies.
ORCID iDs
Ethical considerations
The study was conducted in accordance with the Declaration of Helsinki and approved by Chalmers Data Protection Officer. The data have been managed in accordance with Chalmers University of Technology's policies and undergone review by Chalmers Data Office. Under the Swedish Ethical Review Act (SFS 2003:460), ethics approval was not required as no sensitive personal data or data about legal violations were processed. Any personal data inadvertently included were excluded from the research material.
Consent to participate
All participants provided written informed consent prior to participating in the workshop.
Contributorship
AB, AJ, BAS, ECC, MAH, MS, and SC were involved conceptualization; AB in data curation, formal analysis, software, visualization, and writing—original draft; AB, AJ, BAS, and SC in funding acquisition; AB, BAS, ECC, and MAH in investigation; AB, AJ, BAS, ECC, EL, MAH, MS, and SC in methodology; AB and SC in project administration; AB, BAS, ECC, MAH, and SC in resources; AJ, BAS, ECC, MAH, and SC in supervision; BAS, ECC, and MAH in validation; and AB, AJ, BAS, ECC, EL, MAH, MS, and SC in writing—review & editing.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Swedish Carnegie Hero Fund; the European Union through the Norwegian-Swedish European Interreg project "Kontiki - Artificiell intelligens (AI) som beslutsstöd för patienter och hälso- och sjukvård"; the Center for Disaster Medicine at University of Gothenburg; and the Strategic Innovation Program IoT Sweden, a joint venture by Vinnova, Formas and the Swedish Energy Agency, through the IoT project "ASAP - Bättre civila och militära prehospitala Point-of-Care beslut med hjälp av datafusion och AI" (grant number 2022-03748).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The workshop datasets created and analyzed based on voice recordings are not publicly available due to the potential identification of participants. Access to the data is restricted to ensure participant confidentiality and privacy. Process description, generated customer journey map, charted data from the review, and the refined OSISP UI are available in supplemental files (![]() ).
).
Guarantor
SC
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.