
Abstract
Background
The rising prevalence of mental health disorders such as depression and anxiety challenges traditional treatments limited by resource shortages, poor accessibility, and low adherence. Digital health technologies—particularly digital mental health interventions—offer innovative, scalable, and personalized solutions. Mobile health applications, online cognitive behavioral therapy (CBT), and AI-driven tools are becoming essential in mental health care.
Methods
This study employs bibliometric methods to examine research trends and thematic evolution in digital mental health self-management interventions, using data retrieved from the Web of Science Core Collection (WoSCC). CiteSpace, VOSviewer, and Bibliometrix were applied to quantify research output, collaboration networks, and influential topics. The analysis covered English-language publications from 2006 to 2025, with internal consistency checks and sensitivity analyses within the WoSCC dataset ensuring robustness.
Results
A total of 2262 eligible publications were retrieved, showing a clear growth trajectory. The United States led with 932 publications, followed by the United Kingdom and Australia. Citations surged after 2016, peaking in 2023, reflecting increasing academic and clinical relevance. Research has shifted from feasibility studies to AI-enhanced and personalized interventions. Keywords such as “artificial intelligence,” “digital CBT,” and “personalized care” showed notable growth. International and interdisciplinary collaborations also expanded, underscoring the field's global integration.
Conclusion
Digital mental health interventions are evolving from traditional models to intelligent, personalized solutions, providing scalable solutions to global mental health challenges. This study offers insights into future research directions, focusing on technology integration, ethical issues, and clinical validation to drive global application.
Introduction
Depression, anxiety, and mood disorders are among the leading causes of disability and are increasingly recognized as a major global public health challenge. 1 According to the World Health Organization (WHO), over 400 million people worldwide suffer from depression, making it the leading cause of disability.2,3 These mental health issues significantly affect individuals’ quality of life and pose substantial economic and social burdens. Traditional therapeutic approaches, including psychotherapy and pharmacological treatments, have shown effectiveness in alleviating symptoms. 4 However, these methods face significant barriers, such as limited access to qualified mental health professionals, long waiting times for appointments, and high treatment costs, particularly in low- and middle-income countries. These limitations highlight the urgent need for scalable, accessible, and cost-effective solutions to address the growing global mental health crisis.5,6 Digital health technologies, including mobile health applications (mHealth), telehealth platforms, and artificial intelligence (AI)-driven interventions, present promising solutions to these challenges.7–9 By overcoming geographical and temporal limitations, these technologies provide scalable and personalized interventions that can be delivered globally, particularly benefiting underserved populations who lack access to traditional face-to-face therapy. They also enable real-time monitoring, tailored treatment strategies, and continuous support, thereby improving outcomes and adherence.
Over the past decade, digital mental health interventions have expanded to include formats such as mHealth applications, online cognitive behavioral therapy (CBT), virtual platforms, and remote consultations. 10 These tools have demonstrated effectiveness in enhancing self-management and reducing symptoms of depression, anxiety, and post-traumatic stress disorder (PTSD),11,12 complementing conventional therapies by offering more accessible and affordable solutions, especially in remote or underserved settings.13,14 The integration of AI and machine learning has further advanced the field, enabling precision-based therapeutic models that dynamically adapt to individual needs.15–18 Importantly, the scalability of these approaches ensures their potential for wide deployment across large populations. 19 Given this rapid evolution, there is a pressing need for systematic approaches to capture the field's development. Traditional narrative reviews often fall short in encompassing such a complex and interdisciplinary domain. 20 Bibliometric methods, by quantifying research output, collaboration patterns, and thematic evolution, provide a powerful tool to map intellectual trajectories, identify influential contributors, and highlight emerging research priorities in digital mental health. This makes bibliometric analysis particularly valuable for understanding both the progress and future directions of this field. Through the use of citation analysis, keyword co-occurrence networks, and author collaboration maps, bibliometric methods allow for a comprehensive understanding of the field's intellectual structure. These tools help researchers identify emerging topics, track the development of new technologies, and uncover gaps in the existing literature. In comparison to traditional qualitative analysis, bibliometric methods provide a more objective and holistic view of the research landscape, enabling the identification of influential studies, key areas of growth, and potential directions for future research.
However, a consolidated bibliometric synthesis that concurrently profiles geographic and institutional leadership, maps influential authors and landmark publications, delineates emerging themes and technology trajectories (e.g. AI-enabled, mHealth-based, personalized digital CBT), and characterizes patterns of international and interdisciplinary collaboration remains lacking. Previous bibliometric reviews—such as those published in JMIR outlets and other digital health journals—have provided valuable insights into publication trends and collaboration structures but were generally limited to shorter time spans (often ending before 2023), single-tool analyses, or narrower thematic scopes. By contrast, the present study extends coverage through mid-2025 and integrates multiple analytic frameworks (Bibliometrix, VOSviewer, and CiteSpace) to ensure methodological triangulation and transparency. It further incorporates emerging domains such as AI-driven and ethics-informed digital mental health research, expands visualization techniques through dual-map overlays and author-institution-keyword Sankey networks, and situates findings within global policy frameworks including the WHO Mental Health Action Plan and the WHO Guideline on Digital Interventions for Health System Strengthening. Collectively, these advances enable a deeper, more contemporary, and policy-relevant understanding of how digital mental health interventions are evolving in the post-pandemic and AI-driven era.
This study employs bibliometric methods to systematically analyze the current state of research on digital mental health self-management interventions. Specifically, we quantify publication and citation dynamics; identify leading countries and institutions; chart author collaboration networks and highly cited works; trace keyword co-occurrence and thematic evolution; and describe cross-national and cross-disciplinary collaboration structures and their contribution to field development. By examining research output, collaboration networks, and keyword evolution, this study aims to map the intellectual development of the field and provide insights into emerging trends and future directions. The results of this analysis will help guide further research in the area, providing a data-driven foundation for the ongoing evolution of digital mental health interventions.
Materials and methods
Data source and search strategy
All bibliometric data were retrieved from the Web of Science Core Collection (WoSCC), including the Science Citation Index Expanded (SCI-E) and Social Sciences Citation Index (SSCI). WoSCC, recognized as one of the most authoritative and widely used bibliographic databases, offers rigorous inclusion standards, standardized citation data, and extensive coverage of high-quality core journals across multiple disciplines. 21 It has been extensively applied in bibliometric analyses of medicine, psychology, and digital health, providing a reliable source for mapping the intellectual structure and evolution of this field. The search strategy targeted three thematic components: digital health technologies, mental health outcomes, and behavioral/psychological interventions. Search terms were combined using Boolean logic to ensure comprehensive coverage, and the complete search string is provided in Supplemental Table S1. The search was conducted on 25 July 2025, covering literature from 1 January 2006 to 20 July 2025. Filters were applied to include peer-reviewed Articles and Reviews published in English. A total of 3004 records were initially retrieved, of which 2262 remained after applying inclusion and exclusion criteria.
Inclusion and exclusion criteria
To ensure the quality and consistency of the data, the following inclusion and exclusion criteria were applied: Inclusion criteria: Publication type limited to peer-reviewed Articles and Reviews; Indexed in SCI-E or SSCI; Published in English; Publication date between 1 January 2006, and 20 July 2025. Exclusion criteria: Non-journal content such as Meeting abstract, Editorial materia, Proceedings paper, or corrections; Incomplete metadata (e.g. missing author or institution); Duplicate records. After applying these criteria and performing manual de-duplication and quality checks, a total of 2262 records were retained, comprising 1763 articles and 499 reviews. The literature selection process is visualized in Figure 1.

Literature retrieval and analysis process.
Data cleaning and preprocessing
All bibliographic records were exported in plain text format (“Full Record and Cited References”) and imported into RStudio (version 2023.03.0). The bibliometrix R package (version 4.2.1) was used for preprocessing and data cleaning, including the following steps: Deduplication: Standardization of author names, institutions, and keywords by correcting inconsistent spellings and formatting. Field harmonization: Consolidation of key bibliographic fields, including first author (FAU), corresponding author (RP), country (CU), organization (C1), and keywords (DE, ID). Data transformation: Conversion of bibliographic records into a structured data frame suitable for quantitative and network analysis.
Bibliometric and visualization techniques
A hybrid bibliometric framework combining multiple software tools was applied to enable a multi-dimensional exploration of the literature. Descriptive bibliometric analysis was conducted using the bibliometrix R package (v4.2.1) to extract key indicators such as annual publication output, productive authors, country and institutional contributions, and journal distributions. 22 Collaboration network analysis was performed in VOSviewer (v1.6.20) and Pajek (v5.17). For network construction, a minimum occurrence threshold of 10 and full counting were used, followed by association-strength normalization. Communities were detected using a modularity-based clustering algorithm (resolution parameter = 1.0; minimum cluster size = 5), consistent with prior bibliometric studies in digital health. Co-citation and burst detection analyses were conducted with CiteSpace (v6.2.R6) using 1-year time slices (2006–2025), Top-50 records per slice, and Pathfinder + MST pruning. Clusters were identified using the log-likelihood ratio algorithm, and burst detection employed γ = 0.8 with a minimum burst duration of 2 years to capture emerging topics and intellectual bases. Trend analyses were performed in R (v4.3.1) using a cubic polynomial regression model (R2 = 0.95, p < 0.001), consistent with established strategies for modeling nonlinear publication trends. Robustness was verified through ±20% threshold sensitivity tests, confirming the stability of observed patterns. Figure refinement was completed in Scimago Graphica (v1.0.26), exporting all maps at 400 dpi, with a minimum font size of 8 pt and color-blind-safe palettes. All analytical scripts were cross-checked for internal consistency and reproducibility, ensuring full methodological transparency.
Statistical methods
Descriptive statistics were used to quantify publication outputs, citation distributions, H-index values, and author productivity, providing an overview of global research activity. Annual trends from 2006 to 2025 were visualized to assess growth. Linear regression models estimated yearly increases, while Spearman's rank correlation coefficients evaluated relationships between bibliometric indicators (e.g. citation frequency and publication output by country or institution). 23 A two-tailed p < 0.05 was considered statistically significant. All analyses were conducted in R (version 4.3.1), ensuring reproducibility and robustness, with findings interpreted to identify influential contributors, impactful topics, and disparities within the digital mental health research landscape.
To enhance methodological transparency, this study was conducted in accordance with the BIBLIO reporting guideline for bibliometric reviews. The completed BIBLIO checklist is provided in Supplemental File 1.
Results
Analysis of publication dynamics and citation patterns
From 2006 to July 2025, 2262 eligible publications on digital health interventions for anxiety and depression self-management were retrieved. Output showed a two-phase pattern: a slow growth period (2006–2012, fewer than 30 publications annually) followed by rapid expansion after 2016, peaking in 2023 with over 300 articles (Figure 2(A)). This peak likely reflects the combined effects of the COVID-19 pandemic accelerating telehealth adoption, the widespread penetration of mobile technologies, and increasing regulatory and funding support. Publication numbers slightly declined afterward, though overall activity remained high, consistent with the normalization of post-pandemic research. Citations rose sharply between 2021 and 2023, paralleling publication growth and underscoring rising academic and clinical influence. This surge also aligns with the typical 12–24 month citation lag, indicating that studies conducted since 2019 were increasingly recognized during this period. Subject category analysis highlighted “Health Care Sciences Services” and “Psychiatry” as the largest contributors, followed by “Medical Informatics” and “Clinical Psychology” (Figure 2(B)). This reflects a disciplinary shift from feasibility research toward implementation science, service delivery, and clinical outcome evaluation, with informatics providing critical methodological support. Cubic polynomial fitting confirmed the accelerating growth of both publications and citations, with R2 values exceeding 0.95 (Figure 2(C)). The turning point after 2016 marked the transition from pilot studies to large-scale trials and real-world applications, suggesting that digital mental health interventions are entering a rapid expansion phase with increasing potential to address the global burden of depression and anxiety.

Publications and citation analysis. (A) Annual scientific production and citations from 2006 to 2025. (B) Distribution of publications across subject categories. (C) Cubic polynomial fitting of annual citations and publications.
Global landscape of national contributions and collaborations
Figure 3 and Table 1 illustrate the global distribution and collaborative dynamics of digital mental health research. The international co-authorship network (Figure 3(A)) shows a densely connected cluster dominated by high-income countries, with the United States, the United Kingdom, Australia, and Canada serving as central hubs of collaboration. Since 2015, these countries have demonstrated a steep rise in publication output (Figure 3(B)), reflecting both the worldwide expansion of digital platforms and the growing prioritization of mental health on global policy agendas. Co-authorship network analysis (Figure 3(C)) highlights the dominance of English-speaking nations, while countries such as Switzerland and the Netherlands act as important bridges in transcontinental collaborations, strengthening knowledge exchange across regions. The visualization of publication density and collaboration strength (Figure 3(D)) further confirms that Western countries not only produce the largest research volume but also occupy central roles in shaping collaborative networks, thereby amplifying their academic influence. As shown in Table 1, the United States led with 932 publications and 31,257 citations, maintaining its dominant academic influence, while the United Kingdom (n = 301) and Australia (n = 271) followed as major contributors. Notably, Switzerland demonstrated the highest proportion of international collaboration (53.8%), underscoring how smaller nations can achieve outsized impact through extensive cross-national partnerships. Of particular note, Switzerland demonstrated the highest proportion of international collaboration (53.8%), suggesting that smaller nations can achieve global impact through extensive cross-national cooperation. Collectively, these findings indicate that global leadership in digital mental health is strongly linked not only to research productivity but also to the ability to engage in international collaboration, which enhances both research quality and global impact. To improve readability, a simplified version of the co-authorship network is presented in Figure 3, highlighting only the most influential countries and collaborations. The full, detailed network is provided in Supplemental Figure S1 for readers who wish to explore the complete structure.

International collaboration and country-level publication analysis. (A) Global collaboration network of contributing countries. (B) Temporal trends of publications in leading countries. (C) Co-authorship network among major contributing countries. (D) Visualization of publication volume and collaboration strength by country.
Top 10 contributing countries in digital mental health research.

Evolution of scholarly collaboration and institutional influence
Collaboration in digital mental health research has become increasingly concentrated. As shown in Figure 4(A)–(C), core scholars such as Alvarez-Jimenez, Mario and Torous, John demonstrate not only high productivity but also strong centrality within co-authorship networks, underscoring their pivotal role in advancing the field. Their influence extends beyond output volume to connecting otherwise fragmented research groups, shaping knowledge flow, and setting methodological standards for digital psychiatry. At the institutional level, analyses in Figure 4(D) and (E) highlight organizations such as King's College London, Harvard Medical School, and the University of California system as persistent leaders in both collaboration and citation networks. As shown in Table 2, Harvard Medical School ranked first among institutions with 112 publications, followed by King's College London with 61 publications and the University of Washington with 70 publications, reflecting sustained leadership. Among individual scholars, John Torous led with 112 publications and 4925 citations, while Mario Alvarez-Jimenez contributed 95 publications with 3642 citations, confirming their central roles in shaping the field. These institutions function as global hubs, integrating interdisciplinary expertise from psychiatry, informatics, and public health to drive innovation. The Sankey diagram in Figure 4(F) illustrates triadic linkages between authors, institutions, and high-frequency keywords. Terms such as “telemedicine” and “mobile app” recur across clusters, suggesting convergence in thematic priorities. This convergence indicates that the field is moving toward standardized and scalable digital solutions rather than fragmented innovations. Together, these findings underscore that a small set of highly productive authors and institutions—quantitatively verified in Table 2—serve as both intellectual and organizational anchors for digital mental health research.

Co-authorship and institutional collaboration networks. (A) Co-authorship clusters. (B) Author collaboration network. (C) Temporal trends among top authors. (D) Institutional collaboration map. (E) Institutional citation network. (F) Preliminary links among authors, institutions, and keywords.
Top 10 institutions by publication volume in digital mental health research.

Core journals and foundational literature shaping the field
The co-citation and source analysis delineates the intellectual foundation of digital mental health self-management research. As shown in Figure 5(A), a small set of journals—most prominently the Journal of Medical Internet Research (JMIR), JMIR Mental Health, and Internet Interventions—dominate the co-citation network, serving as the primary venues for dissemination and influence. Figure 5(B), consistent with Bradford's Law distribution, confirms that after this core group, productivity declines sharply, underscoring the centrality of these few outlets. Table 3 reinforces this concentration, with JMIR exhibiting the highest h-index (62) and impact factor (6.0), reflecting both consistent output and strong citation performance. The intellectual trajectory of the field is further illuminated through Figure 5(C), which depicts the reference co-citation network, and Figure 5(D), which presents the LCS timeline. Together, they reveal how conceptual priorities evolved from feasibility and app-based delivery to CBT efficacy, patient engagement, and, more recently, to ethical governance and AI personalization. Foundational works by Firth (2017), Torous (2018), and Alvarez-Jimenez (2018) serve as key anchors in this evolution. Finally, Figure 5(E), showing citation burst analysis, highlights the surging influence of keywords and references aligned with AI-driven personalization and digital ethics. Table 4 complements these results, listing the most locally cited documents, with Firth's meta-analysis (2017) and Torous's mobile health framework (2018) exemplifying works that continue to anchor subsequent scholarship. To enhance clarity, only a simplified version of the co-citation and reference networks is displayed in Figure 5 within the main text, highlighting the most influential nodes and clusters. The complete, more complex network visualizations are provided in Supplemental Figure S2 for readers seeking detailed exploration.
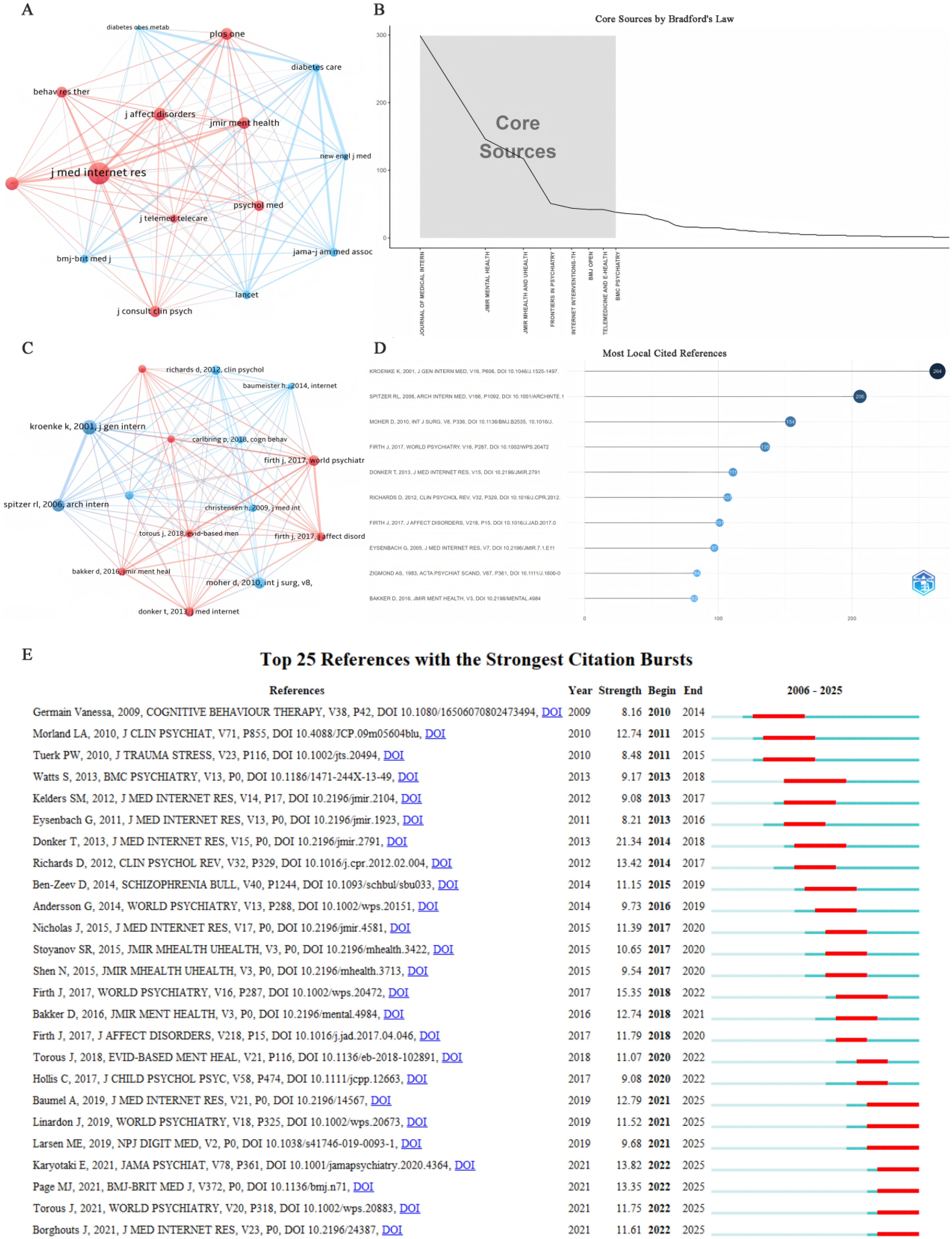
Core journals and foundational literature. (A) Co-citation network of journals showing inter-journal intellectual linkages. (B) Core source identification based on Bradford's Law. (C) Highly co-cited references network map. (D) Top 10 most locally cited references. (E) Top 25 references with the strongest citation bursts from 2006 to 2025.
Top 10 core journals contributing to the field of digital mental health self-management.

Top 10 most locally cited references in the field.

Keyword evolution reveals emerging hotspots and thematic shifts
Keyword analysis provided a comprehensive overview of research hotspots and thematic evolution. High-frequency terms such as “mHealth,” “mental health,” “eHealth,” “telemedicine,” and “depression” dominated the landscape, underscoring a sustained research focus on integrating digital tools into mental health interventions (Figure 6(A)). The keyword co-occurrence network (Figure 6(B)) reflected strong interconnections among terms, while cluster analysis (Figure 6(C)) identified distinct thematic modules, including “#0 mobile phone intervention,” “#1 cognitive behavioral therapy,” and “#3 youth mental health.” These clusters demonstrate how digital mental health research has gradually evolved from technology-driven approaches toward population-tailored and therapy-specific applications. Burst detection analysis (Figure 6(D)) illustrated the temporal dynamics of research interest. Early bursts were observed in keywords such as “telemedicine” and “internet,” which maintained strong citation momentum from 2006 onward. This early focus reflected the field's initial reliance on digital infrastructure as a substitute for traditional care. In contrast, recent surges in “collaborative care,” “smartphone application,” and “peer support” signaled a shift toward patient-centered care, digital self-management tools, and integrated therapeutic models. The timing of these bursts coincides with the global proliferation of mobile devices and heightened interest in scalable, community-based interventions, which may explain their rapid rise in prominence.

Keyword and topic network analysis. (A) Treemap of high-frequency keywords, highlighting dominant research focuses. (B) Keyword co-occurrence network showing interconnected research themes. (C) Clustered thematic map revealing distinct topic communities based on co-occurrence patterns. (D) Top 25 keywords with the strongest citation bursts from 2006 to 2025, indicating temporal shifts in research attention.
Emerging themes and disciplinary evolution
Figure 7 systematically maps the evolving thematic landscape and disciplinary shifts within digital mental health research. The thematic map (Figure 7(A)) identifies “self-management,” “care,” and “health” as motor themes, while “depression,” “mental health,” and “anxiety” remain in the basic but highly central quadrant, underscoring their enduring importance as foundational anchors. Conversely, topics such as “telepsychiatry” and “posttraumatic stress disorder” appear as niche or declining, suggesting that scholarly attention has shifted away from disorder-specific approaches toward broader, technology-enabled strategies. The heatmap (Figure 7(B)) highlights the surge of emerging terms like “apps,” “machine learning,” and “digital health” after 2020, reflecting both the rapid diffusion of mobile technologies and the growing integration of AI into mental health services. Co-word cluster analysis (Figure 7(C)) confirms ten dominant research directions, with clusters such as “digital health” (#1), “mobile health” (#2), and “medication adherence” (#3) representing the most interconnected and dynamic fronts. This indicates a paradigm transition from feasibility validation to clinically embedded interventions aimed at improving adherence and long-term outcomes. The dual-map overlay (Figure 7(D)) reveals extensive transdisciplinary citation patterns linking psychology, education, and healthcare with molecular biology and systems science, demonstrating that the field is no longer siloed but increasingly embedded within broader biomedical and computational ecosystems. To enhance clarity and readability, a simplified version of the dual-map overlay is presented here, while the full-scale, detailed network is provided in the Supplemental Figures (Figure S7D) for reference.

Thematic evolution and disciplinary trends. (A) Thematic map identifies core themes such as “self-management” and “mental health.” (B) Heatmap shows rising prominence of keywords like “apps” and “digital health.” (C) Co-word clustering reveals 10 major research topics, with “digital health” and “mobile applications” leading. (D) Dual-map overlay illustrates citation paths across disciplines, linking psychology, medicine, and biology.
Discussion
Over the past two decades, digital mental health research has undergone a clear transformation. As summarized in Figure 8, milestone studies across this period collectively illustrate the field's progression from early feasibility trials to AI-driven, precision-oriented interventions. Beyond describing quantitative growth, these developments reflect deeper structural forces—policy priorities, technological maturation, and funding incentives—that shape research focus and collaboration patterns. The steady expansion of publications and collaborations therefore reflects not only academic interest but also system-level responses to the demand for scalable, cost-effective mental health care in low- and middle-income countries. At the same time, disparities persist—such as English-language dominance and regional underrepresentation—highlighting the need for balanced global participation. The rise of personalized and context-sensitive digital CBT suggests a shift from feasibility to user-centered implementation, where interventions adapt dynamically to individual needs and engagement barriers. Interdisciplinary collaboration between clinicians, computer scientists, and policymakers indicates that digital mental health has evolved from an experimental niche to a mainstream innovation ecosystem. Collectively, these patterns point to a maturing field focused on responsible, evidence-informed implementation at scale, rather than asserting clinical effectiveness that bibliometric data cannot directly evaluate.

Milestone studies shaping the field of digital mental health.
Digital mental health research has evolved from early feasibility studies to sophisticated, personalized, and AI-driven interventions. 24 Our bibliometric maps trace this trajectory and situate it within existing evidence. In the initial phase (2006–2012), internet-delivered CBT established feasibility and efficacy, 25 with meta-analyses consolidating its effectiveness for depression and anxiety.26,27 From 2013 to 2018, the expansion of mHealth and hybrid care models reflected a shift toward real-world usability and integration.28,29 Empirical studies demonstrated that user engagement, design quality, and affordability were as critical as therapeutic content30,31—an insight that remains central to the success of digital interventions.
Since 2019, the rapid integration of AI, deep learning, and natural language processing has marked a turning point toward precision-oriented, adaptive, and data-driven interventions. 32 Keyword co-occurrence analysis revealed surging attention to “digital phenotyping,” “AI,” and “personalized intervention,” consistent with a global shift toward context-aware systems. Evidence shows that AI integration enhances personalization, optimizes outcomes, 33 and reshapes the clinician's role in decision-making.34,35 However, this transformation also raises critical questions of accountability, fairness, and governance.36,37 Ethical and regulatory considerations—data privacy, ownership, and algorithmic bias—are now central to ensuring trust and equity in deployment. International frameworks such as the GDPR and WHO's digital ethics guidance offer practical blueprints for transparency, accountability, and user autonomy. Integrating these principles into AI-enabled digital psychiatry is essential for responsible innovation and sustained public confidence.
Geographic and institutional analyses reveal structural rebalancing. While high-income countries (e.g. the United States, the United Kingdom, and Australia) remain dominant, emerging contributions from East Asia and Northern Europe indicate diversification and increasing global collaboration. 38 This trend not only enriches the research landscape but also creates opportunities for culturally adapted, locally relevant digital interventions in resource-limited contexts. Moreover, the field has gained granularity, with targeted attention to condition- and population-specific approaches (e.g. PTSD, eating disorders, psychosis; youth, veterans, postpartum populations).39,40 Concurrently, the integration of “telepsychiatry,” “wearables,” and “virtual reality” shows that digital components are becoming embedded across broader service infrastructures, signaling a transition from experimental tools to integral healthcare elements.41–44
One of the key strengths of this study lies in its multi-tool bibliometric design, combining CiteSpace, VOSviewer, and Bibliometrix for triangulated mapping of intellectual structures and thematic evolution. To avoid overstatement, we clarify that our design cannot measure clinical efficacy; it identifies where confirmatory and implementation studies are needed. Internal consistency checks and sensitivity analyses were performed within the WoS Core Collection, but our dataset was limited to English-language publications. This limitation may exclude relevant evidence from non-English contexts (e.g. Yin, H., 2020; Wani et al., 2024).45,46 Future studies should incorporate multi-database searches (e.g. Scopus, CNKI, Scielo, LILACS, Ichushi) to improve representativeness and inclusivity. Despite these limitations, a longitudinal bibliometric lens remains valuable for identifying knowledge gaps, guiding hypotheses, and informing strategic directions for future empirical work.
This bibliometric analysis has several limitations that should be acknowledged. First, the data were derived exclusively from the WoSCC, which—despite its comprehensive coverage—may omit relevant studies indexed in other databases such as Scopus, PubMed, or regional repositories. Second, the analysis was restricted to English-language publications, potentially underrepresenting research contributions from non-English-speaking regions and introducing linguistic bias. These constraints may limit the global representativeness of our findings. Future studies integrating multi-database and multilingual evidence are needed to enhance inclusivity and cross-cultural validity.
From a translational standpoint, our results inform research and policy implications rather than direct clinical recommendations. The identified emphasis on AI integration, mobile CBT, and personalization can guide standards for data governance, transparency, and human-centered design, aligned with the WHO's Mental Health Action Plan and WHO guidelines on digital interventions. Real-world implementations such as conversational agents (e.g. Woebot and Wysa) demonstrate feasibility but require rigorous evaluation and ethical oversight to ensure equity and safety. Evidence from community-based and non-specialist contexts shows that digital tools can expand mental health service capacity in resource-constrained settings.47,48 Collectively, these findings highlight that digital mental health solutions can advance equity only when embedded within culturally responsive, ethically governed, and evidence-based frameworks.
Looking forward, future research should integrate multi-database evidence, strengthen ethical governance, and prioritize hybrid implementation-effectiveness designs. Large-scale, culturally diverse trials and adaptive real-time interventions should be tested to ensure scalability and inclusiveness. For instance, recent trials in Japan (Yokomitsu, K., 2023) 49 demonstrate the feasibility of smartphone-delivered CBT adapted to local contexts, underscoring the importance of cultural tailoring. In sum, the discussion underscores digital mental health as an evolving, ethically grounded research ecosystem—one that must continue advancing methodological rigor, inclusiveness, and responsible innovation to realize its transformative potential.
Conclusion
This study provides a bibliometric overview of digital mental health interventions over the past two decades, demonstrating a steady rise in research productivity, increasing academic influence, and a thematic transition toward AI-driven and personalized approaches. On the basis of these findings, several priorities should guide future work. A primary task is the adoption of cross-database integration, extending analyses beyond Web of Science to Scopus, PubMed, and non-English resources to enhance global representativeness. Equally important is the rigorous validation of digital interventions through large-scale, longitudinal randomized controlled trials that assess real-world effectiveness, scalability, and acceptability. Another essential direction is the establishment of internationally recognized ethical and regulatory frameworks, particularly concerning privacy, data ownership, and algorithmic transparency, to ensure responsible AI deployment. Finally, translating research evidence into health policy and practice is critical for improving accessibility, equity, and sustainability. These priorities collectively provide a roadmap for advancing digital mental health research and practice globally.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076251403203 - Supplemental material for Trends in digital mental health interventions: A 20-year bibliometric analysis
Supplemental material, sj-docx-1-dhj-10.1177_20552076251403203 for Trends in digital mental health interventions: A 20-year bibliometric analysis by Boxiang Zhang, Lucy Yue Lau and Yi Chen in DIGITAL HEALTH
Supplemental Material
sj-pdf-2-dhj-10.1177_20552076251403203 - Supplemental material for Trends in digital mental health interventions: A 20-year bibliometric analysis
Supplemental material, sj-pdf-2-dhj-10.1177_20552076251403203 for Trends in digital mental health interventions: A 20-year bibliometric analysis by Boxiang Zhang, Lucy Yue Lau and Yi Chen in DIGITAL HEALTH
Footnotes
Acknowledgement
The authors thank VOS viewer, CiteSpace, Scimago Graphica, and R-bibliometrix techniques for their support.
Ethical approval
As this study is a bibliometric analysis based on previously published data, no human participants, animals, or clinical samples were directly involved. Therefore, ethical approval was not required.
Consent to participate
Not applicable. This study did not involve human participants or patient data.
Consent to publish
All authors have read and approved the final version of the manuscript and consent to its publication in this journal.
Author contributions
Boxiang Zhang: conceptualization, data curation, formal analysis, investigation, methodology, software, writing – original draft; Lucy Yue Lau: conceptualization, data curation, methodology, software; Yi Chen: conceptualization, data curation, formal analysis, methodology, software, supervision, visualization, writing – review & editing.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
All data generated or analyzed during this study are included in this published article and its supplemental information files. The raw dataset used for bibliometric analysis (Bibliometrix-Export-File.xlsx), which contains the list of included articles and relevant metadata, is provided as a supplemental file to enhance transparency and replicability.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.