
Abstract
Despite the impact and prevalence of maternal mental illness, access to evidence-based treatment remains limited. This article examines the feasibility, acceptability, and usability of a 12-session cognitive behavioral therapy-based mobile intervention tailored to pregnant and postpartum individuals, Maya Perinatal Skills Program (Maya PSP), based on responses from three English-speaking perinatal individuals over age 18 who participated in an open pilot trial between 8 May 2024 and 14 January 2025. Participant feedback suggests that the program is an easy to use platform for accessing evidence-based coping skills. Recommendations for improving future iterations of the app are discussed. This research underscores the potential of digital interventions to expand access to maternal mental health resources, addressing unmet needs in a scalable, user-centered manner.
Keywords
An app-based perinatal cognitive behavioral skills program: a case series
In the last several years, there has been a growing maternal health crisis, with mental health conditions ranking among the top causes of preventable pregnancy-related deaths.1,2 Despite the rising prevalence of psychological disorders during the perinatal period and the potential adverse consequences of untreated maternal mental illness,3–6 access to evidence-based treatment remains limited. There are numerous barriers to care, including stigma and prohibitive costs, and they tend to be especially prominent within low to middle income communities.7,8 These roadblocks are exacerbated by a shortage of mental health providers, particularly in underserved areas.9,10
Cognitive behavioral therapy (CBT) has a strong evidence-base as an effective treatment for depression and anxiety in both prenatal11,12 and postpartum populations.13,14 While telehealth-delivered CBT has shown comparable effectiveness to in-person therapy, the efficacy of app-based CBT requires further research.15,16 App-based CBT may increase the availability of evidence-based tools, particularly for individuals with limited access to care17,15 and thus warrants further research.
Preliminary data suggests that perinatal individuals are open to using mental health-related apps 18 and that such apps may reduce anxiety and stress during pregnancy. 19 However, many of the currently available perinatal mental health apps were not developed with input from mental health professionals and offer minimal evidence-based coping tools. 19 There is thus a pressing need for dependable, expert-informed, research-backed perinatal mental health apps that comprehensively address the varied needs of this population.20,18 This case series evaluates the feasibility, acceptability, and usability of the Maya Perinatal Skills Program (Maya PSP), an app that teaches evidence-based strategies to manage mood and anxiety symptoms during and after pregnancy, among several pilot participants.
Methods
Maya perinatal skills intervention
Maya PSP was created within Maya CBT (M-CBT), an umbrella CBT skills app that has demonstrated significant reductions in anxiety and depression among young adults. 21 Maya PSP is a 12-session adaptation of M-CBT for pregnant and postpartum populations. It was developed by a team of clinical psychologists and reproductive psychiatrists who used their expertise in CBT and perinatal mental health to create the specialized skill modules that demonstrate how to apply evidence-based skills to the perinatal experience. The app interface begins with a welcome screen that introduces users to the program and initiates navigation, as shown in Figure 1. Throughout program development, pediatric primary care physicians, mental health clinicians, and obstetricians were consulted to provide additional insight into the unique needs of perinatal individuals.

Screenshot of the Maya PSP welcome screen, which introduces users to the app and initiates program navigation.
Participants self-navigate through the 12 sessions, each consisting of three main sections: Learn (psychoeducation about specific skills), Practice (opportunities to practice skills), and Review (summary of skills). Skills-based exercises are delivered in interactive formats, as shown in Figure 2. Sessions include instructive text, videos, and activities to reinforce skill use, as illustrated in Figure 3. While it does not mirror a specific manual, the program integrates widely used evidence-based practices found in standard CBT treatments such as functional assessment, cognitive restructuring, behavioral activation and exposure strategies, problem solving, relaxation techniques, distress tolerance, and assertiveness skills. A full list of session content is provided in Table 1.

Skills-based exercise page where users practice CBT techniques tailored to perinatal experiences. CBT: cognitive behavioral therapy.

Sample session pages showing integrated multimedia content and guided skill instruction.
Session content.

Participants can also customize their experience by tracking their mood and anxiety symptoms within the app, applying skills to personal examples, planning between-session practice, and choosing which exercises to try. Progress is further supported through a goals page that allows participants to track objectives and monitor improvements, as shown in Figure 4.

Goals page allowing users to track personal objectives and measure progress through the app.
Procedure
Participants are recruited from a large healthcare system in a major metropolitan area through listservs, clinician information sessions, and flyers. Individuals who were interested in participating, or their providers, provided their contact information via a HIPAA-compliant survey platform. These individuals then completed an eligibility screen with a study staff member via Zoom. Participants must be 18 years or older, pregnant or up to 12 months postpartum, score from 8 to 16 on the Edinburgh Postnatal Depression Scale or 5–14 on the General Anxiety Disorder-7, be able to read and speak English, and have access to an iOs-based smartphone or mobile device with regular internet access. Participants or their child must also be a patient at one of several medical practices within the associated health system. Participants are excluded if they present with current substance use disorder, current symptoms of psychosis or mania, a history of bipolar or psychotic disorder, or safety concerns at the time of enrollment, including suicidal ideation within the last year.
This manuscript presents qualitative feedback from three early participants enrolled in a larger ongoing 3-year pilot trial. These participants were selected as a convenience sample to provide preliminary insights into participant experience, engagement, and acceptability prior to completion of the full trial. They were enrolled over a 3-month period and each completed all 12 sessions of the program.
Eligible participants received further details about study participation, provided informed consent, and completed several initial questionnaires. They then downloaded and were oriented to the app. Participants were asked to complete two sessions per week and were recommended to use the app for 10 min per day, 4 days per week. Within a week of intake, study staff conducted a brief phone check-in to ensure participants had been able to utilize the app and answer any questions.
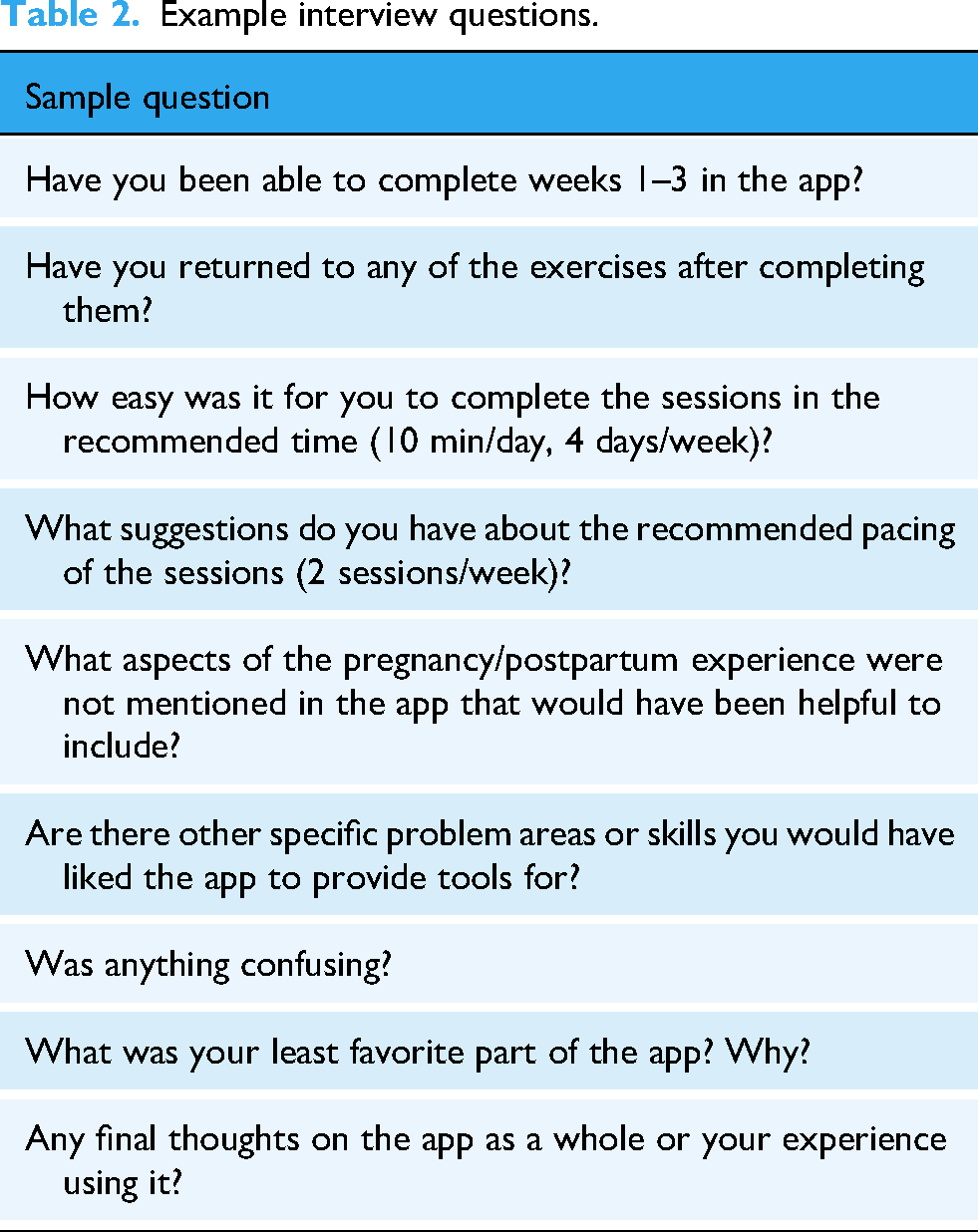
Assessments were completed at three time points throughout the study, occurring at Midpoint (following completion of session six), Post (following completion of session 12), and Follow-Up (six weeks after Post). These assessments were conducted via Zoom and included staff-led, semi-structured qualitative feedback interviews. Questions garnered participants’ feedback on timing and pacing for completing the program, session content, ways to improve the program, any topics that were not included in the program that would be helpful, and general feedback about the program. Kindly refer to Table 2.
Example interview questions.
The collected, transcribed qualitative feedback interviews were analyzed by the research team using thematic analysis. Each member independently reviewed the transcripts to identify recurring themes, which were then collaboratively coded into three primary categories: feasibility, accessibility, and usability. The coded findings were incorporated into the case series, with participants’ direct quotes included to illustrate key points and accurately represent their perspectives.
In addition to qualitative interviews, participants completed the User Version of the Mobile App Rating Scale (uMARS) at Midpoint, Post, and Follow-Up to quantitatively assess usability and acceptability. The uMARS is a validated measure that evaluates mobile health apps across domains such as engagement, functionality, esthetics, and information quality.
Case series
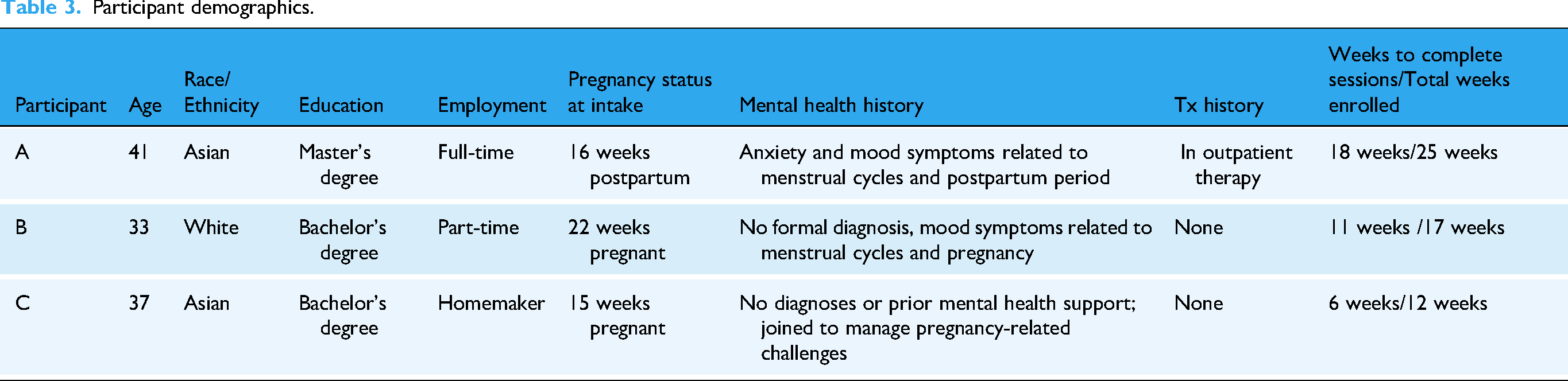
Table 3 summarizes the three participants’ demographics, mental health history, and intervention timelines. The average age of these participants was 37 years, and all were married and living with their spouses.
Participant demographics.
Qualitative feedback from these three participants is presented below.
Acceptability
Participants found the cognitive restructuring tools particularly helpful. Participant A shared that the “thoughts exercise helped me to process what I was thinking and how to reframe those thoughts more practically.” Similarly, Participant B highlighted the value of the thinking traps section, noting it “showed me how to evaluate whether my thoughts were grounded in reality or just in my imagination,” which helped her feel more in control. Participant C also returned frequently to the cognitive strategies, describing them as “practical and effective.”
Relaxation tools were especially appreciated by Participants B and C. Participant B reported that muscle relaxation “helped [her] consciously relax” and suggested expanding the relaxation component. Participant C, initially skeptical of mindfulness, found the program's approach “surprisingly helpful,” particularly muscle relaxation for stress management.
Participants also emphasized areas for improvement. A noted that reflection prompts would benefit from a higher word limit, explaining, “I think increasing the word count would allow for more thorough reflections.” She also requested more targeted content related to “parenting multiple children, returning to work, and collaborating with childcare providers.” Participant C echoed the need for more personalization, suggesting content on “dealing with bodily changes and physical limitations.” She also found that “the [between-session] homework felt a bit redundant and could have been combined with the sessions.”
The uMARS information subscale received a mean score of 4.4/5 across participants and timepoints, suggesting that users found the app's content accurate, helpful, and relatively well-tailored to the perinatal population.
Feasibility
The app fit well into the daily routines of all participants. A found “the pacing and session lengths very reasonable,” often completing them in less than the recommended time frame. She acknowledged, however, that “it worked well for me because I was three months postpartum, but I can see it being harder for someone who's earlier on.”
Participant B appreciated the flexibility to engage while multitasking: “I liked that I could do some of the sessions on the subway, so I didn’t have to dedicate specific time for it.” Still, she had mixed feelings about the pacing: “I wanted to have access to more sessions when I had time, but on the other hand, the regular pacing helped me build a consistent routine.”
Participant C also described the structure as compatible with her schedule, completing sessions during “small gaps in [her] day, such as over breakfast or on the subway.” However, she expressed a desire for more autonomy, saying she “would have liked more flexibility to move through the content at my own pace,” and proposed a “choose-your-own-adventure” format to enhance responsiveness to user needs.
Usability
The app was consistently described as user-friendly and well-organized. A found the layout intuitive but criticized the task list: “The task list could be a bit frustrating since I had to go back and re-rate items, which was time-consuming.” Participant B noted that while she appreciated the simple design, “the typing could be a bit much sometimes,” and suggested additional input methods like tapping or multiple choice. Participant C praised the ease of navigation and recommended adding in-app notifications to promote engagement.
Usability was also measured quantitatively through the uMARS domains of esthetics, engagement, and functionality. Across all three participants and timepoints, the program was rated as easy to navigate (mean functionality = 4.22/5) and visually appealing (mean esthetics = 4.11/5). Participants reported moderate engagement with the program (mean engagement = 3.70/5).
Overall experience
Participants expressed high overall satisfaction with the program. A reflected, “As a first-time mom, I would have been all over this app because I didn’t get the help I needed back then.” Participant B described the app as “convenient, flexible, and genuinely helpful in keeping me on track,” and recommended the inclusion of “more engaging visuals, such as video characters with more relatable facial features.”
Participant C appreciated how the app “brought together so many great resources into one place,” and described it as “a comprehensive and empowering resource.” While she had suggestions for improving redundancy, personalization, and pacing, she concluded, “This app has a great proof of concept and is much-needed for pregnant women. With a few more tweaks, I think it could be even more valuable.”
Figure 5 displays daily engagement data for each participant. Engagement is defined as accessing at least one session or skill on a given day. Participant A engaged on 21 days, Participant B on 18 days, and Participant C on 14 days. All participants show an initial period of engagement followed by a gap, which corresponds to the weeks following completion of the app, before re-engaging for the follow-up interview. Participant A is unique in demonstrating intermittent engagement after the initial gap, suggesting continued independent use beyond the structured intervention period.

Daily engagement timeline.
Discussion
Perinatal mood and anxiety disorders are a critical yet often overlooked aspect of maternal health, particularly in underserved communities.1,7 Mobile mental health apps offer a promising solution by delivering evidence-based interventions like CBT in accessible and flexible formats. 15 However, the programs in development or currently available have several limitations in terms of scope and rigorous testing. While small, this case series highlights a number of potential unique benefits of Maya PSP. This includes the focus on both depression and anxiety, experiences in both pregnancy and postpartum, a program developed directly by experts in the field and grounded in evidence-based practices. While this pilot is in early stages, there are future plans for more rigorous testing, and feedback from three pilot participants suggests that Maya PSP shows promise as an acceptable, feasible, and usable tool to support perinatal individuals.
The three participants discussed here represent a small subset of a larger ongoing pilot trial. Their feedback helped to flag early concerns and strengths of Maya PSP and informed necessary minor adjustments (for example, to the pacing of sessions). Feedback from the larger pilot trial will be used to guide development of future iterations of the app, with the ultimate plan to conduct an effectiveness trial with a larger, more diverse population. One limitation of the current pilot is the absence of fidelity checks to assess how participants applied CBT techniques within their written or exercise completion. Future phases of the study will include procedures to evaluate skill application and treatment fidelity. Data from these three participants shed light on potential means of improving future iterations of Maya PSP, including changing app content to address common perinatal concerns (e.g. newborn care, returning to work, parenting multiple children) and tailoring sessions to different pregnancy/postpartum stages. Other key recommendations included adding interactive input methods beyond typed responses, streamlining features to reduce time burden, and consolidating homework and exercises.
Conclusion
Feedback suggests that Maya PSP was perceived as both useful and acceptable by participants. The app is worth further study and may represent a potentially effective means of managing anxiety and mood during the perinatal period. Next steps include larger trials with a more diverse population. The feedback highlighted several areas that could further improve the program. One limitation of the current study is a narrow participant pool, with limited diversity in regards to race, education level, marital status, and household income. It is possible acceptability, feasibility, and usability ratings would not generalize across different populations. As digital mental health interventions grow in importance, refining tools like Maya PSP will be crucial to ensuring they meet the needs of diverse perinatal individuals. Future iterations will incorporate participant feedback to offer a more personalized, flexible, and comprehensive experience. Continued research is needed to assess the long-term effectiveness of Maya PSP in reducing perinatal mood and anxiety symptoms across broader populations.
Supplemental Material
sj-pdf-1-dhj-10.1177_20552076251382084 - Supplemental material for A novel app-based cognitive behavioral perinatal skills program: A case series
Supplemental material, sj-pdf-1-dhj-10.1177_20552076251382084 for A novel app-based cognitive behavioral perinatal skills program: A case series by Andrea B Temkin-Yu, Ace Oh, Isabelle E Siegel, Michael X Liu, Meredith J Seewald, Ella Blicker, Aliza Ayaz, Alison D Hermann, Soudebah Givrad, Lara M Baez, Lauren M Osborne, Cori M Green, Maddy M Schier, Avital Falk and Shannon M Bennett in DIGITAL HEALTH
Footnotes
Acknowledgements
The authors would like to thank the participants for their time and thoughtful feedback, as well as the clinical staff and healthcare providers who assisted with recruitment and provided valuable insights during program development. The authors also acknowledge the contributions of the broader research team and institutional partners who supported this project.
Ethical approval
This study was reviewed and approved by the Institutional Review Board of Weill Cornell Medicine. All participants provided informed consent prior to enrollment and participation.
Author contributions
ATY led the study conception and design, development of the intervention, and drafting of the manuscript. AH, SG, and SB made substantial contributions to study conception and design. LB, LO, and CG contributed significantly to the study design. ATY, AO, and IS led data acquisition and drafted portions of the manuscript. EB and ML drafted portions of the manuscript. MS and SZ contributed to the development of the intervention and the design for data acquisition. AF led the development of the original intervention and the conception of the overall app-based programming. All authors reviewed and approved the final manuscript.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Weill Cornell Medicine Ritu Banga Healthcare Disparity Research Award and the Weill Cornell Medicine Children's Health Council. Dr Lara Baez receives funding through the National Institute of Mental Health (NIMH) training grant T32 MH115882.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.