
Abstract
Background
With an aging population and the intensification of digital trends, the relationship between technology readiness and health-related quality of life (HRQoL) among middle-aged and older adults has garnered significant academic attention, although existing research presents inconsistent findings.
Objective
Drawing on conservation of resources theory and social support theory, this study investigates the mechanisms through which technology readiness affects HRQoL, focusing on the serial mediation effects of e-Health literacy and family support.
Methods
A cross-sectional survey was conducted by 489 internet-experienced middle-aged and older adults who completed questionnaires measuring technology readiness, e-Health literacy, family support, and HRQoL. Structural equation modeling was employed to examine the relationships between variables.
Results
The results indicated that technology readiness significantly and positively influenced HRQoL, with a direct effect size of 0.529, and that e-Health literacy partially mediated this relationship. Both e-Health literacy and family support jointly contribute to a serial mediation effect, with a standardized coefficient of 0.081.
Conclusions
These findings suggest that enhancing e-Health literacy and family support can amplify the positive impact of technology readiness on HRQoL. This research provides strategies for improving HRQoL among middle-aged and older adults in the digital era, offering new theoretical perspectives for promoting active aging and equitable access to digital dividends.
Keywords
Introduction
With declining fertility rates and increasing life expectancy, population aging has emerged as one of the most significant global public issues of this century. 1 By 2033, comprise over 20% of the total population. 2 As a result, the health-related quality of life (HRQoL) of older adults has become a central focus of research and policy, due to its predictive value for morbidity and mortality rather than population size alone. At the same time, the global digital transformation has become a pivotal aspect of contemporary development. Rapid advancements in science and technology, including the Internet, e-commerce, and telemedicine, are profoundly reshaping people's lives. For middle-aged and older adults, Internet safety and equitable access to digital resources have emerged as pressing concerns. 3 Evidence shows that technology adoption varies by age 4 and education level, 5 which strongly influences health and HRQoL.6,7 This digital divide represents a substantial barrier to ensuring equal sharing of the benefits of social development.
Existing studies indicate that higher levels of acceptance and utilization of new technologies, such as the Internet use, are positively related to quality of life in older adults. 8 Technology readiness, in particular, plays a vital role in facilitating telemedicine, promoting independence, 9 reducing loneliness, 10 and fostering social participation and support. 11 However, rapid technological progress has also widened internal disparities, as benefits concentrate among those with higher education and stronger family support.12,13 This highlights the importance of technology readiness as a determinant of HRQoL in the digital era.
Guided by the conservation of resources (COR) theory, technology readiness is conceptualized as an energy resource that enables older adults to access health information and digital services. Prior studies show that Internet use increases health awareness and reduces anxiety, thereby mitigating inequalities. 12 Nonetheless, empirical studies on technology readiness remain limited, and findings on its association with HRQoL are inconsistent, with both positive and negative results reported.12,14 This inconsistency underscores the need for an integrated framework combining technology readiness, e-Health literacy, and family support.
Emerging evidence suggests that this divergence may partly stem from differences in e-Health literacy. Older adults frequently use the Internet to search for disease prevention and healthy lifestyle information, but their ability to identify, evaluate, and apply such information depends heavily on their e-Health literacy.15–17 High e-Health literacy does not always correspond to better outcomes, while low levels may exacerbate health inequalities.18,19 Inadequate e-Health literacy has been recognized as a critical driver of inequities in the digital era.
According to social support theory, in family-oriented Chinese communities, older adults often experience disruption in their previous social interactions. This disruption reduces communication with the wider community, making spouses and family members increasingly important sources of support. Family support not only facilitates the use of new technologies but also strengthens the application of health information obtained online. Some studies suggest that technological readiness has a stronger positive effect on well-being in old age under conditions of strong family and social support. 20 Conversely, older adults lacking family support may experience lower well-being, underscoring the critical role of family support in shaping the benefits of technology. However, family factors have received insufficient attention in prior research. To better understand the relationship between technology readiness, e-health literacy, and HRQoL, this study incorporates family support as an additional variable. Specifically, it investigates whether family support mediates the relationship between technological readiness and HRQoL in older adults.
Existing studies have examined the relationship between technology readiness and HRQoL among older adults, but findings remain inconclusive. Moreover, critical factors such as e-health literacy and family support have not been a sufficiently considered. Therefore, this study aims to establish a unified model that integrates technology readiness, e-Health literacy, family support, and HRQoL in older adults. We seek to investigate the impact of the digital era on HRQoL while validating and extending the conservation of resources theory and social support theory. Guided by these theories, this research explores the relationship between technology readiness and HRQoL, examining the mediating roles of e-Health literacy and family support. The study draws on survey data from middle-aged and older adults in Wuxi, Jiangsu Province, to validate and extend these theoretical models. This approach complements and extends the current theoretical framework, establishing a comprehensive model to improve HRQoL among older adults in the digital era. The findings are intended to provide evidence-based insights into how digital technologies can enhance HRQoL, reduce health inequities, and promote active and healthy aging.
Literature review and hypotheses
Technology readiness and HRQoL
Technology readiness is often regarded as the attitude and acceptance of individuals and organizations towards specific technologies. It encompasses four dimensions: Optimism, Innovation, Discomfort, and Risk. These dimensions reflect individuals’ perceptions and expectations regarding technology, making them a significant area of research related to technology readiness. The social construct theory has profoundly influenced the study of technology acceptance. Research by Ren and Liu (2003) demonstrates that social factors are closely linked to technology. 21 Davis (1996) developed the Technology Acceptance Model (TAM) to assess users’ acceptance of information technology, emphasizing perceived usefulness and perceived ease of use as its two core constructs. 22 This model demonstrates that both factors positively shape individuals’ evaluations of technology. Subsequent studies confirmed their influence on technology training and acceptance among urban employees. 23 Later extensions, such as those by Bansah and Agyei (2022), introduced additional dimensions (e.g., perceived convenience, perceived effectiveness, user acceptance) to adapt TAM to contemporary digital contexts, 24 but perceived usefulness has always remained a central construct of TAM rather than a new addition. The quality of life in old age encompasses multiple dimensions, including physiological, psychological, social participation, and identity, often used to describe well-being, satisfaction, or perceived value among the elderly.
Research in the field of sociology has elucidated the relationship between technological readiness and quality of life. Mayer-Foulkes et al. (2021), in a study on socio-technical capacity, posits that enhancing the technological capacity of disadvantaged groups is crucial for achieving health and social development. 25 Empirical evidence indicates that the use of Information and Communication Technologies (ICTs) can significantly enhance social participation and mitigate loneliness among older adults, thereby improving their mental health and overall quality of life. 26 Wang et al. (2025) contend that the adoption of smart home technologies by older individuals can promote their independence and safety, leading to an improved quality of life. 27 Khan et al. (2022) investigated the willingness of older adults in developing economies to utilize electronic devices for accessing healthcare services. 28 Their findings reveal that perceived ubiquity and trust—key indicators of technological readiness—are significantly and positively correlated with the willingness to use such devices. In summary, technological readiness is closely linked to HRQoL among middle-aged and older adults, with numerous studies demonstrating its potential to enhance this aspect of well-being.
Accordingly, we propose Hypothesis 1 (H1): Technology readiness is positively associated with HRQoL. Specifically, middle-aged and older adults with higher technology readiness and usage tend to experience improved quality of life.
Potential mediating role of e-Health literacy
E-health literacy refers to an individual's ability to search for, assess, and apply e-health information. It encompasses various aspects, including the collection of health information, the evaluation of its credibility, and the practical application of the acquired e-health information. 29 This concept represents a comprehensive assessment of an individual's access to and utilization of e-health information.
Based on the literature review, we identified a significant correlation between technology readiness and e-health literacy, with higher levels of technology readiness contributing positively to e-health literacy. Research indicates that factors such as optimism, innovativeness, and discomfort significantly influence patients’ e-health literacy, positioning technology readiness as a crucial determinant of e-health literacy. 30 In a survey of older adults, Terp et al. (2021) concluded that while most older adults exhibit readiness for electronic information technology (e-IT), lower levels of technology readiness impede their utilization of health technology. 31 Furthermore, when considering various ethnic groups, the study revealed that the older adults surveyed demonstrated a limited propensity to engage with e-health-related facilities and information. 32 This highlights the need to address the digital divide in e-health literacy.
There is a significant positive impact of e-health literacy on HRQoL. A local study in China conducted by Liu et al. (2021) found that e-health literacy can enhance life satisfaction among older adults. 33 Several studies indicate that older adults with high e-health literacy are better equipped to utilize e-health information for effective personal health management, thereby improving their quality of life. 34 Furthermore, e-health literacy influences health promotion behaviors among older adults, with self-efficacy and self-care abilities acting as mediators. Specifically, e-health literacy enhances health promotion behaviors among older adults through improved self-efficacy and self-care abilities. 35 These studies demonstrate that technology readiness, e-health literacy, and quality of life in older age are interrelated, establishing a basis for mediation. More importantly, research indicates that e-health literacy mediates the relationship between healthy personality traits and quality of life among older adults, 36 as well as the serial between depression and HRQoL in older adults with chronic diseases. 37 Collectively, these findings suggest that e-health literacy not only directly impacts quality of life but also serves as a mediating variable that influences the effects of technological readiness on HRQoL.
Thus, we propose Hypothesis 2a (H2a): E-Health literacy mediates the relationship between technology readiness and HRQoL.
Potential serial mediation of e-Health literacy and family support
Family support encompasses multiple dimensions, including material, emotional, and instrumental assistance among family members. 38 Shaped by traditional cultural values, the family has long been a primary source of support and companionship for middle-aged and older adults in China, playing a pivotal role in enhancing health-related quality of life (HRQoL). Prior studies have shown that family guidance can improve e-health literacy among older adults, 39 and that family support s significantly predicts e-Health literacy in this demographic. 40 Moreover, older individuals with higher levels of family support tend to demonstrate better e-health literacy. Evidence from a large-scale survey in Guangdong Province revealed that family support positively affects physical, psychological, and social dimensions of older adults’ quality of life, underscoring its broad influence. 41 Related research has also indicated that social connectedness behaviors, such as interactions with family and friends, can mediate the effects of short video use on the well-being of middle-aged and older adults. 42 Furthermore, studies on elderly patients with hypertension suggest that family support may function as a mediator rather than a direct determinant of health-related behaviors, 43 highlighting its close association with family functioning, health, and well-being.
Despite these findings, existing research provides only a partial understanding of the mechanisms through which family support operates. Many studies conflate family support with broader social support, failing to disentangle it from contextual influences such as national policies and community services. This limits a precise examination of the unique role of family members, who remain the most immediate and consistent caregivers for older adults. At the same time, technology readiness has been shown to shape older adults’ HRQoL through the adoption of new technologies, 26 while e-health literacy enhances health outcomes and well-being. 34 Family support facilitates this process by enabling access to health information and validating its reliability. Together, family support, technology readiness, and e-health literacy influence HRQoL through distinct yet interrelated pathways.
Grounded in social support theory and empirical evidence, we argue that family support may independently mediate the relationship between technology readiness and HRQoL. Older adults with higher levels of technology readiness are more likely to adopt and actively use digital devices; when supported by strong family encouragement, instrumental assistance, and guidance in applying health information, this readiness can be translated into measurable improvements in HRQoL. Conversely, insufficient family support may constrain the transformation of technology readiness into tangible health benefits.
Thus, we propose Hypothesis 2b (H2b): Family support mediates the relationship between technology readiness and HRQoL.
Importantly, empirical findings suggest that these relationships are not simply juxtaposed but are intricately interwoven through their roles in technology adoption and use44. While e-health literacy and family support have each been identified as mediators of the impact of technology readiness on HRQoL, prior studies have rarely integrated these variables into a unified framework. In particular, the potential serial mediating effects of e-health literacy and family support remain untested, and no comprehensive theoretical model has been established. Therefore, this study seeks to advance understanding by examining the mediating and serial mediating roles of e-health literacy and family support in the relationship between technology readiness and HRQoL, with the aim of developing an integrative mechanism model.
Accordingly, we propose Hypothesis 3 (H3): e-Health literacy and family support jointly serve as serial mediators in the relationship between technology readiness and HRQoL.
Methods
Study design
The analysis of this cross-sectional study is based on data collected from a school-local cooperation project entitled ‘Healthy Living Practices of Community Residents and the Construction of Healthy Communities.’ The project's objective was to investigate the health status, health behaviors, attitudes, and e-health literacy of community residents in the digital era, as well as the status of digital health infrastructure and services within the community. Prior to the formal survey, a pilot study was conducted among 80 participants, who were not included in the subsequent main investigation. The pilot procedure consisted of six steps: selecting the survey instruments, expert review for content validity, obtaining ethics committee approval, recruiting participants, conducting the pre-test, and evaluating the results. After confirming that all instruments demonstrated satisfactory reliability and validity and that all questionnaire items were easily understood, the formal survey was initiated.
The main survey was carried out in Wuxi City, Jiangsu Province, from January to May 2024, covering 21 communities (13 urban and 8 rural). The inclusion criteria were: (1) adults aged 18 years or older; (2) ability to complete the questionnaire independently; and (3) prior experience with Internet use. Quota sampling was employed to ensure representation across key demographic groups. Data were collected through face-to-face interviews with structured questionnaires. All investigators had relevant field experience and disciplinary training and received standardized instruction to ensure adherence to established procedures for distributing and retrieving questionnaires. The study protocol was reviewed and classified as exempt by the Medical Ethics Committee of Jiangnan University. All participants were informed of the study objectives and provided written informed consent prior to data collection.
Participants
A total of 2200 questionnaires were distributed, and 2130 were returned, resulting in a response rate of 96.81%. To ensure the validity of data collection, two criteria were applied: (1) the questionnaire had to be fully completed without missing responses; and (2) respondents were required to avoid deliberately providing repetitive or false answers. After excluding 256 invalid questionnaires that did not meet these criteria, 1874 valid responses were obtained. Among these, 489 middle-aged and older adults aged 45 years and above were included in the present study. The mean age of participants was 58.4 years (SD = 8.42), with 59.9% male and 40.1% female. Additional socio-demographic characteristics are presented in Appendix Table 1.
Measurement
Health-related quality of life (HRQoL)
The Physical and Mental Summary Scale, developed by Ware (1996), 44 served as a reference for designing a comprehensive assessment scale of HRQoL in middle-aged and older adults. This scale comprises 12 items categorized into two dimensions (KMO = .904, p < .000): physical health and mental health. Respondents rated each item using a unified 6-point Likert scale ranging from 1 (not matching at all) to 6 (indicating a perfect match), with higher scores reflecting better HRQoL. The overall reliability of the scale, indicated by Cronbach's α = 0.725, is considered good.
Technology readiness
The technology readiness of middle-aged and older adults was comprehensively assessed using the Index of Technology Readiness scale developed by Parasuraman (2000). 45 The scale includes 12 items across four dimensions (KMO = .82, p < .000): optimism, innovativeness, discomfort, and insecurity. All items were rated on the 6-point Likert scale described above. The overall reliability of the scale was assessed using Cronbach's α, which yielded a value of 0.766, indicating good reliability.
e-Health literacy
The e-Health literacy measure utilized the Digital Health Literacy Assessment Scale developed by Liu (2022). 46 This scale was adapted to include 15 questionnaire items categorized into two dimensions (KMO = .931, p < .000): access and assessment and interaction and application. Responses followed the 6-point Likert scale, with higher scores indicating greater eHealth literacy. The overall reliability of the scale was assessed using Cronbach's α, which yielded a value of 0.914, indicating good reliability and validity.
Family support
The level of family support was assessed using a single-item question, phrased as “What extent do you receive emotional support, informational support, and instrumental support” Respondents were recorded on the unified 6-point Likert scale, with higher scores reflecting stronger support.
The detailed on all measurement tools (HRQoL, technology readiness, e-Health literacy and family support) are presented in Appendix Table 3, including items, anchors, and scoring rules.
Statistical analysis
The study was statistically analyzed using SPSS 25.0 and AMOS 25.0 software. Initially, descriptive analyses and correlation tests were conducted using SPSS 25.0. Subsequently, structural equation modeling (SEM) was performed using AMOS 25.0 to examine the serial mediating effects of e-health literacy and family support on the relationship between technology readiness and HRQoL. Our analyses were organized into five steps: (1) Descriptive analyses were conducted to identify the sociodemographic characteristics of the respondents. (2) Exploratory factor analysis and confirmatory factor analysis were employed to ascertain the structural validity of the data. (3) Reliability tests were conducted through reliability analysis. (4) Correlation analysis was performed to explore the relationships among the primary variables. (5) SEM was utilized to analyze the relationship between technology readiness (independent variable) and HRQoL (dependent variable), and to evaluate the serial mediation effects of e-health literacy and family support.
Results
Descriptive statistics and normality of key variables
The model for the current study included one observed variable, family support, and three latent variables: technology readiness, e-health literacy, and HRQoL. The results of the factor analysis indicated that HRQoL comprised two subfactors: physical health and mental health. Technology readiness was found to include four factors: optimism, innovativeness, discomfort, and insecurity. Additionally, e-health literacy consisted of two factors: access and assessment, interaction and application. The analysis results demonstrated that the absolute values of skewness were less than 2 and kurtosis was less than 3 for all key variables (see Table 1), confirming a normal distribution. 47
Descriptive analysis of the main variables.

+ The mean score on scale items.
Respondents indicated that while they engage in browsing online health information and utilizing digital health products, they often lack the ability to critically evaluate this information. Additionally, the participants showed a good level of family support. Furthermore, the factors related to technology readiness were found to have a positive correlation with both physical and mental health status, all of which were statistically significant, as detailed in Appendix Table 2.
Mediation analysis with structural equation modeling
This study examined the mediating effects of e-Health literacy and family support between technology readiness and the quality of healthy life using structural equation modeling. The results of the analysis are presented in Table 2. The model fit indices were acceptable (χ²/df = 2.11, CFI = .92, TLI = .91, RMSEA = .082, SRMR = .045). Although the RMSEA value slightly exceeds .08, prior research considers values up to .10 as acceptable.48,49 Given the satisfactory performance of other indices and the strong theoretical basis of our model, the overall fit was deemed adequate.
Results of the multiple mediation model analysis.
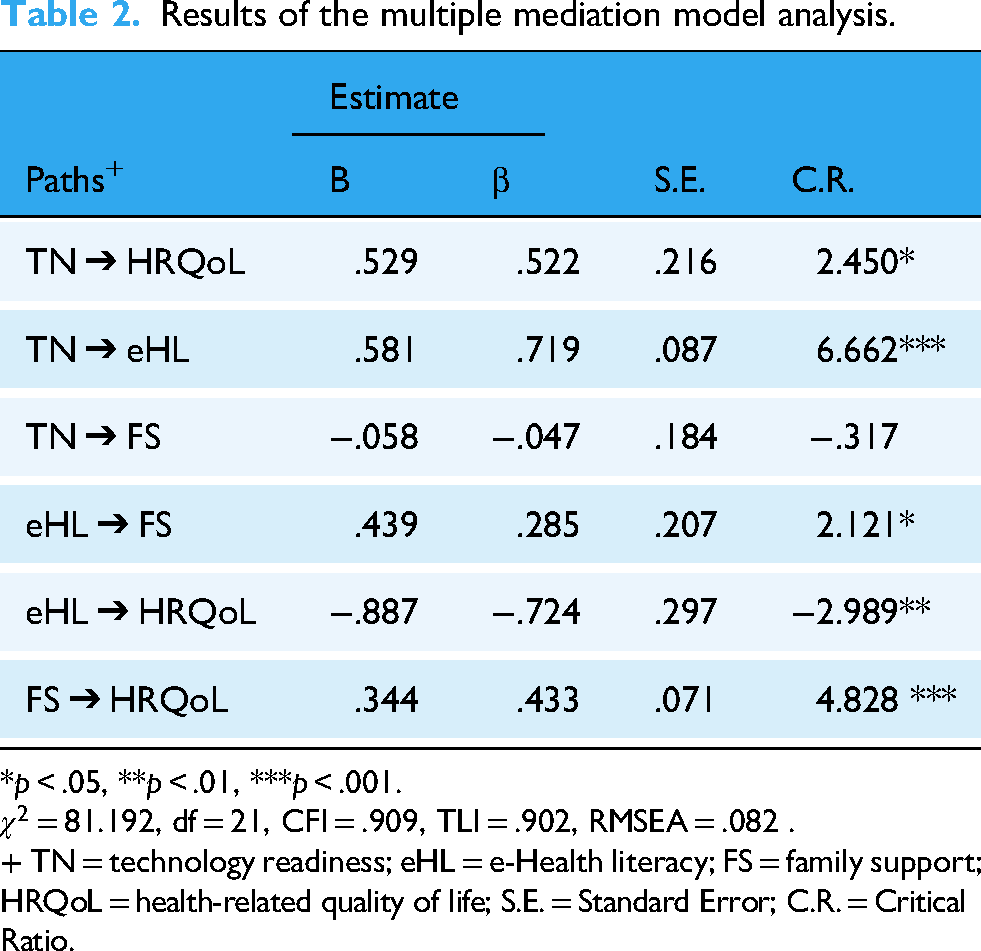
*p < .05, **p < .01, ***p < .001.
+ TN = technology readiness; eHL = e-Health literacy; FS = family support; HRQoL = health-related quality of life; S.E. = Standard Error; C.R. = Critical Ratio.
The path coefficient from technology readiness to the quality of healthy life was statistically significant (C.R. = 2.450, p < .05). Additionally, the path coefficient from technology readiness to e-Health literacy was significant (C.R. = 6.662, p < .001). The path coefficient from e-Health literacy to the quality of healthy life was also significant (C.R. = −2.989, p < .01), as was the path coefficient from e-Health literacy to family support (C.R. = 2.121, p < .05). Furthermore, the path coefficient from family support to the quality of healthy life was significant (C.R. = 4.828, p < .001). However, the path coefficient from technology readiness to family support was not significant (see Figure 1).
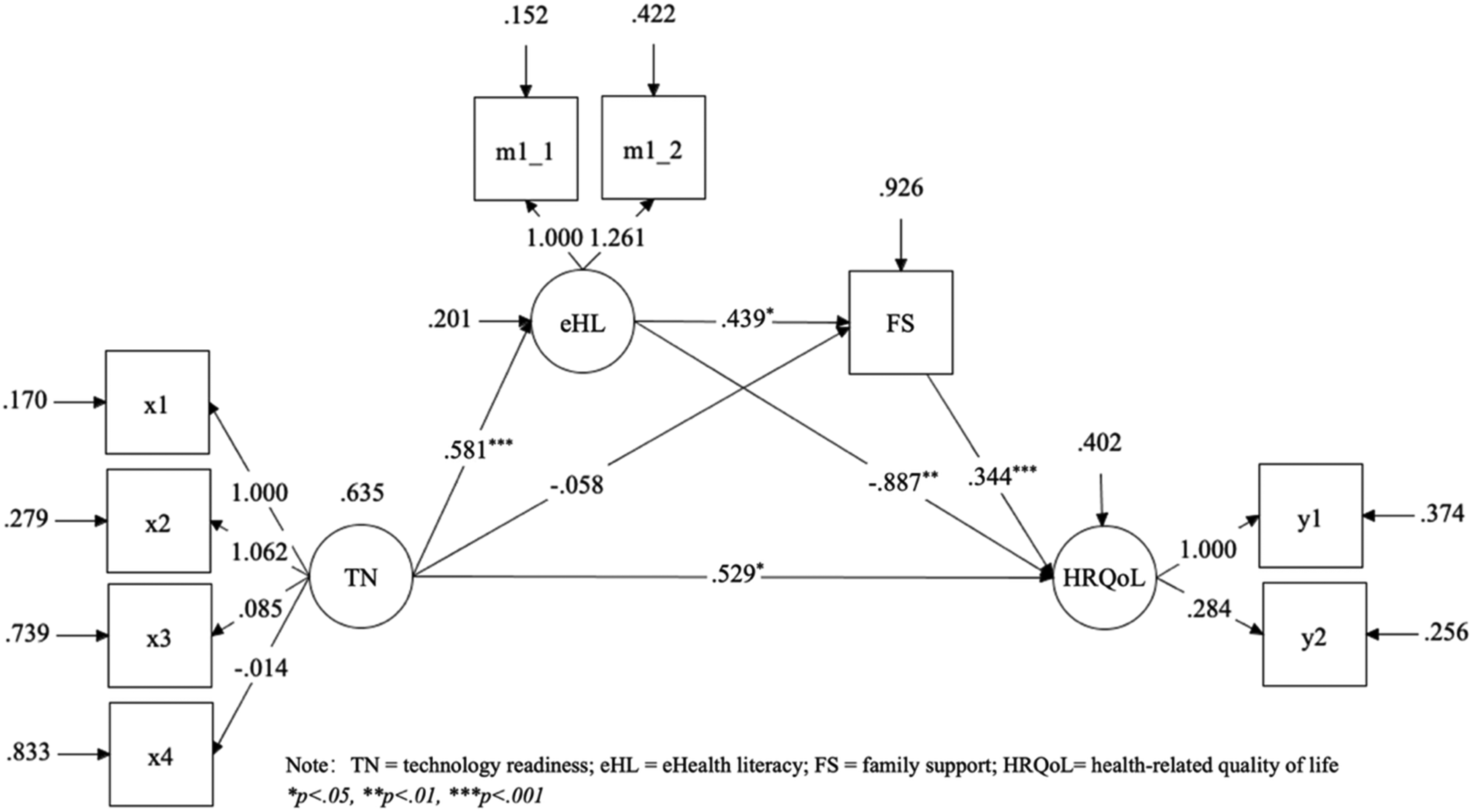
Path coefficients of the multiple mediation model.
In this study, the Bootstrap method was employed to examine the mediating roles of e-Health literacy and family support. The results, presented in Table 3, indicate that e-Health literacy and family support significantly mediate the relationship between technology readiness and HRQoL (95% CI = 0.208 to 0.940). The total effect size is 0.081, comprising a direct effect size of 0.529 and an indirect effect size of −0.448. eHealth literacy demonstrated a significant indirect mediating effect of −0.515 (95% CI = −0.902 to −0.214). Family support exhibited a mediating effect size of −0.020 (95% CI = −0.155 to 0.059). Furthermore, the effect size of the serial mediation involving eHealth literacy and family support was 0.081 (95% CI = 0.021 to 0.219).
Results of the multiple mediation effect test.

TN = technology readiness; eHL = e-Health literacy; FS = family support; HRQoL = health-related quality of life; CI = Confidence Interval.
Discussion
The current study investigates the impact of technology readiness on the health-related quality of life (HRQoL) of middle-aged and older adults, mediated by eHealth literacy and family support. The first finding reveals a significant positive effect of technology readiness on HRQoL, thereby supporting H1. This finding aligns with prior evidence showing that technology readiness enhances the physical and mental health of older adults by facilitating access to telemedicine, increasing opportunities for health information acquisition, and alleviating feelings of loneliness. Previous studies have demonstrated that the duration of Internet usage positively impacts the health literacy of the elderly. 50 From a practical perspective, strategies such as structured programs to gradually increase Internet usage among older adults, the design of tailored digital engagement plans, and providing guidance for the adoption and independent use of digital devices may further enhance the positive effects of technology readiness on HRQoL.
However, Hypothesis 2, which posited the mediating roles of eHealth literacy and family support, received only partial support. On one hand, the finding indicated that the mediating effect of eHealth literacy was statistically significant, supporting H2a. Notably, the path from eHealth literacy to HRQoL was negative (β = −0.724, p < 0.01), indicating a significant negative direct association between eHealth literacy and HRQoL when controlling for technology readiness and family support. This counterintuitive result may arise from problem-driven health information seeking, as older adults with poorer health are more likely to search for and focus on health information,48,51 leading to an observed coexistence with lower HRQoL in cross-sectional data. It may also reflect a mismatch between evaluative capacity and available resources, where information overload and cyberchondria undermine well-being. In such cases, older adults may be capable of identifying and assessing health information but lack the social or service support needed to translate it into effective care. 52
On the other hand, the study found that mediating effect of family support was weak and not statistically significant, leading to the rejection of H2b. This finding suggests that, although family support is theoretically important, its independent role in transforming digital readiness into improved HRQoL appears limited—particularly given that family support was measured with a single-item indicator in this study. This implies that interventions should not rely solely on family support but must integrate community-level resources, professional guidance, and public service programs to reduce disparities in access to the benefits of digital health. Such integration is especially critical for socially disadvantaged groups, including older adults without local ‘Hukou’, who face structural barriers to equitable health services.
Nevertheless, the findings supported H3, which asserts that eHealth literacy and family support jointly exert serial mediating effects in the relationship between technology readiness and health-related quality of life (HRQoL). Specifically, when older adults with higher technology readiness also demonstrate stronger eHealth literacy and receive adequate family support, their HRQoL can be significantly enhanced. This underscores an important practical implication: effective interventions should integrate both digital and social resources. For instance, designing family-inclusive digital literacy workshops and encouraging intergenerational participation can bolster older adults’ confidence in utilizing health technologies and promote sustainable improvements in HRQoL.
This study develops a comprehensive model that links technology readiness, eHealth literacy, family support, and health-related quality of life (HRQoL) in older adults. The contrast between the partially supported H2 and the supported H1 and H3 reveals an important nuance: technology readiness has a clear direct effect on HRQoL, as well as a significant sequential indirect effect through eHealth literacy and family support. However, its independent indirect effect through family support alone is weak. From a policy perspective, this implies that digital health interventions should be designed to simultaneously enhance individual competencies and family involvement, thereby bridging the digital divide and promoting equitable health outcomes. Previous evidence indicates that lower digital competence is a significant predictor of depressive symptoms 53 and that individuals with lower health literacy are more likely to refuse the use of e-health services, 54 which further reinforces the importance of our findings.
Considering the digital divide exacerbated by global digitalization trends, 55 disparities in digital literacy remain a significant challenge for older populations. Our study demonstrates that the positive impact of technology readiness on health-related quality of life (HRQoL) is amplified by higher levels of eHealth literacy and family support, underscoring the practical importance of integrating digital and social resources into intervention design. Family members play a crucial role in facilitating older adults’ adoption of digital tools, thereby maintaining social connections, enhancing participation, and reducing social isolation. Additionally, it has been suggested that technological readiness can mitigate feelings of loneliness, thereby improving the overall well-being of older adults. 56 Therefore, targeted initiatives should support not only older adults but also their families, enabling joint engagement in digital health practices.
This study acknowledges several limitations. Firstly, the research sample is confined to the Wuxi area of Jiangsu Province, which constrains the generalizability of the findings and the applicability of the recommendations. Future research should aim to broaden the scope by including multiple cities across the country, employing random sampling to select cities and respondents based on indicators such as economic development levels and the average technology acceptance among the elderly, thereby enhancing the general applicability of the conclusions drawn from this study. Secondly, the content focus of this research is predominantly on a single factor related to technology readiness and quality of life in older age, specifically e-health literacy. Other potential factors, such as economic status, educational attainment, Internet usage patterns, and mental health status, have not been explored. Future studies should consider the elderly in relation to their individual circumstances and external conditions, investigating how various characteristics influence their use of electronic devices and access to health information. This approach may yield more nuanced and comprehensive actionable recommendations for enhancing the quality of life among older adults through a thorough examination of related factors. Thirdly, this study employed a single-item measure to assess levels of family support, which may limit its reliability. While we utilized three dimensions (emotional, informational, and instrumental support) to evaluate family support in an effort to enhance measurement reliability, certain limitations in dimensional completeness and measurement precision remain when compared to established scales. Future research should consider incorporating validated multi-dimensional family support scales to provide more reliable evidence for investigating the relationship between family support and health-related quality of life among older adults. Lastly, due to the inherent limitations of cross-sectional studies, the health conditions assessed in this research reflect the respondents’ current health status, making it impossible to establish causal relationships. Consequently, while this study indicates that older adults who are technologically prepared exhibit a higher quality of life, it does not conclusively demonstrate that adequate technology readiness directly contributes to improved quality of life in older age. Future research should use longitudinal surveys to explore the causal relationship between technology readiness and quality of life in old age among older adults.
Conclusion
Technology readiness significantly influences the lives of middle-aged and elderly individuals in the context of the digital era, shaping multiple dimensions of their quality of life, including both physical and mental health. This study concludes that enhancing technology readiness among middle-aged and elderly populations can positively affect their health and well-being. Conversely, inadequate technology readiness hinders the integration of older adults into the digital landscape, leading to challenges in adopting and utilizing digital devices, which ultimately reduces the potential benefits of digital engagement. Furthermore, e-health literacy and family support serve as mediators in the relationship between technology readiness and HRQoL. The effective use of digital health devices, coupled with the ability to access and apply online health information, can strengthen older adults’ self-efficacy, which is essential for achieving favorable health outcomes. Additionally, these factors help to mitigate feelings of loneliness by fostering stronger family support and enhancing communication within families. The study advocates for t initiatives aimed at improving technology readiness among middle-aged and elderly individuals as a critical component of quality-of-life enhancement. It also emphasizes the necessity of integrating e-health literacy and family support into intervention strategies, thereby maximizing the positive impacts of digital health engagement and contributing to the promotion of positive aging and equitable access to the benefits of a digital society.
Supplemental Material
sj-pdf-1-dhj-10.1177_20552076251393411 - Supplemental material for A serial mediation effect of technology readiness on health-related quality of life in middle-aged and older adults: The role of e-Health literacy and family support
Supplemental material, sj-pdf-1-dhj-10.1177_20552076251393411 for A serial mediation effect of technology readiness on health-related quality of life in middle-aged and older adults: The role of e-Health literacy and family support by Dongdong Wang, Zifan Wang and Sheng Sun in DIGITAL HEALTH
Footnotes
Acknowledgements
The authors would like to thank all researchers, participants and others who were involved directly or indirectly during data collection and reviewed this manuscript.
Ethical approval and participant consent statement
This paper was reviewed and considered human subjects exempt by Jiangnan University Medical Ethics Committee. The participants were informed about the purpose of this research and provided written informed consent before administering the questionnaire. To maintain confidentiality, personal identifiers were omitted from the questionnaires and the collected data were stored in a secure, password-protected database without identifiers.
Contributorship
All authors made significant contributions to the conception or design of the study, as well as the processing and interpretation of data. Additionally, all authors participated in the critical review and revision of the manuscript and approved the final version. Furthermore, all authors have agreed to take responsibility for all aspects of the work.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work is supported by General Project of Philosophy and Social Science Research in Colleges and Universities of Jiangsu Province (2022SJYB0950).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Guarantor
SS will serve as the Guarantor for the described research activities.
Supplemental material
Supplemental material for this article is available online.
Appendix
The details of the measuring tool.

| Dimension | Items | Scoring Rules |
|---|---|---|
| Technology readiness | By using digital health products, I can clearly understand my own health status. | 6-point Likert scale; 1 = Completely disagree … 6 = Completely agree; Scale ranged from 1 to 6, with higher scores indicating a better state of technical readiness |
| I am very interested in using digital health products. | ||
| I believe I can operate digital health products with ease. | ||
| I want to purchase digital health products. | ||
| I can use digital health products without assistance from others. | ||
| Among my friends, I am usually the first to try new technologies. | ||
| Many functions of digital health products are not user-friendly. (Decoding) | ||
| The technical terms used in digital health products are difficult to understand. (Decoding) | ||
| Learning to use digital health products requires a lot of time. (Decoding) | ||
| I worry that digital health products may leak my personal information. (Decoding) | ||
| I worry that others may see my health information through digital health products. (Decoding) | ||
| I am uncertain whether the data shown by digital health products are accurate. (Decoding) | ||
| e-Health literacy | I am interested in learning health knowledge or skills online | 6-point Likert scale; 1 = Completely disagree … 6 = Completely agree; Scale ranged from 1 to 6, with higher scores indicating greater levels of e-health literacy. |
| I will check health information pushed to me online | ||
| I will actively search online for health information I need | ||
| I can understand the content of online health information | ||
| I can judge whether online health information is correct | ||
| I will consult others to judge the reliability of online health information | ||
| I can filter out the content I need from online health information | ||
| Even for credible and high-quality online health information, I will carefully consider whether it is applicable to my personal situation | ||
| When searching for and sharing health information online, I will pay attention to protecting my own and others’ privacy | ||
| I can share or comment on health information resources online (e.g., forwarding or commenting on health information in WeChat Moments) | ||
| I can participate in health forums (websites) or online health discussions (e.g., in WeChat groups, QQ groups) | ||
| I can participate in online voting or surveys on health topics | ||
| I can provide doctors with necessary diagnostic information (e.g., symptom description, medical history, health indicators) during online consultations | ||
| I can use functions of health websites or online platforms (e.g., appointment booking, online payment, accessing electronic medical records) | ||
| I can use electronic devices to record and manage personal health indicators (e.g., blood pressure, heart rate, weight) | ||
| Family support | To what extent do you receive emotional support (e.g., sharing happiness and troubles, providing care and support, etc.) from family/relatives. | 6-point Likert scale; 1 = None … 6 =always; Scale ranged from 1 to 6, with higher scores indicating more support from the family. |
| To what extent do you receive informational support (e.g., providing necessary information, giving advice, etc.) from family/relatives. | ||
| To what extent do you receive instrumental support (e.g., financial help, assistance with daily tasks, etc.) from family/relatives. | ||
| HRQoL | Health problems limited vigorous activities (e.g., running, lifting heavy objects) | 6-point Likert scale; 1 = Completely disagree … 6 = Completely agree; The scale's ratings range from 1 to 6, with higher scores reflecting a better HRQoL. |
| Health problems limited moderate activities (e.g., sweeping, moving a table). (Decoding) | ||
| I reduced work time or other daily activities due to health problems. (Decoding) | ||
| I had difficulty completing work or other activities due to health problems. (Decoding) | ||
| Emotional problems (e.g., anxiety, depression, stress) reduced my work time or daily activities. (Decoding) | ||
| I was very satisfied with my social activities and interpersonal relationships (e.g., gatherings with friends or relatives). | ||
| I often experienced physical pain. (Decoding) | ||
| I was generally satisfied with my health status. | ||
| I was usually full of energy. | ||
| I often experienced negative emotions (e.g., depression, anxiety, stress). (Decoding) | ||
| I had good sleep quality. | ||
| Overall, my quality of life during the past month was good. |
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.