
Abstract
Objectives
We aimed to investigate the moderating effect of social support and its subscales on the relationship between social media addiction (SMA) and anxiety symptoms in young Taiwanese adults.
Methods
A cross-sectional study was conducted on young adults in universities across regions in Taiwan. 1324 Taiwanese young adults aged 20–40 participated in this survey. Sociodemographics, health-related behaviors, social media use, perceived social support (including family, friends, and significant others), and anxiety symptoms were assessed. Linear regression models were used to examine the associations and interactions.
Results
Of the sample, 21.4% exhibited SMA symptoms. The mean anxiety symptoms and social support scores were 6.7 ± 5.4 and 61.8 ± 14.2, respectively. SMA was associated with higher anxiety scores (adjusted coefficient [aB] = 2.02, 95% confidence interval (CI) = 1.35, 2.70; p < .001). Social support was associated with lower anxiety scores (aB = −0.06, 95% CI = −0.08, −0.04; p < .001). Among individuals with SMA, higher overall social support (aB = −0.05, 95% CI = −0.10, −0.01; p = .033), family support (aB = −0.14, 95% CI = −0.26 to −0.02; p = .025), and support from significant others (aB = −0.13, 95% CI = −0.25, −0.01; p = .047) were each associated with lower severity of anxiety symptoms. Conclusions: Overall social support, particularly support from family and significant others, is associated with reduced anxiety symptom levels and serves as a moderating factor in mitigating the adverse effects of social media addiction on anxiety symptom severity. Social support plays an important role in protecting young adults’ mental health from social media use.
Keywords
Introduction
Social media has become an integral and influential aspect of modern life. Social media use can impact individuals in several ways: updating and maintaining connections with family and friends, altering everyday behaviors and routines, and influencing emotional states by creating or sustaining positive and negative experiences.1,2 In May 2024, more than 5 billion people were using social media worldwide. 3
While social media use offers many benefits, it has also been described as a double-edged sword with potential health consequences. High-intensity and prolonged social media use over an extended period can lead to excessive preoccupation and compulsion to use social media, a condition known as social media addiction (SMA). 4 A meta-analysis study of 2,123,762 individuals from 64 countries revealed that the global pooled prevalence was 17.42% for SMA. 5 Substantial evidence showed that SMA is associated with a risk of depression, anxiety, poor sleep quality, and suicidality.6–8
Region-specific data highlight the importance of studying SMA in Taiwan. A report on Statista showed Taiwan ranks among the highest in Asia for internet and social media usage, with approximately 19 million users (accounting for 80.2% of the total population) in 2024. 9 Huang et al. (2023) conducted a study on 598 university students in Taiwan, indicating that SMA was closely related to psychological distress, which includes anxiety symptoms. 10 A longitudinal study of university students in Hong Kong and Taiwan also demonstrated a bidirectional relationship, in which anxiety predicted higher social media use and greater social media use exacerbated anxiety. 11
Anxiety disorder is the most common psychiatric disorder, and it affects 30% of people worldwide in their lifetime. 12 The characteristics of anxiety dissorders include excessive, intense, persistent worry or panic, difficulty controlling and interfering with daily activities, and impaired functioning daily. 13 Social media use may exacerbate anxiety symptoms in people with SMA. Their habitual checking creates a sense of urgency to keep up with news or trends from social media. 14 People also tend to compare themselves to others, causing them to feel insufficient and anxious or envy. 15 Besides, young individuals are strongly associated with a high risk of cyberbullying when they are SMA. 16 Furthermore, SMA has been associated with unhealthy lifestyles such as smoking, alcohol use, poor diet, and irregular exercise. 17 People with unhealthy lifestyles are strongly associated with their susceptible of developing anxiety disorders. 18 Excessive social media use can negatively impact young people, increasing their vulnerability to mental health issues through exposure to negative content, altered self-concept, and feeling rejected by others. 19
Social support has been identified as a critical protective factor for maintaining and enhancing an individual's mental health. Social support is a multidimensional concept that refers to the structure (number of relationships) and function (emotion, information, guidance, and practical help) of social networks. 20 Family, lovers, friends, or any group they join are the actual sources of social support.21,22 Perceived social support, a person's subjective perception of available support sources, has a positive impact on mental health rather than received social support (referring to the actual support received). 23 Social support provides resources to alleviate stress and cope with difficulties and challenges, thereby diminishing negative impacts on mental health. 24 Strong evidence highlights that high social support is associated with a low risk of anxiety.25,26 People with SMA often develop compulsive behavior regarding social networks, resulting in reduced interactions in real life, denial of duties or responsibilities, and feeling more alone in the real world.27,28
Although many studies have documented a close association between SMA and anxiety, important gaps remain. Most previous studies in Taiwan have focused mainly on the direct association between SMA and anxiety, with little attention to potential moderating factors. The potential moderating role of social support, especially when considering different sources such as family, friends, and significant others, in the relationship between SMA and anxiety has not been fully explored. Therefore, the present study addresses this gap by answering the following question: “Does social support, including support from family, friends, and significant others, moderate the relationship between social media addiction and anxiety among young adults in Taiwan?.” Specifically, we hypothesized that higher levels of perceived social support, including overall and from family, friends, and significant others, would moderate the association between SMA and anxiety.
Materials and methods
Study design and population
An online cross-sectional study was conducted across Taiwan in young adults aged 20–40 years. This study used data from a larger project on COVID-19 and health literacy conducted among university students in 2021. 29
Inclusive criteria were aged between 20 and 40 years, active university students at the time of data collection, and able to read and complete an online Chinese-language questionnaire. Exclusive criteria included self-reported diagnosis of any mental disorder, severe refractive disorders, and any other reasons hindering participation (e.g., inability to provide informed consent or complete the survey). The recruitment criteria were introduced in the online survey, using a convenience sampling method. Participation was voluntary, and all participants provided electronic informed consent before completing the survey.
For the moderation analysis, we conducted an a priori power analysis using G*Power 3.1 for linear multiple regression (fixed model, R² increase). 30 Parameters were set at f2 = 0.02 (small effect size), α = 0.05, power = 0.80, one tested predictor (interaction term), and a total of 14 predictors. The analysis indicated a minimum required sample size of N = 395. The final sample of 1324 was analyzed.
Data collection procedure
The data collection period spanned from November 2022 to December 2023. We invited a teacher or staff member from universities across Taiwan to help us contact students and general publics via their social networks. These contact people sent out the Google Form link and QR code via the school mailing system, school social media pages, student clubs/associations, and personal social networks/media. The reminder posts/messages/emails were posted/sent out within 1 week and 2 weeks apart. The recruitment criteria were integrated into the online consent form so potential participants could decide whether to join our survey. On the first page, all participants were briefly informed about the research project and asked for their volunteer to join the study before participating. If participants agree to take the survey, they can proceed to the following pages until it is completed. In addition, there were no gifts or incentives for participants; participation was entirely voluntary, and all individuals could freely decide whether to take part or withdraw at any time without consequence, in line with IRB-approved ethical standards. There were no gifts for participants. It takes about 20 min to complete the survey questionnaires. The principal investigator saved/stored all responses on Google Drive with a secure password in Google Sheets. Finally, researchers confidentially coded, cleaned, and analyzed the data, ensuring the highest data integrity and security level.
Measurements
Socio-demographic information
Participants provided about their age (year), gender (men vs women), marital status (single vs ever married), education levels (undergraduate vs graduate), working status (studying/unemployed vs part-time/full-time job), ability to pay for medication (difficult vs easy), living status (with family members, with a partner (cohabiting), with a friend, alone).
Health-related behaviors
Health-related behaviors consist of current smoking status, alcohol consumption, eating behaviors, and physical activity. Participants reported their smoking status: current smoking, used smoked but stopped, and never smoked. They were divided into two groups of current smoking: no vs. yes. Alcohol consumption was defined as when an individual drank at least once per week for over 30 days.
Healthy eating behavior was evaluated using the 5-item healthy eating score (HES-5). 31 This scale was compared with the 2015 Healthy Eating Index to assess overall diet quality. 32 Participants report their eating/drinking frequency of fruits, vegetables, whole grains, dairy, and fish over the last 30 days on a five-point scale from 0 (rarely or never) to 1 (1–2 times/week), 2 (3–6 times/week), 3 (once/day), 4 (twice/day), and 5 (3 or more times/day). The total HES-5 scores range from 0 to 25; a higher score indicates healthier eating behavior.
The short version of the International Physical Activity Questionnaire (IPAQ) with seven items was applied to evaluate physical activity level, which is widely used. 33 IPAQ provided information about the number of days and duration (minutes) that a person spent at least 10 min over the last week for vigorous activity, moderate activity, walking, and sitting. The total scores of physical activities were expressed as the metabolic equivalent of task (MET) minutes per week. MET score is calculated by multiplying the number of minutes spent in vigorous activity, moderate-intensity activity, walking, and sitting by 8.0, 4.0, 3.3, and 1.0, respectively, and summing the four components of physical activity. In this study, the levels of physical activity were subgroups: Tertile 1 (MET < 975.0), Tertile 2 (975.0 ≤ MET < 1872.0), and Tertile 3 (MET ≥ 1872.0).
Social media addiction
We used the Bergen Social Media Addiction Scale (BSMAS) to assess social media addiction. 34 BSMAS is a self-reported questionnaire that consists of six items that reflect the six features of addiction (salience, tolerance, mood modification, withdrawal, conflict, and relapse) proposed by Griffiths. 35 Participants report their experiences of using social media (Facebook, Twitter, Instagram, and the like) over the past year (e.g., Use a lot of time thinking about or planning using social media) on a five-point Likert scale ranging from 1 = very rarely to 2 = rarely, 3 = sometimes, 4 = often, 5 = very often. A higher total score (6–30) indicates a greater likelihood of being at risk of developing a social media addiction. The BSMAS has appropriate psychometric properties with Taiwan university students. 36 A score of 19 or higher is classified as social media addiction.4,36
Social support
Social support is assessed using the Multidimensional Scale of Perceived Social Support (MSPSS) developed by Zimet et al. 37 MSPSS is a self-reported instrument comprising 12 items designed to assess an individual's perception of the adequacy of social support they receive. Each item was scored on a 7-point Likert-type scale, from 1 = very strongly disagree to 7 = very strongly agree. This scale assesses support from three subscales, including family (items 3, 4, 8, and 11), friends (items 6, 7, 9, and 12), and significant others (items 1, 2, 5, and 10). The total scale score and each subscale score are obtained by summing the scores of items, with higher scores reflecting higher perceived support. The MSPSS has been validated in the Chinese population, showing internal consistency, Cronbach's α = 0.91; split-half = 0.87; test-retest = 0.84–0.91. 38 The reliability of this scale in this study is high, with a Cronbach's alpha of 0.95.
Anxiety symptom
The Generalized Anxiety Disorder-7 (GAD-7) was employed to evaluate participants’ generalized anxiety symptom levels. 39 The GAD-7 has been validated in Chinese-speaking populations, including Taiwan 40 and mainland China. 41 Participants self-rated how often they felt bothered with each of the seven core symptoms of GAD-7 over the past 2 weeks. Each item was scored on a four-point Likert scale, with 0= “not at all,” 1= “several days,” 2= “more than half the days,” and 3= “nearly every day.” Total GAD-7 scores range from 0 to 21, with the higher scores on the scale indicating a higher level of anxiety. GAD-7 has high internal consistency, with Cronbach's alpha of 0.94 in this study.
Statistical analysis
We checked the assumption of normal distribution of GAD-7 based on skewness and kurtosis values. The skewness and kurtosis values were already between −2 and 2, considered the acceptable limit for a variable to be a standard distribution with a large sample size. 42 Several demographic and health-related variables were included as covariates to address potential confounding. These variables were selected based on prior evidence of associations with both social media use and anxiety. T-test and one-way ANOVA tests were performed to examine the difference in GAD-7 mean scores between subgroups of independent variables. Besides, the assumption of linear regression was assessed. Variables with p < .05 in the simple model were selected for multiple models to analyze (Supplementary Table 1). The Spearman correlation was run to avoid multilinearity in the multiple linear regression model, and all independent variables showed mild correlations (rho < 0.3) (Supplementary Table 2). The multicollinearity of linear regression with variance inflation factor values was less than 2. The interaction analysis was used to explore the modified effects of social support on the association between SMA and anxiety level. We also investigated the modification of social support subscales in this association. We tested whether perceived social support moderated the association between social-media addiction and anxiety (GAD-7 score) using PROCESS Model 1 in SPSS, with 5000 bootstrap samples to obtain bias-corrected 95% confidence intervals for conditional effects. Interaction effects were probed using simple slopes at −1 SD, the mean, and +1 SD of social support and visualized using predicted GAD-7 scores. SPSS software version 25 (IBM Corp., Armonk, NY, USA) and PROCESS version 4.2 (developed by Hayes) were applied to statistical analysis.
Results
The participant's characteristics
The age of the study participants was 24.3 (± 4.7) years old. Most participants were single (91.5%), and women were more than two-thirds (69.9%). The scores of anxiety and perceived social support were 6.7 ± 5.4 and 61.8 ± 14.2. The scores of family, friends, and significant others' support were 20.0 ± 5.6, 21.2 ± 5.1, and 20.6 ± 5.4, respectively. The prevalence of SMA was 21.4%. Of 1324 participants, 72.6% were studying with undergraduate degrees, 47.8% lived with family, and 56.1% worked. Besides, the majority of participants did not smoke (84.6%) and did not consume alcohol (89.6%). The mean anxiety levels differed significantly by gender, marital status, ability to pay for medications, smoking, alcohol consumption, and SMAs (Table 1).
The characteristics of participants (n = 1324).

Note. Data were presented with the number (percentage), mean ± standard deviation (SD).
Abbreviations: GAD-7: the generalized anxiety disorder 7 items, HES-5: five-item healthy eating score; MET: mins/week, metabolic equivalent task minutes per week; MSPSS: multidimensional scale of perceived social support.
The association of social support and social media addiction with anxiety
After adjusting covariates, in Table 2, the results of multiple linear regression showed that one-score increments of social support were associated with low anxiety levels (adjusted coefficient [aB] = −0.06; 95% confidence interval [95%CI] = −0.08, −0.04; p < .001). Compared to individuals without SMA, those with SMA had higher levels of anxiety (aB = 2.02, 95% CI = 1.35, 2.70; p < .001).
The association between social support and social media addiction with anxiety.
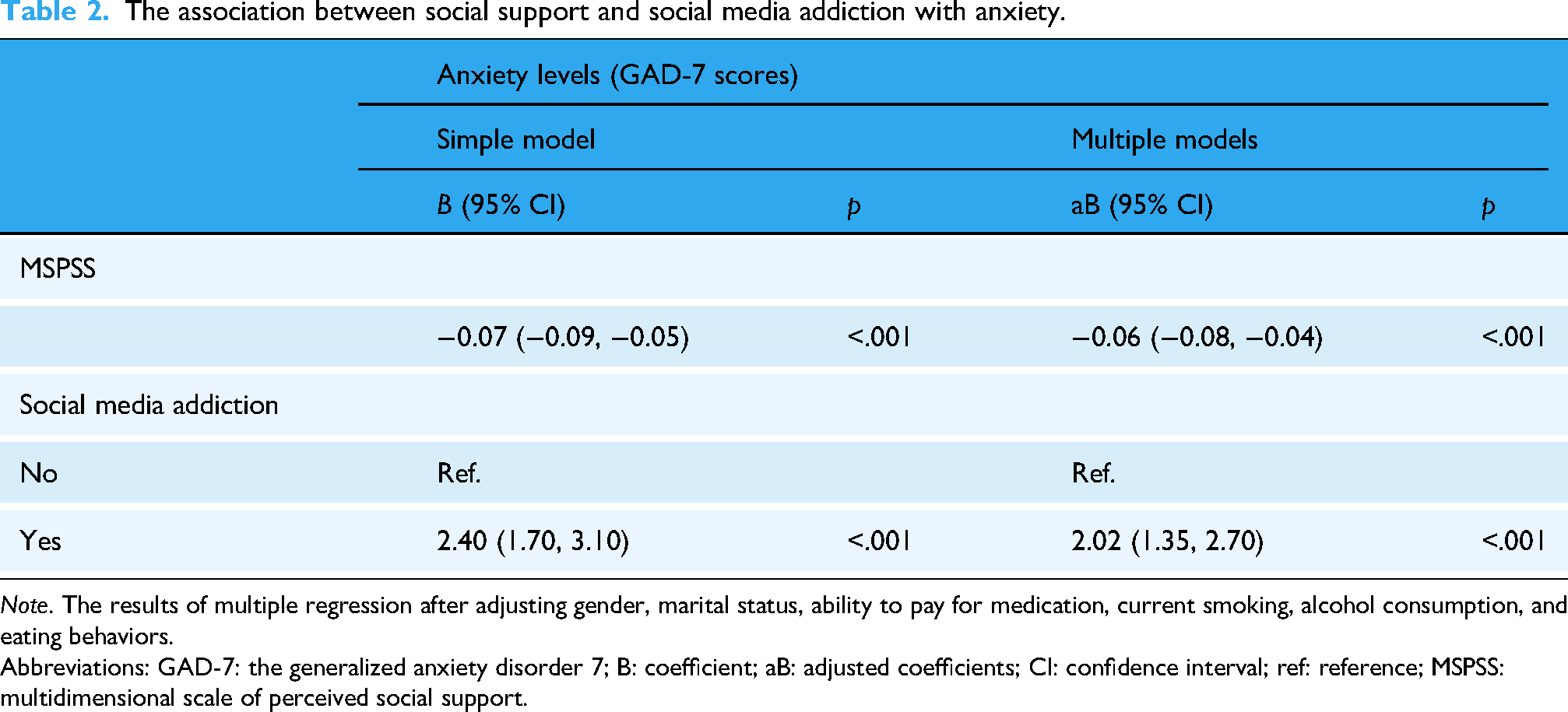
Note. The results of multiple regression after adjusting gender, marital status, ability to pay for medication, current smoking, alcohol consumption, and eating behaviors.
Abbreviations: GAD-7: the generalized anxiety disorder 7; B: coefficient; aB: adjusted coefficients; CI: confidence interval; ref: reference; MSPSS: multidimensional scale of perceived social support.
The interaction of social media addiction with social support and its subscales on anxiety
Table 3 presents the results of the interaction of SMA and social support and its subscales on anxiety levels. The findings indicated that individuals with SMA who have high perceived social support were associated with low anxiety levels (aB = −0.05, 95% CI = −0.10, −0.01; p = .033), suggesting that each one-point increase in social support was linked to a 0.05-point reduction in GAD-7 anxiety scores. The interaction of social support and SMA on anxiety level was more clearly demonstrated in the simple plot graph (Figure 1). At mean−1 standard deviation (SD), mean, and mean + 1SD values of social support, SMA participants had corresponding decreases in anxiety levels (from B = 2.66, 95% CI = 1.77, 3.55 at MSPSS (mean−1SD) to B = 1.24, 95% CI = 0.25, 2.23 at mean + 1SD of MSPSS) (Supplementary Table 3).

Interaction effect of overall social support and SMA on anxiety symptom levels (GAD-7 scores). The simple plot graph illustrates the interaction of social media addiction and social support on anxiety levels. GAD-7: the generalized anxiety disorder 7 items; MSPSS: multidimensional scale of perceived social support; SD: standard deviation.
Interaction of social media addiction and social support and three subscales of social support (family, friends, and significant others) on anxiety levels.
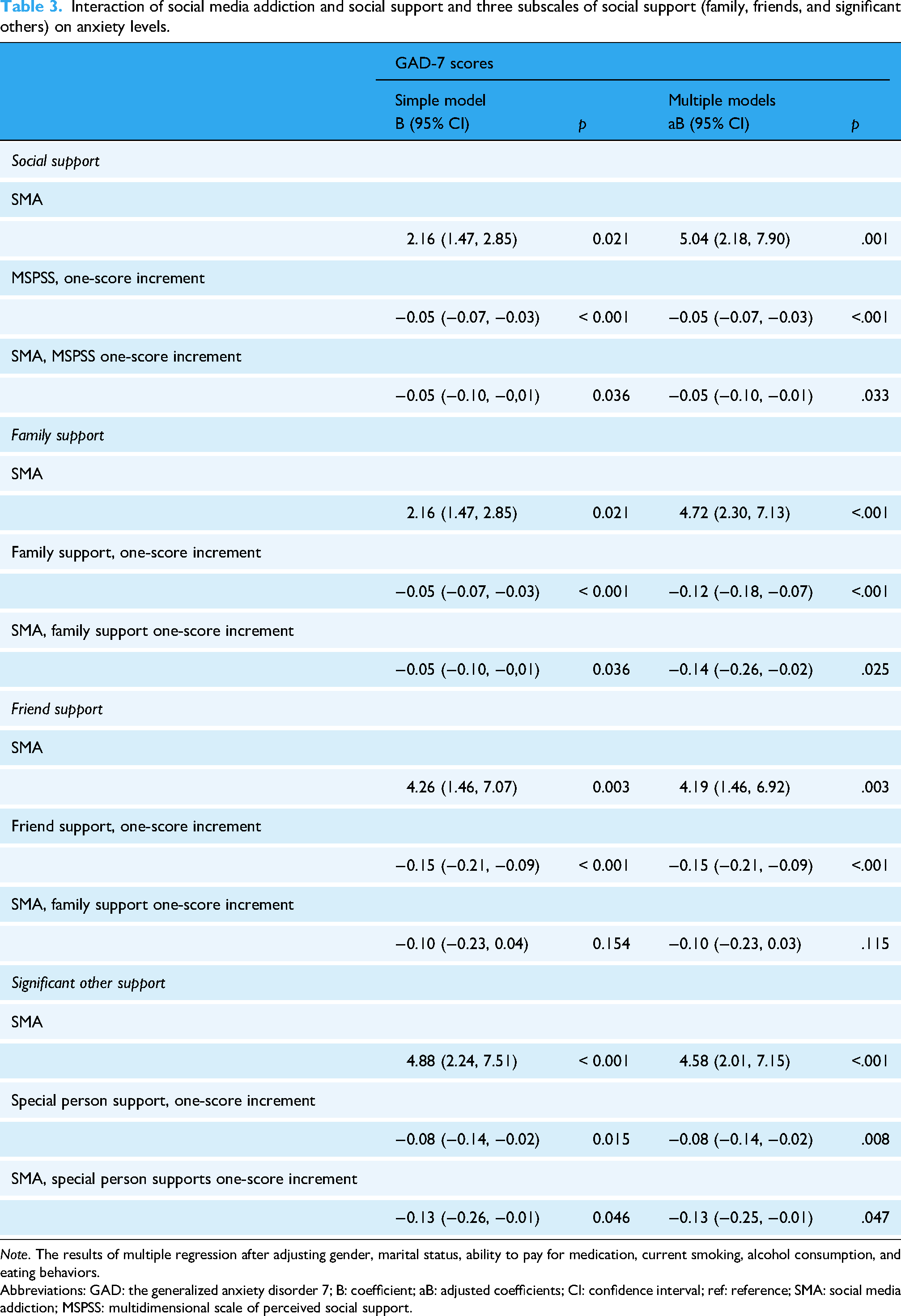
Note. The results of multiple regression after adjusting gender, marital status, ability to pay for medication, current smoking, alcohol consumption, and eating behaviors.
Abbreviations: GAD: the generalized anxiety disorder 7; B: coefficient; aB: adjusted coefficients; CI: confidence interval; ref: reference; SMA: social media addiction; MSPSS: multidimensional scale of perceived social support.
Additionally, people with SMA were associated with low anxiety levels when they had support from family (aB = −0.14, 95% CI = −0.26, −0.02; p = .025) or from significant others (aB = −0.13; 95% CI = −0.25, −0.01; p = .047). However, the interaction of SMA and friend support on anxiety levels was not statistically significant (aB = −0.10, 95% CI = −0.23, 0.03; p = .115). The interactions between support from family and significant others with SMA on anxiety scores were more clearly illustrated in the simple plot graphs, Figures 2 and 3.
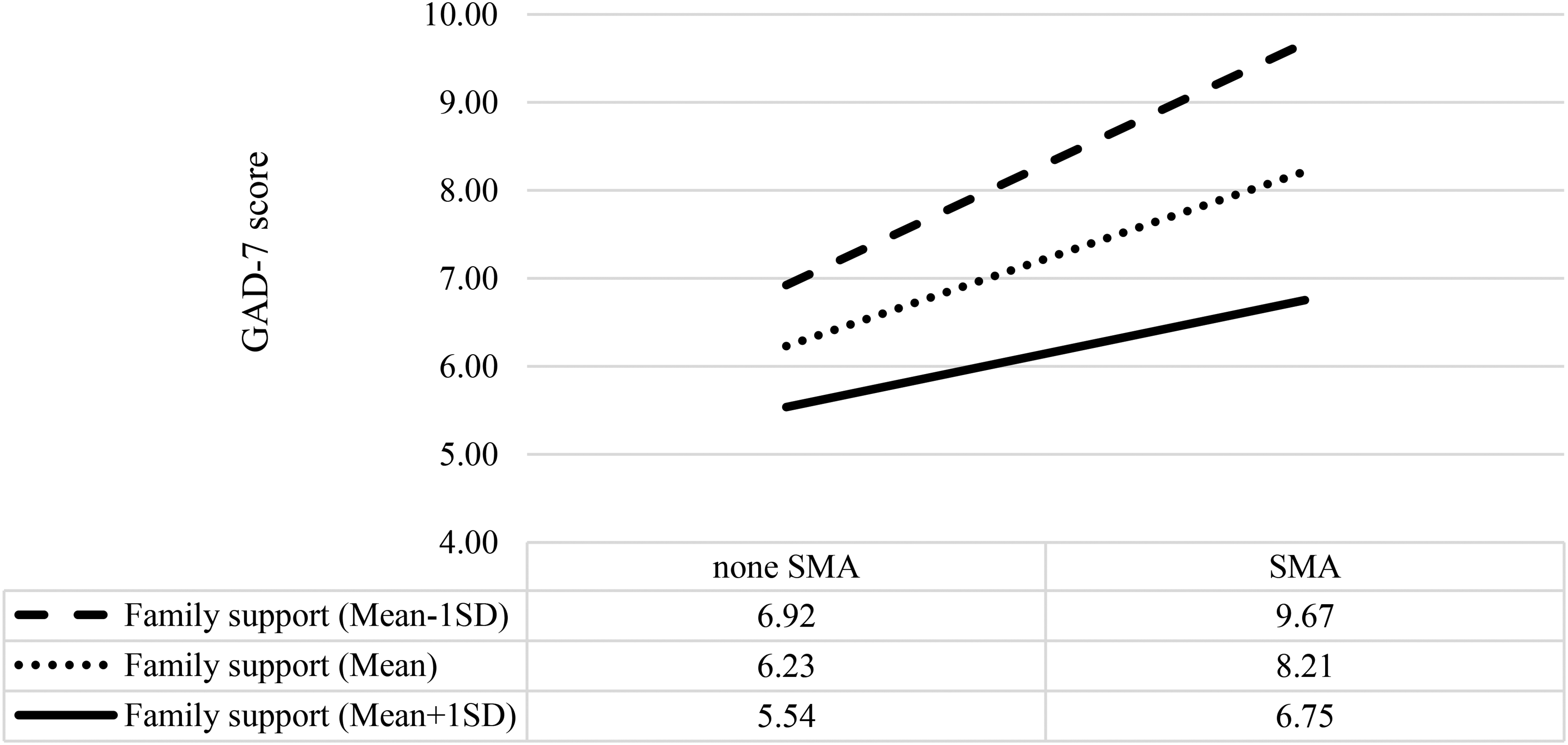
Interaction effect of family support and SMA on anxiety symptom levels (GAD-7 scores). The simple plot graph of the interaction of SMA and support from family on anxiety scores. GAD-7: the generalized anxiety disorder 7 items; SMA: social media addiction; MSPSS: multidimensional scale of perceived social support; SD: standard deviation.

Interaction effect of significant others support and SMA on anxiety symptom levels (GAD-7 scores). The simple plot graph of the interaction of SMA and support from significant others on anxiety scores. GAD-7: the generalized anxiety disorder 7 items; SMA: social media addiction; MSPSS: multidimensional scale of perceived social support; SD: standard deviation.
In summary, higher social support, particularly from family and significant others, moderates the association between social media addiction and anxiety levels, whereas support from friends did not show a significant moderating effect.
Discussion
This study revealed a significant correlation between SMA and high anxiety levels, whereas high social support was linked to low anxiety levels. Furthermore, social support, particularly from family and significant others, was observed to moderate the association between SMA and anxiety.
Our results were aligned with previous research indicating a strong link between SMA and anxiety.2,43,44 People with SMA may experience greater loneliness, 28 be more exposed to fake news or misinformation, 45 face negative interactions such as cyber-bullying, 46 and compare themselves to others negatively. 47 Social media use tends to be addictive, leading to compulsive use that can increase stress and anxiety as users cannot stop engaging or feel they have to connect constantly. 48 Collectively, these findings underscore that SMA as a significant predictor of anxiety, emphasizing the need for mindful and balanced use of social media platforms to mitigate mental health risks. Although the effect size of social support was small, the consistent negative association suggests that its buffering role should receive more attention.
The most notable finding of our study is the moderating effect of social support on the relationship between SMA and anxiety, especially support from family and significant others. This suggests that SMA individuals with higher social support have lower anxiety levels. Our study had similar results to well-documented literature that social support, associated with low anxiety, is a protective factor for mental health.49,50 Marengo et al. found that social support has a positive role in mediating the association between SMA and cyberbullying (a risk factor that leads to anxiety) in adolescents. 51 When people have strong connections with others, they can talk and share concerns, feel less loneliness or isolation, have emotional support and reassurance, which in turn could contribute to enhancing their self-esteem and resilience.52,53 Conversely, social support contributes to reinforcement, encouragement, and self-affirmation of people with SMA, helping mitigate the adverse effects of cyberbullying and social comparison, thereby lowering anxiety levels. 54 Besides, supportive relationships promote healthier coping strategies and lifestyles, such as regular exercise, balanced nutrition, and adequate sleep, which can help reduce anxiety in individuals with SMA. 55 Our findings also revealed that support from family and significant others could buffer the positive association between SMA and anxiety levels. Perceived family support was negatively associated with problematic internet use and had a mediating effect on the relationship between problematic internet use and anxiety.56,57 SMA positively correlated with low family functioning, adolescent-parent conflicts, and poor parent-child relationships.58,59 A family characterized by low conflict, strong and close relationships among members, and consistent emotional and material support serves as a protective factor against psychological distress, including anxiety. In short, these results emphasize the importance of strengthening family and significant others’ support to protect and enhance young adults’ mental health.
This study did not observe the moderating effect of friend support on the relationship between SMA and anxiety symptoms. This contradicts studies that found support from friends or peers as a protective factor for mental health in adolescents and young adults. 60 The difference in how significant family and significant others’ support, but not friend support, moderated the relationship between SMA and anxiety may be due to cultural and contextual factors. In collectivist cultural contexts such as Taiwan, support from family members and significant others tends to represent the most dependable and enduring source of psychological assistance. By contrast, support from friends may be less consistent or less effective in alleviating stress. Consistent with this notion, Fan et al. (2021) reported that only family support predicted symptomatic remission among community-dwelling individuals with schizophrenia. 61 Chen et al. (2025) also noted that family support often serves as a structural foundation that facilitates broader social support, which may explain why, in our study, support from family and significant others was more protective against anxiety than friend support. 62 Peer support may become more influential in longitudinal or stress-specific contexts, which our cross-sectional design could not detect. These discrepancies highlight the need for future research to explore cultural, developmental, and methodological differences in how social support from friends functions as a buffer against anxiety.
These findings have practical implications. Interventions that enhance family support and close relationships may help reduce the risk of anxiety in people with SMA. At the same time, raising awareness about healthy social media use remains essential to reduce the risk of anxiety.
This study has several limitations. First, the study was designed as a cross-sectional study, so a causal relationship cannot be assumed from the results. Therefore, additional research is needed to better understand the relationship between SMA, social support, and anxiety. Second, participants were recruited primarily through university channels, which may introduce selection bias and limit the generalizability of the findings to young adult populations. Furthermore, the use of self-reported measures may introduce potential biases, as responses can be influenced by personal perceptions, memory recall, or social desirability. Despite these limitations, our study contributes new evidence on the protective role of social support, especially from family and significant others, in moderating the relationship between SMA and anxiety symptom levels in young adults in Taiwan.
Conclusion
This study highlights the positive association between social media addiction and heightened anxiety among young adults. Importantly, social support, particularly from family and significant others, was observed to moderate this association. These findings highlight the importance of family and peer support, as well as the integration of social support strategies for both digital health policies and university mental health programs, and mitigating the negative effects of social media addiction. Future research should adopt longitudinal designs to clarify causal relationships and examine the role of friend support in greater depth which social support protects against the mental health risks of problematic social media use.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076251393393 - Supplemental material for Impact of social media addiction on anxiety symptoms as modified by social support and its subscales
Supplemental material, sj-docx-1-dhj-10.1177_20552076251393393 for Impact of social media addiction on anxiety symptoms as modified by social support and its subscales by Chuan-Rong Yeh, Han T. Vo, Cheng-Yu Lin, Chih-Feng Lai, Tru C. Tran Le, Shwu-Huey Yang, Jane C.-J. Chao, Pei-Shan Tsai and Tuyen Van Duong in DIGITAL HEALTH
Supplemental Material
sj-docx-2-dhj-10.1177_20552076251393393 - Supplemental material for Impact of social media addiction on anxiety symptoms as modified by social support and its subscales
Supplemental material, sj-docx-2-dhj-10.1177_20552076251393393 for Impact of social media addiction on anxiety symptoms as modified by social support and its subscales by Chuan-Rong Yeh, Han T. Vo, Cheng-Yu Lin, Chih-Feng Lai, Tru C. Tran Le, Shwu-Huey Yang, Jane C.-J. Chao, Pei-Shan Tsai and Tuyen Van Duong in DIGITAL HEALTH
Footnotes
Acknowledgments
We also appreciate students and the general public who were willing to participate in this survey.
ORCID iDs
Ethical approval
All participants provided electronic informed consent before beginning the survey. The study was reviewed and approved by the Taipei Medical University-Joint Institutional Review Board (TMU-JIRB No: N202201099). The study was conducted in accordance with the Declaration of Helsinki (1980).
Authors’ contributions
CRY, HTV, CYL, CFL, TCTL, SHY, JCJC, PST, and TVD conceptualized and developed the study; CRY, CYL, CFL, SHY, JCJC, PST, and TVD conducted the investigation and managed data; HTV and TVD performed formal analysis and drafted the manuscript; CRY, HTV, CYL, CFL, TCTL, SHY, JCJC, PST, and TVD revised manuscript and agreed final version to be submitted.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by Taipei Medical University (TMU113-F-005), National Science and Technology Council (grant number: NSTC113-NU-E-128-001-NU; and MOST 111-2410-H-038-008-MY2).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
The data supporting this study's findings are available from the corresponding author upon reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.