
Abstract
Objective
Artificial intelligence (AI)-enabled Socially Assistive Robots (SARs) are reshaping dementia care in long-term care (LTC) settings. This critical reflection paper, co-authored by co-researchers (people living with dementia and family partners), explores the perceived potential, limitations, and ethical considerations of implementing a robot LOVOT in LTC.
Methods
This paper presents a critical reflection based on interviews conducted and analyzed using a reflexive thematic approach. Among 12 co-researchers, three were older adults living with dementia; eight were family care partners and one was an older adult partner.
Results
Three themes identified include (a) LOVOT's role in supporting engagement and stimulating conversation, (b) the irreplaceability of human touch and emotional nuances, and (c) concerns about ownership and equitable resource allocation.
Discussion
Older adults emphasized that LOVOT has the potential to act as an active role as a companion for older adults with dementia. They also identified opportunities for improvement in design, especially around cultural responsiveness, technological familiarity and safety.
Implications
This reflection brings forward the lived experience perspectives from older adults with dementia, and family partners as co-researchers, offering valuable insights to guide ethical and person-centered implementation of SARs like LOVOT in LTC settings.
Keywords
Background and objectives
Artificial intelligence (AI)-enabled socially assistive robots (SARs) are emerging as innovative solutions to address key challenges in dementia and senior care, including caregiver burnout and staffing shortages in long-term care (LTC) homes. 1 These AI-enabled SARs have been functionally categorized into (a) service robots (e.g., Care-O-bot, Cody), which assist with activities of daily living, and (b) companion robots (e.g., PARO, LOVOT), which provide psychosocial support by acting as a social communication link and comforting companion.2–4 Studies have shown that SAR-mediated group activities in LTC settings can enhance social engagement of older adults by encouraging both human-to-human and human-to-robot interactions. 5 A systematic review and meta-analysis suggest that while SARs are generally feasible and acceptable to people living with dementia, family caregivers, and staff in LTC, there are inherent practical limitations that inhibit their adoption. 6 Despite their potential to alleviate staff burden, LTC healthcare providers have raised concerns that SARs could increase workload rather than reduce it due to the need for staff training, as well as regular robot cleaning and maintenance.1,6 Financial constraints further limit adoption and uptake in LTC, as advanced SARs often have high upfront and ongoing maintenance costs. Prior work has cited a single PARO unit price to be at USD $6675, 6 while LOVOT, the newer mobile companion robot developed by Japanese company Groove X, has been marketed with not only an upfront cost of ¥450k (approx. USD $3000) in Japan for its base model but also an ongoing monthly service fee of ¥10,998 (USD $74) – ¥21,998 (USD $149), 7 making widespread implementation challenging for underfunded public LTC homes. Moreover, resistance to SARs with limited social and auditory capabilities was also reported among people living with dementia. 8
LOVOT was able to address the limitations in communication identified in previous studies through its AI-enabled recognition and response to facial expressions, verbal cues, and touch. 8 LOVOTs primarily communicate through body language and non-verbal sounds (e.g., cooing), making them accessible for older adults living with dementia who may have reduced language or cognitive skills. 9
Dinesen et al. (2022) conducted the first known study testing the use of LOVOT with people living with dementia in Denmark nursing homes. 7 While there were no clinical significant changes in resident wellbeing, face scale results showed that residents tend to show more positive facial expressions post-session with LOVOT. 7 Hung et al. (2025) also explored the use of LOVOT to foster meaningful interactions between older adults and social robots, highlighting its potential to provide emotional support in Canadian LTC settings. 9
Understanding older adults’ experiences with LOVOT can help identify opportunities to improve the robot's ability to support the well-being of seniors, improve their daily interactions, and better address their needs with their experiences in LTC. Current literature on LOVOT in LTC settings suggests that LOVOT demonstrates the capacity to support emotional well-being, reduce loneliness, and foster social interaction among older adults. In an ethnographic study, researchers found that LOVOT elicited joy and a sense of unconditional acceptance and encouraged creativity among older adults living in a Canadian LTC home. 9 These findings highlight the importance of acknowledging the various ways older adults perceive and engage with social robots in LTC, suggesting that devices like LOVOT could serve as a valuable tool in addressing older adults’ psychosocial needs across diverse LTC environments. See Figure 1 for an image of LOVOT.

A LOVOT robot.
Research gap, reflection question and objectives
While previous exploratory studies in Denmark and Canada have reported on interactions between residents living with dementia and LOVOT in LTC homes,8,9 there remains a significant gap in understanding how people living with dementia and family caregivers perceive the adoption and use of AI-enabled SAR in LTC. This study contributes to the literature by exploring the perspectives of these individuals on practical and ethical implications of implementing such technologies. The paper addresses the gap by presenting the perspectives of older adults with dementia and family partners who served as co-researchers. Through their reflection, this study explores not only their experiences with the LOVOT robot, but how they envision its role, limitation and ethical considerations in LTC.
Research question:
What are the perspectives of older adults with dementia and family partners on the use of AI-enabled socially assisted robot, LOVOT, in LTC homes?
Objectives:
To explore perceived potentials and limitations of using LOVOT in LTC homes To examine ethical considerations for adopting LOVOT in LTC homes
Research design and methods
The following sections describe the team composition, data acquisition and collection, and ethical considerations.
Team composition
Our interdisciplinary research team comprised of 12 co-researchers––including three older adult patient partners living with dementia (JM, LJ, and one additional partner), eight family care partners, and one older adult partner––alongside graduate and undergraduate students (KL, JOYW, KLYW, JW, RS, AF, RL) and academic researchers (JCG, LH). They came from diverse backgrounds. The older adult and family partners on the team had lived experience in aging, living with dementia, and caring for family members with dementia. The academic researcher and students were from various disciplines, including nursing, social work, sociology, microbiology, and integrated sciences.
Data acquisition
This paper focused on the critical reflection of older adults and family partners. For their background information, please see Table 1. Our team reflected on the data depth and richness with the research question to determine the dataset size. 10 The inclusion criteria for our partners are 1) to be able to speak and understand English, and 2) to have lived experiences with dementia, e.g., a person living with dementia and family partners. There are no exclusion criteria. The first author (KL) and two coauthors (LH and JOYW) facilitated individual or group interviews with the co-researchers between February and March 2025 using a semi-structured interview guide, which is presented in Table 2.
Background information of co-researchers.

List of questions asked in the interview.

Group interviews consisted of 2 to 3 partners. Each interview lasted from 30 min to an hour via Zoom or in-person meetings. All interviews were recorded and transcribed. Facilitators of the interviews also took notes during the interviews.
Data analysis
We conducted a reflexive thematic analysis
10
with detailed steps outlined as follows:
Two authors (KL and JOYW) read and re-read the transcripts and notes to familiarize themselves with the data. KL and JOYW independently coded the data, grouped similar codes into categories, and grouped similar codes into themes, constantly comparing the codes, categories, and themes. KL and JOYW presented the themes to other team members for feedback and refined them according to the feedback. The themes are presented in the results section.
Ethics
This paper is a part of a larger study of implementing LOVOT in LTC settings. Consulted the University of British Columbia Ethics Board; this is a critical reflection paper, so consent is not required.
Results
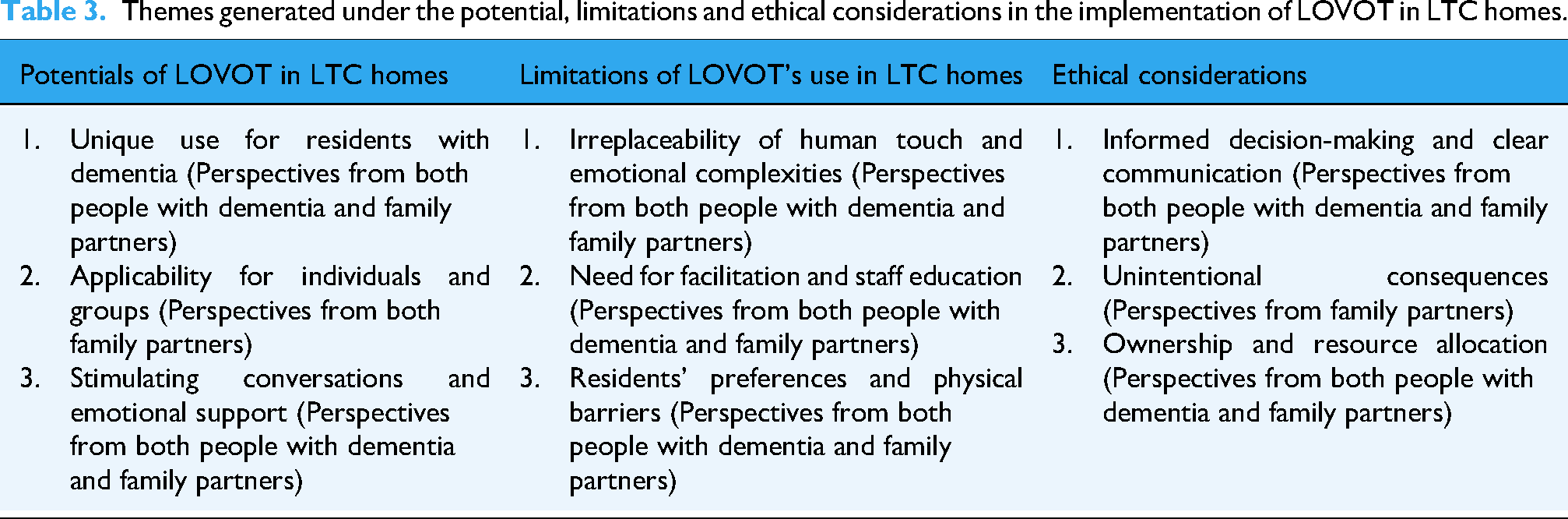
Our analysis, grounded in critical reflection by older adults with dementia and family care partners as co-researchers, generated three overarching thematic domains: potentials, limitations, and ethical considerations regarding the use of LOVOT in long-term care (LTC) settings. See Table 3.
Themes generated under the potential, limitations and ethical considerations in the implementation of LOVOT in LTC homes.
Potentials of LOVOT in LTC homes
Unique use for residents with dementia
Many partners mentioned the uniqueness of LOVOT regarding how their “language” supports equal opportunities, non-selective responses, non-judgmental presence, and its appropriate use with residents living with dementia in LTC. A family partner said one thing she liked about LOVOTs for residents with dementia was that LOVOTs “do not speak in words.” A patient partner commented, “The thing [LOVOT] doesn't talk, so it's an equal opportunity robot… because it doesn't talk, it could be appealing to anybody.” (Jim, patient partner) Another patient partner echoed, “Everyone has an equal opportunity, whether they [staff] think they [residents] can understand it [LOVOT] or not. But you know you give them [residents] a chance [to interact with LOVOT].” (Lynn, patient partner)
Many partners also emphasized how LOVOT is non-judgmental in interactions. A family partner said, “LOVOTs provide a non-threatening presence. Unlike human beings, LOVOTs are non-judgmental and do not place any social expectations [on residents].” (Hossein, family partner) A few family partners appreciated the simplicity of LOVOTs with only the function of “being cute” and as an accompaniment, which provides a non-stressful presence. One of them stated, “He [LOVOT] couldn't offend me or… I didn't need to have to respond to a question… for people with dementia, they may not know what to say, but the squeaks were just really cute.” (Cindy, family partner)
Many partners shared that LOVOT's uniqueness is that it gives people an immediate feeling of happiness, pleasure, and comfort and can serve as an object to share emotions, mainly due to its outlook. One older adult commented, “They're so cute that you want to hug them.” (Milena, older adult partner) One family partner commented on the bright colored clothes that LOVOTs wore: “I love LOVOT; I like their orange and green coats, which they are pleasant to look at.” (Zarina, family partner). Partners expressed the happiness, joy and positive emotions that LOVOT brought. An older adult with dementia stated, “may be overwhelmed with that feeling of joy. It's so joyful.” (Jim, patient partner) Another family partner shared how LOVOTs can be comforting, “It gives a feeling to people [residents] that it [LOVOT] can help them and comfort them whenever they feel sad… there is someone share their feelings, someone that understands.” (Alice, family partner)
Applicability for individuals, in groups and beyond
When discussing how LOVOT can be adopted in LTC homes, most of the partners expressed that LOVOTs could be used in both group and individual settings. A family partner explained, “In a group setting, observing how each other interacts with LOVOTs helps some people to know ‘Oh, that's what I do, too?’ and want their turn [to participate and interact with LOVOTs]. People who are maybe more shy or holding back, like [name of her husband with dementia], probably wouldn’t pick up the robot in a group setting. But he would really like to if it was one-on-one [interaction]…he would talk to it. It just depends upon the person.” (Cindy, family partner)
A few partners added that knowing the stages of dementia could help determine the appropriate way to adopt LOVOTs for the residents. A family partner shared, “In a later stage, some residents might have lost their ability to communicate and socialize with each other, so if we use LOVOT in a group, it will not work for those individuals. For this group of residents, definitely one-to-one sessions will be better. For residents who have mild dementia, group sessions might be good.” (Alice, family partner)
One older adult partner commented on the physical size of LOVOT when considering how LOVOT should be used. She said, “I would not put them into a group but more with individual persons or with two people because LOVOTs are small.” (Milena, older adult partner)
Our partners also suggested ways to enhance LOVOT to be best used in LTC settings for residents with dementia. One family partner suggested having a function to warn residents of LOVOT's presence to prevent the risks of falls. She said, “Flashing or something, like a warning, so the person would not trip over.” (Lily, family partner) Another family partner who works as a nurse suggested a function to signal staff about residents’ needs. She described, “If LOVOTs can understand the residents’ facial expressions, they may notice residents’ unmet needs, such as the need to change their pads. The healthcare staff can be notified through LOVOTs; we can address those needs earlier and improve the quality of care.” (Alice, family partner)
Offering support and stimulating conversations
Our partners discussed their perceived roles of LOVOTs in providing psychosocial, emotional and physical support. A family partner mentioned the benefit of LOVOTs in combating social isolation: “I think what I see with [the two people that I'm with] is isolation is really big… they kind of withdraw because they're afraid to talk or show that they're being forgetful or something like that. I feel like this robot would be a safer place for them.” (Jo-Ann, family partner)
Another family partner added on how LOVOTs could offer emotional support. She said, “If one resident is feeling anxious or scared or they're upset, maybe bringing the robot in to see them might take them to another place so that they forget about what they were feeling and feel better.” (Cindy, family partner) An older adult with dementia thought LOVOTs would enhance the verbal and physical abilities of residents in LTC. She said, “They [LOVOTs] would increase their [residents’] verbal ability… [residents] trying to talk to LOVOT… maybe the resident is not used to talking very much, and it [LOVOT] brings out their language. It brings out maybe some more physical activity.” (Lynn, patient partner)
Many partners described LOVOT as a companion for residents, often comparing LOVOTs to pets, grandchildren or babies. A patient partner with dementia stated, “It [LOVOT] gives them [a resident] a sense of, ‘okay, I'm talking to my grandson.’” (Mario, patient partner) A family partner shared her experience interacting with LOVOT: “When I picked it [LOVOT] up as a baby, I started talking to it like he was a baby.” (Cindy, family partner) Two family partners commented on how LOVOT was like a pet. One said, “[LOVOTs] can help comfort them [residents] like having kept a dog as a company.” (Alice, family partner) Another family partner echoed, “I am treating the robot as a kind of live animal. They are bumping into something, and then they turn around.” (Zarina, family partner)
Another role the partners described was how LOVOTs could act as a medium for interaction and conversation. Two patient partners said how LOVOT could connect people. One shared, “Something like LOVOT would bring people together.” (Jim, patient partner) Another patient partner said, “I think that is a very good impact of the robotic device [LOVOT] in the sense that it could bring out a person's ‘aloneness,’ like being by himself, and it [LOVOT] allows him to be part of the conversation.” (Mario, patient partner) A family partner shared how LOVOT could allow interactions for residents who cannot join group activities: “I think it [LOVOT] was a wonderful thing to use with people for engagement…I see that it would be great that if I have somebody that particular day can't make it to their events, a LOVOT for a few minutes would be some nice interaction.” (Bubli, family partner)
The role LOVOT has in communication was also perceived as beneficial for family care partners in communicating with residents. A family partner stated, “LOVOTs can help initiate the conversation… You can think of other things to talk about instead of just ‘how are you? I'm doing fine or not fine,’ and it's [LOVOT's] a conversation piece.” (Lily, family partner)
Limitations of LOVOT's use in LTC homes
Irreplaceability of human touch and doubt on comprehension related to emotional complexities
Most partners thought LOVOT would not be able to replace the human touch and highlighted that human interactions are still needed. A family partner said: “I wouldn't like to see them [LOVOTs] take over, like be relied on too much, they [residents] still need the human interaction.” (Jo-Ann, family partner) Another family partner also said: “Never. Never. No. You can't replace that human touch. The little squeaks and burps or whatever that robot has, you can't, the gentleness and kindness of the voice and the touch that can't be replaced by a robot” (Cindy, family partner)
Some partners showed concern regarding LOVOT's capacity to understand humans’ complex emotions. A patient partner questioned, “If I'm sad and maybe I'm crying, or I don't feel very good. Will they [LOVOTs] commiserate with me?” (Lynn, patient partner) While another family partner added: “Maybe sometimes LOVOTs might not understand because human beings’ emotions, conversations and facial expressions can be very complex. If that happened, LOVOTs may not understand what the older adults with dementia experience at that time.” (Alice, family partner)
The need for facilitation and staff education
Some partners shared that some residents might not understand what LOVOT's gestures or sounds may mean to them and cannot proactively initiate interactions with LOVOTs without any prompts. One family partner said, “LOVOT is like a ‘mobile emoji’ with the changes in the eyes and their moving body. However, it also depends on whether the residents understand what the meaning of the eyes show.” (Felicia, family partner)
Many of our partners agreed that there was a need for a person to facilitate the interactions. A patient partner said, “Somebody will need to be in that area to monitor…At least at the start, have someone introduce it [LOVOT]. Otherwise, it could end up like plopping it [LOVOT] on the floor or a table, and then people [residents] sort of look at it and just go back into their [residents’] shell.” (Jim, patient partner)
Another patient partner also stated the importance of a human facilitator: “A human intervener or a person who would make sure [to convey the message] that the robot is a friend to everybody.” (Mario, patient partner)
A few partners mentioned the importance of staff education on LOVOT to prepare staff to make the interaction between the residents and LOVOT easier. A patient partner said, “I think the staff should have training and that they should do that training to everybody.” (Lynn, patient partner).
Residents’ preferences and barriers to using LOVOT
Although LOVOT looked pleasant for many partners, some partners described how LOVOT may not be a preference for some residents at LTC homes. For example, a patient partner mentioned that LOVOT might “infantilize” people and a family partner echoed that LOVOT “wasn’t for everybody.” A patient partner mentioned possible intimidation of residents by the robot. The patient partner stated, “I can see people being intimidated by it [LOVOT], being afraid of it.” (Lynn, patient partner) A family member added the fear of the LOVOT could be due to its programmed behavior of moving towards people: “Some residents might be scared by the movements of LOVOT, not knowing what LOVOT is.” A patient partner explained the preference of residents with the feeling of unfamiliarity and the potential cultural influence. He said, “Older adults [in North America] probably may not have a sense of familiarity with robotic devices, unlike the people from the Oriental such as Japan, wherein robotic devices are ubiquitous in almost everyday life.” (Mario, patient partner)
There were also barriers identified for residents to interact with LOVOT, including LOVOT's heavyweight and short height, potentially making it hard to pick up. A few partners commented on LOVOT's weight as “heavy” and with a hard machine in their body. A family partner described, “Mango and Kiwi are quite difficult to be lifted [by residents] from the ground or the table because they are AI-equipped, so they are sort of a little bit hard and not like a fluffy animal.” (Zarina, family partner).
Due to the small size of LOVOT, a family partner shared a challenge for residents in wheelchairs to interact with them. She said, “As LOVOT often move on the floor, residents may need to bend down to interact with LOVOT, which may be difficult for older adults.” (Felicia, family partner) A patient partner shared his comment regarding the challenge posed by the difference in height with LOVOT: “Like I'm six [feet tall], I need to look down at this little thing. It was a long way to pick it up. I think you would get a different feeling sitting down with this [LOVOT] on your lap, and then you'd feel a lot closer to it.” (Jim, patient partner) A few partners also addressed the possibility of falls for the residents. One family partner said, “The person cannot see well, and if they're moving and that old person is walking, they may trip over.” (Lily, family partner)
Ethical considerations
Informed decision and clear communication
A majority of our partners discussed the importance of informed decisions by users of LOVOTs in LTC homes. A patient partner stated that an introduction was crucial to ensure the users’ understanding. He stated, “We focus on residents’ autonomy… we are not pushing the robot [LOVOT] to them. Rather, it's more like allowing them to understand that there is a device that they might be interested in.” (Mario, patient partner). Another patient partner echoed the importance of having the residents aware of what they are provided with: “You need to tell them [the residents] there's a camera [on LOVOT]” (Cindy, family partner)
Another patient partner suggested that informing the family council could ensure transparent communication between the LTC administrators, family members and residents on the adoption of LOVOTs. He stated, “This is where the family council comes into it … the connector between the home [and the family and residents] … briefing the family council on what we've got and give advance notice to some families [on the use of LOVOTs].” (Jim, patient partner)
One important aspect was the concern around privacy. As LOVOTs have cameras installed on the body, our partners raised some privacy issues. A family partner stated, “There might be a concern about the robot [LOVOT] taking information; it might be perceived as, ‘Ooh, there's this strange technology in my room that's listening to what I'm saying.’” (Jo-Ann, family partner) Some suggested the need to learn how the cameras and recording functions can be turned off. One family partner said, “While privacy may be a concern if the users have a better awareness of the setting, the privacy risks can be reduced.” (Felicia, family partner)
Unintentional consequences of using LOVOT
Some partners raised concerns over misuse and unintentional consequences regarding over-reliance on LOVOT. A family partner said, “While LOVOT offers comfort, there is a risk that individual might become too reliant on the robotic [LOVOT].” (Hossein, family partner) Another family partner added how older adults might react when considering LOVOT as living animals or humans. She said, “If I were an older adult and I saw the robot going really near the table edge, I would jump up first or try to save it right before going to the logic.” (Zarina, family partner) She further elaborated on how the residents might perceive LOVOT like a pet and might feel guilty if they realize LOVOT hasn’t been fed. She said, “Older adults in long-term care sometimes think of feeling guilty and not taking care of the pet. For example, if they are eating pudding and think that it is a real animal, they would like to feed the animal so that they both enjoy it. But in this kind of setting, the robot cannot eat, right?” (Zarina, family partner)
Another family partner pointed out that when LOVOT may not fully comprehend the resident's emotions, it may cause distress to the residents: “It can be negative because the robot is showing that I do not understand you. This might trigger the emotional responses of residents. It can be possible, and maybe the connection [between the resident and LOVOT] will be broken.” (Alice, family partner)
Concerns regarding ownership and resource allocation
Our patient and family partners commented on the ownership and resource allocation around LOVOTs. Some mentioned the high cost of LOVOT and how this could make access unequal. A family partner said, “Cost and accessibility. LOVOTs and similar technology can be expensive, limiting their widespread use in long-term care settings.” (Hossein, family partner) However, another patient partner said the cost factor could be spread if it is shared use. He commented, “Looking at it [LOVOT] to be implemented in long-term care home wherein a lot of people can be using it, the cost factor diminishes, and I see the value of it being used in many people's settings.” (Mario, patient partner)
The concern around ownership of LOVOTs was brought up, possibly causing conflicts among the residents, families and LTC settings. A patient partner said, “So who's going to look after them [LOVOTs]? If the long-term care buys them, then they [LTC staff] should look after it.” (Mario, patient partner) While another patient partner said: “To me, … I can understand why long-term care home would have the policy that you won't have something that is just yours. It won't be just yours for very long because, I mean, let's face it, most of the residents have some dementia. And they are going to take it out of the room.” (Jim, patient partner)
Two partners mentioned how the limited number of robots could impact residents. A patient partner said, “It's always nice to have somebody who can make sure that one of them [residents] do not hug or use the robotic device [LOVOT] [for too long] because at some point, it could be very engaging and then that person may just want to keep using the robot.” (Mario, patient partner)
A family partner also gave an example of using LOVOT in a group session: “We just didn't get enough one-on-one time because we were in a big group” (Cindy, family partner).
Discussion
The adoption of SARs in LTC settings has generated interest and debate, particularly in dementia care.11–15 This study offers a unique contribution by presenting a critical reflection grounded in the voices of older adults living with dementia and family partners who acted as co-researchers.
One of the most prominent insights from this study was how LOVOT's emotional accessibility allowed partners to reimagine social connection. Participants emphasized its warmth, non-judgmental presence, and predictability, as meaningful qualities in the context of dementia, where communication challenges often create social distance. This aligns with previous research identifying the value of SARs as emotionally safe companions that support affective therapy, particularly for those at risk of social exclusion.2,9 What emerges here is not simply confirmation of existing findings, but a deeper look into how relational interpretations such as viewing LOVOT as a pet, grandchild, or infant, mediate emotional attachment. These analogies offer insight into how users assign meaning to SARs through personal and cultural frameworks, reinforcing prior work on anthropomorphism and emotional proxy. 6
Beyond emotional impact, participants offered reflections on LOVOT's functionality within diverse care contexts. They envisioned both group and one-on-one applications, tailored to the cognitive and social capacities of residents. This echoes literature advocating for adaptable SAR use that can scale to different dementia stages and settings. 4 However, participants went further in suggesting specific design modifications such as fall detection or easier handling, which suggests a shift in the discourse from acceptance to co-creation. Rather than merely receiving technological solutions, these partners actively imagined what SARs should do, emphasizing a need for future design processes that are participatory and inclusive.
A key strength of this study lies in the inclusion of three patient partners living with dementia, whose contributions moved beyond user feedback. Their reflections underscored that LOVOT did not just offer comfort, but also invited expressions of care. Describing moments of “taking care of” the robot, they framed it not simply as a receiver of affection but as an agent through which purpose and reciprocity could emerge. These moments challenge simplistic narratives of passivity in dementia and point toward SARs as tools that can reinforce identity and agency.
However, participants also offered critical insights about LOVOT's limitations. Many emphasized that the robot could not replicate human empathy, intuition, or the emotional nuance required in sensitive care situations. This mirrors ongoing concerns in the literature about the superficiality of robotic companionship when compared to authentic human connection.9,16 The question, then, is not whether SARs should be in LTC, but how they are framed: as complements to care rather than replacements. This is a crucial distinction, especially in overstretched care environments where the temptation to substitute technology for human labor may be strong.
Several participants highlighted the importance of structured facilitation for successful interaction. Without guidance or contextual introduction, they worried that residents might find LOVOT's movements confusing or meaningless. These concerns echo prior research showing that meaningful engagement with SARs often depends on caregiver mediation and scaffolding. 2 Here, participants call not just for operational training, but for thoughtfully designed integration strategies that attend to residents’ emotional and cognitive readiness.
Concerns around design aesthetics and cultural reception also emerged. Some partners found LOVOT's childlike or pet-like design unsettling, raising concerns about infantilization. Others pointed out that unfamiliarity with robotic movement or sound might trigger anxiety, especially for older adults with limited exposure to such technology. These critiques underscore that SAR acceptance is not uniform; it is shaped by intersecting factors such as personal history, cultural values, and design aesthetics.9,16 Additionally, partners raised important accessibility issues such as the robot's weight and low height arguing that these features may make it difficult for people with mobility or vision challenges to engage comfortably. These insights reinforce calls in the literature for universal design principles in SAR development. 9
Notably, the reflections of patient partners added critical depth to these concerns. One described LOVOT as “emotionally helpful” but incapable of truly understanding him, highlighting the gap between affective simulation and authentic empathy. Another stressed the importance of choice and preparation, noting that sudden movements could be unsettling. These comments do more than recount personal impressions, they ask us to confront the limits of affective computing in care. The presence of these voices reminds us that ethics is not merely a technical checklist, but a relational practice grounded in experience. While studies have shown that SARs can reduce loneliness and support mood, 9 they also caution that successful use depends not just on the design, but on the way the robot is introduced, contextualized, and supported. Partners’ voices in this study reinforce that SARs should be introduced with ethical care, supported by transparency, and a commitment to the dignity of those it seek to serve. This is echoed by recent reviews highlighting that long-term success of SARs depends equally on ethical governance and personalized integration strategies. 17
Ethical concerns were further articulated in discussions around transparency, consent, and emotional boundaries. Participants called for clear, accessible communication about what LOVOT does and what it does not do including data use and camera functionality. Gradual, supported introductions were seen as necessary to build trust. These reflections resonate with ethical frameworks that prioritize informed participation and psychological safety in technology integration.1,4 Asada and Okada (2025) further advocate for culturally grounded, relationally responsive SAR design and governance, urging developers to consider emotional authenticity, local values, and adaptive consent processes as essential to ethical care integration. 18 Moreover, some participants raised concerns about emotional dependency, questioning what would happen if LOVOT became unavailable or malfunctioned. These tensions echo prior studies warning that SARs may create emotional dissonance if they are perceived as more emotionally aware than they actually are. 2
Lastly, equity and access were central to the ethical landscape participants described. While LOVOT was seen as potentially beneficial, its cost raised questions about who would get access, and how often. Some proposed shared-use models, but acknowledged the potential for conflict over time, ownership, and emotional attachment. These concerns reflect broader debates about fairness in resource distribution and the ethics of selective enhancement in LTC contexts. 1
Taken together, these reflections move the conversation beyond surface-level acceptability toward a more nuanced, person-centered evaluation of SAR integration. The implications are twofold. First, the emotional, cognitive, and ethical variability among LTC residents demands flexible, adaptive implementation strategies. Second, SAR development and deployment should not be viewed as value-neutral processes; they are shaped by and shape social relationships, cultural norms, and institutional structures.
By centering the voices of people with dementia and their families as co-analysts, this study invites a shift in how SAR research is conducted. Rather than asking only whether SARs “work,” it asks how they are experienced, interpreted, and judged by those most affected. Future studies may benefit from formal qualitative coding or comparative methods, but what this study offers is equally valuable: a thick, grounded account of lived experience that both affirms and complicates prevailing narratives of SAR use in dementia care.
Implications
Our study provides integral insight into AI-enabled SARs in LTC among people with dementia and family caregivers. Some practical implications regarding the implementation and usage of LOVOT in LTC settings may involve education, transparency, improvements in design, research implications, long-term effects of using LOVOT, and the need for diverse study populations.
The training on SAR utilization may help to foster increased understanding. The implementation of training could start at the healthcare professional school curriculum level or the facilities. Training at LTC homes or schools on SARs and how to facilitate older adults’ interactions with these devices may reap benefits and reduce older adults’ uncertainty of interactions, as many feel unfamiliar with these technologies. 19 Education of SARs can also describe the recommended use for individual or group settings, ensuring tailored use based on the residents. It was reported that the acceptance of innovative assistive technologies increases when older adult users see an increase in safety perceptions, 20 suggesting education on how to explain and increase the perception of safety to residents in LTC homes will be beneficial.
The design and functional update of LOVOT, which can include auditory and visual warnings to prevent falls or injuries, can allow increased practical uses in LTC settings. Certain SARs, such as Robot NAO, are already looking at being able to detect falls of users. 21 Robots with bright colors and the use of lights can also be engaging for certain users. 22 Possible changes in the appearance of LOVOT, addressing cultural relevance and privacy concerns, may increase the acceptability of the device. Wang et al. (2024) reported the older adult culture influenced the acceptability of robotic technology. 4 The issue of being watched, resulting in an invasion of privacy, was stated by other scholars as well. 19
Researchers could explore the perspectives and effects of the long-term implementation and usage of SARs in LTCs, possibly in a longitudinal study design. This might provide insights into whether the findings will enhance the psychological and emotional impact and improve quality of life through sustained interactions. While Rass et al. (2025) concluded there was a potential to have improved well-being, engagement, and social interaction by using social robots for 10 months, 23 whether these effects manifest later than the periods studied needs further investigation. Future studies could also explore the impact of SARs, such as using LOVOT, in more diverse racial, cultural, and SES contexts, as there may be differences in the perspectives and acceptability of SARs in LTCs. Investigating the implementation, acceptability, and perspectives of AI-enabled SARs may allow researchers to help develop more equitable technologies individualized to older adults with dementia that are cross-culturally acceptable.
Lastly, the perspectives of older adults with dementia and family partners on LOVOT could be analyzed using the Technology Acceptance Model (TAM), which is applied to examine how the users accept new technologies. 24 There are increasing studies relating SAR to TAM. 25 One scoping review that explored the technology acceptance theories or models, including TAM, with SAR, found that participants from all included articles included older adult users. 25 As the review paper reported, our study aligned with the stigma related to using robots, while we report that the acceptance may depend on an individual's preferences. 25 Another paper explored the barriers and facilitators to accepting SAR for older adults. 26 When comparing the themes from the paper, we report a similar theme where LOVOT provides emotional support and helps with socialization. 26 Further, our study also echoes some of the barriers, such as challenges associated with finance and regulations. 26 Our study also showed the factors that impact LOVOT acceptance among older adults with dementia and family partners.
Strengths and limitations
Our study is unique, adding to the literature through multiple perspectives from diverse participants. One strength is the incorporation of patient and family partners; this allowed us to see perspectives on LOVOT from those with dementia, as well as from the caretakers interacting with people with dementia. Both of these perspectives are critical to further our understanding of how AI-enabled SARs have a place in LTC homes. Our family partners came from various ethnic backgrounds and had different levels of experience regarding dementia caretaking, reducing biases that may be attributed to a particular ethnic group or experience level. Our choice to use data from patient partners was also strength of this research project; previous papers relied on information collected from residents with more advanced forms of dementia. These patients had more difficulty answering complicated and imaginary questions, which required more advanced reasoning skills that would have deteriorated due to the progression of their condition. 27 Hence, this study utilized patient partners who exhibited milder forms of dementia and could still provide answers to the questions that may have been more difficult for LTC residents. This does, however, highlight the inevitable limitation that answers are unable to be drawn from patients with more advanced forms of dementia. To support broader participation, we conducted interviews via Zoom, telephone, and in-person. This flexible approach addressed potential accessibility barriers, particularly for participants who faced challenges with digital technology.
While our study adds to the literature by sharing the perspectives of older adults with dementia and family partners, we had some limitations. One limitation of our study was the various methods for conducting the interviews, which may have introduced biases. Partners may have behaved or answered differently without the physical researcher's presence under the observer effect. Thus, partners who had the interviews in-person may have subconsciously answered differently than they would have if it were conducted remotely. The distribution of patient partners was another limitation of this study, as females were significantly overrepresented; 75% of patient and family partners were female. This could affect the data, as the caring nature of women may contribute to their favorable opinions of LOVOT; we saw this in one of our family partners, who consistently compared LOVOT's behaviors to those of a small child. Future research could attempt to control these confounding variables or study them independently to learn about trends in respective groups. Additionally, we also recognize that the role of the staff is not limited to facilitating SAR but also in creating a supportive and engaging environment. While our study focused on the staff education, other important roles of staff presence were not explicitly mentioned in our study. The future study could incorporate how the staff not only facilitate SAR but also create an open, judgment-free space, allowing for interaction with LOVOT in more personalized and imaginative ways.
Conclusion
This critical reflection highlights the perspectives of older adults with dementia and family partners on the use of the AI-enabled SAR, LOVOT, in LTC. Older adult partners/co-researchers identified meaningful benefits alongside important limitations and ethical concerns. Their insights emphasize the value of involving people with lived experience in decisions about technology adoption. Including older adults in research is essential to understanding what technologies truly support dignity, connection, and quality of life in care settings. Future research should address the concerns identified from this study and continue to center the voices of older adults to guide ethical design, implementation, and evaluation of socially assistive technologies in LTC.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076251393299 - Supplemental material for Perspectives on artificial intelligence-enabled socially assistive robots in long-term care: Experiences with LOVOT among people with dementia and family caregivers
Supplemental material, sj-docx-1-dhj-10.1177_20552076251393299 for Perspectives on artificial intelligence-enabled socially assistive robots in long-term care: Experiences with LOVOT among people with dementia and family caregivers by Kayoung Lee, Joey Oi Yee Wong, Karen Lok Yi Wong, Jeffrey Wong, Javier Cabrera-Guerra, Riea Singh, Arwen Fong, Ray Lou, Jim Mann, Lynn Jackson and Lillian Hung in DIGITAL HEALTH
Footnotes
Acknowledgements
We would like to thank Bonnie Hyunh for helping with the transcript cleaning.
ORCID iDs
Ethical considerations
This paper is part of a larger study on the implementation of LOVOT in long-term care (LTC) settings. This manuscript presents a critical reflection co-authored by patient and family partners drawing on their own perspectives lived experiences. The University of British Columbia Behavioural Research Ethics Board was consulted, and as this is a critical reflection paper, consent was not required.
Consent to participate
We have verbal consent for all partners to participate in our reflection and for publication.
Consent for publication
Not applicable.
Author contributions
Conceptualization – KL, JOYW, KLYW, LH; Investigation – KL, JOYW, JM, LJ, LH; Data analysis – KL, JOYW, JW, JCG, RS, AF, RL; Writing the original draft – KL, JOYW, KLYW, JW, JCG, RS, AF, RL, LH; Editing and revising the draft – KL, JW, JM, LJ, LH.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by funding awarded to LH from the Canada Research Chairs Program [grant number: GR021222].
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
Data from this study is available from the corresponding author (LH) upon request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.