
Abstract
Objective
This nationwide study aimed to assess the attitudes and awareness of artificial intelligence (AI) among nurses in Palestine to develop targeted strategies to support nurses in adapting to AI innovations while ensuring high-quality, patient-centered care.
Methods
The study was a nationwide quantitative, descriptive cross-sectional survey across seven governmental and private hospitals (N = 2132 nurses; n = 290 respondents) in Palestine between first of April and end of May in 2025. Inclusion: registered nurses employed at one of the seven target hospitals who consented. Exclusion: nurses working in nontarget hospitals, non-nursing health professionals, and nurses not actively on hospital duty. Data were collected via a self-administered questionnaire comprising: (a) sociodemographics and work characteristics; (b) attitudes toward AI measured by the General Attitudes toward Artificial Intelligence Scale (validated; present sample reliability: attitude α = 0.75); and (c) AI awareness (7 dichotomous items; previously validated; present study α = 0.77).
Results
The findings showed that slightly more than half of the participants had adopted some form of AI technology (55.5%), with ChatGPT being the most widely used. Despite over half using AI tools, a majority reported limited awareness, underscoring a knowledge gap. Most nurses viewed AI positively, though a substantial portion remained skeptical, reflecting both openness to and hesitation toward its adoption in the profession.
Conclusion
There is a need for targeted policies and education to enhance AI awareness and acceptance among nurses. The nursing education curriculum needs to be supplemented with courses on AI using case scenarios and incorporate simulation-based training. There should be increased funding for continuing education programs, and the organizational culture needs to be made supportive of these changes. Policies and education of AI, should emphasize ethical use, patient privacy, and accountability to build trust and reduce fear of AI replacing nurses.
Introduction
Artificial intelligence (AI) is progressively reshaping healthcare at a time when demand for digital literacy and AI-related competencies in the labor market has become imperative. Globally, AI is regarded as a disruptive force capable of transforming care delivery through automation, predictive analytics, and personalization of treatment.1,2 By automating repetitive administrative tasks and streamlining workflows, AI reduces the burden on healthcare personnel, thereby freeing time for direct patient care. 3 Equally important, AI facilitates early disease detection and preventive intervention by identifying at-risk patients through predictive algorithms and supporting the development of individualized treatment strategies. 4 Wearable devices and Internet of Medical Things platforms further enable real-time monitoring of patients’ health status, supporting timely responses to clinical deterioration.5,6 Collectively, these innovations hold substantial promise for improving patient outcomes and enhancing the efficiency of healthcare systems.
In addition to clinical benefits, AI improves patients’ access to healthcare by enabling self-service tools, enhancing data management, and facilitating virtual consultations. 7 Nevertheless, despite these advances, obstacles persist. A consistent barrier across healthcare systems is the limited awareness and preparedness of healthcare professionals, which constrains AI's effective implementation. Recent surveys suggest that only a minority of practitioners, around 25%, report confidence in their ability to use or interpret AI technologies.8,9 This digital skills gap underscores the urgency of integrating AI education into both undergraduate curricula and continuing professional development to ensure safe and effective use of AI in healthcare.10,11
The applications of AI in nursing are especially noteworthy. Artificial intelligence–enabled clinical decision support systems can analyze large datasets to assist nurses in diagnosing conditions, planning individualized care, and monitoring patients’ vital signs continuously. 12 Automation of routine documentation and scheduling reduces administrative overload, allowing nurses to focus more on patient-centered tasks. 13 Furthermore, AI enhances interdisciplinary collaboration by improving communication and coordination among healthcare teams. 14 However, for these benefits to materialize, nurses must be adequately trained to use AI responsibly and effectively. Insufficient training and limited awareness may foster resistance, misperceptions, or ethical concerns, thereby hindering adoption.15,16
Despite rapid global progress, significant disparities exist between countries in AI adoption. Advanced health systems are actively incorporating AI into hospitals and clinics, while resource-limited contexts face infrastructural, financial, and regulatory challenges.17,18 In Palestine, AI applications in healthcare remain scarce. Barriers include limited digital infrastructure, lack of funding, insufficient institutional support, and low awareness among healthcare professionals.19,20 Additionally, there is a shortage of empirical studies exploring how AI can be leveraged to enhance patient care in Palestinian hospitals.21,22
Given the central role of nurses as the largest workforce in healthcare and their frontline engagement with patients, their readiness to adopt AI is pivotal to successful implementation. Although international studies have examined nurses’ attitudes and awareness toward AI,23–25 evidence from Palestine is absent. Understanding Palestinian nurses’ perspectives is especially critical given the unique contextual challenges, including political instability, resource constraints, and fragmented healthcare systems.
Theoretical framework
This study is underpinned by two complementary frameworks that explain how healthcare professionals perceive and adopt AI technologies: the Technology Acceptance Model (TAM) and Rogers’ Diffusion of Innovation (DOI) Theory.
The TAM, originally proposed by Davis, 26 emphasizes two key determinants of technology adoption: perceived usefulness (PU) and perceived ease of use (PEOU). In nursing practice, PU may reflect whether nurses believe AI tools enhance efficiency, decision-making, or patient care outcomes, while PEOU captures the perceived effort required to learn and apply AI systems in clinical settings. Previous studies in healthcare demonstrate that both constructs significantly influence professionals’ attitudes toward AI and their subsequent intention to use such systems.27,28 By applying TAM, this study seeks to clarify how nurses’ perceptions of AI's benefits and usability affect their overall acceptance and willingness to integrate AI into their workflows.
In addition, Rogers’ DOI Theory provides a broader sociocultural lens to understand how new technologies are adopted within healthcare organizations. According to DOI, five attributes—relative advantage, compatibility, complexity, trialability, and observability—determine adoption rates. 29 Within the nursing context, relative advantage relates to AI's ability to improve patient care compared to existing methods; compatibility refers to alignment with nurses’ values and workflows; complexity highlights perceived difficulties in understanding AI; trialability indicates opportunities for pilot use; and observability reflects the visibility of AI's positive outcomes in clinical practice. These attributes directly shape nurses’ awareness, attitudes, and readiness for adoption.
Integrating these frameworks is particularly relevant in Palestine, where digital infrastructure and institutional support for AI remain limited. By combining individual-level determinants (TAM) with organizational and contextual factors (DOI), this study provides a comprehensive theoretical basis for examining how nurses’ awareness and attitudes toward AI are shaped. 30 This framework also informs the interpretation of demographic differences, such as variations in acceptance by age, education, or institutional type. Ultimately, the theoretical framework suggests that improving awareness (knowledge of AI concepts and applications) and addressing attitudinal barriers (concerns about complexity, risks, and ethical issues) are prerequisites for enhancing AI adoption among nurses.
Methods
Aim and research questions
The purpose of this study was to assess the attitudes and awareness of Artificial Intelligence among nurses in Palestine to develop targeted strategies to support nurses in adapting to AI innovations while ensuring high-quality, patient-centered care.
The research questions were:
What are the attitudes toward AI among nurses in Palestinian hospitals? What is the awareness of AI among nurses in Palestinian hospitals? Is there any statistically significant difference in the level of awareness of AI among nurses in Palestinian hospitals based on their demographics (age, sex, educational level)? Is there any statistically significant difference in attitudes toward AI among nurses in Palestinian hospitals based on their demographics (age, sex, educational level)?
Research design
A descriptive cross-sectional study was used to assess the AI attitudes and awareness of nurses in Palestinian hospitals.
Participants and settings
The study was conducted in (n = 7) major private and governmental Palestinian hospitals in Palestine, with the target population consisting of 2132 nurses working in these hospitals: Al-Makassed Governmental Hospital, Beit-Jala Governmental Hospital, Alia Governmental Hospital, Arab Society for Specialized Rehabilitation Hospital, Al-Mezan Specialized Hospital, Al-Ahli Hospital, and Palestine Governmental Medical Complex Hospital. Data were collected from the nursing staff through a self-administered questionnaire.
Sampling and sample size
The sample size was calculated based on Online Sample Size Calculator, with a population size of 2132 nurses in Palestine, a 5% margin of error, a 50% population proportion, and a 90% confidence level, the required sample size is 242 nurses. A total of 290 questionnaires were distributed, and 100% were responded to; thereby providing a sample size that was adequate for the study population. The type of sample was convenience sampling technique.
Participants must meet the following criteria:
Inclusion criteria:
Nurses working in the specified Palestinian governmental and private hospitals. Nurses who agree to participate during the data collection period.
Exclusion Criteria:
Participants were excluded if they met any of the following conditions:
Nurses working in other Palestinian hospitals were not mentioned in the study. Health professionals other than nurses, such as pharmacists, lab technicians, and doctors. Nurses who were not actively working in hospitals during the data collection period.
Instruments
A valid and reliable self-administered questionnaire was obtained from previous literature. 31 The questionnaire, composed of three parts, explains the data collection procedure, introduces the study, and ensures the privacy and confidentiality of the provided information.
Part I:
Investigates participants’ sociodemographic data, including sex, marital status, age, place of residence, educational level, years of nursing experience, type of institution, type of unit, work shift, monthly income, technology and AI Usage in the Workplace, and training and Experience in AI.
Part II:
This section consists of 20 items. It is a 5-point Likert-type scale ranging from 1 (strongly disagree) to 5 (strongly agree). It measures the nurses’ attitudes toward the application of AI in healthcare settings.
Part Ill:
This section consists of seven items measured as “Yes or No” questions to assess the level of nurses’ awareness of common terms of AI used in healthcare. This part is a previously validated instrument, and the tool's internal consistency of the used subscales was shown by Cronbach's alpha values of 0.795. 32
Instrumentation validity and reliability:
The researchers utilized a valid and reliable published and previously developed tool, the “General Attitudes Toward AI Scale (GAAIS),” to assess nurses’ attitudes toward the use of artificial intelligence technologies in clinical practice. The GAAIS exhibited good convergent and divergent validity with a related scale. The internal consistency of the study scales, as measured by Cronbach's Alpha, indicates good reliability: attitude (α = .75) and awareness (α = .77).33,34
Data collection
After obtaining the required ethical approvals, we visited the nurses in the targeted hospitals, informed them about the study, and introduced them to it. The purpose and importance of the study were also explained, and participants’ questions and concerns were addressed throughout the study. Targeted nurses were assured that their participation in this study was voluntary, without any direct or indirect harm. Data collection was between first of April 2025 and end of May 2025.
Data analysis
The collected data were analyzed by the Statistical Package for Social Sciences Version 27. Data analysis of descriptive and inferential statistics was conducted. Regarding descriptive statistics, frequency, percentages, mean score, and standard deviation (SD) were used to describe the study variables. Regarding inferential statistics, independent t-test and one-way ANOVA were used to assess the difference between study variables after assessing the normality of the data using the Kolmogorov–Smirnov and Shapiro–Wilk tests (p ≥ 0.05) and confirming data from a normally distributed population.
Ethical considerations
Ethical approvals were obtained from Al-Quds University with Ref No: (RESC/2025-42), in addition to the IRBs from the settings data were collected. The authors first contacted the administrations of the hospitals where the questionnaires were distributed. As befits research involving human participants, strict ethical principles were adhered to. Once identified, participants were assured of their right to anonymity, confidentiality, and the ability to withdraw from the study at any time. Further, they were informed that any information they provided would not be used against them. Additionally, they were reassured that their confidentiality and anonymity would be fully protected, and that controls were in place to maintain confidentiality and to prevent unauthorized access to the data. Participants were then asked to provide their written informed consent before taking part in the study.
Results
Sociodemographic characteristics
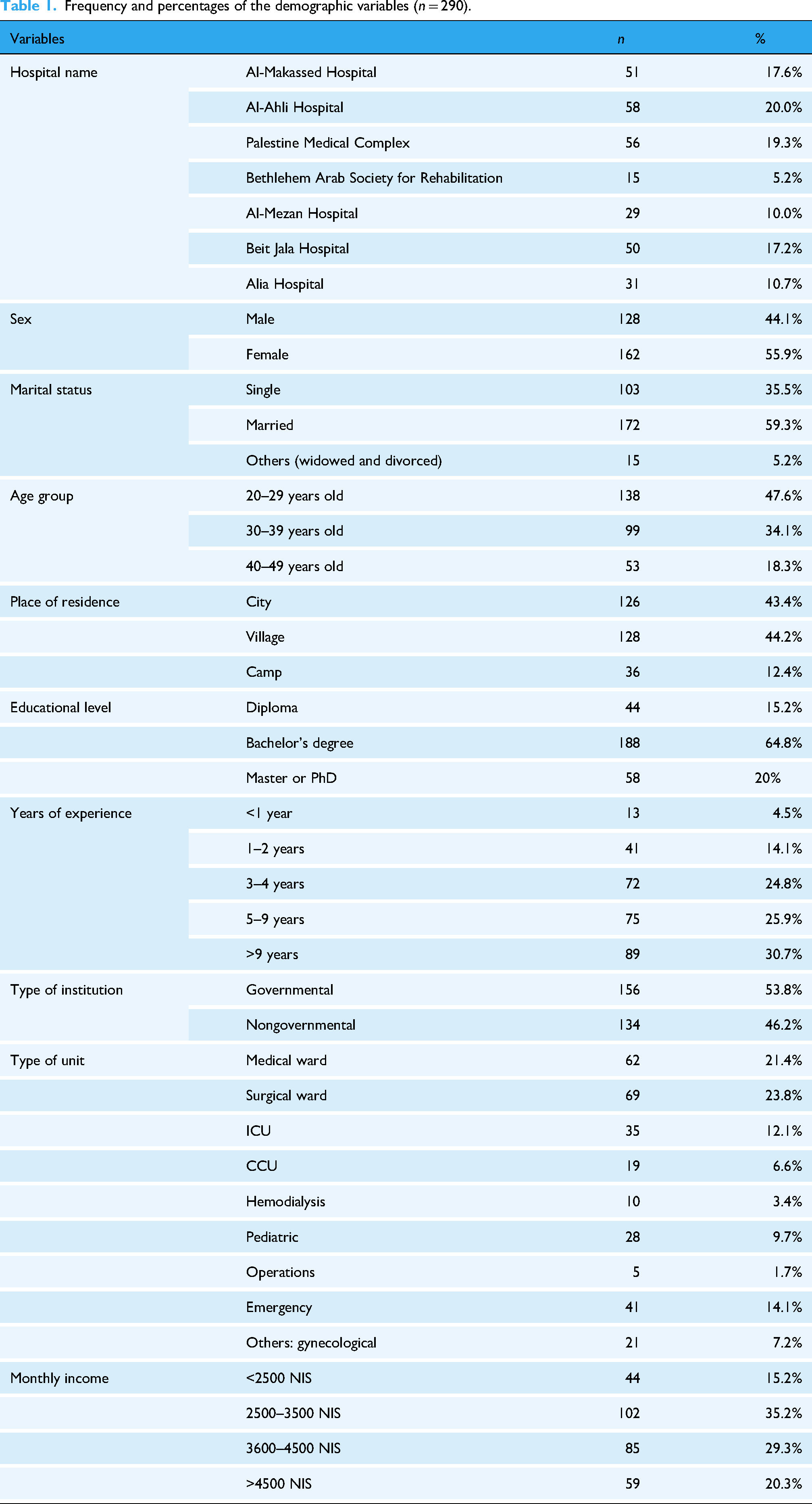
The current study included 290 participants. Most were from Al-Ahli Hospital (n = 58, 20.0%) and Palestine Medical Complex (n = 56, 19.3%). The majority were female (n = 162, 55.9%), married (n = 172, 59.3%), and aged 20–29 years (n = 138, 47.6%). Most lived in villages (n = 128, 44.2%) or cities (n = 126, 43.4%). Most of participants held a bachelor's degree (n = 188, 64.8%), with 30.7% having over 9 years of experience (n = 89). More than half worked in governmental institutions (n = 156, 53.8%). Common work areas included surgical (n = 69, 23.8%) and medical wards (n = 62, 21.4%). Shift work was split between double shifts (n = 133, 45.8%) and day shifts (n = 131, 45.2%). Most earned 2500–3500 NIS monthly (n = 102, 35.2%), as seen in Table 1.
Frequency and percentages of the demographic variables (n = 290).
Artificial intelligence–related information
Out of 290 nurses, 161 (55.5%) reported having used AI. Among those who used AI, the most used tool was ChatGPT (35.2%). Regarding formal training or education in AI or related technologies such as machine learning or health informatics, 171 participants (59.0%), reported receiving no training, while the majority as seen in Table 2.
Artificial intelligence–related information (n = 290).

Level of attitude toward AI Among nurses
The pie chart shows that more than half of the nurses (n = 171, 59%) held a positive attitude toward AI, as seen in Figure 1.
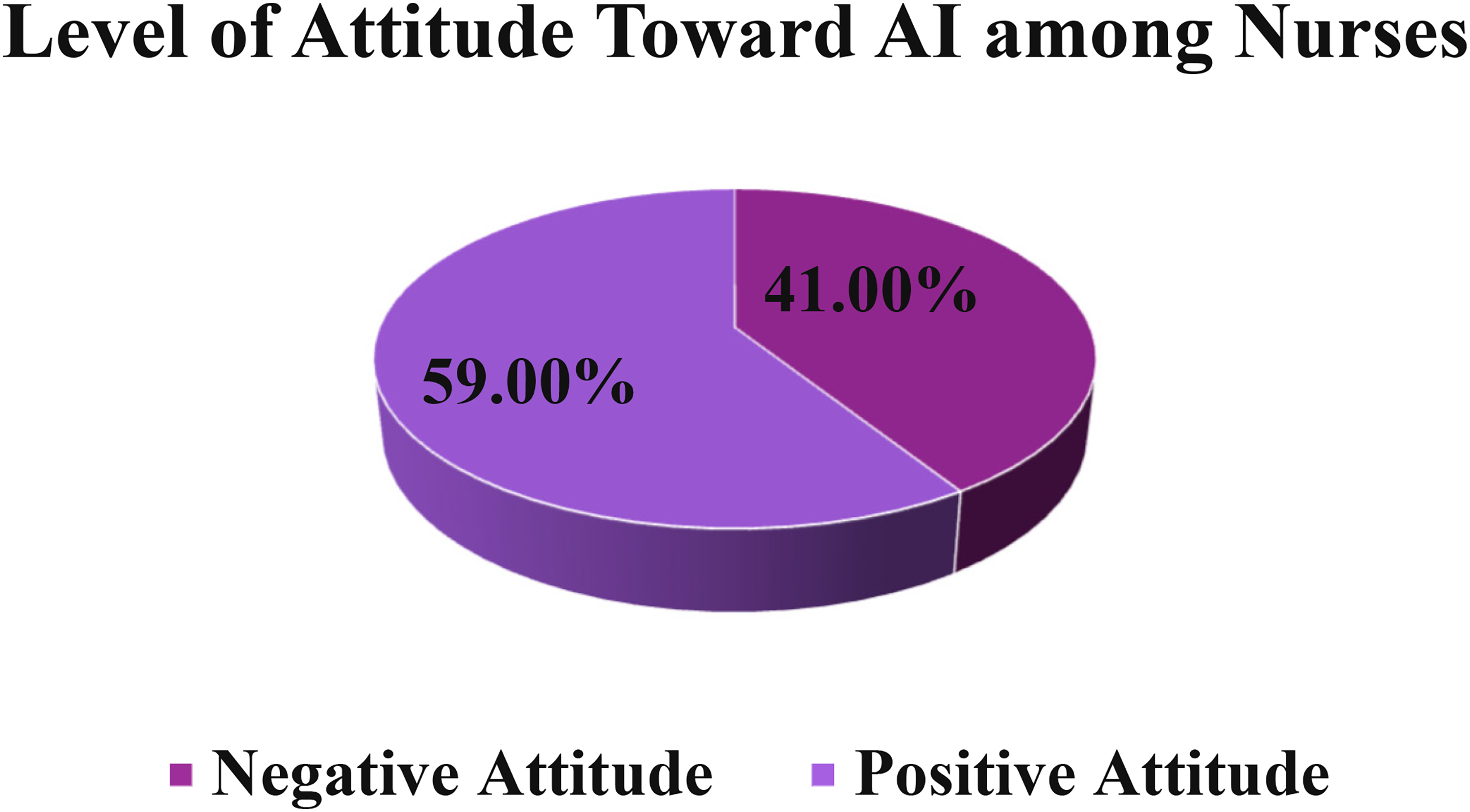
Level of attitude toward artificial intelligence (AI) among nurses.
The results showed that nurses held a slightly positive overall attitude toward AI, with a total mean score of (M = 3.01, SD = 0.36). In the Perceptions domain, attitudes were positive (M = 3.09, SD = 0.695). Nurses agreed that AI is exciting (M = 3.18, SD = 1.11), impressive (M = 3.15, SD = 1.12), and beneficial for well-being (M = 3.11, SD = 1.12), but showed concern about AI taking control (M = 2.88, SD = 1.13). The Concerns and Risks domain had a slightly negative attitude (M = 2.99, SD = 0.58), with participants recognizing AI's societal benefits (M = 3.15, SD = 1.09) yet expressing worry about potential harm (M = 2.99, SD = 1.04), errors (M = 2.90, SD = 1.05), and danger (M = 2.87, SD = 1.16). In Workplace Integration, attitudes were negative (M = 2.89, SD = 0.82), with low agreement on using AI at work (M = 2.99, SD = 1.15) or preferring AI over human interaction (M = 2.84, SD = 1.02). The Ethical and Societal Implications domain was slightly positive (M = 3.05, SD = 0.77), reflecting mixed views, including concerns about AI misuse (M = 3.15, SD = 1.09) and surveillance (M = 2.94, SD = 1.05) (see Table 3).
Mean score for attitude subdomains toward AI among nurses (n = 290).

Cutoff points (<3 = Negative attitude, ≥3 = Positive attitude).
*Reverse coded.
Level of awareness toward AI Among nurses
The bar chart titled “Level of Awareness Toward AI Among Nurses” indicates that most nurses (60.3%) were not aware of AI, as seen in Figure 2.

Level of awareness toward artificial intelligence (AI) among nurses (median = 4) (<4 = not aware, ≥4 = aware).
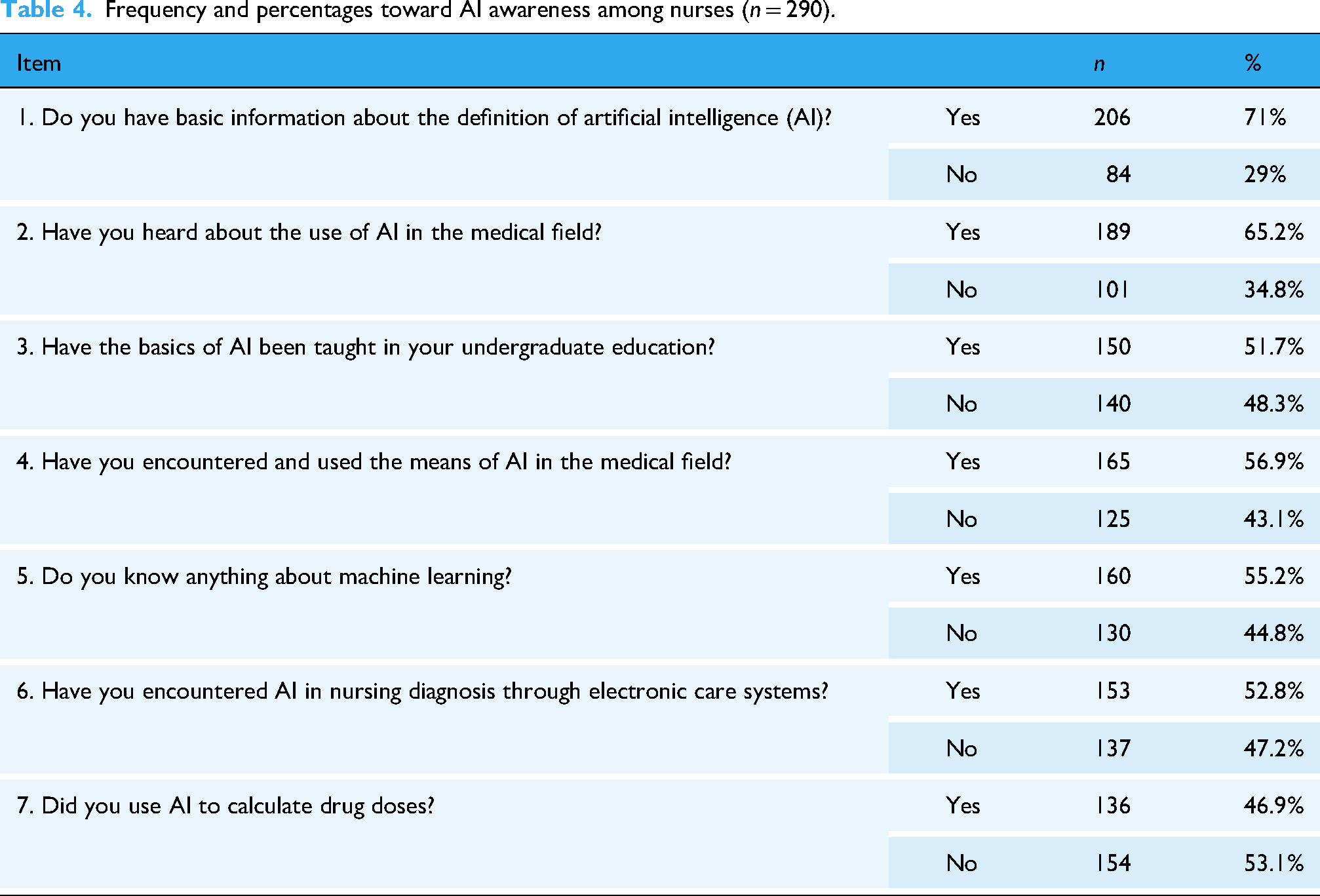
Out of 290 participants, 206 (71.0%) reported having basic information about the definition of AI. A total of 189 (65.2%) had heard about the use of AI in the medical field, and 150 (51.7%) stated that the basics of AI had been taught in their undergraduate education. Furthermore, 165 (56.9%) encountered and used AI tools in the medical field, and 160 (55.2%) indicated that they knew something about machine learning. Artificial intelligence use in nursing diagnosis through electronic care systems was reported by 153 (52.8%) participants, while 136 (46.9%) mentioned having used AI to calculate drug doses, as seen in Table 4.
Frequency and percentages toward AI awareness among nurses (n = 290).
Differences between demographic variables of nurses in terms of attitude toward AI
Among the demographic variables examined, statistically significant differences in nurses’ attitudes toward AI were found based on hospital name (p = 0.034) and type of institution (p = 0.016). Post hoc tests indicated that nurses from the Palestine Medical Complex reported the highest mean attitude score (M = 3.11, SD = 0.34), while those from Alia Hospital had the lowest (M = 2.87, SD = 0.28), suggesting that the institutional setting may influence perceptions of AI. Additionally, nurses working in nongovernmental institutions demonstrated slightly better attitudes (M = 4.06, SD = 2.04) compared to those in governmental institutions (M = 3.98, SD = 2.16). No statistically significant differences were observed in attitudes based on sex, marital status, age, place of residence, educational level, years of experience, unit type, shift work, or monthly income, as seen in Table 5.
Differences between demographic variables of nurses in terms of attitude toward AI (n = 290).

Independent t-test and one-way ANOVA.
*Significant at p-value ≤ 0.05.
CI: confidence interval.
Discussion
The main purpose of this study was to assess the attitudes and awareness of AI among nurses in Palestine, with the ultimate goal of informing strategies that facilitate their adaptation to AI innovations while safeguarding high-quality, patient-centered care. The findings illustrate a mixed but important picture: while over half of the respondents had adopted AI tools in some form, awareness levels remain low, and attitudes toward AI were divided, reflecting both enthusiasm and resistance. These outcomes resonate with global literature but also highlight contextual challenges unique to Palestine.
Attitude toward AI
Overall, 59% of nurses expressed positive attitudes toward AI, while 41% held negative views. This reflects cautious optimism but highlights persistent skepticism. Positive attitudes often stem from PU, such as efficiency gains, enhanced diagnostic support, and improved patient care. Negative perceptions, however, are rooted in concerns about ethical risks, potential errors, and fears of AI replacing human roles, which align with previous findings in nursing and medical literature.35–37
The TAM provides a valuable lens for interpreting these findings. Nurses who perceived AI as useful and relatively easy to use demonstrated more favorable attitudes, while those perceiving AI as complex or threatening were more resistant.38,39 Rogers’ DOI theory also explains these dynamics: positive attitudes align with perceptions of relative advantage and compatibility, while negative views may arise from concerns about complexity, trialability, and lack of observability of AI's benefits. 40
Personality traits also influence receptivity. Tsiara et al. 41 reported that openness to experience among nursing students was positively correlated with favorable attitudes toward AI adoption. Similarly, Alruwaili et al. 31 found that reluctance to change was inversely associated with positive AI perceptions. These findings suggest that interventions must address both individual-level factors (confidence, openness, skills) and organizational-level enablers (policies, infrastructure).
Awareness of AI
Despite moderate adoption rates, only 39.7% of nurses demonstrated awareness of AI concepts and applications, indicating a substantial knowledge gap. Awareness is the foundation for responsible adoption, and its absence creates risks of misuse or superficial application.
These findings parallel research from Pakistan, where Naureen et al. 15 found that although 59.9% of nursing students had heard of AI in healthcare, only 43.8% possessed sufficient skills to engage with AI-related literature. Similarly, in Jordan, Migdadi et al. 16 reported low AI knowledge and attitudes among nursing students, underlining the regional need for curriculum reform. In a systematic review, Labrague and Aguilar-Rosales 17 confirmed that digital literacy, knowledge, and prior exposure were the strongest predictors of AI readiness in nursing students.
Globally, a lack of AI awareness among healthcare professionals has been reported as a persistent challenge. A systematic scoping review by O’Connor et al. 18 emphasized that inadequate training and poor awareness impede the safe integration of AI tools into clinical workflows. Similarly, Kelly et al. 19 noted that workforce preparedness remains one of the most critical barriers to realizing AI's clinical impact. One possible explanation for the limited awareness and adoption of AI among nurses in Palestine is that cultural and systemic barriers—exacerbated by the country's low-income status and ongoing political conflict—may hinder the integration of AI in healthcare practice.
Thus, bridging the awareness gap requires integrating AI-related competencies into undergraduate and postgraduate nursing curricula, as well as providing continuing education programs that enhance digital literacy, critical thinking, and ethical use of AI technologies.
Differences between variables for both attitude and awareness
Significant differences were found in attitudes across institutional settings, with nurses at the Palestine Medical Complex reporting the most positive perceptions (M = 3.11), while those at Alia Hospital reported the lowest (M = 2.87). These disparities suggest that institutional climate and resource availability are stronger determinants of attitudes than individual demographic variables such as resources, leadership support, and digital infrastructure. Research by Alruwaili et al. 14 and Ahmad et al. 20 supports this, highlighting the role of organizational policies, leadership support, and infrastructure in shaping willingness to adopt AI.
Interestingly, while younger nurses (20–29 years) showed higher awareness, no significant differences were observed in attitudes across sex, education, or years of experience. This finding aligns with international literature showing that digital natives are generally more open to emerging technologies due to greater exposure. 21 However, the lack of broad demographic differences underscores that institutional readiness, rather than individual characteristics, may be the primary driver of AI adoption in clinical nursing practice.
Limitations
Three constraints of this study should be noted. First, the results may not be generally applicable to nurses in other areas or healthcare systems, as the data were gathered from a particular set of nurses inside certain hospitals, knowing that Gaza was excluded due to the political conflict and inability to collect data from this area. Second, the use of convenience sampling and self-reported surveys might introduce response bias, which may negatively impact the generalizability of the findings given Palestine's ongoing topographical difficulties and fragmentation. Third, the cross-sectional design cannot capture evolving attitudes as AI exposure increases. Therefore, future studies should use a larger sample size that represents all geographic areas to enhance the internal validity and generalizability of the findings. Interventional research, including putting in place AI education programs, may also assist Palestinian nurses in learning, adjusting to, and becoming proficient with new AI-based medical technologies.
Conclusion
This study sought to assess the adoption, perception, and awareness of AI by nurses, as well as the effect of selected demographic characteristics on these factors. Findings showed that slightly more than half of the participants had adopted some form of AI technology (55.5%), with ChatGPT being the most widely used. Despite these technological advances, a large proportion of nurses, 60.3%, remained unaware of AI, demonstrating a significant knowledge gap. Concerning perceptions, most nurses, 59%, viewed AI positively, while 41% held negative views; this indicates some willingness to accept AI, yet strong reluctance within the profession. The demographic analysis showed that perceptions toward AI differed significantly by institution, with nurses working at the Palestine Medical Complex showing the most positive attitudes. Moreover, AI awareness was significantly higher among younger nurses aged 20–29, which suggested an age difference regarding the level of exposure and adaptability to new technologies. Lastly, it is highly advised that thorough AI literacy modules be incorporated into nursing programs for undergraduate students and that practice-focused, hospital-based AI workshops be established to give nurses the know-how to use AI technologies in clinical decision-making and patient care.
Study implications in nursing
This study underscores the urgent need to develop structured educational and organizational strategies to enhance nurses’ awareness and acceptance of AI. At the educational level, undergraduate curricula must incorporate AI literacy, covering machine learning basics, ethical frameworks, and clinical decision support systems. Simulation-based training could further build confidence and demonstrate AI's potential benefits in real-time clinical scenarios. 22
At the organizational level, healthcare institutions in Palestine should promote a supportive culture for AI adoption by ensuring access to digital infrastructure, creating opportunities for trial use (pilot projects), and addressing ethical concerns through clear policies. National policymakers should allocate funding for AI education, establish regulatory frameworks to address data privacy and algorithmic bias, and create cross-disciplinary platforms for knowledge exchange.23,24
From a theoretical standpoint, this study validates the relevance of TAM and DOI in explaining nurses’ adoption behaviors. Improving perceptions of usefulness, ease of use, compatibility, and trialability while reducing perceptions of complexity and risk are crucial for increasing adoption rates. These insights provide a framework for designing interventions that simultaneously target individual confidence and organizational readiness.
Footnotes
Acknowledgements
Authors would like to thank all nurses who participated in this study.
Ethical approval
Approvals were obtained with help of the Al-Quds University Ethical Committee with (Ref. No.: RESC/2025-42). In addition, IRBs were obtained from the hospitals where the questionnaires were distributed. The first step was to distribute the questionnaires and then each participant provided written informed consent before taking part in the study, they were assured of their right to anonymity, confidentiality and the ability to withdraw from the study at any time. Since the research involves human participants, adherence to strict ethical principles was essential, participants were informed that their consent was required and that any information that they provided would not be used against them, additionally they were reassured that their confidentiality and anonymity would be fully protected, measures were taken to maintain confidentiality by preventing unauthorized access to the data.
Contributorship
AA, SA, and AT: Conceptualization, Methodology, Software, Data curation, Validation, Resources, Project administration, Formal analysis, Visualization, Writing—original draft, Writing—review & editing. RH and LH: Methodology, Writing—original draft, Validation. AA, SA, MK, BS, YG, BH, CD, NZ, and ATs: Writing—original draft, Writing—review & editing, Formal analysis, Supervision, Validation, Visualization, Methodology, Investigation.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
All listed authors meet the authorship criteria and that all authors agree with the content of the manuscript. The data that support the findings of this study are available from the corresponding author upon reasonable request.