
Abstract
Introduction
Worldwide, healthcare systems aim to achieve the best possible quality of care at an affordable cost while ensuring broad access for all populations. The use of artificial intelligence (AI) in healthcare holds promise to address these challenges through the integration of real-world data-driven insights into patient care processes. This study aims to assess nurses’ awareness and attitudes toward AI-integrated tools used in clinical practice.
Methods
A descriptive cross-sectional design captured nurses’ responses at three governmental hospitals in Saudi Arabia by using an online questionnaire administered over 4 months. The study involved 220 registered nurses with a minimum of one year of clinical experience, selected through a convenience sampling method. The online survey consisted of three sections: demographic information, an assessment of nurses’ AI knowledge, and the general attitudes toward the AI scale.
Results
Nurses displayed “moderate” levels of awareness toward AI technology, with 70.9% having basic information about AI and only 58.2% (128 nurses) were considered “aware” of AI as they dealt with one of its healthcare applications. Nurses expressed openness to AI integration (M = 3.51) on one side, but also had some concerns about AI. Nurses expressed conservative attitudes toward AI, with significant differences observed based on gender (χ² = 4.67, p < 0.05). Female nurses exhibited a higher proportion of negative attitudes compared to male nurses. Significant differences were also found based on age (χ² = 9.31, p < 0.05), with younger nurses demonstrating more positive attitudes toward AI compared to their older counterparts. Educational background yields significant differences (χ² = 6.70, p < 0.05), with nurses holding undergraduate degrees exhibiting the highest positive attitudes. However, years of nursing experience did not reveal significant variations in attitudes.
Conclusion
Healthcare and nursing administrators need to work on increasing the nurses’ awareness of AI applications and emphasize the importance of integrating such technology into the systems in use. Moreover, addressing nurses’ concerns about AI's control and discomfort is crucial, especially considering generational differences, with younger nurses often having more positive attitudes toward technology. Change management strategies may help overcome any hindrances.
Introduction
Healthcare systems globally confront notable obstacles in attaining the objectives of the “quadruple aim” in healthcare, which include enhancing population health, improving patient care experience, increasing caregiver satisfaction, and mitigating the escalating costs of healthcare. 1 Moreover, healthcare systems encounter the challenge of delivering effective, high-quality care and orchestrating large-scale transformations. This necessitates incorporating real-world data-driven insights directly into patient care processes.2,3 Integrating technology and artificial intelligence (AI) in healthcare holds promise for addressing these supply-and-demand challenges.2,3 The term “AI” refers to a high-performance computerized setup that can perform similar tasks to humans in a more effective manner.4,5 These include research, gathering information, acquiring knowledge, making predictions, and helping in making decisions.4,5 AI-integrated systems can anticipate and address issues proactively, operating with intention, intelligence, and adaptability. Their strength lies in learning from large data sets to recognize patterns and relationships, and they remain dynamic and autonomous, evolving with the availability of more data.4,5
AI is defined as the simulation of human intelligence processes by machines, especially computer systems.5,6 These processes include learning (the acquisition of information and rules for using the information), reasoning (using the rules to reach approximate or definite conclusions), and self-correction.5,6 Particularly in healthcare, AI technologies, which encompass machine learning algorithms, and natural language processing, promise to revolutionize diagnostic and therapeutic processes by enhancing decision-making through robust data-driven insights and facilitating automation in routine tasks.5–7
Healthcare systems worldwide aim to enhance patient outcomes, optimize cost management, and expand access to services. 8 AI is integral to addressing these challenges by improving the accuracy of diagnostics, personalizing treatment protocols, and managing patient care more efficiently. 8 These capabilities are critical as healthcare providers strive to balance quality care delivery with cost-efficiency and accessibility in increasingly complex healthcare environments. 9 In alignment with Saudi Arabia's Vision 2030, which prioritizes innovation in healthcare, AI's integration into this sector is accelerating. 10 AI applications are notably effective in diagnostics support, patient monitoring, personalized medicine, and administrative processes. 11
The practice of nursing was significantly affected in the last decade by the introduction of AI. 12 As for nurses, many gaps still exist where nurses are not yet involved in the process of developing, integrating, and implementing AI in healthcare, especially since they are among the most involved professions with AI technology applications and functions. 13 It has also been shown that the use of AI may improve the proactiveness of patient treatment regimens by processing many repetitive tasks efficiently. At the same time, those tasks are clinically relevant in the process of identifying and treating patients. 14 Nurses’ experiences with AI in terms of competence, understanding, reliability, and confidence in its potential as an alternative to human interventions in healthcare vary. Some nurses perceive AI as a threat to the presence of the human factor in the healthcare system, and reactions vary in terms of proponents and opponents.12,15 Involving nurses in the process of integrating AI into healthcare systems is suggested as it may enhance the functionalities of the AI applications. 7
Many AI programs have been developed to help treat patients and change the role of caregivers. 16 In the context of healthcare, AI is often viewed as the ability of a computer to independently transform data into knowledge to guide decisions or autonomous actions. 16 AI could help solve some of the problems facing the nursing profession, such as job dissatisfaction and unintended deficiencies in patient care (such as errors in the administration of medication and identification of at-risk clients).15,17 However, this may cause concerns among nurses, especially when it comes to incorporating new technologies into practice. 15 Smart technology may eventually be able to affect routinely performed nursing tasks, such as measuring vital signs, administering medications, and infection protocols, which may result in changing the role of nurses in the healthcare system. This new change may create a concern for nurses as they are moving out of their “comfort zone” by changing the way nursing tasks get done, in addition to the concern that AI-integrated technology can be used for surveillance and monitoring, thus invading the privacy of practitioners and patients.12,15,18 Nevertheless, nursing informatics, discussing the advancements in AI, has undergone noteworthy developments in the last two decades.
Advancements in AI technologies represent valuable tools for revolutionizing healthcare delivery.7,19 AI technologies, with their related products of predictive analytics, natural language processing, computer vision, and machine learning, may enable the extraction of actionable insights from data, enhancing clinical workflows, diagnostic accuracy, and treatment recommendations. 7 Nursing informatics helps to integrate information technology and nursing science to support evidence-based practice, streamline documentation, and improve communication among healthcare team members through electronic health records and clinical decision support systems. 7 These advancements serve as valuable tools that can assist nursing educators in reshaping their curricula and adapting their practices. 19
Despite significant advancements, these valuable tools have not been effectively utilized or promoted since their inception several years ago.19,20 Nursing professionals may lack the knowledge, skills, and confidence to see the utilization of AI and digital health approaches, which explains why these resources aren’t utilized, or viewed as utilized, widely. Therefore, to effectively present the integration of AI into clinical practice, we must first understand how nurses, as end users, think about and interact with current and future AI-integrated tools. Because nurses are the end users of the technology and interact directly with patients, it is critical to assess their current understanding of AI to determine future training needs. 21 The use of AI is not yet well understood among Saudi Arabian nurses, as little is known about their readiness, confidence, attitudes, and barriers to embracing AI in the clinical setting. This study aims to assess Saudi Arabian nurses’ awareness and attitudes toward AI-integrated tools and systems, addressing both barriers and enablers, to inform future training and facilitate the effective integration of AI-integrated technology in healthcare.
Study objectives
To assess the levels of awareness among Saudi nurses toward AI-integrated tools used in clinical practice.
To evaluate the attitudes of Saudi nurses toward AI-integrated tools used in clinical practice.
To explore the relationship between demographic factors and Saudi nurses’ awareness and attitudes toward AI-integrated tools.
Methods
Design
A descriptive cross-sectional design was employed to assess the nurses’ awareness and attitudes toward AI-integrated tools used in clinical practice.
Sampling and setting
The study was conducted in the northern region of Saudi Arabia, encompassing three main governmental hospitals located in the Jouf region (King Abdulaziz Hospital, Prince Mut'eb Hospital, and Domat Al-Jandal Hospital). A convenience sampling method was employed to enroll Saudi nurses from the health sector in the Kingdom of Saudi Arabia. The sampled nurses held various educational backgrounds, with 60.0% possessing a baccalaureate degree, 24.5% holding a master's degree, 13.6% having a diploma, and only 1.8% reporting a doctorate. The sample size was determined through a power analysis conducted with G*Power 3.0.10 software. In alignment with the available literature at that time, the researcher established a medium effect size (f = 0.25) using the chi-squared (χ2) test in comparing five groups (the maximum groups in demographic variables), adhered to a significance level of α = 0.05, and a power of 0.80. The computed necessary sample size was 191 nurses. However, a total of 220 nurses participated in the study, providing complete responses to the questionnaire, exceeding the anticipated recruitment target. The inclusion criteria for participants involved registered nurses in Saudi Arabia with at least one year of clinical experience, ensuring foundational insights into healthcare practices relevant to the comprehensive exploration of nurses’ awareness and attitudes toward AI.
Instrument
The researcher utilized a three-section instrument to address the aim of this study. The first section addresses the nurses’ characteristics including age, gender, marital status, level of education, years of nursing experience, shift worked, type of unit, and previous involvement with AI-integrated technology in healthcare settings. The second section is a previously validated instrument (Nurses’ AI knowledge questionnaire) by Swed et al. 22 to address the level of nurses’ awareness of AI. It consists of seven items measured as “Yes or No” questions to the common terms of AI used in healthcare. The tool's internal consistency of the used sub-scales was shown by Cronbach's alpha values of 0.795, as reported by Swed et al. 22 This section consists of seven items measured as “Yes or No” questions to assess the level of nurses’ awareness of common terms of AI used in healthcare. The third section is the 20-item General Attitudes toward AI Scale (GAAIS) developed by Schepman and Rodway. 23 It is a 5-point Likert-type scale ranging from 1 (strongly disagree) to 5 (strongly agree). It measures the nurses’ attitudes toward the application of AI in healthcare settings. The GAAIS demonstrated good internal consistency, with Cronbach alpha values of 0.88 for the Positive GAAIS (12 items) and 0.82 for the Negative GAAIS (8 items), as reported by Schepman and Rodway. 24 Additionally, the GAAIS exhibited good convergent and divergent validity with a related scale.23,24 Formal permission was secured from the original authors of the scales for their utilization, thereby ensuring adherence to copyright protocols.
Data collection
A total of about 350 nurses from King Abdulaziz Hospital, Prince Mut'eb Hospital, and Domat Al-Jandal Hospital were invited to participate in the survey. Nurses were encouraged to engage in the online survey through a provided “Google Forms” link. The selection of participants was conducted by the researchers, who collaborated with the nursing department managers of each hospital to ensure comprehensive coverage. The researchers emailed the survey link directly to the nursing department managers, who then facilitated the distribution of the survey link to the nurses under their supervision. The invitation email included detailed information about the study's objectives and requested participants’ consent. To proceed to the survey, participants had to click to confirm their consent, and completing the survey indicated their agreement to participate. Moreover, a web link invitation was shared with staff nurses via email and various social media platforms (Messenger, Instagram, and WhatsApp) to encourage wider participation. Emphasizing anonymity, participants were assured they could withdraw at any point before submission without consequences. The data was collected over four months (April to September 2023), accompanied by regular email reminders every second week. Missing data were handled by excluding cases with incomplete responses from the analysis. There was only one case with missing data for the variables analyzed in this study, which was excluded to ensure transparency in data reporting.
Statistical analysis
The study employed different statistical approaches involving descriptive and inferential analyses to investigate the viewpoints of Saudi Arabian nurses regarding the integration of AI in clinical practice. Descriptive statistics, such as frequencies and percentages, were utilized to extensively analyze nurses’ sociodemographic and clinical characteristics, encompassing various factors like gender, marital status, age, education levels, and work-related details. Similarly, frequencies and percentages were applied to assess nurses’ AI awareness and knowledge items. Mean scores and standard deviations were employed to summarize nurses’ attitudes toward AI across multiple scale items. The study also utilized the χ2 test to assess the significance of associations between categorical variables, specifically examining the relationship between various demographic factors (gender, marital status, age, level of education, and years of experience) and the attitudes of Saudi nurses toward AI.
Ethical consideration
The study obtained approval from the Bioethics Institutional Review Board at Jouf University (Approval no. 3-06-44, 7 February 2023), adhering to the principles outlined in the Helsinki Declaration. 25 To ensure confidentiality and anonymity, various measures were implemented, including assigning a distinct code number to each participating nurse and presenting all data in aggregated form. Electronic handling of data occurred through a password-protected account, and participants were granted electronic informed consent before completing the survey on a Google form.
Results
Sample characteristics
A total of about 350 nurses were invited to participate in the survey. In total, 220 nurses responded to the invitation, representing approximately a 62.9% response rate. A substantial proportion of nurses were female, constituting 73.6% of the sample. The marital status distribution indicated that a significant portion of participants were married (58.2%), while a smaller percentage reported being single (37.3%), and a few were either separated, divorced, or widowed (4.5%). Age-wise, the majority fell within the 30–39 years bracket (54.5%), with the 20–29 years group making up 27.3% of the participants. Educational background varied, with 60.0% of nurses holding a Baccalaureate degree, 24.5% having a Master's degree, and 13.6% possessing a Diploma. Only 1.8% reported having a Doctorate. In terms of nursing experience, over half of the participants (45%) had a decade or more of experience. Regarding employment details, a significant majority of nurses worked full-time (90.9%), with a smaller proportion engaged in part-time roles (9.1%). In terms of work shifts, 52.7% of nurses were assigned to day shifts, 44.5% had rotating shifts, and a minority worked night shifts (2.8%). Examining the type of units in which nurses were stationed, medical/surgical wards emerged as the most common (28.3%), followed by intensive care unit/critical care unit (ICU/CCU) at 22.7%. Obstetric/pediatric units constituted 8.1%, psychiatric units comprised 10.0%, and all other units collectively accounted for 30.9% of the responses (Table 1).
Frequencies of nurses’ sociodemographic and clinical characteristics (N = 220).
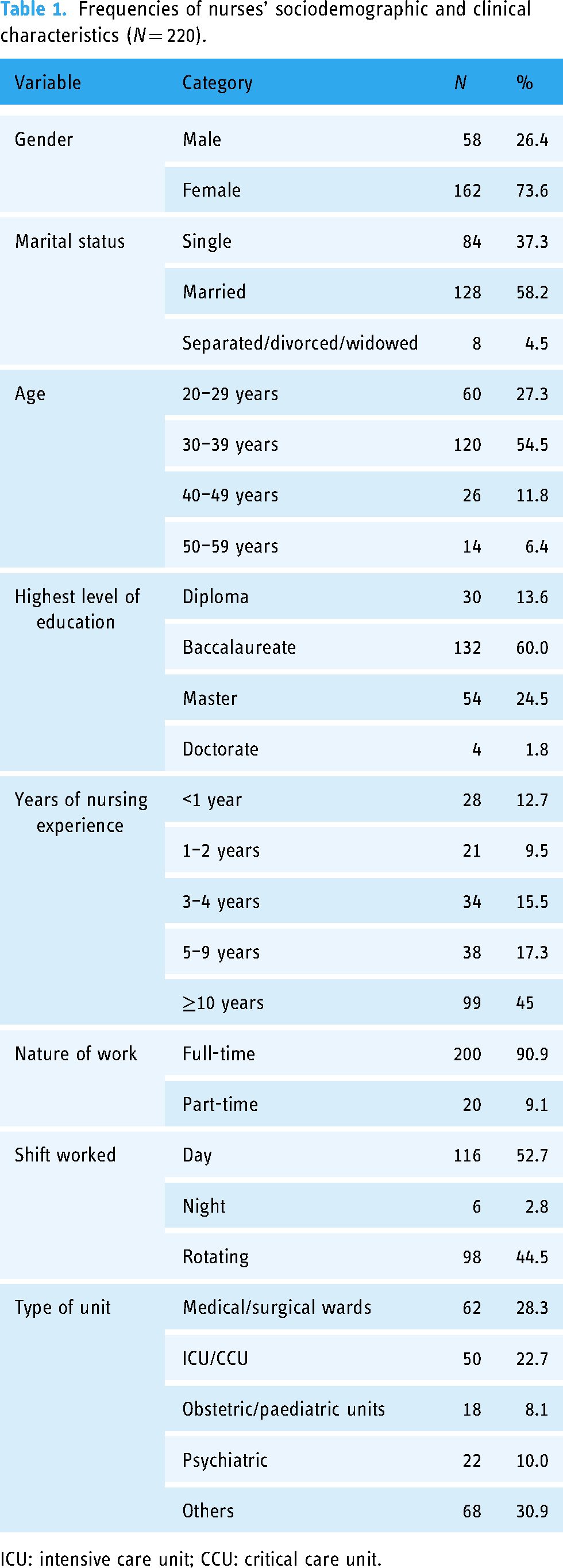
ICU: intensive care unit; CCU: critical care unit.
Nurses’ awareness toward AI
Table 2 presents the frequencies and percentages of nurses’ responses to items assessing their awareness regarding AI technology. For the definition of AI, 70.9% of nurses indicated having basic information, while 29.1% reported not having such knowledge. A substantial majority (67.3%) acknowledged being aware of the use of AI in the medical field, with 32.7% indicating no familiarity with AI applications. In terms of educational background, 39.1% of nurses reported that the basics of AI were covered in their undergraduate education, while the majority (60.9%) stated otherwise. Additionally, 58.2% of nurses reported encountering and using AI means in the medical field, whereas 41.8% had not. Concerning AI-integrated applications, 60.0% of nurses reported knowledge about it, while 40.0% indicated a lack of knowledge. Furthermore, 40.0% of nurses reported encountering AI in nursing diagnosis through electronic care systems, and 45.5% reported that they had used AI to calculate drug doses.
Nurses’ responses to awareness items (N = 220).

Nurses’ attitudes toward AI
Table 3 presents a comprehensive overview of nurses’ attitudes toward AI, encompassing perceptions, concerns, workplace integration, and ethical implications. In terms of perceptions (Items 1–8), nurses expressed moderate agreement on the beneficial applications of AI (M = 3.66) and an overall positive sentiment toward AI's capabilities. Notably, nurses scored high in their interest in incorporating AI into daily life (M = 3.51), indicating openness to AI integration. The lowest mean score was for the belief that much of society will benefit from a future full of AI, suggesting some reservations about widespread AI benefits. Regarding concerns and risks of AI (Items 9–13), nurses exhibited moderate apprehension about potential control by AI (M = 3.15) and personal consequences with increased AI use (M = 3.10). The perception that AI could make errors (M = 3.04) and the concerns associated with future AI uses (M = 3.02) were moderately expressed.
General attitudes of Saudi nurses toward AI (N = 220).

AI: artificial intelligence; Min: minimum score; Max: maximum score; M: mean; SD: standard deviation.
In terms of workplace integration (Items 14–17), nurses showed positive inclinations, particularly in their willingness to use AI-integrated tools in their jobs (M = 3.50). While recognizing the potential efficiency of AI-integrated tools in routine tasks (M = 3.08), nurses maintained a moderate perception of AI-integrated tools outperforming humans (M = 2.99). In terms of ethical and societal implications (Items 18–20), nurses expressed a moderate level of concern regarding the darker aspects of AI-integrated tools. Specifically, they indicated a perception of AI-integrated tools as having sinister attributes (M = 2.98), highlighting a cautious view of its potential negative consequences. Additionally, nurses reported a level of unease with the idea that AI could be employed for surveillance purposes (M = 2.88), suggesting a sensitivity to privacy and ethical considerations in the use of AI. The concern extended to organizations using AI unethically (M = 2.87), emphasizing nurses’ awareness and apprehension about the potential misuse of AI technologies.
Differences in nurses’ attitudes toward AI
Chi-squared (χ²) test was applied to determine if there were any significant differences in attitudes toward AI based on gender, marital status, age, level of education, and years of experience among Saudi nurses. Results listed in Table 4 revealed that a higher proportion of female nurses (41.4%) expressed negative attitudes toward AI compared to male nurses (10.5%), with statistically significant differences (χ² = 4.67, p < 0.05). However, when considering marital status, no significant differences were observed in attitudes toward AI between single/divorced (20%) and married nurses (26.4%) (χ² = 0.14, p = 0.71). Regarding age groups, nurses aged 20–29 years demonstrated the highest positive attitude toward AI (20.5%), whereas those aged 50–59 years exhibited the lowest (2.7%). Statistically significant differences were found across age categories (χ² = 9.31, p < 0.05). In terms of educational attainment, nurses with undergraduate degrees demonstrated the highest positive attitude toward AI (32.3%), followed by postgraduate degree holders (17.4%), and those with diplomas (5%). Significant differences were observed among educational levels (χ² = 6.70, p < 0.05). However, no significant variations in attitudes toward AI were found based on years of nursing experience (χ² = 2.67, p = 0.61).
Differences in nurses’ attitudes toward AI by gender, marital status, age, level of education, and years of experience (N = 220).

N: number of cases; %: percentage; χ² test: chi-squared test; *p < 0.05.
Discussion
Despite the opportunities afforded by AI, the results of the current study revealed only a “moderate” level of awareness toward AI among practicing nurses. Just above half (58.2%) of the participating nurses demonstrated practical knowledge of AI-integrated technology.4,5,13 This highlights the importance of integrating AI-related terminology and applications into the nursing educational programs and the continuous education efforts for practicing nurses; which may extend to other healthcare workers as well. 26 Nurses need to be introduced to the imminent transformation of nursing practice as AI and other technology applications are becoming part of their daily work for nurses. Nurses’ roles and functions are being assisted by the different applications of technology including AI. This can be considered a main change in the traditional roles and functions of nursing professionals. It may lead to stress, anxiety, and the development of negative attitudes among nurses toward such technology if it is not properly introduced.12,15,18 To integrate AI effectively into nursing education, nursing educators must assess the training needs specific to this endeavor. This assessment will enable them to tailor educational materials and tools accordingly. 21
The analysis revealed that nurses’ attitudes toward AI can be described as conservative, with the mean scores indicating a general hesitancy to feel comfortable with AI-integrated technologies. For instance, on a Likert scale from 1 (strongly disagree) to 5 (strongly agree), the mean score for the item “I would like to use AI in my job” was 3.50 (SD = 0.99), while the item “AI systems can perform better than humans” scored lower at 2.99 (SD = 1.07). These scores suggest a cautious approach to fully endorsing AI-integrated tools in clinical practice. In further support of these conservative attitudes, a χ2 test revealed significant differences based on demographic factors such as age and gender. Female nurses and those older than 50 years demonstrated more conservative attitudes compared to their counterparts, with χ2 values of 4.67, p < 0.05, and 9.31, p < 0.05, respectively. This can be explained by the thoughts of nurses about the changes that can be introduced to their role in practice settings as AI-integrated technology may affect the decision-making process and lead nurses and other healthcare practitioners in that. 12 The changing role of nurses may introduce anxiety toward AI, 27 which directly affects the attitudes toward AI and the resulting potential difficulties in future adoption and usage of its applications in practice in addition to the concern of invaded privacy that may result from some AI-integrated technology applications. 27 Nurses who have positive views and attitudes toward AI are more likely to feel comfortable using AI applications and they view AI and other technology applications as useful and easy to use.28,29
The findings of this study indicate that a considerable proportion of nurses hold conservative attitudes toward AI, which encompasses a spectrum of hesitancy from mild caution to significant resistance against the integration of AI technologies in nursing practices.7,12 These conservative attitudes are particularly pronounced among female and older nurses, suggesting that demographic factors play a crucial role in shaping perceptions of technological advancements.7,26,30 Conservative attitudes toward AI may stem from various concerns, including fears about job displacement, doubts about AI's reliability and accuracy, and ethical worries about patient privacy and the depersonalization of care.7,26 Addressing these concerns through targeted education about the benefits and ethical use of AI, and providing empirical evidence of AI's positive impacts on patient outcomes and workflow efficiency could be vital strategies for fostering more receptive attitudes.7,26,30
The current study results about the conservative attitudes and concerns toward AI technology come in contrary to the results reported by Kwak et al., 31 as they examined the attitudes of student nurses toward AI technology and resulted in the positive willingness of the students to work with AI-integrated applications in nursing practice with ease. These results can be related to the generational differences among nurses. 30 Younger nurses tend to hold more positive attitudes toward technology in general compared to elder nurses. 29 This suggests adapting the educational and administrative interventions in this regard based on the different generations of nurses found in the workforce of healthcare organizations.
Nurse managers, healthcare policymakers, and educators should collaboratively develop and update policies aimed at addressing challenges or opportunities within the nursing workforce, including initiatives to promote education and cultivate positive attitudes toward AI integration. 26 Moreover, understanding the conservative attitudes of nurses toward AI technology provides crucial insights for healthcare administrators and policymakers in designing and implementing AI technologies in a way that considers the values and reservations of the nursing workforce.7,26 Ensuring that AI tools are introduced with adequate support and training, and are aligned with nurses’ professional values and ethics, will be essential in overcoming resistance and integrating these technologies successfully.7,26
Limitations and recommendations
Caution should be practiced in the generalization of the current study results as it is limited to nursing professionals in a specific setting in addition to its cross-sectional nature. Longitudinal as well as qualitative studies including nurses and other healthcare workers are recommended to expand the knowledge about AI's effects on healthcare practices, which directly and indirectly affect the quality of care provided at healthcare organizations.
Conclusions
The current study investigated the practicing Saudi nurses’ AI awareness levels and their attitudes toward such technology in nursing practice. The results showed moderate levels of awareness among Saudi nurses toward AI technology applications and conservative attitudes toward these applications as well. Nurses have concerns that the application of different AI tools in nursing practice may result in a major transformation of the traditional nursing role in healthcare settings. This increased the Saudi nurses’ anxiety and concerns toward AI technology which may take over or control the nursing functions. Proper introduction of educational programs that are tailored to different audiences considering the generational differences may help in intervening in this regard. It may help in alleviating the anxiety toward AI and increase the potential adoption and usage of AI in nursing practice. Healthcare and nursing stakeholders need to develop and update the needed educational and practice policies to ensure a smooth transition toward the presence of AI in healthcare settings.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076241271803 - Supplemental material for Exploring nurses’ awareness and attitudes toward artificial intelligence: Implications for nursing practice
Supplemental material, sj-docx-1-dhj-10.1177_20552076241271803 for Exploring nurses’ awareness and attitudes toward artificial intelligence: Implications for nursing practice by Majed Mowanes Alruwaili, Fuad H. Abuadas, Mohammad Alsadi, Abeer Nuwayfi Alruwaili, Osama Mohamed Elsayed Ramadan, Mostafa Shaban, Abdulellah Al Thobaity, Saad Muaidh Alkahtani and Rabie Adel El Arab in DIGITAL HEALTH
Footnotes
Contributorship
Conceptualization: FHA, MMA, MS, AL, OMR, MSH, AA, SMA, and RAA; methodology: FHA, MMA, MS, AL, RAA, MSH, and AA; formal analysis: FHA, MMA, AL, OMR, MS, SMA, and AA; investigation: FHA, MMA, MS, AL, OMR, MSH, SMA, RAA, and AA; data curation: FHA and MMA; writing–original draft preparation: FHA, MMA, RAA, MS, AL, OMR, MSH, SMA, and AA; writing–review and editing: FHA, MMA, MS, AL, OMR, MSH, SMA, and AA; funding acquisition: MMA.
Availability of data and materials
The data sets generated and/or analyzed during the current study are not publicly available due to ongoing project policy, as the data may be subject to restrictions on data sharing imposed by the university. However, the data are available from the corresponding author on reasonable request.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval and consent to participate
This study was approved by the bioethics institutional review board of Jouf University and was performed in accordance with the Helsinki Declaration. 25 The study received the approval number (no. 3-06-44, 7 February 2023). To ensure confidentiality and anonymity, several strategies were implemented, such as assigning a unique code number to each nurse and reporting all data in aggregate form. The data was handled electronically through a password-protected account, and participants provided electronic informed consent before completing the survey on a Google form.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research is funded by the Deanship of Graduate Studies and Scientific Research at Jouf University through the Fast-Track Research Funding Program. The authors extend their appreciation to the Deanship of Graduate Studies and Scientific Research at Jouf University for funding this work.
Guarantor
MMA.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.