
Abstract
Background and aim
Patient- and family-centered care in pediatrics is associated with improved outcomes and cost-effectiveness, yet current models often overlook the needs of diverse and racialized families. Digital health innovations offer new opportunities to address inequities and tailor care to the needs of racialized patients and their families. This study explores gaps in pediatric patient experience and examines how emerging digital health technologies can support more equitable, effective care by engaging diverse communities through semi-structured interviews with caregivers.
Methods
We conducted a retrospective qualitative study using quota-based sampling at BC Children's Hospital. Caregivers of children with complex healthcare experiences—including surgery, rehabilitation, chronic conditions, or hospital stays over 14 days—were recruited and interviewed through semi-structured interviews conducted via Zoom. Transcripts were thematically analyzed and categorized using the BC Health Quality Matrix to identify key gaps and opportunities in pediatric care.
Results
Interviews revealed gaps in pediatric care, including inconsistent shared decision-making, pre-procedural patient anxiety, barriers to access, misdiagnoses, and long wait times. We identified digital health solutions such as mobile health apps, telehealth, and artificial intelligence as opportunities to address these solutions, but found that many of these solutions have not yet been implemented within a pediatric population or may exacerbate disparities.
Discussion
Digital health technologies show potential to improve pediatric care by addressing gaps in racialized patient experience as identified in the current study. Incorporating diverse patient and caregiver perspectives is essential to ensure innovations are equitable and responsive to the diverse needs of British Columbia residents. Achieving digital health equity remains critical to realizing the broader benefits of patient-centered innovation and advancing the Quadruple Aim.
Keywords
Introduction
Patient- and family-centered care is a cornerstone of high-quality pediatric healthcare. When effectively implemented, patient- and family-centered care in pediatrics is associated with better outcomes, higher staff satisfaction, and greater cost-effectiveness. 1 However, these benefits are not the same for all pediatric populations. Current patient- and family-centered care models often fall short for racialized individuals, families, and/or communities, 2 potentially due to a dearth of diverse patient perspectives, especially in Canada. 3
In Canada—and particularly in British Columbia (BC)—incorporating a diverse patient perspective is a pressing challenge. British Columbia is a diverse province with 34% of its residents identifying as a visible minority, 6% as indigenous, and 29% as immigrants. 4 The specific needs of BC residents are as diverse as its population. Yet healthcare services have not consistently adapted to the cultural, linguistic, and experiential contexts of BC's populations, leading to inequities in access, experience, and outcomes. Addressing this gap requires intentional engagement with racialized communities to co-develop care models that are equitable, responsive, and contextually grounded.
Digital health and its associated technologies have the potential to enhance healthcare. Defined by the World Health Organization as, “the development and use of digital technologies to improve health,” digital health encompasses tools such as wearables, mobile health apps, virtual health, and artificial intelligence (AI). These innovations have shown promise in improving diagnosis and treatment, ensuring continuity of care, and reducing error and inefficiencies, 5 aligned with the Quadruple Aim. 6 Importantly, digital health also has the capacity to improve equity by offering customizable solutions tailored to each person that can be adapted for varying literacy levels, languages, and cultural norms—if designed with inclusivity in mind. 7 However, general barriers to implementing digital health innovations exist.8,9 A review of 34 studies that included diverse populations, identified key barriers to digital health such as limited digital skills, the cost of phones and data, limited English literacy, lack of cultural representation, and limited recognition of cultural concerns. 9 For racialized families in pediatric care, these findings highlight the need to integrate cultural and linguistic perspectives (among others) at all stages of digital health design. Without the intentional co-design grounded in the lived experiences of diverse patients and their families, digital health risks inadvertently reinforcing existing health inequities.
This study addresses that risk by exploring how digital health can be leveraged to improve pediatric patient and family health care experience in BC. Specifically, we aim to identify the gaps, needs, and opportunities in pediatric care delivery from the perspective of diverse patients and families, and to explore how emerging digital health technologies might be leveraged to address these gaps.
To achieve this, we conducted semi-structured interviews using quota-based sampling to reflect BC's diverse population, with intentional inclusion of racialized patients and families to ensure their perspectives were represented.
Findings from this study will inform the co-design of inclusive, digitally enabled pediatric programs tailored to the needs of BC's diverse communities.
Methods
Study design
This was a retrospective qualitative study employing quota-based sampling conducted at BC Children's Hospital in Vancouver, BC Canada between February 2023 and August 2023. This qualitative study was primarily anchored by phenomenology to capture lived experiences in racialized individuals and their families; however, we also used content analysis to understand how digital health innovations could potentially be used to address each issue. This study was approved by the University of British Columbia and Children's and Women's Health Centre of British Columbia Research Ethics Board (H22-00247).
Recruitment and participants
Participant recruitment included standard third-party recruitment methods (e.g. posters, social media, and ReachBC). Consistent with prior guidance for phenomenological qualitative studies, we targeted a sample of 5–25 participants.10,11 Prior to data collection, we identified four unique healthcare experiences that have benefited from advancements in digital innovations in adult populations, but have not yet been implemented in pediatric populations. To be eligible, each potential participant had to have experienced one of the following healthcare scenarios: (1) surgery 12 or medical imaging5,13; (2) treatment in cardiology, orthopedics, neurology, or for chronic pain14,15; (3) rehabilitation for any condition 16 ; or (4) hospital stay of ≥14 days. 17 Additionally, potential participants (i.e. caretakers) also had to be living in Canada during the time of the interview, comfortable talking about their and/or their child's experiences, and had to have access to a laptop or computer with stable internet connection. To ensure we heard from individuals experiencing underrepresentation and systematically excluded groups, we employed a quota-based sampling technique.18,19 In addition to healthcare experience, quotas were based on sex (male/female) and ethnicity (racialized vs non-racialized), with the aim of ensuring participation from females and/or racialized patients and their families. An electronic consent form was sent via email to individuals who expressed interest in the study. The study protocol and activities were reviewed with prospective participants over the phone and an e-consent was administered through REDcap. Thus, a relationship between the study team and the participants was established prior to study commencement. Informed consent was obtained from all participants prior to any data collection.
Interview
Zoom (Version 5.13.3) was used for all the interviews with the audio recorded. Interviews with caregivers were done using a semi-structured discussion approach where participants were asked to recall and reflect on their and/or their child's unique healthcare experience. Caregivers would elaborate on their and/or their child's lived experience and the interviewer would ask clarifying follow-up questions when appropriate. Primary interview questions were provided to participants ahead of the session to accommodate processing differences. Questions were internally reviewed by the study team. At the beginning of the interview session, we introduced the research team and walked participants through the study protocol and what to expect, and how we intended to use the results. The interviewer was a female qualitative researcher and Research Project Coordinator at BC Children's Hospital Research Institute at the time of the interviews. The interviewer had a Master of Public Health with a focus on social inequities and social justice and had training in interviewing and therefore was interested in the research topic. The interviewer took field notes during and after the interview. Only the interviewer and the participant were present for the interview. There were no repeat interviews carried out.
Data analysis
Semi-structured virtual interviews were transcribed removing identifiers (e.g. name, location, gender). The data were analyzed using interpretive phenomenological analysis involving multiple readings of the transcripts and note taking, transforming notes into emergent codes, and clustering these into higher level themes 20 which were then categorized into the dimensions of the BC Health Quality Matrix. While interpretive phenomenological analysis does not typically use open/axial coding, we did use those practices for theme development. We began with noting, comments, and open coding to capture initial ideas directly from the data, followed by axial coding to connect related codes and refine categories. The goal of the analysis was to create, categorize, and organize any potential themes while carefully considering the unique experiences of each participant. Thus, we used a blended approach. Data were managed using the software NVivo 13. Transcripts were not returned to the participants. Data was analyzed by a single person (BG). As this study focused on BC residents, themes were binned into one of seven dimensions based on the BC Health Quality Matrix 21 (see Figure 1). In addition, we explored whether themes were more prominent within subgroups (e.g. age range, ethnicity, etc.). Reporting adhered to the Consolidated Criteria for Reporting Qualitative Research checklist 22 (see Supplemental Material).

Quality matrix as defined by BC Health Quality Matrix. The first five dimensions (respect, safety, accessibility, appropriateness, and effectiveness) focus on the individual perspective, whereas the two (equity and efficiency) focus on the system perspective. Image is reproduced with permission from Health Quality BC.
Results
Patients
Six individuals participated in our study. Fifty individuals expressed their interest in the study and were invited to undergo screening, of which 13 did not complete screening. From the eligible 37 participants, nine were consented, of which six had an interview. Reasons why participants did not complete screening or consent are unknown. Average interview time was 01:16:05 (hh:mm:ss) (range: 00:53:42–1:45:16). Patient demographics are reported in Table 1. Three (50%) of the participants were between the ages of 2 and 11 years, whereas the other three participants were between 12 and 17 years. Two (30%) participants were female, two (30%) participants reported mixed, two reported Asian-Indian, one (17%) reported Other-African, and one reported White for their ethnicities. Note, however, caregivers spoke on behalf of their child/the patient. The demographics of the caregivers are not given. Descriptive subgroup comparisons within each theme did not reveal consistent or interpretable differences among subgroups. Participants did not provide feedback on the findings.
Patient demographics.

Patient healthcare experiences
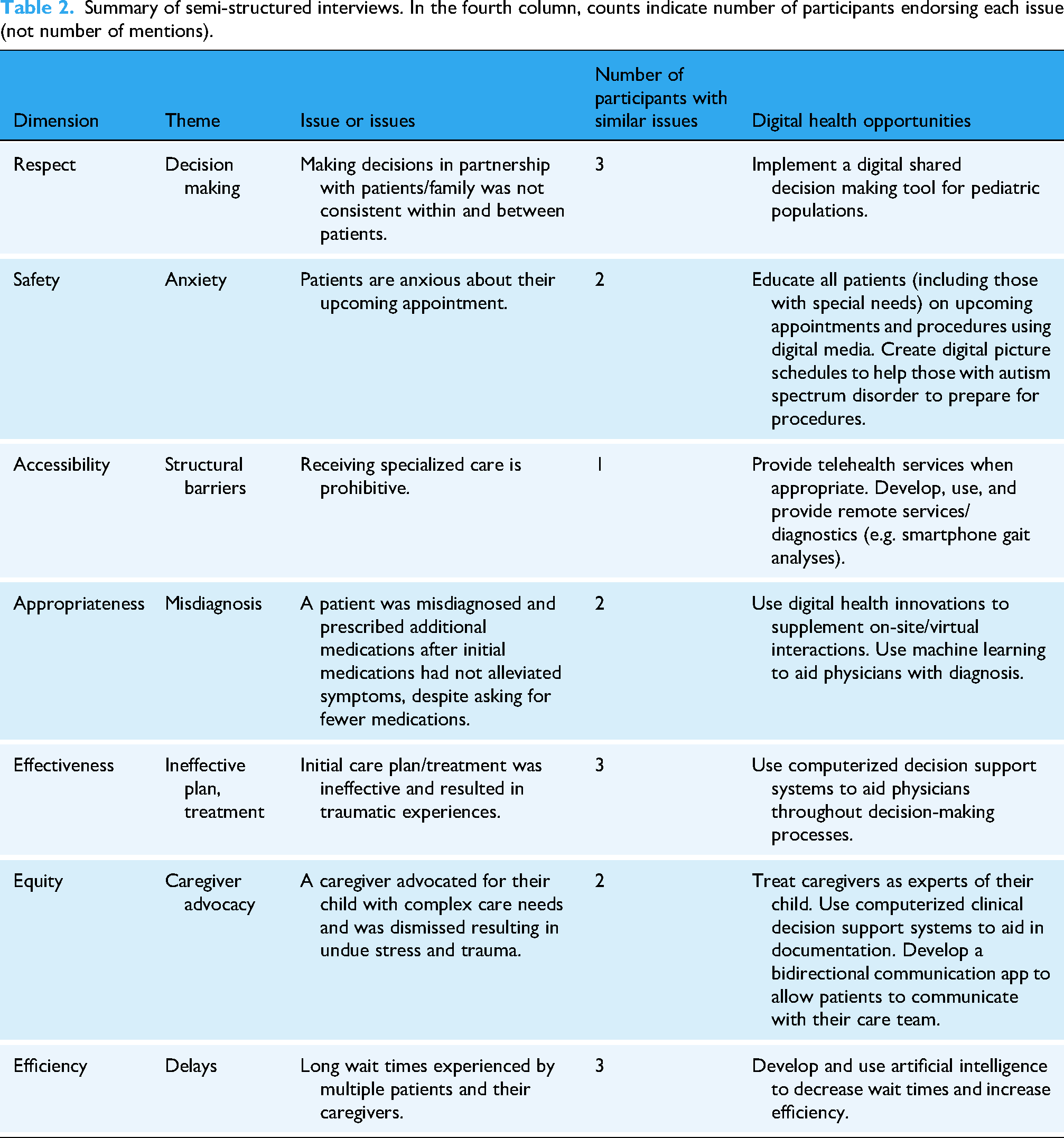
Themes taken from the interview were categorized into each dimension of BC Quality Matrix. Results are thus structured and organized using the BC Quality Matrix (Figure 1), starting with Respect and ending with the Efficiency dimension. Similar to the BC Quality Matrix, a definition of each dimension is provided followed by a summary. We then identify the issue that the caregiver/patient had, outline the digital health opportunity, provide relevant background information, and include a poignant quote from the interview, followed by a brief discussion. A summary of the results with the corresponding dimension, theme, issue or issues, number of participants with similar issues, and digital health research or innovation opportunity is presented in Table 2.
Summary of semi-structured interviews. In the fourth column, counts indicate number of participants endorsing each issue (not number of mentions).
Respect
Respect recognizes and upholds a person's preferences, values, and individual needs. Respect minimizes power imbalances and involves the healthcare provider being open to making decisions in partnership with a person, family, caregiver, and/or community.
Background
Making health decisions in partnership with a person, family, caregiver and/or community is more formally known as shared decision making. Shared decision making is an evidence-based approach that promotes collaboration,
23
is considered essential for patient- and family-centered care, and comes recommended by the Canadian Paediatric Society.
24
We found evidence that shared decision making did not always happen, or happened to such an extent that it put a significant burden on the caregiver. “One of the times there was a clear plan made … with my [child], my [partner], and the medical team about what we're gonna do in one of the next steps of the plan. And for those … they give us a copy of it … so we can all see it … at the bottom it says, the above was discussed with … patient and parents … and then it's electronically signed by the doctor. … So there was something … written there [the care plan] that we had never, ever, ever, ever discussed that [the physician] had put in there, signed a legal document saying that … we've discussed this, which we haven't [sic].” (#3)
In contrast to the above patient experience, we also heard from another caregiver that noted several instances concerning the burden of shared decision making. “…we were surprisingly involved in [deciding whether we should or should not administer] drugs too. It's like, I don't know what that drug does, you tell me. Should [child] take it, like you're the doctor.” Adding, “…so the nurse would be like ‘as a parent, do you think we should give [child] morphine?’ And it's like … [child] hasn’t had a bowel movement in days, but I hate seeing [child] in pain.” (#4)
Digital health opportunity—Implement a digital shared decision making tool for pediatric populations
In addition to improving communication skills, assessing caregivers’ preferences in their involvement in the decision making process, understanding cultural differences, and knowing when a situation is appropriate for shared decision making, 25 some shared decision making barriers may be overcome using digital tools. 26 For example, one research team developed an app to support shared decision making within a pediatric mental health context. 27 The app reported by Liverpool and Edbrooke-Childs was developed using an evidence-based process, motivated by shared decision making guidelines, and involved caregivers, patients, and researchers. However, a randomized controlled trial conducted by the same authors found that the app had a high attrition rate during follow-up. 28 Therefore, combining strategies such as assessing parents’ preferences in their involvement in the decision making process and digital tools such as smartphones and web-based apps aimed at enhancing shared decision making has the possibility to reduce decision regret and increase patient satisfaction. Additionally, it is important to note that there is a lack of representation of racialized patients, families, and communities in the shared decision making literature, 29 making it difficult to develop evidence-based digital healthcare apps aimed to enhance shared decision making for systemically excluded groups.
Safety
Safety, or avoiding harm and fostering security, is the extent to which services prevent or minimize harm (e.g. actual and perceived physical, cultural, and psychological) that could result from the delivery of care and to the extent to which they promote trust.
Background
One patient we interviewed mentioned the anxiety around an upcoming procedure (e.g. gait analysis). The caregiver said, “[Child] was nervous. … the uncertainty is what causes the anxiety. So, you know, I think … definitely, being able to maybe show kids what's gonna happen before it happens, lessens the anxiety before they get there…” (#6)
Similarly, another caregiver noted that visual and auditory aids that depict and describe upcoming activities work well for their child with a high need for support (e.g. nonverbal, moderate to severe autism). “So one of the big things we do is we do visual scheduling. So we have [child's] therapy iPad, and we’ll make a schedule that just says get ready, which is like, put on your shoes, and get in [caregiver's] car … [Child] tends to get anxious with outings … And so [child] actually having … audio telling [child] what the thing is, and then an ‘all done’ … can be very, very helpful.” (#1)
Digital health opportunities—Make procedural education standard-of-care for all patients using digital media. Create digital procedure storybooks and visual activity schedules to be inclusive for all patients, including those with high support needs
Anxiety centered around a hospital visit is a result of the uncertainty. 30 Unfamiliar environments, instruments, and the procedure itself can all contribute to pre-procedural anxiety. As such, patient education and exposure has shown to be an effective strategy in alleviating pre-procedural anxiety. Educational tools, including verbal briefings, written or pictorial materials, and even guided tours of medical facilities, have shown to diminish pre-procedural anxiety in pediatric patients. 31 The use of digital immersion, notably through virtual reality (VR), in preparing patients for medical procedures also shows promise in reducing pre-procedural anxiety.32,33
Visual activity schedules, or picture schedules, are an evidence-based approach to help prepare individuals—particularly those with communication or cognitive challenges—for upcoming procedures. 34 For example, in a pilot study involving children with autism spectrum disorder, 88% of staff and 78% of caregivers found picture schedules decreased patient anxious behaviors across a variety of standard procedures. 35 The same study also reported that 75% of medical staff thought that picture schedules made it easier to complete the procedure, suggesting that the creation of procedure-based digital media has the potential to reduce anxiety and improve patient care more broadly.
The use of VR to support patient preparation has been gaining interest across pediatric populations. For example, VR has been argued to be especially helpful to children with autism as it can offer real-world simulations in a controlled and safe environment. 36 While many VR applications for this patient population have focused on social skill development, 37 it is feasible that using picture schedules in VR could help reduce preprocedural anxiety. To our knowledge, no study has explored this research topic. Therefore, it is currently unknown whether VR-based picture schedules are more effective in alleviating pre-procedural anxiety compared to traditional paper-based picture schedules.
Accessibility
Accessibility, or the ease with which health and wellness services are reached, is the degree to which individuals can receive care when and where they need it. Accessibility can encompass physical, financial, cultural, and psychological barriers to receiving care. It also includes a welcoming entry and easily transitions between and within services.
Background
One caretaker reported financial strain receiving adequate care. Specifically, they had to travel to BC Children's Hospital for a gait analysis that was not available in their location. When discussing the visit to BC Children's Hospital the caregiver said, “We did it in one day. Can't afford to stay over …” Adding, “I think it's important that they hear about … the experiences of … people because, you know, BC is a huge province … Really hard for a lot of people to … come to Vancouver, to go to these specialist clinics…” (#6)
Digital health opportunity—Develop, use, and provide remote services/diagnostics (e.g. smartphone gait analysis)
A key benefit of digital tools, such as telehealth and mobile health, is their ability to reach patients in rural, underserved, or remote areas. Mobile health, or mHealth, is the general term for the application of mobile devices, their components, and related technologies in medical care. Telehealth is the use of electronic communication technologies (e.g. video calls, secure messaging) to deliver clinical health care services remotely. There have been significant inroads into using mHealth within the field of gait analysis. For example, in one study researchers compared a smartphone to the gold standard of gait analysis (e.g. wearable sensors) and found comparable results. 38 Sixty community-dwelling adults walked on a path for 2 min with a smartphone in their front pocket and then walked the same path wearing sensors. Gait speed, cadence, and step length all showed good to excellent agreement between the smartphone and the sensors. 38 Remote gait analyses via smartphones need not be for major medical decisions, but could confirm the need for patients to come on-site for further specialized care, increasing accessibility and reducing costs. To date, no study has combined mHealth with telehealth for gait analysis in pediatric populations. Whether this approach is feasible in children and adolescents has yet to be determined and is therefore worthwhile exploring. Moreover, it is important to recognize that those who stand to gain the most from telehealth and mobile health are often the least able to access and use these services. 39 Ensuring equitable access and quality care through virtual health integration will require thoughtful attention to the diverse resources and infrastructure across different communities and settings.
Appropriateness
Appropriateness, or appropriate care that is specific to a person's or community's context, is evidence-based and guided by best practices that optimize care to achieve a patient's health and wellness goals. In appropriate care, decisions are considered using risks and benefits to prevent the over or underuse of treatments or services.
Background
One caregiver felt that they were misdiagnosed with bipolar disorder and heavily medicated for years. “I feel I was misdiagnosed with bipolar disorder and heavily medicated for a period of 15 years. I had been asking for two years for a med vacay. To get off everything and start from scratch because I'm taking all these pills and I'm still having lots of episodes …. I would go to the doctor and I'm still suffering. I'm still suffering, I'm still suffering. And they would just give me more pills …. I was just like, I'm done. I just don't trust you anymore.” (#6)
Digital health opportunity—Use digital health innovations such as AI and machine learning to supplement on-site or virtual interactions and aid in diagnosis or combat misdiagnosis
It is well evidenced that psychiatric illnesses such as bipolar disorder are often misdiagnosed.40–42 However, pinpointing the cause(s) of a misdiagnosis is complicated. Misdiagnoses may be due to complex presentations, poor communication between physician and patient, and/or challenging behavior of the patient. 41 Related to the complex presentations of psychiatric illnesses, another qualitative study found that physiatrists reported that information crucial to evaluating bipolar disorder may be hidden from clinical observation. 40 Artificial intelligence, more specifically, machine learning has been proposed to address this issue. A recent systematic review found high sensitivity (88%) and specificity (89%) in discriminating between those with bipolar disorder and healthy controls in an adult population. 43 While the prevalence of bipolar disorder has been reported to be quite low in pediatric populations, 44 the prevalence for attention deficit hyperactivity disorder and emotion disorders (anxiety or mood disorder) is varied in Canada. This variability is attributed to low agreement between health processional, parents, and physician claims data (i.e. administrative records). 45 Similar to adult studies, one research group used a fear and an anxiety inducing task coupled with a belt-worn inertial measurement unit and machine learning to accurately (92%) classify 63 children with internalizing disorders. 46 Thus, while there seems to be no absolute solution to preventing misdiagnoses, digital technologies such as machine learning can be used to reduce them, facilitating appropriate care.
Effectiveness
Effective care, or care that is known to achieve the intended outcomes, is informed by evidence (e.g. knowledge gained through formal education, clinical research, and lived experience) and best practices to optimize the health and wellness of individuals and populations.
Background
A family who sought care for their child's arm fracture encountered ineffective treatment. During the initial visit, the technician recommended manipulating the fracture under anesthesia to properly set it, however, the physician declined. The physician then told the caregiver to contact a nearby orthopedic surgeon for follow-up. “And they gave us a contact for an orthopedic surgeon who was nearby in [city]. And then I waited for like one week before calling them, and they said, they're still trying to get the response from the emergency care to take us in. But then it didn't happen. And then, 2 weeks later I again call [sic] them. And then they're saying that the orthopedic surgeon is going on a vacation for one month. So I said …, this is ridiculous because [child] has not been seen for like … 2 weeks, and I don't know whether the fracture has been set properly or not. And so [physician] called us next day and said … there is another doctor who's agreed to look at my child. So we ended up taking [child] to the [non-pediatric hospital] again. And [new physician] was very, very concerned … and [new physician] immediately did an X-ray for the hand and then [new physician] found out that it was not like put on properly. And so [new physician] ended up cutting the cast off and … said is going to redo it and going to also talk with people at [pediatric hospital] to see what's going on, and then if this is okay.” (#5)
Digital health opportunity—Use computerized decision support systems to aid physicians in decision making processes
Computerized clinical decision support systems (CDSSs) are software tools that use targeted clinical knowledge, patient information, and other relevant health information to aid clinical decision making. 47 These systems can also leverage AI to enhance clinical decision making. Related to the caregiver's experience reported above, the Food and Drug Administration has permitted the marketing of AI for aiding providers in detecting wrist fractures since 2018. 48 Within the context of medical imaging diagnostics, CDSS can augment extraction, visualization, and interpretation of medical images. 49 However, as software, CDSS can only recommend and aid in diagnostics. The physician ultimately has to be open to the recommendation. In a meta-analysis, researchers found that CDSS physician uptake was only 34% and that features relating to CDSS context and implementation strategy predicted update, 50 with user friendliness, alignment with existing workflows, and adequate training key factors influencing CDSS uptake. 51
In addition to CDSS aiding in fracture diagnostics, CDSS has also been used as a semi-automatic care plan management tool. Congruent with the need personalized care, 52 one team created a Personalized Care Plan Development Platform implemented as a web-based portal for those with chronic conditions. 53 Within the tool, the semi-automated care plan was linked to patient data and provided recommendations. With the use of CDSS care plans, concerns around a child's treatment plan could potentially be addressed in advance, thereby preventing harm, increasing capacity and efficiency. In conclusion, the development and use of CDSS can aid in diagnostics and care planning, have the potential to increase effectiveness, and achieve the best outcome for patients and their families.
Equity
Equity, or the fair distribution of services and benefits according to population need, involves understanding the individuals being treated, with a focus on the social determinants of health, or nonmedical factors that affect health outcomes. Equity is when all persons have the opportunity to achieve their health and wellness. Each person should receive care tailored to them and based on their circumstances, histories, and needs.
Background
An indigenous caregiver communicated the complex care needs of their child with the care staff prior to a procedure that required sedation. During this instance, the care plan was to use a mild sedative in order to place an IV into the child's arm that would allow care providers to administer a stronger sedative for a standard procedure. The caregiver informed the care staff that, based on past experiences, their child might not be as sedated as the medical staff would expect after the initial mild sedative. The initial care plan was followed without any modifications. Even after the administration of the mild sedative the child was crying and screaming when the medical staff attempted to put the IV in. A physician then suggested that they could administer ketamine, an alternative medication the caregiver did not have time to research and had to make a decision in the moment. Replying to the doctor's request, the caretaker said, “Again, I feel like I told them, you know, your idea of giving [child] the little spray … to get [child] … complying … and chilled out enough to put an IV may not work with my [child]. It would be really nice if they had talked to me about what we would do if it didn't work … I do feel like there had to have been a smoother induction that could have taken place than that. That couldn't have been the only way that had to go.” (#1)
The caregiver suggested the creation of a patient summary profile, “…patient profile that would … outline what some of [child's] specific special challenges might be in a setting like that.” (#1)
Digital health opportunity—Use CDSSs to enhance documentation
In addition to aiding in diagnoses, CDSS can also improve the quality of clinical documentation. It is well described that there is a lack of consistency in documentation for individuals with chronic, complex diseases. Additionally, lack of codes are disproportionately present in racialized groups, with one study reporting that African Americans were 58 times less likely to have a code status discussion compared to white individuals. 54 To combat this issue, the implementation and use of CDSS is also appropriate in supporting equity. One study found that prior to the implementation of CDSS, clinicians struggled with obtaining and documenting the data needed to support clinical interventions. 55 However, after implementation, CDSS enhanced communication and knowledge among staff and saved an estimated 3 million USD. In a separate study, the use of a CDSS increased documentation rates by 24%, 56 suggesting that CDSS has the potential to enhance care through increased patient documentation.
Enhanced electronic communication, combined with face-to-face interactions and the recognition of caregivers as experts of their child, may have helped prevent this and other negative healthcare experiences. The integration of personal health records, records where patients can record and manage their health data, and electronic health records, records only accessible to the providers and specialists, have been used with success in a mobile app. 57 Others have also developed apps to facilitate patient–physician communication. 58 It is possible that care plans that are available to review ahead of the scheduled procedure and that can be accepted or flagged before appointments could be an effective approach to excessive wait times. Future work could explore how this strategy impacts workflow and patient outcomes.
Efficiency
Efficiency, or optimal and sustainable use of resources to yield maximum value, involves the thoughtful use of financial, environmental and human resources to deliver health and wellness services. Efficiency includes maximizing capacity to deliver more and better services by minimizing waste such as unnecessary energy, materials, and money spent.
Background
A family went to the emergency room at BC Children's Hospital because of their child's severe stomach pain. The child came home from school and was unable to walk due to the pain they were experiencing. “…couple of weeks ago, my [child] had some stomach issues and the primary care doctor said they didn't have any openings. We had to wait like 3 days or 4 days, and [child] couldn't wait because [child] was complaining …. so we waited for 5 h before the doctor saw [child].” (#5)
A different caregiver also experienced long hospital wait times. After significant swelling of their child's arm, they decided to go to the hospital because they thought it was something potentially serious. They recalled, “we had to wait for like close to five hours plus in the waiting room.” (#2)
Finally, a caregiver with a complex care needs child also echoed the long wait times of the hospital. “It would've [been] really nice if it could have been a bit more streamlined, especially the induction time. We just sat around for ages. It was ridiculous. And that would make [child's] anxiety build.” (#1)
Digital health opportunity—Implement technological solutions such as AI to reduce wait times
Long hospital wait times can not only lead to patient frustration and dissatisfaction, but also result in delayed diagnosis and treatment, worsening time-sensitive conditions. 59 Longer hospital waits also increase healthcare costs. 60 Artificial intelligence has shown promise in reducing wait times by increasing efficiency. Within the context of hospital wait times, AI can analyze complex and large patient data including arrival patterns, resource availability, patient preferences, and expected duration visits61,62 to find ways to improve wait times where humans cannot. Implementing such techniques in the real world is possible and has shown to be highly effective. For example, Johns Hopkins collaborated with GE Healthcare to establish a state of the art capacity command center, which uses AI to improve efficiency. This program resulted in more capacity, with bed use improving from 85% to about 94%, opening up approximately 16 beds on a daily basis without building a new wing or adding new staff, translating into 16 million USD in annual revenue. 63
Discussion
This study highlights the potential of digital health solutions to address the unique challenges experienced by racialized BC residents within the healthcare system. Semi-structured interviews of patients’ caregivers revealed themes such as decision making, structural barriers, and ineffective care plans, or treatments. The burden of shared decision making (or its absence), the financial strain of traveling for specialized care, and ineffective care plans resulting in traumatic experiences, were some of the issues exemplified by these themes. For each issue, we identified opportunities where digital tools have or could help address these challenges.
Anxiety, specifically pre-procedural anxiety, was a recurrent theme that emerged from our interviews. Educational interventions such as verbal briefings, visual aids, 64 and VR 65 are effective in reducing pre-procedural stress and anxiety. Digital technologies like VR offer immersive, scalable approaches to procedural preparation, especially when tailored to age and neurodevelopmental needs. Developing picture schedules in VR for neurodiverse children, or children who have high support needs, may be a promising yet unexplored avenue to alleviating pre-procedural anxiety in this population. These digital tools empower both children and caregivers, facilitating more positive care experiences.
We also observed evidence of financial barriers to specialized care. Smartphone-based monitoring can offer low-barrier access to specialized clinical insights (e.g. gait analysis) reducing the need for on-site hospital visits. In parallel, misdiagnoses (e.g. mental health conditions) and poor continuity of care underscore the need for better diagnostic support. Computerized clinical decision support systems, including those powered by AI, hold promise in both diagnostic accuracy and personalized care planning. However, their utility depends on physician buy-in and institutional readiness for digital integration. More importantly, some of these digital innovations (e.g. apps) presume that all patients have access to smartphones and stable internet connections, which can inadvertently widen existing health disparities. 66 Thus, while digital tools like smartphone-based monitoring have the potential to bridge gaps in specialized care, their success hinges on equitable access, clinical integration, and systemic commitment to digital health equity.
Although this study has many strengths, it should be interpreted within the context of several limitations. One such limitation is the absence of children in the interviews. All interviews were conducted with the caregiver. While all the caregivers we interviewed unequivocally advocated for their child, our report would have been strengthened by the inclusion of the patient themselves. 67 However, including children in qualitative studies imposes additional demands during the interview, such as whether open-ended questions are appropriate and ensuring that questions do not lead or impose a bias on the child. 68 Moreover, including the child may not have been appropriate within our study, as some of the pediatric patients were quite young, with one pediatric patient being nonverbal.
A general limitation concerning the integration of digital innovation within healthcare is the acceptance of technology among caregivers, and their views on the use of technology with their children. The Canadian Paediatric Society recommends the minimization of screen time, especially for children from 2 to 5 years old, and altogether for children younger than 2. 69 The Canadian Paediatric Society also recommends being mindful of screen time and encourages the use of other non-screen activities (e.g. shared reading, outdoor play, and crafts). 69 Thus, it is possible that even if digital interventions are developed to enhance pediatric care, they should only be accessible to limited age groups, for limited durations, and uptake may be limited.
Another limitation of this study is that the data were coded and analyzed by a single researcher. Consequently, there is no intercoder reliability score. While including multiple coders in qualitative research can strengthen internal quality, it is also recognized that intercoder reliability is not a panacea. 70 Moreover, empirical work suggests that while multiple coders tend to converge on basic themes, coders often diverge in how those themes are “packaged,” making reliability coefficients a less informative indicator of quality. 71 In this study, themes were organized within the dimensions of the health matrix. Nevertheless, further research is needed to explore how digital health technologies may support or hinder racialized individuals and their families.
A further methodological limitation is that no formal assessment of saturation was performed. Data saturation is one criterion in qualitative research for concluding data collection, 72 but it is not without issues.72–74 Despite not assessing saturation formally, several indicators suggest we were approaching it. The facilitator in the current study was experienced in conducting interviews and engaged participants in long sessions, averaging 76 min per session, 16 min longer than typical interviews. 75 Longer interviews can allow for richer accounts, thereby increasing the chance of reaching saturation with smaller sample sizes. We also observed data redundancy (see Table 2). For example, across themes, two to three participants often described similar issues.
Our study's findings may lack generalizability. We had a small sample size with missing ethnicities. Our intent is not to generalize participants’ experiences to the broader population, but rather to highlight the perspectives and experiences of racialized individuals within the healthcare system. Despite observing similar experiences across participants (see Table 2), suggesting systemic issues affecting multiple racialized individuals, we caution against assuming these commonalities apply uniformly to all racialized people or across all healthcare contexts. As Leung notes, “most qualitative research studies, if not all, are meant to study a specific issue or phenomenon in a certain population or ethnic group, of a focused locality in a particular context, hence generalizability of qualitative research findings is usually not an expected attribute.” 76 The strength of this study lies in its contextual depth into systemic barriers experienced by racialized participants. Future research should build on these findings by including larger, more diverse samples, employing multiple coders, and exploring new themes to enhance generalizability.
Finally, another major limitation of digital health innovations is the careful consideration of their use among racialized populations. While digital health holds promise for advancing the Quadruple Aim, its implementation faces significant barriers, especially for racialized patients, families, and communities. Digital health equity, defined as “the readiness of all individuals to access digital health, regardless of age, race, income, or technology,” 77 is especially critical in pediatric care. As health systems adopt and increasingly rely on tools like telehealth and patient portals, gaps in access, literacy, and trust risk excluding racialized, underserved families. Addressing these barriers will require frameworks that incorporate structural and societal factors such as racism, policy, and broadband inequity. 78 Integrating digital health equity into patient- and care is essential to ensure inclusive and effective innovation.
Conclusion
In conclusion, our study highlights the potential that digital health technologies can have on improving patient care, particularly for children and their families. By identifying key gaps in patient experience and leveraging digital tools (e.g. VR, AI, and mHealth), digital health may help alleviate anxiety, enhance inclusivity, while improving patient outcomes. Our data highlight the importance of incorporating patient and caregiver perspectives into the development of these technologies, ensuring they are tailored to meet diverse needs of BC residents. Continued investment in digital innovations and patient-centered approaches will be crucial in achieving the Quadtriuple aim. However, achieving digital health equity remains critical, as barriers in access, literacy, and trust risk excluding marginalized families. Moving forward, continued investment in patient-centered, equitable digital innovation will be essential to improving health outcomes and system performance.
Supplemental Material
sj-pdf-1-dhj-10.1177_20552076251393277 - Supplemental material for Opportunities for digital health innovations to address patient-centered priorities in racialized pediatric populations: A qualitative study in British Columbia, Canada
Supplemental material, sj-pdf-1-dhj-10.1177_20552076251393277 for Opportunities for digital health innovations to address patient-centered priorities in racialized pediatric populations: A qualitative study in British Columbia, Canada by Brian Greeley, Sima Zakani and John Jacob in DIGITAL HEALTH
Footnotes
Acknowledgments
We would like to thank all patients and their families who participated and shared their stories. Special thanks to Sarah Morehart, the interviewer for this study and the following Digital Lab team members for their assistance in this study: Chelsea Studen, Puneet Khosa.
Ethics approval statement
Ethical approval for this study was obtained from the University of British Columbia and Children's and Women's Health Center of British Columbia Research Ethics Board (H22-00247).
Patient consent statement
Written informed consent was obtained from all participants.
Permission to reproduce material from other sources
Author contributions
X: conceptualization (equal); formal analysis (lead); visualization (lead); writing—original draft preparation (lead); and writing—review and editing (equal); X: conceptualization (equal); formal analysis (equal); visualization (equal); writing—original draft preparation (equal); and writing—review and editing (equal); and X: conceptualization (lead); formal analysis (lead); visualization (lead); writing—original draft preparation (lead); and writing—review and editing (equal).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: funding for this research was supported by a Planning and Dissemination Grant CIHR Grant PSC-183497.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data that support the findings of this study are available on request from the corresponding author, BG. The data are not publicly available due to containing information that could compromise the privacy of research participants.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.