
Abstract
Objective
This study aimed to evaluate the efficacy of an artificial intelligence (AI) and digital twin (DT)-based telemedicine system in enhancing health outcomes among elderly adults in China's townships.
Methods
A six-month controlled trial was conducted involving 252 adults aged ≥60 from 12 townships in Zhejiang Province. Participants were allocated to either an intervention group using the AI-DT telemedicine system or a control group receiving routine health monitoring. Health indicators including blood pressure, glucose levels, body mass index (BMI), and health anxiety were assessed pre- and postintervention. Statistical analyses were performed using SPSS, incorporating Chi-square tests, t-tests, and mediation analysis via the PROCESS macro.
Results
The intervention group demonstrated significant improvements in systolic blood pressure (136.30–130.07 mmHg, q < 0.001), diastolic blood pressure (83.42–79.36 mmHg, q < 0.001), blood glucose (98.36–90.43 mg/dL, q < 0.001), BMI (23.80–22.90, q < 0.001), and health anxiety (43.17–30.58, q < 0.001). Mediation analysis indicated that reductions in health anxiety partially accounted for improvements in physiological metrics. Satisfaction survey results, analyzed using the Kano model, identified emergency alarms as a Must-be need and blood pressure monitors and glucose meters as One-dimensional needs.
Conclusion
The AI-DT telemedicine system significantly enhances both physiological and psychological health outcomes among elderly adults in townships, demonstrating high acceptability and potential for broader implementation.
Introduction
During the COVID-19 pandemic, older adults have become a high-risk group for COVID-19 infections due to their weakened immune systems and the risk of other chronic underlying diseases.1–5 According to statistics from the China Centers for Disease Control and Prevention, between 8 December 2022 and 12 January 2023, the average age of death cases was 80.3 years, with approximately 90.1% of deaths occurring in adults aged 65 and above, and 56.5% of deaths in those aged 80 and above. 6 Additionally, there was a higher proportion of deaths in rural and remote areas, highlighting the medical risks faced by elderly people in China's townships. These regions not only have limited access to healthcare, but the demand for services also exceeds the supply. As China faces a deepening trend of aging and an increasing elderly population, the healthcare service gap between urban and rural elderly populations will become even more pronounced.
With the development of artificial intelligence (AI) and digital twin technology (DT), various software applications and medical devices have driven the development of health services.7–9 The AI and DT can be integrated to provide noncontact telemedicine services for older adults. Through AI-DT, health assessments can be conducted for elderly people in townships based on factors such as blood pressure, sleep conditions, heart rate, blood sugar, and weight, while also evaluating their health anxiety. In response to the scarcity of elderly care resources in urban and rural areas, AI-DT can provide exercise and dietary planning, as well as develop health supervision and promotion programs for the elderly.
Several countries have conducted research on telemedicine and AI-DT, and although telemedicine offers structural advantages comparable to traditional clinical services, its long-term impact on the elderly population, including cost-effectiveness, sustainable physical health improvements, and mental well-being, remains underexplored.10–13 Furthermore, due to the relative lag in digital development in rural areas compared to cities, over-reliance on online services to replace in-person services may exacerbate the digital divide among older adults.14–16 Against this backdrop, it is necessary to integrate existing telemedicine technologies with AI-DT to develop an AI-DT-telemedicine healthcare system that is effective and acceptable to service users.
Recent studies have shown that wearable medical devices play a key role in ensuring that elderly people have access to effective rehabilitation services.17–19 In telemedicine, the Internet of Things (IoT) system is used to collect elderly people's physical data and perform real-time monitoring.20–23 However, the application of AI-DT, which integrates advanced data analysis capabilities, in the field of telemedicine is still insufficient.
The core goal of this study is to establish an AI-DT-telemedicine healthcare system that collects multiple health indicators from older adults, assesses their physical conditions and potential health risks, and provides relevant treatment, dietary, and exercise recommendations. Considering the lack of healthcare resources in townships and the cognitive barriers in rural environments, satisfaction surveys will be conducted to ensure the system's effectiveness and personalized services, ultimately reducing unnecessary medical visits, alleviating health anxiety, and improving healthcare resources in rural China.
Specifically, a six-month controlled trial will be conducted with elderly adults from 12 townships in Zhejiang Province, China, to assess the effectiveness of the AI-DT-telemedicine system and conduct a satisfaction survey with participants.
Methods
The framework of this study
As of 2020, there are more than 30,000 township administrative districts in China. Many townships in China are still disconnected from urban centers, making it difficult for them to integrate with the vast urban healthcare system. Most of the healthcare services and facilities in townships are provided by local general practitioners. Additionally, the high proportion of elderly people in rural areas, coupled with the prevalence of infectious diseases since the COVID-19 pandemic, has resulted in persistent shortages of medical resources in these regions.
This study employed a controlled trial design to evaluate the effectiveness of an AI and DT-based telemedicine system for elderly adults in townships. The trial was conducted over a six-month period in 12 townships located in Zhejiang Province, China.
The system proposed in this study evaluates the health factors of elderly adults in townships through AI-DT-telemedicine, with the AI-DT module being the core of the system. As shown in Figure 1, the system comprises five parts: Health device, DT models, Data center, AI analytics architecture, and Service demand. The Health device module tracks the physical health data of elderly adults through IoT devices such as airbag protective belts, smart wristbands, and cameras and transmits the data in real time to the data center. The DT models receive multisource data from the data center and dynamically analyze multimodal health data streams from wearable and home monitoring devices. The data center module serves as the visualization part and transfers data to other modules. The AI analytics architecture module aims to identify health risk factors in the health data processed by the DT models and provide related treatment and preventive methods, thereby enhancing the decision-making capabilities of general practitioners. The Service demand module outputs the results for review and decision-making by general practitioners. This system ensures that even in townships in China, where medical resources are limited, comprehensive and accurate monitoring and prevention can still be provided for elderly adults.

Artificial intelligence-digital twin (AI-DT)-telemedicine system for resource-constrained townships healthcare in China.
Sample size justification with power calculation
To ensure the study had sufficient statistical power to detect meaningful differences in health outcomes between the study and control groups, a priori power analysis was conducted using G*Power software (version 3.1). Based on previous similar studies investigating telemedicine interventions among older adults, a medium effect size (Cohen's d ≈ 0.5) was assumed. With an alpha level of 0.05 and a desired power of 0.80 for independent t-tests, the analysis indicated that a minimum of 64 participants per group would be required. To account for potential attrition and increase the robustness of the findings, we aimed to recruit a larger sample. Thus, a total of 252 participants (126 per group) were enrolled, providing adequate power to detect statistically significant differences in the primary health outcomes measured in this study.
Throughout the six-month trial period, no participants withdrew from the study, resulting in a complete dataset for all 252 enrolled individuals. Therefore, no statistical methods for handling attrition were required, and the per-protocol analysis was conducted on the full sample.
Artificial Intelligence-Digital Twin model
The core of our AI-DT telemedicine system is a predictive model designed to assess holistic health status and potential risks by integrating multimodal data. The model takes as input both discrete data (e.g., body mass index [BMI], self-reported dietary habits) and continuous physiological time-series data (e.g., heart rate, blood pressure, blood glucose, and physical activity levels). We employed a hybrid architecture combining a Spatiotemporal Transformer and a Dynamic Graph Neural Network. This design leverages the multihead attention mechanism to effectively capture long-range dependencies and complex temporal patterns within the continuous physiological signals.24,25 Discrete features were encoded and normalized before fusion. The model's output includes risk assessments for conditions such as hypertension and hyperglycemia and personalized recommendations for diet and exercise.
To ensure the reliability and accuracy of the AI-DT model in assessing health factors, its performance was rigorously evaluated. The model was trained on a subset of the collected data and validated using k-fold cross-validation (k = 5) to mitigate overfitting and provide a robust estimate of its predictive capabilities. The following performance metrics were employed to evaluate the model's effectiveness in classifying health risks and predicting physiological trends:
Accuracy: The proportion of total correct predictions (both positive and negative) among the total number of cases examined. Precision: The proportion of true positive predictions among all positive predictions made by the model. Recall (Sensitivity): The proportion of actual positives that were correctly identified by the model. F1-Score: The harmonic mean of precision and recall, providing a single metric that balances both concerns.
Area Under the Receiver Operating Characteristic Curve (AUC-ROC): A measure of the model's ability to distinguish between different health risk classes across all classification thresholds. An AUC of 0.5 represents no discriminative ability, while 1.0 represents perfect discrimination.
Furthermore, for the regression tasks involving continuous physiological data prediction (e.g., forecasting blood glucose trends), the mean absolute error (MAE) and root mean square error (RMSE) were calculated to quantify the average magnitude of prediction errors. The model demonstrated consistently high performance across these metrics on the validation set, confirming its suitability for providing reliable health assessments and recommendations within the telemedicine system.
Data integration and interoperability
To address the integration of data from diverse medical and IoT devices, a structured interoperability framework was implemented. The system was designed to accept data inputs from a variety of commercially available and clinically validated devices, including smart wristbands, Bluetooth-enabled blood pressure monitors, glucometers, and smart weight scales. Device interoperability was ensured through a multilayered approach:
Hardware and Protocol Layer: The system utilized a gateway device equipped with multiple communication interfaces, including bluetooth low energy and WiFi. This gateway acted as a central node to pair with and collect data from the peripheral health devices. Standard communication protocols were leveraged to establish connections and read data from compatible devices, mitigating vendor-specific lock-in.
Data Standardization Layer: Upon data acquisition, a critical step was the transformation of heterogeneous data formats into a unified standard. We employed the Fast Healthcare Interoperability Resources (FHIR) standard, specifically leveraging the FHIR Observation resource, to structure all incoming physiological data. This involved mapping raw data points to the corresponding fields in the FHIR resource. This standardization ensured that data from different manufacturers could be consistently interpreted, stored, and processed by the central AI-DT analytics architecture.
Application programming interface and Integration Layer: The standardized FHIR resources were then transmitted securely to the cloud-based Data Center via a Representational State Transfer (RESTful) application programming interface (API). This API enforced a consistent data schema for all incoming requests, regardless of the source device. The Data Center served as the single source of truth, where all patient data were aggregated into individual longitudinal health records.
Data collection and health assessment
This study utilized the health statistics database of middle-aged and elderly adults from the China Health and Retirement Longitudinal Study. 26 Data were collected in 2020, covering 150 regions, 450 villages, and urban communities across China, involving 17,708 people from 10,257 households. All participants were aged 45 and above, effectively reflecting the overall health status of middle-aged and elderly adults in China. The health assessment based on this database can effectively identify health disparities among elderly adults or groups, providing a basis for health promotion programs for the elderly.27–29
The health assessment includes comprehensive physical data of the elderly, with heart rate, blood pressure, BMI, blood glucose, dietary habits, and exercise data collected through wearable devices. These indicators form the characteristics of health factors affecting elderly health. The health factors of the elderly are then analyzed through AI-DT-telemedicine, and relevant suggestions are provided.
A total of 252 elderly adults aged 60 and above from 12 different townships in Zhejiang Province, China, were recruited for this study. The age distribution was 143 adults aged 60–69, 102 adults aged 70–79, and 7 individuals aged 80 and above (including 137 males and 115 females). All participants consented to participate in this study. A total of 126 elderly adults who were willing to accept the AI-DT-telemedicine service were selected as the study group, and 126 elderly adults who only agreed to regular health data monitoring but declined to use the AI-DT-telemedicine system were selected as the control group. The inclusion criteria for participants were as follows: (a) aged 60 years or older, (b) living in a township environment, (c) able to use a mobile phone or access the internet, and (d) providing informed consent. The exclusion criteria were (a) individuals with cognitive impairments or severe comorbidities that may affect participation, and (b) individuals unwilling to participate in the study.
To address potential biases in self-reported measures, we triangulated the health anxiety scores with objective physiological markers and behavioral data. Specifically, we examined the correlation between reductions in self-reported health anxiety and improvements in objectively measured physiological indicators. Additionally, we monitored system usage logs as behavioral proxies for anxiety and satisfaction.
We explicitly defined the primary and secondary health endpoints used in this study and justified their relevance based on established clinical guidelines and their significance in geriatric health monitoring.
Primary endpoints
Systolic blood pressure (SBP) and diastolic blood pressure (DBP): These are key indicators of cardiovascular health. Elevated blood pressure is a major risk factor for stroke, heart failure, and chronic kidney disease, particularly in older adults. The relevance is supported by guidelines from the American Heart Association and the Chinese Hypertension League.
Blood glucose level: Fasting blood glucose was selected as a critical metric for metabolic health and diabetes risk. It is a standard screening tool for hyperglycemia and diabetes, which are prevalent among the elderly and associated with multiple complications.
Body mass index: BMI was used as a surrogate measure of body composition and obesity-related risk. It is widely recognized for its association with cardiovascular diseases, diabetes, and functional decline in the aging population.
Secondary endpoints
Heart rate: As an indicator of autonomic function and cardiovascular fitness, heart rate variability and resting heart rate are relevant to overall cardiac health and stress levels.
Health Anxiety Score: Measured using a validated scale, this endpoint captures psychological well-being, which is often overlooked in physical health interventions but is critically linked to adherence and quality of life in elderly populations.
Behavioral metrics
Healthy Diet Days per Week and Exercise Days per Week were included to assess lifestyle changes, which are modifiable risk factors for chronic disease prevention and management.
These endpoints were chosen because they are:
Clinically meaningful and commonly used in geriatric and public health research.
Feasible to measure reliably in a community-based setting using standardized devices and questionnaires.
Sensitive to change over a six-month intervention period, making them suitable for evaluating the impact of a telemedicine system.
This clear definition and justification ensure that the selected health data points are appropriate for assessing the intervention's effectiveness in improving the health of elderly adults in township settings.
The selection of the eight health indicators—SBP, DBP, blood glucose, BMI, heart rate, health anxiety score, healthy diet days per week, and exercise days per week—was based on their established clinical relevance, feasibility of measurement in community settings, and sensitivity to change within a six-month intervention period.
Clinical relevance: Each indicator is a well-validated measure of health status in older adults. The SBP, DBP, and blood glucose are key predictors of cardiovascular and metabolic diseases. Body mass index is a widely accepted indicator of nutritional status and obesity-related risks. Heart rate reflects autonomic nervous function and cardiovascular health. Health anxiety is a critical psychological factor influencing self-management and quality of life in the elderly.
Guideline alignment: The selection aligns with recommendations from leading health organizations, including the American Heart Association, the Chinese Hypertension League, and the World Health Organization, which emphasize the importance of these metrics in geriatric health monitoring and chronic disease prevention.
Feasibility and standardization: All indicators can be reliably measured using standardized, noninvasive devices (e.g., blood pressure monitors, glucometers, weight scales) or validated questionnaires (e.g., health anxiety scale), making them suitable for use in township settings with limited medical infrastructure.
Sensitivity to intervention: These outcomes are known to be modifiable through lifestyle interventions and remote health monitoring, making them appropriate for evaluating the impact of an AI-DT telemedicine system over a six-month period.
By focusing on these eight endpoints, the study aimed to capture a holistic view of physical and psychological health changes resulting from the intervention.
Study design and steps
A controlled trial was conducted over six months. Participant flow throughout the trial is summarized in the CONSORT diagram (Figure 2). Initially, 280 elderly adults from 12 townships were assessed for eligibility. Of these, 28 were excluded (20 did not meet the inclusion criteria and 8 declined to participate). The remaining 252 participants were randomly assigned to either the intervention group or the control group using a computer-generated random number sequence. The allocation sequence was concealed until interventions were assigned, and the randomization process was carried out by an independent researcher not involved in participant recruitment or outcome assessment. This resulted in 126 participants in the intervention group using the AI-DT telemedicine system and 126 in the control group receiving standard care (Figure 3). To minimize assessment bias, outcome assessors responsible for collecting and analyzing the health data (e.g., blood pressure, glucose levels, BMI, and anxiety scores) were blinded to group allocation throughout the study. These assessors did not participate in the intervention delivery and were unaware of which participants belonged to the intervention or control group. The usual care provided to the control group consisted of no active intervention beyond the initial health assessment. Specifically, participants in the control group did not receive access to the AI-DT system, no personalized health feedback, no remote consultations, and no interactive health monitoring services. They continued with their routine health behaviors and any existing healthcare arrangements without additional guidance or support from the study team. This approach was adopted to establish a baseline comparison that reflects the natural health trajectory of elderly adults in township settings without telemedicine support.

CONSORT diagram.

The four-step implementation process of the artificial intelligence-digital twin (AI-DT)-telemedicine system-based elderly health improvement program.
Throughout the six-month intervention period, no participants withdrew from the study. Therefore, data from all 126 participants in the intervention group and all 126 in the control group were included in the final per-protocol analysis.
Data analysis
In appraising health data from the AI-DT-telemedicine system, various statistical tests were performed using SPSS 26.0 software.
30
Chi-square tests and t-tests were conducted to assess the changes in health factors among older adults during the experiment.31,32 Prior to analysis, data completeness was assessed. Throughout the six-month intervention period, no participants withdrew from the study, and there were no missing values in the primary or secondary outcome measures collected at baseline and postintervention. Therefore, no data imputation methods were required. To control the risk of Type I error due to multiple comparisons, the Benjamini–Hochberg false discovery rate procedure was applied with a significance threshold of q < 0.05. The significance level was set at q < 0.01 and 0.05.The formulas for Chi-square tests and t-tests are as follows:


where
Furthermore, to address the potential interrelationships between the improved health factors and reveal the direct and indirect influence pathways of the AI-DT-telemedicine intervention, a mediation analysis was conducted using the PROCESS macro (Version 4.2) for SPSS. Health anxiety was hypothesized as a key mediator, given its significant improvement postintervention and its potential psychological influence on physiological outcomes. The analysis assessed whether changes in health anxiety mediated the relationship between the intervention (independent variable: group assignment) and the physiological outcomes (dependent variables: e.g., SBP, DBP, blood glucose). Bootstrapping with 5000 samples was used to generate bias-corrected confidence intervals (CIs) for the indirect effects. An indirect effect was considered statistically significant if the 95% CI did not include zero.
Kano model survey design and implementation
To comprehensively evaluate user satisfaction with the AI-DT telemedicine system, a structured Kano model-based survey was conducted among the intervention group participants (*n* = 126) at the end of the six-month trial. The Kano model is a well-established methodology for classifying and prioritizing user requirements based on their impact on satisfaction.33,34 It distinguishes between five types of attributes: Must-be (M), One-dimensional (O), Attractive (A), Indifferent (I), and Reverse (R) needs.
The Kano questionnaire was developed based on the 13 service features of the AI-DT system (e.g., emergency alarm, blood pressure monitor, and diet plan). For each feature, a pair of questions was formulated: one functional form (e.g., “How do you feel if the system has an emergency alarm?”) and one dysfunctional form (e.g., “How do you feel if the system does not have an emergency alarm?”). Responses were captured on a 5-point Likert scale: 1 = “I dislike it that way,” 2 = “I can live with it that way,” 3 = “I am neutral,” 4 = “It must be that way,” and 5 = “I like it that way.”
The survey was administered face-to-face by trained research assistants to ensure comprehension among the elderly participants, considering potential literacy or digital barriers. All 126 participants in the intervention group completed the survey, resulting in a 100% response rate. The sample characteristics are consistent with those described in Table 1, ensuring representativeness. The final attribute for each feature was determined by the modal category (i.e., the most frequent response). Additionally, the Satisfaction Coefficient (SI) and Dissatisfaction Coefficient (DSI) were calculated as follows:


Demographic characteristics of the study and control groups participating in the AI-DT-telemedicine system.

Data are presented as numbers with the percentages (%) or mean ± standard deviation.
*Normally distributed data were compared using t-test.
BMI: body mass index.
where A, O, M, and I represent the counts of responses classified as Attractive, One-dimensional, Must-be, and Indifferent, respectively. These coefficients quantify the degree to which a feature can increase SI or cause DSI if absent.
Results
Investigation of demographic characteristics
To ensure comparability between the study and control groups, comprehensive baseline characteristics were collected and analyzed. As shown in Table 1, the study group consisted of 65 males (51.6%) and 61 females (48.4%), with a mean age of 67.31 years (SD = 5.74) and a mean BMI of 23.8 (SD = 2.85), indicating an overall risk of obesity. In terms of education, 24 participants (19.0%) had a university degree, 45 (35.7%) had a high school education, and 57 (45.3%) had junior high school education or below. Regarding life satisfaction, 34 participants (27.0%) were satisfied with their current life, 67 (53.2%) found it fairly good, and 25 (19.8%) were somewhat dissatisfied. In the study group, 38 participants (30.1%) had hypertension, 27 (21.4%) had dyslipidemia, 19 (15.2%) had diabetes, and 13 (10.3%) had other chronic diseases.
The control group included 126 participants, with 72 males (57.1%) and 54 females (42.9%), a mean age of 68.65 years (SD = 5.12), and a mean BMI of 23.5 (SD = 2.91). In terms of education, 20 participants (15.9%) had a university degree, 38 (30.1%) had a high school education, and 68 (54.0%) had junior high school education or below. Regarding life satisfaction, 32 participants (25.4%) were satisfied, 62 (49.2%) found it fairly good, and 32 (25.4%) were somewhat dissatisfied. In the control group, 42 participants (33.3%) had hypertension, 24 (19.1%) had dyslipidemia, 20 (15.9%) had diabetes, and 14 (11.1%) had other chronic diseases. There were no significant differences in the basic demographic characteristics between the two groups (p > 0.05), confirming that the groups were comparable at baseline.
Table 2 presents the initial health data of older adults who participated in the AI-DT-telemedicine system. The average heart rate of the study group was 72.11 bpm (SD = 5.04). The average SBP and DBP were 136.30 mmHg (SD = 14.12) and 83.42 mmHg (SD = 9.23), respectively, indicating a general risk of hypertension. The average blood glucose level was 98.36 mg/dL (SD = 16.74), suggesting the need for enhanced blood glucose monitoring. In addition, the average number of healthy diet days per week was 3.6 days (SD = 1.20), and the average number of days with exercise over 30 min per week was 5.4 days (SD = 1.00). Aside from the need to optimize dietary structure, the exercise level exceeded the average level in China, possibly due to physical activities related to farming or other nonleisure activities in rural areas, which may require adjustments for low-intensity activities. There were no significant differences in the health data between the study group and the control group (q > 0.05), further confirming the comparability of the two groups at baseline.
Baseline health data of the study and control groups in the AI-DT-telemedicine system.

Data are presented as numbers with the mean ± standard deviation.
Results of the impact of the AI-DT-telemedicine
The evaluation of health assessment and management results before and after six months of using the AI-DT telemedicine system in the study group is presented in Table 3.
Health assessment of the study group after participating in the AI-DT-telemedicine system (N = 126).

BMI: body mass index; SBP: systolic blood pressure; DBP: diastolic blood pressure; HDW: healthy diet days per week; EDW: exercise days over 30 min per week.
As demonstrated in Table 3 and visually summarized in Figure 4, the AI-DT-telemedicine system intervention yielded statistically significant improvements across multiple critical health indicators for the study group. Most notably, participants experienced clinically relevant reductions in SBP (from 136.30 mmHg to 130.07 mmHg, q < 0.001), DBP (from 83.42 mmHg to 79.36 mmHg, q < 0.001), and blood glucose (from 98.36 mg/dL to 90.43 mg/dL, q < 0.001). Body mass index also showed a significant decrease (from 23.80 to 22.90, q < 0.05), reducing obesity risk. Furthermore, adherence to a healthy diet improved substantially (Healthy diet days/week: from 3.60 to 5.90, q < 0.001). Perhaps most striking was the dramatic reduction in health anxiety levels (from 43.17 to 30.58, p < 0.001). These findings provide robust evidence for the effectiveness of the system in promoting health among rural elderly adults.

A comparison of multiple key health indicators in the artificial intelligence-digital twin (AI-DT)-telemedicine system.
The superiority of the AI-DT intervention is unequivocally shown by the significant differences observed between the study group and the control group at the end of the six-month period, as detailed in Table 4 and graphically highlighted in Figure 4. Compared to the control group, the study group exhibited significantly lower values for BMI (q = 0.017), heart rate (q = 0.014), SBP (q < 0.001), DBP (q < 0.001), blood glucose (q < 0.001) and, most profoundly, anxiety level (q < 0.001). Conversely, the study group reported significantly more healthy diet days per week (q < 0.001). These group comparisons provide strong validation that the observed improvements in the study group are directly attributable to the AI-DT-telemedicine intervention, rather than time or other external factors.
Health data of the study group and control group after participating in the AI-DT-telemedicine system.

Data are presented as numbers with the mean ± standard deviation.
BMI: body mass index; SBP: systolic blood pressure; DBP: diastolic blood pressure; HDW: healthy diet days per week; EDW: exercise days over 30 min per week.
Result of the mediation analysis on health anxiety
To elucidate the mechanism through which the AI-DT-telemedicine system exerts its effects, mediation analyses were performed. The results indicated that the reduction in health anxiety significantly mediated the intervention's effect on several physiological health factors.
As shown in Table 5, the indirect effect of the intervention on reducing SBP through lowered health anxiety was significant (indirect effect = −2.15, Boot SE = 0.78, 95% CI [−3.85, −0.78]). Similarly, significant mediation effects were found for DBP (indirect effect = −1.23, Boot SE = 0.48, 95% CI [−2.30, −0.42]) and blood glucose levels (indirect effect = −3.05, Boot SE = 1.12, 95% CI [−5.52, −1.15]). This suggests that a portion of the improvement in these physiological metrics can be attributed to the alleviation of health anxiety resulting from the use of the AI-DT-telemedicine system.
Results of mediation analysis with health anxiety as a mediator.

Boot SE: Bootstrapped standard error; CI: confidence interval.
The intervention (study group vs. control group) is the independent variable. Health anxiety score change is the mediator.
To validate the self-reported reduction in health anxiety, we correlated anxiety score changes with improvements in physiological metrics (Table 6). Significant negative correlations were observed between anxiety reduction and decreases in SBP (r = −0.32, q < 0.01), DBP (r = −0.28, q < 0.01), and blood glucose levels (r = −0.35, q < 0.01). Furthermore, lower anxiety scores were associated with decreased use of the emergency SOS feature (r = −0.24, q < 0.05), suggesting that improved psychological well-being was reflected in reduced urgent health-seeking behaviors.
Correlations between health anxiety and objective physiological/behavioral measures.

BMI: body mass index.
Although health anxiety was measured via self-report, we triangulated these findings with objective physiological and behavioral data (as shown in Table 6), which consistently supported the validity of the reported improvements. The significant negative correlations between anxiety reduction and improvements in blood pressure and glucose levels, alongside the positive correlation with decreased emergency system usage, suggest that the self-reported outcomes are not merely perceptual but are grounded in tangible health and behavioral changes. This multimethod approach strengthens the conclusion that the AI-DT system contributes to both psychological and physiological well-being.
Performance metrics of the AI-DT model
The AI-DT model exhibited strong performance in analyzing health data and identifying risk factors. On the validation dataset, the model achieved an overall accuracy of 92.4% in classifying individuals into predefined health risk categories. The detailed classification performance is summarized in Table 7. The model's macro-average F1-score was 0.918, indicating a robust balance between precision and recall across all classes. The AUC-ROC score reached 0.974, demonstrating excellent discriminatory power.
Performance metrics of the AI-DT model in health risk classification.

Note: AUC-ROC = 0.974.
For predicting continuous physiological values, such as next-week average blood glucose levels, the model achieved a MAE of 4.21 mg/dL and a RMSE of 5.87 mg/dL, indicating high predictive precision suitable for clinical advisory purposes.
Satisfaction survey on the AI-DT-telemedicine system
Figure 5 shows the interface of the AI-DT-telemedicine system designed for elderly adults in rural areas. On the left side, there are five buttons: “Home,” “Disease Prevention,” “Life Planning,” “Social Circle,” and the red “SOS” button. In the center of the interface, various health data are displayed, and users can communicate with other elderly adults who are using the system. Additionally, the system provides users with features such as AI-DT model-based intelligent remote consultations and medication reminders.

Home page of the artificial intelligence-digital twin (AI-DT)-telemedicine system user interface.
Figure 6 shows the doctor management interface of the system, where detailed real time and historical health data of each participant can be queried. The interface also displays abnormal health data identified and analyzed by the AI-DT model. This enables doctors to provide feedback on exercise plans, dietary optimization, and remote consultations.

Administrator interface of the artificial intelligence-digital twin (AI-DT)-telemedicine system.
This study uses the model attribute classification method to categorize the frequency statistics of each service item. The study classifies the demand attributes for the community elderly telemedicine system into four categories: Must-be Needs (M), One-dimensional Needs (O), Attractive Needs (A), Indifferent Needs (I), and Reverse Needs (R). Based on the attribute classification results, the Satisfaction-Importance (SI-DSI) coefficients are calculated (29,30). The SI coefficient ranges from [0, 1], with a higher value or one closer to 1 indicating a greater impact on the elderly's satisfaction with the service demand. The DSI coefficient ranges from [−1, 0], with a larger absolute value or one closer to 1 indicating a greater impact of the service demand on the importance for the elderly. Through the Kano model attribute classification method, the attribute with the highest frequency proportion among M, O, A, I, and R for each item is considered the final attribute of the item.
Lastly, the satisfaction analysis in Table 8 shows that among the 13 service demand items for elderly people in townships in China provided in this study, there is 1 Must-be Need (M), 6 One-dimensional Needs (O), 3 Attractive Needs (A), and 3 Indifferent Needs (I). The SI coefficients for the AI-DT-telemedicine system service demands range from 0.372 to 0.633, while the DSI coefficients range from −0.648 to −0.290.
Satisfaction-importance coefficients of each module of the AI-DT-telemedicine system.

SEM: smart electrocardiogram monitor; DSI: Dissatisfaction Coefficient.
Discussion
As a result of the study, the findings suggest that the designed AI-DT-telemedicine system has a significant impact on promoting the health of elderly adults in townships. The study also validated the participants’ satisfaction with the various service modules provided by the system.
The significant improvements observed in the intervention group are underpinned by the robust performance of the AI-DT model, which accurately identified health risks and generated personalized recommendations, as evidenced by its high accuracy (92.4%) and AUC-ROC score (0.974). This technological efficacy was crucial for delivering timely and precise interventions. The statistical results show that after receiving services from the AI-DT-telemedicine system, participants experienced a decrease in blood glucose, SBP, DBP, heart rate, and BMI (Table 3). Participants demonstrated significant improvement in their health status over six months, reducing the risks of chronic diseases such as hypertension, heart disease, and diabetes, while effectively avoiding obesity. Additionally, dietary optimization and exercise planning effectively improved in participants’ eating habits and exercise routines.
Recent case studies have shown that elevated SBP increases the risk of cardiovascular and cerebrovascular diseases.35–37 In elderly populations with long-term effective control of SBP and DBP, the rate of cognitive decline is significantly slower compared to the uncontrolled group.38–42 Additionally, elderly individuals with blood glucose levels above 126 mg/dL have a higher incidence of diabetes and retinal diseases compared to those with normal blood glucose levels.43,44 Therefore, in essence, this study on the effective management of SBP and blood glucose suggests that the AI-DT-telemedicine system can effectively prevent cardiovascular and cerebrovascular diseases, as well as health issues like elderly diabetes.
Additionally, when compared to the control group of elderly adults who did not use the system during the same period, there was a significant difference in health data between the two groups (Table 4). Furthermore, the study group's healthy diet days per week increased significantly, and exercise days over 30 min per week showed a slight increase. In addition to having healthier BMI, SBP, DBP, heart rate, and blood glucose levels compared to the control group, the study group elderly participants experienced a significant reduction in health anxiety, effectively alleviating daily anxiety and improving their psychological well-being. These findings are consistent with the research of Oliveira, who found that remote chronic disease management effectively alleviated anxiety and depression among elderly patients. 45 Therefore, the widespread adoption of this system may help improve the mental health of elderly adults.
As summarized in Table 9, our results not only align with the general promise of telemedicine but also extend it by showcasing more comprehensive outcomes and elucidating the underlying mechanisms.
Comparison of key findings between the current study and previous relevant literature.
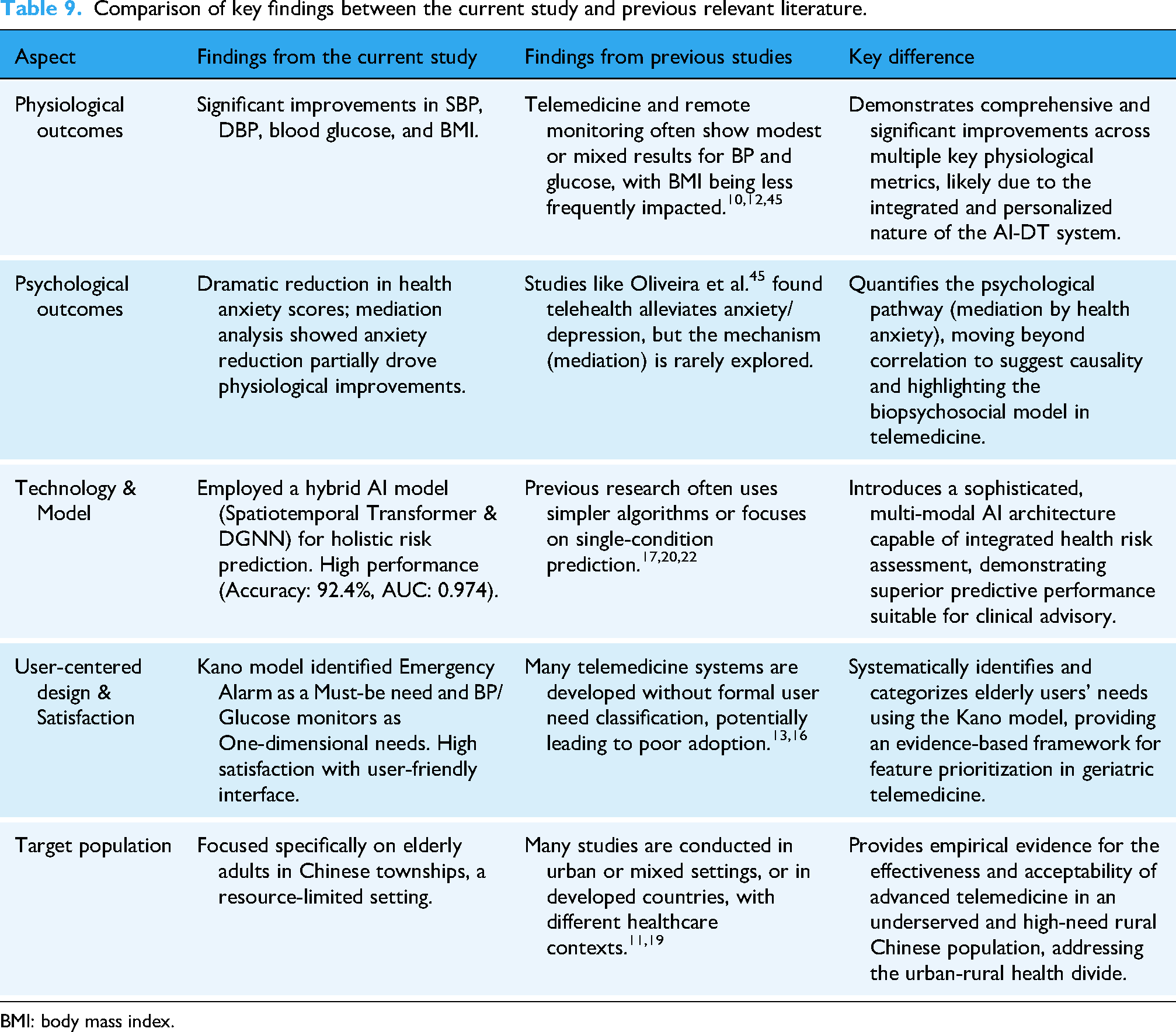
BMI: body mass index.
The robust performance of our AI-DT model (Accuracy: 92.4%, AUC-ROC: 0.974) was crucial for generating timely and precise personalized recommendations, which likely contributed to the significant improvements observed in the intervention group. While previous studies have reported the benefits of remote monitoring,10,12 our study showed clinically relevant reductions in SBP, DBP, blood glucose, and BMI (Table 3). This consistent, multifaceted physiological improvement suggests that the integration of AI and DT technology for holistic health assessment and management may be more effective than simpler telemonitoring approaches.
Furthermore, the dramatic reduction in health anxiety and the subsequent mediation analysis represent a significant advancement. While other researchers, such as Oliveira et al., 45 have found that remote management can alleviate anxiety, our study statistically demonstrates that this reduction in anxiety is a significant mediator for improvements in SBP, DBP, and blood glucose (Table 5). This finding provides a plausible psychological mechanism for the physiological benefits, aligning with the biopsychosocial model of health and underscoring that addressing mental well-being is a potential catalyst for physical health improvement in telemedicine for the elderly.
The application of the Kano model for satisfaction analysis offers another distinct contribution. By systematically classifying user needs (e.g., Emergency Alarm as a Must-be need), our study moves beyond simple satisfaction scores to provide an evidence-based framework for prioritizing features in geriatric telemedicine design (Table 8). This user-centered approach likely contributed to the high acceptability of the system, addressing a common pitfall in technology interventions for older adults.13,16
It is important to consider the potential influence of the Hawthorne Effect in this study. Participants in the intervention group, aware that they were using a novel AI-DT telemedicine system and being actively monitored, might have been motivated to improve their health behaviors simply due to the awareness of participation. This psychological phenomenon could partially contribute to the observed improvements in health outcomes. However, several factors suggest that the Hawthorne Effect is not the sole explanation for our findings. First, the control group also received regular health monitoring, meaning both groups were subject to a degree of observation, which helps mitigate the differential impact of being studied. Second, the significant mediation effect of reduced health anxiety provides a plausible psychological mechanism that is intrinsically linked to the system's functionalities, going beyond mere participation awareness. Third, the objective physiological improvements were substantial and clinically meaningful, and they were strongly correlated with the reduction in self-reported anxiety and changes in system usage behavior (Table 6), indicating a response to the specific intervention rather than just a nonspecific study effect. While the Hawthorne Effect cannot be entirely ruled out, the design of our study and the nature of the results indicate that the AI-DT system itself likely played a central role in driving the observed benefits.
Beyond the Hawthorne Effect, the potential influence of participant expectations warrants consideration. Participants allocated to the intervention group were aware of using a novel AI-DT telemedicine system, which may have generated positive expectations about its benefits. Such expectations could introduce bias, potentially leading to overestimation of the intervention's efficacy through mechanisms such as the placebo effect, increased motivation for behavioral change, or a tendency to report more favorable outcomes.
However, several aspects of our findings suggest that the observed improvements cannot be solely attributed to expectation bias. Firstly, the significant outcomes included robust, objective physiological measures such as systolic and DBP and blood glucose levels, which are less susceptible to subjective reporting biases. The clinically meaningful improvements in these metrics provide strong evidence for a physiological effect beyond perception. Secondly, the mediation analysis revealed a plausible mechanism of action intrinsic to the system's design: the reduction in health anxiety mediated the improvements in key physiological parameters. This pathway aligns with the system's goal of providing reassurance through continuous monitoring and personalized feedback, suggesting that the effects are rooted in its specific functionalities rather than nonspecific expectation effects alone. Furthermore, the control group also received regular health assessments, which partially controls for the general effect of study participation and attention.
Notwithstanding these considerations, it is acknowledged that participant expectations represent an inherent challenge in trials of novel technological interventions where blinding is not feasible. Future research could employ designs such as a three-arm trial comparing the full AI-DT system against a basic telemonitoring system (active control) and usual care to better disentangle the technology-specific effects from the general influence of participant expectations and attention.
The findings of this study are further enriched by the mediation analysis, which statistically reveals the direct and indirect pathways through which the AI-DT-telemedicine system improved health outcomes. The significant mediating role of health anxiety reduction in improving SBP, DBP, and blood glucose levels provides a plausible psychological mechanism for the observed physiological benefits. This aligns with the biopsychosocial model of health, which posits that psychological states can profoundly influence physical health. The constant monitoring, personalized feedback, and readily accessible consultation provided by the system likely empowered the elderly participants, reducing uncertainty and fears about their health, which in turn manifested in improved cardiovascular and metabolic metrics. This finding is crucial as it moves beyond establishing mere association and begins to unpack the process of change, highlighting that addressing mental well-being is not just an independent outcome but a potential catalyst for broader physical health improvement in telemedicine interventions for the elderly.
In addition, frailty in elderly individuals can lead to a decline in cognitive abilities, which in turn contributes to dementia and a decrease in quality of life.46,47 However, scientific dietary and exercise planning can effectively break this vicious cycle, delaying physical function deterioration while promoting neuroplasticity to maintain cognitive function.48,49 Therefore, this study demonstrates that the AI-DT-telemedicine system helps improve the health levels of elderly individuals by enhancing their dietary and exercise habits.
Specifically, the AI-DT-telemedicine system is an elderly friendly application. The limiting factors for elderly individuals using the application include font color, size, and type, as well as the complexity of interface colors and navigation design. Due to the lower average education level of elderly individuals in townships in China, which leads to limited cognitive abilities, the application system designed in this study uses fewer navigation buttons and appropriate interface colors. Therefore, in the satisfaction survey of the study group, the color combination and interface combination were identified as Attractive Needs (A), which confirms the correctness of the design in this study (Table 6). What's more, the satisfaction survey also showed that the emergency alarm was recognized as a Must-be Need (M), indicating that elderly individuals in townships in China have concerns about their health, which may be related to the high number of empty-nest or solo-living elderly individuals in rural areas.
Notably, blood pressure monitors and blood glucose meters were considered One-dimensional Needs (O), likely related to the higher prevalence of hypertension and diabetes among the elderly in China. The health services provided in this study effectively met these needs. Other One-dimensional Needs (O) include weight scales, exercise plans, chat systems, and location services, all of which reflect the daily needs of the elderly population and highlight the need for reasonable design and planning of the application. The AI-DT-telemedicine system achieved good satisfaction in these areas.
Overall, the evaluation results demonstrate that the AI-DT-telemedicine system significantly improves the health status of elderly individuals in townships, and the application designed in this study has good acceptance.
Limitations
The participants in this study were mainly distributed across various townships in Zhejiang Province, China. The data sample is unevenly distributed geographically, which may present certain limitations. The uneven geographic distribution may lead to some flaws in the demand survey for the elderly population. Additionally, the sample size in this study is relatively small, which limits the ability to analyze different subgroups, such as those with chronic diseases, older age groups, and lower socioeconomic status.
This study also has the following limitations: although there was no significant difference in baseline comorbidities between the two groups, we did not systematically collect and compare all participants’ concurrent medication information. Differences in medication use may represent a potential confounding factor. Future studies should prospectively and meticulously document medication history and employ more sophisticated designs (such as randomized controlled trials) or statistical methods (such as propensity score matching) to more rigorously control for these confounding factors.
Conclusion
This study provides empirical evidence that an AI-DT-based telemedicine system can effectively improve key health outcomes and reduce anxiety among elderly adults in Chinese townships. The integration of real-time monitoring, personalized feedback, and a user-centered design addresses critical healthcare access issues in resource-limited settings. The Kano model analysis offers a practical framework for prioritizing features that meet the essential and attractive needs of elderly users. While the system shows significant promise, its broader implementation requires validation across more diverse regional settings and long-term assessment of sustainability and cost-effectiveness.
Footnotes
Ethical considerations
This study was approved by the Institutional Review Board of Hangzhou Dianzi University. All methods were carried out in accordance with relevant guidelines and regulations or the Declaration of Helsinki. Written informed consent was obtained from all participants.
Consent statement
Written informed consent was obtained from all participants prior to their inclusion in the research. The consent process explicitly outlined the study's purpose, procedures, potential risks, and benefits, as well as participants’ right to withdraw at any time without penalty. All data were anonymized prior to analysis to ensure confidentiality. Participants were informed that anonymized findings may be published in an open-access format, freely accessible to the public. No personally identifiable information (e.g., images, names, medical records) is included in this manuscript.
Contributorship
CC and YY involved in conceptualization; CC in methodology, data curation, and writing original draft preparation; RQ and LP in software and investigation; LY in validation; XH in formal analysis, resources, supervision, project administration, and funding acquisition; XJ and YS in writing review and editing; and FL in visualization. All authors have read and agreed to the published version of the manuscript.
Funding
This research was supported by the National Social Science Fund of China (No. 23BXW011).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.