
Abstract
Background
The integration of artificial intelligence (AI) into dentistry has potential to improve diagnostic accuracy and enable more personalized treatment planning. However, the practical and legal aspects of obtaining informed consent in this context remain unresolved.
Objectives
The present article aimed to unify current positions found in the ethics literature with current legal standards in order to develop clinically applicable decision flowchart and checklist for patient consent in AI-assisted dentistry.
Methods
A qualitative thematic synthesis of 50 publications addressing AI, ethics, and informed consent in dentistry was conducted using Braun and Clarke's six-phase framework. Insights were translated into a structured consent checklist and a decision-making flowchart, which were then evaluated through a pilot survey of practicing dentists in Serbia who use AI tools.
Results
Twelve dentists completed the survey. Most rated the checklist and flowchart as clear, practical, and feasible for clinical application. Over 90% agreed that standardized consent improves patient communication and trust when AI is explained as being under clinician supervision.
Conclusions
The proposed consent checklist and flowchart provide a clinically applicable framework that strengthens patient autonomy, supports ethical and transparent AI use in dentistry, and offers guidance for practitioners navigating emerging regulatory requirements.
Introduction
Artificial intelligence (AI) refers to computer-based systems that perform tasks typically requiring human cognition, such as pattern recognition or decision-making. In the context of dentistry, we use the term “AI tool” to describe various applications, including algorithms, software, or systems designed to support clinical decision-making.1,2 The integration of AI tools into dentistry has enhanced diagnostic accuracy and personalized treatment planning, with a focus put on patient-centered AI-enhanced dental care, which emphasizes the patient's overall experience and their active involvement in the treatment decisions. 1 While some AI tools are commercially available, and approved by regulatory bodies, such as VideaHealth's, which has been shown in clinical trials to be superior to dentist in detection of caries, Overjet's Dental Assist, which automatically measure bone loss in radiographs, thereby speeding the time necessary to begin periodontal disease treatment, or Pearl's Second Opinion solution, which helps dentist to spot conditions like cavities, tartar and inflammation, other AI tools are still in the research phase.2–5 As dental professionals adopt AI tools in the practice and research, it is imperative to address the ethical and legal considerations surrounding AI-enhanced dentistry. The currently two major legal and ethical frameworks, EU AI Act 6 and The Right to Notice and Explanation of AI Systems Used in Health Care 7 aim to govern the use of AI systems in the healthcare, with the EU AI Act providing legal safeguards and the Right to Notice and Explanation ensuring ethical transparency for patients. One should distinguish between regulatory frameworks—binding legal instruments such as the EU AI Act, which applies across EU member states—and ethical guidelines, such as the Right to Notice and Explanation of AI Systems Used in Health Care, which represents a bioethical standard without formal legal force but with strong influence on practice and debate. The sensitive issue of informed consent represents one of the most challenging issues regarding AI use in practice and research, yet the consensus surrounding this issue is lacking. 8 The aims of this study were: first, to identify key ethical principles, dilemmas, and regulatory gaps related to AI use in dentistry through thematic synthesis of the literature; and second, to translate these insights into a legally supported and clinically applicable informed consent checklist and decision-making flowchart, whose practical relevance was then evaluated through feedback from practicing dentists.
Method
Thematic analysis
This study employed a qualitative research design using thematic synthesis, to explore the ethical and legal dimensions of informed consent in the application of AI within dental practice. A comprehensive literature search was conducted using the following electronic databases: PubMed, Google Scholar, Web of Science, and covered publications from January 2016 to January 2025
Empirical assessment
An online self-administered, 14-item questionnaire in Serbian, consisting of closed-ended questions, was designed to explore dentists’ perceptions and opinions of the proposed checklist and decision flowchart. The questionnaire was developed de novo, based on themes identified in the literature synthesis and aligned with regulatory and ethical requirements for AI use in dentistry and it took approximately 10 min to complete survey. Items were designed to assess clarity, practicality, and feasibility of the proposed checklist and flowchart. A three-point Likert-type scale was used to collect clear and straightforward responses in a forced-choice format. This simplified scale (“agree,” “neutral,” “disagree”) was selected to encourage unambiguous responses and reduce bias in a pilot study with a small sample size. The initial draft was reviewed by two colleagues, to ensure face validity and linguistic clarity. Minor modifications were made to improve readability before distribution. Participation invitations were distributed via email to experienced dentists which use AI tools in private practices (purposive sampling), and participants were informed about research aims and investigator role. The study on the use of AI in dentistry received ethical approval from the Ethical Committee of the School of Dental Medicine (approval no. 36/7). The survey was administered by the author (JR), which holds a PhD in Medicine and MSc in Bioethics, at the time of study employed as university professor. No prior relationship was established with participants, who were only informed of the study's aims and procedures, while researcher's characteristics such as professional background and interest in AI ethics were disclosed to ensure transparency. As this was a pilot feasibility survey, no a priori sample size calculation was conducted. The survey was designed to provide preliminary insights into the clarity, practicality, and feasibility of the proposed checklist and flowchart rather than to achieve statistical generalizability. Data saturation was not applicable to the survey component, which employed closed-ended items, but was considered in the thematic synthesis of literature used to construct the framework.
Results
Overview of included literature
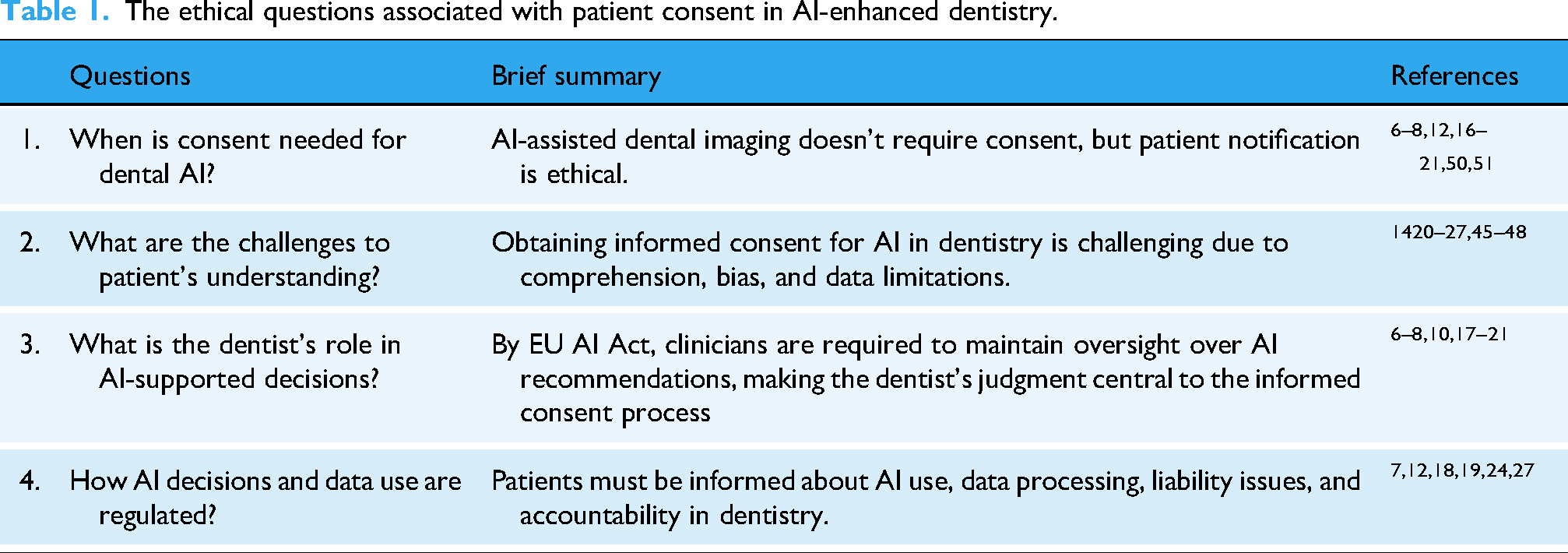
From 252 records identified, after duplicate removal and abstracts screened, 67 documents were assessed for eligibility. Of the 67 full-text articles reviewed, 17 were excluded due to insufficient detail on informed consent, lack of relevance to dentistry, or methodological inconsistency. The final 50 were subjected to thematic synthesis (Figure 1). These comprised 45 peer-reviewed journal articles, four legal or regulatory documents, and one book chapter. Namely, data extraction focused on identifying ethical challenges, regulatory frameworks (e.g. EU AI Act), and proposed strategies for informed consent in AI-enhanced dentistry. Extracted data were analyzed qualitatively to identify key themes and patterns (Table 1).

Flow diagram of literature search and selection.
The ethical questions associated with patient consent in AI-enhanced dentistry.
Thematic findings
A qualitative thematic synthesis was conducted following Braun and Clarke's six-phase framework, which is widely used for identifying patterns across literature. This method was selected due to its flexibility in analyzing diverse ethical, legal, and regulatory texts and its suitability for synthesizing complex issues where empirical consensus is lacking. 9 The process involved analysis of 50 selected publications: initial coding of relevant text segments, generation of candidate themes, refinement and naming of themes, and final synthesis. Thematic analysis was applied to data extracted from peer-reviewed literature and legal/regulatory documents related to AI ethics and informed consent in dentistry. Four key questions/themes were identified: (1)When is consent needed for dental AI?/ the uncertainty around when explicit patient consent is required, (2) What are the challenges to patient's understanding?/the difficulties around patient understanding of AI's role, (3) What is the dentist's role in AI-supported decisions?/ the importance of clinician oversight in maintaining trust, and (4) How AI decisions and data use are regulated?/the legal obligations related to automated decision-making and data use. These themes were critically compared and interpreted to inform a practical framework for consent in AI-enhanced dental care (Table 1).
Consent checklist and flowchart
Following the thematic synthesis of selected articles, key findings were converted into usable guidelines for everyday dental practice. A structured, dentistry-specific informed consent checklist (Table 2) was created to address recurring ethical concerns and communication gaps revealed in the literature such as patient understanding, clinician oversight, and legal obligations. This checklist provides clear recommendations for dental professionals to ensure they transparently communicate the role, function, and implications of AI tools used in diagnosis or treatment planning. In order to complement the checklist, a decision-making flowchart (Figure 2) was constructed to support dentists in evaluating whether explicit informed consent is required for AI tool which should be used. The flowchart categorizes AI tools based on their clinical function (e.g. supportive vs autonomous) and data use (e.g. dental care vs research/or algorithm training), aligning with current regulatory standards such as the GDPR 10 and EU AI Act. 6 These tools are designed to improve consistency in informed consent practices, translating ethical and legal principles into feasible actions in routine dental practice.
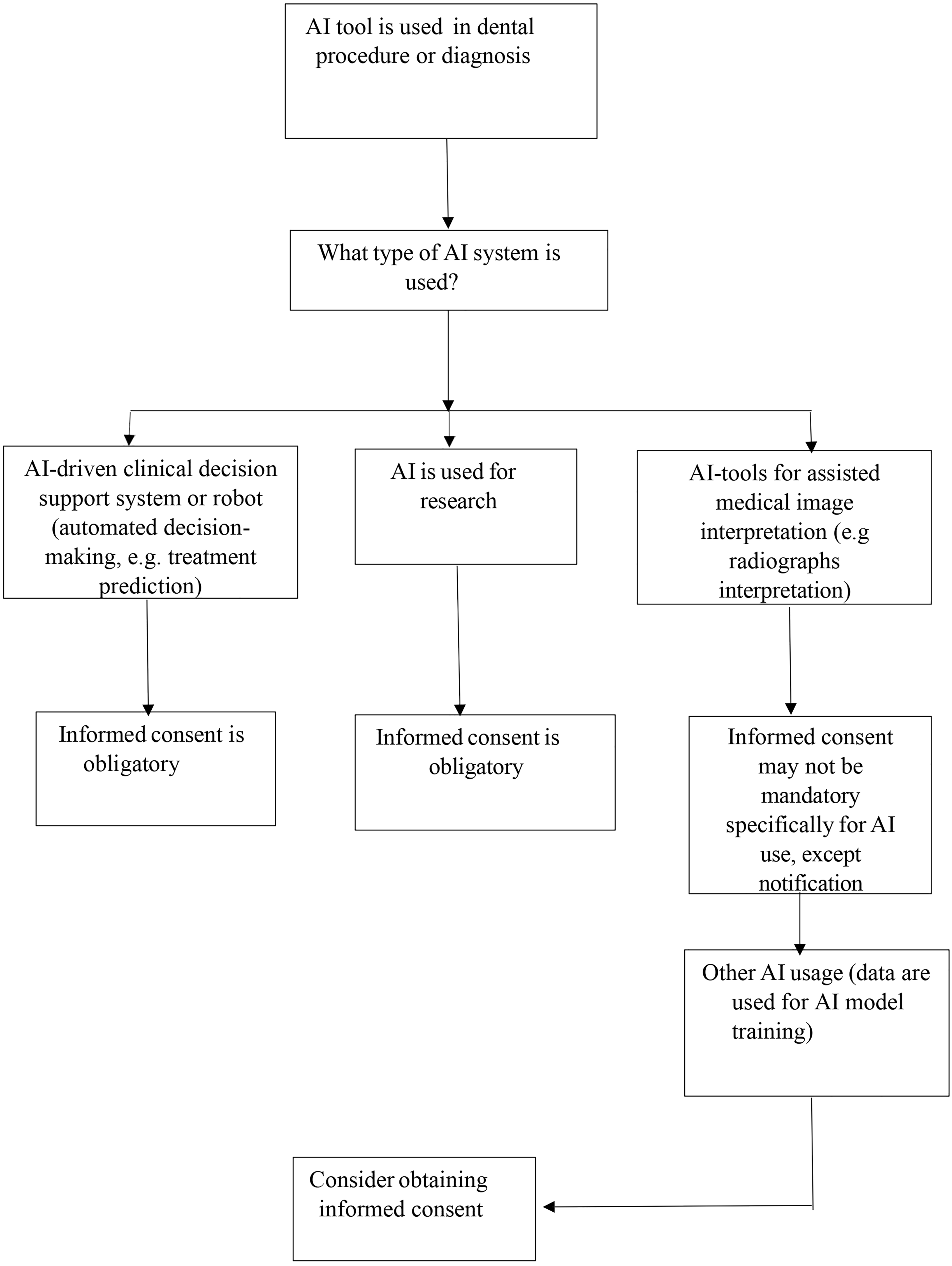
Decision flowchart for patient informed consent in AI-assisted dentistry.
Patient consent checklist in AI-enhanced dentistry.

Practicing dentists’ assessments on proposed consent checklist and flowchart
While invitations were sent to 30 e-mail addresses of Belgrade private dental offices, only 12 dentists responded, and answered the survey, nine women and three men, most respondents (58.3%) were aged 30–45 years; 16.7% were under 30 and 25.0% were over 45 years old and 11 of them had more than 10 years of working experience. Survey comprised of three parts: (1) checklist assessment; (2) flowchart assessment; (3) communication with patient. Based on the results presented in Table 3, the majority of dentists found both proposed checklist and flowchart highly acceptable and practical. Specifically, 83.3% of dentists agreed that the checklist is understandable, while 91.7% stated they would consider incorporating it into everyday dental practice. Moreover, 66.7% found the checklist feasible for daily practice, and the same percentage indicated that the flowchart aids in determining when explicit consent is required. Importantly, 91.7% agreed that standardized consent would improve communication, and an equal percentage noted patients feel reassured when AI is explained as being under clinician supervision. These findings affirm the checklist and diagram as supportive tools for enhancing patient autonomy and ethical practice in AI-assisted dentistry.
Practicing dentists’ assessments of consent checklist and flowchart.

Discussion
Presently proposed informed consent checklist and decision-making flowchart, to our knowledge, represent first attempt to guide dentist through informed consent process during AI use in dentistry, and, based on survey results, highly graded by practicing dentists which use AI tools. Previous studies have emphasized ethical principles and regulatory challenges2,11,12 but have not offered structured, clinically applicable tool tailored to dental practice. Failure to comply with emerging AI regulations may expose dentists and institutions to legal liability, including claims of negligence or breaches of data protection law.6,8 In particular, lack of explicit consent for AI-assisted decisions could be interpreted as a violation of patient rights under GDPR or the EU AI Act.6,10 The proposed checklist and flowchart serve as practical safeguards by standardizing consent procedures, thereby reducing legal risk while strengthening transparency and patient trust. The fact that only 12 dentists responded may be explained by the still limited adoption of AI tools in local dental practice, lack of confidence among practitioners unfamiliar with AI, and common barriers such as workload or lack of incentives. Additionally, the sensitivity of ethical and legal questions surrounding AI might have discouraged some dentists from participation as has been shown recently. 13 Namely, an international cross-sectional survey among dentists, showed that 70% of dentists endorsed obtaining written patient consent before medical interventions (25% disagreed, 5.7% were uncertain), while additional concerns were raised about AI's potential to influence clinical judgment, the need for transparency in algorithms, and the safeguarding of patient information. 13 Furthermore, it seems that factors related to sex, age, physical activity, and ethnicity play into preference for consent communication. 14 Noteworthy, presently developed clinically applicable tools were estimated as understandable, feasible, and supportive of both ethical practice and improved communication, with over 90% of responding dentists agreeing that standardized consent enhances patient trust when AI use is properly explained. Having in mind that recent study revealed that only about 10% of surveyed Serbian dentists were currently using or familiar with AI applications in dentistry, 15 it was challenging to identify and recruit participants who actively use these tools in practice. This limited adoption may be partly explained by a scepticism toward AI use among dentists shown in the same study, closely linked to a lack of both basic and continuing education on the topic, concern that AI might replace dental professionals, and anxiety related to the absence of clear regulatory policies and guidelines. 15 Therefore, the aim of this study was to develop a checklist and decision-making flowchart to address existing ethical gaps and as guidelines support dentists in responsibly integrating AI into everyday clinical practice.
As most regulatory-approved dental AI tools assist in image interpretation rather than making autonomous decisions, 5 their use generally falls under implied consent as part of routine clinical care.8,16,17 Namely, implied consent is consent assumed from a patient's actions in routine care, for example when a patient sits for a radiograph. Explicit consent, by contrast, is a clear oral or written agreement given after the patient receives full information about the procedure, risks, and alternatives, as required by GDPR Articles 13–15 and 22 for AI systems that process health data or make autonomous recommendations.10,16,17 Dentists already use digital imaging tools without separate consent, and AI is viewed as an extension of these technologies. 16 However, when AI tools function autonomously or process data such as in treatment recommendations, algorithm training, or third-party sharing, explicit consent is required under GDPR Articles 13–15 (which require patients to be informed about data processing and its purpose) and 22 (which restricts fully automated decision-making without explicit consent) as well as in line with recommendations from WHO and FDI World Dental Federation.10,18,19 Ethical literature supports this distinction, stressing transparency and informed consent especially for autonomous systems.6–8,16,17,20,21 Therefore, while AI-supported radiographic interpretation may not demand explicit consent, ethical practice supports patient notification about AI use and obligatory dentist oversight.
The main problem when obtaining informed consent for using AI lies in the lack of a certainty that the patient fully understands the technology, its risks and benefits, and can make an informed, voluntary decision. 20 There is also a question what kind of information is sufficient and optimal to achieve patient comprehension, necessary for the informed decision.14,22 The risk of consent without comprehension was noted as an ethical vulnerability, 23 particularly in procedures involving irreversible decisions in dentistry, such as teeth extractions or prosthodontic interventions.
The process of informed consent for AI deployment or research can involve complex theoretical concepts and terminology, not even well comprehended by dentists or medical doctors, and that may overwhelm or confuse patients.24,25 On the other side, patients often have limited knowledge of AI technology, particularly in how it is applied in dental care, and when patients do not fully understand the information, they might feel more anxious about the proposed procedure. 26 Therefore, some authors suggest that explanation should be limited to only a broad generic explanation of how the AI tool operates. 21 One such example could be like this: “The AI tool is based on a huge number of data, like thousands of books, and then AI found a pattern between patient data, symptoms, dental treatment he/she receives and treatment success. Thus, when AI tool looks at your health data, like your symptoms or anatomic details on your radiographs, it compares it with the patterns it has learned and based on it, predict will the dental treatment be optimal for you.”
By current regulations, such as the EU AI Act, clinicians are required to maintain oversight over AI recommendations, making the dentist's judgment central to the informed consent process. 27 Thus, patients should perceive AI tools as a “second opinion” which dentist critically assess and adapt AI suggestions to individual needs. In such circumstances, patient-doctor trust is reinforced and understanding improved. 27 This supports a model of balanced transparency which aims to focus not on how AI reaches its conclusions, but on why the clinician recommends a specific treatment. Thus, the emphasis should move from explaining how an AI tool generates its recommendations, which often challenges the feasibility of informed consent, to clarifying how the clinician interprets those suggestions, and makes the final decision (EU AI Act argues for obligatory human oversight). Since doctors are responsible for evaluation of AI recommendations and provide the final judgment, their reasoning becomes the central element to communicate to patients, much like in traditional informed consent. When patients see that the clinician values AI input but verifies and tailors it to their individual needs, they tend to perceive AI as enhancing—not replacing—the dentist's expertise. This balanced approach can foster trust and optimism by combining advanced technology with professional judgment.
The primary goal of AI in dentistry is to enhance diagnostic accuracy and treatment outcomes, particularly in areas prone to subjective interpretation.15,28 AI systems have shown high efficacy in detecting caries, periodontal disease, oral cancer, vertical root fractures, and periapical lesions.29–35 They also support orthodontic treatment planning, pulp diagnosis, and individualized care recommendations.36–44 Still, limitations in dental data quality, diversity, and standardization can introduce algorithmic bias, especially for underrepresented patient groups.45–47 Furthermore, cognitive biases from human-AI interaction—such as altered expectations based on system familiarity—must be considered when evaluating AI's impact in practice. 48
Under the GDPR, AI tools that process personal health data must meet standards of transparency, fairness, and data minimization. Patients should be informed about what data are collected, how they are processed, the logic of any automated decisions, and who will access the data and for how long. 10 Although digital health systems have long posed privacy risks, AI amplifies these concerns, highlighting the ongoing need to strengthen data security in clinical practice. 49 In dentistry, AI tools used for image interpretation generally carry low risk, as dentists retain full responsibility for treatment decisions and use AI as a supportive tool.12,50,51 However, questions of liability remain unresolved when adverse outcomes arise. According to WHO and FDI guidance, assigning responsibility is difficult due to the shared roles among clinicians, AI system developers, and approving institutions18–19,24 dentists may be liable if they misuse AI tools, fail to review recommendations, or apply unapproved systems. Conversely, regulatory bodies and developers could be accountable for harm caused by poor design, inadequate approval processes, or lack of training. Even when fault is unclear, patients should be eligible for compensation. To address these concerns and improve practice, a structured consent checklist is presently proposed to guide dentists in discussing AI-supported treatment predictions and addressing patient concerns.
Limitations
This study has several limitations. First, no formal sample size calculation was performed for the pilot survey, and data saturation was not applicable to its closed-ended design. The number of dentists who responded to survey was limited to 12, and all respondents were recruited from Serbian dental clinics, which introduces a potential sampling bias and limits the generalizability of the findings to other cultural and regulatory contexts. Second, while the informed consent checklist was developed through a synthesis of international ethical and legal frameworks and informed by expert discussion during manuscript preparation, it has not yet undergone formal external validation by independent expert panels or tested across diverse international cohorts. Consequently, present findings should be interpreted as preliminary and exploratory and future research should focus on validating the checklist content and evaluating its applicability in cross-cultural settings.
Conclusions
The implementation of informed consent in AI-assisted dentistry can vary significantly depending on cultural norms, legal frameworks, and regulatory requirements. These differences influence how practitioners approach transparency, communication, and ethical obligations when using AI in patient care. The proposed consent checklist and flowchart provide a clinically applicable framework that strengthens patient autonomy, supports ethical and transparent AI use in dentistry, and offers guidance for practitioners navigating emerging regulatory requirements.
The rapid progress of AI tools suggests that in the near future it may not be possible to offer non-AI-enhanced medical or dental practice nor to avoid use of autonomous robots, and probably that would impose different ethical standards in the patient care. For now, patients should be provided with all necessary information about AI tool used in dental treatment prediction or recommendation, and respect their right to consent or decline the use of AI in their care.
Best practice
In AI-assisted dentistry the focus should be put on translating ethical principles into actionable protocols aligned with evolving regulations. For dentists, the proposed checklist and consent flowchart can guide decisions on when explicit consent is required, while patient discussions should emphasize the clinician's reasoning rather than technical details of algorithms. The educators should integrate AI consent training into curricula through case-based discussions and simulations, ensuring that students develop both ethical awareness and communication skills. The AI developers should be encouraged to design transparent and comprehensible systems that preserve privacy protection, and the central role of human oversight. The Ethics committees should periodically review AI-informed consent procedures to ensure alignment with legal frameworks and provide structured feedback to clinicians and developers. Finally, the regulators should work toward harmonizing international consent requirements and monitoring compliance to safeguard transparency, privacy, and patient autonomy.
Footnotes
Acknowledgements
The author would like to thank Dr Milena Barać for assistance.
Ethical approval
Ethical approval was obtained from the Ethical Committee of the School of Dental Medicine, number 36/7.
Author contribution
J.R.: conceptualization, methodology, analyses, review.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.