
Abstract
Objectives
Globally, the prevalence of long-term conditions (LTCs) continues to rise. The impact of LTCs presents significant challenges for international health and social care systems and continues to be a leading cause of mortality. Despite this, digital health coaching interventions (DHCIs) appear to be a promising strategy for managing chronic disease. The aims of this systematic review and narrative synthesis were to explore the barriers and enablers for the use of DHCIs and to gather valuable information to inform the development of a new DHCI for LTC management.
Methods
Six major databases were searched for studies published in the English language between January 2012 and December 2022. Qualitative and mixed methods studies were included if there was an intervention of digital health coaching alongside the use of a digital component. Interventions were suitable if completed in community settings, amongst adults aged over 18 with a LTC, or amongst informal carers, health coaches, or health and care professionals. Included studies were assessed for quality, and results were analysed with narrative synthesis.
Results
Ten studies met the inclusion criteria, covering a range of LTCs and interventions which included digital health coaching (telephone, video, online, text) and the use of a digital component (online, application-based). Results showed that DHCIs require personalisation and feedback, and cannot be overcomplex. Importantly, an element of human connection is favourable.
Conclusions
The acceptability of DHCIs is variable- and context-dependent. Further research is needed to focus on the breadth of LTCs in order to generalise findings.
Introduction
Globally longer life expectancy, improved healthcare, physical inactivity, obesity, socio-economic deprivation and increasingly unhealthy lifestyles have led to an increase in long-term conditions (LTCs). 1 LTCs are defined by the World Health Organization (WHO) as being of long duration, generally slow in progression and not transmissible from person to person. 2 Common LTCs are hypertension, chronic obstructive pulmonary disease (COPD), asthma, type 2 diabetes mellitus (T2DM), and heart failure. 3 In the United Kingdom (UK), almost half of the adult population reported living with a LTC in 2019. 4 LTCs constitute one of the single greatest challenges for UK and international health and social care systems, with LTCs the leading cause of morbidity, disability, and cost. 1 Projections from the global mortality and the burden of diseases estimate that LTCs will account for around 75% of all global deaths in 2030 and will result in enormous socio-economic impacts due to the costs of expensive and often prolonged treatments.1,5
Digital health interventions (DHIs) (i.e., health interventions delivered via digital technologies such as a smartphone, website, or text messaging) can provide effective, safe, cost-effective, and scalable interventions to improve preventative healthcare strategies. 6 DHIs have been shown to be effective for a range of conditions and demonstrate behaviour changes, such as smoking cessation amongst adult smokers and adults with T2DM,7,8 increasing physical activity amongst adults with chronic diseases9,10 and improving knowledge, self-efficacy, and clinical outcomes amongst adults with diabetes mellitus, ischaemic heart disease, asthma, chronic obstructive pulmonary disease, epilepsy, Parkinson's disease, Alzheimer's disease, arthritis and renal failure. 11 DHIs are often complex interventions with multifaceted components, with multiple aims including health education, modifying health beliefs, assessing or monitoring health states, providing medication advice, clarifying health priorities, and improving communication between patients and healthcare professionals (HCPs). 6 Despite the potential healthcare benefits of DHIs, implementation is not straightforward, especially when supporting the management of LTCs. 12 First, it is difficult to create a universally accepted ‘digital recipe’ for a LTC because, from a patient's perspective, strategies for the self-management of the LTC may vary depending on factors such as intrinsic motivation, 13 socio-cultural and socio-economic status. 12 Second, from the perspective of a healthcare system, different healthcare organisations have varying legislative and policy implications for adoption of DHIs. 14 Further, most current DHIs are at different stages of development and evaluation, with some being well-established, and others more novel. Consequently, the strength of evidence for studies using DHIs for LTCs varies significantly. 6
It appears that DHIs which incorporate social support, prompts or cues, credible sources of information and behaviour change achieve effective outcomes for the prevention and management of LTCs. 15 One particular intervention known as Health and Wellbeing Coaching (HWBC) is an embedded service within UK primary care services 16 and aims to incorporate the aforementioned factors and has been shown to be a promising intervention to support effective lifestyle changes to improve the management of LTCs such as asthma, T2DM, cardiovascular disease, and mental illness. 17 Unfortunately, evidence to support effective delivery of HWBC delivered digitally, alongside a DHI is lacking as well as what people living in the community with LTCs and their carers perceive and experience when engaging with digital HWBC. There is also limited evidence and understanding from health coaches and health and social care professionals (HSCPs) about their perceptions and experiences of digital HWBC. Further research is needed to explore this gap to provide new knowledge of the perceptions and experiences from multiple stakeholder perspectives to improve the management of LTC in the community using DHIs. To address these issues, this systematic review and narrative synthesis aims to understand i) the barriers and enablers to effective digital HWBC from multiple stakeholders’ perspectives and ii) provide new knowledge to inform the development of well-designed DHIs for LTC management.
The research question was ‘What are the perspectives and experiences of digital health coaching interventions among adults living with long term conditions, carers, health coaches, and health and social care professionals?’. Digital health coaching interventions refer to both the health coaching and digital support (e.g., apps, websites) given alongside this.
Methods
This is a systematic review and narrative synthesis design. The methodology for this review was submitted to PROSPERO (International Prospective Register of Systematic Reviews) and is available online (CRD42022347876). 18
Search strategy
The electronic databases MEDLINE Complete, Web of Science, CINAHL, PsycInfo, SCOPUS, and PubMed were searched in December 2022. The search was limited to articles published in English between January 2012 and December 2022; due to digital innovation being so fast-paced, any studies published before this date were deemed likely to be less relevant. The search and screening process was repeated in April 2024 to capture any articles between December 2022 and April 2024.
The search terms were defined using the SPIDER mnemonic for qualitative evidence synthesis. 19 An example of the search strategy used is long term condition* OR long-term condition* OR chronic disease* OR multimorbidit* OR multi-morbidit* OR adult* OR people OR frail* OR ‘living with frail*’ AND carer* OR caregiver* OR health coach* OR health care professional* OR health care provider* OR social care professional* OR social care provider* AND behaviour change interven* OR health coach* OR wellbeing coach* OR self-management AND Mhealth OR mobile health OR telehealth OR ehealth OR telemedicine AND interview* OR ‘focus group*’ OR case stud* OR ‘observ*’ OR questionnaire* OR survey* OR perspective* OR view* OR experience* OR opinion* OR attitude* OR perception* OR belief* OR feeling* OR knowledge OR understanding* OR barrier* OR facilitator* OR outcome*. This syntax was adapted for each database, including the same keywords in each. Following the initial study selection, additional search strategies were used to identify potentially relevant papers. These included searching the publications of the first and last authors for highlighted papers, citation tracking to capture any newer studies not previously highlighted by search terms, and bibliographic mining of the reference lists of included studies.
Study selection
A two-stage screening process was completed by RAC between December 2022 and April 2024. This included an initial screening of titles and abstracts and full-text screening. A further two researchers (MS and MAP) were involved in full-text review for eligibility and inclusion. A quality appraisal team (JM and ES) reviewed the final inclusion list and any articles where the researchers could not make a decision. The research team used EndNote 20 20 for screening papers from imported searches and reference management.
Inclusion and exclusion criteria
Included in this review were studies involving adults with a LTC, who received a digital health coaching intervention in a community setting and where qualitative evaluation methods were used to examine the experiences of adults with LTCs, carers and/or the HSCPs involved. Specific inclusion and exclusion criteria are shown in Table 1.
Study inclusion and exclusion criteria.

Theoretical framework
Our narrative synthesis was informed by Normalisation Process Theory (NPT). 21 NPT is a framework to aid understanding of the process of implementing and embedding a new innovative complex intervention into routine practice, such that it becomes a part of routine care practices, i.e., is ‘normalised’. NPT has four main inter-related determinants related to the work of embedding innovations into routine practice which are shaped by contextual factors such as organisational structures and social norms. These are coherence (or sense-making), cognitive participation (engagement), collective action (joint work to enact in practice), and reflexive monitoring (ongoing appraisal).21,22 NPT was used in our narrative synthesis because it offered a useful framework to understand the factors perceived to promote and inhibit the incorporation of complex digital health care interventions into healthcare systems from the perspectives of service users and professionals.
Data extraction and synthesis
The selected papers used different study designs and methods and covered a wide range of interventions for different LTCs. To understand the barriers and facilitators of digital health coaching initiatives a narrative synthesis approach was used to examine the similarities and differences in the experiences of people with LTCs, carers and HSCPs. The Economic and Social Research Council (ESRC) framework for conducting a narrative synthesis 23 was used to guide the conduct of the narrative synthesis.
An inductive approach was used for the narrative synthesis; the first step was to tabulate the key characteristics and main findings of the selected studies (Table 2). Qualitative data were extracted in the form of quotations from participants, sub-themes, and themes identified by the study's authors. The findings were coded into initial themes and the one sheet of paper method 24 was used to visually map and develop these themes, identifying similarities and differences to produce broader conceptual themes and subthemes. Finally, the findings were mapped to the Normalisation Process Theory 21 which informed further theoretical insights from the qualitative data and to guide and evaluate the process of interventions.
Study characteristics.
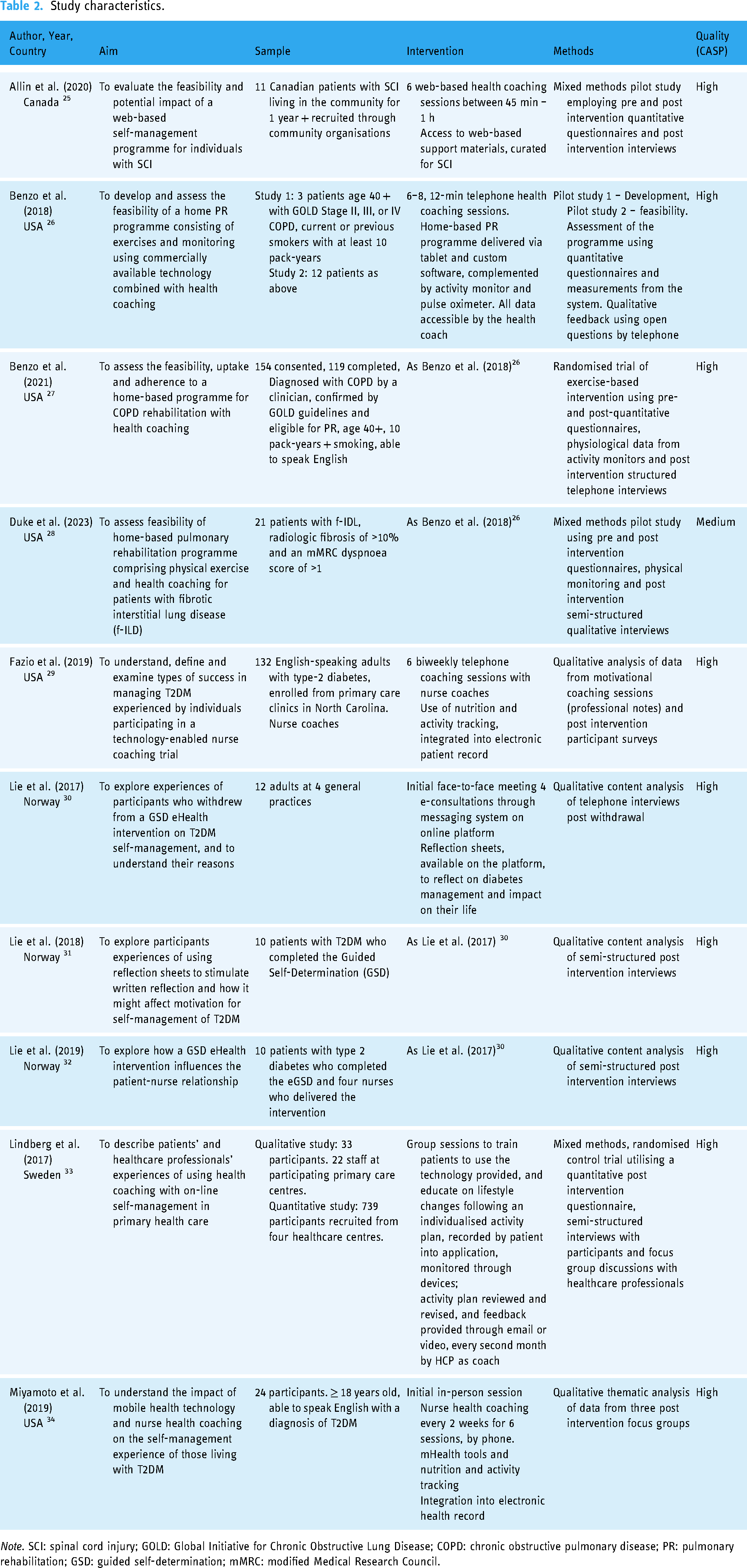
Note. SCI: spinal cord injury; GOLD: Global Initiative for Chronic Obstructive Lung Disease; COPD: chronic obstructive pulmonary disease; PR: pulmonary rehabilitation; GSD: guided self-determination; mMRC: modified Medical Research Council.
Methodological quality
The methodological quality of the studies was assessed using the CASP (Critical Appraisal Skills Programme) checklist for Qualitative studies 35 independently by one author initially (MAP), and independently by two other authors (KL and RAC) to provide their own rating. This was then cross-checked against each author's score. A quality appraisal team (MS, RAC, and KL) then discussed each paper and any inconsistencies to derive a consensus rating, as shown in Table 2. All studies were included in the analysis as they were all rated to be medium to high quality. The included25–34 papers all used the appropriate methodology and research design, and all demonstrated significant value in the results through novelty, transferability to similar populations, and identification of new areas for research. In addition, there was a clear statement of findings in each. Duke et al. 28 had a medium-quality rating, compared to the other high-quality studies. This was because it did not include a clear statement of the aims of the research, or the recruitment strategy, and the method of qualitative analysis was not explained, so could not be said to be of sufficient rigour. Additionally, there was no statement of ethical considerations or evidence of consideration between the researcher and participants.
Results
Our database searching (see Figure 1) returned 11,222 records, of which 4329 were removed before screening due to duplication. A further 6750 were removed as not answering the question, following title and abstract screening. One hundred and forty-three articles were retrieved for full-text screening, and 8 were deemed to meet our inclusion criteria. A further two articles were identified through citation tracking, bibliographic mining, first and last author searches, and contacting experts.

PRISMA flowchart of the screening process.
Study characteristics
The characteristics of the synthesised studies are summarised in Table 2.
The included studies were published from 2017 until 2021. The majority of studies were from North America, with five from the United States26–29,34 and one from Canada. 25 The remaining studies were Scandinavian, with three studies from Norway30–32 and one from Sweden. 33 None of the identified studies included carer perspectives, with all of them exploring patients’ perspectives of digital health coaching. Six of these looked solely at patient perspectives,25–28,30,31,34 with two examining combined patient and health coach perspectives,29,32 and one assessing patient and health care professionals’ views. 33 No studies examined social care professionals’ perspectives.
The subject of the digital health coaching interventions was largely focussed on T2DM. Five of the ten studies focused solely on T2DM,29–32,34 with a further one exploring patients with either T2DM, heart disease, or hypertension. 33 Of these, three studies were about one guided self-determination protocol.30–32 One study focused on individuals who had been living with spinal cord injury in the community for a year or more. 25 Two studies examined COPD,26,27 with one being the development stage and the latter a feasibility study. A further study tested the same home-based PR protocol on participants with fibrotic interstitial lung diseases (f-ILDs). 28
Five of the studies used only qualitative methods,29–32,34 with the remaining five being mixed methods where the qualitative work was part of a larger trial.25–28,33 For the purpose of this synthesis, only the qualitative work has been included.
Narrative synthesis
Four main themes were identified, ‘Perception and prioritisation of health condition’, ‘Environment’, ‘Sustained change’, and ‘Embedding change’, with an overarching theme of ‘Reflection’ interwoven with these. Themes in this synthesis will be discussed in relation to service users, health coaches, or health care professional perspectives and experiences, perceived outcomes and barriers and facilitators. Table 3 shows the themes, subthemes, and relevant studies associated with the different perspectives.
Themes, subthemes and related study perspectives.

Reflection
Reflection was an overarching theme, apparent in each of the four main themes presented: ‘Perception and prioritisation of health condition’; ‘Social and physical environment’; Sustained change’; and ‘Embedding change’. Reflection encompassed the process of developing a deeper understanding of a situation and one's self in order to inform future practice. 36 This can be done individually or in a group scenario. Within NPT, reflection relates to the construct of reflexive monitoring, the process of assessing and understanding the impact of new processes on themselves and others. 37 This involves reviewing how useful a process may be, working together or individually, and changing and shaping it as needed.
In the context of the theme ‘Perception and prioritisation of health condition’, interventions involving a conversation with a health coach led to deeper reflection for participants in three US-based studies on their diagnosis and its impact on their health.26,28,34 In each of the studies, telephone-based health coaching was provided and was complemented by an mHealth platform. Where the use of mHealth was in the form of online pulmonary rehabilitation (PR) for COPD, 26 one participant reflected on how the intervention as a whole had improved how they feel, and stated it ‘opened [their] eyes to what [they] should be doing’. 26 The use of mHealth by other participants was not defined but was a support to the health coaching for f-ILDs 28 and T2DM. 34 In this study, a participant stated that taking part in the intervention caused her to reflect on her identity as being ‘diabetic’. 34 Similarly to the participant in the COPD study, another focused on the realisation of their inactivity, and how becoming aware of this made them more motivated and focused to practise more self-management behaviours. 34 In both studies, it can be inferred that digital health coaching provided the space for participants to reflect on the role of their health condition within their life, and therefore make improvements to their health. In summary, reflection allowed participants to review their own perception of their health condition, and how they prioritised the management of their health.
Within the theme of ‘social and physical environment’, the novel delivery of digital health coaching, and the use of reflection, provided empowerment and a sense of clarity in the reasoning behind their healthcare.30,31,34 These studies were in patients with a diagnosis of T2DM, one being a US-based study with mHealth alongside telephone health coaching,
34
and the others Norwegian studies of a more ‘pure’ digital health intervention, with one or two face to face sessions and four consultations through secure messaging on a web portal.30,31 Participants across these studies reported that digital health coaching and reflection enabled them to give their health coach more accurate information about how they were progressing with the coaching and digital intervention and their condition, suggesting that they were able to access better care as it would be more tailored to their needs. This was echoed by several health coaches in a Norwegian study, who noted that patients benefitted from having to reflect on their experience and share what matters to them when using written reflection as a tool.
31
In contrast, where one participant in a Norwegian study did not allow themselves space for reflection, there was a clear disconnect between the benefits of looking after their health to live their life, and the reality of their diabetes, exemplified here: Because I feel healthy, and I do not want to be sick. But I am sick… But I want to live life as well. There is a limit there somewhere.
30
Reflection in terms of ‘Sustained change’ enabled participants to realise how the process of digital health coaching benefitted them, whether facilitated by the health coach or on their own.27,34 Reflections where this was exemplified were from American studies, one focused on T2DM, 34 the other on COPD. 27 Across these studies, participants reflected that digital health coaching gave them the confidence to look after their health, and acknowledge their own role in taking care of their condition. One man in the diabetes study reflected that he ‘got the sense that [the coach] was trying to empower [him]… it gave [him] that responsibility for [himself]’. 34 A woman in the same study illustrated the impact of not reflecting on her own responsibility in managing her health, as she stated her blood glucose levels now ‘get too good, they get too low’. 34 These comments demonstrate the value of reflection and acknowledging one's own impact on health in the management of LTCs, suggesting that it is a vital component of digital health coaching.
‘Embedding change’, like reflection, aligns closely with reflexive monitoring in NPT. The focus of these reflections was the relationship and shared experience participants had with their health coaches, and importance of feedback. Three studies from Canada, Norway, and Sweden of participants with spinal cord injury, 25 T2DM, 32 and T2DM, heart disease or hypertension 33 provided evidence for the value of individualised feedback and consistent relationships with the health coach. One participant in the Norwegian T2DM study emphasised the importance of this consistency for the health coach to know what advice is appropriate based on what other areas of life are impacting the patient. 32 Furthermore, several participants in the Canadian Spinal Cord Injury study perceived the advice from their coaches to be more valuable as they could identify with their disabilities/LTCs, due to having similar lived experiences. 25 Similarly, the majority of participants across three studies highlighted the necessity of regular personalised feedback from their coach25,32,33; for example, one participant in the Swedish LTC study reported they ‘don’t believe technology can be good if you do not have individual follow-up or feedback, but … the feedback can be handled by phone or mail; it's not necessary to have personal meetings’. 33 Similarly, a health coach in another Norwegian T2DM study emphasised that consistency with the coach, and an initial face-to-face meeting were essential in building a relationship with patients, and the patient being able to reflect further. 31
Perception and prioritisation of health condition (distancing from diagnosis, health literacy, and knowledge about LTC and patient experience)
This theme related to how participants viewed and valued digital health coaching interventions for the management of their LTC. It comprised two subthemes: ‘Distancing from diagnosis’ which focused on the role of identifying with or accepting a diagnosis, and ‘Health literacy, and knowledge about LTC and patient experience’ related to how participants’ knowledge of health care and their LTC, as well as providers’ understanding of the patient experience impacts digital health coaching. This relates to the NPT concept of ‘Coherence’ because it is about understanding the value of digital health coaching and making sense of the intervention in the context of LTCs.
Distancing from diagnosis
In two papers from a Norwegian study, participants’ described how their identity related to their diagnosis of T2DM had a pronounced impact on their engagement with digital health coaching and self-management of their condition.30,31 One paper focused on those who had dropped out of the study, and their reasons for doing so.
30
Participants had a clear disconnect from the identity of ‘being sick’
30
and saw focusing on their diabetes as taking away from their life, perhaps not understanding the improved quality of life they would experience with better self-management. This was also evidenced by a participant in the US study on f-ILDs,
28
who spoke of their realisation they had been in denial about the impact of their health, previously putting faith in a magic cure: Then I had that epiphany moment… I’m in denial about my lung disease. That was a pivotal moment for me. It changed how I looked at it.
28
Health literacy, and knowledge about long-term conditions and patient experience
Knowledge, whether in the form of health literacy, or understanding of LTCs and how this impacts people with that condition, was highlighted in all but one of the studies in this synthesis.25–28,30–34 A Canadian study on digital health coaching for spinal cord injury (SCI) found that knowledge imparted by the coach to the patient was a key feature of the intervention, for example with coaches acting as role models or supporters to enable behaviour change, or advisors when participants had technical requests.
25
Two American studies with COPD patients found that participants knowing, or learning through their coach, that exercises were specifically geared to the participants’ diagnosis increased motivation to complete exercises and stay ‘regimented’
26
to the program.26,27 For example, participants in one study said: …when you explained to me that the slow walking really helps me work on my balance, I really thought about it and plan to really work on it.
26
A Swedish study which included participants with T2DM, heart disease, or hypertension found that participants became empowered through knowledge of their health condition and the value of exercise, by making them ‘feel confident when [they] have control’. 33 This was echoed by a number of participants in US studies on health coaching for Type 2 diabetes, 29 and f-ILDs. 28 Participants also stated that the visual representation of their improvement, via a health tracker and changing clothes sizes, led to a change in mindset and therefore better self-management behaviours.
Two papers from the Norwegian T2DM study found that patients’ knowledge about their diabetes and experience of digital health coaching was enhanced through the method of communication, and having the space and time to reflect on their experiences.31,32 For instance, one service user reflected that having regular online communication facilitated more open communication as the coach is aware ‘perhaps the family situation indicates that I cannot do all these things’, 32 so would not set unrealistic tasks for the participant. One coach in a Norwegian study with patients with T2DM highlighted the importance of the patient knowing that they have understood and reflected upon the information they have shared, and suggested an initial face-to-face meeting was essential in order to facilitate this open communication. 32
A lack of knowledge and/or health literacy also had a significant impact on patient experience. Dropouts were reported in three studies30,31,33 due to a lack of knowledge on how digital systems work, 33 what the purpose of coaching activities was, 30 and not understanding the impact of their health conditions and the importance of self-management for this.30,31 This observation was also reported in a Swedish study using digital health coaching for patients with diagnoses including T2DM, heart disease, and hypertension as health coaches felt digital health coaching was something for the future, as they were not in the generation to use digital interventions. 33 This suggests that appropriate and high quality education, for both service-users and health coaches, is essential in ensuring that interventions can be delivered effectively and in minimising dropouts.
Furthermore, although for some participants in a US study a visual representation of their activity provided a positive change in mindset and motivation to continue working on their health, in other studies the inverse was shown.
29
This could be accounted by the problem of ‘how inactive [they] had been’,
29
without providing any solutions. In addition, participants reported that there was confusion when the actual benefit reported did not match the perception they had of the impact the intervention would have on their health.29,33,34 For example, in a US study on T2DM, one participant stated: If all of this is good, why did my A1C go up? It just baffles me. I guess that's what's frustrating.
29
Social and physical environment (shifting interpersonal dynamics associated with intervention delivery, frustrations around managing LTC)
This theme largely focuses on how the setting of digital health coaching, or social and physical aspects of it, impacted participants and providers. The subtheme ‘Shifting interpersonal dynamics associated with intervention delivery’ related to how the relationship between the participant and health coach was influenced due to its frequency and telehealth delivery. Whereas the subtheme ‘Frustrations around managing LTC’ encompassed participants’ frustration with the impact of their conditions, as well as with digital health coaching in managing their LTC. This aligns with the NPT concept of ‘Cognitive participation’ as it highlights factors which impact participants’ and providers’ engagement with digital health coaching.
Shifting interpersonal dynamics associated with intervention delivery
The diversion of digitally enabled health coaching from the traditional setting of a GP surgery led to some patients having differing experiences of their healthcare, which impacted the relationships with the interventions and with their health coaches. Some patients reported that having ‘an exercise program that's specifically designed for [their health condition]’ 27 was very encouraging as they knew that they could do the activities. Similarly, in a Norwegian study, participants valued the additional contact with a coach as it made it easier for them to access information specific to their health as the threshold for contacting an HCP was much lower. 32
Patients in two studies also found that reflection tasks enabled them to provide more accurate information
30
and prioritise their health
31
than in traditional contact with HCPs. For example, one service user in a Norwegian study on coaching for T2DM reflected: Earlier follow-up has just been blood samples and other tests, and then finished and “goodbye”. I have not had time to express thoughts and emotions, and […] That was what I appreciated, that I could finally communicate with someone about it. How I experience all of it.
31
However, the counterpoint to this was that a number of patients across two studies missed having face-to-face encounters, where they could see the person they were talking to.30,32 This was due to them feeling that misunderstandings were easier to rectify when sitting next to each other, 30 and asking for support would result in a more immediate response when face-to-face. 32
Frustrations around managing LTC
A minority of participants in four studies25,28,29,34 reported their frustration with their health; some stated that monitoring their health had made them go from having too little control over blood glucose to being far too strict and at risk of hypoglycaemia. 34 Some participants had a goal of reducing their levels of frustration and depression due to their LTC, 25 or expressed frustration at the changes they had to make to their lifestyles. 28 Frustration was also caused by the health coaching benefits not matching participants’ perceived or ideal benefits. 29 In one study, some participants also reported that they found ‘traditional’ interactions with HCPs frustrating, as there was not time to fully communicate their thoughts and feelings. 31
Two studies26,30 reported that many of the participants found the technology a barrier to them engaging in the intervention. For several participants, this was due to bugs or the technology being too complex. For others, the main difficulty with using digital health coaching was the impact it had on usual communication, whether it was due to them feeling less able to access support if stuck on a task 32 or lacking feedback, 33 saying they could never go without face-to-face contact.32,33 A health coach in a Norwegian study also found the use of online communication to be a barrier to engaging with patients, as they lost moderation through humour and support words. 32
In two studies,26,31 participants found digital health coaching to be frustrating, with a desire for more variety than the prescriptive nature of the digital platforms allowed,
26
or difficulties understanding the tasks set, which meant they would have to wait until a face-to-face session to progress in the intervention.
31
Several participants in two studies found that the time they had to dedicate to the intervention was frustrating, finding it a burden on top of other priorities in life.30,31 For example, one participant stated: It became a bit too much on top of everything else, having to sit down and spend time there, and remember to send and, yeah… There was too much else that had to be paramount somehow. Therefore, I simply had to downgrade it.
30
Sustained change (stages of behaviour change process, discipline and factors affecting motivation)
‘Sustained change’ is about the processes and motivations underlying behaviour change within digital health coaching interventions. This includes two subthemes: ‘Stages of behaviour change process’ which relate to participants’ willingness and readiness to change, examined through the lens of The Transtheoretical Model. 38 ‘Discipline and factors affecting motivation’ focuses on what impacts participants’ motivation, and whether they act on this. This aligns with the NPT concept of ‘collective action’, which focuses on enabling factors for interventions to happen.
Stages of behaviour change process
Individuals with LTCs described being at varying stages of behaviour change in seven of the ten included studies in relation to improving self-management of their long-term conditions as a result of receiving digital health coaching.26,29–34 The Transtheoretical Model presents behaviour change as a sequential process through six defined stages, and is often used to model health behaviour change such as smoking or alcohol cessation, and weight loss. 38 Despite the authors of these studies not applying behaviour change models to their work, this synthesis is applying them retrospectively to infer why participants may, or may not, have improved their self-management behaviours.
A minority of participants, who dropped out of the health coaching, described being at the precontemplation stage of behaviour change.29,30 Precontemplation is defined as where an individual does not intend to change their behaviour within the next 6 months, whether due to not being aware of the consequences of their current behaviour, or being in doubt of their ability to change. 38 There was a lack of understanding of the reasoning and methods of digital health coaching, in particular the reflective activities, which led to a loss of interest. 30 Some also reflected they were at the contemplation stage, now being aware of how inactive they had been, but not yet in the process of changing those behaviours. 29 This was echoed by healthcare personnel in a Swedish study, who expressed reluctance to deviate from traditional forms of patient interaction. 33 For example, one participant expressed that they only looked at data input by the patient when they attended face-to-face appointments, rather than following up via the application as intended. However, in a Norwegian study on coaching for T2DM, nurses acknowledged the value of digital communication for patients, but stated that it became too complex and time consuming as a new intervention, but could be more valuable with extra training and time, once embedded in standard practice. 32
A more common observation was participants in two studies described being at the preparation stage of the TTM, where they were acknowledging their new knowledge and motivation to make improvements to their health,26,34,38 with several participants acknowledging the importance of the health coach and digital support in providing the foundations for behaviour change to be possible, as it ‘helped [them] focus a little better’.
34
This suggests that they were ready to receive the support of digital health coaching, as they were feeling ready to take action on their behaviour, exemplified by a participant in a US study: When you explained to me that the slow walking really helps me work on my balance, I really thought about it and plan to really work on it.
26
Many participants with T2DM across three studies29,32,34 described being in the final stages of behaviour change, action and maintenance, 38 although the success of this varied between them. A number of participants expressed being more able to ask for support from their coach, 32 and reflected on their lifestyle changes being matched by their mindset, for example changing their perception from being too busy to go on walks. 29 Some participants in one study shared that they were able to be more intuitive with their blood glucose levels after support from their coach had ended, 34 suggesting the power of this approach enable sustained behaviour change.
This was also reflected in nursing notes in a US study on nurse-led coaching for T2DM. 29 Reflections were made by a small number of nurses on improved attendance of health appointments, physical aspects such as stamina, fatigue and walking pace, and mental health improvements. This highlights how the impact of digital health coaching was recognised by the health coaches, on both the participants’ behaviour and the subsequent improvement of their health.
Several participants in two studies from Norway and Sweden reflected on the difficulty maintaining their health once support from the health coach had ceased,31,34 as they no longer had someone to hold them accountable and were relying on their own will. For example, a female participant with T2DM described: I continued to wear my watch, but I didn’t watch what I ate as well as I should have. So, not having that person check on me regularly… it's on you.
34
A minority of people with T2DM in one study also reflected that their health monitoring behaviour had changed too drastically, with their blood glucose levels changing from being too high to at risk of hypoglycaemia. 34 Others reflected that although they saw the value of digital health coaching, they could never see a full system change occurring due to their need for face-to-face appointments. 32
Discipline and factors affecting motivation
In two studies,33,34 some participants reported the importance of having an innate motivation or sense of discipline in order to action their coach's advice. 34 It was stated that the action of talking about themselves and being more aware of their behaviour led to this innate motivation.33,34 However, a majority of participants reported that the coach and use of digital monitoring provided the motivation and discipline they needed to become more adept at managing their long-term conditions.25–29,34 This was noted by some of the health coaches in a US and a Swedish study, where one health coach in the US study acknowledged the shift in a participant's mindset as they were no longer missing or cancelling appointments, 29 and several in the Swedish study encouraged the participants’ discipline and motivation by emphasising their responsibility and that the digital platform was ‘for them’. 33
Many participants in three studies27,29,34 reflected on the modality of the intervention leading to a change in mindset and feeling better, which provided them with the discipline and motivation to continue to practise good self-management. Several found the written communication through digital coaching, or reflection sheets, to provide more discipline than traditional discussions with healthcare professionals, as it formed a contract in their mind. 31 A possible reason was that the increased contact allowed the health coach to be more aware of what was going on in each service user's life, which meant that they were able to give more appropriate advice which was therefore easier to follow. 32
Some participants from a US study acknowledged that they recruited friends and family members to support them in sustaining their health goals, utilising all available support to increase their motivation and discipline: I need help when I just say – like I told everybody, I don’t wanna eat the – help me know. Help me make that decision.
34
Many of the studies reported that participants lacked discipline and motivation to change their behaviour,29–31,33,34 despite the coaching input.29,30 Several of the participants reported that this was due to written or online communication lacking the same ‘“disciplining” effect that one might have by meeting up at the doctor's office’, 30 (p6) so not having as great an impact. 31 This lack of discipline was echoed by one health coach in a Swedish study, who reflected that they only used the digital health coaching platform when they were seeing a patient face-to-face, rather than following up on patient data remotely, which was the intended use. 33 A minority fed back that the improvements that they had made reverted to their previous behaviour after support from the coach finished, 34 with some also reflecting how they had become too disciplined in their approach and were being too extreme with their healthy eating and monitoring. 34
Burden of health condition and intervention
Many found that the use of technology and easy access to the health coach reduced the burden of their LTC; some stating that the technology being easy to use was a huge factor in this,26,33 and that it aided their focus on their health, 34 others reported that it was a lower burden as they felt more able to ask their coach for support. 32 In a Swedish study, several health coaches echoed that they saw the use of digital self-monitoring platforms as something that decreased the burden of long-term condition management for patients. 33 Digital health coaching, and self-monitoring, could therefore be hugely beneficial for patients to reduce the burden of managing their conditions. A participant in a US study on f-ILDs emphasised the burden of managing their LTC, 28 highlighting how impactful successful digital health coaching could be.
However, a minority of participants in two studies communicated that the use of technology increased the burden on themselves, as it required too much time and effort to operate.25,30 This was echoed by a minority of health coaches in a Swedish study, who suggested that they, and their patients, were not in the right generation to use digital health coaching.
33
Some in a Norwegian study focusing on patients with T2DM also emphasised the time burden of the health coaching, which caused them to drop out of the intervention. For example, one of the participants commented: It became a bit too much on top of everything else, having to sit down and spend time there, and remember to send and, yeah… There was too much else that had to be paramount somehow. Therefore, I simply had to downgrade it.
30
Embedding change (reassurance and empowerment of access to health coach)
This theme focuses on how behaviour change can be reinforced and maintained by participants, through ‘Reassurance and empowerment of access to health coach’ which highlights how participants use their health coach to support and affirm their behaviour change, and the importance of having feedback. This aligns with the NPT concept of ‘Reflexive monitoring’, as it exemplifies how participants use access to a health coach as a way of reflecting on their behaviour.
Reassurance and empowerment of access to health coach
Many participants in two studies emphasised the importance of the health coach as a source of accountability for their health25,26 ensuring that they were committed to their goals. Furthermore, a minority reported their goals as having ‘someone to talk to’, 25 which was echoed throughout other comments on the value of feeling cared for and having a form of emotional support.26,27,34
Patients with T2DM in two Norwegian studies were appreciative of the extra follow-up and communication they received, when compared with traditional healthcare.31,32 Moreover, there was also reflection by some people with spinal cord injuries on the value of having the health coach as someone to relate to.
25
A minority in the study focused on spinal cord injuries expressed that, due to this increased contact, their coach knowing them better enabled them to provide better advice, and the participant could therefore trust them more: It's not just the diagnosis and the test results. There are thoughts and feelings, and more. I felt the better we know each other, the easier it is to see ‘where the shoe pinches’, if it pinches.
32
Several health coaches taking part in a Norwegian study on digital health coaching for T2DM reflected that consistent communication and a lack of face-to-face contact, enabled participants to open up more, and gain trust in the coach. 32 This is indicative of the potential of digital health coaching for those patients who find traditional face-to-face settings inaccessible, as it could facilitate more consistent healthcare appointments.
The majority of participants in three studies commented how digital could not completely replace person-to-person contact, with several finding the coach as an essential source of support for technical issues or questions about the intervention itself,25,31 and acknowledging that this support is not as easy to get online. 32 A number of participants reflected that they missed that face-to-face contact, 30 and needed a form of external support. 34 Some health coaches in the Norwegian study echoed this, stating that an initial face-to-face contact was essential in establishing a relationship with their patients, and finding the lack of non-verbal communication you would have in a face-to-face appointment difficult to contend with. 32 However, some participants in a Swedish study focused more on the importance of feedback and monitoring; this could be done digitally, but knowing that their results and responses were being looked at by their coach, rather than ‘sending [data] into a black hole’. 33
Discussion
In this study, 10 qualitative and mixed methods studies were identified, with five main themes synthesised relevant to the perspectives and experiences of digital health coaching among adults with LTCs, health coaches, and health care professionals. To the best of the authors’ knowledge, this is the first systematic review and narrative synthesis to focus on stakeholder views of digital health coaching for LTCs.
There was variation between participants’ and health coaches’/health care professionals’ perspectives and experiences of digital health coaching for LTCs. No studies included carers perspectives which appears to be a significant limitation within the current evidence base. Our first synthesised theme, Reflection emphasised the importance and value of reflecting on both health and digital health coaching to facilitate a successful digital intervention. This theme overarched all other synthesised themes, emphasising the importance of reflection within all concepts of NPT. Views and experiences of reflection were largely similar between stakeholders, with all emphasising that reflection led to better care, and reflecting on the value of consistency in digital health coaching. In addition, participants frequently reflected on their feelings towards and treatment of their health and LTCs.
Second, the theme of Perception and prioritisation of health condition was highlighted by both participants and health coaches as a significant contributor to digital health coaching. For participants, their identification with their health condition was related to whether they completed digital health coaching, and how their behaviour changed as a result of it. For both stakeholders, knowledge and education was essential to the success of the intervention. For participants, this was knowledge about the implications of their LTC and the potential benefits from digital health coaching, whereas for health coaches this was education around the patients’ experience and digital technology.
Our third theme, Social and physical environment, inferred the impact of frustration for both participants and health coaches. Frustration with the mode of communication or the digital health coaching was experienced by both stakeholders, and often led to participants disengaging or dropping out of digital health coaching. In addition, participants’ perceptions of the intervention delivery were impactful upon their experience of digital health coaching.
Sustained change found there were similarities between participants and health coaches’ fidelity to the digital health coaching intervention related to their stage of behaviour change, and levels of intrinsic and extrinsic motivation and discipline. For participants, it was important that the use of digital technology reduced the burden of caring for long term condition and did not add unnecessary burden due to the technology being too complicated or unresponsive.
Finally, Embedding change illuminated the shared importance for both stakeholders of the relationship between a service user and their health coach. Whereas health coaches focused on the importance of consistency the contact with the patient for this, participants valued feedback more highly. Both stakeholders recommended that an initial face-to-face session could be essential for building rapport, and the participants emphasised that the importance of having a health coach was building trust and having a source of accountability.
How findings relate to existing literature
Our findings highlight the differing considerations needed to embed a digital health coaching approach for long term conditions that is acceptable to both participants and health care providers. Existing literature emphasises the importance of motivation 39 and support 40 to ensure successful behaviour change in participants. Similarly, our review found that participants acknowledged the significant value that their own motivation had, in order to engage effectively with their health coach. This was also related to the stage of behaviour change which participants were at, in line with our synthesis, current literature suggests that coaching can enable participants to move from a stage of ‘contemplation’ or ‘preparation’ to ‘action’.40,41 This may be due to the increased support, providing more confidence in changing their behaviours.
However, there was also acknowledgement of the failures of digital health coaching, elucidating where further support may need to be targeted. As our synthesis highlighted the need for good digital support, an existing study on an unsuccessful randomised trial has suggested that technical support, independent of the health coaching was essential. 42 Furthermore, a study on digital health coaching for cancer survivors found that some participants will struggle to adapt to a less directive approach to health advice, 43 in line with our synthesis. Existing literature has also shown that providers may not have the resources to support the embedding of new digital health interventions, 40 which was echoed by health care providers in our synthesis. In terms of NPT, this relates to the components of ‘cognitive participation’ and ‘collective action’ as it illustrates how change to routine care practices cannot be successfully enacted without having the social and system-wide structures in place to support changes of behaviour.
Strengths and limitations of the synthesis
Our systematic review and narrative synthesis employed rigorous methods to search and synthesise data from qualitative and mixed methods studies. However, we acknowledge that we may not have included some relevant literature due to only including studies published in English, and not searching grey literature.
A potential methodological limitation of this review was that we used a single screening approach. We acknowledge that some papers may have been missed by using this methodology. However, because of the nature of DHI research and the need for review, we felt that we needed to take a pragmatic approach via single screening. This approach has been shown to be an appropriate methodological shortcut for rapid research. 44 We mitigated for the risks associated with single screening by ensuring that the individual was supported by additional experienced researchers throughout the search process.
All of the studies included in this synthesis had medium- to high-quality ratings. The results of this synthesis remain the same when the lowest scoring paper is removed, suggesting that the synthesised evidence is robust. The initial coding was completed by one author (RAC) suggesting consistency across the studies, and themes developed with the wider team (MAP and MS) to reduce bias. This involved group discussion on the initial coding, and reaching a consensus on these, before agreeing on themes. This suggests strong interrater validity of the results.
RAC did not disclose any prior assumptions or reasons for doing the review and synthesis. Analyses were completed by RAC, MS, and MAP with iterative discussions with MB and ES. RAC is a psychologist and research assistant, MS is a physiotherapist and researcher with experience in systematic reviews, and MAP is an occupational therapist and researcher. ES is a social scientist and physiotherapist specialising in social science applied health and implementation research, and MB is a nurse and qualitative researcher specialising in creative approaches to collect and present research data. As such, we feel our interdisciplinary research team increased the quality of this study because it brought together multiple perspectives to better understand how patients can experience digital health coaching and what this can be impacted by.
There may have been a significant impact on some of the included studies due to the COVID-19 pandemic, where digital innovations in healthcare were rapidly adopted due to not being able to see patients. Although some of the studies were published between 2019 and 2023, none provided a timeline which covered the pandemic, or acknowledged it having taken place. Therefore, this context is not included in our analysis.
We used NPT to help us understand factors promoting and inhibiting the implementation of digital health technologies into healthcare systems from the perspectives of service users and professionals. The strength of NPT was that it enabled a better understanding of the implementation process within a social and organisational context. However, we acknowledge that the process of implementing digital health technologies in practice is complex and using a combination of different theories could provide a more comprehensive understanding of implementation processes. 45 NPT did not centrally focus on how digital health interventions were perceived to work for whom, under what circumstances, how and why and so combining NPT with realist approaches could usefully address this complexity. 46
This synthesis has highlighted the small body of qualitative studies evaluating digital health coaching for people with LTCs, particularly for social care providers and carers, whose views were not included as in our protocol. It was apparent the lack of studies which included a carers’ perspective of digital health coaching and represents a significant gap in the research literature. Individuals with LTCs are often dependent on caregivers, including informal carers and family members for support in accessing digital support, however there is some evidence to indicate that carers of people with LTCs have reservations about digital health interventions due to unfamiliarity with IT and preferences for face-to-face interactions. 47 This highlights an important consideration when evaluating the success of digital health interventions and provides a potential area for further research to be directed.
Conclusions and implications for policy, practice, and research
The evidence highlighted by this systematic review and narrative synthesis has demonstrated the limited evidence currently available about the experiences and perceptions of home-based digital health coaching from different stakeholders. All of the current evidence is from North America or Scandinavia, so further research from wider countries including UK and diverse populations is needed to highlight differing experiences of digital health coaching. Further research should also focus on more LTCs, as the current body of research is limited to T2DM, COPD, SCI, F-ILDs, heart disease, and hypertension, therefore it may not be generalisable to all conditions.
This synthesis has emphasised the importance of personalised support and regular feedback, alongside consistency of care, which can provide the space for reflection. This is more likely to engage participants in digital health coaching, allowing them to internalise behaviour change and providing them more likelihood of maintaining these changes. Furthermore, ensuring that participants and health coaches understand their LTC, digital software, and the purpose of digital health coaching is vital for facilitating engagement and success with the intervention. These factors should be considered and embedded within any further research, and by healthcare providers offering digital health coaching for LTCs.
Footnotes
Contributorship
All authors contributed to the analysis, and review and editing of the article. In addition, the following contributions are noted; RAC contributed to the conceptualisation, investigation, methodology, and writing the original draft. ES contributed to the conceptualisation and methodology. MIS and KL contributed to the conceptualisation and writing of the original draft. CC, MB and MAP contributed to the conceptualisation of the article. JM contributed to the conceptualisation and funding acquisition of the project.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and publication of this article: This work was supported by the NIHR ARC Wessex (grant number ARC 001).