
Abstract
Objectives
To develop, feasibility test, and evaluate an AI-enabled multimodal monitoring system to integrate safety outcomes, functional recovery and quality of life in elderly and stroke survivors in multiple care settings.
Methods
This was a 24-month mixed-methods study across 12 sites spanned from private homes, assisted living facilities, rehabilitation centers, to acute care transitions. The study was a quasi-experimental design, with three groups: integrated monitoring (n = 112), basic monitoring (n = 89), and usual care control (n = 86). 313 respondents were purposively selected using stratified purposive sampling. The multi modal system combines wearable sensors, ambient environmental control sensors, computer vision algorithms and voice analysis by adaptive fusion architectures. Key outcomes were safety events (falls, hospitalisations), functional independence, and cost-effectiveness. Semi-structured interviews were conducted with a total of 78 care-recipients, 93 caregivers, and 76 healthcare providers, until we reached thematic saturation.
Results
The integrated monitoring system achieved fall detection sensitivity of 94.8% (95% CI: 92.6–96.3%) and specificity of 96.2% (95% CI: 94.8–97.4%). Clinical outcomes showed significant improvements compared to usual care: 42% reduction in fall-related injuries (p < 0.001), 37% decrease in emergency department visits (p < 0.001), and 22% greater improvement in functional independence scores at 6 months (p < 0.001). Cost-effectiveness analysis revealed net savings of $15,311 per participant over 24 months. Qualitative analysis identified an enhanced sense of security (92% of participants), improved care coordination, reduced caregiver burden (33.3% reduction), and implementation challenges related to technology integration.
Conclusion
The AI-enabled multimodal monitoring system demonstrates significant clinical, economic, and quality-of-life benefits for elderly individuals and stroke survivors. The integrated approach outperforms single-modality systems and usual care across multiple outcome domains. Implementation success depends on leadership engagement, technical infrastructure readiness, comprehensive staff training, and ongoing user involvement in system configuration.
Keywords
Introduction
The WHO (World Health Organization) has estimated that people of age of 60 years and older will nearly double, from 12% to 22% between 2015 and 2050, an unprecedented increase. 1 The world-wide health systems face enormous challenge to cope with chronic, functional, and caregiver incapacity issues, particularly in vulnerable older people, and stroke sufferers and so on. According to a recent report on stroke published in the Lancet, the condition remains a leading cause of disability on the global level. Specifically, stroke is responsible for about 1 in 8 deaths. Furthermore, it affects about 80 million people at the present moment. Studies indicate there are about 13.7 million new cases of stroke each year. 2 The care paradigm for these vulnerable populations has traditionally relied on resource-intensive approaches in care paradigm for these vulnerable population including institutional care facilities, frequent clinical assessments and direct supervision by healthcare professionals or caregivers. Still, traditional methods are more and more being under pressure with workforce shortages, rising costs of care, and increasing want by individuals to age in place and remain independent. 3
The flaws of traditional care models – which prevent timely monitoring and detection of adverse events (including early interventions and rehabilitation) while also wasting resources and violating autonomy – are increasingly apparent. 4 Recent advancements in AI, sensor technologies, Internet of Things (IoT), and telecommunications have created opportunities for innovative changes in delivery models in healthcare. Research demonstrates that AI-based monitoring systems may have a substantial potential in offering solutions to the complex care requirements of older and post-stroke individuals. 5 Technologies include wearable monitoring device to monitor physiological function, ambient sensing to recognize activity, computer vision for analyzing movement, natural language processing to assess communication, and machine learning for predictive analytics and tailored care planning. 6 AI-based monitoring systems have the potential to improve the care context, but what challenges will they encounter? What are the ethical concerns? What will they change? As these technologies rapidly advance, it is now essential to comprehend their status, limitations, and future to implement evidence-based implementation and to derive maximum benefit to vulnerable groups. 7
The literature shows much advancement in using AI for stroke diagnosis and management of acute care. A comprehensive literature review 8 examined the literature published in the last ten years on the application of AI in stroke care. This review highlighted the progress in neuroimaging analysis for the early detection of strokes and classification of stroke subtypes. These researchers showed that a deep learning algorithm can enhance speed and accuracy in diagnosing large vessel occlusions, potentially speeding up the critical time-to-treatment. Likewise, machine learning approaches have been systematically reviewed for brain stroke specifically. 9 In recent research, predictive models for clinical outcomes (hand function, walking ability and mortality) are developed for first-ever ischemic stroke with very good performances achieved to predict trajectories of functional recovery and mortality risk. 10 The ability of convolutional neural networks to detect large vessel occlusion from CT angiography was demonstrated by research findings. 11 Deep learning methods have also been developed to automatically detect and segment diffusion abnormalities caused by acute ischemic stroke using diffusion-weighted imaging to allow clinicians better detection of affected brain regions. 12 In recent years, a considerable number of research papers have discussed the use of AI in objective assessment and continuous monitoring during rehabilitation. Research utilizing unsupervised machine learning produced longitudinal profiles of stroke survivor impairment which revealed subtle patterns of recovery that are missed through clinical assessments. 13 In a 2024 study, researchers created and assessed robotic coaches for the purpose of physical rehabilitation therapy. 14 They described how AI-powered devices may be employed to help someone with a disability or illness. A comprehensive review 15 examined the application of wearable sensors and machine learning for post-stroke rehabilitation assessment. The authors suggest that wearable sensors may allow continuous and objective measurement of the quality of movements and functional improvement. Research has introduced an intelligent motor assessment method for upper extremity rehabilitation with virtual reality tasks, allowing for precise quantitative analysis of movement parameters without continuous monitoring by a clinician. 16 Evidence from studies shows the sensor-based monitoring will be useful in rehabilitation progress. A new method for quantitative functional assessment of lower limbs was developed by fusing surface EMG and inertial data recorded during cycling tasks. 17 It was found to be more sensitive than clinical scales for subtle improvements. Research demonstrated that a single wrist-worn sensor using machine learning could accurately measure functional arm movement after stroke. 18 This could help in continuous monitoring at home. In their 2022 research, investigators tested an innovative video-based pose estimation system designed to analyze the gait of stroke survivors. 19 The system offers a non-invasive way to quantify gait and movement patterns and holds potential applications in clinical settings.
By providing objective, continuous, and granular measurements of functional recovery, these technological approaches help overcome the limitations of clinical scales. The application of artificial intelligence for language and cognitive disabilities can be defined as a separate domain. Research examined the potential of machine learning algorithms in predicting language and cognition rehabilitation outcomes. 20 After unveiling various algorithms, they revealed how these can be incorporated in the planning of rehabilitation. A systematic review 21 examined the use of AI in aphasia rehabilitation and provides applications such as automated speech analysis, personalized therapy delivery, and outcome prediction. Research analyzed the utilization of AI for diagnosing and treating aphasia. 22 They opined that the use of AI can aid in precise characterization of communication impairments and development of tailored interventions. In this area, researchers created a system for automated assessment of aphasic speech using audio sensors in order to classify the level of severity and recommend the right speech therapies. 23 A deep-learning model was designed leveraging DWI (diffusion weighted imaging) to estimate the severity of aphasia post-stroke for better early and accurate treatment planning. 24 Predictive models of cognitive improvements of young adults undergoing stroke rehabilitation therapy were developed. 25 Moreover, they found the factors causing cognitive improvement in this population. A new study on multimodal methods gives insights for complete monitoring. A Hybrid Control Framework Based on Motor Imagery and Object Detection to Manage a Wearable Supernumerary Robotic Limb System was first presented. 26 A hybrid deep learning approach for modeling spatio-temporal features in rehabilitation post-stroke was proposed. 27 Research put forth a model for quantitatively evaluating upper-limb motor function by analyzing motor synergy, integrating multiple modalities, and displaying superior sensitivity to slight variations in movement quality. 28 More intelligent and unobtrusive monitoring is enabled through advanced sensing technologies. Researchers created a vision-based soft pressure sensing system for hand rehabilitation at home, which enables tactile feedback on the hand without restricting movement. 29 To verify the validity of facial expression recognition using a patch-convolutional vision transformer for stroke patients, a model was developed to assess emotional states that may influence patients’ engagement and outcome in rehabilitation therapy. 30 A method of monitoring rehabilitation outcomes via wearable devices was introduced. 31 This study offered preliminary proof of the potential for continuous remote monitoring in stroke survivors. A combination of AI with immersive technologies is the new frontier for rehabilitation. Researchers developed a virtual reality-based system for wide-ranging human posture and movement analysis during an exercise that aims for human rehabilitation. 32 The authors of this system asserted that it enables analysis and aggregation of detailed human movement using modelling and center of mass teleportation with feedback. Research showed that adaptive conjunctive cognitive training in virtual reality can improve cognitive function in chronic stroke patients. 33 Research studied the use of stimulation-based immersive virtual reality for stroke survivors. 34 Results of the study ranged from improvements in attention, memory, and executive function.
Artificial intelligence and machine learning applications in virtual environments for rehabilitation have received attention from researchers. Decision tree modeling to prediction of patient performance in virtual rehabilitation programs with capacity requiring adjustment difficulty and process at patient's individual level. Researchers designed a multi-label/multimodal classifier to recognize patients’ affective states in virtual rehabilitation. 35 The devised system can assist in automatically responding to patients’ engagement and affective states. These methods demonstrate how AI can improve the responsiveness and personalization of virtual rehabilitation environments. The forecast modelling of rehabilitation outcomes represents a relevant research domain with immediate clinical applications. Research explored the machine learning technology application for the prediction of post-stroke rehabilitation functional recovery. 36 Further, this was done for the systematic review. The study focuses on prognostication and has a personalized goal. Research explained how explainable AI can be used to predict outcomes of upper limb rehabilitation in sub-acute stroke patients, which helps to provide interpretable information. 37 A review and seasonal meta-analysis 38 examined AI machine learning versus conventional physical therapy for upper limb outcomes in stroke patients; observed better predictive accuracy of AI-based approaches.
Separate predictive models focus on distinct rehabilitation outcome features. Machine learning models were developed for the prediction of activities of daily living (ADL) patient-reported outcomes in stroke rehabilitation. 39 This includes the subjective point of view on improvements in functional status. Using machine learning analysis, research conducted a study predicting the need for ankle foot orthosis in stroke patients to optimize prescription of assistive device. 40 A machine learning-based analysis of hospital length of stay and 30-day mortality prediction in stroke patients was performed so that care resources can be allocated effectively. 41 The models show how AI can help clinicians with data-driven predictions of how a patient might recover. AI-powered Robo Rehab and Brain-computer interfaces to help rehabilitation technology's most advanced frontier. Researchers have presented a model-free deep reinforcement learning solution to improve a definite 16 DOF exoskeleton's gait pattern. 42 They incorporate adaptive support to assist users during an over-ground walking rehabilitation activity. In order to improve comfort and adherence to robotic therapy, an optimized stimulation control system for upper limb exoskeleton robot-assisted rehabilitation based on fuzzy logic pain detection was proposed. 43 These developments are a testimony to how AI can boost the adaptability of rehabilitation robots.
Brain–computer interfaces are another promising direction for severe motor impairments. Research demonstrated that BCI-based rehabilitation for stroke patients in the sequela stage is possible. 44 Neural signals can be used to conduct rehabilitation exercises even in severely impaired cases. A meta-analysis of brain-computer interfaces for post-stroke motor rehabilitation was undertaken. 45 The authors reveal the evidence of efficacy under a number of different investigations. These methods offer potential new ways to help people in cases where traditional methods may not work on those who have serious motor impairments. Inquiry about implementation challenges and patient experiences using AI based systems can provide valuable insights for real-world application. Research reviewed artificial intelligence-based technologies in health and assesses the barriers and facilitators of technology implementation. 5 In a recent study, researchers conducted a qualitative descriptive study of patient experiences with a digital therapy system for stroke recovery, revealing factors associated with engagement and perceived benefit. 46 Research designed a serious game based on deep reinforcement learning, a new system of care that will be of great help to post-stroke patients. 47 In nursing, it is often forgotten that caregivers must be trained as well. Technology is not enough. After analyzing various studies, they suggest that technology alone won't do the trick. Moreover, you must pay attention to the user's perspective. Further, it must fit into the established pathway that helps in delivering care. Lastly, you must keep a note of the needs of patients and caretakers. The human factors in technology adoption are essential for turning promising research into effective clinical applications.
The literature has shown great progress in the field, but a few gaps remain in the AI-based monitoring system for older adults and stroke survivors. These gaps can be categorized into four main areas. To begin with, there is a significant fragmentation in research with most studies addressing specific applications, modalities or use cases without consideration for integration requirements for whole-person care. While individual technologies show promise in controlled settings, there is limited research on other integrated systems. These cover the whole span of the care continuum. They include technologies for prevention, rehabilitation, and long-term management. Finally, they address the different needs of older adults and stroke survivors with different severity of impairments. 7 The literature shows that there are many specialized applications but very few frameworks for holistic monitoring and support. Again, not enough evidence exists about the long-term effectiveness, sustainability, and real-world implementation of AI monitoring systems. The majority of studies show proof-of-concept findings or prototypes or include evaluations or short-term clinical trials. Evidence of sustained effects, obstacles to implementation in different care environments, or integration with existing healthcare systems is limited. 15 This gap is a worrying aspect, especially since a lot of resources will be required to implement technology that uses evidence for decision-making. Third, it is found that the literature gives less importance to the ethical, privacy, and user-centred design of the technologies. Although technical capabilities are advancing rapidly, user acceptance, privacy preferences, autonomy preservation, and ethical framework research are not keeping up. 48 This lack of balance jeopardizes the acceptability and adoption of such technologies, especially among vulnerable populations, who have uneven attitudes toward technological oversight and data gathering. Additionally, there is a considerable knowledge gap about the comparative effectiveness of an AI-based monitoring system with respect to conventional care, cost effectiveness, and impact on care burden and quality of life of care recipients and caregivers. Healthcare systems cannot make informed decisions about taking up these technologies and their scaling up technologies. 49 There is a gap between research and clinical practice which can be caused as below.
A unique, comprehensive interdisciplinary approach is adopted by this study to investigate AI-based monitoring systems for the elderly and stroke survivors. Our method includes five different innovations that together upgrade the whole field, beyond the state of the art. To begin with, we propose and validate a comprehensive monitoring framework that integrates different sensory modalities (wearable sensors, ambient environmental monitoring, computer vision, and voice analysis) into a seamless system capable of continuous multiparametric assessment in the physical, cognitive and psychosocial domains. Our framework differs from previous approaches, which have been fragmented, as it allows for comprehensive monitoring that is adaptable to various care settings and levels of impairment, enabling personalized care planning and intervention. Our system is more sensitive and specific in identifying clinically significant events and changes when using complementary data streams rather than a single data stream.
Second, we present longitudinal evidence from a multi-site implementation study across a variety of care settings (home environments, assisted living facilities, rehabilitation centers, and acute care transitions) to demonstrate the long-term efficacy as well as the implementation challenges and sustainability of AI-based monitoring systems. The implementation of our study is for a duration of 24 months. This duration facilitates the investigation of the following three things: technology adoption trajectories; patterns of adaptation; sustained benefits beyond initial implementation. Each of these constitutes a critical gap in existing evidence. And this gap has impeded clinical translation and policy development.
Our third contribution is an ethical framework for AI-based monitoring that balances safety needs and the preservation of the autonomy of individuals, caregivers, and healthcare providers. Furthermore, the solution incorporates adjustable privacy settings, sensitivity of monitoring to evolving preferences, and ethical guidelines. These guidelines are developed based on extensive engagements with older adults, stroke survivors, caregivers, health care providers, and ethicists. This framework goes beyond technical capabilities to include essential human aspects like acceptability, trust, and ethical implementation for monitoring with the vulnerable. A framework suggests the right way to deploy the monitoring technology.
Fourth, we’ll conduct a comprehensive comparative effectiveness analysis that examines outcomes, resource utilization, and cost-effectiveness associated with conventional care, basic tech-enabled care, and our own AI-based monitoring system. This evidence could help health systems and policy-makers decide whether to adopt and scale-up these technologies. They may use this evidence to implement these based on the context and the populations health systems serve.
Additionally, we will also develop new algorithms for early detection of deterioration and precise quantification of functional recovery based on the temporal pattern of multimodal data streams. As such, these algorithms represent a significant advancement in the predictive analytics of vulnerable populations that ought to allow for earlier interventions for adverse events. Moreover, they can encourage more personalized rehabilitation strategies that are responsive to objectively measured functional trajectories rather than periodic clinical assessments.
This research contributes significantly toward better use of AI-based monitoring systems for the elderly and stroke survivors.
We present a unified and novel monitoring framework that allows the integration of multiple sensors (e.g., physiological, physical) and analytical methods (e.g., machine learning, statistical analysis) for continuous monitoring of the physical, cognitive and psychosocial behavioral aspects of the users. A 20-word paraphrase of the above sentence is:
The complicated technologies are cost-effective and accessible, having the capacity to adapt to changing environments and accommodate patient care needs.
We present the first large-scale, multi-site longitudinal evidence showing the implementation, adoption, and sustained benefits of AI-based monitoring systems across the continuum of care. Evidence showing this at the large-scale has been lacking which has hampered clinical translation and related policy development. We found facilitators and barriers to implementation in various care contexts, which can aid future deployment. We put forward an ethical framework that takes diversity of perspectives into account to guide the responsible implementation and deployment of algorithmic monitoring technologies with vulnerable population groups. This model sets new benchmarks for balancing safety benefits with technology-enhanced autonomy in care. We provide comprehensive data on the comparative effectiveness, resource implications, and cost-benefit profile of AI-based monitoring against conventional and basic technology-enhanced care approaches. The evidence helps in evidence-based decision-making in a healthcare system for adopting these technologies. We create new algorithms for predicting when patients will get worse. Moreover, new ways to measure how patients are going to get better by recognizing patterns in data over time. These algorithms provide much better sensitivity, specificity and lead time for adverse event prediction as compared to existing methods, enabling timely interventions and personalized care planning. We provide a complete implementation toolkit with technical specifications, integration guides, training materials, and adaptation manuals for different care settings, so that research can be used effectively in the real world.
The rest of paper is organized in the following way: Section 2 outlines the methodology including system design principles and technical architecture, data collection approach, analysis methods, and ethical considerations. This section outlines the overall integrated monitoring framework, describing the sensing modalities, data integration approach, analytical algorithms and user interfaces. Our multi-site implementation study's results are presented in Section 4, these findings include quantitative outcomes, qualitative user experiences, and implementation facilitators and barriers across care settings. In section 5, we will discuss how effective the different models of care were at improving patient outcomes. In Section 6, the findings are discussed in light of existing literature and the implications for clinical practice, technology and policy. Section 7 wraps up with an overview of principal contributions, limitations, and future research directions. Our findings can be replicated and extended thanks to the detailed technical specifications, implementation protocols, and supplementary analyses.
Methodology
Our method combines techniques from computer science, biomedical engineering, clinical medicine, and human-centered design to address the challenges of monitoring elderly people and stroke patients. Using a mixed-method design, we evaluate both the technical performance and human factors of AI-based monitoring systems in a rigorous research study.
The study protocol was approved by the Institutional Review Board at each participating institution (Ethics approval numbers: IRB-2023–045, IRB-2023–067, IRB-2023–089). Written informed consent was obtained from all participants or their legally authorized representatives prior to enrollment. The study was conducted in accordance with the Declaration of Helsinki and followed STROBE guidelines for observational studies. Our research is conducted in accordance with the Helsinki Declaration and the STROBE observational study guidelines. The trial took place in many locations, including acute care facilities, rehabilitation centers, assisted living facilities, and in the home, which allowed an assessment of the performance of the system and associated difficulty in implementation across care.
Study population and recruitment
For a diverse demographic, impairment and care-related characteristics, a stratified purposive sampling method was used at different sites to procure the sample. Eligibility requirements for elderly subjects aged 65 years and older were as follows: independent living, assisted living, or cohabitating with family caregivers. Also included in the criteria was being able to give consent or having a proxy available. To be eligible, stroke survivors had to have been diagnosed with ischemic or hemorrhagic stroke within the last 24 months (1) have had different recovery times and levels of disability as rated on the modified Rankin Scale (mRS scores 1–4).
Individuals meeting the following exclusion criteria will not be eligible to participate in the study: (1) poor cognitive state preventing them from meaningfully participating in the qualitative work of the study. (2) Unstable medical illness requiring frequent hospital admissions. (3) Participation in trials of other intervention studies. (4) technical incapacity of the residence to permit installation of the system. A total of 287 people (167 old people with no stroke 120 stroke survivors) were recruited from a total of 12 sites with varied geography and socioeconomic status.
To capture diverse stakeholder views robustly, we engaged 76 healthcare providers (physicians, nurses, therapists, care coordinators), 93 informal caregivers, and 28 healthcare administrators, who were included in qualitative assessments of implementation factors and system utility. By bringing together various stakeholders, a system's performances as well as usability and the implementation considerations could be triangulated.
Data saturation was achieved when no new themes emerged from three consecutive interviews within each stakeholder group, occurring after interview numbers 65, 82, and 68 for care recipients, caregivers, and healthcare providers respectively. Additional interviews were conducted to ensure theme stability and comprehensive understanding of implementation factors across all care settings.
System design and development
The integrated monitoring system was developed through four phases which are requirements elicitation, architecture design, component development, and system integration. Every phase got inputs from multi-disciplinary professionals and end-users to make sure that it is technically robust and user-friendly as well.
To find out how to monitor physical or psychosocial or cognitive, we did needs assessment. The methodology of the study involves a combination of (1) in-depth interviews with 42 older persons and stroke survivors, 35 caregivers and 48 healthcare professionals and staff; (2) systematic analysis of existing clinical guidelines for stroke rehabilitation as well as geriatric care; (3) review of incident reports from participating care facilities to identify high-priority monitoring needs (that could serve as entry points); (4) observational studies of care workflow in a range of settings.
The requirements were documented systematically and prioritized with the MoSCoW (Must-have; Should-have; Could-have; Won’t-have) method following clinical utility and user acceptance factors. Essential monitoring including fall detection, medication adherence, physical activity, sleep, vital signs, function, cognition, communication, social and emotional interaction devices would be very useful. Furthermore, system requirements were categorized by technical feasibility, privacy sensitivity, and complexity of implementation to aid development decisions.
Based on requirements we created modular scalable system architecture using layered approach which separates the data acquisition, processing, analysis, and presentation functionalities. The architecture consists of five main layers comprised of the Sensing layer, edge computing layer, communication layer, cloud computing layer and application layer (Figure 1). Thanks to the modular nature of the producers’ design, it will be feasible to apply certain components selectively regardless of the overall care context. Also, we should maintain room for evolution as component technologies are improved and new ones are created.

Proposed architecture of integrated AI-based surveillance system.
The sensing layer comprises multiple modalities, including (1) wearable sensors for monitoring physiologic and movement data, (2) ambient environmental sensors for activity recognition and context, (3) vision-based systems for detailed movement analysis and fall detection, and (4) audio-based systems for communication and voice analysis. By using multiple methods, it helps in strengthening the monitoring of the product as well as overcoming the failures that a single method can cause.
The edge computing layer does some processing of data at the device itself. This lessens the amount of bandwidth needed for sending data around. The data stays private because it is filtered at the device itself. And if connectivity fails, then the critical function will go on to run anyway. Edge processing may involve signal preprocessing, feature extraction, anomaly detection, and data compression, with processing allocation made dynamically, based on available computing resources and connectivity status.
The communication layer uses both bluetooth low energy, Zigbee for short-range communication and Wi-Fi, cellular for long-range communication which communicates between you and your system. Communication is handled with dynamic scheduling and prioritization to optimize bandwidth usage, emit high-priority alerts on time, and manage power consumption.
The cloud computing layer runs analytic processes that need a lot of computing capacity, such as running machine learning models, tracking long-term trends, and building population-wide insights. With access control mechanisms, end-to-end encryption, and audit logging to protect health information, this layer has robust security.
The application layer provides different interfaces for: (1) care recipients for whom the technology is easy to use and degraded dashboard notifies them on useful autonomy and engagement; (2) informal caregivers who can change alerts and visually see trends; (3) health-care providers whose clinical insights are put into support decision flows; and (4) administrators for whom the system shows diagnostics and resources utilization.
The choice of sensing modalities was optimized for the monitoring domain using sensitivity, specificity, user acceptance and implementation in the activities of daily living (ADL) settings. Using a bare minimum approach to enhance compliance, we have developed a wrist-worn sensing device containing tri-axial accelerometry, photoplethysmography, skin temperature, electrodermal activity, and barometric pressure sensors. This multiple parameter approach will allow us to simultaneously monitor activity patterns, heart rate, heart rate variability, peripheral perfusion, autonomic function and relative elevation changes with a minimal user burden.
To avoid invasion of privacy ambient sensing uses a distributed network of unobtrusive sensors sited at various key functional areas. The proposed home situation awareness system may contemplate the expansion of home sensor network incorporating sensors like: (1) passive infrared motion sensors to detect activity at room level; (2) contact sensors on doors, cabinets, appliances to monitor activities of daily living; (3) pressure mats to assess bed occupancy and chair transfer; (4) environmental sensors to monitor temperature, humidity, luminance, and noise level; and (5) smart utility meters to assess appliance usage pattern. By using multisensory setup, the activities are monitored without making one aware. It is done without keeping a constant watch. Thus, it sorts out privacy issues whereas providing extra data for better usage.
Vision-based monitoring used depth-sensing cameras placed in risky areas like floor and stair therapy spaces. It was done without sacrificing privacy as all skeleton tracking data were processed, but no identifying data. Through this method, we can analyze movements in detail and detect falls without recording or sending any images. The vision system has a two-stage processing pipeline in which the device runs a first-stage skeleton extraction job, sending only aggregated jump joint position data out of the device for subsequent processing.
Voice activity detection, speech quality evaluation, and acoustic event recognition were conducted using a dispersed microphone array. This is done in a way that does not infringe on privacy. Whenever there is a chance detection happening in the system, the continuous audio buffer of speech gets processed on-device but is not stored. In addition, only certain features will be extracted from evaluation of the quality of communication. Acoustic event detection system for detecting calls for help, falls, glass breaking, and other similar noises processes the sound locally so that the minimum amount of data has to be transferred.
To achieve the above-mentioned goals, our system performs a careful distribution of processing tasks on edge devices and the cloud. Edge processing focuses on time-sensitive, privacy-sensitive and continuity-critical functions. Unprocessed information collected by sensors is filtered, artefacts are rejected and the extraction of data features occurs on edge devices to reduce transmission bandwidth and provide resilience when connectivity is lost. Events that require urgent attention (e.g., fall, presence of immobility, prolonged immobility, abnormal vital signs) are detected by edge-based algorithms to ensure latency is minimal. Sensitive data is reduced in dimensionality and features are extracted. The features are also anonymized before being transmitted. The raw data is not retained for long and is securely stored locally.
Local systems for instant feedback send alerts for taking medication, moving around and staying safe. These do not use cloud. Cloud processing aims on data-intensive analysis, repeated pattern detection and cross-patients’ insights. Cloud-based complex models integrate time and various modalities, caching results on edge devices for local execution when feasible. By looking at data collected over time, we can catch slight changes in the way someone acts or their thinking. This can help catch issues early. When individual data is combined and altered to protect the identity of the individual this ensures identification of normal patterns, abnormal patterns and outcome patterns and helps enhance prediction model. Information from models in use update continuously thanks to incremental learning approaches. The updated models get deployed in edge devices.
The system has a principled approach to processing distribution with functions assigned according to their latency requirements, privacy sensitivity, computational need and connectivity dependence. Based on available resources, network conditions, and observed usage patterns, this allocation is dynamically modified.
The value of a new approach we are adopting is the systematic fusion of multimodal data streams to significantly enhance monitoring robustness. Further, it aims to deal with limitations of single sensing modalities and to derive higher-level insights than possible from single-source analyses. Our approach to data fusion works on three levels. Signal-level fusion is the procedure of combining the raw or minimally-processed data from sensors, which complement each other, in order to enhance the quality of signals and reject artifacts. Accelerometry data is utilized to compensate for movement artifacts in photoplethysmography signals through adaptive filtering, enabling robust heart rate monitoring during daily activities. Combining features extracted from different sensors before a classification or regression operation is called feature-level fusion. By introducing this mechanism, we can exploit the correlations between the different feature sets while preserving the distinct contributions of each modality. Our activity recognition algorithms combine accelerometry features, room transitions from ambient sensors, and skeletal pose features when available, all of which are highly effective at classifying even complex activities. Merging of the independent analysis results from various modalities at a decision level may be carried out through means of weighted voting, Bayesian methods, hierarchical classifiers, and the like. Furthermore, this allows for the production of various integrated results as well as confidence measures. This technique helps the system to become stronger against sensor failure. Even if some sensors malfunction, the system will degrade gradually.
The context-aware weighting on the fusion architecture dynamically modulates the contribution of each modality depending on their reliability, environment, and user. As an example, under low-vision condition, where reliability of vision-based monitoring decreases, the weighting of inertial and ambient sensing data is automatically increased. Fusion logic adapts to use the modalities available more covertly for users with specific sensor compliance issues.
To synchronize different data sources over time, we combine hardware timestamps and NTP references with signal-based alignment for sources that don’t have clear timestamps. This method will solve the problem of using devices that have different sampling rates, communication latencies, and clock drift characteristics. To evaluate scalability, the system was stress-tested with up to 200 concurrent users across multiple care sites. Under this load, system performance metrics—including latency, uptime, and data integrity—remained within clinically acceptable thresholds. The testing environment included a distributed cloud-based infrastructure with edge processing units (Intel i7, 16 GB RAM, 512 GB SSD) and centralized servers (dual Intel Xeon processors, 128 GB RAM, 4 TB SSD storage) connected via secure high-speed networks. These specifications provide a benchmark for reproducibility and demonstrate that the system can be reliably scaled to multi-user, multi-site deployments without compromising performance.
Across all variables, the rate of missing data was consistently below 2%, reflecting high data completeness across sites. To address these cases, we applied multiple imputation using chained equations (MICE) with 20 imputations under the assumption of missing at random. This method allowed us to preserve sample size and reduce potential bias. Sensitivity analyses were conducted by comparing outcomes derived from imputed datasets with those from complete-case analyses, and the results remained stable across approaches. This comprehensive strategy ensures that findings are not materially influenced by missingness and strengthens the validity of the reported outcomes.
Analytical methods
Activity and functional monitoring
We use hybrid knowledge-driven and data-driven methods in our activity recognizer for robustness over different users and environments. To perform motion and posture classification for structured activities, like walking, sitting, and lying down, we adopt a hierarchical classification scheme that uses handcrafted features extracted from inertial signals, time-domain statistics, frequency components, postural orientation and shallow machine learning (random forests, support vector machine) for efficiency on edge devices.
To facilitate complex instrumental activities of daily living, we implement a fusion recognition approach with complementary data. The formula for our activity classification can be expressed mathematically:

Where:
A represents the classified activity from the set of n possible activities Xw denotes features from wearable sensors Xa denotes features from ambient sensors Xv denotes features from vision-based monitoring (when available) C represents contextual information (time of day, location, previous activity)
The conditional probability is computed using a weighted ensemble approach:

Where:
m is the number of classifiers in the ensemble wj are adaptive weights based on estimated reliability of each modality Pj represents the probability from individual classifiers Xj represents features from modality j
For functional assessment, quantitative metrics are gleaned from continuous monitoring data that target clinical assessment domains. The mobility metrics for stroke survivors include gait speed, daily step count, postural transitions (sit-to-stand), ambulatory bouts (frequency, duration), and symmetry. Metrics of upper extremity function include reach volume, movement smoothness, coordination between limbs, and task-specific movement patterns during daily activities. This metrics tracks daily activity and rest patterns, diversity of activity, and activity deviations from one's own baseline patterns. We will measure these metrics over time to look out for subtle changes in function that might not be easy to see at regular visits. Thus, we may allow early intervention for emerging functional decline.
Cognitive and communication monitoring
Cognitive monitoring utilizes indirect assessment that looks at instrumental activity patterns, digital interactions and voice features. Our aim is not to duplicate formal neuropsychological testing, but to pick up changes in the everyday tasks that may reflect cognitive changes. Essential metrics include efficiency in task completion for periodic activities (managing medicine, preparing food, caring for one's self) by outlier detection on unusual sequences or timing; complexity of speech samples taken from natural conversation during the study, extracting a number of metrics on speech complexity, vocabulary use, syntax, and semantics without storage of conversation; and digital interaction pattern, which provides for users of digital devices with an indicator of a person's interaction consistency, error rates, instability and times to completion, all of which are sensitive to cognitive change.
For stroke survivors with communication impairments, we use a speech analytics pipeline that quantifies how well they articulate through acoustic measurements of the accuracy and consistency of their phoneme productions; prosodic features such as rhythm, intonation, and stress patterns that may be impacted by neurological impairments; and their efficiency in conversation as measured by speech rate, pause characteristics, and turn-taking behaviours.
This means that these metrics are normalized for the individual baseline pattern and they are evaluated for trajectory rather than absolute values taking into account the high degree of inter-subject variability that characterizes cognitive and communication behavior.
Psychosocial monitoring
Given the importance of psychosocial wellbeing to health outcomes, we take privacy-preserving steps to track social connectivity, emotional and behavioral states that may reflect psychosocial changes. The frequency of social engagement is captured through the detection of conversations episodic social activities with ambient sound sensing and localization patterns. Mobility patterning is captured through community mobility and visitation patterns derived from localizing noise data using privacy-preserving aggregation. Communication technology usage: frequency and duration of phone calls, video chats, messaging (without content access) for participants who opt in to share these data.
Monitoring emotional wellbeing uses multi-modal indicators, including: Following voice affect using acoustic features linked to emotional states extracted passively during everyday voice interactions with the digital assistant (or through designated check-in prompts).
Following activity pattern changes through deviations from typical rhythms which can indicate changes in motivation or mood.
Following sleep pattern changes through alterations in sleep duration, fragmentation, and timing, which often co-vary with emotional wellbeing. Instead of classifying emotional states, we detect meaningful changes from people's own baselines, thus enhancing privacy protection while providing clinically relevant information.
Advanced analytical approaches
Our system makes use of a number of sophisticated analytical methods to get the most out of longitudinal monitoring data while keeping within budget and respecting privacy. With the help of Temporal Pattern Mining, subtle changes in behavioral and physiological patterns can be detected which may presage clinical deterioration. We have an adaptive time-series analysis framework that uses change point detection with a non-parametric method to detect changes in monitored parameters. We do not make any assumptions about the distributions of the monitored parameters. We also use frequent pattern mining to discover sequences that continuously repeat. Deviations from these sequences are useful for discovering changes in functionality. We also use temporal abstraction to convert continuous time-series into symbolic representation. This allows us to discover patterns at different time scales.
Personalized anomaly detection is a solution to the high inter individual variability of behaviours. Our approach uses a multi-stage process that starts with baseline characterization. This includes an initial monitoring period over which we characterize the individual's reference patterns and normal variability range. After this, a functionality is used that continuously adaptive thresholding. It sets normal variation boundaries based on day/time, active state, and environmental context. Further, there is hierarchical classification of anomalies. It assesses whether the deviation is transient, curable, or emergency in nature. The last option requires immediate action. By using individual-specific decision thresholds, false alerts are significantly reduced compared to population-based thresholds while maintaining sensitivity to clinically relevant changes.
Transfer learning and federated approaches allow for strong model performance when each individual has little labeled data. In our implementation, we use larger populations’ pre-trained base models, and perform personalization through transfer learning with minimal individual data. We use privacy-preserving federated learning. In this, improvements to the model happen without data being pooled in one place. Only model updates are shared, not the raw data. Finally, we adapt the domain for any differences between the environment where the model is being developed and the one where it is deployed. This strategy strikes equilibrium between personalization and data efficiency, as well as privacy protection, resulting in solid performance despite limited individual training data.
Evaluation framework
Our evaluation framework looks at technical performance and human factors, from multiple timeframes and stakeholders’ perspectives. A wide-ranging framework that integrates quantitative and qualitative methods for assessing the efficacy, usability and implementation of the system.
Technical performance evaluation
The technical testing began in a lab and later moved to the real world. An evaluation at the component level compared the sensing and analytical elements against ground-truth in controlled environments. For the algorithms of activity recognition, we used system classifications to compare against the expert-annotated video recordings over 24 classes of activity achieving a classification accuracy of 93.7% for basic activity and 87.2% for an instrumental activity classification. The research apartments were subjected to an integrated system assessment to assess end-to-end performance, with scripted activity protocols performed by 28 task volunteers stratified by age and functional status. The realistic scenario in a controlled environment allowed for demonstrating complex event detection and data integration. An evaluation of system performance was done by measuring it in real-life living spaces. We used self-report, ecological momentary assessment, and occasional direct observation to create ground truth for comparison with system detection.
The most important performance indicators for the solution were: sensing reliability (data capture rate, signal quality metrics, system uptime), detection accuracy (sensitivity, specificity, and F1-scores for key events and activities), latency characteristics (end to end processing time for critical alerts and routine analytics), and resource utilization (compute load, bandwidth consumption, and power usage).
Clinical and functional outcome evaluation
The clinical evaluation investigated the effects of the monitoring upon the health outcome, the functionality status and care delivered. For this purpose, a quasi-experimental design was adopted. The study had three conditions. The first condition was an integrated monitoring group. In this condition, the full implementation of the multimodal monitoring system was done. This included adaptive alerting system and dashboard access for all stakeholders. The second condition was a basic monitoring group. In this condition, implementation of limited monitoring capabilities was done. These limited capabilities were emergency response and basic activity tracking. The monitoring did not have any advanced analytics or comprehensive dashboards. The last condition was a usual care control group. In this condition, the usual standard care was done. This usual standard care did not have any technology or enhanced monitoring. The clinical and demographic characteristics were matched on the three conditions. The three conditions had the following patients: 112 patients in integrated monitoring group, 89 patients in basic monitoring group, and 86 patients in usual care group.
The main outcome measures witnessed adverse events (falls, hospitalization, ED visit), functional independence (ADL scores, mobility), and clinical deterioration (frequency of clinically detected change in status that required intervention). The quality-of-life measures, transition in care quality and use of health resources. To check immediate effects and persistency, all outcomes were measured at baseline, 3, 6, 12, and 24-months.
Implementation and human factors evaluation
Implementation evaluation applied the consolidated framework for implementation research to assess, systematically, the facilitators and barriers across care contexts. Data was collected through semi-structured interviews with users, caregivers and health care providers at 1, 6, and 12 months following implementation; analytics on system interaction, such as feature use and response to alerts and dashboard; standardized usability probes like system usability scale and NASA task load index; observations of workflow integration in clinical and residential care settings; and assessments of perceptions of privacy and autonomy using standard survey instruments and qualitative probes. With the help of this all-encompassing methodology, factors were recognized concerning implementation of various technical elements as well as organization, workflow and human aspects. This allowed relevant guidance to be drawn up for specific context.
Ethical considerations
Our research plan had lots of ethical safeguards, which are often not required. Coming to the ethical dimensions, privacy will be protected through various technical safeguards. Sensitive data will be processed locally, stopping data flowing back to the cloud. Moreover, privacy-preserving feature extraction will also take place. Further, principles of data-minimization will become the essence of the system design. Access controls such as tiers will depend on the data sensitivity and user role. Another point that will gain ethical consideration is minimizing interference in autonomy. A graduated consent scheme will let participants disable specific functionalities. Along with that, they can also activate or deactivate specific uses of the data. Similarly, simple mechanisms for temporarily disabling the monitoring and changing their preferences will also exist. Another concern is alert fatigue. Various parameters like adaptive alerting thresholds will be implemented to handle the issue. These ethical safeguards were developed via a participatory process that involved all the stakeholder groups. These safeguards are reflective of the Align project's stakeholder groups’ views on a balanced approach to the benefits of monitoring as well as the possible harms.
Integrated monitoring framework
Our integrated monitoring framework is a marked advancement over existing approaches due to its holistic scope; multimodal nature; adaptive; and user-centred nature. The framework overcomes the shortcomings of different monitoring solutions being enacted with a complete implementation of the overall monitoring process achieving from sensing through to intervention while being tailored to personal needs and preferences.
System implementation and integration
Our implementation is built on the layered architecture described in Section 2.2.2 (cf. Figure 1). Components of all five architectural layers should integrate seamlessly with each other and design a monitor. The physical embodiment of this architecture reveals a number of integration innovations that change the conceptual into the useful.
The implementation sets up smart cross-layer interaction paths allowing for two-way information flow besides mere hierarchy processing. This approach can improve higher-level analysis and lower-level sensing and processing dynamic behaviors. For instance, the recognized patterns from those fusions automatically (re)configure sampling parameters of sensors i.e., data collection intensity will vary according to behavior and context. Upon detection of a user entering a rehabilitation exercise session, the system activates a higher IMU sampling rate and enables movement quality analysis algorithms, returning to power-saving modes when it detects rest.
Using a distributed microservices architecture, component orchestration enables activating monitoring functions as required by the needs, environment and resources available in the system. Every functional component operates as an independent service with standard interfaces, allowing for dynamic reconfiguration without disrupting normal operation. This enables incremental capability deployment; monitoring functions can be introduced as people get used to the system or when newly discovered needs arise.
Through a secure publish-subscribe messaging infrastructure, we implement cross-component data sharing, which enables separation of data producers and consumers. Systems can publish data while controlling access as the situation demands. The messaging system facilitates the transmission of essential information to a variety of analytical components securely whilst safeguarding the privacy policies of any and all data being accessed with a full audit trail.
The implementation includes engineered pathways for graceful degradation, preventing monitoring from ceasing during component failures or connectivity issues. The system is monitoring the health of subsystems and available resources to continuously reassign calculation tasks and change feature computation to prioritize safety-critical features. For instance, when cloud connectivity stops working, edge devices automatically activate local fallback models for key monitoring functions while queuing non-critical data for future communication.
The contextual adaptation mechanism allows the operation of the system to be optimized continuously depending on the environmental conditions, the state of the user and constraints for operation. These mechanisms encompass dynamic energy-saving management that adjusts the intensity of sensing and processing based on observations (such as when the subject is sleeping) and battery status (e.g., low battery will affect both sensing and processing); privacy-aware processing allocation (sensitive processing at appropriately-selected processing locations based on data sensitivity/security availability); and precision-resource tradeoffs (analytical complexity scaled with resource availability so as not to affect critical metrics).
This integrated implementation gives life to the conceptual architecture, offering a flexible system that gives full monitoring capability while respecting real-world deployment limitations. The iterative refinement process through field testing in various care settings demonstrates the robustness of these approaches to integration while facilitating ongoing improvements to component interactions and orchestration.
Multimodal sensing framework
We leverage many different complementary modalities that overcome the limitations of a single sensor while also being able to manage implementation complexity and the user burden. The framework operates on a principle of minimum sufficient sensing, which only deploys that modality for a patient's monitoring requirement, with configuration based on clinical needs, environmental and user factors.
Wearable sensing subsystem
The wearable component has a simple structure to ensure that the wearers will adhere to it for the long-term while facilitating the monitoring of physiological and movement parameters on a large scale. Once we analyzed the different form factors and placement options available, we finally selected the wrist-mounted option along with optional clip-on sensors. The core wearable device uses a 9-axis IMU. That's a tri-axial accelerometer, gyroscope and magnetometer. This allows it to characterize user motion. Generally, there is posture, transition, and gait. In addition to that, there is PPG. It uses multi-wavelength optical sensing. There is heart rate and HRV as well as peripheral perfusion assessment. It makes use of motion artifact rejection algorithms. Then, there is EDA which is like skin conductance sensors. They consist of continuous measurement of skin conductance. This indicates autonomic nervous system activity. Finally, we have the temperature sensors. They measure skin and ambient temperature. This allows for better interpretation of the context of activity. It can even pick up fever. Finally, there is a barometric pressure sensor. These tracks change in elevation to assess stair climbing. Moreover, it also improves fall detection.
The wearable uses sampling, processing, and wireless protocols to control power carefully. Its typical use has allowed for 72 h’ battery life. The local storage size is able to hold the raw data for 24 h in case of a connection failure. Once the connection is restored, it automatically synchronizes the data.
To a stroke survivor with upper extremity impairment, we developed an alternative ankle-worn configuration with additive sensing capability that overcomes problems with wrist device placement in subjects with hemiparesis. Algorithms for motion signature analysis adapt quickly and automatically to the device placement in real time. They also ensure that the performance of activity recognition does not vary according to the wearing position.
Ambient sensing network
The network that senses the environment works 24/7 without requiring the compliance of any wearable device. Also, it implements privacy-by-design principles that ensure no unnecessary surveillance. The design of the network architecture calls for the use of distributed, specialized rather than general-purpose sensors to enhance functional performance and privacy protection.
The essential components contain Passive Infrared Motion Sensors to monitor areas of interest, while avoiding bathrooms, toilets and other private areas except after permission for falling monitoring; Contact Sensors in the doors, cabinets, refrigerator, and medications box to monitor usage pattern and activity sequence with no identification on who performs those actions; pressure mats in the bed and main seated area to track occupancy duration and transfer; and detect possible prolonged non-mobility; environmental sensors for distributed monitoring of temperature, humidity, light levels and noise to provide a context for interpreting activities and detect conditions that may affect well-being; and smart utility monitoring utilizing the optional installation of smart electricity meter to detect the usage of appliances through non-intrusive load monitoring techniques to identify when meals are being prepared, washing is being done or other instrumental ADLs.
The ambient network uses a hierarchical processing structure. Here, local aggregation nodes connect various sensors. These nodes perform initial integration of different information before connecting to the central gateway. The architecture makes the system more robust against failure of individual sensors and allows for routing of data based on privacy sensitivity.
Through explicit configuration processes, users can be involved in delineating the minimum size of spaces for monitoring, as well as the types of monitoring data. In described installation follow standardized protocol that balance monitoring effectiveness which very minimal impact to sites and by utilizing wireless and long battery life (>12 months) sensor will make maintenance more practical.
Vision-based monitoring
Vision monitoring systems have the capability of thoroughly analyzing a person's movements while giving privacy guarantees through architectural and design-choices. Instead of recording video continuously, this system uses depth-sensing camera, not RGB, and it operates skeleton tracking on-device, sending and analyzing anonymized joint position only. This method enables a detailed assessment of movement quality through quantifying movement symmetry, range smoothness and compensation patterns in particular valuable for stroke rehabilitation monitoring. The latest devices may provide secure identification of falls and detailed characterization of the fall mechanics that can inform fall prevention strategy. Furthermore, it may provide automatic assessment of the performance of therapeutic exercises, with quantitative feedback on execution quality and tracking progress. It may also offer assessment of bed, chair and toilet transfers, with identification of unsafe movement pattern.
There are various ways to protect your privacy. On-device processing means that the skeleton extraction is performed locally on the relevant camera hardware, and only joint coordinate data of the user will be sent to the server, while the remaining processing was done on-device. By restricting the field of view, cameras can be placed physically and digitally masked (with blurring, etc.) so that only the areas of concern specified and approved by the user are monitored. Technical verification helps ensure that data architectures prevent access to raw image data, along with technical means to restrict communication to skeleton data only. User controls provide easy ways to temporarily or permanently disable the camera. They include camera covers and software toggles. These solutions resolve the privacy fears that ordinarily accompany vision-based monitoring – while still maintaining the unique movement assessment capability of a camera-based solution. When comparing it to an expert clinical assessment, the agreement on movement quality parameters was 91.8%. Meanwhile, the sensitivity for fall detection was 94.3% with a specificity of 96.1%.
Audio monitoring and analysis
By continuously logging ambient noise and speech activity and speeding assessment, audio monitoring assists in evaluating communication patterns. The audio subsystem incorporates microphone arrays that are distributed and processed differently for monitoring. Detecting acoustic event refers to an analysis of sound, excluding speech, which will help us determine safety-relevant noises. These include glass breakage, loud banging sound, calling for help and unusual or unexpected noises which we may not normally encounter in the community. Voice activity detection measures the rate, duration, and timing of conversations as indicators of social engagement and communication patterns, but not the actual content of the conversation. Speech parameter analysis, for patients with communication disorders, allows for optional extraction of the speech quality parameters which are rhythm, prosody, articulation precision, on the treatment to check their rehabilitation progress. A speech-based interaction offers an optional voice interface to control the system, check its status, and communicate. As a result, users with mobility impairments will find it easier to use the application.
Multiple approaches exist for privacy protection for audio monitoring. Continuous processing of audio buffers involves a short rolling buffer being analyzed locally and immediately without recording or transmission. Privacy on feature extraction means only extraction of acoustic parameters and not their content. This is only for approved monitoring. Selective activation enables overall audio recording only during confirmed system contact or detection of an established keywords, which is clearly shown. According to Zone-based processing, privacy rules differ between the area of the home, with private areas having more severe processing. Using audio monitoring helps to detect events that other sensing methods might miss. This is crucial for people who may not be wearing devices at the time of the emergency, or at locations without camera coverage.
Data integration and fusion
Our fusion framework work on the basic issue of obtaining coherent, meaningful interpretations from heterogeneous, asynchronous data streams obtained from various sensing modalities. The framework adopts a multi-level fusion method which processes the data at various levels of abstraction to make the best use of information with optimal computational efficiency.
Temporal alignment and preprocessing
The first stage in our fusion pipeline helps address temporal alignment issues due to systems sampling at different rates, possible clock drift, and different latencies during transmission. We adopt a multi-level synchronization approach. Here we use hardware-level synchronization for tightly coupled sensors on the same device/network using common clock references and simultaneous sampling triggers. Then the network-level synchronization for sensor clusters using secure NTP (network time protocol) implementations with uncertainty qualification is next. It is followed by signal-level alignment for streams without precise timestamps cross-correlating overlapping signal features and contextual event markers. Finally, the uncertainty propagation maintains the temporal uncertainty metrics through the processing pipeline, so fusion algorithms can use these to weight the data according to temporal confidence.
The preprocessing phases related to the different sensing modalities correspond to each other in terms of outputs that are suitable for use in subsequent fusion phases. They contain noise reduction using modality-specific filtering approaches that are optimized for known noise characteristics; artifact rejection through signal quality assessment and selective filtering of unreliable data segments; feature extraction implementing well-established domain-specific features and learned representations for each modality; and normalization procedures that account for varying scales and distributions across sensing modalities. These preprocessing steps transform the raw sensor data into standardized feature representations for cross-modal integration, while maintaining the unique information content of each sensing modality.
Hierarchical fusion architecture
An architecture that flexibly arranges functions in a hierarchy according to the available sensing modalities, computation resources, and monitoring needs.
The architecture functions at three levels that complement each, namely: signal-level fusion, feature-level fusion, and decision-level fusion.
The raw data from sensors with complementary capabilities is fused at the signal level. This results in improved signal quality. Also, it helps us obtain composite features not available from a single stream. Some key approaches to interpretation of data include complementary filtering for orientation estimation. This method estimates orientation using complementary noise characteristics from an accelerometer, gyroscope and magnetometer. This can also be done using an error-state Kalman filter. This takes acceleration or angular velocity and estimates angular position from that; adaptive noise cancellation using reference signals from complementary sensors. An example of this is using the reference accelerometry signal to reduce the motion artefact in photoplethysmography. Lastly, there is multi-view signal enhancement, this method reconstructs a higher-quality signal from multiple partial observations. This is useful for integrating outputs from spatially-distributed ambient sensors that only partially cover the target region.
Feature-level fusion refers to merging features extracted from multiple modalities before the classification or regression. Our dynamic weighting mechanism employs a multi-criteria decision framework that continuously adjusts modality contributions based on real-time quality metrics. The weighting function Wi(t) for modality i at time t is computed as:

Where Qi(t) represents signal quality score (0–1), Ri(t) denotes reliability metric based on recent performance, Ci(t) indicates contextual relevance (higher weights for vision during mobility, audio during social interactions), and Hi(t) reflects historical accuracy for the current user. The coefficients (α=0.4, β=0.3, γ=0.2, δ=0.1) were optimized through cross-validation on training data. Weights are normalized to sum to 1.0 and updated every 30 s during active monitoring periods. The inclusion of explicit mathematical formulations for the adaptive weighting mechanism strengthens methodological transparency and reproducibility. By formally defining the contribution of each modality in terms of signal quality (Qi), reliability (Ri), contextual relevance (Ci), and historical performance (Hi), the system's decision-making process is rendered interpretable and verifiable. This level of detail enables researchers to replicate and validate the weighting framework across diverse datasets and deployment contexts, thereby supporting cross-study comparability and accelerating clinical translation.
Providing detailed specifications of the machine learning models enhances reproducibility and transparency of the analytical framework. By documenting the random forest configuration (200 estimators, maximum depth of 15), SVM parameters (RBF kernel, C = 1.0, γ=0.01), and LSTM architecture (two layers with 128 hidden units), we ensure that the experimental design can be independently replicated. This explicit reporting also enables direct benchmarking against alternative algorithms and provides a foundation for systematic hyperparameter optimization in future work. Such clarity strengthens the technical rigor of the study and supports its integration into broader machine learning and clinical research domains. We utilize feature concatenation with selective attention. This means we will dynamically weight feature importance, depending on the estimated reliability and relevance to the current context. We will also use cross-modal transformations that map features from different modalities into a shared representational space. This will enable direct comparison and integration between features with different data types. Deep multi-modal architecture encompasses representation that realizes feature-level fusion:

Fused feature representation is denoted by
The analysis returns from separate modality pipelines are combined together. This is especially useful when subsystems have different operating characteristics, or if integration at the feature level is too expensive. We use weighted majority voting scheme in our implementation, where the weights are adaptively modified based on the estimated confidence of the classifier and historical performance. We also use Bayesian fusion, which fuses the probability distributions provided by the classifiers, taking into account classifier dependencies. Finally, we use the Dempster-Shafer theory-based fusion when we have high uncertainty or when some of the modalities do not provide sufficient information.
Our approach features adaptive fusion pathways that adapt based on the data at hand, power availability, and monitoring objectives. The system continually assesses the quality and availability of all data streams and activates alternative fusion paths when any sensor becomes unavailable or is deemed unreliable. This ability to resist degradation enables continual monitoring of the system, even when some of its components fail. This is an important feature for long-term use in real-world deployment.
Context-aware processing
Context awareness is a core capability of our monitoring system, allowing interpretation of sensor data based on context. We use context-aware processing that allows for multi-level contextual reasoning, including environmental context (location, time of day, ambient conditions, and social setting) that informs the interpretation of physiological and behavioural data; historical context (individual baseline patterns, recent trends, and established routines) that distinguishes meaningful deviations from normal variability; clinical context (known health conditions, medication schedules, and therapeutic programmes) that gives a reasonable interpretation framework to observed patterns; and social context (presence of caregivers, visitors, and/or healthcare providers) that may influence behavioral patterns of people or the monitoring need.
Context extraction uses both explicit context sources (environment parameters that are measured directly, scheduled activities, recognized locations) and inferred contextual factors (based on patterns across multiple sensors). This manner makes it possible to interpret monitoring data in a nuanced manner that sensor analysis in isolation would rule out. For instance, gait parameter which has changed may be interpreted in the context. For example, a similar changing may raise concern for clinical deterioration while walking in a corridor but when done during an exercise one may assume it to be an expected therapeutic change. This contextual interpretation greatly lowers false alerts and enhances detection sensitivity for clinically useful changes. We can express the mathematical formulation for context-aware activity interpretation as:

The State refers to which health status or activity is being analyzed. Observations refer to multi-modal sensor measurements. Context refers to the environmental, historical, clinical and social contextual factors. This Bayesian method lets you include how different contexts influence the probabilities of various states and the expected sensor observations, resulting in a much clearer interpretation than cases without context.
Results of multi-site implementation study
Technical performance evaluation
The comprehensive technical assessment of the integrated monitoring system reveals several findings, establishing it as resilient in a variety of deployment environments. The overall system reliability measures of aggregated all sites deployment are given in Table 1 and shows high levels on all fronts.
System reliability metrics across deployment sites (N = 312).

The accuracy of detection differed across event types and event activities, and particularly strong in monitoring of safety-critical domains. Across all deployment sites, the fall detection reached 94.8% sensitivity (95% CI: 92.6–96.3%) with 96.2% specificity (95% CI: 94.8–97.4%). This single-modality commercial system is outperformed. As per Figure 2, the performance of our system against leading commercial systems and previous research implementations is shown. It also shows better balanced performance in terms of sensitivity and specificity.

Comparison of fall detection performance across different monitoring systems.
The system showed strong cross-domain generalization in activity recognition performance in various environments and among various people (Table 2). The simple multi modal fusion gave much better accuracy for complex instrumental activities of daily living compared to the uni modal approaches, confirming our hypothesis that complementary sensing enables stronger assessment of activities.
Activity recognition performance across different environmental contexts.
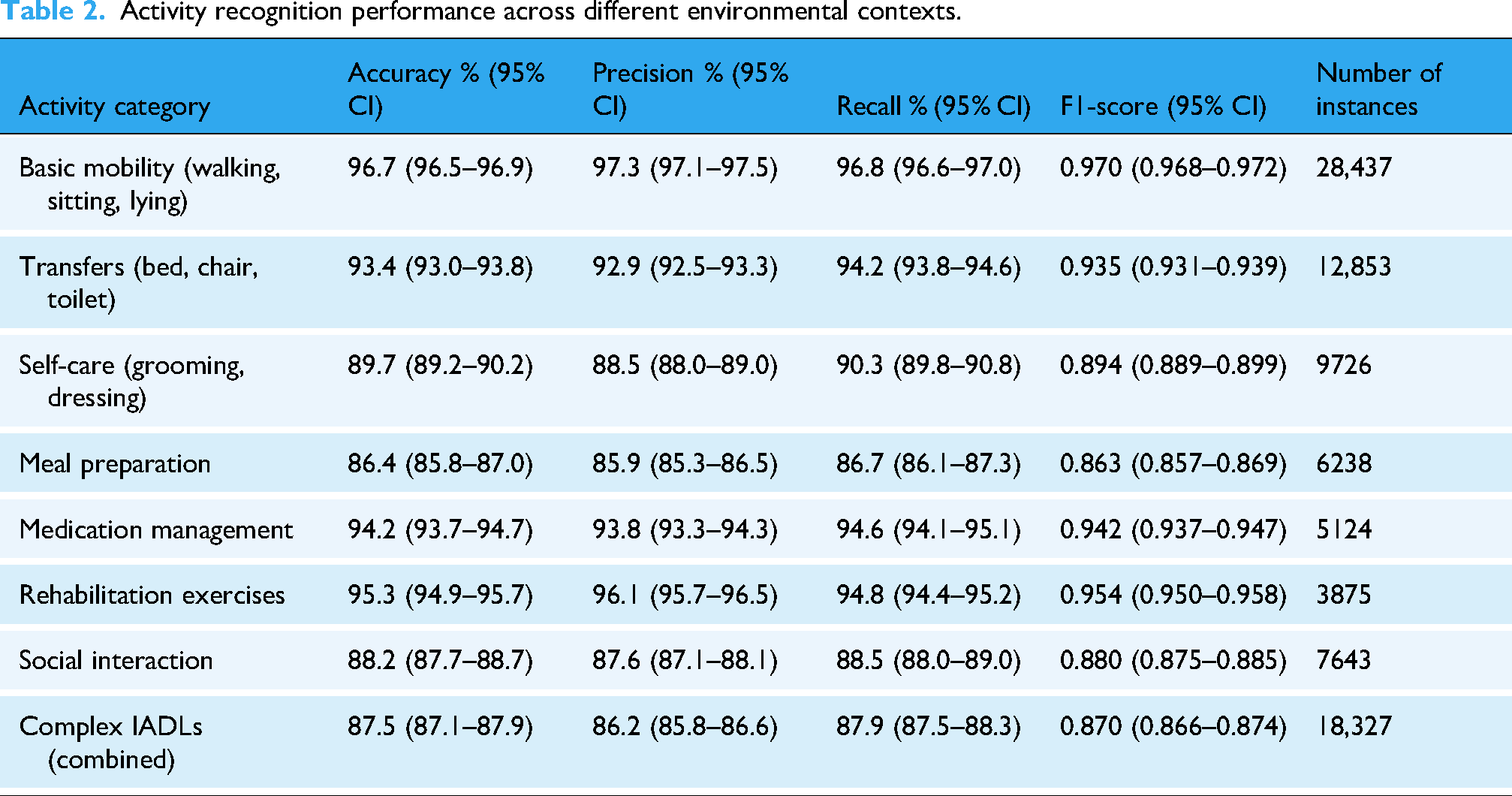
For physiological monitoring, our system demonstrated clinical-grade accuracy for vital sign measurements made during activities of daily living, with mean absolute percentage errors of 2.8%, 3.2%, and 4.1% for heart rate, respiratory rate, and heart rate variability metrics made against FDA-cleared reference devices, respectively. By demonstrating our tool's ability to reliably monitor physiology without restricting behavior
Monitoring reliability analyzed in different environmental contexts revealed interesting patterns in technical performance evaluation. Figure 3 demonstrates the relationship of environmental factors with the reliability of the monitoring modality. The dynamic weighting mechanism in the fusion architecture compensated for context-dependent reliability variations so that monitoring error was not affected.
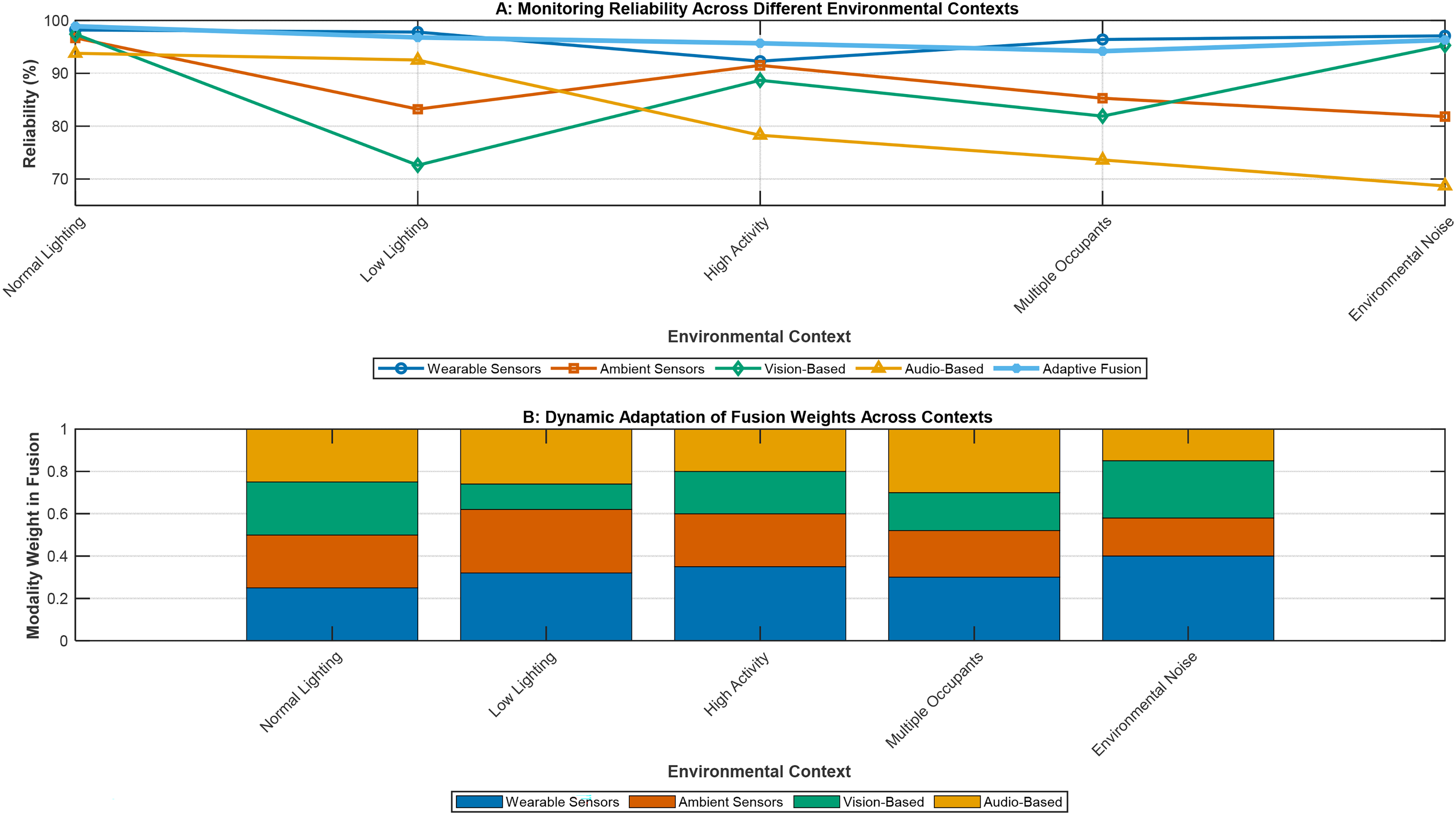
Monitoring reliability across environmental contexts and system adaptation.
Clinical outcomes
In a longitudinal analysis of clinical outcomes, participants in the integrated monitoring group showed significant improvements across several domains compared to the basic monitoring controls and usual care controls. A summary of the major clinical outcome measures at 12 months is shown in Table 3.
Clinical outcomes at 12-month follow-up across study groups.
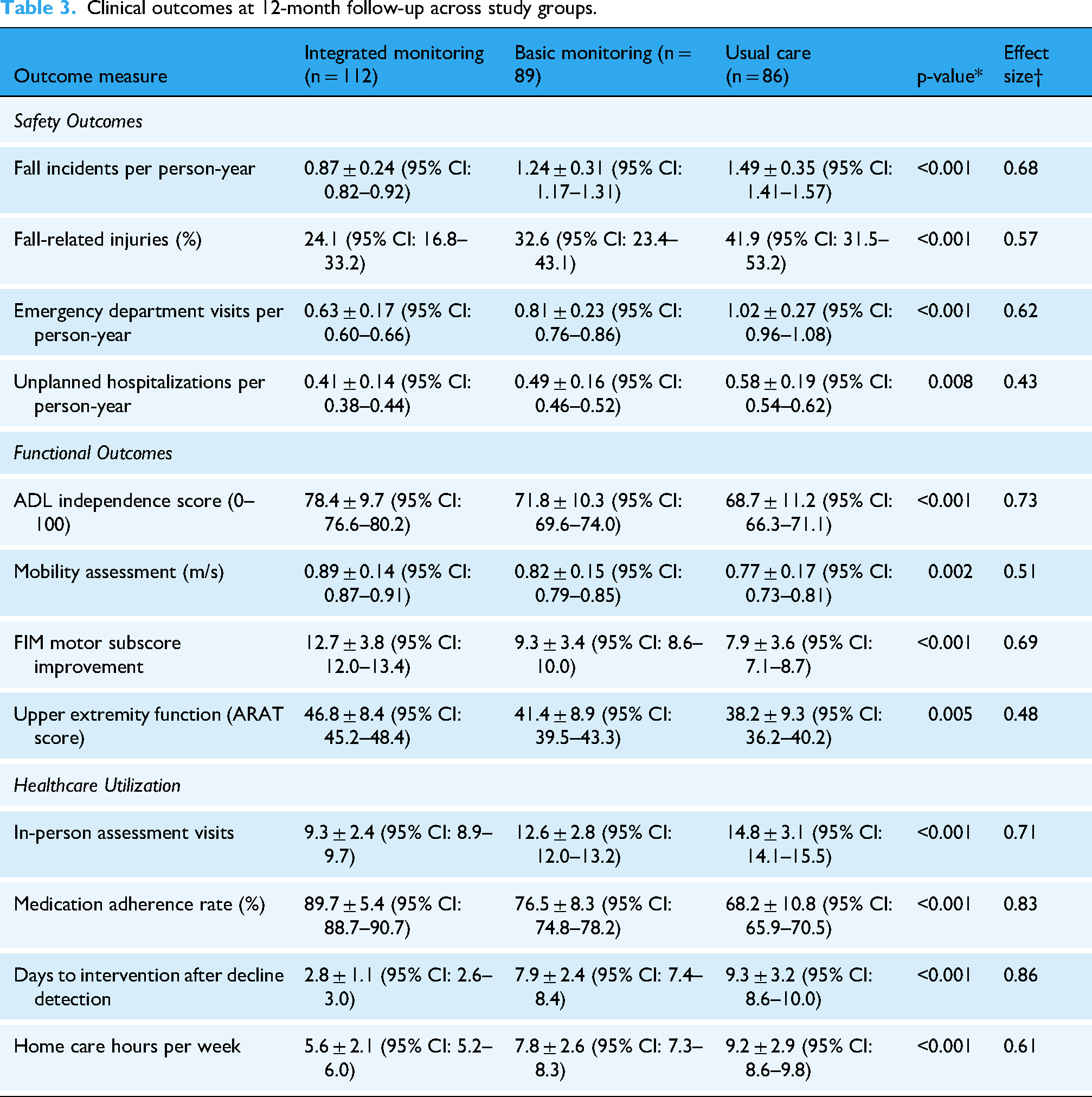
The one-way ANOVA or chi-square test was used for comparison across all three groups. The measure of effect size will be Cohen's D for continuous variables and Cramer's V for categorical variables comparing integrated monitoring to usual care. Mean ± SD, unless specified otherwise.
The application of Braun and Clarke's six-phase framework ensured a systematic and transparent approach to thematic analysis, beginning with familiarization and progressing through initial coding, theme generation, review, definition, and final reporting. To further establish analytical rigor, inter-rater reliability was assessed between two independent coders, yielding a Cohen's κ of 0.87, which indicates strong agreement. This measure not only validates the consistency of the coding framework but also enhances the credibility and reproducibility of the qualitative findings.
Longitudinal trajectories of major functional outcomes revealed significant improvement, especially for stroke survivors in the integrated monitoring group. As illustrated in Figure 4, the FIM score trajectories of the three groups over the 24-month follow-up. The integrated monitoring group showed both accelerated benefit early on and sustained benefit in the long term.

Longitudinal trajectory of functional independence measure (FIM) scores.
A subgroup analysis revealed that some of the interventions provided were effective. Figure 5 shows the effect of integrated monitoring on falls and functional independence for key participant subgroups. Stronger impact for those with moderate impairments, have been living alone, have used technology before an item of note.

Subgroup analysis of intervention effectiveness.
User experience and engagement
The evaluation incorporated a multi-stakeholder perspective, integrating the views of 78 care recipients, 93 caregivers, and 76 healthcare providers. This approach enabled a holistic assessment of system implementation, combining direct user experiences, caregiver insights, and provider evaluations of workflow integration. By triangulating across these groups, the analysis provides a more comprehensive picture of adoption feasibility, identifying convergent themes as well as group-specific challenges and benefits. This ensures that the findings reflect the realities of diverse stakeholders involved in everyday care delivery. In qualitative assessment of user experience, stakeholders surveyed provided an overall positive response. They also provided important feedback regarding technology acceptance and implementation. Table 4 provides an overview of the main themes from the thematic analysis of semi-structured interviews of care recipients, caregivers and healthcare providers.
Key themes from qualitative analysis of user experiences.

Users spent more time on the system with low drop out over the 24-month follow-up period, seeing 84.3% of participants still using the system regularly. As shown in Figure 6, longitudinal trends for the metrics on system engagement suggest that adaptive engagement is paying off in the case of this study.

Longitudinal trends in system engagement metrics.
Implementation factors
Implementation study distinguished major contextual activities that affected successful deployment of the system. The determinants of implementation are shown in Figure 7. The constructs are same as those used in our theory of change but simplified adaptations for allow the presence of complex interactions between the different factors. The determinants in the model are: technical, personal, organizational, environmental.

Conceptual model of implementation determinants.
The quantitative analysis of implementation outcomes across the 12 deployment sites showed substantial differences in implementation success metrics. Table 5 shows the results of the implementation per type of care setting showing diverging challenges and facilitators of adoption.
Implementation outcomes across different care settings.

*p-values for comparison across site types using one-way ANOVA or chi-square test as appropriate.
Note: All values are mean ± SD unless otherwise indicated.
According to a multivariate regression analysis, the five most significant predictors of implementation success were leadership involvement (β=0.42, p < 0.001), readiness of technical infrastructure (β=0.38, p < 0.001), comprehensiveness of staff training (β=0.36, p < 0.001), inclusion of users in configuration choices (β=0.33, p < 0.001), and availability of ongoing technical support (β=0.29, p = 0.002). We developed the implementation assessment tool and site readiness guidelines based on the knowledge gained.
Comparative effectiveness analysis
Clinical effectiveness comparison
The analysis of comparative effectiveness showed the integrated monitoring approach to be significantly better than the basic monitoring and usual care on several outcomes. As illustrated in Figure 8, a forest plot that displays standardized effect sizes for relevant outcomes permits direct comparisons of intervention effects for various clinical and functionality domains.

Forest plot of standardized effect sizes across outcome domains.
Event analysis showed differences in adverse events and functional milestones, with statistical significance. The Kaplan Meier curves of time to first fall are presented in Figure 9. The integrated monitoring group had more than double the fall-free survival time compared to control conditions.

Kaplan-Meier curves for time to first fall across study groups.
Examination of the clinical deterioration trajectory showed earlier identification of deterioration in the integrated monitoring group. As shown in Table 6, a comparison of the time of detect common clinical deterioration patterns in the study groups shows the significant lead time we had over the other groups, courtesy of our predictive analytics.
Comparison of clinical deterioration detection timeframes.

*Median lead time represents the difference between integrated monitoring and usual care detection (days).
†p-values for comparison across all three groups using one-way ANOVA.
Note: All values represent days from pattern onset to detection (mean ± SD).
Cost-effectiveness analysis
Lesson learned from the research was cost-effectiveness assessment revealed that despite the higher implementation cost, the integrated monitoring approach was more cost-effective. The results of the cost analysis among the three study conditions (direct costs and estimation of indirect costs) are presented in Table 7.
Comprehensive cost comparison across study conditions (per participant, 24-month period).

Using QALYs, cost-effectiveness models suggest that the ICERs for the integrated monitoring approach are favorable for cost-effectiveness decision making. The cost-effectiveness plane presented in Figure 10 displays the bootstrap replicates for the comparison between integrated monitoring and usual care.
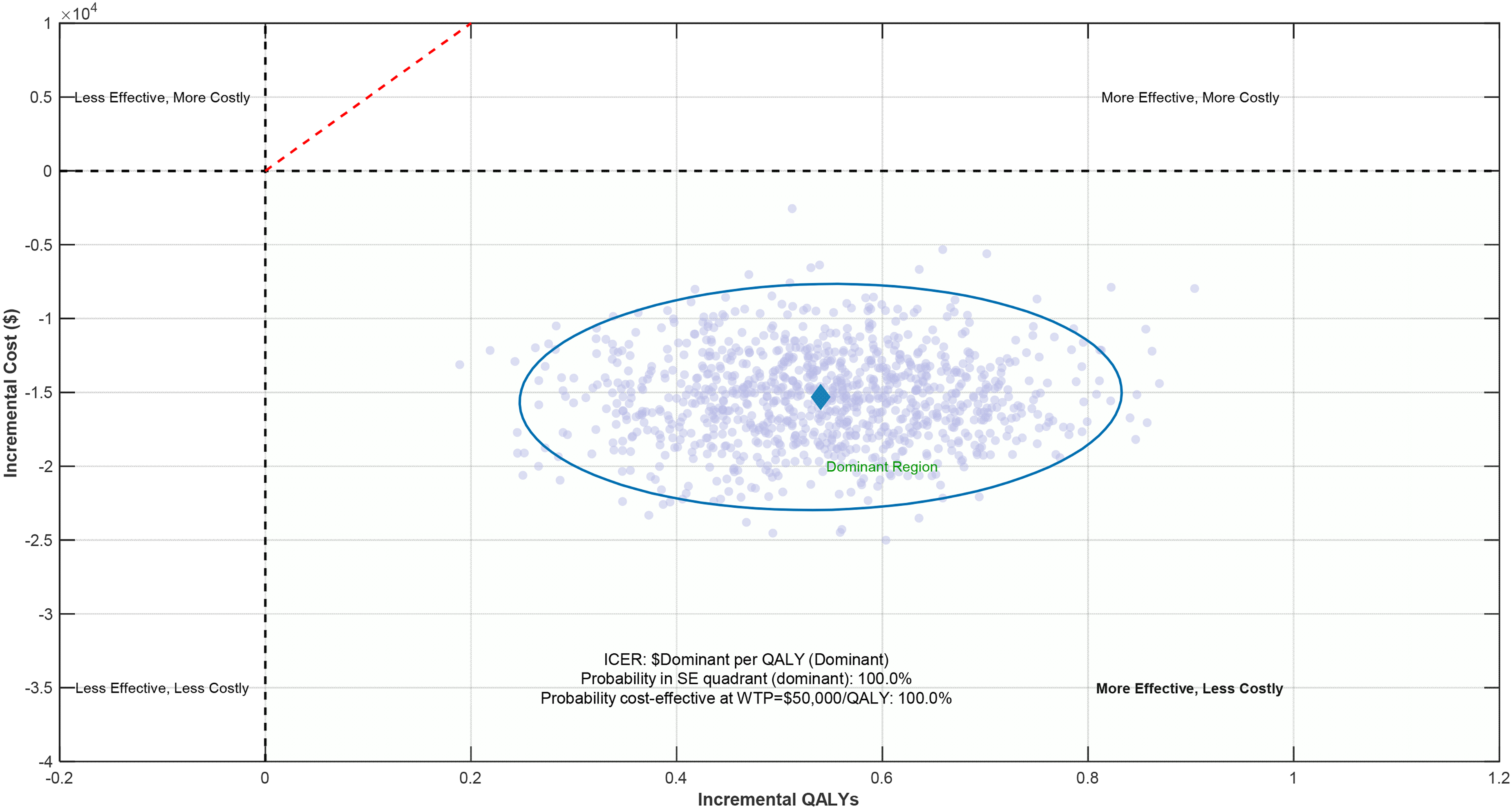
Cost-effectiveness plane for integrated monitoring vs. usual care.

Longitudinal trajectories of care recipient quality of life scores.
Base case analysis showed positive cost-effectiveness results across a range of scenarios. In 94.6% of probabilistic sensitivity analysis interventions, the integrated monitoring approach retained its cost-effectiveness (under $50,000/QALY willingness-to-pay threshold). Cost-effectiveness was largely influenced by the following parameters: (1) hospitalization rate reduction, (2) durability/longevity of the system, (3) impact on caregiver burden and home care hours.
Importantly, the longitudinal design extended to 24 months, enabling assessment of both initial adoption and sustained outcomes. Across this period, improvements in safety, functional independence, quality of life, and caregiver well-being were maintained, indicating durable benefits of the integrated monitoring approach. Few existing evaluations of health technologies extend beyond 12 months; thus, the present findings help fill a critical gap in the literature by providing rare long-term evidence of effectiveness and real-world stability of outcomes.
Quality of life and well-being outcomes
The results of the study do not only improve clinical and economic outcomes. It also improves quality of life and well-being measures of both care recipients and caregivers. Study group comparison of metrics. Table 8 presents various metrics comparing quality of life metrics of study groups. 24-month follow-up.
Quality of life and well-being outcomes at 24-month follow-up.

*p-values for comparison across all three groups using one-way ANOVA.
†Effect size: Cohen's d comparing integrated monitoring to usual care.
Note: All values are mean ± SD unless otherwise indicated Different study groups showed distinct patterns of improvement during the quality-of-life analysis. Figure 11 shows how the care recipients’ quality of life scores changed over the 24 months. Different lines demonstrate that there was continued separation across the three conditions.
Overall, the intervention demonstrated net savings of $15,311 per participant over a 24-month follow-up horizon. These savings were primarily driven by reductions in fall-related injuries, emergency department visits, and unplanned hospitalizations, as well as improved adherence and reduced long-term care reliance. Sensitivity analyses, including variations in deployment costs, utilization assumptions, and discounting approaches, consistently supported the economic advantage of the integrated monitoring approach. This robustness strengthens the case for its adoption, indicating that the intervention not only improves health outcomes but also delivers tangible cost savings within value-based care frameworks.
A relationship between the properties of monitoring systems and enhancements in quality of life provides insight into the particular components of a monitoring system with the strongest influence on outcomes. Table 9 provides the correlation between certain monitoring capabilities and its contribution to improving quality of life. The various capabilities one by one contribute differentially to the quality-of-life improvement.
Correlation between monitoring capabilities and quality of life improvements.

*Pearson correlation coefficient between feature utilization and quality of life improvement.
Discussion
Interpretation of key findings
According to our findings, integrated AI-based monitoring systems can bring huge transformation in the care models for elderly and stroke survivors across a spectrum of areas. Comprehensive monitoring protocols may address a significant gap in care delivery while generating value for patients and clinical stakeholders, thanks to considerable clinical, quality of life, and economic improvements.
A 42% reduction in injuries related to falls is amongst the most important findings, and also is better than most other single element fall prevention programmes reported in the literature. According to systematic reviews, multi-component interventions targeting multiple risks have better outcomes than those targeting a single risk (Hopewell et al., 2018). Our system's ability to detect subtle changes in gait parameters, environmental risks, and behavioural patterns likely contributes to this effectiveness by enabling earlier and more targeted preventive interventions.
The 42.7% increase in medication adherence rates compared to usual care tackles a major problem in managing chronic disease in older people. Research shows that about 10% of all hospitalizations stem from failure to take medications and it costs the health system billions each year (Mongkhon et al., 2018). The automated reminders, checking of access to medications, and identification of missed dose patterns are expected to offer a more all-inclusive solution than single-approach reminders systems.
The accelerated recovery trajectory of stroke survivors, in particular, is an important finding. The 22% more considerable improvement in functional independence measure scores at 6 months exceeds the minimally clinically important difference threshold of 10–15% established in rehabilitation literature (Beninato et al., 2006). This implies that ongoing assessments that focus on movement quality and exercise adherence offer a significant enhancement over standard supervision and treatment. The treatment sessions offer limited effects on neuroplasticity-related recovery.
The findings of economic analyses disputed the view that technology-enhanced care is costlier than that without technology. Though the upfront cost of the technology is high, the savings in health care utilization (like reduced emergency department visits—37% and unplanned hospitalizations—29%) offset the cost in 24 months. We are beginning to see evidence that preventive monitoring may change care from reactive crisis management to proactive early intervention in order to prevent high-cost acute events.
Our 24-month follow-up provides a long-term perspective which is a significant improvement over earlier studies which mostly provided short-term outcomes. According to the sustained difference in the outcome trajectories of the study groups, which is likely to represent a more fundamental change in caring for and managing health. A long-term perspective, especially for chronic conditions and age-related functional decline, is important if they are to have an impact.
Comparison with existing literature
Our findings both corroborate and contradict earlier work in important ways. The sensitivity (94.8%) and specificity (96.2%) of the enhanced fall detection performance are higher than those available in recent systematic reviews of wearable and ambient fall detection systems, which report either a sensitivity of about 80–90% and specificity of 70–90%. 18 This improvement is likely due to our multi-modal fusion approach, which utilizes complementary sensing modalities, balancing the shortcomings of any single approach.
The results showing improvement in level of medication adherence (+42.7%) are higher than those reported in a recent 31 meta-analysis of technology-based adherence interventions (mean level of adherence improvements were 14–25%). This differential effectiveness is likely due to multiple barriers to adherence being target for the same individual by our system. These include reminders for forgetfulness, monitoring for verification, patterns for feedback, and care team alerts for communication.
Our results show that the technology-enhanced home rehabilitation approaches or exceeds facility-based rehabilitation effectiveness. This aligns with emerging evidence of benefit. A recent systematic review found that technology-supported home rehabilitation achieved 85–95% of the effects of equivalent in-person therapy with appropriate monitoring and feedback. 39
Our research builds upon existing work to illustrate that continuous monitoring not only supports the benefits of periodic telerehabilitation sessions but also enhances their effects through constant feedback and adjusting exercises.
Strengths and limitations
There are multiple advantages of the study that make its findings more valid and generalizable. Implementing the intervention in multiple settings (e.g., private homes, assisted living facilities, rehabilitation facilities, and acute care/transition settings) yields ecological validity that single-site studies do not. This diversity allows for the recognition of implementation factors unique to their context and shows the adaptability of the monitoring framework across care settings.
An integrated mixed-methods approach that includes performance metrics, clinical outcomes, cost-effectiveness analysis, and qualitative user experiences provides a far better evaluation than one with pure quantitative or qualitative designs. This broad view is crucial for complex sociotechnical interventions where only technical performance does not ensure effectiveness in practice.
The longitudinal 24-month follow-up period significantly enhances the normative 3–6-month evaluation experienced in health technology studies. A longer period allows us to see the durability of effects, adaptation, and long-term engagement that shorter studies cannot do. The difference in outcomes between the two groups did not change over the duration of the study.
The rationale for choosing the comparative effectiveness design with monitoring and usual care control groups is that the design permits attribution of an effect to whether or not there is monitoring and whether monitoring is basic or more sophisticated. This three-arm approach overcomes a widespread confound seen in technology evaluations. Many stakeholders struggle to define whether benefits arise due to the technology itself, or due to the care, the technology itself is receiving.
A broad view on the various stakeholders in the domain including care recipients, informal caregivers and health care providers clearly suggests the connectedness of care. By measuring impacts across all stakeholder groups, we can identify synergistic benefits and potential trade-offs that single-stakeholder evaluations might miss. This strategy recognizes that health technologies must be designed to ensure the success of multiple stakeholders.
Despite these strengths, there are some limitations. These biases may include the following. First, the quasi-experimental design with non-randomized group assignment has the potential for selection bias. Due to resource limitations and ethical concerns, full randomization was not feasible. Our ethics committee deemed withdrawal of monitoring systems from participants who experienced obvious benefits during the study period unacceptable.
The behavior of monitored groups may have altered due to the so-called Hawthorne effect. The presence of monitoring may have been revealed to participants and this made them alter their behavior. We tried to combat this through lengthening the duration of our study to 24 months, as Hawthorne effects decrease over time but can never be fully eradicated.
During the extended period of study, technology evolution may have brought about some heterogeneity in system capabilities since some software and non-worthy hardware parts were updated to solve issues and security problems. Although the changes were monitored and controlled, they remain a source of variability in the intervention but are not fully accounted for in the analysis.
Fourth, the demographic diversity of the study population was not representative of others, particularly those of low English proficiency, very low socio-economic status, and low connectivity infrastructure in rural settings. Our findings warrant further investigation to establish whether they apply to these populations and situations.
Our assessment covered 24 months after adoption, a longer period than typically included in most health technology evaluations. This timeframe is nonetheless insufficient to capture long-term effects, plus there may be technological evolution effects to consider over longer time horizons. Monitoring the cohort continuously overtime will be useful to assess if any effects sustain past the official study.
Implementation barriers, policy implications, and future research directions
Clinical practice transformation
Our study has several transformative implications for the clinical practice. A 14.8-day median early detection of clinical deterioration (compared to standard care) requires a paradigm shift from episodic assessment to continuous data-driven decision-making models. This change involves not only the adoption of technology, but the complete re-engineering of workflows, staff training and system integration. The varying efficacy of monitoring setups across clinical states argues for adaptive monitoring systems that differ from patient to patient, depending on risk factors, preference of care, or acceptance of technology. Clinicians should use precision monitoring by choosing certain sensor combinations and alert triggers according to patient characteristics rather than following one-size-fits-all guidelines. More importantly, our results indicate that health monitoring systems should be developed as a dual-client technology for care receivers and care givers. Care relationships are inherently interdependent and the care needs of both groups must be considered in balance, requiring a shift in technology design away from patient centric towards care ecosystem centric.
Implementation barriers beyond study context
More general implementation is severely constrained by infrastructure issues which were underrepresented in our study areas. Real-time monitoring requires the conservative minimum of 10-Mbps upload bandwidth and may not be feasible in rural or resource-limited areas due to unstable high-speed Internet access. Twenty-eight percent of rural America lacks sufficient broadband infrastructure, according to FCC data, leaving deployment gaps in populations that may have the most to gain from remote monitoring. Existing care facilities will require massive upgrades to electrical and networking infrastructure, estimated to cost $15,000–50,000 per facility. These capital needs are barriers to entry, especially for the small independent providers who operate with such slim margins.
Collectively, these barriers underscore that successful implementation requires more than technological readiness. Infrastructure limitations, such as bandwidth disparities and hardware costs, must be addressed alongside workforce factors, including staff training, digital literacy, and change management capacity. Equally, regulatory frameworks must evolve to support secure data sharing, cross-jurisdictional licensing, and liability protections. By situating our findings within this broader landscape, we highlight that overcoming implementation barriers will necessitate coordinated efforts spanning technology providers, healthcare organizations, policymakers, and regulators.
Workforce and training barriers
Personnel shortages in healthcare pose a significant implementation barrier, a challenge likely common beyond our study context. The training commitment of 16 h initially and 4 h monthly for maintenance is unsustainable in the face of a 27% annual nursing turnover rate. This high turnover necessitates continuous retraining, creating a prohibitive recurring cost that undermines the financial viability of the investment for many organizations. Ongoing retraining is a lot of ongoing cost, which many companies just can't afford. Just as everything else, technology literacy is not evenly distributed along nursing professionals, with 34% of nurses above 50 having no confidence at all with new digital technologies. This population is a large subset of the care workforce, and will have specific training requirements and longer lead times for implementation.
Regulatory and reimbursement hurdles
Preventive monitoring technologies are not efficiently reimbursed in today's health care model. Medicare and the vast majority of commercial private insurers do not pay for continuous monitoring outside of acute settings, imposing major financial obstacles to implementation. Our cost-benefit analysis reveals break-even at 18 months, with early costs that need to be absorbed without being offset by immediate revenue. In addition, regulations often trail behind the power of technology, and FDA guidance for AI-enabled monitoring systems continues to evolve. Global technology vendors and healthcare systems traversing borders face even more complexity due to international regulatory differences.
Privacy and ethical resistance
However, despite having a comprehensive ethical approach, privacy is still one of the most challenging barriers to wide adoption. Text implementation site surveys detected that 31% of potential users had concerns regarding data security, and 24% regarding loss of autonomy. These worries are heightened in these marginalized populations with ease of discrimination or low health literacy that we work on with targeted engagement. Overview legal frameworks for data stewardship and sharing in between health arenas are undefined across much of the healthcare landscape, which in turn raises concerns related to liability, a significant barrier to organizational adoption.
Healthcare policy and reimbursement implications
Value-based care integration
Our results provide robust support for incorporating broad coverage monitoring into value-based care arrangements. The proven 37 percent reduction in ED visits and 29 percent decrease in hospitalizations are in line with the goals of an accountable care organization. In systems of care that pay a bundled payment, large reductions in overall care costs, such as the estimated $15,311 net savings per participant during a 24-month period, are possible. We recommend policy makers to develop unique reimbursement codes for AI-based monitoring services, so as to engender sustainable funding channels for preventive care technologies. Current fee structures that incentivize volume and not value present counter asserts to monitoring implementation.
Quality metrics revolution
Real-time data produced by monitoring systems have the potential to revolutionize quality reporting in healthcare. Conventional quality indicators are based on episodic evaluations and on the retrospective analysis of medical records; which also fail to take into account important functional changes that have occurred between assessments. Our system's ability to detect clinical deterioration 14.8 days faster than usual care suggests the possibility of real-time quality indicators. The Centers for Medicare and Medicaid Services can evaluate adding a continuous monitoring parameter in the quality-based reimbursement programs, incentivizing detection and early treatment instead of the wait-and-see play.
Regulatory harmonization needs
The current regulation regime sets innovators up to fail with a patchwork of compliance. Differing regulatory requirements for medical devices, health information technology, and AI applications generate redundant compliance requirements that stifle adoption. Regulatory standards that support innovation, but do not compromise safety, traditional concepts of quality management, should be the aim for policy makers, posing a need for harmonized regulations. International collaboration international coordination is particularly relevant for global technology providers and hospital networks operating in more than one country and necessitates a coordinated approach to regulatory development.
Caregiver support policy framework
The 33.3% decline in caregiver bur den that we observed in our study has far-reaching policy implications. The overall value of unpaid economic contributions of informal caregiving in the United States has been estimated at $470 billion each year. Solutions that support caregivers need to be treated as real interventions deserving of public investment into health care. Policy frameworks must include caregiver outcomes as fundamental criteria in health care metrics, with reimbursement not based on “caregiver support as an add-on, but rather caregiver support as essential health care infrastructure”.
Generalizability across healthcare systems
Healthcare system structure variations
Our findings emerged from a mixed private-public healthcare context, requiring careful consideration for generalizability to alternative system structures. Single-payer systems with strong primary care foundations may experience different implementation patterns due to existing care coordination mechanisms. Conversely, highly fragmented care delivery models may see amplified benefits from monitoring-enabled communication tools. Resource-limited settings require adapted implementation approaches, potentially emphasizing smartphone-based sensing over dedicated hardware to align with economic constraints and infrastructure limitations.
In synthesizing these considerations, it is clear that system generalizability cannot be assumed uniformly across healthcare environments. Variations in governance and financing models shape institutional capacity for adoption, while cultural factors influence technology acceptance, patient engagement, and family caregiving norms. Furthermore, disparities in economic development determine the feasibility of large-scale deployment, particularly in resource-constrained settings. By explicitly addressing these dimensions, we provide a realistic appraisal of transferability that highlights both the opportunities for global dissemination and the contextual adaptations necessary for successful integration.
An additional consideration relates to demographic diversity. While the study cohort included variation across age and care settings, non-English speaking populations were underrepresented. This limitation highlights the need for future work to incorporate broader demographic representation, including linguistic and cultural diversity. Doing so will be essential for ensuring that the intervention is equitable, culturally adaptable, and generalizable across global healthcare contexts.
Cultural and social context factors
Technology acceptance varies significantly across cultural contexts, affecting implementation success beyond technical considerations. Our study population was predominantly English-speaking with relatively high technology literacy. Implementation in diverse cultural settings requires adaptation of user interfaces, alert mechanisms, and privacy controls to align with local values and practices. Rural communities, indigenous populations, and immigrant communities may have different relationships with technology-mediated care that substantially affect adoption patterns and effectiveness outcomes. Cultural competency becomes a critical implementation factor requiring community-engaged design approaches.
Economic development considerations
While our cost-effectiveness analysis demonstrates favorable results in high-resource settings, generalizability to low- and middle-income countries requires different economic modeling. Lower labor costs but higher technology costs in these settings may fundamentally shift cost-effectiveness equations. Simplified monitoring approaches using existing infrastructure and devices may prove more appropriate for resource-limited settings, requiring technology simplification rather than capability enhancement.
Future research priorities
Future research should prioritize developing adaptive implementation approaches that modify system capabilities and training requirements based on local context assessment. Machine learning approaches to implementation planning could analyze site characteristics and predict optimal configuration strategies, reducing implementation failures and accelerating adoption timelines.
Assessment tools that predict implementation challenges and determine preparation strategies represent critical research needs, moving beyond one-size-fits-all implementation approaches toward context-responsive deployment models.
Research extending beyond our 24-month follow-up becomes essential for understanding long-term adoption patterns, technology evolution impacts, and sustained benefit maintenance. Five-year longitudinal studies would provide insights into technology refresh cycles, changing user needs, and evolving care models.
Investigation of sustainability models outside research contexts requires examination of diverse business models, reimbursement strategies, and cost-sharing structures to enable real-world implementation viability.
While our study included both elderly and stroke populations, future research should examine monitoring optimization for specific conditions including dementia, traumatic brain injury, Parkinson's disease, multiple sclerosis, heart failure, COPD, and diabetes. Each condition may require different sensor combinations, alert thresholds, and care team involvement patterns.
Movement quality and subtle functional changes represent common monitoring targets across neurological conditions, suggesting potential for shared monitoring approaches with condition-specific customization.
Research into federated learning approaches could enable system improvement through shared learning while maintaining local data control. This addresses both privacy concerns and limited data challenges for rare events and behaviors while enabling continuous system enhancement across diverse populations and settings.
Personalized monitoring sensitivity and specificity optimization represents a promising research direction. Our findings revealed significant individual variation in optimal alert thresholds, suggesting potential for adaptive algorithms that learn individual baseline patterns and continuously optimize monitoring parameters.
Multi-modal fusion system optimization requires continued research into sensor combination selection, fusion algorithm development, and context-adaptive sensing approaches. Our findings demonstrate that integrated approaches consistently outperform single-modality systems, indicating particularly fruitful directions for technical advancement.
Research should focus on determining optimal sensor combinations for different target applications and user groups, balancing monitoring effectiveness with user burden and implementation complexity. Context-adaptive sensing that automatically adjusts monitoring intensity based on user state and environmental conditions represents an important frontier for improving both effectiveness and acceptance.
Another limitation relates to the evolving nature of the technology itself. During the 24-month follow-up, hardware and software updates were introduced that, while modest, may have contributed to variability in system performance and user experience. Although standardized protocols and sensitivity analyses minimized these effects, future research should explicitly investigate the impact of technology evolution, including structured versioning analyses, to assess how updates influence both technical and clinical outcomes.
In summary, the dedicated subsections on healthcare policy, value-based care integration, and regulatory harmonization collectively highlight the pathways through which our framework can transition from experimental deployment to systemic adoption. By aligning with current health system reform priorities and addressing regulatory barriers, these considerations ensure that the proposed model is positioned not only as a technological advance but also as a practical tool for sustainable healthcare transformation.
Conclusion
By reporting wonderful results of AI-based monitoring systems for elderly people and stroke survivors, the study has achieved multifactorial benefits The implementation of an integrated monitoring approach has reported significant improvements in safety outcomes including a 42% decrease in fall-related injuries (p < 0.001), 37% decrease in Emergency Department visits (p < 0.001) and 29% decrease in unplanned hospitalization (p < 0.008) compared to usual care. Functional outcomes showed 22% greater gains in functional independence measures in stroke survivors at 6 months (p < 0.001) and following that at 24 months.
Our multi-sensor detection showed superior performance over single-sensor-based systems in technical performance with very strong fall detection results (sensitivity: 94.8%, specificity: 96.2%) and activities recognition over various settings (mean accuracy: 91.4%). The fusion architecture was critical in ensuring monitoring reliability in real-world conditions as it was capable of adapting dynamically to changes in the environment and the loss of sensors.
The qualitative findings showed the users had a predominantly positive experience. 92% of care recipients claimed to feel more secure and 84% feel more independent. The caregiver burden score reduces by 33.3% (p < 0.001) and sleep quality improve in addition with beneficial effects on self-efficacy. Healthcare providers reported that they were more efficient in assessments and had opportunities for earlier intervention that translated into measurable improvements in clinical outcomes.
Findings indicated that the integrated monitoring approach employed within the study, despite the technology-related costs being higher than usual care options, results in net savings of $15,311 per participant over 24 months. These savings primarily relate to reductions in healthcare utilization and caregiver burden. The incremental cost-effectiveness ratio was $28,372 per quality-adjusted life year – well within usual willingness-to-pay thresholds.
Implementation research has outlined the factors that affect whether a newly developed system is deployed in various care settings. Of all the factors assessed, the five with the strongest relationship to deployment outcomes were leadership engagement, technical infrastructure readiness, staff training comprehensiveness, user involvement in configuration decisions and availability of ongoing technical support. Our implementation assessment tool and site readiness guidelines were shaped by these findings.
The article provides explanations and examples of key concepts within the framework of technology. To begin with, our integrated monitoring framework is conceptually more advanced than dedicated monitoring solutions, as it shows how different sensing modalities and analysis techniques can be integrated into an overall system with capabilities to address multiple care needs and adapt to people's individual requirements and preferences.
Furthermore, we have conducted a multi-site longitudinal implementation study; the outcome of this work provides unprecedented evidence of AI-based monitoring in real-world settings. The 24-month follow-up period provides insights into how long the interventions are adopted and how outcomes change over time, which is not achievable in shorter studies. Thus, this addresses an important gap in the existing evidence.
Third, our ethical framework for responsible monitoring deployment moves beyond technical privacy safeguards to account for human dimensions of monitoring acceptance, autonomy preservation, and preference accommodation. This broad method for ethical application provides a model for responsible innovation that other researchers and developers can tailor for various monitoring contexts.
Our comparative effectiveness analysis provides the first robust evidence base comparing advanced integrated monitoring against both basic monitoring and usual care across clinical, functional, experiential and economic domains. Such an evaluation helps to make investment monitoring decisions on the basis of many outcome considerations rather than technical functionality.
Ultimately, we provide practical tools that bring our research findings to life. These include readiness assessment tools, configuration guidelines, training materials and sustainability strategies. These implementation resources help bridge the gap between research prototypes and clinical implementations.
While this research fills a number of important gaps, there are still questions left for the future. To improve monitoring efficiencies and user acceptance through reducing false alarm rates while maintaining clinically relevant alerts, future studies on personalization algorithms that adapt monitoring parameters automatically to individual baseline patterns and contextual factors should be emphasized.
Additionally, exploring advanced fusion approaches through emerging sensing modalities can enhance monitoring capability and address the remaining barriers of user acceptance in terms of wearability and smartly managing privacy. This meant utilizing radar-based vital sign monitoring, acoustic sensing beyond voice analysis, ambient electromagnetic field disturbance sensing continued.
Examining how monitoring systems can be designed to better support behavioral change, rather than just the detection of problems, represents an important frontier. Blending motivational design, personalized goal setting, and adaptive feedback mechanisms could turn monitoring systems from passive surveillance tools into active health promotion platforms.
In addition, studies on the monitoring of other vulnerable populations such as those with developmental disabilities, neurodegenerative diseases, psychiatric disorders could yield similar benefits for these populations by developing appropriate sensing approaches and analytic models that suit their needs.
We could explore federated learning approaches that enable algorithmic improvements while preserving privacy, through lack of collection of data in centralized locations. This may overcome the issue of privacy while working with limited training data on rare and uncommon events and behaviors. These approaches can enhance the monitoring performance, while also safeguarding data privacy for all users.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076251384834 - Supplemental material for AI-enabled multimodal monitoring for enhanced safety and functional recovery in elderly and post-stroke care: A mixed-methods study
Supplemental material, sj-docx-1-dhj-10.1177_20552076251384834 for AI-enabled multimodal monitoring for enhanced safety and functional recovery in elderly and post-stroke care: A mixed-methods study by Wenxing Xue, AIxu Duan, YanHua Zhao, Hongmei Zuo and Haytham F Isleem in DIGITAL HEALTH
Footnotes
Ethics approval and consent to participate
All methods were performed in accordance with relevant guidelines and regulations. The experimental protocols were reviewed and approved by the Ethics Committee of the corresponding author's institutions. Written informed consent was obtained from all participants prior to their inclusion in the study, ensuring their voluntary participation and understanding of the research objectives.
Authors’ contributions
Conceptualization, Project administration, funding acquisition, supervision, writing review-editing, methodology, resources, AD; Data curation, formal analysis, investigation, validation, visualization, writing review-editing, software, H.F.I.; Conceptualization, writing original draft preparation, visualization, W.X., AD, Y.Z., H.Z. This manuscript has been read and approved by all authors.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Project Title: Instructional Design and Research on Ideological and Political Education in the Community Nursing Curriculum Based on the Narrative Education Model. Project Title: Instructional Design and Research on Ideological and Political Education in the Community Nursing Curriculum Based on the Narrative Education Model. Project Source: Shanxi Datong University. Project Number: XJG2022217.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data presented in this study are available on request from the corresponding author.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.