
Abstract
Background
Information asymmetry remains a critical challenge in doctor–patient relationships. Although the adoption of eHealth technologies has substantially improved patients’ access to medical information, the extent of these benefits largely depends on individuals’ levels of eHealth literacy. This study aims to investigate the association between inpatients’ eHealth literacy and doctor–patient relationships, while exploring the mediating role of eHealth utilization and the moderating effect of age.
Methods
In 2023, a cross-sectional study was conducted among 1307 inpatients, selected through simple random sampling from three tertiary hospitals in Jinan, Shandong Province, China. The Patient–Doctor Relationship Questionnaire-9 (PDRQ-9) was employed to assess the quality of doctor–patient relationships, while the eHealth Literacy Scale was used to evaluate participants’ levels of eHealth literacy. Stepwise and bootstrap tests were applied to examine the mediation effect, and hierarchical regression analysis combined with bootstrap testing was used to assess the moderating role of age.
Results
eHealth literacy was significantly positively correlated with eHealth utilization (β=0.150, p < .001). A significant negative correlation was found between eHealth utilization and PDRQ-9 scores (β = −0.270, p < .001). eHealth utilization acted as a significant suppressor between eHealth literacy and doctor–patient relationships (indirect effect = −0.040, 95% CI [−0.061, −0.022] direct effect = 0.076, 95% CI [0.028, 0.124]). In adults aged 18–59, eHealth utilization played a partial mediating role (indirect effect = 0.333, 95% CI [−0.055, −0.011] direct effect = 0.192, 95% CI [0.129, 0.255]). In older adults aged 60 and above, eHealth utilization played a complete mediating role (indirect effect = −0.038, 95% CI [−0.071, −0.001] direct effect = −0.051, 95% CI [−0.130, 0.027]). Compared to the inpatients under 60 years old (effect = −0.022, 95% CI [−0.045, −0.001]), the negative effect of eHealth utilization on PDRQ-9 scores was more evident in inpatients aged 60 and above (effect = −0.70, 95% CI [−0.103, −0.040]).
Conclusion
Bridging the digital divide among elderly patients is essential for mitigating information asymmetry and promoting more harmonious doctor-patient relationships.
Keywords
Introduction
The doctor–patient relationship plays a pivotal role in enhancing the quality of medical care and is closely associated with patient's treatment outcomes. 1 It is generally defined as the unique therapeutic interaction between doctors and patients throughout the course of medical care.2,3 With the growing emphasis on patient rights and self-awareness, 4 patients are increasingly seeking active participation in treatment decisions and greater psychological comfort. 5 Inpatients, who generally suffer from more severe or complex conditions than outpatients, engage in more prolonged and frequent interactions with their doctors. 6 These patients often experience elevated levels of anxiety, sadness, and depression, 7 which can pose substantial challenges to maintaining a healthy doctor–patient relationship. 8 Prior research has identified a variety of factors that differentially influence the doctor–patient relationship. 9 Positive influences include patient satisfaction with medical consultations, 10 the frequency and quality of doctor–patient communication 11 and patients’ health literacy. 12 Conversely, negative impacts may arise from language barriers, 13 violent behavior toward doctors 14 and information asymmetry between doctors and patients. 15 In recent years, there has been increasing emphasis on the doctor-patient relationship as an epistemic collaboration. 16 Effective communication not only enhances patient satisfaction but also contributes to improved health outcomes. 16 Despite the information asymmetry between doctors and patients is an inherent characteristic of the medical market, this collaborative perspective recognizes patients’ knowledge and experiences as valuable complements to clinicians’ expertise. 17 The quality of doctor–patient relationships is ultimately manifested through patients’ perceived health benefits and treatment adherence. As the direct recipients of healthcare services, patients’ subjective experiences constitute core indicators of relational quality. 18 From the patient perspective, subtle communication barriers—often imperceptible to medical professionals—thus providing critical access points for optimizing information exchange and enhancing mutual understanding.
Information asymmetry refers to the unequal access to critical information between parties involved in a transaction or cooperative relationship, resulting in adverse selection or other suboptimal outcomes. 19 In the context of healthcare, the information asymmetry between doctors and patients is a defining feature of the healthcare service market, reflecting the disproportionate distribution of medical knowledge between the two. 20 eHealth, which encompasses remote diagnosis and treatment, health information consultation, disease screening and health management, 21 has established new communication channels between doctors and patients 22 thereby partially mitigating the effects of information asymmetry. 23 Studies have revealed that online interaction models provide scalable and cost-effective options for individuals with limited or no access to mental healthcare, while also freeing doctors from routine tasks to focus more on the doctor–patient relationship. 24 Notably, as an emerging diagnostic and treatment paradigm, telemedicine has demonstrated significant potential to enhance trust by improving the exchange of information between patients and doctors. 25 However, eHealth utilization can also negatively impact doctor–patient relationships due to concerns related to data privacy, ambiguity in professional responsibility and increased costs.26,27
Health literacy refers to the extent to which individuals possess the capacity to obtain, process and comprehend basic health information and services necessary for making appropriate health decisions. 28 It forms the foundation of eHealth literacy, which constitutes its digital extension. 29 In the context of the internet era, patients’ eHealth literacy denotes the capacity to seek, access, comprehend and evaluate health information from electronic sources to address health issues, thereby exerting a significant influence on the dynamics of doctor–patient relationships. 30 Without this capability, individuals are at risk of marginalization, inefficiency or compromised rights within an increasingly digitalized healthcare landscape. 31 Existing research has predominantly focused on younger populations, generally indicating a positive correlation between eHealth literacy and doctor–patient relationships,32,33 as well as a similarly positive association with eHealth utilization.34,35 However, the specific impact of eHealth utilization on doctor–patient relationships remains inconclusive. While some studies highlight its positive role in promoting communication and trust,36,37 others raise concerns about potential negative effects, such as depersonalization, diminished empathy and exacerbated technical barriers.38,39
The advancement of eHealth technologies has profoundly reshaped patient engagement in healthcare interactions. 40 However, age-related technological gaps generate digital divides, thereby impeding equitable access to healthcare. 41 Younger populations tend to exhibit higher eHealth literacy competencies and actively employ digital tools to enhance self-care practices and communications, 42 whereas older adults often demonstrate lower eHealth literacy and reduced eHealth utilization, primarily due to barriers such as technophobia, a preference for traditional care and cognitive or physical limitations. 43 These age-driven disparities in both eHealth literacy and utilization not only exacerbate existing healthcare access inequalities but may also impact doctor–patient relationships. 44 Nevertheless, prior studies have predominantly treated age as a mere control variable or focused exclusively on the behaviors of either younger or older adults. 45 This study sampled both older and younger adults within the same research settings to investigate whether the mediating role of eHealth utilization between eHealth literacy and doctor–patient relationships varies by age, while further examining age as a moderating variable to explore its underlying mechanisms through which it may influence this relationship. Regarding research subjects, this study focused on inpatients, who generally present with more complex medical conditions and engage in more frequent and prolonged interactions with healthcare providers than outpatients. This inpatient-centered approach offers a novel perspective for investigating doctor–patient relationships. From a theoretical standpoint, most existing literature emphasizes the direct effects of eHealth literacy on doctor–patient relationships, while neglecting the mediating role of behavioral pathways. 46 This study highlights the mediating role of eHealth utilization, thereby revealing the bridging function of behavioral pathways between eHealth literacy and doctor–patient relationships.
Methods
Data source
This study conducted a quantitative cross-sectional survey and was carried out in three representative tertiary hospitals located in Jinan, Shandong Province, China. Hospital A has been recognized as a “Shandong Province Internet Hospital” and has taken the lead in implementing a nationwide cross-provincial online medical insurance settlement service. Hospital B offers online preconsultation, medication guidance and psychological counseling, and has established dedicated positions for internet-based physicians. Hospital C provides an “Internet + Nursing Service,” enabling patients to schedule high-quality and convenient home nursing services online. The research was carried out from June to October 2023, employing a simple random sampling method. The recruitment of participants was conducted by interviewers who randomly selected inpatients from wards during their hospital internship period, with one patient chosen per ward. Questionnaires were administered after obtaining informed consent. Initially, 1330 participants were surveyed. After excluding missing values in the Patient–Doctor Relationship Questionnaire-9 (PDRQ-9) and participants aged 15–17 years, the final sample comprised 1307 individuals. All questionnaires were administered through face-to-face interviews to ensure data accuracy and quality control. Inclusion criteria targeted inpatients aged 18 years and older who were conscious, capable of effective communication, and able to independently complete the interview process. Exclusion criteria applied to inpatients admitted for accidental injuries, obstetric conditions, severe comorbidities or cognitive impairments that hindered their ability or willingness to participate. Detailed reasons for exclusion are provided in the supplementary materials.
Sampling methods
The sample size for simple random sampling was calculated using the following formula:

Z is the critical value corresponding to the confidence level, p is the proportion of eHealth utilization among surveyed patients, δ is the allowable sampling error, and α is the significance level. At a 95% confidence level with an allowable sampling error δ set to 3%, the required sample size was approximately 1000. By setting p = .5, α = .5, Z = 1.96, δ = 3%, the required sample size at a 95% confidence level with a 3% sampling error was calculated to be 1034.
Measurement of doctor–patient relationship
Compared with other measurement tools, the PDRQ-9 quantifies patients’ emotional experiences regarding their doctor's care, empathy, understanding and acceptance. Unlike instruments that primarily focus on behavioral or transactional aspects, the PDRQ-9 captures patients’ deeper psychological perceptions within the doctor–patient interaction. 47 The advantages of the PDRQ-9 are multifaceted. First, the original PDRQ-9, developed by Van der Feltz-Cornelis et al., 48 evaluates doctor–patient relationships from the patient's perspective, aligning perfectly with the survey subjects of this study. Second, the Chinese version of the PDRQ-9 by Wang et al. has demonstrated strong reliability and validity among inpatients in Chinese general hospitals. 49 Third, the PDRQ-9 typically consists of concise and straightforward questions, making it easy for patients to comprehend and complete. The PDRQ-9 comprises nine items, each rated on a 5-point Likert scale, with total scores ranging from 9 to 45, where higher scores indicate more positive perceptions of the doctor–patient relationship. 50 These characteristics confer high operational practicality, enabling efficient collection of patient feedback in real-world clinical settings. In this study, the Cronbach's alpha coefficient for the PDRQ-9 was 0.972, and the validity test of the PDRQ-9 showed an average variance extracted (AVE) value of 0.794.
Measurement of eHealth literacy
Compared with other measurement tools, the eHealth Literacy Scale (eHEALS) effectively captures key dimensions of health behavior in the digital era. 51 Regarding the advantages of the eHEALS: On one hand, it was specifically designed to assess an individual's ability to access, comprehend, evaluate, and apply health information in an electronic health environment, thereby offering precise measurement of eHealth literacy in contexts relevant to digital health and health communication. 52 On the other hand, the original eHEALS was developed by Cameron D Norman and Harvey A Skinner. 53 This study employed the Chinese version of the eHEALS, adapted by Guo et al., which has demonstrated strong reliability and validity across diverse populations in China. 54 The adaptation of terminology in the localized version ensured that question phrasing aligned with Chinese cognitive patterns, and examples of digital health information sources were replaced with platforms commonly used in China (e.g. WeChat, Dingxiang Doctor). While the original version was designed as a unidimensional scale, the adapted Chinese version comprises three dimensions: application ability of online health information and services (Items 1–5), critical evaluation ability (Items 6–7), and decision-making ability (Item 8). The scale contains a total of eight items, each rated on a 5-point Likert scale ranging from “strongly disagree” (1 point) to “strongly agree” (5 points), consistent with the original version. Total scores range from 8 to 40 points, with higher scores indicating better eHealth literacy.53,54 Its concise and user-friendly design improves user acceptance and facilitates application in empirical research.55,56 In this study, the Cronbach's alpha coefficient of the eHEALS was 0.975, and the validity test showed an AVE value of 0.819 for each dimension.
Measurement of eHealth utilization
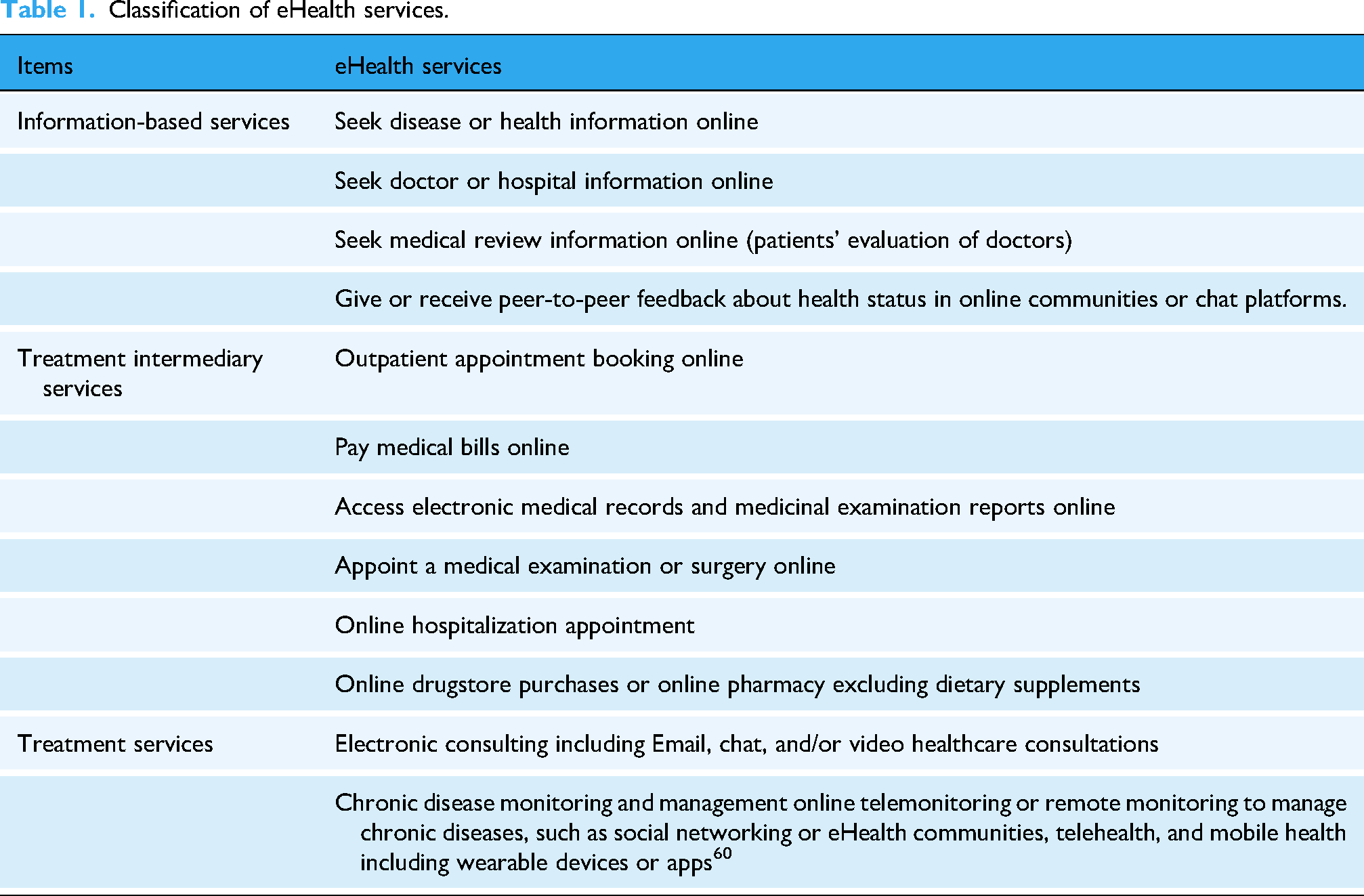
eHealth services refer to information and communication technologies and their practical applications that support and enhance various aspects of healthcare, including health promotion, disease prevention, diagnosis, treatment, monitoring and lifestyle management through digital solutions. 57 Following the stages of the patient journey, 58 these 12 services were categorized into three types: information-based eHealth services, treatment intermediary services and treatment services, as detailed in Table 1. Drawing upon the framework established by Mijke Rhemtulla et al., each item was scored 1 point, with the total score for eHealth utilization ranging from 0 to 12. 59 Higher scores indicated greater engagement with eHealth services.
Classification of eHealth services.
Control variable
The control variables included gender (0 = male, 1 = female), age (0 = under 60 years old, 1 = 60 years old and above), marital status (0 = unmarried, 1 = married), educational level (1 = primary school, 2 = junior high school, 3 = high school, 4 = above high school), place of residence (0 = urban, 1 = rural), subjective economic status (1 = relatively poor, 2 = average, 3 = relatively wealthy), 61 whether to suffer from chronic diseases (0 = yes, 1 = no), whether anxious (1 = none, 2 = slightly, 3 = moderate, 4 = severe, 5 = extremely severe), 62 subjective health status (1 = very poor, 2 = poor, 3 = average, 4 = good, 5 = very good), 63 whether to have commercial medical insurance (0 = no, 1 = yes), social support, outpatient expenses amount (log-transformation), and outpatient waiting time (log-transformation).
Statistical analysis
In Stata 18.0, one-way analyses were conducted using the Wilcoxon rank-sum test and the Kruskal–Wallis test. Spearman correlation analysis was employed to examine the relationships among eHealth literacy, eHealth utilization and PDRQ-9 scores in inpatients. To investigate whether the effect of eHealth literacy on PDRQ-9 scores was mediated by eHealth utilization, stepwise and bootstrap analyses were performed using the SPSS-Hayes PROCESS 3.3 macro. Furthermore, hierarchical regression and bootstrap tests were also applied to assess the moderating role of age in the relationship between eHealth utilization and PDRQ-9 scores.
Mediation analysis was conducted to explore the underlying mechanism through which eHealth literacy influenced doctor–patient relationships, with eHealth utilization tested as a potential mediator. 64 The total effect represented the direct impact of eHealth literacy on doctor–patient relationships without considering eHealth utilization. Upon introducing eHealth utilization as a mediator, the effect was partitioned into the direct effect (eHealth literacy's unmediated influence) and the indirect effect (mediated through eHealth utilization), with the total effect equaling their sum. Mediation analyses were performed for the full sample as well as for age subgroups, including elderly and adult populations. To further investigate age-related variations, a moderated mediation model was applied, incorporating age as a moderator to assess whether the mediating role of eHealth utilization in the relationship between eHealth literacy and doctor–patient relationships differed across age groups. 65
The stepwise testing procedure for mediation analysis was conducted as follows. First, the significance of the effect of eHealth literacy on eHealth utilization was tested. Second, the significance of the effect of eHealth literacy on PDRQ-9 scores was investigated. Third, the effect of eHealth utilization on PDRQ-9 scores was assessed. Fourth, the direct effect of eHealth literacy on PDRQ-9 scores was evaluated. The mediation effect was considered statistically significant if the 95% confidence interval derived from bootstrap testing excluded zero.
A bootstrap test was employed to examine the significance of the effect of eHealth literacy on eHealth utilization, confirming the robustness of the mediating path. Additionally, regression analysis of PDRQ-9 scores on eHealth literacy, eHealth utilization, age and the interaction between eHealth utilization and age were conducted, with the significance of the coefficients tested accordingly.
Results
Descriptive analysis
Following the exclusion of participants with missing PDRQ-9 data and those aged 15–17 years, the final analysis sample comprised 1307 individuals. Table 2 presents the descriptive statistics of the sample along with the results of univariate analyses. The findings reveal that patients aged ≥60 years exhibited lower levels of eHealth literacy and eHealth utilization compared to those aged 18–59. Higher education attainment was positively associated with both higher eHealth literacy and eHealth utilization. Patients with better subjective health status demonstrated higher eHealth literacy and greater engagement with eHealth services. Additionally, compared with patients without chronic diseases, those with chronic conditions exhibited poorer doctor–patient relationship scores. Regarding anxiety, individuals without anxiety reported the highest doctor–patient relationship scores, whereas patients with slightly, moderate, severe, or extremely severe anxiety demonstrated progressively lower scores.
Results of univariate analysis.
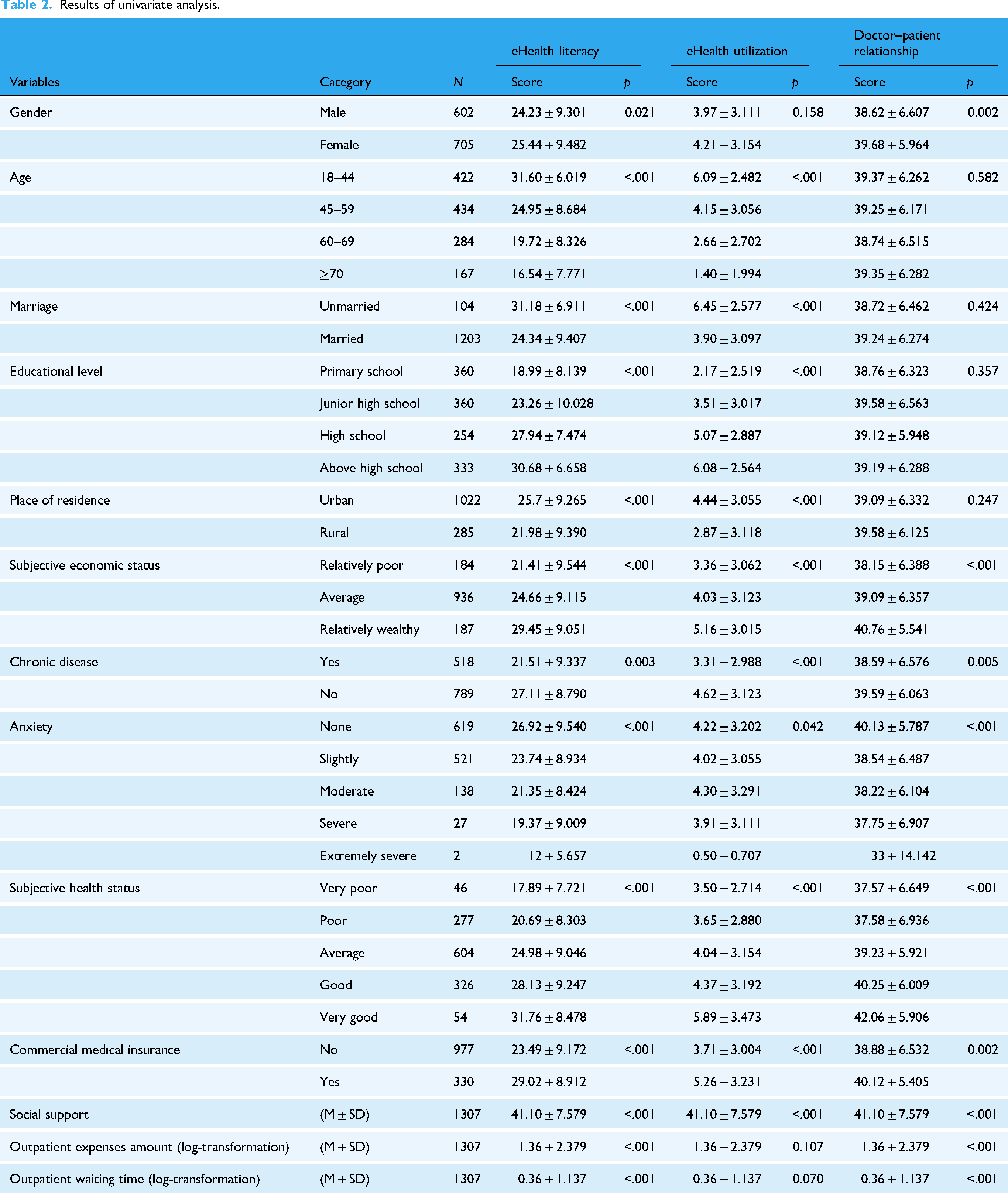
Table 3 presents the descriptive statistics and univariate analysis results stratified by age group, specifically comparing adult and elderly samples. Analysis of adults aged 18–59 showed that 79.32% resided in rural areas, while 20.68% lived in urban areas. None of the participants in this age group reported experiencing severe anxiety. The largest proportion of adults reported “average” subjective health status (45.21%). Additionally, 29.21% of adults were covered by commercial medical insurance. The average social support score was 42.46 (±7.23). The average log-transformed outpatient expenses were 1.08 (±2.16). The average log-transformed outpatient waiting time was 0.23 (±0.65) hours. In contrast, among elderly patients aged 60 and above, 49.45% had attained only a primary school education, and the largest proportion (46.23%) reported “moderate” levels of anxiety. The average log-transformed outpatient expenses were higher at 1.88 (±2.68). The average log-transformed outpatient waiting time was also longer at 0.61 (±1.69) hours.
Results of univariate analysis by age group.

Note: PDRQ-9: Patient–Doctor Relationship Questionnaire-9; Z: Wilcoxon rank-sum test; ρ: Spearman correlation analysis; H: Kruskal–Wallis test.
Mediation analysis
Appendix Table 1 presents the correlations among eHealth literacy, eHealth utilization and doctor–patient relationships in inpatients. The Variance Inflation Factor (VIF) test confirmed the absence of multicollinearity, with all independent variables exhibiting VIF values below 10. Bootstrap testing with 5000 iterations confirmed significant mediation effects, with 95% confidence intervals excluding zero.
Appendix Figure 1 illustrates the mediation effect model among eHealth literacy, eHealth utilization and doctor–patient relationships. In this model, coefficient

The mediating effect results among samples aged 18 years and above.
As shown in Figure 2, among adults aged 18–59, eHealth literacy was positively associated with eHealth utilization (β = 0.139, p < .001), and with doctor–patient relationships (β = 0.192, p < .001). Conversely, eHealth utilization was negatively associated with doctor–patient relationships (β = −0.239, p < .05). These findings suggest that eHealth utilization partially mediated the relationship between eHealth literacy and doctor–patient relationships in this age group.
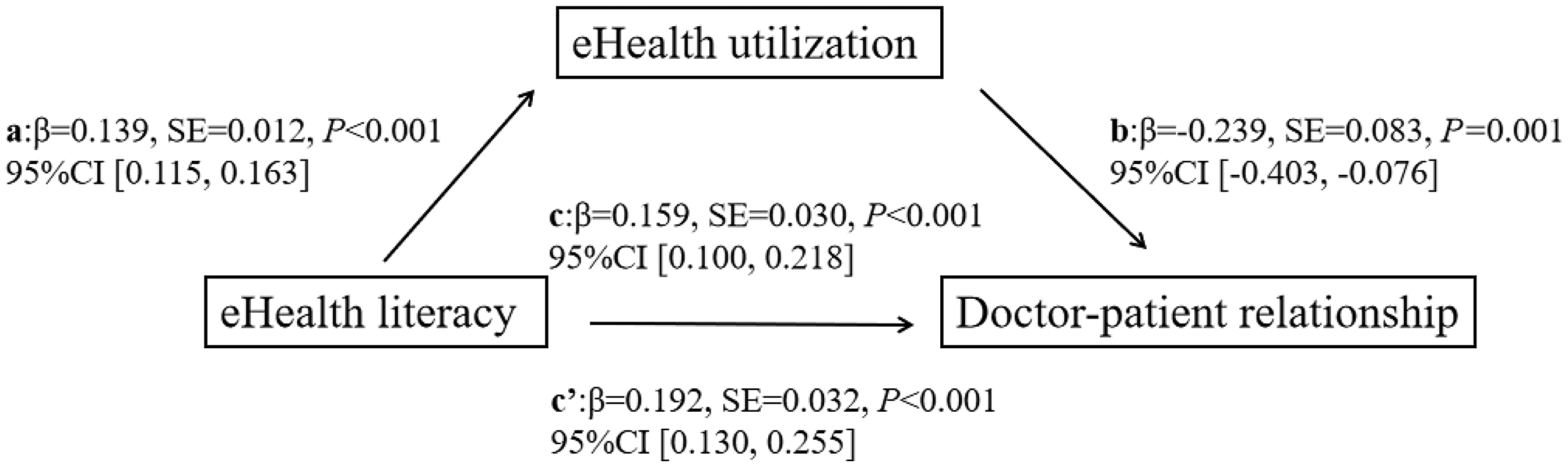
The mediating effect results among samples aged 18–59 years.
Figure 3 results showed that among elderly adults ≥ 60 years, eHealth literacy was positively associated with eHealth utilization (β = 0.129, p < .001). However, no significant correlation was observed between eHealth literacy and doctor–patient relationships. In contrast, eHealth utilization was negatively associated with doctor–patient relationships (β = −0.299, p < .05). These findings indicate that eHealth utilization fully mediated the relationship between eHealth literacy and doctor–patient relationships in the elderly population.

The mediating effect results among samples aged 60 years and above.
As shown in Figures 4 and 5, a supplementary analysis was conducted by stratifying the sample according to the presence of chronic diseases. The results revealed that the negative association between eHealth utilization on doctor–patient relationships was significantly attenuated among patients with chronic diseases (β = −0.240, p = .051) compared with those without chronic diseases (β = −0.299, p < .001). Moreover, the indirect effect of eHealth literacy on doctor–patient relationships through eHealth utilization (β = 0.153, p < .001) was significant only in the nonchronic disease group.

The results of the analysis of mediating effects among chronic patients.

The results of the analysis of mediating effects among nonchronic patients.
Moderation analysis
Appendix Table 2 illustrates the moderating effect of age on the relationship between eHealth utilization and doctor–patient relationships. As shown in Table 4 and Figure 6, age significantly moderated the relationship between eHealth utilization and PDRQ-9 scores, with differential effects observed across age groups. Specifically, among inpatients under 60, eHealth utilization exhibited a modest mediating effect on the relationship with PDRQ-9 scores (Effect = −0.149, Boot SE = 0.080, 95% CI [−0.307, −0.008]). In contrast, for those aged 60 and above, the mediation effect was more substantial (effect = −0.465, Boot SE = 0.117, 95% CI [−0.695, −0.235]).

Moderating effects of age on eHealth utilization and the doctor–patient relationships.
The conditional indirect effect of age in eHealth literacy and the doctor–patient relationship.

Note: ***p < .001, *p < .1.
Discussion
Main findings
This study investigates the association between eHealth literacy and doctor–patient relationships among inpatients, with a particular focus on the mediating role of eHealth utilization and the moderating effect of age. The findings reveal a significant positive association between eHealth literacy and doctor–patient relationships, aligning with the results reported by Luo et al. 66 This finding suggests that individuals with higher eHealth literacy often possess stronger communication skills and cognitive abilities—traits that inherently facilitate positive and effective doctor–patient relationships. 67 Patients with higher eHealth literacy are more likely to develop a preliminary understanding of their health conditions, 68 enabling them to articulate symptoms more accurately and comprehend medical advice more effectively. Such preparedness fosters mutual trust and collaboration, thereby strengthening the doctor–patient relationship. 69 Furthermore, elevated eHealth literacy contributes to better patient adherence to treatment regimens and medical recommendations, 70 which not only supports better health management but also reduces the risk of misunderstandings and potential conflicts between patients and doctors. 71 Collectively, these findings underscore the critical role of improving eHealth literacy in fostering better doctor–patient relationships.
Consistent with prior study by Sjöström A et al., 72 the present study confirmed a positive association between eHealth literacy and eHealth utilization. On one hand, as research results show, patients with higher educational attainment have both greater eHealth literacy and higher eHealth utilization scores. Patients with elevated eHealth literacy demonstrated enhanced capabilities in seeking, comprehending and evaluating online health information critically, 53 enabling them to avoid misinformation interference, thereby improving both the efficiency and confidence of eHealth utilization. 73 On the other hand, as evidenced by the study, individuals with better subjective economic status are more likely to possess higher eHealth literacy and higher eHealth utilization. Individuals with elevated eHealth literacy exhibit a stronger sense of personal responsibility for health management. 74 They demonstrate familiarity with and preference for adopting teleconsultation platforms and health monitoring apps to address health concerns, as evidenced by practices such as synchronizing health data through wearable devices, remote monitoring of diabetes and online vaccine appointment scheduling.75,76
This study indicated that eHealth utilization exhibits a significant negative correlation with doctor–patient relationships across both age groups, aligning with findings from Hill JH et al., 77 but inconsistent with the research by Carini E et al. 78 This negative association may be attributable to limitations in information transmission through digital platforms. For instance, teleconsultation may delay doctors’ responses or restrict their ability to capture patients’ nonverbal cues, potentially resulting in misdiagnoses or overlooked symptoms. 79 Additionally, the variable quality of online health information can result in misinterpretation or overinterpretation. When such information conflicts with a doctor's diagnostic advice or guidance, it can undermine patients’ trust and damage the doctor–patient relationships. 80
The adverse effect of eHealth utilization on doctor–patient relationships was particularly pronounced among older adults aged 60 and above. This resulted in a negative direct effect of older adults’ eHealth literacy on doctor–patient relationships. Due to negative attitudes toward technology, cognitive impairments, poorly designed electronic interfaces and limited interest in digital technologies, older adults usually had lower eHealth literacy scores and lower eHealth utilization rate.81,82 Comparative data further supported disparities: Compared to adults with average eHealth literacy scores of 28.23 ± 8.19 and average eHealth utilization scores of 5.10 ± 2.95, whereas elderly individuals demonstrated lower average eHealth literacy scores of 18.54 ± 8.26 and average eHealth utilization scores of 2.19 ± 2.54. In real-world contexts, the eHealth utilization among elderly adults may not necessarily stem from autonomous or informed decision-making. 83 Poor digital communication may exacerbate more negative emotions and erode trust toward doctors during eHealth utilization among older adults, 84 underscoring the need to gather patient's feedback systematically and optimize service design to minimize trust crises caused by misinterpretations in eHealth utilization. 85 Simplifying operational procedures and implementing age-friendly interfaces could further reduce technical barriers from operational complexity and enhance elderly adults’ effective participation in eHealth services. 86
Limitations
This study has several limitations that should be acknowledged. First, as a cross-sectional survey, it precludes the establishment of causal relationships between eHealth literacy and doctor–patient relationships. Second, although the findings provide valuable insights into the experiences of the sampled inpatients, the sample may not fully represent the broader patient population within the region. Consequently, the generalizability of the results should be interpreted with caution and adapted flexibly in diverse clinical or geographical contexts. Third, the study relied exclusively on self-reported data from the inpatient perspective to measure PDRQ-9 scores. However, given that doctor-patient relationships are inherently complex, dynamic and bidirectional, relying on the single perspective of patients may not fully capture their multidimensional nature. Fourth, reliance on self-reported information may introduce recall bias and subjective interpretation, potentially affecting the accuracy and reliability of the findings. Fifth, although using the age of 60 as the threshold for defining elderly in China has a legal basis, within-group differences between newly retired individuals and older seniors may potentially influence the observed effects and warrant careful consideration in future research.
Conclusion
The total effect of eHealth literacy on doctor–patient relationships was not statistically significant. However, after accounting for the mediating effect of eHealth utilization, eHealth literacy became positively related to doctor–patient relationships. Additionally, this study identified age as a significant moderating factor, indicating that the negative impact was more pronounced among older patients aged 60 and above compared to younger counterparts. Furthermore, this research provided empirical evidence challenging the commonly held assumption that eHealth utilization universally improved doctor–patient relationships, emphasizing the necessity of age-specific interventions in healthcare settings to address older adults’ disadvantages in information access and technology usage.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076251384135 - Supplemental material for eHealth literacy and doctor–inpatient relationships: The mediating role of eHealth utilization and the moderating role of age
Supplemental material, sj-docx-1-dhj-10.1177_20552076251384135 for eHealth literacy and doctor–inpatient relationships: The mediating role of eHealth utilization and the moderating role of age by Yi Huang, Wen Wen, Shiju Dong and Jiajia Li in DIGITAL HEALTH
Supplemental Material
sj-docx-2-dhj-10.1177_20552076251384135 - Supplemental material for eHealth literacy and doctor–inpatient relationships: The mediating role of eHealth utilization and the moderating role of age
Supplemental material, sj-docx-2-dhj-10.1177_20552076251384135 for eHealth literacy and doctor–inpatient relationships: The mediating role of eHealth utilization and the moderating role of age by Yi Huang, Wen Wen, Shiju Dong and Jiajia Li in DIGITAL HEALTH
Footnotes
Abbreviations
Acknowledgments:
We are grateful to the internet + medical health survey team for their invaluable contributions to the research.
Ethics approval and consent to participate
This study was conducted in accordance with the Declaration of Helsinki. We adopted the Strengthening the Reporting of Observational Studies in Epidemiology reporting guidelines. The informed consent form was reviewed and approved by Ethics Committee of the School of Public Health, Shandong University, validating the research protocol (Approval No. LL20230602). All participants were fully informed about the purpose, content and confidentiality of the study. Participants indicated their consent by signing the informed consent form and providing their contact information at the beginning of the questionnaire.
Authors’ contributions
W.W. designed the study and revised the manuscript; J.L. and Y.H. drafted and revised the manuscript and participated in the data analysis; S.D. and L.Z. offered revisions to the manuscript. All authors contributed to the data investigation and approved the final manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Humanities and Social Sciences Foundation of Ministry of Education, National Natural Science Foundation of China, and Natural Science Foundation of Shandong Province (Grant Nos. 21YJC630060, 72274108, and ZR2022MG003).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Availability of data and materials
The datasets analyzed during the current study are available from the corresponding author on reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.