
Abstract
Objective
The study aimed to assess the effectiveness of mental health literacy digital awareness campaign, on the levels of social discrimination against mental illness, willingness to seek professional psychological help, and intended future behaviors among high school students in Jordan.
Methods
A one-group pre-test–post-test study design was used, involving 43 high school students. The intervention included posting podcast series and reels through private Facebook groups over 1 month.
Results
The students demonstrated significantly lowered perception of social discrimination (ʌ = 0.35, p < .001), more intended future behaviors (ʌ = 0.08, p < .001), and increased willingness to seek help (ʌ = 0.84, p = .029) over time. The magnitude of these changes was large for social discrimination (Cohen's d = 1.34) and intended behaviors (d = 3.00), and small to medium for willingness to seek help (d = 0.42). Male students (M = 16.3, SD = 2.1) scored significantly lower in willingness to seek help (M = 18.4, SD = 2.6) than females. Those with prior psychological referrals had higher social discrimination (t = 2.47, p = .018).
Conclusion
This study offers school mental health professionals a valuable tool to support high school students through accessible platforms like social media.
Introduction
High school students are challenged to manage their academic pressures, family responsibilities, and psychosocial needs due to the accelerated changes characteristic of adolescence. These developmental changes might contribute to an increased vulnerability to mental health issues including depression and anxiety.1,2 Previous literature has emphasized the significant burden of depression and anxiety which are associated with disability-adjusted life years. In fact, depression and anxiety account for more than 45% of the global burden of disease. 3 This highlights their far-reaching impact on individual well-being, healthcare systems, and the economy. For those at the high school level, addressing these issues is therefore both timely and critical. Notably, half of mental conditions emerges before the age of 14, 4 and three-fourths occur by the age of 24. 5 Despite this, many high school students rely heavily on online resources for health information. 6 However, the quality of these sources can vary widely, which may affect the students’ ability to understand and manage their mental health. In this context, mental health literacy (MHL) is a vital framework for developing school-based mental health interventions.
Universally, schools are recognized as the prime environment for implementing health promotion programs. 7 However, in low- and middle-income countries (LMICs), school-based mental health services are underdeveloped. 8 There is a lack of national mental health initiatives or discussions regarding mental health and illness within school settings. Particularly, in Jordan, this situation is exacerbated by the scarcity of mental health services for children and adolescents, and the lack of psychological counseling services at higher institutions. 9 Instead, children and adolescents get evaluated by non-specialized personnel or primary care providers in primary healthcare centers. 10 Moreover, those professionals are less likely to deal with mental health problems due to stigma. 11 This creates additional barriers to access care and suggests a pressing need to foster early intervention.
MHL is believed to have the potential to bridge the gap between the need for mental health treatment and its availability or accessibility. 12 Currently, MHL refers to the knowledge and skills needed to foster mental health. 13 A wide range of interventions have been developed to improve MHL. Among these are multicomponent community campaigns, structured training courses, and internet-based programs. 14 However, many of these interventions have not been evaluated. 14 In recent years, there has also been a growing demand using online digital platforms within the realm of mental health. 15 Individuals with a higher level of MHL are more likely to recognize early signs of mental health problems, seek help, and engage in self-care. 16 This can facilitate earlier intervention, and potentially prevent the escalation of mental health issues. 14 In contrast, low MHL, cultural beliefs, and heightened stigma inhibit the students from seeking psychological help.11,17 Particularly, students with limited MHL are less likely to either seek or receive treatment for a mental illness. 18 This has been connected to the student's experience of psychological distress and their academic level.12,18 Moreover, students experiencing mental health problems often report feelings of fear, isolation, guilt, and embarrassment. 17 Research indicates that longer delays between the onset of these problems and the time of seeking professional help are linked to poorer outcomes into adulthood. 19 This impacts the student's academic, social, emotional, and behavioral aspects later into adulthood. Furthermore, these impacts may be amplified by the widespread use of social media among this group.
While digital platforms provide support and engagement, they may also be places where discrimination can be reinforced. 20 Studies indicate that the students often prefer self-help strategies rather than professional psychological help and are more likely to seek informal support from friends and family. 21 This raises concerns about the adequacy and reliability of such networks in providing guidance. Coughlan and his colleagues found that individuals are more likely to interact with health-related messages when the content aligns with their values and is delivered through familiar channels. 22 Podcasts, a popular digital intervention, have become particularly appealing to younger populations. 23 This highlights the potential of digital media in delivering mental health content. To enhance the effectiveness of such interventions, evidence supports the incorporation of co-creation and social marketing techniques when designing MHL initiatives for these platforms. 24
To maximize the benefits of these digital strategies, support from school-based professionals is critical. School mental health professionals have the potential to guide students toward accurate digital resources and encourage help-seeking behavior. Understanding the impact of MHL on such behaviors is essential for delivering effective interventions. In Jordan, the Ministry of Education (MoE) mandates the presence of educational counselors in schools to support the student's personal development within the school environment and implement life skills programs. 25 They may also address some emotional and psychological concerns among students. Educational counselors hold at least a bachelor's degree in counseling, mental health, or psychology. Notably, as per the 2024/2025 schools staffing plan, 26 nurses are allocated specifically to specialized vocational schools, which focus solely on vocational tracks. This gap underscores the need for mental health interventions that complement existing support systems in reaching students effectively. In this context, the intervention provides a valuable tool to guide students toward reliable health information and essential mental health resources through accessible platforms like social media.
This study, based on the theory of planned behavior (TPB) proposed by Ajzen, 27 suggests that the MHL digital awareness campaign has the potential to positively impact the intentions and behaviors of high school students in Jordan. The theory has three key components: individual attitude, subjective norms, and perceived behavioral control. These constructs collectively guide individuals’ readiness to perform a given behavior. In the context of this study, the MHL awareness campaign is designed to target each of these components. First, by enhancing students’ understanding of mental health conditions, the campaign aims to improve attitudes toward individuals experiencing anxiety or depression, thereby reducing social discrimination and promoting acceptance. Second, the intervention addresses subjective norms by reshaping perceived societal perceptions where seeking help becomes acceptable and even encouraged among peers. Third, the campaign seeks to strengthen perceived behavioral control by increasing students’ confidence in their ability to seek professional psychological help and engage in an intended future contact with persons experiencing anxiety or depression; without facing social or personal barriers. Collectively, social discrimination, help-seeking intention, and intended future contact behaviors offer a comprehensive assessment of the campaign's effectiveness in influencing both cognitive and behavioral dimensions of mental health engagement among high school students.
The purpose of this study is to assess the effectiveness of the MHL digital awareness campaign, focusing on anxiety and depression, on the levels of social discrimination against mental illness, willingness to seek professional psychological help, and level of intended future behaviors among high school students in Jordan. The research questions of this study are:
What is the effectiveness of the MHL digital awareness campaign focusing on anxiety and depression, on the levels of social discrimination, willingness to seek professional psychological help, and the level of intended future behaviors among high school students in Jordan? What are the differences in the levels of social discrimination, willingness to seek professional psychological help, and level of intended future behaviors in relation to selected sociodemographic characteristics among high school students in Jordan?
Methods
Study design
This is a quasi-experimental pre-test–post-test design with repeated measures over time. Data were collected at three time points: baseline (T1), 1 month post-intervention (T2), and 3 months post-intervention (T3). The study was implemented over 1 month period from June 9 to July 14, 2024, with follow-up assessments extending through mid-October 2024. This approach allowed for the assessment of both immediate and sustained intervention effects.
Sample and setting
The study was conducted in public high schools located in the central region of Jordan. In line with the MoE policy, male and female students attend separate institutions. Accordingly, recruitment and intervention delivery were stratified by sex to ensure cultural appropriateness and feasibility.
Eligible participants were Jordanian high school students aged 15 to 18 who met the following inclusion criteria: (1) had access to an electronic device with internet connectivity to access the proposed digital awareness campaign materials, and (2) had access to Facebook, either through an active account or via linked Meta platforms. Students were excluded if they were: (1) currently undergoing psychological counseling, or (2) enrolled in the 12th grade due to concurrent national exams. The national exam determines their eligibility for university enrollment, which could introduce confounding stress-related variables.
Sample size
Sample size was calculated using G*Power 3.1, targeting the use of repeated measures multivariate analysis of variance (RM-MANOVA) with three within-subject time points (pre, post, and 3-month follow-up). Parameters included: a medium effect size (f = 0.3), α = 0.05 (two-tailed), statistical power = 0.80, and an estimated correlation of 0.5 among repeated measures. The minimum required sample was 39 participants. To compensate for 10% potential attrition, the target recruitment was 50. A final sample of 43 students completed all assessments and were included in the final analysis, exceeding the minimum required sample size.
Recruitment and ethical procedures
Ethical approval for this study was granted from the University of Jordan. Before data collection, formal permissions were granted by the Jordanian MoE, including approvals from its Educational Research and Counseling Departments. Recruitment was coordinated through educational counselors in each participating school. Counselors were briefed on the study objectives and eligibility criteria. Then, they disseminated an informational announcement to eligible students and collected Facebook profile details of those expressing interest. Passive parental consent procedures were adopted in accordance with the MoE regulations. Students who expressed willingness and meanwhile did not receive a signed opt-out were considered to have passive consent to participate in the study. Counselors provided the principal investigator (PI) with a list of student Facebook profiles for eligible participants. Students were invited to join gender-specific private Facebook groups created for the intervention (see Figure 1). Upon joining, students reviewed and electronically signed an informed consent form and were briefed on group rules, including conduct expectations and ethical standards (e.g. zero tolerance for cyberbullying or inappropriate content). Students were informed of their rights to decline or withdraw from participation at any stage without penalty. No participants were excluded for behavioral violations.
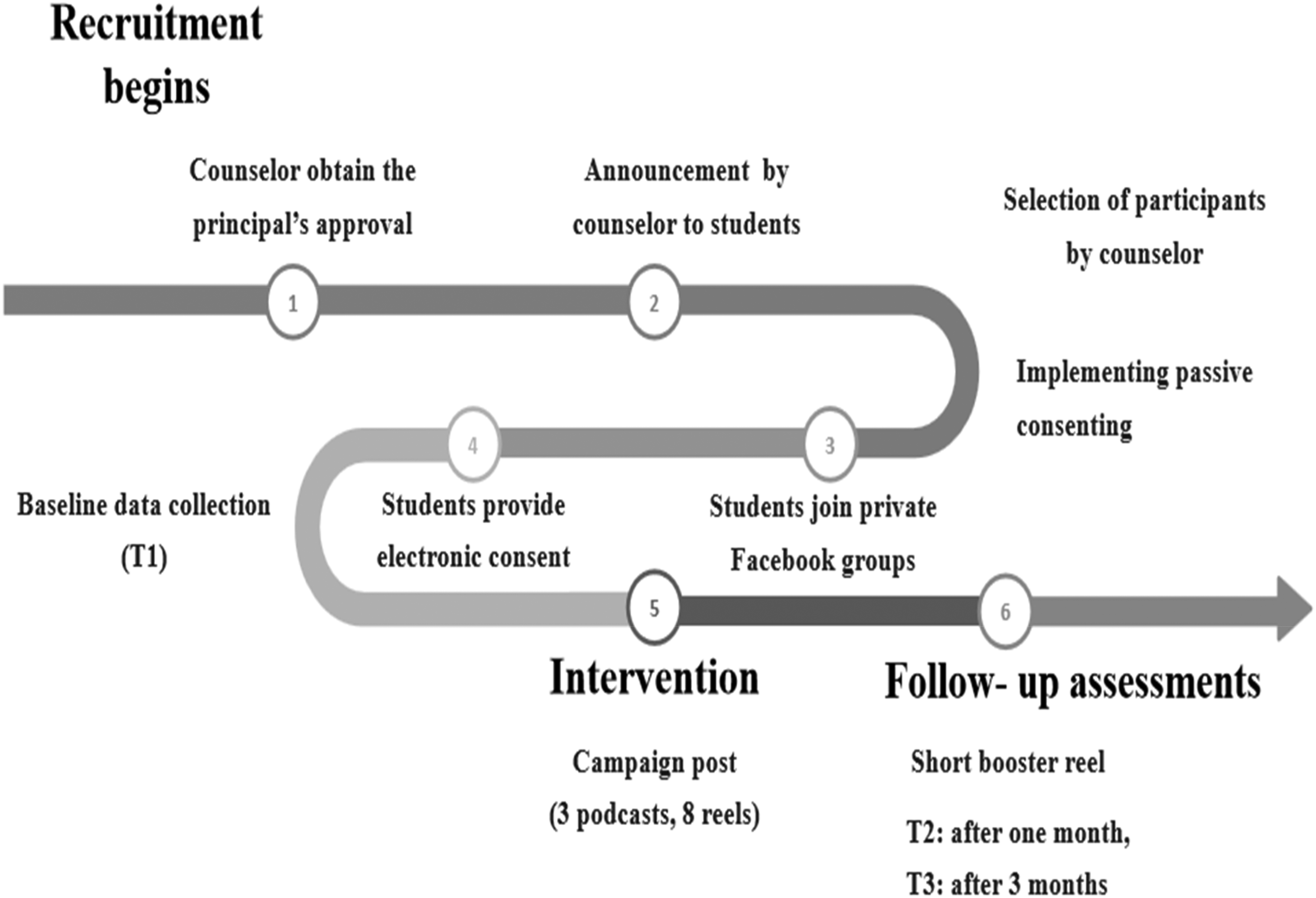
Flowchart representation of the recruitment and data collection.
Study intervention
The intervention consisted of a digital awareness campaign titled “Live it well!”; (عيشها صح!), which included:
A three-podcast series featuring a dialogue between a psychiatric mental health nurse (PI herself), and a consultant in child and adolescent psychiatry. Each episode lasted 20–25 min and addressed key topics in anxiety and depression. The episodes were recorded in a warm, café-style setting, with ambient lighting and gentle background components. This informal style was chosen to appeal to the target audience. A series of short-form vertical video reels (60–90 s). The reels were made visually appealing with the use of filters, effects, and music. The themes were: introduction to mental health, understanding depression, understanding anxiety, breaking-down stigma, connecting to help seeking resources, positive mental health practices, and peer support. The final reel included review and reinforcement of the key messages.
The content was co-created with media and social media specialists, a graphic designer, two camera operators, and a producer. They were also validated by a panel of experts in mental health. The timing, delivery, and thematic structure of the digital campaign were pre-scheduled using a comprehensive content calendar (see the Supplemental file). This calendar details the sequence and type of content delivered, with built-in gender sensitivity and cultural norms. Before dissemination, the materials underwent quality assurance checks to ensure audiovisual clarity and adherence to platform compatibility.
Data collection procedure
At three time points (T1, T2, T3) students completed self-report questionnaires via Google Forms. The links were posted within private Facebook groups created for the study. To maintain anonymity while allowing for longitudinal tracking, each student chose a unique code. Questionnaires were administered in Arabic and optimized for mobile devices to facilitate accessibility. At each data collection point, students were reminded of their rights to voluntary participation and withdrawal. Seven participants withdrew after the baseline (T1) for unspecified reasons. Data were stored in password-protected files accessible only to the PI. No data were extracted from students’ personal Facebook activity. A booster reel was published 3 months after the intervention, coinciding with the T3 data collection point.
Enhancing fidelity of the intervention
To ensure fidelity, the intervention was delivered by a single trained interventionist. A daily activity log was maintained to document the delivery of each session. Additionally, random sessions were reviewed by an independent rater to assess adherence to the intervention protocol. General feedback was also collected from students who received the intervention to gather insights on its delivery and consistency. These measures have been incorporated into the intervention protocol.
Measurement
The data were collected using an Arabic version of adapted self-reporting questionnaires. Two tools were already adopted in Arabic versions (Social Discrimination Scale (SDS), and Attitudes Toward Seeking Professional Psychological Help-Short Form (ATSPPH-SF).11,28 For the other tool, the World Health Organization guide of translation and tool adaptation was used.
29
Initially, a professional expert in psychiatry revised and translated the English form of the questionnaires into Arabic. Then, a bilingual expert was used to identify and resolve the inadequate concepts of the translation, as well as any discrepancies between the forward translation and the previous versions of the items. Then, the instrument was translated back to English by an independent translator, whose mother tongue is English and who has no knowledge of the questionnaire. The two English forms (the original and the translated) were compared in terms of conceptual rather than literal meanings of the items by experts in the field. The instruments were:
Social Discrimination Scale. The adopted version of the Arabic version of SDS was used.
11
Permission was obtained from the authors. The SDS comprised of 18 items where students were asked to make responses on a Likert scale of 5 points from strongly disagree (1) to strongly agree (5). A higher score meant a higher perception of social discrimination. The adoption was in terms of changing the context of the scale from targeted patients with the COVID-19 virus to targeted patients with mental illnesses like anxiety and depression. The scale had good internal consistency with Cronbach's alpha of .88. Reported and Intended Behavior Scale (RIBS).
30
This scale evaluated four distinct domains of reported (items 1–4) and intended (items 5–8) behavior outcomes: living with, working with, residing nearby, and maintaining a relationship with someone who had a mental health issue. For this study, only items 5–8 were used. Items 5–8 were rated on a scale ranging from 5 = “strongly agree” to 1 = “strongly disagree.” The RIBS demonstrated a strong overall test–retest reliability of 0.75, indicating consistency in responses over time. Additionally, the scale exhibited high internal consistency with an overall score of 0.85.
30
Attitudes toward Seeking Professional Psychological Help-Short Form. The original tool was developed by Fischer and Turner,
31
and the short form was later modified.
32
The Arabic version was adopted (ATSPPH-SF).
28
Permission was obtained from the authors. It included 10 items rated on a 4-point Likert scale (3 = Agree, 0 = Disagree), where items 2, 4, 8, 9, and 10 were reverse scored. Scores were then summed together, with higher scores indicating more positive attitudes toward seeking professional help. This tool has been used cross-culturally. The tool had good reliability and validity. It exhibited high internal consistency with an overall score of 0.84 and a strong overall test–retest reliability of 0.74.
28
Sociodemographic characteristics: Age, gender, school grade, history of mental illness in the student's family (parent, relative, or friend), previous referral of participant to a (psychologist/psychiatrist) for psychological problems, sources of information about mental health, and parent's level of education.
Pilot study
Prior to data collection, all questionnaires were pilot-tested with a small sample of students (n = 10) to ensure clarity, comprehension, and cultural appropriateness. No major modifications were required following the pilot test.
Data analysis
The data were analyzed utilizing the Statistical Package for the Social Sciences (IBM-SPSS, Version 27). Descriptive analyses of the data were carried out to determine the means, standard deviation (SDs), frequencies, and percentages of the responses. In addition, the RM-MANOVA test was used to evaluate the difference in social discrimination, willingness to seek professional psychological help, and level of intended future behaviors among the students. Assumptions of normality, homogeneity of variance–covariance matrices, and sphericity (Mauchly's test) were checked. Greenhouse–Geisser corrections were applied when sphericity was violated. Also, t-test for two-independent samples and one-way analysis of variance (ANOVA) were used to examine the difference between students in relation to selected sociodemographic characteristics. Alpha was set to .05.
Results
Sociodemographic characteristics
A total of 43 students represented the sample of the study. Students aged 15–17, with a mean age of 16.4 (SD = 0.7). Table 1 shows the sociodemographic characteristics of the students. Of the students, 37.2% (n = 16) were in the 10th grade, and 62.8% (n = 27) were in the 11th grade. Males constituted 62.8% (n = 27) of the students, whereas the females were only 37.2% (n = 16). Among the 43 students, 23.3% (n = 10) had previous referrals for psychological problems. The majority of the students came from families with educated parents with levels of education ranging between high school and graduate school. Only 7% of the students’ mothers (n = 3), and 18.6% of the students’ fathers (n = 8) were illiterate. Few of the students reported having a history of mental illness in their father (4.7%; n = 2), relative (18.6%; n = 8), and in their friend (9.3%; n = 4). The sources of information on the mental issues normally used by the students were mostly through social media (n = 18) followed by self-readings (n = 11). However, 32.6% (n = 14) reported that they never looked up mental health issues. Interestingly, none (n = 0) used TV or radio as a source of information.
Sociodemographic characteristics of students (N = 43).

Testing the effect of the MHL digital awareness campaign
A RM-MANOVA was conducted (Table 2) to assess the effect of the digital MHL awareness campaign on the levels of social discrimination, willingness to seek professional psychological help, and levels of intended behaviors. The results indicated a significant effect of the intervention on social discrimination scores (Wilk's ʌ = 0.35, F(2,41) = 38.90, p < .001) over time. However, Mauchly's test of sphericity indicated a violation of the assumption of sphericity (W = 0.006, χ2 = 210.25, df = 2, p < .001), and therefore, the Greenhouse–Geisser correction was applied (ε = 0.501, df = 1.003). However, the F value remained significant (F(2,41) = 77.09, p < .001), indicating that time had a significant effect on the student's perception of social discrimination. Interpreting eta-squared suggests that 66% of the variance in social discrimination is explained by the intervention over time. This is considered a large effect, indicating that the changes in social discrimination across the three points of measurement are substantial.
Repeated measure MANOVA analysis for mental health literacy digital awareness campaign on social discrimination, intended behaviors, and willingness to seek professional psychological help among students (N = 43).

MANOVA: multivariate analysis of variance.
Regarding the intended behaviors of the students, the results indicated a significant effect of the intervention (Wilk's ʌ = 0.08, F(2,41) = 214.03, p < .001) over time. However, Mauchly's test of sphericity indicated a violation of the assumption of sphericity (W = 0.44, χ2 = 33.76, df = 2, p < .001), and therefore, the Greenhouse–Geisser correction was applied (ε = 0.64, df = 1.281). However, the F remained significant (F = 375.88, p < .001) indicating that time had a significant effect on the students’ intended future behaviors. An eta-squared of 0.91 infers that the intervention had a strong and meaningful impact on the student's intended behaviors, likely encouraging more favorable mental health behaviors or attitudes.
The results indicated a significant effect of the intervention on the students’ willingness to seek professional psychological help scores (Wilk's ʌ = 0.84, F(2,41) = 3.85, p = .029) over time. However, Mauchly's test of sphericity indicated a violation of the assumption of sphericity (W = 0.41, χ2 = 37.09, df = 2, p < .001), and therefore, the Greenhouse–Geisser correction was applied (ε = 0.627, df = 1.254). However, the F remained significant (F(2,41) = 6.51, p = .009), indicating that time had a significant effect on the student's attitudes and willingness to seek psychological help. While the intervention over time does have an effect, it accounts for only a moderate proportion of the variability in these attitudes.
To quantify the magnitude of these changes, Cohen's d effect sizes were calculated for pre-intervention to first follow-up (T1 to T2) and pre-intervention to second follow-up (T1 to T3). The intervention produced large and sustained effects in reducing social discrimination (d = 1.34 at both T2 and T3) and increasing intended behaviors (d = 3.00 at T2 and 3.18 at T3). The increase in willingness to seek professional psychological help showed a small to medium effect initially (d = 0.42 at T2) that was largely maintained at follow-up (d = 0.37 at T3). These results indicate meaningful and lasting impacts of the digital MHL campaign on students’ mental health attitudes and intended behaviors. Figure 2 summarizes the changes in social discrimination, intended behaviors, and willingness to seek professional psychological help across the three measurement points.

Changes in social discrimination, willingness to seek professional psychological help, and intended behaviors among students over time. Note. T1 = pre-intervention; T2 = 1 month post-intervention; T3 = 3 month post-intervention. Scores reflect mean total scores on each outcome measure across time.
Differences in social discrimination, intended behaviors, willingness to seek professional psychological help regrading sociodemographic characteristics
To examine the differences between the study's dependent variables and dichotomous variables (gender, having a history of father's mental illness, history of referral for psychological help) independent t-test was conducted (see Table 3). The analysis showed that there was a significant difference in scores between gender and attitudes toward seeking psychological help (t = −2.73, p = .009) with equal variances assumed (Levene's test, p ≥ .05). These findings implied that male students (M = 16.3, SD = 2.1) scored significantly lower in their willingness to seek psychological help (M = 18.4, SD = 2.6) than females. This may reflect potential gender barriers, such as societal norms discouraging emotional expression and help-seeking in males.
Differences in social discrimination, intended behaviors, and willingness to seek professional psychological help in relation to selected sociodemographic factors (N = 43).

The analysis showed that there was a significant difference between having a history of previous referral for psychological help and the students’ perception of social discrimination (t = 2.47, p = .018) with equal variances assumed (Levene's test, p ≥ .05). This suggests that individuals with previous referral have higher perceived social discrimination (M = 47.0, SD = 11.5). These mean scores are compared to those without such a history who have lower perceived social discrimination (M = 37.8, SD = 9.9).
Concerning the students’ scores related to their father's history of mental illness, there was no significant difference (p > .05). This suggests that family history may not always directly play a role in shaping individuals’ attitudes toward mental health.
To examine the differences in the variables of the study regarding the sources of information the students use about mental health, one-way ANOVA was conducted. There was no difference between students’ scores related to their used source of information (p > .05). This result suggests that the type of information source (social media, self-reading, or no prior information-seeking) did not have an effect on students’ outcomes.
Discussion
Given young population reliance on digital media as a primary source of information, it becomes essential to create content that promotes healthier mental health-related behaviors. This study found that the MHL digital awareness campaign positively influenced high school students. Specifically, the campaign led to a substantial reduction in social discrimination and a significant improvement in intended future contact behaviors. These changes were supported by large effect sizes, suggesting meaningful behavioral and attitudinal shifts among students. After the intervention, students were more willing to live, work, and continue a relationship with someone with mental health problems. These changes may be explained by the TPB. 27 The campaign likely improved students’ attitudes toward mental health and changed their perceptions of what is socially acceptable. In turn, these shifts may likely increase their intentions to engage in future contact behaviors with individuals affected with mental health problems. The campaign also improved students’ willingness to seek professional psychological help. However, the effect size was moderate. This pattern of limited improvement in help-seeking is consistent with prior research findings.33–35 Similar interventions have shown that while knowledge and attitudes may shift, translating these changes into actual help-seeking behavior remains challenging. More intensive, sustained, or personalized approaches may be needed to achieve meaningful changes in this domain.
The intervention's smaller effect on help-seeking may also reflect persistent gender and cultural barriers. In this study male students reported lower willingness to seek professional psychological help. This is consistent with studies suggesting that societal norms around masculinity may inhibit emotional expression and reduce help-seeking. 36 However, findings in the literature on gender differences remain mixed. Some studies report greater help-seeking tendencies among females, 37 while others show no gender effect. 18 In the Arab context, both males and females tend to link emotional and mental issues with religious and social beliefs. 38 However, when it comes to MHL, findings remain inconsistent. Depression literacy was associated with sex among students in one study, 39 and had no significant effect in another. 40 These mixed results highlight the need for context-specific investigations to clarify how sex differences impact MHL and attitudes across different populations and settings.
A primary contribution of this study lies in demonstrating the feasibility and impact of delivering MHL interventions through digital platforms preferred by high school students. Podcasts and reels offered a medium that was both accessible and engaging for high school students, aligning with their digital consumption patterns. Furthermore, this affected the students’ willingness to seek professional help. Among high school students, social media serves as a source of support, information, and relaxation. 41 This may have made the intervention more engaging and accessible, enhancing its effect. Furthermore, students prefer visual and easily accessible content aligns with their learning preferences. 42 The visually appealing format of videos uploaded to the intervention platform may allow the students to process topics like mental health more effectively and critically assess their attitudes and behaviors toward them. The use of podcasts as digital intervention is particularly appealing to younger populations. 23 The podcast series was tailored to challenge common misconceptions among students and reshape their perceived discrimination attitudes. Although the content and the key messages of the podcast prepared for this study were pre-planned, improvisation played a key role in the conversation, which allowed for spontaneous insights and a more natural flow of dialogue. Importantly, the intervention's content was not only informative but also emotionally resonant, incorporating real-life narratives from mental health settings that likely enhanced students’ empathy and identification with affected individuals. Prior research supports the efficacy of narrative formats in reducing stigma and enhancing mental health knowledge, especially among youth.42,43 Behaviors are facilitated by the person's level of mental health knowledge and attitudes toward mental illnesses. 44
Students with a history of referral for psychological help demonstrated higher perceptions of social discrimination compared to those without a referral history. This suggests that prior exposure to mental health services may be associated with negative experiences that might contribute to feelings of stigmatization or reinforce existing perceptions of social discrimination. Such findings align with previous research indicating that individuals who have sought psychological help in the past may face stigma or be reluctant to engage with mental health resources again. 45
The recruitment of students from the same school environment may have fostered a supportive peer context during the intervention, potentially enhancing receptivity and group engagement. The use of a private online group for intervention delivery may have further contributed to a safe, interactive space that reinforced message retention and reduced the stigma associated with discussing mental health topics.
Limitations of the study
Several limitations should be acknowledged in this study. First, the intervention was implemented exclusively through a social media platform, which may have limited the participation of students without consistent internet access or social media accounts. Furthermore, the relatively short follow-up period (post-2 measurement) may not fully capture long-term behavioral change, particularly in domains like help-seeking, which are known to be resistant to rapid transformation. Moreover, while this study focused on MHL and related attitudes, it did not assess changes in students’ well-being or stress levels. Including such measures in future research could provide a more comprehensive picture of the intervention's impact. Finally, the study sample was limited to public schools in Amman, which may affect the generalization of the findings to other regions or educational settings.
Conclusion
Given the scarcity of mental health research and resources in LMICs, this study underscores the urgent need to develop and evaluate scalable, culturally sensitive interventions. The findings provide preliminary yet compelling evidence that a digital MHL awareness campaign, delivered via podcasts and reels, can meaningfully improve mental health outcomes among high school students. Improvements were observed in MHL levels, reductions in social discrimination, and increased willingness to seek professional help. However, help seeking behaviors remained the most resistant to change.
The intervention's effects varied by demographic factors. Male students scored significantly lower in willingness to seek help than females, underscoring the need for gender-sensitive approaches. Additionally, students with prior psychological referrals exhibited higher levels of social discrimination, suggesting that previous experiences with mental health services may reinforce stigmatizing attitudes.
This study highlights the value of establishing collaborative platforms where mental health nurses, media professionals, educators, and policymakers can co-create effective mental health awareness programs. At the research level, these findings offer baseline data that can guide future research studies and contribute to broader mental health promotion efforts in Jordan and similar LMICs.
Supplemental Material
sj-xlsx-1-dhj-10.1177_20552076251381761 - Supplemental material for The effectiveness of mental health literacy digital awareness campaign on social discrimination, willingness to seek professional psychological help, and intended behaviors among high school students in Jordan
Supplemental material, sj-xlsx-1-dhj-10.1177_20552076251381761 for The effectiveness of mental health literacy digital awareness campaign on social discrimination, willingness to seek professional psychological help, and intended behaviors among high school students in Jordan by Nuha R. Y. Amer and Ayman M. Hamdan-Mansour in DIGITAL HEALTH
Supplemental Material
sj-pdf-2-dhj-10.1177_20552076251381761 - Supplemental material for The effectiveness of mental health literacy digital awareness campaign on social discrimination, willingness to seek professional psychological help, and intended behaviors among high school students in Jordan
Supplemental material, sj-pdf-2-dhj-10.1177_20552076251381761 for The effectiveness of mental health literacy digital awareness campaign on social discrimination, willingness to seek professional psychological help, and intended behaviors among high school students in Jordan by Nuha R. Y. Amer and Ayman M. Hamdan-Mansour in DIGITAL HEALTH
Footnotes
Acknowledgments
I would like to sincerely thank the Middle East University for their support in facilitating the publication of this research. This manuscript is derived from a doctoral dissertation. Appreciation is also extended to the educational counselors in the participating high schools for their cooperation, and to the students for their participation in the study.
Ethics approval and consent statements
This study received ethical approval from the Institutional Review Board at the University of Jordan and formal permissions from the Jordanian Ministry of Education—specifically, the Educational Research and Educational Counseling Departments on May 23, 2024. All participants provided electronic informed consent prior to enrollment. The research was conducted in accordance with the ethical principles outlined in the World Medical Association Declaration of Helsinki.
Consent for publication
Not applicable. This manuscript does not contain any individual person's data in any form (including individual details, images, or videos), and publication consent was therefore not required.
Author contributions
All authors participated in all steps of this project until the last edit was sent to the journal.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Middle East University is providing support for the publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Availability of data and materials
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.