
Abstract
Background
Digital technologies offer the potential to promote mental health by improving older adults’ digital and mental health literacy. Intergenerational support is a promising medium to promote the mental health of older adults. Nonetheless, the effects of interventions employing digital and mental health literacy training through intergenerational support on the mental health of older adults remain unclear.
Objectives
This study evaluated the effects of the Digital Buddy programme on the mental health of older adults.
Methods
This study used a multi-centre, cluster-randomised, two-parallel-group (1:1 allocation ratio), controlled trial design. People aged ≥60 years without diagnosed mental illnesses were eligible. In the intervention group, participants attended 14 training sessions conducted by young volunteers over 2 months, using materials on a website and a smartphone app. The content included digital skills and mental health knowledge. Volunteers continued tele-coaching participants for 6 months. The control group received usual care. Outcomes measured at baseline (T0) and 1-week post-intervention (T1) included mental well-being, depressive symptoms, health-related quality of life, self-efficacy, and perceived social support. Generalised estimating equations tested the hypotheses.
Results
A total of 310 participants from 15 clusters entered the study, with each group containing 155 participants. The WHO-5 (mean difference = 7.0, d = 0.32, p < .001) and Patient Health Questionnaire-9 scores (mean difference = 0.9, d = 0.24, p = .02) of the intervention group improved after the intervention with statistical significance, but not in the control group. Likewise, the interaction effects of group and time on the two outcomes were not statistically significant.
Discussion
There was a main effect of time in the intervention group over the outcomes of mental well-being and depressive symptoms. However, the interaction was non-significant and therefore the change over time did not differ between groups and therefore groups had similar change trajectories. However, future studies should devise measures to enhance its effects.
Trial registration
This trial has been registered at ClinicalTrials.gov (NCT05553730) on 23 September 2022, https://clinicaltrials.gov/ct2/show/NCT05553730
Introduction
Approximately 14% of older adults live with a mental disorder, and one of the most common mental health conditions for older adults is depression, according to the WHO. 1 There is a bidirectional relationship between social disconnectedness and depression, which is mediated by self-perceived social isolation. 2 Social relationships play an essential role in maintaining and promoting people's mental well-being in later life.
The digital technology revolution has rapidly changed people's lives and ways of maintaining health (e.g. accessing health information and connecting with others). However, technology adoption among older adults is lower than among younger people. 3 Even in developed countries, digital exclusion remains a significant challenge for older adults, preventing them from fully participating in and benefiting from the digital technology revolution. 4 Evidence shows that how the person perceives the importance of smartphones in daily life, rather than the hours of using smartphones, correlates with lower levels of depression symptoms and loneliness. 5 Social-use digital literacy is positively associated with mental well-being and quality of life, and its effect on loneliness is also mediated by social connectedness and reduced loneliness. 6 Therefore, in a digitalised society, the ability of older adults to use smartphones to address daily challenges and maintain social connections is crucial and could play an essential role in their mental well-being. This substantiates the potential effects of promoting older adults’ mental well-being through enhancing their digital literacy.
Although digital technology competence is important for the mental well-being of older adults, a systematic review has shown that this successful adoption of digital technology still depends on many factors, including perceived usefulness, effort commitment, cost, and self-efficacy. 7 Evidence indicates that older age is associated with a lower level of digital technology usage; however, digital literacy support can mitigate the barriers related to age and socioeconomic resources. 8 Consequently, effective digital literacy support could enhance the use of digital technology, which can be therapeutically employed to promote mental well-being. Additionally, digital mental health interventions can facilitate resistance against stigma surrounding mental health, educate the public to encourage help-seeking, as well as promote social contact, all of which have been proven to be effective measures for reducing stigma related to mental health problems. 9
Intergenerational support is defined as the provision and receipt of financial, emotional, and physical assistance across different generations. 10 Intergenerational interventions (e.g. visiting programs and school volunteering programs) improve the mental well-being and self-efficacy of older adults, likely due to the development of social relationships, as demonstrated in a systematic review. 11 Evidence from an observational study also showed that older adults with higher levels of intergenerational support have better subjective well-being. 12 However, older adults in modern societies are more likely to become socially isolated and unsupported by their children due to an increasing trend of older individuals who are unmarried or childless. 13 Nevertheless, the benefits of intergenerational activities on mental well-being are not limited to familial relationships. Evidence also suggests that non-familial activities reduce loneliness, improve mental health, increase mutual understanding, and address ageism. 14 Additionally, intergenerational learning activities have improved depressive symptoms, social support, mental well-being, and quality of life. 15 This provides an opportunity to employ non-familial younger volunteers to offer intergenerational support to older adults, thereby promoting their mental health, social support, self-efficacy, and quality of life; although the evidence supporting the effectiveness of using intergenerational support as a therapeutic element is still scarce.
To summarise the evidence in the literature, the rapid development of digital technology is gradually excluding older adults from social engagement and access to health information, jeopardising their mental well-being. Digital literacy support could promote the adoption of digital technology among older adults. Intergenerational support is favourably associated with the mental health of older adults. However, there needs to be more evidence showing that digital technology training, coupled with digital literacy support through an intergenerational platform, can promote the mental well-being of older adults. If such evidence were established, it would provide a basis for developing interventions that bridge the digital divide and improve older adults’ mental health. This could influence policy and foster more inclusive communities for the ageing population.
Objectives
The objectives of this study were to evaluate the effects of the new Digital Buddy programme on the mental health of older adults. The focal interest of this study was to examine the interaction between time and group allocation. Accordingly, we hypothesised that, following completion of the intervention, participants in the intervention group would exhibit, in comparison to the control group, a greater degree of:
Improvement in mental well-being, Reduction in depressive symptoms, Improvement in health-related quality of life, Improvement in self-efficacy, and Improvement in perceived social support
Methods
This cluster randomised controlled trial is reported following the Consolidated Standards of Reporting Trials (CONSORT) 2010 statement: extension to cluster randomised trial. The study protocol was published on 7 February 2023. 16
Trial design
The study employed a multi-centre, cluster-randomised, two-parallel-group, noninferiority, controlled trial design with a 1:1 group allocation ratio.
Participants
A total of 15 centres for older adults in Hong Kong participated in the study and were randomised into intervention or control groups. A convenience sampling approach was used to recruit all eligible participants from the 15 centres. The primary purpose of this study is to understand whether a primary health and preventive intervention is effective in promoting the mental health of the general population; the study did not target people specifically with signs and symptoms of mental health issues (e.g. depressive symptoms). The eligibility criteria of the participants are below:
Eligibility criteria
Aged 60 + years,
Speak Cantonese and read traditional Chinese characters, and
Mentally capacitated is defined as having no diagnosed mental diseases leading to being mentally disabled and certified by a psychiatrist
Interventions
Details of the interventions are clearly described in the published protocol, and a summary of the conditions in the intervention and control groups is listed below. 16
Intervention group
The intervention aimed to enhance information and communication technology (ICT) skills, improve digital literacy, and promote mental well-being among participants through a series of training sessions. As shown in Table 1, a list of skills about ICT and mental health promotion was included. The 14-session training course, totalling 23 h, was delivered by interventionists and Digital Buddies – young volunteers from Hong Kong – who facilitated both learning and relationship building. Digital Buddies were undergraduate students aged 18 to 29 years from Tung Wah College, studying in various fields such as nursing, allied health, and management. The project team contacted both the Digital Buddy and the older participants by telephone at least once a week, known as the weekly check-in. The purpose of the weekly check-in was to ensure satisfactory adherence to the intervention, to identify any difficulties encountered in participating, and to provide support in resolving technical problems. The adherence of the intervention was measured by recording attendance at ICT skills and mental health training sessions.
ICT skills and mental health contents in the training sessions.

ICT: information and communication technology.
To maintain intervention fidelity across multiple sites, a standardised train-the-trainer program was implemented by the research team for young adult participants (i.e. the Digital Buddies). After completing a structured 2-h training, these participants were qualified as Digital Buddies, equipped with knowledge of ICT skills, mental health promotion, and effective communication with older adults. All training materials were made accessible via a newly developed web-based platform (www.twc.digitalbuddy.hk), ensuring that every site used the same comprehensive resources – including videos, micro-movies, and demonstrations – delivered in Chinese. This centralised approach facilitated uniformity in both content and training quality, regardless of location.
Control group
Those assigned to the control group continued with their routine care, which included participation in the regular activities organised by the residential care homes, such as social gatherings. The research team did not alter or influence the activities available to these participants in any way.
Outcomes
Baseline demographic information was collected at timepoint T0, encompassing variables of age, gender, educational attainment, employment status, financial satisfaction, living arrangement, years of smartphone usage, daily average of internet usage, perceived ability to use a smartphone, and perceived ability to use the internet. The five outcome measures were evaluated both at baseline (T0) and in the week following the conclusion of the intervention (T1). The principal outcome assessed was mental well-being, while four secondary outcomes – depressive symptoms, health-related quality of life, self-efficacy, and perceived social support – were measured.
The primary outcome of mental well-being was the World Health Organization Five Well-being Index (WHO-5), which evaluates psychological well-being over the preceding 2 weeks. 17 The WHO-5 consists of five items, each rated on a six-point Likert scale ranging from 0 (at no time) to 5 (all of the time), resulting in a total score between 0 and 25. Higher scores reflect a greater sense of psychological well-being. The Cantonese adaptation of the WHO-5 has demonstrated robust internal consistency (α = 0.86) as well as satisfactory concurrent validity with quality of life indices (r = 0.41–0.51). 17
Depressive symptoms were assessed using the nine-item Patient Health Questionnaire (PHQ-9), which measures symptoms over the preceding 2 weeks. 18 Each of the nine items is scored on a four-point Likert scale from 0 (not at all) to 3 (nearly every day), yielding a composite score ranging from 0 to 27. Elevated scores denote more pronounced depressive symptoms. The Cantonese version of the PHQ-9 has shown good internal consistency (α = 0.82), test–retest reliability (r = 0.76), and acceptable concurrent validity with the mental component of quality of life (r = −0.60). 18
Health-related quality of life was evaluated using the 12-item Short Form Health Survey Version 2 (SF-12v2), which covers the previous 4 weeks. 19 The SF-12v2 encompasses 12 items rated on scales of varying points, each assessing one of eight health domains: physical functioning, role physical, bodily pain, general health, vitality, social functioning, role emotional, and mental health. These domain scores are combined into two summary indices: the physical component summary and the mental component summary, calculated according to a standardised algorithm. Higher summary scores indicate more favourable health-related quality of life. The Chinese translation of the SF-12v2 has exhibited good test–retest reliability (r = 0.67–0.82) and strong construct validity, with the two-factor model accounting for over 80% of the total variance.20,21
Self-efficacy was measured using the 10-item General Self-Efficacy Scale (GSES-10), which has been translated and culturally adapted into Chinese. 22 Each of the 10 items is rated on a four-point Likert scale from 1 (not at all true) to 4 (exactly true), producing a cumulative score between 10 and 40. Higher scores signify greater self-efficacy. The Chinese version of the GSES-10 has demonstrated excellent internal consistency (α = 0.91), along with strong criterion validity in relation to well-being (r = 0.56–0.63, p < 0.001), self-esteem (r = 0.40–0.49, p < 0.001), and mental health (r = 0.39–0.41, p < 0.001). 23
Perceived social support was assessed using the 12-item Multidimensional Scale of Perceived Social Support (MSPSS-12). 24 This measure comprises 12 items distributed across three subscales, each corresponding to a source of support – family, friends, and significant others – with four items per subscale. Each item is rated on a seven-point Likert scale from 1 (strongly disagree) to 7 (strongly agree), yielding a total score from 12 to 84. Higher scores reflect greater perceived social support. The Chinese version of the MSPSS-12 demonstrates excellent internal consistency (Cronbach's α = 0.95), high test–retest reliability (intra-cluster correlation coefficient (ICC) = 0.91), and satisfactory concurrent validity with perceived stress (r = −0.221) and rewarding feelings associated with caregiving (r = −0.327). 25
Sample size
This trial followed the sample size estimation method as outlined in the published protocol. 16 A prior power analysis was conducted using the statistical test for the ‘mean difference between two independent groups’ in G*Power. The significance level was set at .05, and the power was set at .8. The group allocation ratio between the intervention and control groups was set at 1:1. The effect size was estimated according to a similar pilot study, which examined the impact of an intergenerational mentoring programme on the same primary outcome as the present study (i.e. well-being), and found that Cohen's d was 0.5. 26 Therefore, a sample size of 102 participants was needed.
We adopted Hemming's method to adjust the sample size required under individual randomisation for a cluster RCT with fixed and equal-sized clusters. 27 This study assumed that six clusters would participate, and the ICC was 0.01. The estimated total sample size was 244 (122 per arm). Assuming a dropout rate of approximately 20%, a total sample size of 292 was estimated, with 146 participants in each arm.
Randomisation
The cluster randomisation method was employed to reduce the risk of within-cluster contamination, as most of the training materials are open source and could be shared among participants within the same cluster. A permuted block (block size = 6) random allocation sequence list with an allocation ratio of 1:1 for either the intervention or control group was generated using the random number generation function in Microsoft Excel. More details can be found in the published protocol. 16
Blinding
In this study, only the outcome assessors were blinded to the group labels. It was impossible to blind the participants or the interventionists; therefore, they were not blinded to the group labels.
Statistical analysis
Data on demographic and outcome variables collected at baseline are reported either as means with standard deviations or as frequencies with percentages, depending on the level of measurement. Generalised estimating equations (GEEs) were used to test the hypotheses on the five outcomes. In the GEEs, the dependent variables were mental well-being, depressive symptoms, health-related quality of life, self-efficacy, and perceived social support across the two time points. The independent variables for all GEEs were the same: group (i.e. intervention and control groups), time (i.e. T0 and T1), and the interaction term of group and time (i.e. group × time). The interpretations of the hypotheses were based on the intention-to-treat analysis and the models without adjusting for covariates. The level of significance was set at 0.05. Missing data were replaced by estimation within the GEE because GEE includes samples with data from only one time point. For samples with missing data at both time points, the baseline data were first replaced by the mean value and then estimated by the GEE.
Results
Participant flow
Fifteen clusters, including 511 potential participants, were invited to attend the assessment for eligibility, as shown in Figure 1. 301 potential participants were excluded because they did not enrol for the screening (n = 82), did not meet the inclusion criteria (n = 96), or declined to participate after being screened as eligible (n = 23). Three hundred and ten participants from 15 clusters entered the study. Seven clusters were randomly allocated to the intervention group, which included 155 participants, while eight clusters were randomly allocated to the control group, which also included 155 participants. At the follow-up (i.e. T1), 12 participants in the intervention group did not attend the follow-up assessment due to conflicts between the available assessment dates, the availability of the assessment venue, and outcome assessors with their scheduled activities (n = 7) or health issues, including medical follow-ups or illnesses (n = 5). Forty-three participants in the control group reported that the follow-up assessment dates conflicted with their scheduled activities (n = 11) or health issues (n = 32).

CONSORT flowchart. CONSORT: Consolidated Standards of Reporting Trials.
Recruitment
The study was started on 1 April 2022, and the study was completed on 14 Dec 2023. The trial stopped as planned because the planned number of participants had been recruited. Facilities for older adults (e.g. community centres and nursing homes) within the institution that had previous collaborative experience were all invited to participate in the study. Promotional seminars were conducted in the facilities that had preliminarily agreed to participate in the study. During the seminars, the study was introduced to the centre staff members and some potential participants. Both printed and electronic posters were sent to the members of the facilities and displayed at the facilities. The staff members of the facilities invited all their members to participate. All interested members signed up voluntarily for the eligibility screening. All eligible participants were then invited to participate in the study.
Baseline data
The demographic and outcome variables are as shown in Table 2. Participants allocated to the intervention group, compared with the control group, were older (p < .001), perceived to have fewer financial resources (p = .046), perceived to be more able to use smartphones (p < .001), perceived to be more able to use the internet (p < .001), included more female participants (p < .001), had more participants owning a smartphone for more than four years (p < .001), and had more participants with a daily average internet usage of four times or more (p < .001). Gender and employment status were comparable between groups at baseline. For participants allocated to the intervention group, compared with the control group, the baseline mean PHQ-9 score was lower (p = .006), while the SF12v2-PCS score (p < .001), the mean MSPSS-12 score (p = .001), and the mean GSES-12 score were higher (p < .001). The mean WHO-5 and the mean SF12v2-MCS scores were comparable between groups at baseline.
Demographic and outcome variables at baseline.

*p < 0.05; WHO-5: the World Health Organization's Five Well-being Index, PHQ-9: 9-item Patient Health Questionnaire, SF12v2-MCS: 12-item Short Form Health Survey Version 2-Mental Component Summary, SF12v2-PCS: 12-item Short Form Health Survey Version 2-Physical Component Summary, MSPSS-12: 12-item Multidimensional Scale of Perceived Social Support, GSES-12: 10-item General Self-Efficacy Scale.
Numbers analysed
There were missing data among the participants included in the analysis. As shown in Figure 1, a total of 55 participants (12 participants in the intervention group, 43 participants in the control group) did not attend the follow-up assessment. The missing data were imputed using GEE as planned. Given that the intention-to-treat analysis was adopted as the primary analysis strategy, all eligible participants were included in the analysis.
Outcomes and estimation
The WHO-5 score of the participants in the intervention group significantly improved (mean difference = 7.0, d = 0.32, p < .001) after the completion of the intervention, but the improvement in the control group was not statistically significant (mean difference = 2.7, d = 0.10, p = .24). However, the interaction effect of group and time on the WHO-5 score was not statistically significant (p = .18), as shown in Table 3.
Outcome estimates.
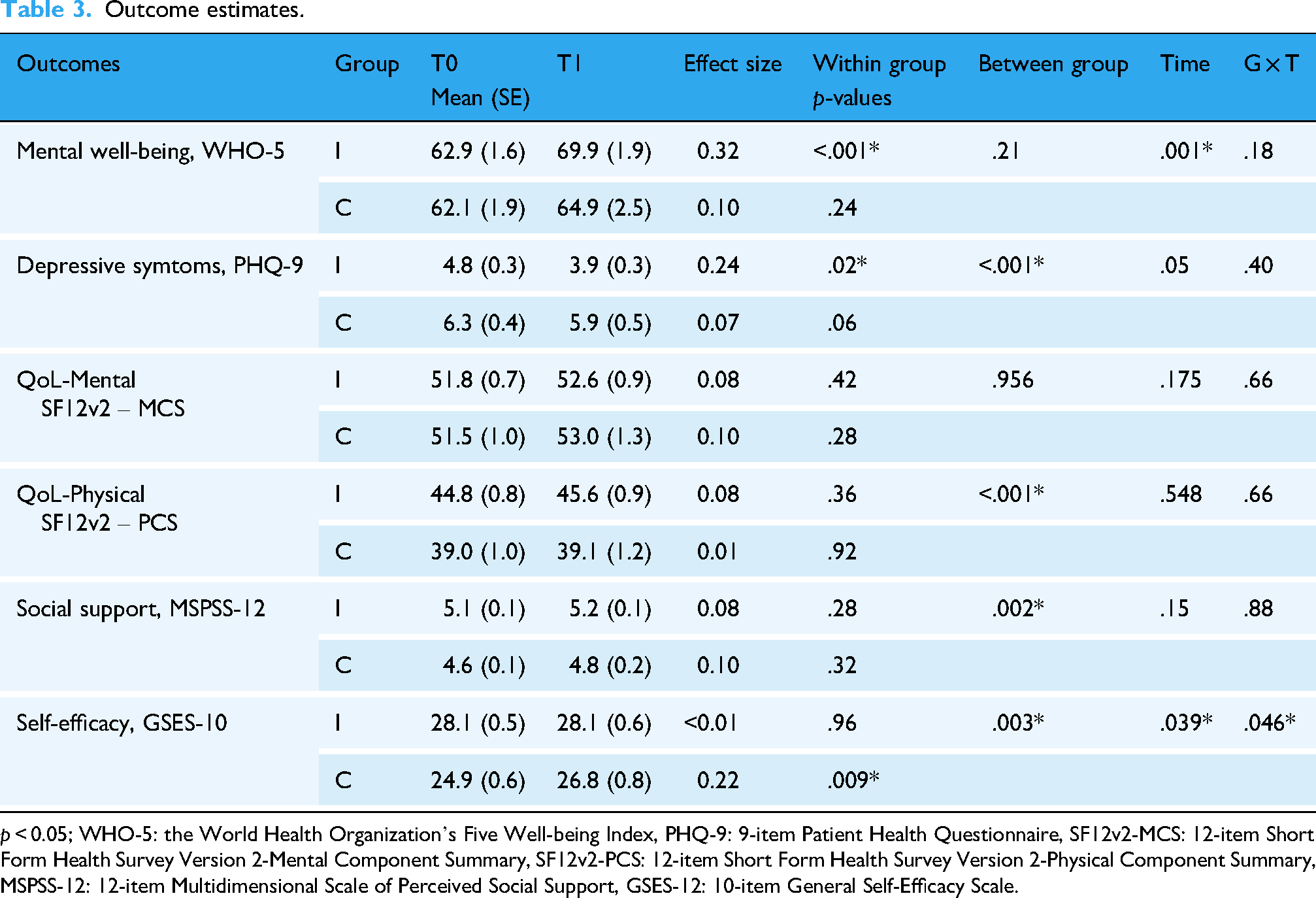
p < 0.05; WHO-5: the World Health Organization's Five Well-being Index, PHQ-9: 9-item Patient Health Questionnaire, SF12v2-MCS: 12-item Short Form Health Survey Version 2-Mental Component Summary, SF12v2-PCS: 12-item Short Form Health Survey Version 2-Physical Component Summary, MSPSS-12: 12-item Multidimensional Scale of Perceived Social Support, GSES-12: 10-item General Self-Efficacy Scale.
The PHQ-9 score of the participants in the intervention group significantly reduced (mean difference = 0.9, d = 0.24, p = .02) after the completion of the intervention, but the reduction in the control group was not statistically significant (mean difference = 0.4, d = 0.07, p = .06). However, the interaction effect of group and time on the PHQ-9 score was not statistically significant (p = .40), as shown in Table 3.
The SF12v2 and MSPSS-12, and GSES-12 scores showed no statistically significant changes in the intervention group after the completion of the intervention. However, the improvement of the GSES-12 score in the control group was statistically significant (mean difference = 1.9, d = 0.22, p = .009), and the interaction effect of group and time on the GSES-12 score was also statistically significant (p = .046), as shown in Table 3.
Ancillary analyses
Although statistically significant results were observed for two outcomes (i.e. WHO-5, PHQ-9) in the intervention group and one outcome in the control group (i.e. GSES-12), statistically significant differences in PHQ-9 and GSES-12 at baseline between groups were observed. As shown in Table 4, the group effect on PHQ-9 at T1 was statistically significant (β = 1.6, p = .006) after adjusting for the PHQ-9 observed at baseline, while the group effect on GSES-12 at T1 was no longer statistically significant (β = .2, p = .856) after adjusting for the GSES-12 observed at baseline.
Group effects on outcomes at T1 adjusted for outcomes observed at T0.

p < 0.05; PHQ-9: 9-item Patient Health Questionnaire, GSES-12: 10-item General Self-Efficacy Scale.
Harms
No untoward effects or incidents were reported by the participants, data collectors, or staff members of the elderly community centres throughout the study period.
Discussion
The Digital Buddy programme significantly improved the mental well-being and reduced depressive symptoms of participants in the intervention group. Yet, the changes in the control group were not statistically significant. However, the extent of improvement was not significantly greater than that in the control group. Nevertheless, after the completion of the intervention, the participants’ mental well-being and depressive symptoms were better in the intervention group than in the control group. These findings remained consistent after adjusting for the baseline imbalance of these two outcomes, as observed in the ancillary analysis.
Interpreting the reported results, a 7-point improvement out of 100 on the WHO-5 in the intervention group suggests a modest positive shift in participants’ well-being, though it falls short of the typically referenced 10-point (10%) threshold for clinical significance. 28 This implies that, while there was some improvement in well-being following the intervention, it may not be considered clinically meaningful in the context of depressive symptom improvement. Likewise, the reduction in depressive symptoms as measured by the PHQ-9 – a mean difference of 0.9 points – does not reach the minimum clinically important difference of 5.0 points. 29 This small change indicates that, although participants in the intervention group experienced a slight decrease in depressive symptoms, the effect might not be clinically meaningful. Taken together, these findings suggest that while there are some measurable improvements in both well-being and depressive symptoms, the magnitude of change is limited to translate into significant clinical benefits for most individuals.
A systematic review of community-based mental health and well-being interventions for older adults showed that educational interventions on various mental health-related topics (e.g. basic knowledge about sleep hygiene and emotion regulation) do not improve mental well-being or reduce depressive symptoms. 30 However, social engagement interventions (e.g. intergenerational programmes and home visits by trained volunteers) demonstrated favourable effects in reducing depressive symptoms. 30 There is a dearth of evidence from randomised controlled trials demonstrating that community-based interventions can simultaneously promote mental well-being and reduce depressive symptoms in older adults.
This study extends our understanding by suggesting that mental health education alone might not effectively promote mental well-being. However, when combined with other therapeutic elements (e.g. intergenerational support and digital literacy education), the effects on promoting mental well-being are significantly enhanced. Nevertheless, since no group in this study used only intergenerational activities, it remains unclear whether the mental health promotion effects mainly stem from intergenerational activities or the interaction among mental health education, digital literacy education, and intergenerational support. Further studies should examine the relationship between the effects of these intervention components on mental health promotion.
Evidence has shown that social connectedness and social support are associated, but social support may be relatively more important to well-being than social connectedness. 31 Additionally, social support is correlated with mental health in older adults. 32 Surprisingly, the study revealed that the intervention is effective in promoting mental health but not in enhancing perceived social support. This may be because the intervention promotes mental health not by increasing social support, but possibly through other pathways, such as digital technology literacy or social connectedness. Past research evidence also indicates that acceptance of technology is associated with the health outcomes of older adults. 33 Future studies should measure technology literacy or acceptance and social connectedness to expand our understanding of how this type of intervention works.
Early studies have already proven that physical activity is very effective in promoting mental well-being. 34 However, a portion of older adults cannot participate in physical activity due to functional limitations secondary to chronic illnesses. 35 This intervention might be particularly useful for promoting the mental health of older adults with functional limitations who cannot engage in an adequate amount of physical activity. The present study does not employ physical activity as a component in the intervention programme, yet can still be effective in promoting mental health. Therefore, the present study recommends applying this intervention to individuals, particularly those who are restricted to physical activity. It is because this intervention, without physical activity components, can still promote their mental health. Future studies should also examine the effects of this intervention specifically in this population.
Before the COVID-19 pandemic, the uptake of digital health technologies had been unsatisfactory; however, it accelerated during and after the pandemic. 36 In the post-pandemic era, mental health services will increasingly rely on digital technologies to alleviate the burden on the mental healthcare system, as the impact of digitalisation is expected to be widespread and will encourage the emergence of new digital services. The present study demonstrated that tele-coaching can be effectively used as a form of prolonged intergenerational support for older adults to promote their mental health. It is recommended that a similar approach be adopted as a public mental healthcare policy to more efficiently promote the mental health of older adults in community settings.
The intervention showed promising results in promoting mental well-being and reducing depressive symptoms. The improvement in the intervention group was not significantly higher compared with the control group. One possible reason is that the present study was conducted during the year immediately following the subsiding of the COVID-19 pandemic. Research has shown that most mental health symptoms subsided compared to the onset of COVID-19. 37 This effect from the relenting of COVID-19 may have censored part of the intervention effects, making the interaction effects between group and time insignificant.
This study showed that the effect size of the intervention on the mental health outcomes is not large. This study did not track the level of participation in the home-based training part and the utilisation of the knowledge transferred, although Digital Buddies were invited to weekly tele-support with them. Evidence showed that adherence to internet-based intervention is positively associated with mental health outcomes (e.g. depression). 38 The sub-optimal effect size could be due to the sub-optimal adherence and the uptake of the home-based training of the app. To increase the effect size, it is recommended to provide additional support to enhance adherence to the home-based training and uptake of the training content. For example, multiple e-health strategies – such as automated advice, which have been shown to be effective in improving adherence to health behaviours, 39 could be incorporated into the apps for future intervention development. Nevertheless, one of the strengths of this intervention is that it can be applied to a large population, not restricted to those with mental illness symptoms. The potential number of beneficiaries could be large for it to serve as an effective intervention for primary health prevention.
This study targeted the general population of older adults, but its core elements (e.g. intergenerational support, digital literacy education, and tele-coaching) could be adapted for other groups facing barriers to mental health support, such as those in rural areas, people with disabilities, or the socially isolated. The digital format allows flexible delivery tailored to local culture, language, and technology access. When intergenerational links are impractical, peer- or community-mentor models could be used. 40 Digital literacy modules could be adjusted for different skill levels. Scaling up may require collaboration with community organisations, healthcare providers, and public agencies to ensure fair access and sustainability. Future research should address cultural adaptations and test the Digital Buddy programme in varied contexts, considering technology infrastructure, social support, and health policy to maximise effectiveness for wider populations.
Limitations
There are several limitations to this study. Firstly, the demographic and clinical profiles of the participants were not balanced between the groups. Given that cluster randomisation was used, the participants (by cluster) randomly allocated to the control group happened to be older and have a lower level of digital literacy and education than those in the intervention group. Although this is a randomised controlled trial and the imbalance is likely to have occurred randomly, there is a risk that these factors might have confounded the effects of the intervention on the outcomes.
Secondly, many baseline outcomes were also not balanced between the groups. We attempted to adjust for the outcomes with favourable effects, considering the observed imbalance at baseline in the ancillary analysis, the results still showed that the group effect was significant. However, the risk of confounding effects due to the baseline imbalance of the outcomes cannot be confidently eliminated.
Thirdly, it was surprising to detect a significant interaction for self-efficacy, with improvement observed in the control group but not in the intervention group. In theory, no intervention was provided to the control group. It is possible that activities known to enhance general self-efficacy (such as those promoting successful ageing, learning, and practising meta-cognitive strategies) were available at the centres assigned to the control group, thereby contributing to the increase in self-efficacy. Furthermore, the control group's lower baseline self-efficacy may have made them more likely to experience improvement. However, based on the data available in this study, the reason cannot be determined with confidence. Further research should investigate which aspects of usual care commonly provided in centres for older adults may contribute to the enhancement of general self-efficacy. Future studies should also exercise measures to improve the quality of cluster randomisation (e.g. defining clusters and selecting individuals within clusters more strategically) to minimise the risk of these unexplained observations. 41
Finally, this study only assessed the immediate effects, namely the outcomes measured directly following completion of the intervention. The long-term effects and changes occurring throughout the intervention period remain unknown. This lack of information may limit the generalisability of the intervention concerning both short-term outcomes (i.e. those observed during the intervention period) and long-term outcomes.
Conclusion
In conclusion, the Digital Buddy programme demonstrated modest improvements in mental well-being and reductions in depressive symptoms among older adults, though these gains were not clinically significant or substantially greater than those seen in the control group. The study does not support the notion that Digital Buddy improves quality of life, self-efficacy, or perceived social support. Nevertheless, the interaction of mental health education, digital literacy education, and intergenerational support appears to be the active ingredient in yielding favourable effects on older adults’ mental health in other domains, specifically in mental well-being and depressive symptoms. Digital and mental health literacy training, coupled with intergenerational support, could be adopted as public policy to promote the mental health of older adults in community settings. Future studies should devise measures to enhance its effects.
Footnotes
Acknowledgements
The authors would like to thank the organisations providing all the facilitations, including manpower and venues, for participant recruitment and intervention implementations.
Ethical approval
Ethical approval for this project was granted by the Research Ethics Committee, Tung Wah College [Ethics application number: REC2022143].
Author contribution
SC is the guarantor of the project. SC, FN, and RK conceptualised the idea and designed the research methods, including data collection, intervention, and analysis. ML coordinated the implementation of the project. TT and EL facilitated the team's connection with the organisation providing venues and manpower for the study's implementation, and also offered advice on the research design. RK and ML drafted the manuscript. SC, FN, TT, and EL reviewed and commented on the manuscript. The final version of the manuscript was reviewed and approved by all authors.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was funded by the Mental Health Initiatives Funding Scheme, Food and Health Bureau, Hong Kong (grant number MHI_0028).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data are available from the corresponding author upon a reasonable request.
Protocol
The study protocol was published on 7 February 2023. 16