
Abstract
Objective
Investigating the digital health literacy of university students can facilitate their effective acquisition of health information and adoption of appropriate protective behaviors. This study aims to explore the subtypes of digital health literacy among university students during the COVID-19 pandemic and their association with mental health outcomes.
Methods
From 17 November to 14 December 2022, a stratified random sampling approach was used to conduct an online questionnaire survey on digital health literacy, fear of COVID-19, and depression status among students at Jilin University, China. A total of 1060 valid responses were obtained in the survey. Latent profile analysis identified subtypes of digital health literacy and linear regression analyses were used to examine the association of digital health literacy to the mental health outcome.
Results
Three latent profiles were identified: Profile 1—low digital health literacy (n = 66, 6.23%), Profile 2—moderate digital health literacy (n = 706, 66.60%), and Profile 3—high digital health literacy (n = 288, 27.17%). Results from linear regression demonstrated a negative correlation between digital health literacy and fear of COVID-19 (B = −2.954, P < 0.001) as well as depression (B = −2.619, P < 0.001) among university students.
Conclusions
This study indicated that the majority of university students exhibit a moderate level of digital health literacy during the COVID-19 pandemic. Additionally, the study validates a negative correlation between digital health literacy and mental health among university students.
Introduction
The COVID-19 pandemic has had a significant impact on various aspects of health. To mitigate the transmission of COVID-19, preventive measures such as lockdowns have been widely implemented by countries around the world. 1 The internet and social media have consequently become the major tools for the public to obtain information related to COVID-19. 2 It is well-recognized that major disease outbreaks are often accompanied by a surge of misinformation, which is exacerbated by social media networks.3–5 A study revealed that among 1225 fake news stories related to COVID-19 from January to April 2020, 50.5% of the misinformation was disseminated through social media platforms. 6 Rumors regarding the curative effects of neat alcohol on COVID-19 spread through social media, resulting in hundreds of Iranians succumbing to poisoning. 7 This phenomenon has been coined an “infodemic” and calls for appropriate countermeasures. 8 Addressing the Munich Security Conference, the Director-General of the World Health Organization remarked on 15 February 2020, “We are not only just fighting an epidemic, but also an infodemic.” 9 A survey indicated that as many as 87% of internet users have been exposed to misinformation pertaining to the pandemic. 10
Handling complex health information during an epidemic necessitates that the public possesses sufficient digital health literacy. 11 Digital health literacy encompasses the capacity to search, select, evaluate, and apply online health information and digital applications related to health care. 12 Digital health literacy enables the public to access timely and adequate information that is essential for making health-related decisions that have a positive impact, thereby contributing to the promotion of health equity in terms of health, well-being, and resilience during epidemic situations. Despite some progress in studies that aim to fully automate the identification of information validity, the accurate identification of disinformation on social media during the COVID-19 epidemic remains below an acceptable level.13,14 Previous studies have demonstrated the noteworthy influence of digital health literacy on individuals’ ability to access accurate knowledge, 12 cultivate favorable attitudes toward preventive measures, 11 and engage in behaviors such as vaccination 15 during epidemic outbreaks.
University students constitute a demographic that relies heavily on digital technologies and primarily accesses health-related information through online platforms.16,17 A study revealed that 95.8% of Chinese university students obtained information about the COVID-19 pandemic through new media platforms such as WeChat and Weibo. 18 Some studies have claimed that university students rely more on personal decision-making and life circumstances than on parental or adult guidance.19,20 This highlights the need for this population to possess sufficient digital health literacy. Various countries have conducted research on digital health literacy among university students during the COVID-19 pandemic. Findings indicate that university students encounter challenges, particularly in assessing the reliability of information.16,21 However, previous studies have predominantly used variable-centered approaches and lacked individual-centered analysis methods, potentially obscuring the heterogeneous profiles of digital health literacy among university students. Latent profile analysis (LPA), a person-centered algorithm, partitions individuals into unobserved groups with similar (more homogeneous) patterns to simulate heterogeneity. 22 In recent years, latent profile analysis has found extensive application in the analysis of feature structures.23–27 Utilizing latent profile analysis can overcome the limitations of previous research, allowing for the exploration of unobserved subgroups in digital health literacy.
A substantial body of research indicates that university students’ mental health is particularly susceptible to the impact of the COVID-19 pandemic when compared to other populations.28,29 There is plenty of literature from multiple countries validating the importance of studying university students’ mental health as a population of particular interest.30–32 Due to containment measures such as school closures and restrictions on social gatherings, 33 university students are confronted with the challenges of coping with uncertainty, semester interruptions, and prolonged social disconnections from friends and campus peers. 34 During the COVID-19 pandemic, numerous students encountered complicated negative emotions and increased risks of loneliness, isolation, suicidal ideation, and excessive alcohol consumption. 35 Previous research has substantiated the associations between e-health literacy and factors such as fear 36 and depression. 37 However, although the terms are occasionally used interchangeably in research, “e-health literacy” and “digital health literacy” have distinct differences. 12 In contrast to e-health literacy, digital health literacy emphasizes not only the capacity to collect, comprehend, evaluate, and integrate health information but also interactivity within online platforms, encompassing content creation and privacy protection. 11 Hence, there is a need to further explore the association between digital health literacy and the psychological well-being of university students.
Therefore, this study employs latent profile analysis to comprehensively examine typologies of digital health literacy among university students and explore their association with mental health.
Methods
Study design and participants
This cross-sectional investigation was conducted at Jilin University in China using an online survey instrument from 17 November to 14 December 2022. Since March 2022, a new outbreak caused by the SARS-CoV-2 Omicron variant has appeared rapidly in Jilin, China. Despite progress in controlling the COVID-19 pandemic, sporadic cases of COVID-19 cases persisted throughout the investigation period. A stratified cluster sampling design was employed for participant selection. Two medical colleges and six nonmedical colleges were included in the study: College of Software, College of Electronic Science and Engineering, College of Veterinary Medicine, School of Mathematics, School of Life Sciences, School of Humanities, School of Mechanical and Aerospace Engineering, the First Hospital of Jilin University, and the School of Public Health. Within each college and academic year, one class was randomly selected for participation in the study. The study population included both undergraduate and graduate students. The inclusion criteria for participants in this study were as follows: (1) currently enrolled students at Jilin University in China, (2) students who agreed to participate in the study, and (3) students who were fully capable of answering the survey questions. Exclusion criteria: university students who were not in school during the investigation period.
Ethical approval for this study was obtained from the Medical Ethics Committee of Jilin University (IRB code No. 2022-11-05). The purpose and protocol of the study were clearly explained to the participants at the beginning of the survey. Informed consent was obtained from all participants prior to their participation in the study. A total of 1070 individuals completed the survey. After verification, 10 questionnaires with logical errors were excluded, resulting in a final sample size of 1060 (99.1% of returned questionnaires) for inclusion in the data analysis.
Instruments and measurements
Digital health literacy
In this study, we utilized the validated Digital Health Literacy Instrument (DHLI) to assess the digital health literacy of college students. The DHLI was developed by Rosalie van der Vaart and comprises seven subscales. 12 Bak et al. 38 adapted the scale to fit the context of the COVID-19 pandemic during the investigation. The revised scale includes five subscales: (1) information searching, (2) evaluating reliability, (3) determining relevance, (4) adding content, and (5) protecting privacy. Each subscale contains three items that are rated using a 4-point Likert scale based on the original scale (1 = very difficult; 4 = very easy). Some studies also argue that a four-point Likert scale can mitigate the presence of a neutral option, which tends to engender doubt regarding the accuracy of respondents’ choices. 39
In this study, the overall Cronbach's alpha for the digital health literacy scale was 0.951, while the subscale Cronbach's alphas were 0.937, 0.889, 0.936, 0.948, and 0.824, respectively, indicating good internal consistency reliability of the instrument. Confirmatory factor analysis results showed that the scale had an acceptable model fit with root mean square error of approximation (RMSEA) = 0.078, comparative fit index (CFI) = 0.969, and Tucker–Lewis index (TLI) = 0.959.
Fear of COVID-19
In this study, we employed the Fear of COVID-19 Scale (FCV-19S) to assess the level of fear among college students. 40 The FCV-19S comprises seven items, each rated on a 5-point Likert scale (1 = strongly disagree; 5 = strongly agree). Higher scores indicate greater fear of COVID-19. Studies conducted in various regions have demonstrated that the scale possesses good psychometric properties.41,42 In this study, the Cronbach's alpha for the FCV-19S was 0.916, indicating good internal consistency reliability. Confirmatory factor analysis results showed that the scale had an acceptable model fit with RMSEA = 0.079, CFI = 0.992, and TLI = 0.973.
Depression
The PHQ-9 questionnaire was used to assess depressive symptoms in college students. The PHQ-9 is a self-report rating scale for depressive symptoms over the past 2 weeks that consists of nine items. 43 The scale uses a 4-point Likert scale (0 = not at all; 3 = nearly every day). Higher scores indicate higher levels of depression in college students. The PHQ-9 has demonstrated good reliability and validity in previous research.44,45 In this study, the scale had a Cronbach's alpha of 0.948, RMSEA = 0.057, CFI = 0.992, and TLI = 0.985, indicating a good model fit.
Statistical analysis
We performed a descriptive analysis of the demographic variables. Continuous variables are reported as the mean ± standard deviation, while categorical variables are expressed as the frequency (percentage).
Latent profile analysis was used to identify different subtypes of digital health literacy among college students during the COVID-19 pandemic. Latent profile analysis is based on the principle of conditional independence and classifies individuals into different groups based on the responses of multiple continuous indicators. 46 Latent profile analysis was initiated with a one-class solution, and the number of profiles was subsequently increased. The study used the following statistical fit indices to determine the optimal number of profiles. The Bayesian information criterion (BIC), the Akaike information criterion (AIC), and the sample-size-adjusted Bayesian information criterion (aBIC) were utilized for model comparisons. Smaller values of the BIC, ACI, and aBIC indicate better model fit. 47 The entropy value was used to assess the accuracy of profile classification, with higher values (i.e. above 0.8 and closer to 1) indicating greater accuracy.22,48 The Lo-Mendell-Rubin likelihood ratio (LMR) test and the bootstrap likelihood ratio test (BLRT) were employed to compare the fit between the k and k−1 profile models. If the P value is < 0.05, the k-profile model is considered more suitable than the k−1 model. 49
The chi-square test, analysis of variance (ANOVA), and Fisher's exact test were conducted to examine the difference in the latent profiles by characteristics. Independent samples t-test and ANOVA were used to compare the differences in mean scores of fear of COVID-19 and depression among groups. Multiple linear regression analysis was used to examine the association between digital health literacy and variables including fear of COVID-19 and depression. All variables were simultaneously entered into the linear regression model.
Descriptive analysis, chi-square test, ANOVA, Fisher's exact test, independent samples t-test, and multiple regression were performed using SPSS 25.0 software (SPSS Inc., Chicago, IL, USA). Latent profile analysis was conducted using Mplus 7.31 software (Muthén & Muthén, Los Angeles, CA, USA). All tests were two-tailed with a significance level of P < 0.05.
Results
Sociodemographic characteristics of the respondents
As presented in Table 1, 51.42% of the students were male, and 48.58% were female. Undergraduates constituted 77.83% of the sample, while 22.17% of students were pursuing a master's or doctoral degree. The mean age of the sample was 21.72 ± 2.50 years. Of the students, 28.02% were from medical schools, and 71.98% were not medical students. A total of 25.66% of the students reported poor health, while 74.34% reported good health. Among the subjects, 99.53% had not been infected with COVID-19, while 0.47% had been infected. A total of 97.26% of the students had no contact with COVID-19 patients, while 2.74% had contact with COVID-19 patients. Precisely, 5.8% of participants reported that their parents or friends had contracted COVID-19, while 94.2% did not.
Sociodemographic characteristics of respondents (n = 1060).

Latent profiles of university students’ digital health literacy
Table 2 presents the one- to seven-profile models used to determine the optimal number of profiles. The results of the model suggest that the LMR-LR test was not significant for the four-profile model, indicating that it was less parsimonious and desirable than the three-profile model. The LMR-LR test for the three-profile model was significant, suggesting that it was more suitable than the two-profile model. Additionally, the AIC, BIC, and aBIC values for the three-profile model were lower than those for the two-profile model, indicating that it was more suitable. The entropy value for the three-profile model was 0.993, demonstrating the accuracy of classification. From this, we infer that there are three latent profiles of college students’ digital health literacy within the research population.
Fit statistics for latent profile analysis.

BIC: Bayesian information criterion; AIC: Akaike information criterion; aBIC: adjusted Bayesian information criterion; LMR: Lo-Mendell-Rubin likelihood ratio; BLRT: bootstrap likelihood ratio test.
The mean digital health literacy score for all participants was 3.00 (SD = 0.49). Figure 1 illustrates the average scores for each item within the three-profile model of digital health literacy, representing the distinct characteristics of the three profiles.
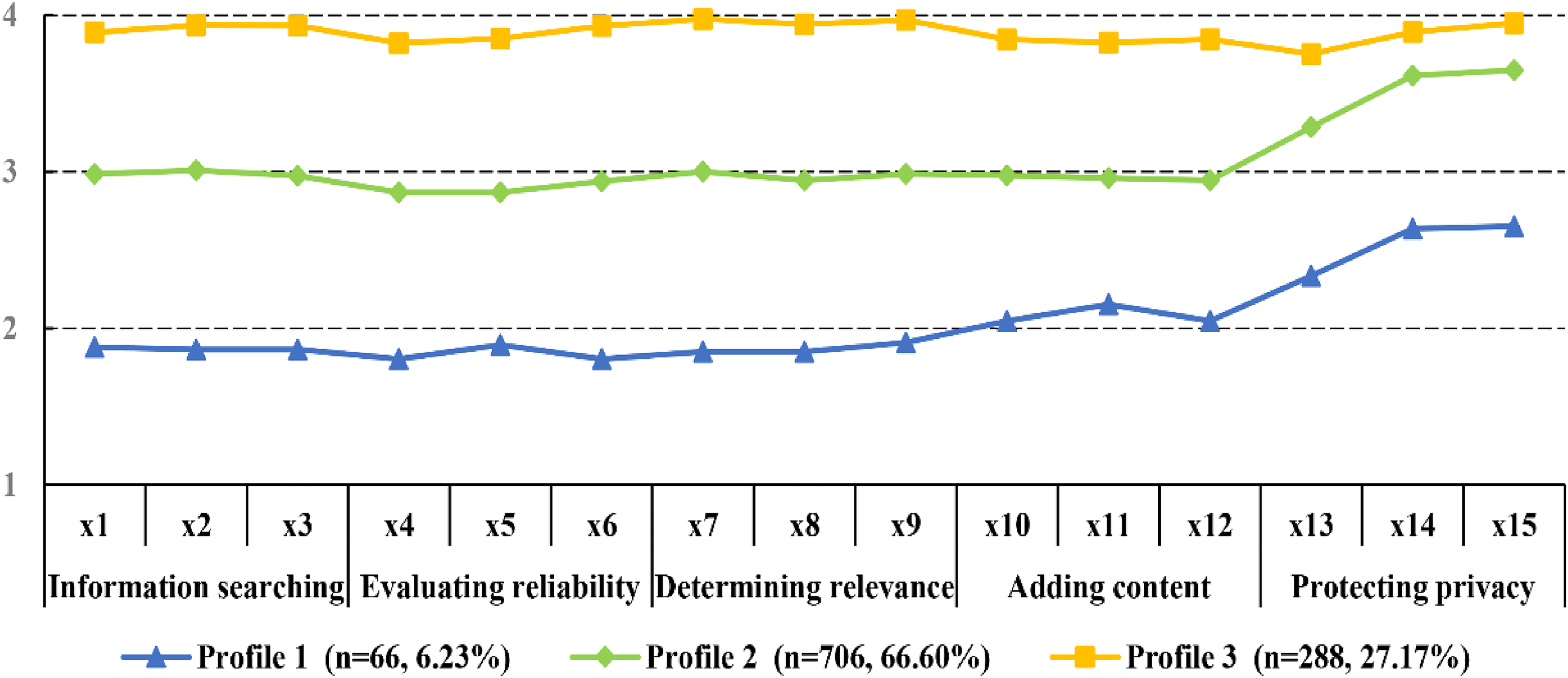
Latent profiles of digital health literacy. Note: Profile 1 = low digital health literacy group, Profile 2 = moderate digital health literacy group, and Profile 3 = high digital health literacy group.
Given the lowest response rates in the dimensions of information searching, evaluating reliability, determining relevance, adding content, and protecting privacy, Profile 1 was identified as the “Low Digital Health Literacy Group.” The overall average digital health literacy score for this profile was 1.88 (SD = 0.43), with the lowest mean score in the dimension of evaluating reliability (1.83 ± 0.51) and the highest mean score in the dimension of protecting privacy (2.54 ± 0.98). Profile 1 comprised 66 students (6.23% of the participants).
Profile 2, with mean scores falling between the other two profiles, was identified as the “Moderate Digital Health Literacy Group.” The average digital health literacy score for this profile was 2.85 (SD = 0.17). Within this profile, the lowest mean score was observed in the dimension of evaluating reliability (2.89 ± 0.31), while the highest mean score was observed in the dimension of protecting privacy (3.52 ± 0.57). Profile 2 included 706 students (66.60% of the participants).
Profile 3, characterized by the highest mean scores across all items, was labeled the “High Digital Health Literacy Group.” Profile 3 included 288 students (27.17% of the study population) and exhibited a mean score of 3.64 (SD = 0.15). This profile demonstrated elevated levels of digital health literacy, with mean scores ranging between 3.84 and 3.96 across various dimensions.
Difference in the latent profiles by characteristics
The statistical description for distributions of different latent profiles is shown in Table 3. Significant differences were also indicated among gender (P < 0.001) and self-reported health (P = 0.003). Profiles 1 and 3 both had a high proportion of males (59.1% and 60.4%, respectively) while Profile 2 was most mostly female (53.0%). All subgroups were primarily comprised of university students who self-reported better health status, with Profile 2 (97.3%) exhibiting the highest health status than Profile 3 (95.5%), which in turn reported higher health status than Profile 1 (89.4%).
Characteristics of individuals in different subgroups.

Note: a Chi-square.
Analysis of variance (ANOVA).
Fisher's exact test.
Score of mental health
Table 4 shows that all university students who participated in this study had a fear of COVID-19 score of 14.35 ± 6.13 and a depression score of 4.85 ± 5.68. A one-way ANOVA was employed to compare fear of COVID-19 and depression scores across all three profiles. As depicted in Table 4, statistically significant differences were observed in the fear of COVID-19 (F = 49.487, P < 0.001) and depression (F = 56.326, P < 0.001) scores among the three profiles. Study subjects within Profile 1 exhibited the highest fear of COVID-19 scores (16.98 ± 7.02), while Profile 3 had the lowest scores (11.49 ± 6.25) and Profile 2 ranked in the middle (15.27 ± 5.58). The post-test results indicated significantly elevated fear of COVID-19 scores in Profile 1 compared to Profile 3 (P < 0.001) and in Profile 2 compared to Profile 3 (P < 0.001), while no significant difference emerged between Profiles 1 and 2. Similarly, study participants in Profile 1 recorded the highest depression scores (10.11 ± 8.49), Profile 3 had the lowest scores (2.68 ± 4.99), and Profile 2 had intermediate scores (5.25 ± 5.19). The post-test results exhibited the following ranking of depression scores: Profile 1 > Profile 2 > Profile 3, with significant differences observed between all three profiles (P < 0.001).
The mean scores of fear of COVID-19 and depression of samples.

Note: aModerate > high (P < 0.001), low > high (P < 0.001).
Low > moderate (P < 0.001), moderate > high (P < 0.001), low > high (P < 0.001).
Furthermore, as shown in Table 4, self-reported health was significantly associated with scores of fear of COVID-19 (P < 0.001) and depression (P < 0.001). Gender (P = 0.009) and major (P = 0.025) were significantly associated with fear of COVID-19.
Results of multiple linear regression analysis
Table 5 presents the results of the multiple linear regression analysis. After controlling for factors such as gender, grade, age, major, self-rated health, COVID-19 infection experience, COVID-19 close contact experience, and family members or friends infected with COVID-19, digital health literacy exhibited negative associations with fear of COVID-19 (B = −2.954, P < 0.001) and depression (B = −2.619, P < 0.001).
Results of multivariate linear regressions.

Discussion
Exploring the latent profiles of digital health literacy among university students and the association of digital health literacy with mental health provides a vital research perspective for infodemic management among university students and the improvement of their psychological well-being in the context of infectious disease outbreaks. This study, conducted at Jilin University in China, surveyed 1060 university students to explore subtypes of digital health literacy and validate their influence on fear of COVID-19 and depression.
In this study, we identified three distinct categories of digital health literacy among university students in the context of the COVID-19 pandemic. These categories were labeled the “high digital health literacy group,” “moderate digital health literacy group,” and “low digital health literacy group.” Among the 1060 surveyed university students, a majority (66.60%) fell into the “moderate digital health literacy group,” while approximately a quarter (27.17%) belonged to the “high digital health literacy group.” The proportion of students in the low digital health literacy group was the lowest, accounting for 6.23%. Our investigation revealed that the overall mean score across the digital health literacy scale was 3.00 ± 0.49 among the 1060 survey participants. This result was consistent with the findings of previous studies. A study involving university students from China, Malaysia, and the Philippines found that the digital health literacy score for university students in East Asia and Southeast Asia was 2.89 (SD = 0.42). 50 A survey of Vietnamese university students revealed that among 1003 participants, the mean score of digital health literacy related to COVID-19 was 2.87 ± 0.32. 51 Rivadeneira's research with 2138 university students from Spain, Puerto Rico, and Ecuador revealed that the mean score for digital health literacy was 2.94 with a standard deviation of 0.57. 52
Our study identified challenges among university students with low-level digital health literacy and those with moderate-level digital health literacy in evaluating information reliability while demonstrating higher scores in the domain of privacy protection. The assessment of information reliability is a multifaceted skill critical to health literacy. 53 Research indicates that even young individuals struggle to evaluate health information related to COVID-19 despite their familiarity with digital media usage.54,55 A German study revealed that nearly half of students encounter difficulties in assessing the reliability of online information, particularly concerning the identification of commercial interests behind news content, and this challenge is more pronounced among female students. 16 Similar challenges were observed in studies of intern nurses who faced difficulty evaluating information and distinguishing between high-quality and low-quality sources.56,57 A semistructured interview study in the United States revealed that students tend to prioritize the characteristics of the information source or content over the qualifications of information publishers. 58 Furthermore, digital health services introduce an increased risk of privacy breaches. 59 In this digital era, data have emerged as a pivotal factor that shapes societal and environmental structures. 60 Hence, the capacity to safeguard privacy constitutes an essential facet of digital health literacy. Our investigation revealed high privacy protection scores across three profiles of digital health literacy among university students. A study focused on American adolescents revealed that social media usage plays a pivotal role in increasing adolescents’ concern for online privacy. 61 Considering the elevated frequency of social media utilization among college students, this trend could potentially contribute to heightened privacy awareness.
Comparisons of demographic variables across different profiles revealed that university students in the low digital health literacy group and high digital health literacy group had a higher proportion of males. In addition, individuals in the high digital health literacy group and moderate digital health literacy group reported better self-rated health statuses. Previous studies have shown that female students are more frequent users of health information on the internet, but male individuals have higher proficiency in using online applications, 62 which may explain the gender differences observed in this study. Other related studies have also verified a significant positive correlation between digital health literacy and self-reported health, 63 which is consistent with the findings of this study.
Consistent with previous studies, our investigation revealed mental health concerns among university students (fear of COVID-19 score: 14.35 ± 6.13, depression score: 4.85 ± 5.68).64,65 An Israeli study reported an average fear of COVID-19 score of 14.95 ± 4.80 among university students during the COVID-19 pandemic. 64 Similarly, a study from China indicated a depression score of 5.49 ± 4.81 among students. 65 Furthermore, our study indicated that fear of COVID-19 scores were significantly higher in the low and moderate digital health literacy groups than in the high digital health literacy group. A similar pattern was observed for depression scores, which showed a notable increase with varying levels of digital health literacy. Regression analysis further revealed a negative association between digital health literacy and fear of COVID-19 and depression among university students during the COVID-19 epidemic. The results aligned with findings from previous research. Digital health literacy is considered a crucial determinant of public mental health during epidemics. 66 Choukou's research demonstrated that higher levels of digital health literacy are associated with lower levels of fear of COVID-19. 67 A study conducted in Taiwan indicated a significant and complete mediating effect of fear of COVID-19 between digital health literacy and future anxiety among university students. 68 A study conducted in Ghana revealed a significant impact of digital health literacy on depression, particularly among male students. 66 Research has suggested that digital health literacy can enhance individuals’ self-efficacy. 69 According to social cognitive theory, self-efficacy is a crucial determinant of health. 70 Several studies have confirmed the association between general self-efficacy and mental health issues during the COVID-19 pandemic.71,72 Moreover, research on SARS has highlighted the significant role of self-efficacy in mitigating mental health concerns. 73 Given these considerations, we speculate that digital health literacy may mitigate the occurrence of mental health issues by boosting individuals’ general self-efficacy. Furthermore, research suggests that individuals may experience anxiety or stress when they cannot comprehend or locate health information. 74 Previous studies have indicated that despite the high frequency of social media usage among college students, obstacles in understanding and evaluating information persist. 16 This finding may elucidate the negative association between digital health literacy and mental health issues within the college student population.
Furthermore, our study revealed a negative impact of self-reported health on fear of COVID-19 and depression among university students, which was consistent with previous studies.75,76 A study conducted in Ecuador has found a significant and independent association between self-reported health status and depression. 75 The negative relationship has also been demonstrated by an investigation conducted in Poland. 76 Previous studies have demonstrated that mental health issues are highly prevalent among adolescent populations with chronic medical conditions, which may be exacerbated by the COVID-19 pandemic. 77 This finding highlighted the importance of conducting mental health assessments for youth with pre-existing health conditions during the pandemic.
In addition, our study found that university students who were female and in medical school had higher scores for fear of COVID-19 in univariate analysis. Many studies have verified that women have higher fear during the COVID-19 pandemic, which may be due to women's greater emotional reactivity. 78 Medical students were required to be in hospitals or other healthcare facilities for internships or clinical courses during the investigation period and had a higher risk of infection. 79 This could be the potential explanation for the higher levels of fear of COVID-19 among medical students.
While research suggested that college students face a relatively low risk of COVID-19 infection, 80 our study indicated a remarkably low percentage of students who either self-reported a COVID-19 infection or were exposed to COVID-19 cases. This contrasts with the 7% self-reported infection rate among American university students. 81 This difference may be attributed to the rigorous public health policies implemented in China. During the initial COVID-19 outbreak, Chinese universities suspended in-person classes, mandating home isolation for all students. Subsequently, online education became the primary mode of instruction in Chinese higher education. Even after the return to in-person classes, universities across China continued to implement strict preventive measures, such as restrictions on gatherings, social distancing, and mask-wearing. 82
Conclusions
This study explored subtypes of digital health literacy among university students and their impact on mental health during the COVID-19 pandemic. Utilizing latent profile analysis, three distinct profiles were identified: a low digital health literacy group, a moderate digital health literacy group, and a high digital health literacy group. The low digital health literacy group exhibited lower scores across all items compared to the other two groups, while the high digital health literacy group demonstrated higher scores across all items. University students’ digital health literacy displayed a significant negative correlation with fear of COVID-19 and depression during the COVID-19 pandemic.
Limitations
We acknowledge several limitations in our study. First, due to the cross-sectional design, establishing causal relationships between variables was challenging. While we can establish an association between university students’ digital health literacy and their mental health, causation remains uncertain. Hence, additional prospective cohort studies are needed to clarify this relationship. Second, our study participants were exclusively from a single comprehensive university in China, which may restrict the generalizability of the research findings. Future studies are advised to consider diverse settings for participant selection. Third, most university students in our study were not directly or indirectly exposed to COVID-19, limiting the generalizability of our findings to other populations with higher exposure rates.
Despite certain limitations, our study utilized a latent profile analysis approach to reveal three distinct digital health literacy profiles among university students and examine associations between their digital health literacy and mental health during the COVID-19 pandemic. By conducting a “person-centered” latent profile analysis, we compensated for the shortcomings of previous research which obscured the heterogeneous profiles. This study can provide practical guidance for teachers and policy makers, including targeted digital health literacy education based on the unique characteristics of each subgroup and timely psychological counseling.
Footnotes
Acknowledgements
The authors would like to thank all the study investigators, research coordinators, and participating students.
Contributorship
Xihe Yu and Dahai Yi contributed to the formulation of the research design, coordination, and manuscript composition. Liangwen Ning participated in conceptualizing and designing the study, data collection, data analysis, and drafting the manuscript. Zhou Zheng contributed to the revision of the analytical framework and data interpretation. Minghui Liu, Shang Gao, and Xin Yang participated in data analysis and revising the manuscript. Jiasi Bi contributed to the study design and data collection. All authors reviewed and approved the final version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethics approval for the study protocol was obtained from the Medical Ethics Committee of Jilin University. IRB code is No. 2022-11-05. Informed consent was obtained from all participants through online responses before the start of the survey.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Health Commission of Jilin Province (grant number 2021GW002).
Guarantor
XY and DY.