
Abstract
Background
Music attuned technology – care via eHealth (MATCH) supports caregivers to use music-based strategies to enhance the care of people with dementia. It comprises a mobile app with an embedded training programme co-designed by music therapy experts and service users. This article presents findings from the first MATCH trial in the community.
Methods
Thirteen dyads (caregivers and care-recipients) trialled MATCH in an 8-week pre-post single-arm proof-of-concept study. We evaluated the acceptability (Acceptability E-Scale (AES)) and usability (System Usability Scale (SUS)) of MATCH, knowledge gain (Knowledge Assessment), and preliminary effects of MATCH strategies on mood and agitation (Neuropsychiatric Inventory Questionnaire (NPI-Q); Cohen-Mansfield Agitation Inventory (CMAI)). Caregivers also completed weekly check-in interviews and maintained a paper diary, where they reported their use of MATCH (adherence) and any perceived effects; this data was analysed using thematic analysis.
Results
Participants found MATCH acceptable (combined AES median score of 28, range 25–34) and useful (SUS median score of 73.5, range 55–100). NPI-Q scores showed a reduction in the severity of neuropsychiatric symptoms of dementia (median change: −5, 95% confidence interval (CI): −9, 0) and associated caregiver distress reduction (median change: −7, 95% CI: −13, 0). Qualitative findings revealed overall positive impacts of MATCH, including perceived benefits for mood, cognition, engagement and connectedness, easing personal care, and reducing agitation and caregiver stress. Additionally, findings highlighted barriers, enablers, and instances where MATCH was less helpful.
Conclusion
MATCH has the potential to help people with dementia and caregivers develop new music-based routines that can support wellbeing and connectedness and reduce distress.
Background
Dementia is a global public health concern. The number of people living with dementia worldwide is projected to increase from an estimated 57 million in 2019 to 153 million by 2050. 1 Remaining at home for as long as possible is associated with improved health and wellbeing outcomes,2–4 and significant economic benefits. 5 In Australia, approximately 67% of people with dementia reside in the community, 6 with potentially higher rates globally. 7
Informal caregivers, such as family members or close friends, provide an average of over 40 hours of care per week to people living with dementia living at home.5,8 While caregiving can have positive aspects, it is also associated with stressors such as grief, insufficient resources, competing demands, and behavioural and psychological symptoms of dementia (BPSD) in the care-recipient.9–14
BPSD, particularly agitation, significantly impacts caregiver resilience and quality of life, 15 and contributes to increased care costs. 16 These behaviours are a leading factor in the early transition to long-term care, 17 which negatively impacts both the person with dementia 18 and their caregivers. 17 Treating neuropsychiatric symptoms is challenging, with pharmacological treatments increasingly recognised as sub-optimal due to concerns around efficacy, contraindications, and polypharmacy risks.19–23 Non-pharmacological interventions for caregivers include acceptance and commitment therapy, behavioural activation, mindfulness, multi-component intervention, psychoeducation, and cognitive behavioural approaches, which show inconsistent effects. 24
Music therapy has evidence from systematic reviews and randomised controlled trials demonstrating significant psychological, emotional, and cognitive benefits.25,26 These include reductions in BPSD and depression, especially for people with severe symptoms. 27 However, expanding access to music therapy services faces many barriers, including a shortage of trained music therapists, lack of standardisation in music therapy approaches, and difficulty integrating programmes into healthcare systems.26,28 These challenges highlight the need for innovative solutions to scale music interventions. 29
There is a growing evidence base for the use of technology to support care at home for people with dementia.30,31 The use of music technology to support enjoyment, engagement, and connection in dementia care has been explored in both community and formal care contexts.32,33 However, there is minimal research to date that examines the use of music technology for strategic care purposes.34,35
Family caregivers play a crucial role in the care of people with dementia, drawing on their familiarity with the person's preferences and using music to personalise music experiences, curate personalised play lists, and evoke autobiographical recall. 36 Empowering family caregivers to integrate music intentionally into daily care can enhance engagement in caregiving, create meaningful moments of connection, and improve outcomes for people living with dementia. 37 Providing caregivers with education and support to strategically incorporate music into daily care routines can improve outcomes for caregivers and people with dementia. 38 Technology offers a scalable solution for caregiver training and intervention delivery.39,40
Background to music attuned technology – care via eHealth
Music attuned technology – care via eHealth (MATCH) integrates a music therapy-informed caregiver training (MATCH Training) into a mobile application (MATCH App) and aims to support caregivers of people with dementia who experience agitation and other neuropsychiatric symptoms. The MATCH Training is embedded in the MATCH App; caregivers are guided to complete video modules that demonstrate how music-based strategies can be used to support someone with dementia. The MATCH Strategies draw on music therapy principles and are based on several developed iterations of in-person caregiver training delivered by a credentialed music therapist.38,41
The MATCH Training begins with two mandatory modules that introduce the general concepts and science behind using music to support care, while up to five other modules are recommended based on an in-app assessment of caring needs. Modules include guidance on how to implement MATCH Strategies, including using music to de-escalate agitation and regulate mood (attunement), support personal care tasks, and promote relaxation, reminiscence, and movement and exercise. MATCH Strategies are intended for caregivers to use both pre-emptively and in the moment to reduce neuropsychiatric symptoms and promote overall wellbeing. Content and face validity of MATCH Training has been tested by expert music therapists and caregivers, who assessed it as clear, accurate, and relatable. 42
In addition to training, the MATCH App provides an in-built music streaming player, which enables users to build playlists based on music therapy principles and strategies that they learn throughout the training. Sample playlists are provided as an example for caregivers, however, the importance of creating personalised playlists is emphasised throughout the Training and the App itself. The MATCH App prototype was developed using user-centred design principles, which aimed to support caregivers in implementing these strategies and measuring their impact. 43 In this prototype stage, the Training and App were designed for use by caregivers supporting people with dementia who experience agitation and distress. The prototype App reported in this paper was the first iteration and was designed for the purpose of this research. Following feedback reported here, we are planning future iterations of MATCH to ensure it is fit-for-purpose, can be integrated seamlessly into day-to-day life, and includes design for use by people with a diagnosis themselves. Further information about the design of the MATCH Training and App has been published elsewhere.40,42Our previously published qualitative study focused on the experience family caregivers who participated in this initial 8-week trial of the MATCH prototype. Findings from this study revealed that caregivers reportedly experienced enhancements to their care partnerships and day-to-day management of care needs, while there were barriers and enablers to adapting MATCH to their unique contexts. 40 This paper reports the main findings from this mixed-methods single-arm proof-of-concept study, 44 which evaluated the MATCH prototype's acceptability, usability, and preliminary effects on BPSD, caregiver distress, and caregiver knowledge.
Methods
Study design and data collection
This mixed-methods proof-of-concept study tested the MATCH Training and MATCH App prototype in an 8-week community-based trial. The prototype was available only to participants of this study; a detailed description of the functionality is reported elsewhere. 40 Participants completed pre- and post-trial assessments, post-trial surveys, and interviews to capture MATCH acceptability, usability, and user experience, changes in care-recipient neuropsychiatric symptoms, caregiver distress, and knowledge of how to strategically use music. Qualitative data (via diary entries, participant interviews, and weekly phone check-ins) were also collected to better understand the experiences and perspectives of participants. Data were collected remotely via phone or video calls, and online surveys using REDCap.45,46 Diary data were collected in printed diaries posted to participants; on return, these were scanned and uploaded to REDCap for secure storage, while physical copies were shredded. This study was approved by The University of Melbourne Human Research Ethics Committee (HREC). HREC Reference number: 2021-22807-24286-6. Australian and New Zealand Clinical Trials Registry number: ACTRN12622000193774.
Participants
Dyads comprising people with dementia and their nominated caregiver were recruited across Australia from July to October 2022, using purposive sampling via social media advertising, community dementia and aged-care networks, the Australian Step-Up for Dementia research database, and through previously collected expressions of interest to participate in music and dementia studies. Eligible dyads were required to be co-habiting caregivers and care-recipients with a diagnosis of mild cognitive impairment, or dementia, over the age of 18 years. Co-habiting refers to a dyad where the self-identified nominated caregiver lives on the same premises, is on call in close proximity, or is acknowledged by national guidelines as the main caregiver. Caregivers needed to be close in relationship to the person with dementia, including siblings, spouses, adult children, friends, nieces or nephews, and excluding formal paid caregivers. This criterion was included as caregivers needed to be present with the person they care for in order to implement MATCH Strategies. A formal or probable diagnosis of dementia was included, as in Australia, it can take a number of years to confirm an official diagnosis. 6
Exclusion criteria were: (1) dyads who had no access to the internet or a mobile device that could support the MATCH App, which was needed for study participation; (2) either member had a hearing impairment not addressed by hearing support technologies such as hearing aids; or (3) the caregiver did not have an adequate understanding of the English language. Training in other languages is planned for future versions of the MATCH App.
Measures
Demographic data
Demographic information was collected to provide context about the participants’ backgrounds, including age, gender, country of birth, languages, relationship status, and education history. Diagnoses, time since diagnosis, relationship between caregiver and recipient, and history of musical experience were also captured. As the focus of this study relates to neuropsychiatric symptoms, which can occur at any stage of diagnosis, we did not collect data relating to dementia ‘stage’ or severity. Due to the short-term nature and proof-of-concept design of this study, we did not measure decline in overall dementia symptoms.
Acceptability, usability, and user experience
Post-trial acceptability was assessed using a version of the 7-item Acceptability E-Scale (AES), adapted to relate to the MATCH App. 47 It employs a 5-point Likert scale to evaluate overall satisfaction, as well as the clarity and ease of use of the MATCH Training and the MATCH App. The AES provides a combined acceptability score by summing the item ratings resulting in a total score ranging from 7 to 35, with higher scores indicating greater acceptability.
Usability and design of the MATCH App were measured using the System Usability Scale (SUS). 48 The SUS is a 10-item measure each rated on a 5-point Likert scale. The SUS score is calculated by subtracting 1 from each odd-numbered question and subtracting the rating from 5 for even-numbered questions. All the adjusted scores are summed, and the total is multiplied by 2.5 to obtain the final SUS score (range 0 to 100). Higher scores indicate better usability and design. Benchmarks suggest that an SUS score of 68 represents an average usability score, while scores of 80 or higher indicate a good user experience. 49
Caregivers’ perspectives on their experiences of using MATCH were also sought through qualitative interviews. These have been published previously 40 and are summarised briefly in the ‘Background’ section. Further qualitative data on usage and user experience were captured via weekly check-in phone calls starting from week 2 following pre-trial assessments. These calls served to confirm usage and offer technical support; while the calls were targeted at caregivers, care-recipients were welcome to attend and provide feedback if they wished to do so. During the calls a checklist of usage-related questions was completed, supplemented by field notes based on phone call discussions. Additionally, caregivers had the option to document detailed notes on usage and impact in a diary.
Adherence
Adherence during the 8-week trial was captured based on data collected through the weekly phone calls (conducted by ZT and DV). Data from the optional usage diary was used as a secondary source for adherence data. Adherence was defined as using the MATCH App and/or Strategies at least twice per week for a minimum of 6 weeks within the 8-week intervention period.
Preliminary effects
BPSD were assessed pre- and post-trial using the Neuropsychiatric Inventory Questionnaire (NPI-Q) 50 and the Cohen-Mansfield Agitation Inventory (CMAI). 51 For NPI-Q, we calculated score estimates for the severity of BPSD (score ranging from 0 to 36), distress for the caregiver (score ranging from 0 to 60), and NPI-Q severity validated sub-scales 52 : (i) NPI-Q-4-Agitation/aggression comprises the items ‘agitation/aggression’, ‘disinhibition’, ‘irritability/lability’, and ‘motor disturbance’ (score ranging from 0 to 12); (ii) NPI-Q-3-Mood includes ‘depression/dysphoria’, ‘anxiety’, and ‘irritability/lability’ (score ranging from 0 to 9); and (iii) NPI-Q-4-Frontal includes ‘elation/euphoria’, ‘apathy/indifference’, ‘disinhibition’, and ‘irritability/lability’ (score ranging from 0 to 12). Caregivers’ knowledge about using music in dementia care was assessed pre- and post-trial using a 25-item Knowledge Assessment developed by the research team.
Procedures
Following screening, caregivers completed a pre-trial assessment capturing sociodemographic information, NPI-Q, CMAI, and Knowledge Assessment scales. After completing these assessments, caregivers were provided with a link to download the MATCH App (prototype version). They were guided to log in and complete the MATCH Training independently. For those requiring technical support to access the app, a 1-h Zoom demonstration was offered. Upon login, caregivers accessed two training videos introducing the MATCH concept and the science of using music in dementia care. An assessment within the app then determined guided the caregiver towards the training modules best suited to meeting their needs and the care-recipient's needs. Caregivers were asked what areas of care they felt they required the most help with, and what areas they felt the person they cared for would benefit from the most. Questions were related to mood, personal care, physical fitness, energy, connection, and engagement. The five available training modules were designed by music therapy researchers, based on music therapy principles, and validated by music therapy and caregiver experts. 42 Each module contained an instructional video introducing the concept of how music could be used to support the needs of the participants, followed by two to three demonstration videos, which provided examples of how to use music-based strategies in different scenarios. Supplementary information was provided in text within each module, including frequently asked questions and suggestions for actions to take when the proposed strategies did not work. More information about the training modules can be found in our previous publication. 42
After completing the training, caregivers were prompted within the MATCH App to create personalised music playlists tailored to the care-recipients interests and needs. Content within the training highlighted what musical parameters are useful for the different needs in each scenario, which informed caregiver selection of music for the various playlists.
Caregivers were encouraged to use the MATCH App and/or Strategies for 8 weeks (minimum of 2 × 30 min per week). To support adherence, a member of the research team conducted weekly phone calls to confirm adherence to the usage guidelines, collect preliminary data on usage and impact of the MATCH App and Strategies, and troubleshoot any technical difficulties experienced throughout the study. Participants were also provided with an optional diary to record their experiences after each use of MATCH Strategies. Post-trial assessment included the AES, SUS, NPI-Q, CMAI, and Knowledge Assessment scales. Post-trial, participants were allowed to retain the tested version of the MATCH App.
Data analysis
Demographic and pre-trial variables of caregiver and care-recipient participants were summarised and presented using frequencies and percentages for categorical variables, mean and standard deviation for continuous variables, or median and range (minimum and maximum) for non-symmetrical continuous variables. The use of music in daily life, its importance for caregivers and care-recipients in the past, and technology literacy were summarised and presented using frequencies and percentages.
Adherence data (usage per week), post-trial acceptability (AES), and usability (SUS) non-symmetrical continuous variables were summarised using the median and interquartile range (25th and 75th percentiles).
Changes from pre- to post-trial (NPI-Q, CMAI, and Knowledge Assessment) were analysed using Wilcoxon signed-rank tests, and Hodges–Lehmann's median differences for paired samples were calculated with 95% confidence interval (CI). All statistical analyses were conducted using STATA/SE 18.0. 53
Qualitative data from weekly check-in field notes and participant diary entries were analysed using a six-step inductive thematic analysis method, 54 managed using MAXQDA software. 55 Primary analysis was completed by ZT; themes were discussed and finalised with members of the wider research team.
Results
Participant characteristics
Twenty-five dyads expressed interest in participating in the study, and 23 were screened. Three dyads were ineligible because they were not co-habiting. Eighteen dyads consented and completed pre-trial assessments, but one withdrew before receiving the trial demonstration. Seventeen dyads commenced the 8-week trial, and 13 completed. Reasons for withdrawal included care-recipient's hospitalisation (n = 1), caregiver illness and change in circumstances (n = 2), and lost to follow-up (n = 1) (Figure 1).

Study flow diagram, based on the CONSORT statement. 56
Among the 17 dyads that began the trial, most participants living with dementia (median age 79 years, range 62–93) and caregivers (median age 60 years, range 31–84) were female (11 (65%) and 14 (82%), respectively) and born in Australia (12 (71%) and 13 (76%), respectively). Nine (53%) caregivers were spouses or de facto partners, and eight (47%) were adult daughters (one granddaughter). Eight (47%) care-recipients were diagnosed with Alzheimer's disease; three (18%) had young-onset dementia (<65 years of age). Twelve caregivers (71%) had additional support from other family members but held the main responsibility for caregiving ≥80% of the time. Twelve dyads (71%) reported listening to music at least once a day prior to the study (Table 1).
Pre-trial characteristics of care-recipient and caregiver participants.
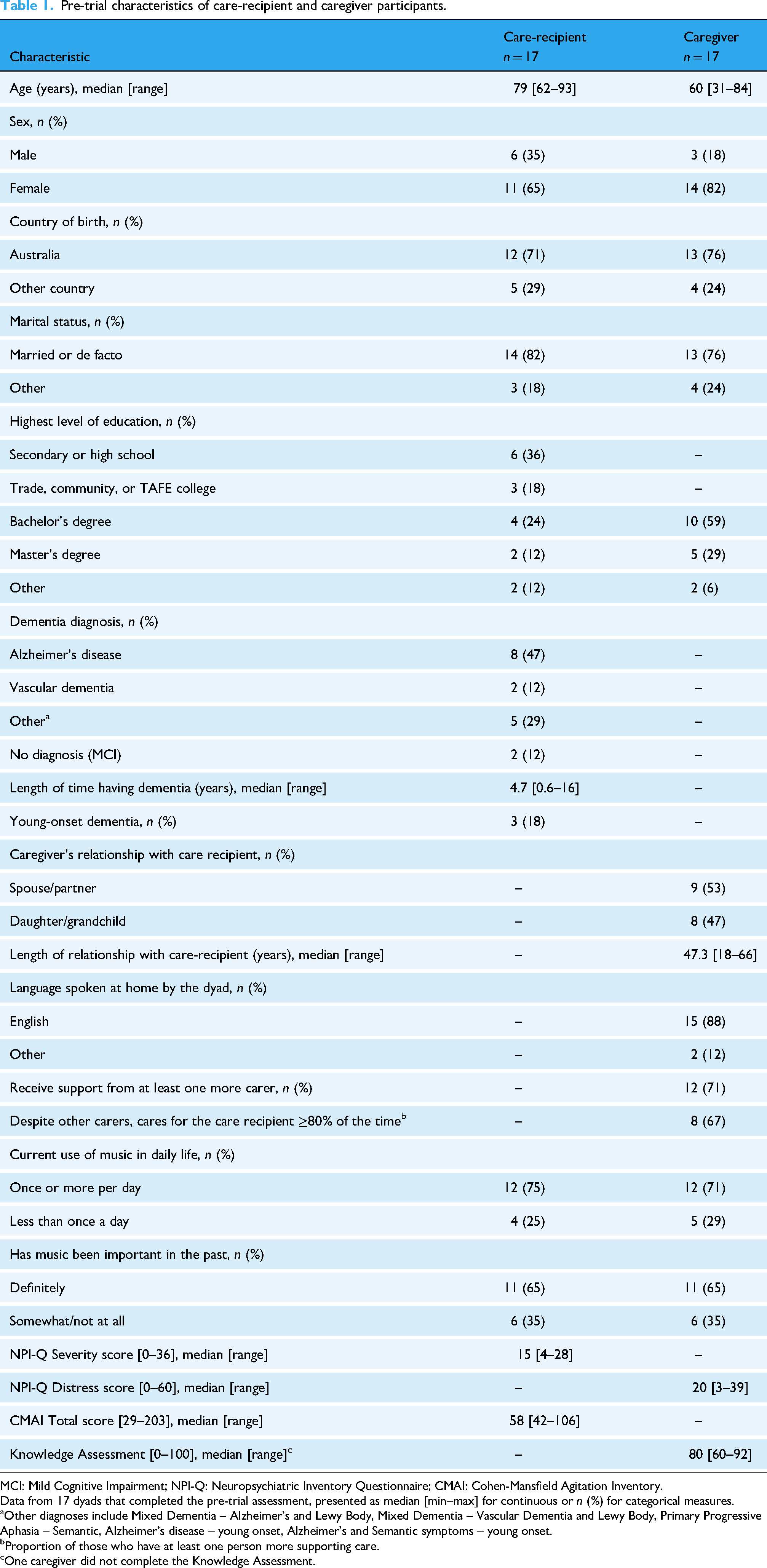
MCI: Mild Cognitive Impairment; NPI-Q: Neuropsychiatric Inventory Questionnaire; CMAI: Cohen-Mansfield Agitation Inventory.
Data from 17 dyads that completed the pre-trial assessment, presented as median [min–max] for continuous or n (%) for categorical measures.
Other diagnoses include Mixed Dementia – Alzheimer's and Lewy Body, Mixed Dementia – Vascular Dementia and Lewy Body, Primary Progressive Aphasia – Semantic, Alzheimer's disease – young onset, Alzheimer's and Semantic symptoms – young onset.
Proportion of those who have at least one person more supporting care.
One caregiver did not complete the Knowledge Assessment.
Caregivers in this study were experienced in using technology, such as computers, mobile devices, and applications. However, they self-reported less experience with music-specific apps, sound devices, and dementia-specific apps (Figure 2).

Pre-trial – caregivers’ experience with technology.
Reasons for use
At initial log-in, caregivers completed a needs assessment in the MATCH App, which linked them to relevant training modules. Check-ins and/or diary entries revealed self-reported reasons for using MATCH Strategies, which aligned with the app's needs assessment (Figure 3). However, qualitative findings revealed more nuanced purposes that informed later training development (Supplemental material 1). Participants were generally successful in adapting the principles taught via the MATCH Training to their individual circumstances, though some sought additional clarification during the weekly check-in calls.

Reasons for using MATCH based on initial ‘In-App’ assessment and weekly check-in data. MATCH: music attuned technology – care via eHealth.
Adherence
Thirteen dyads completed the trial, with pre- and post-trial assessments occurring a median of 79 days apart (range 57–182 days). Some participants paused due to illness or unplanned holidays, and one participant paused a week due to technological challenges (Dyad 10). Due to low recruitment numbers and the exploratory nature of this study, we adopted a pragmatic approach and allowed these participants to resume when they were able to. Therefore, the 8-week trial period was extended for some participants, and the time between pre-post was not consistent with the 8-week trial period. The following information reports on data collected during weeks when participants were active in the study. During the 8 active weeks, caregivers reported using MATCH more than the recommended minimum of two times per week with a median of four uses per week during weeks 3 to 5. Usage patterns varied with mornings more common during weeks 2, 3, and 6 while afternoons were frequent during weeks 4 and 8 (Table 2).
Use of MATCH from week 2 to 8 (adherence based on phone calls).

MATCH: music attuned technology – care via eHealth.
Data from dyads that used MATCH during the trial are presented as median [min–max] for continuous or n (%) for categorical measures. Week 1 was used to install the app and start the training, with no phone calls from the researcher.
Proportion related to the number of dyads who used MATCH that week.
Acceptability and usability
The MATCH Training had high acceptability (median 4 (range 3–5)), with caregivers considering it understandable and helpful. The MATCH App was rated easy to use (median 4 (range 3–5)) and helpful in delivering training (median 4 (range 4–5)), resulting in a combined acceptability median score of 28 (range 25–34) (Table 3).
Post-trial acceptability scale.
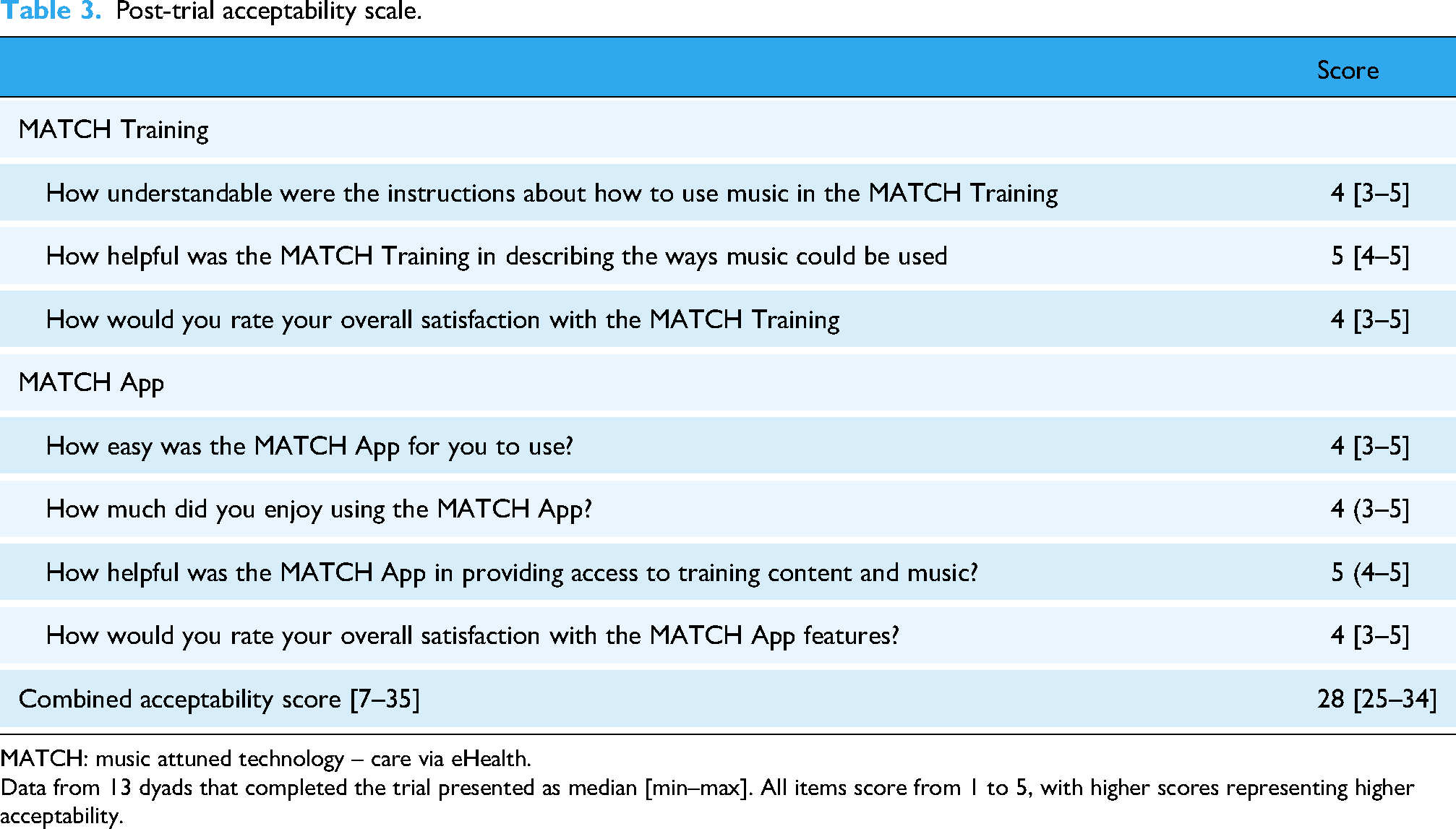
MATCH: music attuned technology – care via eHealth.
Data from 13 dyads that completed the trial presented as median [min–max]. All items score from 1 to 5, with higher scores representing higher acceptability.
The SUS's median scored a median of 73.5 (range 55–100), indicating that the prototype MATCH App was usable and acceptable. Participants appreciated its integration and expressed a willingness to use it frequently (Figure 4).

Outcomes of the System Usability Scale (SUS). 41
Technical events
Throughout the study, there were a number of technical events that impacted participants’ ability to use the MATCH App. In most cases, participants were able to correct the problem independently or use an alternative music player to implement MATCH Strategies. Table 4 describes the types of technical events and impact for participants.
Technical events.

MATCH: music attuned technology – care via eHealth.
Preliminary effects
Between pre- and post-trials, we observed a difference in NPI-Q severity and distress scores, with median changes of −5 (95% CI: −9, 0) and −7 (95% CI: −13, 0) points, respectively. Changes in Mood (median pre- to post-trial difference of −1, 95% CI: −3, 1) and Frontal sub-scale scores (median pre- to post-trial difference of −1, 95% CI: −3, 0) suggested that music may have had a positive impact on symptoms such as depression, anxiety, irritability, and apathy. However, although there was an estimated reduction in the median NPI-Q Agitation sub-scale of −1 (95% CI: −3, 1), consistent with findings for the CMAI total score (median difference of −3, 95% CI: −13, 6), by Wilcoxon matched-pairs signed-rank test, they were not statistically significant. Conversely, a change in knowledge was observed after MATCH Training and the use of MATCH Strategies by caregivers at the post-trial assessment (8, 95% CI: 0, 16) (Table 5).
Pre- and post-trial outcomes.

NPI-Q: Neuropsychiatric Inventory Questionnaire. Sub-scales: NPI-Q-4-Agitation/aggression [agitation/aggression + Disinhibition + Irritability/Lability + Motor Disturbance]; NPI-Q-3-Mood [Depression/Dysphoria + Anxiety + Irritability/Lability]; NPI-Q-4-Frontal [Elation/Euphoria + Apathy/Indifference + Disinhibition + Irritability/Lability].
CMAI: Cohen-Mansfield Agitation Inventory; CI: confidence interval.
Data from 13 dyads that completed post-trial assessment, presented as median (interquartile range, 25th to 75th percentiles); min–max scores of each scale and sub-scale are between [].
The intervention effect was estimated using Hodges–Lehmann's median differences for paired samples with a corresponding 95% confidence interval.
Wilcoxon matched-pairs signed-rank test.
Qualitative findings
Analysis of qualitative data collected via weekly check-in calls and diaries revealed insights into how dyads engaged with MATCH, app usage, perceived impact, barriers, and enablers. Additionally, these findings provided context for how participants experienced dementia-related and other challenges during this time. Data from 14 caregivers who completed a minimum of 4 weekly check-ins were included in this analysis. While care-recipients were welcome to contribute, they generally either declined or were unable to participate in the check-ins due to their diagnosis; three care-recipients provided feedback directly on at least one occasion during a weekly check-in call; their feedback is denoted as ‘care-recipient reports’. Data presented below includes field notes recorded by members of the research team, as well as direct quotes from participant diaries.
Challenging symptoms
During weekly check-ins, caregivers rated and described the levels of agitation that care-recipients experienced that week (Supplemental material 2). While ratings showed that the majority of care-recipients experienced mild agitation across the study, qualitative data provided a deeper insight into the types of agitation and other symptoms experienced by care-recipients. Notably, some caregivers reported feeling uncomfortable with the term ‘agitation’ and tended to resonate more with words such as ‘irritable’ or ‘anxious’. Similarly, some caregivers observed behaviours often classified as signs of agitation, yet they felt these related to more ‘sensory seeking’ behaviours. This aligns with the pre-trial scores from the NPI-Q, which suggest that the sub-category of agitation was not the primary concern for this cohort (Table 4).
Impact of using MATCH
Overall, MATCH was described as positive and beneficial. However, some neutral and negative impacts were also reported. Figure 5 depicts the relationship between the sub-themes relating to the category of ‘impact’ that were deemed beneficial by participants.

Perceived benefits of using MATCH. MATCH: music attuned technology – care via eHealth.
New routines. Twelve out of 14 caregivers reported that they had developed new routines using MATCH Strategies in their day-to-day lives as a consequence of participating in the study. For several participants, this involved incorporating MATCH Strategies into personal care routines (Dyads 01, 07, 08, 09, 10), while others appeared to have developed routine music use as a means of engaging and connecting (Dyads 04 and 14). Some caregivers reported that they developed a routine of using music to help regulate their own emotions (Dyads 03, 11, 12), with one describing the music as having an ‘almost Pavlovian’ effect on her mood (Dyad 12). Three care-recipients (Dyads 03, 06, 12) also reported using music routinely for mood and relaxation.
Reduced agitation. Participants reported that using MATCH Strategies was effective for reducing agitation, both in the moment and more generally over the course of the 8-week intervention period: [Care-recipient] was very agitated, so we sat down together and listened to the music, and I stroked her hand, and her anxious breathing settled down … when I got up, [care-recipient] stayed sitting (as opposed to previous pacing) and closed her eyes and stayed there (eyes open after a few mins) for 15 mins until we had to go out (Dyad 09, diary). Observed reduction in wandering around house, more relaxed and generally in good spirits overall (Dyad 12, check-in).
In several instances, participants reported that using MATCH Strategies pre-emptively helped to prevent or delay the onset of agitation: [care-recipient] appears calm and happy, and [caregiver] believes that doing relaxation in the morning is helpful as a prophylactic for agitation later in day (Dyad 04, check-in). Music and MATCH … is making sundowning easier - helping [care-recipient] to be still and enjoying the moment - might reduce from 1–2 hours to only 1 hour of pacing … (Dyad 01, check-in).
Improved/maintained mood. In addition to agitation, MATCH Strategies reportedly had a positive impact on mood generally. Dyad 14 reported that they had been using MATCH primarily to ‘maintain positive mood’ as it ‘seem[ed] to help prolong engagement/energy levels’ (Dyad 14, check-in). One caregiver reported that using MATCH during and after mealtimes helped to make the care-recipient's mood ‘lighter and happier’ (Dyad 02, check-in).
Some care-recipients, who were in the earlier stages of dementia, were able to use MATCH playlists independently to self-manage their own mood. One care-recipient was able to ‘retreat and put on music’ independently when feeling ‘stressed when there are visitors’; the caregiver reported that this ‘seems to help’ during times that may otherwise be stressful (Dyad 06, check-in).
One dyad reported that ‘MATCH has prompted them both to get back into regular music listening’ (Dyad 03, check-in); other dyads reported that using music regularly had provided increased ‘joy/pleasure’ (Dyad 07, diary) and ‘improved mental state’ in the evening (Dyad 12, diary).
Relaxation. Incorporating MATCH relaxation strategies was seen to be helpful for care-recipients and caregivers alike. One caregiver described how he and his wife were often ‘in two different spaces’ in terms of their needs, but that the MATCH relaxation playlists were able to work for himself and the care-recipient in ‘both spaces’ (Dyad 10, check-in). Music-relaxation strategies were also seen to provide comfort to participants who experienced pain or distress. One care-recipient utilised relaxation playlists over prolonged periods to help cope with pain from a medical procedure (Dyad 04), while another caregiver reported that their care-recipient had a ‘fantastic’ response to relaxation playlists following an injury (Dyad 14, check-in).
Assistance with personal care tasks. Using MATCH Strategies to support care-recipients during personal care tasks was frequently reported and appeared to be particularly meaningful for caregivers. For some participants, MATCH Strategies helped to alleviate tension during support with activities of daily living, which enabled caregivers to ‘reclaim [their] time’ by making routines ‘more simple, less time required for support’ (Dyad 05, check-in).
Showering and grooming were often cited as stressful times where MATCH had been useful: … It did make the task less stressful, as it is hard for her with all the procedural instructions when getting her to wash her hands … She started to giggle as I sang ‘wash that man right out of my hands’…we were both giggling about our song. It did help with the task (Dyad 11, diary).
MATCH Strategies were also reported to help with mealtimes, including encouraging participants with dementia to eat: Very effective use at breakfast, as mum is often drowsy to the extent that she actually falls asleep eating … She had also lost weight, and it was very hard to encourage her to eat due to her lack of interest and tiredness. She required several prompts, and this was the same with taking her tablets and even drinking a cup of tea. There are only so many variations in ways to remind someone to keep eating/taking medications without sounding like you are a nagging (Dyad 07, diary).
Reduced caregiver stress. The use of MATCH Strategies helped to reduce the stress experienced by caregivers. For some, this was due to the reframing of previously tedious and stressful tasks via the use of music: When singing during care routines, it helps to keep both caregiver and care-recipient relaxed and in a good mood – care-recipient sees it as a bonding exercise too … It is helpful when assisting care-recipient to get dressed (e.g. if care-recipient puts top on back to front, caregiver can sing to help her change it. It is playful and care-recipient is more agreeable – avoids caregiver getting stressed and triggering care-recipient's agitation (Dyad 08, check-in).
For others, MATCH provided an increased understanding of why someone with dementia may act in certain ways, which helped them to cope with changing behaviours. One caregiver reported that ‘training from MATCH helped her to cope with agitated reactions from the care-recipient – understanding it's just what's happening, and not taking it personally, responding calmly, going with the flow, etc.’ (Dyad 04, check-in).
Using MATCH Strategies with their loved one also helped to encourage caregivers to use strategies for themselves. One caregiver described how she ‘… used [music] to calm myself. Brought me down from rage’ (Dyad 12, diary). Similarly, some caregivers reported experiencing vicariously improved mood upon seeing their loved one benefit from MATCH. One caregiver reported feeling ‘… happy and heartened – when he's happy, I'm happy’, after seeing her husband respond positively to MATCH (Dyad 05, check-in).
Increased engagement. Several participants reported introducing MATCH Strategies into their routine helped to increase the care-recipient's engagement. For some, this related to increased arousal, which in-turn increased engagement in day-to-day tasks and activities. One caregiver found that using music in the morning was ‘… helping [care-recipient] when “groggy” after waking up (due to medication change)’ (Dyad 03, check-in), while another ‘used [MATCH Strategies] to encourage energy in dull tasks’ (Dyad 12, check-in).
Increased energy and general engagement were important for care-recipients who had previously been withdrawn or experienced apathy because of their changing abilities. One caregiver reported that ‘music seems to be most helpful for engagement and reducing boredom …’, and that the care-recipient was ‘… less likely to fall asleep or scratch at her skin when [she had] the right music playing’ (Dyad 07, diary).
Music was seen to energise participants, which helped them engage in other activities. One caregiver described how she felt that ‘having familiar music on after dinner helps prime [care-recipient] to stay at the table and play some games together’ (Dyad 02, check-in).
Improved cognition. The increased arousal and engagement afforded by MATCH Strategies was, in some cases, seen to stimulate cognitive processes for care-recipients. Strategies taught in the Reminiscence module were particularly helpful in prompting conversation and triggering memories. One caregiver found that ‘sometimes [care-recipient] doesn't recognise self in pictures, but with addition of carols, she seemed to recognise more and more things and was able to talk about memories …’ (Dyad 12, check-in).
One care-recipient reported enjoying being able to ‘independently use music strategically’ for their own cognition (Dyad 03, check-in). This participant had recently disengaged from community dementia supports due to feeling like they were not at the same cognitive level as other attendees but felt that they were able to learn to use MATCH Strategies from ‘Relaxation’ and ‘Engagement’ modules to stimulate their own cognition. They reported that this helped them to engage in discussions about musical themes, which ‘amazed’ their caregiver, who felt this cognitive stimulation ‘might also be impacting other areas of [care-recipient's] life’ [Dyad 03, check-in].
Similarly, ‘stimulating conversation’ was another important impact of the strategies (Dyad 04, diary). Listening to music together helped one care-recipient to ‘initiate’ discussion about memories related to music (Dyad 02), while another reported that using the Reminiscence strategies helped to ‘promote speaking’ (Dyad 05).
Meaningful connection. Participants described ways in which MATCH Strategies helped to foster an increased sense of ‘connectedness’ (Dyad 01, check-in) between themselves and their loved one. For some, music provided an accessible and meaningful way to interact and connect with others: one caregiver described how she ‘… often hear[s] mum say she is bored … she has little opportunity to speak or to participate in any activity. These interactions with music, sitting and talking, looking at photos etc. give mum opportunities to engage in a meaningful way’ (Dyad 11, diary).
For others, this sense of connection evoked strong emotions for caregivers, who were heartened to be able to connect meaningfully with their loved one: … [It was] very positive for [care-recipient]. She took a while to look at … photos on the TV but once she started looking, she relaxed. She tapped to the music. Very successful for her, but it was so beautiful and nostalgic, it made me cry (Dyad 09, diary).
Inconsistent effects and contraindications
Although all participants reported experiencing benefits from using the MATCH App and strategies, there were several instances where MATCH was reported as having no impact, or in some cases, where the use of MATCH Strategies was contraindicated.
Several caregivers highlighted that while sometimes strategies worked well, occasionally they did not, and this was not always predictable. This was captured in a diary entry from Dyad 12: ‘No use at 12.30, worked at 4.30. Neither of us calmed down [at 12.30]. Helped save the day [at 4.30]’.
Another caregiver observed that the efficacy of strategies changed over time: ‘Initially it worked well; however, this week it did not seem to work. [Care-recipient] did not appear to become relaxed and was still agitated post-playlist’ (Dyad 08, check-in).
In some cases, caregivers reported that the music was overwhelming and either had no effect or led to increased agitation. One caregiver described an instance where the care-recipient ‘wandered off (despite having chosen [the song]’ and was ‘agitated by volume (despite having asked for it [to be turned] up)’ (Dyad 12, check-in). For some, it appeared that ‘music is perhaps not helpful for them past a certain threshold of agitation’ (Dyad 04, check-in). In some cases, mood regulation strategies were ‘… not really working so well; once [care-recipient] was escalated, doesn’t really respond to it’ (Dyad 05, check-in). Another caregiver speculated that ‘sometimes [care-recipient] just wants silence, especially when more agitated’ (Dyad 04, check-in). Music also occasionally appeared to trigger low/sad moods: ‘[care-recipient] found the [relaxation list] sad and a bit depressing so we turned it off’ (Dyad 02, diary).
Barriers and enablers to using MATCH
Participants identified factors that either prevented or enabled their use of MATCH each week.
Difficulty selecting appropriate music. The MATCH Training aimed to educate caregivers to select the most appropriate music to support their loved one, and the MATCH App provided pre-made ‘demonstration’ playlists to assist them in creating their own personalised versions within the app. However, findings revealed that selecting appropriate repertoire and creating personalised playlists was, at times, challenging for caregivers. Some caregivers reported difficulty in selecting music due to not knowing the care-recipient's preferences, and/or the care-recipient being unable to communicate their preferences (Dyads 04, 08). Some felt they would benefit from automated music recommendations (Dyad 10), and some dyads utilised the MATCH ‘demonstration’ playlists or used music on the television/radio, rather creating their own personalised playlists (Dyads 04, 11, 12). Some described the process of selecting appropriate music as ‘overwhelming’, requiring too much time (Dyads 07, 10), and at points, a process of ‘trial and error’ (Dyad 13). Simultaneously, caregivers recognised that selection of music was crucial to the success of the MATCH Strategy. Several noted that, in instances where non-preferred/unfamiliar was used (such as the demonstration playlists), the music was either not effective (Dyads 04, 10) or had a negative impact (Dyads 02, 06, 12).
Environmental distractions impacts success. Caregivers reported that environmental noise, such as televisions on in the background, heavy rain, and hospital noises, could have a negative impact on the care-recipient's willingness and ability to engage in music (Dyads 01, 02, 11). One caregiver also reported a limitation of using fixed speakers; as the care-recipient often enjoyed moving around the house, they frequently left the room with the music playing, and it was difficult for the caregiver to follow (Dyad 01). In instances where dyads co-habited with other family members, some caregivers reported competing interests prevented the implementation of MATCH Strategies. One caregiver described needing to wait until another family member had left the house before using strategies with the care-recipient, due to competing needs of the care-recipient and this family member (Dyad 11). Another caregiver similarly reported that the care-recipient was often triggered by the presence of another family member, which seemed to prevent MATCH Strategies from improving anxiety once the MATCH activities stopped (Dyad 08).
Frequency, timing, and dosage impact outcomes. Some caregivers found that changes to routine, such as the caregiver being away for respite (Dyad 04), the presence of visitors (Dyads 05, 11), illness (Dyad 04), or adverse experiences (Dyad 01), could be disruptive for care-recipients and consequently impact the care-recipient's outcomes following the MATCH Strategies. Contrastingly, with consistent use and the development of musical routines, caregivers observed improvements in how care-recipients responded to MATCH Strategies (Dyads 02, 05, 12). One caregiver reported observing that the care-recipient had developed a ‘learnt behaviour’ in response to hearing calming music, following frequent and consistent use of music as a prophylactic (Dyad 12).
Caregivers also noted that timing of using MATCH impacted how receptive care-recipients were to the strategies. Some found that, at times, care-recipients were more receptive to music-based strategies in the early afternoon (Dyads 04, 11). However, other participants frequently used MATCH in the morning (Table 2). This highlights the importance of person-centred approaches when selecting appropriate moments to implement MATCH Strategies.
Caregivers reflected on how the ‘dosage’ amount of music varied, with one highlighting how usage could range from 20 min to 1.5 h per day (Dyad 01). Some caregivers discussed concerns regarding lack of engagement, as their care-recipients were only able to engage for 15–30 min before becoming fatigued (Dyads 09, 11). In these instances, the weekly check-in phone calls provided reassurance and contextualisation to the participants that fatigue may become more common in dementia, and that any engagement is positive.
Personal characteristics influence receptiveness. Some participants highlighted how personal characteristics, including sensory preferences, sense of humour, and social roles in life prior to diagnosis, influenced how receptive the care-recipients were to MATCH Strategies. One caregiver reported that some of the strategies suggested in the MATCH Training for personal care were not appropriate for her situation, as the care-recipient was not receptive to use of humour and song, which was consistent with his life-long personality (Dyad 02). Conversely, another caregiver described how the care-recipient's willingness to engage in MATCH Strategies declined for a couple of weeks during the study, speculating that this may have been due to observed cognitive changes (Dyad 04).
Another caregiver described feeling that the care-recipient's past roles in senior management positions influenced his need for control (Dyad 06). A different caregiver similarly reported that while the care-recipient was open to using music to self-soothe, she disliked the thought of the caregiver using music for a functional purpose without her knowledge, and at times became suspicious at the suggestion of using music (Dyad 12). These instances highlighted the importance of collaborative and person-centred approaches, taking into account pre-existing preferences, and potential changes that may occur as dementia progresses.
Caregiver challenges. Caregivers described three primary barriers that impacted their ability to implement strategies learnt throughout the course of the trial period. Firstly, the time commitment to complete the training (Dyads 01, 03, 08, 10) and prepare the playlists (Dyads 07, 10) was challenging, and at times ‘arduous’ (Dyad 01). One caregiver felt that the number of videos precluded her from revisiting them during the trial period (Dyad 08). Some also reported that during certain weeks, they were unable to engage in MATCH Strategies as much as they would have liked to due to other tasks requiring their attention (Dyads 01, 03, 07).
Three caregivers reported that they had reservations about using their own voice to sing with and/or to the care-recipient (Dyads 02, 08, 13). This related to concern that the care-recipient would not be responsive (Dyads 02, 13), as well as the caregiver's own discomfort with singing (Dyads 02, 08). Other caregivers did not mention this directly but reported that they primarily used pre-recorded and/or instrumental music (Dyads 01, 03). A similar phenomenon was observed in relation to the willingness of caregivers to try the ‘attunement’ techniques suggested in the MATCH Training. Seven caregivers reported feeling reluctant, and at times even fearful, towards implementing the ‘attunement’ strategy when their care-recipient was already in an agitated state (Dyads 01, 04, 05, 09, 12, 13, 14). Sometimes, this was due to the caregiver not understanding how this technique works (Dyad 12), or disbelief that it could work in the circumstance where the care-recipient was already agitated (Dyad 04). There was some concern that using ‘attunement’ techniques would exacerbate the care-recipient's agitation (Dyads 01, 04, 12, 13); one caregiver described feeling that using the strategy at such a moment did not feel safe for her (Dyad 13). Others felt that using ‘attunement’ during night-time agitation was too disruptive for the caregiver, as it required energy and volume, which was not conducive for them to return to sleep (Dyads 01, 09). Some felt the ‘attunement’ strategy itself was too complicated for them to use during a moment of crisis; one participant described how she was often ‘just trying to get through’, so ‘thinking of things in the moment’ was challenging (Dyad 14, check-in). Ultimately, another caregiver acknowledged that not seeing immediate progress when trying a new strategy could deter them from trying the strategy again (Dyad 08).
Finally, three caregivers felt that engaging with MATCH Training or Strategies could trigger emotional responses in themselves. This sometimes made it difficult for them to review the training or implement the strategies. One caregiver felt reluctant to watch some training videos that depicted people who were further progressed in their dementia, as it made her fearful of what may happen in the future (Dyad 14). Conversely, one caregiver reported that witnessing the strategies work well made her feel emotional, as she witnessed abilities in the care-recipient that she thought were lost (Dyad 11). In each of these examples, the caregivers felt that having a warning/reminder for caregivers may alleviate some of the challenges associated with emotional reactions to the MATCH content.
Technological limitations. At times, participants reported technical challenges as a barrier to implementing strategies using the MATCH App (see Table 4). These issues typically related to moments where the MATCH App stopped working (Dyads 03, 04, 08, 10), or design issues (Dyad 10). Several participants similarly reported using alternative music play-back – such as other streaming services, CDs, or radio – citing a preference for the superior audio quality (Dyad 01) or greater ease due to familiarity with these technologies (Dyads 02, 03, 04, 05, 07, 10, 12, 13).
Understanding of training. The final potential barrier that emerged from the analysis related to limitations of the in-app training. During weekly check-ins, it became apparent that there were instances where caregivers had not clearly understood concepts from the training. This was identified via incongruence between the modules that they reported using, and the aims that they described when asked to clarify the impact of the strategies. The most common incongruence appeared to relate to the ‘attunement’ module; several participants described using the ‘relaxation’ playlist for the purpose of ‘attunement’, which was antithetical to the guidance from the training (Dyads 01, 02, 07, 09, 10). Additionally, several participants reported that they had solely used demonstration playlists, rather than create their own personalised versions, as instructed via the training (Dyads 04, 07, 08, 11, 12). Overwhelmingly, participants appeared to rely on the weekly check-in calls to seek clarification on parts of the training that they did not understand, or to troubleshoot and seek reassurance in instances where attempts to use MATCH Strategies were unsuccessful (Dyads 01, 02, 04, 05, 07, 08, 09, 11, 13). On some occasions, participants were unaware that they were misunderstanding strategies, and required prompts to re-visit the videos (Dyads 07, 13). Caregivers felt that re-visiting the training after having a chance to explore and trial the app was helpful, and that the refresher made implementing strategies much ‘easier’ (Dyads 07, 13).
Discussion
This proof-of-concept study investigated the acceptability, usability, and participant adherence to MATCH in community settings with caregivers and care-recipients living with dementia. We also assessed the preliminary effects of MATCH in reducing BPSD and associated caregiver distress. Findings indicate that participants found MATCH acceptable and useful, and care-recipients experienced benefits following the use of MATCH over 8 weeks.
We selected agitation and other associated neuropsychiatric symptoms of dementia as care-recipient outcomes to address the increased level of challenge these symptoms can present for informal caregivers, 15 as well as the lack of effective and safe non-pharmacological approaches. 23 The improvements observed in NPI-Q scores provide preliminary support for the use of MATCH as a suitable and effective alternative or supplement to pharmacological management of neuropsychiatric symptoms. The findings on Mood and Frontal sub-scales of the NPI-Q align with previous research, which showed that music-based interventions can have a significant impact on mood-related symptoms associated with dementia.25,57 While no improvement was observed in the Agitation sub-scale of the NPI-Q and the CMAI, it should be noted that overall pre-test scores for agitation were low, so this result may be due to floor effects and small sample size. Qualitative analysis of weekly check-in and diary data indicated that participants generally perceived a reduction in agitation or responsive behaviours. MATCH was seen as helpful in supporting care-recipients during personal care tasks, and building MATCH Strategies into regular routines was seen to protect against agitation. This supports existing research that has shown integrating music-based strategies into care routines to be helpful in reducing agitation and encouraging task completion.25,57,58 However, as some participants noted, there were times when MATCH Strategies were inconsistent in alleviating agitation. This may have been due to a range of factors, including how well the strategies were implemented, as well as potential external factors, such as varying causes of agitation. Further research is required to better understand whether different causes of agitation result in different responses to MATCH Strategies. 57
Some participants described feeling unsure about the terminology related to ‘agitation’, as they felt it implied aggression, which was not as commonly present, or felt stigmatising. However, the qualitative analysis revealed that terms such as ‘irritable’, ‘unsettled’, and ‘restless’ were used to describe behaviours that often related to more mild forms of agitation. Participants also made a conscious effort to highlight when agitated behaviour appeared to be due to an extenuating circumstance, such as having medical procedures, visitors, or worries about the future. This aligns with recent re-framing of ‘agitation’ in some areas of the literature, with a focus on ‘responsive behaviours’ and viewing BPSD in relation to environmental deficits rather than inherent symptoms of dementia. 19
MATCH is intended to be able to be used independently. In this study, the weekly check-in calls were intended only for data-collection and adherence purposes, and to provide technical support in the event the users experienced technical challenges that precluded use of the App. However, on several occasions, caregivers utilised these calls to ask questions or seek clarification on techniques and concepts taught via the MATCH Training.
For example, some participants reported that they did not resonate with the ‘attunement’ module, as it appeared to focus on agitation symptoms that were either uncomfortable to watch (in the training videos) or not close enough to their experience of milder symptoms. However, following discussion with the researcher during the weekly check-ins, participants were able to reframe their understanding of the module to suit their individual contexts. While this indicates that MATCH was able to be adapted to suit the unique and individualised needs of participants, it also highlights the need, at times, for a research team member (a clinical music therapist with experience in dementia care) to provide additional support to assist in implementation of MATCH Strategies. Although there has been an increase in research into skill-sharing approaches to music therapy and the training of caregivers in music-based strategies, the amount of support provided to caregivers in these approaches is currently highly variable in the literature.36,38,59,60 While the feedback from participants in this study will inform updates for future versions of the MATCH Training, more research is needed to better understand what level of additional support caregivers may need to understand and implement MATCH Strategies. This may include future iterations of the MATCH App with options to virtually consult a certified music therapist.
A notable finding from the qualitative analysis was that several caregivers were initially reluctant to try using ‘attunement’ in supporting care-recipients who were experiencing high levels of agitation in the moment. Our pilot study of the MATCH Training for professional caregivers working in a long-stay hospital setting similarly revealed that staff felt concern that adding higher energy music to initially match a person's heightened energy in such situations would escalate the care-recipient's current state. 61 Although attunement is a common and effective music therapy technique, it is possible that it may be too complex to teach virtually. It is also possible that for people in primary-care roles, the stress of having to ‘attune’ to someone in a volatile situation may outweigh the potential benefit of the strategy. Future versions of MATCH will provide more guidance in the training around this concept; however, more research is needed to understand whether this will be feasible. It may be that such strategies are better suited to in-person training, or to be implemented by a credentialed music therapist. On a few occasions, caregivers reported either no effect or contraindications of using music to support moments of agitation. This also highlights the importance of ensuring that any virtual training or music-based supports are informed by music therapy research and evaluated to ensure safety and effectiveness. Future versions of MATCH are being developed with appropriate warnings and advice for what to do when strategies do not work according to plan.
The version of MATCH tested in this study required participants to create personalised playlists within the app; playlists created in other programmes were required to be input manually. The qualitative analysis revealed that this task was overwhelming for several caregivers, either due to the time commitment required or uncertainty about the care-recipients’ music preferences. This aligns with our post-study interview findings, highlighting high reliance on pre-made playlists and caregivers’ challenges in navigating the user interface to create personalised playlists. 40 These findings confirm long-held music therapy principles relating to the importance of familiar and preferred music when using music to support people with dementia. 62 Future iterations of MATCH are exploring the use of algorithms to recommend appropriate and preferred music to suit the various support needs of people with dementia and their caregivers. Currently, there are several apps available on the market that purport to do this, however, the majority have not been rigorously tested to ensure that music recommended is the right music for the right moment.
Limitations and future research
While the findings of this study are encouraging, they should be interpreted with caution due to the small sample size and proof-of-concept design, and the fact that we did not control for external variables (such as changes to medication during the trial period). Additionally, the study was not powered to detect pre-post changes in care-recipient outcomes and had no pre-specified success criteria to evaluate feasibility and acceptability outcomes. Further research with more rigorous study design is needed.
It was initially intended that the MATCH App collect usage data, which would inform adherence. However, this feature was not developed in time for the study; the weekly check-in phone calls and paper-based diary aimed to compensate for this, by asking participants to report their usage each week. This approach is subject to recall bias, as participants’ recall may not accurately reflect the true use. The lack of care-recipient perspectives in our data is also an acknowledged limitation of this study.
Participants typically spent more time than anticipated during their weekly check-in phone call. At times, they sought additional support from the researcher (a clinical music therapist) in relation to technical challenges of using the device, as well as understanding of MATCH Training and Strategies. It is therefore possible that the support provided via weekly check-ins supplemented the MATCH Training; this should be controlled in future research.
Some participants experienced technological disruptions (either due to their own devices or issues with the MATCH App itself) that precluded them from using the app in the way it was originally intended. A notable example was that while participants were encouraged to design and use the playlists with specific song orders based on their preferences, the playlists would sometimes shuffle, or the app would errantly recommend additional music that did not always meet their needs. While these disruptions did not delay participation overall, they may have reduced the incidences where MATCH was successfully utilised. Although we collected qualitative data regarding technical challenges during the weekly check-ins, we did not log these systematically, and were therefore unable to provide a detailed overview of technical events. In future studies, increased rigour in app testing before deployment is needed to minimise interference from technical events, and comprehensive log is needed to enable analysis of technical events and the impact they may have had on adherence and usage.
Conclusion
This study found that the MATCH was acceptable and useful for caregivers and people living with dementia at home. Results suggest that the MATCH Strategies may help to reduce agitation and promote improved quality of life and connectedness for people living with dementia and caregivers. Findings from this study have been used to update the MATCH Training modules, and participant feedback has contributed to the co-design of the next iteration of the MATCH App. Further research is needed to test the updated version of MATCH and confirm these preliminary findings using more rigorous methods.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076251379768 - Supplemental material for Music attuned technology care via eHealth (MATCH): A proof-of-concept study for community-dwelling people living with dementia and caregivers
Supplemental material, sj-docx-1-dhj-10.1177_20552076251379768 for Music attuned technology care via eHealth (MATCH): A proof-of-concept study for community-dwelling people living with dementia and caregivers by Zara Thompson, Tanara Vieira Sousa, Dianna Vidas, Jeanette Tamplin, Jenny Waycott, Phoebe Stretton-Smith, Kate McMahon, Romina Carrasco, Robyn Woodward-Kron, Libby Flynn, Amit Lampit, Karen E Lamb, Sabine Braat, Nicola T Lautenschlager and Felicity Anne Baker in DIGITAL HEALTH
Supplemental Material
sj-docx-2-dhj-10.1177_20552076251379768 - Supplemental material for Music attuned technology care via eHealth (MATCH): A proof-of-concept study for community-dwelling people living with dementia and caregivers
Supplemental material, sj-docx-2-dhj-10.1177_20552076251379768 for Music attuned technology care via eHealth (MATCH): A proof-of-concept study for community-dwelling people living with dementia and caregivers by Zara Thompson, Tanara Vieira Sousa, Dianna Vidas, Jeanette Tamplin, Jenny Waycott, Phoebe Stretton-Smith, Kate McMahon, Romina Carrasco, Robyn Woodward-Kron, Libby Flynn, Amit Lampit, Karen E Lamb, Sabine Braat, Nicola T Lautenschlager and Felicity Anne Baker in DIGITAL HEALTH
Footnotes
Author note
Dianna Vidas is now at: School of Health and Rehabilitation Sciences, The University of Queensland.
Romina Carrasco is now at: Facultad de Comunicación y Artes Audiovisuales, Universidad de Las Américas, Quito, Ecuador.
Acknowledgements
We acknowledge the contributions of participants in this study and thank them for their time and commitment.
ORCID iDs
Ethical approval
This was approved by The University of Melbourne Human Research Ethics Committee (HREC). HREC Reference number: 2021-22807-24286-6. Australian and New Zealand Clinical Trials Registry registration number: ACTRN12622000193774.
Consent to participate
The participants (care-recipients and caregivers) provided written informed consent to this study.
Author contributions
FB initiated and led the study. FB, TVS, KEL, AL, NTL, JW, and JT obtained funding. FB designed the training content, and this was further developed by JT, LF, ZT, PS-S, KM, RW-K, and JW. RC designed the MATCH App version that was tested in this study. ZT and DV recruited participants, monitored the data collection, and were responsible for the qualitative data analysis. TVS was responsible for the quantitative analysis. SB and KEL revised the quantitative analysis. ZT, DV, JT, TVS, RC, LF, KEL, SB, AL, NTL, KM, JW, AV, RW-K, PS-S, and FB had access to the data and contributed to interpreting the data, drafting the manuscript, and approving the final version of the manuscript and had final responsibility for the decision to submit for publication. All authors contributed to the article and approved the submitted version.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The MATCH App version tested in this study was funded by and End of Year Appeal Initiative and The University of Melbourne Proof-of-Concept (PoC) internal grant, and the NHMRC-ARC Dementia Fellowship (1106603) received by Jeanette Tamplin. This Proof-of-concept study was funded through grants from the National Health and Medical Research Council (NHMRC) and Medical Research Future Fund (MRFF) (grant number MRFF2007411), and Google.org (grant number TF2309-115941).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Clinical trial registration
Data availability statement
The datasets presented in this article are not readily available because as this data relate to review of confidential content. Requests to access the datasets should be directed to ZT,
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.