
Abstract
Introduction
In 2020, more than 50 million people worldwide were diagnosed with dementia, and this number is expected to triple to 152 million by 2050. 1 Meanwhile, more than 80% of the total people living with dementia (PLWD) in the United States in 2017 were found to live in communities, either alone or with others—typically, spouses or other family members—while only 19% of them lived in long-term care settings. 2 These results project that more PLWD will live in community settings in upcoming years, which will significantly increase socioeconomic burdens not only on society but also on the family members living with PLWD.
Caregivers of PLWD need to perform essential daily caregiving tasks, such as helping PLWD with instrumental and personal activities of daily living (ADL) and providing care for other chronic conditions. 3 Managing the behavioral and psychological symptoms of dementia (BPSD), such as aggressive behaviors, agitation, and depressive mood, is also a task for caregivers. 3 When BPSD is not appropriately managed, caregivers of PLWD can experience increased stress and care burden.4,5 Based on informal caregiver reports, BPSD was the most common reason for institutionalization of PLWD. 6 Caregivers of PLWD should be able to efficiently manage BPSD at home to maintain their psychological and physical health and to promote healthy aging of PLWD in their own homes.
Recently, web-based or app-based cognitive assessments and machine-learning approaches have been widely applied for dementia diagnosis. 7 In-home behavior monitoring systems using technologies such as sensors and the Internet of Things have been increasingly developed for PLWD and showed promising results.7,8 Such technologies can help reduce barriers to participation in dementia care programs for those with transportation difficulties or visual/hearing impairments who might otherwise be excluded from such programs. 9 Although the widespread and practical application of such technology among PLWD is still in very early stages, 10 exposing PLWD to digital devices improved attitudes toward technology use and perceived usefulness among PLWD. 11
Several digital interventions using mobile apps and web-based programs have been developed to monitor and manage BPSD. For instance, a caregiver-centered web-based intervention, including remote BPSD assessment and psychoeducation for BPSD management, was effective in decreasing caregivers’ distress. 12 Similarly, a mobile app using a modified and digitally transformed version of the Neuropsychiatric Inventory (NPI) was helpful for caregivers. 13 Using information and communication technologies, such as robots, mobile applications, and smartphones, can help manage the overall BPSD of PLWD, especially depression and agitation. 14 Another mobile app employing digital reminiscence therapy decreased depressive symptoms in PLWD. 15 One recent review summarized that those technological interventions using multimodal sensors or in-home video recordings benefited caregivers of PLWD. These interventions reduced their care burden and depression. 8 This review also noted that the individualization of such technology is necessary and should involve both caregivers and PLWD in the interventions. 8 Individualization is a key component of person-centered care that can improve quality of life and diminish symptoms. 16 However, an easily accessible and remotely available BPSD management system that can be personalized for each person with dementia and their caregivers, is not yet available. 17
Both pharmacological and non-pharmacological interventions have been considered for BPSD treatment. Still, the latter is recommended as the first choice because of the high risk of adverse events associated with pharmacological approaches.18,19 Although various non-pharmacological interventions have been developed and tested among PLWD, only small effect sizes have been reported. 19 Nonetheless, an individualized approach to non-pharmacological interventions has shown superior improvement in BPSD compared to other non-pharmacological interventions or group-based sessions.19,20 A lack of real-time assessment tools that can accurately record the onset and types of BPSD is another possible reason for the small effect sizes. The NPI, one of the most used tools for BPSD, employs a retrospective rating system (up to 1 month) that could lead to recall bias. 21 These limitations necessitate developing a novel non-pharmacological approach to remotely monitor BPSD and provide individualized programs tailored to each person's preferences or functional status.
Therefore, this study aimed (1) to develop a mobile application (app) featuring a real-time BPSD diary, machine-learning-based BPSD prediction, and individualized non-pharmacological care programs and (2) to test the usability, acceptability, and preliminary efficacy of the app among PLWD and their caregivers. This study aims to develop a user-friendly home-based BPSD management program using mobile technologies and provide guidance for the first app upgrade before testing its effectiveness.
Methods
The development process of this Android-compatible mobile app comprised two phases: (1) software development and initial testing with experts and (2) beta-testing with end users who were PLWD-caregiver dyads. The intervention mapping protocol 22 guided the entire development process of this mobile app. The intervention mapping protocol is a stepwise and iterative process to develop a healthcare intervention that consists of the following six steps: needs assessment, objectives formulation, theory-based methods and practical strategies selection, intervention development, adoption and implementation plan, and evaluation planning. 22 This study was approved by the university's Institutional Review Board (No. 4-2021-0359).
Software development and initial testing
Needs assessment
According to the intervention mapping protocol, 22 needs assessment is the phase where researchers identify what is already known and not known about the problem and what further information is needed. In the present development, a literature review and face-to-face interviews were conducted as part of the needs assessment to guide further development. To identify the current state of knowledge, the research team conducted a rigorous literature review to assess the effectiveness of digital non-pharmacological interventions for managing BPSD and to identify the most appropriate types of non-pharmacological interventions conveyed by digital technologies. Understanding the appropriate and effective types of digital non-pharmacological care programs among PLWD and caregivers was necessary to develop an app that benefits target users. The review process has been presented in detail elsewhere. 14
In addition, before initiating the beta-testing process with PLWD-caregiver dyads, we conducted face-to-face interviews with them to understand their needs for the overall content and operational methods of digital non-pharmacological care programs at home and other preferences. These aspects were reflected in the care program content for each person. As we aimed to develop an individualized digital care program for PLWD and caregivers, conducting a needs assessment before beta-testing with the actual app users was imperative to create individualized content. Based on the existing literature, the team used a questionnaire to inform the app development process by assessing each person's preferences and personal memories (Supplementary Appendix 1).23,24 The questionnaire considered the end users’ traditional culture in Korea to ensure user-centered program content. The questions were embedded in the app so that the users could respond to the questions using the app.
Software development
The development process was iterative and incremental until the software reached a satisfactory condition, with continuous development, testing, modification, and retesting. 25 The mobile app was developed with the following features: a real-time BPSD diary using the app, machine-learning-based BPSD prediction using data from baseline questionnaires, BPSD diaries, actigraphy, and individualized non-pharmacological care programs prepared by the research team (Figure 1). The research team includes nursing professors with gerontological nursing expertise, graduate students in nursing, and software development engineers. The users—PLWD and their caregivers—were also involved in the development process by responding to the preference questionnaires and providing personal pictures for reminiscence so that the digital care program's content could be individualized. The dyads also participated in the interviews for needs assessment, usability, and acceptability assessment.

System flow of the mobile app. BPSD: behavioral and psychological symptoms of dementia.
In the present study, data security was achieved using a data cloud platform, Microsoft Azure (Microsoft, Redmond, WA, USA), to store, access, and retrieve personalized data. All data were saved without any identifiable information, and only the research personnel could access the stored Azure data using the designated login information.
Real-time BPSD diary. As the NPI, 26 though a widely used measure for BPSD, has a potential risk of recall bias, 21 the research team developed a BPSD diary by adapting the original NPI. The BPSD diary was developed based on the need-driven dementia-compromised behavior model 27 to assess the following 12 BPSD and associated caregiver-perceived triggers: delusion, hallucination, depression/dysphoria, anxiety, apathy/indifference, agitation/aggression, disinhibition, irritability/lability, elation/euphoria, aberrant motor behavior, sleep and nighttime behavior, and appetite and eating disorders. Detailed information regarding the BPSD diary can be found elsewhere. 28 In the current study, we embedded the BPSD diary into the mobile app so that the caregivers could record whether any BPSD was exhibited during the day, as well as the types and caregiver-perceived triggers of BPSD, if any. Each BPSD record was sent to the cloud server in real-time, and the research team could review and download the data from a web-based portal connected to the cloud server. We also embedded an alarm system into the app to remind the caregiver at least once a day if no records were saved on the server.
Machine-learning-based BPSD prediction. In a previous study, the research team developed a machine-learning-based BPSD predictive model and validated its accuracy among PLWD. 29 The predictive model was developed using demographic and health information (e.g., age, sex, dementia diagnosis), functional status (ADL), premorbid personality, actigraphy data for sleep and physical activity, and BPSD diaries recorded for 2 weeks at baseline. Several prediction models were employed using these data, including logistic regression, random forest, gradient boosting machine, and support vector machine. 29 Although these models showed different predictive performances across BPSD symptoms, the gradient boosting machine models showed the best performance in predicting BPSD, with a higher average area under the receiver operating characteristic curve (AUC) values across the symptoms (AUC > 0.8 except aberrant motor behaviors). This prediction function was installed in the mobile app in this developmemt. We then collected the baseline information and the BPSD diaries from each dyad for the first 2 weeks of the beta-testing period. After 2 weeks of data collection, the data were uploaded to the cloud server via the mobile app to operate the predictive function. Each dyad could perform symptom prediction in the app when available, and the app generated a list of predicted BPSD that were most likely to occur in each PLWD for informational purposes. As shown in the screenshot page (c) in Figure 2, among the 12 symptoms defined in the NPI, the top three symptoms ranked with the highest likelihood to occur in an individual were shown along with the likelihood percentages, and the next five most likely symptoms were listed below that.

Main features of the mobile app. Sample screenshots of the app for each feature: (a) BPSD records for types and duration, (b) BPSD records for severity and caregiver-perceived trigger, (c) BPSD prediction, (d) Individualized non-pharmacological care programs. BPSD: behavioral and psychological symptoms of dementia.
Individualized non-pharmacological care programs. Based on the questionnaire responses, the research team prepared music and reminiscence content tailored to each person's preferences and personal memories and uploaded them to the cloud server connected to each person's account. For reminiscence, we designed the app interface for each user to upload their preferred photos to the app for an individualized reminiscence session. For the exercise program, each user could choose their preferred video based on their perceived mobility status and preferences from several options in the app. Table 1 presents the content of each non-pharmacological care program. The participants were encouraged to use the care programs whenever they wanted but at least once per day. Because the developed care program aimed to be user-centered, participants were allowed to use any care program type they preferred among the four types available.
Detailed information on the individualized non-pharmacological care programs.
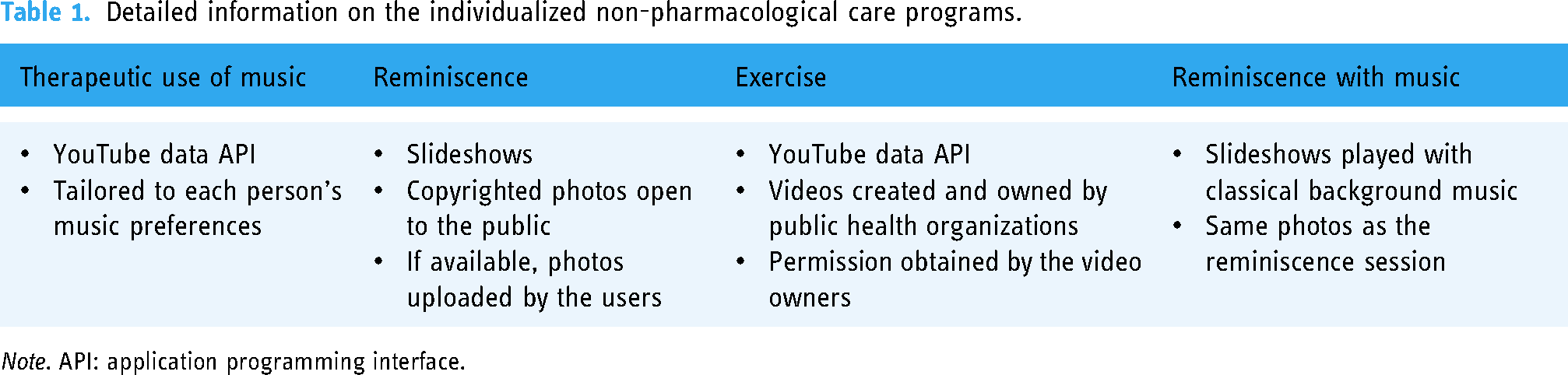
Note. API: application programming interface.
Initial testing with experts
After repeated tests and retests during the development process, the prototype was tested by five experts, including three content experts in nursing informatics or gerontological nursing and two technical experts in the digital health industry. These five experts were informed of the purpose of this study and agreed to participate in the initial testing. The experts were allowed to browse the app freely and asked to assess the quality of the app using the Korean version of the Mobile Application Rating Scale (MARS-K; expert version).30,31 With this measure, the app's objective and subjective qualities were assessed on the following five dimensions: engagement, functionality, aesthetics, information, and subjective quality. The subjective quality was assessed by asking how much they would recommend and how many times they would use the app, whether they would pay for it, and how much they would rate its overall quality. All items for each dimension are rated on a five-point Likert scale from inadequate to excellent. In this development process, a mean score for each dimension equal to or greater than three was considered a positive response. Their opinions on areas for improvement were also collected through an open-ended question. Immediate technical errors identified during the initial testing with experts that were deemed necessary to improve users’ usability and acceptability were addressed in the app's design before beta-testing with end users.
Beta-testing with end users
Participants and procedures
Following the software development and initial testing process, five pairs of PLWD and caregivers recruited by a convenience sampling method beta-tested the app for 3 weeks from 24 October to 23 November 2022. The research team provided each dyad with a tablet device (Galaxy Tab A8; Samsung, Seoul, Korea) with the downloaded app and taught them how to use it before testing. Eligible PLWD and caregivers were recruited as dyads from communities in Seoul, South Korea, using a snowball sampling method from communities or hospitals. The inclusion criteria were as follows: older adults aged ≥65 years who had a diagnosis of dementia, a Korean Mini-Mental State Examination (MMSE) score <24 32 and exhibited BPSD at least once a week (as evaluated by the Korean version of the NPI 33 ). Caregivers of eligible PLWD had to live with the older adults at their homes and be primary caregivers who provided direct care for prolonged hours in a day.
After obtaining signed informed consent from both PLWD and caregivers, each dyad used the app along with undergoing actigraphy (wGT3X-BT activity monitor; ActiGraph, LLC) for 3 weeks, which covered 2 weeks of baseline data collection and 1 week of digital non-pharmacological program participation. All users’ app usage, sleep, and physical activities were recorded in real-time and stored in a data cloud. The stored information could then be presented as a web portal so team members could monitor participants’ activities. All users were provided with written instructions on how to use the app. The users were allowed to contact the team members via phone whenever they experienced technical difficulties during the study period.
Measures
Usability and acceptability were assessed using the Korean version of the MARS-K (user version).34,35 Like the expert version of the MARS-K, the user version has the same scoring system with a five-point Likert scale from inadequate to excellent. Scores equal to or greater than three were considered positive responses. At the end of each program session, we asked how much each PLWD engaged in the session using a five-point Likert scale. Scores equal to or greater than three were considered satisfactory engagement levels in the present assessment. Program logs were created within the app to record users’ activities in BPSD diaries and non-pharmacological programs (i.e., types, time, and duration). Face-to-face interviews were conducted after the study with open-ended, semi-structured questions regarding their overall experiences with the mobile app. Preliminary efficacy was assessed by collecting the baseline BPSD symptoms of PLWD using the Korean version of the NPI, 33 Cohen-Mansfield Agitation Inventory (CMAI), 36 and Cornell Scale for Depression in Dementia (CSDD) 37 at the beginning of the study and by repeating the assessment upon the completion of the study as a follow-up. Caregivers of PLWD reported the baseline and follow-up BPSD symptoms.
Data analysis
Descriptive statistics for continuous variables were performed using Stata IC 15.0 (StataCorp LP, College Station, TX, USA). Statistical significance was not assessed because we performed beta-testing with a small sample size. The values obtained from the baseline and follow-up NPI, CMAI, and CSDD assessments were compared to assess the preliminary efficacy of the app in managing BPSD. Both MARS-K (user version) and log information on user activities in the app were analyzed using descriptive statistics to assess the app's usability. Each dyad's mean engagement level was calculated to assess the app's acceptability. The interview data from face-to-face interviews concerning needs assessment, usability, and acceptability of the app were evaluated. A semi-structured interview organized the interviews, which were audio-recorded. Two co-authors interviewed each participating dyad, PLWD and their caregivers with the same questions and recorded field notes. The interviews were later transcribed and independently reviewed with a content analysis method by two educated, experienced reviewers.
Results
Software development and initial testing
The literature review findings, reported elsewhere, 14 guided the initial development process. In the published review, 14 activity engagement interventions using digital technology that effectively managed BPSD included music, reminiscence, physical exercise, and robot-assisted or telehealth-based interventions. Among these identified interventions, the team chose to develop the prototype app accompanying music, reminiscence, and exercise as they were deemed to be deliverable through the app. In the needs assessment interviews, the five PLWD-caregiver dyads reported that they would favor care programs for managing dementia symptoms at home if the app were attractive and easy to use. They also reported that PLWD would be unable to use the app independently, and thus, the app should be easily operated so that caregivers can assist them with the app.
The app was developed after the iterative process, featuring a real-time BPSD diary, machine-learning-based BPSD prediction, and individualized non-pharmacological care programs (Figure 2). After the prototype app was developed, five content and technical experts tested it and provided feedback (Supplementary Appendix 2). The experts reported that the app had moderate objective and subjective quality based on MARS-K (expert version). Among the objective domains, engagement received the lowest score of 2.84, whereas aesthetics received the highest score of 3.67. The mean score for the overall objective app quality was 3.41, while the subjective app quality score was 2.4 (Figure 3). Some experts also provided feedback that the app should be easy to use and more age-appropriate (e.g., the person icon used in the menu interface) to better illustrate older adults as target users, as shown in Supplementary Appendix 2.

MARS-K scores of experts and users. MARS-K: Korean version of the Mobile Application Rating Scale.
Beta-testing with end users
Baseline characteristics
Five PLWD-caregiver dyads were enrolled. The age of PLWD was between 77 and 87 years, with MMSE scores ranging from 7 to 23 and ADL scores ranging from 7 to 20 (Table 2). Two caregivers were in their 50s, and the remaining were over 70 years old. All caregivers were female, including three spouses and two daughters of PLWD.
Baseline characteristics of study participants.

Note. PLWD: people living with dementia; MMSE: Mini-Mental State Examination; ADL: activities of daily living.
Usability, acceptability, and preliminary efficacy testing
Regarding the app's usability and acceptability, the MARS-K scores from the five dyads were as follows: engagement received the lowest score of 3.52, whereas aesthetics and information received the highest scores of 4.00. The average objective and subjective quality scores were 3.83 and 3.60, respectively. In all categories, the scores of the user group were higher than those of the expert group (Figure 3). Table 3 also summarizes that the dyads created BPSD diary events, ranging from 22 to 48, over the 3 weeks, indicating that the dyads created at least one BPSD diary record per day. However, the records suggested that the PLWD experienced no BPSD symptoms on most days during the testing period (Table 3). Among the four care programs, therapeutic use of music alone was most frequently used across the five dyads. The total time spent participating in the digital care programs for each dyad ranged from 106 to 204 min, and the engagement level of each dyad ranged from 3.38 to 4.94 on a scale of 5. To test the preliminary efficacy, baseline and follow-up BPSD symptoms were assessed using the NPI, CMAI, and CSDD (Table 4). First, the NPI scores decreased for all five users, with the average score falling from 12.2 to 8.4. The CSDD scores decreased for four users, with the average score decreasing from 7 to 5.8. The CMAI scores showed only minimal change, which slightly increased at follow-up.
Summary of the app's usability and acceptability among participants.

Note. BPSD: behavioral and psychological symptoms of dementia.
BPSD symptoms of the participants at baseline and follow-up (3 weeks post).

Note. BPSD: behavioral and psychological symptoms of dementia; NPI: Neuropsychiatric Inventory; CMAI: Cohen-Mansfield Agitation Inventory; CSDD: Cornell Scale for Depression in Dementia.
Interview results
A total of five dyads completed the face-to-face interviews. Only two dyads were able to participate as a pair, but most information was from the caregivers. Three other dyads could not participate as a pair because of the inability of PLWD to participate in the interviews, and thus, only their caregivers completed the interviews. During the interviews, some caregivers reported the immediate positive responses of PLWD to digital non-pharmacological interventions, especially therapeutic use of music or reminiscence. The examples of such statements were as follows: He said the song was good, and when he listened to it, it also made him laugh, so there's that. (P02, caregiver) Looking at pictures was nice, and listening to music was also good. (P03, caregiver)
The participants reported that one of the app's strengths was that they could choose the intervention types based on preferences or health conditions. For instance, some care program types, such as therapeutic use of music or reminiscence, were preferred over others, and thus, the choice could be individualized. One participant noted: Because he is like that, he was not really into exercising, but for singing and pictures, someone came and did it a bit. (P03 caregiver)
Another said that her mom enjoyed the individualized content: My preference … So, even in the music here, a song just came out, right? It's the song ‘Bi-Mo’ with a painting of Geumgangsan. Back in the day, when my mom attended high school, she sang this song as a solo performance during a school presentation. Right, Mom? What else was there? Oh, yes, ‘Dongsimchodo’ was like that too. But when I was a student in high school, when I played the piano for Mom during her presentation, she mentioned how challenging that song was. I think those things are nice. (P05 caregiver)
Some of the caregivers appreciated that they could participate in the program with PLWD and interact with them as follows: Every time I asked, ‘Where is this? When and where did you take this picture?’ You know, right? Yeah, I kept asking those kinds of questions. (P01 caregiver)
Another said: Even though we were both closing our eyes while looking at that, I blatantly sang for an hour. (laughs) … Thanks to this, I sang a lot of songs! (P02 caregiver)
The other strength of the app identified from the interviews was that the digital care programs were easily accessible at home. The users appreciated the fact that they could participate in such activities at home without going outside. One participant said: Exercise-related things, like, you know, on platforms like YouTube, I have to go in and search one by one. If everything is set up like this, it seems more accessible for me. (P04 caregiver)
The other dyad also reported: [Caregiver] Music too … [PLWD] As we’re getting older, it's not like we go out somewhere to do it. We just do it at home as a form of exercise. (P05, caregiver, and PLWD)
The interview data collectively suggested that the app needed upgrades in its content and design or layout (e.g., photo transition speed or size). Some participants especially mentioned the content: Songs came out, and pictures came out. However, when I looked at the pictures, it felt too monotonous. (P05 caregiver) So, I showed the photos this morning, and initially, when she saw them, it kept showing the same pictures. I guess it's because I didn’t add more diverse photos like this, so it's like, “It keeps showing the same pictures?” It's a bit regrettable that they’re not more diverse. (P04 caregiver)
As most of the caregivers were older adults, they reported challenges of using unfamiliar devices and the need for additional technical support from others. Firstly, she didn’t seem to handle machines very well, … it seems like she doesn’t really like machines in general … Because you’re not familiar with it. It's different from television, after all. (P04 caregiver)
The other also experienced difficulties with handling the new technology and thus needed additional support from others: I pressed the wrong icon, and some unrelated program popped up … I called the kids, and they helped me resolve it. (P02 caregiver)
All this verbal feedback on their overall experiences using the app later guided the preliminary app upgrades (Supplementary Appendix 2).
Discussion
The app development and beta-testing results in this study suggest that using digital technology, such as an app, could be an effective means for PLWD and caregivers to monitor and manage BPSD in their homes. Based on the MARS-K scores, the users appraised the app quality more positively than the experts. This may be because the users used the better-quality app with fewer technical errors. Some immediate technical errors identified during the initial testing with experts were addressed in the app before the beta test with users. However, direct comparisons between the scores would not be possible because some questions differed between the MARS-K expert and user versions. For example, the expert version has seven questions in the information domain, while the user version has only four questions.30,35
The users also provided positive feedback on digital non-pharmacological care programs, especially therapeutic use of music and reminiscence. The app was feasible, usable, and acceptable by PLWD and caregivers, as indicated by the outcome and app usage data. Specifically, decreased BPSD symptoms on the NPI and CSDD were observed in PLWD after using the app. Logs for the BPSD diaries and digital non-pharmacological programs were also created by users during the study period. Although the CMAI scores slightly increased at follow-up, we cannot confirm that the app expanded agitation because the results were not powered by a small number of participants.
Considering the existing digital approaches for assessing and managing BPSD, our app has several distinct strengths. First, our app enables ecological monitoring of BPSD for the types of symptoms, duration, severity, and caregiver-perceived triggers without recall bias. Although the current version of the app does not reflect the caregiver-perceived triggers recorded in the app in the individual care programs, the app still benefits caregivers by recording potential triggers for each observed symptom. Future development could assist caregivers in identifying unique patterns of triggers and related symptoms in each person and provide advice for addressing the triggers within the app. Second, it leverages machine learning to generate a list of predicted BPSD, allowing caregivers to predict the type of BPSD that most likely occurs in an individual before it manifests. Finally, digital non-pharmacological care programs in the app can be individualized based on preferences that can enhance overall user experiences and maximize the effectiveness of the programs.
Nonetheless, several limitations of the app development and beta-testing process should be acknowledged. First, the current version of the exercise program was not designed based on participants’ preferences; instead, the users were given a list of exercise options to choose from. As indicated by the interview results, the participants reported that the content was monotonous and should be more diverse. Additionally, some of the participants were unable to use the exercise videos due to their health conditions. Therefore, we realized that the video options should be more diverse and tailored to each person's mobility and functionality. In the next version, the app will include more content for exercise, considering each person's preferences and functional levels, which can differ among individuals. Second, most PLWD included in the current beta-testing exhibited a stable status of dementia with infrequent occurrences of BPSD. Therefore, the usability, acceptability, and preliminary efficacy of the app could potentially differ from those in individuals with acute or severe dementia who exhibit more BPSD. Third, the app's potential effects on caregivers were not investigated during beta-testing. As the existing evidence indicates that such digital technologies can decrease caregiver burden and distress,12,13 the app's effects on caregivers should be examined in the future.
The entire development process highlighted areas for improvement in the upgraded version of the app. The app could provide more diverse digital care programs, considering the wide range of non-pharmacological interventions developed for PLWD.14,19,38 As the app development in this study was our first attempt; we provided only music, exercise, and reminiscence with music in the app. We could not offer more program options for each BPSD predicted by the machine-learning model in the app because no clear guidelines currently exist regarding which non-pharmacological interventions are appropriate for an individual BPSD symptom that differs by its etiology. 39 In the upgraded version of the app, more digital non-pharmacological care programs could be included, such as cognitive training, 40 psychological interventions, 41 and electronic calendars for time orientation, 42 that have shown promising results in individuals with conditions similar to dementia, such as neurocognitive or psychiatric disorders.
Finally, the study findings have implications for researchers planning to develop digital care programs targeting older adults. First, all caregivers in the beta-testing phase were between 50 and 90 years of age and might have experienced a prolonged adaptation period to the novel method using the app. Specifically, during the needs assessment interviews, the PLWD-caregiver dyads highlighted that the app should be easy to use. When adapting to e-health services, older adults experience barriers and challenges such as physical limitations and a lack of perceived self-efficacy or knowledge of using these technologies. 43 Therefore, older adults should be provided with assistive educational tools and sufficient time to adjust before using digital health technology. Second, internet connectivity should be a significant factor when implementing mobile app-based interventions. The research team encountered a technical issue in one dyad that faced an unstable internet connection, especially when providing digital non-pharmacological care programs. Although an increasing number of older people can now access and use the internet, the proportion tends to drop as their age increases. Additionally, it differs by educational status, income level, gender, and health status. 44 Special technical considerations should be given to those with low socioeconomic status when implementing digital health technology in their homes. Third, PLWD and caregivers may use different app functions and have different expectations and experiences with the app, even if they are likely to use the app together. Future studies investigating differences between PLWD and caregivers in experiences and expectations using the app would provide valuable insight for future development to manage dementia and related symptoms at home effectively.
Conclusions
The mobile app we developed was usable, acceptable, and feasible for PLWD and caregivers for monitoring and managing BPSD at home. The app development and beta-testing process in this study envisions the possibility of a home-based BPSD monitoring and management system using a mobile app and guides the future development of similar technologies. Altogether, employing a mobile app among PLWD and caregivers would be a promising strategy to ensure continuity of care at home and enhance the overall care quality for the increasing population with dementia.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076241249277 - Supplemental material for A mobile app to predict and manage behavioral and psychological symptoms of dementia: Development, usability, and users’ acceptability
Supplemental material, sj-docx-1-dhj-10.1177_20552076241249277 for A mobile app to predict and manage behavioral and psychological symptoms of dementia: Development, usability, and users’ acceptability by Eunhee Cho, Minhee Yang, Jiyoon Jang, Jungwon Cho, Bada Kang, Yoonhyung Jang and Min Jung Kim in DIGITAL HEALTH
Supplemental Material
sj-docx-2-dhj-10.1177_20552076241249277 - Supplemental material for A mobile app to predict and manage behavioral and psychological symptoms of dementia: Development, usability, and users’ acceptability
Supplemental material, sj-docx-2-dhj-10.1177_20552076241249277 for A mobile app to predict and manage behavioral and psychological symptoms of dementia: Development, usability, and users’ acceptability by Eunhee Cho, Minhee Yang, Jiyoon Jang, Jungwon Cho, Bada Kang, Yoonhyung Jang and Min Jung Kim in DIGITAL HEALTH
Footnotes
Acknowledgements
The authors appreciate the experts and dyads of people with dementia and their caregivers who provided valuable comments during the mobile app development process. The sponsors of this study had no role in the design, methods, subject recruitment, data collection and analysis, or preparation of this article.
Contributorship
EC: conceptualization, methodology, writing—original draft, review, and editing, and funding acquisition. MY: methodology and writing—original draft, review, and editing. JJ and BK: methodology and writing—review and editing. JC: writing—original draft, review, and editing. YJ: software and writing—review and editing. MJK: methodology, writing—original draft, review, and editing, and formal analysis.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the Basic Science Research Program through the National Research Foundation of Korea (NRF), funded by the Ministry of Education (No. 2020R1A6A1A03041989).
Ethical approval
This study was approved by the university's Institutional Review Board (No. 4-2021-0359).
Guarantor
MJK.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.