
Abstract
Objective
The use of eHealth holds promise for addressing current and upcoming challenges in long-term care (LTC), but implementation is not always successful. To optimize eHealth deployment in LTC, we aim to identify: (1) which eHealth applications are currently (not) used by healthcare professionals (HCPs) in LTC and their respective resident groups; (2) the perceived value of these eHealth applications in LTC; and (3) the drivers behind HCPs willingness and motivation to adopt eHealth technologies in their practice.
Methods
In total, 273 HCPs from LTC in The Netherlands completed an online survey. Items from the Autonomy and Competence in Technology Adoption Questionnaire were used to calculate motivation scores.
Results
The majority of HCPs believed that eHealth is or could be of added value in LTC. Applications such as websites, video calling, and electronic patient records were highly valued, whereas robotics and virtual reality were most frequently left unused due to a lack of knowledge on how to use these products. An average relative autonomy index score of 4.3 indicated autonomous motivation of HCPs to use eHealth, as opposed to being externally pressured.
Conclusion
HCPs in LTC are positive and motivated to use eHealth. However, several eHealth applications remain underutilized due to barriers such as limited knowledge or poor information and communication technology infrastructure. To optimize eHealth adoption, LTC organizations must address these challenges while continuing to support and educate HCPs. By doing so, the right eHealth products can be optimally used in LTC, which may contribute to sustainable LTC.
Introduction
The growing demand for long-term care (LTC), coupled with workforce shortages and rising healthcare costs due to an aging society, presents a pressing challenge to ensuring accessible, high-quality healthcare for all.1,2 Current healthcare delivery models are increasingly unsustainable and thus require transformative approaches across all healthcare domains, including LTC. 3 LTC encompasses care for older adults and people with intellectual disabilities (ID). With a growing population of older adults and 80 million people with an ID (intelligence quotient <70) globally, 4 both of these groups will be profoundly affected by these systemic pressures.
eHealth, defined as “the use of the Internet or related technologies to support health, well-being, and healthcare delivery,” 5 holds significant promises for addressing these challenges in LTC. The broad concept of eHealth includes innovations such as wearables, electronic health records, monitoring technologies, and mobile applications. 6 Beyond the technologies themselves, eHealth can be categorized by its role within the healthcare process or its target users. Potential benefits of eHealth include delivering personalized, cost-effective care, 7 alleviating workforce shortages by reducing healthcare professionals’ (HCPs) workload, 8 enhancing safety and promoting independence among LTC residents,9,10 and reducing the psychological burden on caregivers.9,11
In the past decade, eHealth applications have rapidly proliferated worldwide, with their role recognized as critical in achieving global health objectives. 2 However, the successful implementation of eHealth remains behind. Many innovations are underutilized or fail to achieve widespread adoption within healthcare organizations. 12 Specifically in LTC, the impact of eHealth on residents is insufficiently studied, leaving HCPs questioning its feasibility. 13 This could translate into reluctance to integrate eHealth into practice, impeding its potential to transform LTC.
Hence, successful adoption of eHealth hinges not only on the technology and organizational support but also on HCPs’ motivation and willingness to engage with it. 14 According to the self-determination theory, individuals are most likely to embrace and sustain eHealth when they feel competent and autonomous in its use. These intrinsic motivators foster greater engagement, persistence, and integration into daily practices. 15 Understanding whether HCPs’ motivation to adopt eHealth is primarily autonomous or externally driven can illuminate the factors influencing its uptake or rejection, which, in turn, can be utilized to develop more effective implementation strategies.
This study aims to identify: (1) which eHealth applications are currently used by HCPs in LTC and their respective resident groups (e.g. ID, nursing home care); (2) the perceived value of these eHealth applications in LTC; and (3) the drivers behind HCPs’ willingness and motivation to adopt eHealth technologies in their practice. For each of these objectives, we report differences between nursing home care and care for people with ID. These insights will contribute to optimizing eHealth deployment in LTC, ensuring that its benefits reach both residents and care providers.
Methods
Study design
This study employed a cross-sectional survey design. Data were collected in February and March 2023 in The Netherlands. Reporting followed the Checklist for Reporting Results of Internet E-Surveys. 16 The Leiden-The Hague-Delft Medical Ethical Committee reviewed the study protocol and waived the need for medical ethical approval (22-3087), as the study did not fall under the Dutch Medical Research Involving Human Subjects Act (WMO). Participants did not receive compensation for their participation.
Recruitment
HCPs were recruited through several university networks and academic collaborative centers. Contact persons from these networks distributed an information letter, recruitment text, and survey link via email to affiliated healthcare organizations, requesting them to circulate the invitation internally through digital newsletters, intranets, and email. Additionally, the survey invitation was shared via their social media platforms.
HCPs were eligible to participate if they were ≥18 years of age, had sufficient proficiency in Dutch to complete the survey, had at least 6 months of experience as a HCP in intramural LTC, worked with individuals with ID, dementia, or somatic symptoms, and provided online informed consent.
Procedure and survey
Participants completed an anonymous online survey hosted on Castor. 17 The survey began with an explanation of the study's aims and background, followed by an informed consent form. Participants were required to provide digital written consent before proceeding with the survey. Researchers’ contact details were provided in the invitation and study information to allow participants to seek further clarification if needed.
The survey consisted of 38 questions, with additional follow-up questions based on specific answers, leading to a variable total question count (maximum of 124). The survey took approximately 30 min to complete and was divided into four sections. The first section collected participant characteristics, including age, gender, profession, and work setting. The second section contained 10 questions about specific eHealth applications, their purposes, and usage goals, were based on a previous study 18 and adapted to fit the LTC context. An open-text field allowed participants to report additional eHealth applications not listed in the survey. The third section included the Autonomy and Competence in Technology Adoption Questionnaire, a 12-item questionnaire, validated with satisfactory internal consistency, rated on a 5-point scale. 19 This questionnaire explored reasons for using technology, addressing four behavioral regulation types: external, introjected, identified, and integrated. External and introjected regulations are considered relatively controlled forms of extrinsic motivation, whereas identified and integrated regulations are considered autonomous. The more fully a HCP internalized and integrated the use of eHealth with oneself, the more it will be the basis of autonomous behavior. The four categories were used to calculate individual scores and a relative autonomy index (RAI) score, which ranges between −12 and 12.15,19 The final section included five items about the advantages and disadvantages of eHealth usage, as well as one item addressing unmet informational needs. Answer options in this section were based on previous studies.20–22 Open text fields were included to allow participants to elaborate on additional advantages and disadvantages of eHealth. Necessary (written) permission was obtained from the respective copyright holders for the use of all questionnaires.
Data analysis
Quantitative data were analyzed using SPSS v.29. 23 Only participants who completed at least 34% of the survey, covering informed consent and participant characteristics, were included in the analysis. Descriptive statistics were used to summarize the data. Chi-squared test was conducted to assess differences between care settings (nursing home care and ID care) with statistical difference set at p ≤ 0.05. Scores for the behavioral regulation categories (external, introjected, identified, and intrinsic) were computed and aggregated to calculate the RAI score (RAI = (–2 × External) + (–1 × Introjected) + (1 × Identified) + (2 × Intrinsic)), with a higher RAI score indicating a higher form of autonomous behavior. 19
Results
A total of 350 individuals participated in the survey, with 273 respondents completing at least 34%. The respondents worked in either nursing home care (56.2%) or ID care (43.8%). In the nursing homes, 57.4% provided care to individuals with both somatic symptoms and dementia, 13.5% cared for individuals with somatic symptoms only, and 28.1% cared for individuals with dementia only. For the analysis, all respondents who provided care for individuals with dementia and/or somatic symptoms were grouped into one category: the nursing home setting. Table 1 provides an overview of participant characteristics by setting.
Participant characteristics per setting.

IQR: interquartile range; ID: intellectual disabilities.
A total of 15 participants worked with people with ID and people with dementia. These participants are only described in ID setting.
Primary: (special) primary education, prevocational education, vocational education level 1, senior general secondary education grades 1–3, preuniversity education grades 1–3, trade school; Secondary: senior general secondary education grades 4–5, preuniversity education grades 4–6, vocational education levels 2–4; Tertiary: university of applied sciences, university.
Other includes: social worker, dietician, spiritual caregiver, care director, care advisor.
eHealth use
Most respondents reported using eHealth in their care practices, with 76.5% in nursing homes and 73.0% in ID care. Among HCPs in nursing homes, 64.3% used eHealth on an (almost) daily basis, which was different (p = 0.038) from the 46.9% of HCPs in ID care that indicated to use eHealth on an (almost) daily basis. Weekly use of eHealth was reported by 17.0% in nursing homes and 30.9% in ID care, while 12.5% and 14.8%, respectively, used it a few times per month. Few participants reported almost never using eHealth (6.3% in nursing homes vs. 7.4% in ID care).
On average, respondents across both settings had similar experience with eHealth, with a median of 6 years (interquartile range: 2–10). The vast majority of participants (82.4% in nursing homes and 82.0% in ID care) believed that eHealth either already adds or could add value to LTC.
Table 2 provides an overview of eHealth applications utilized in LTC, highlighting their purposes and perceived value. The most commonly available and used applications were websites, web portals (e.g. electronic patient records), and video calling.
Use, purpose, and perceived value per eHealth application.

EPD/ECD: Electronic patient record/electronic client record; ID: intellectual disabilities.
**p ≤ 0.05 difference between ID care and nursing homes.
Certain applications were more prevalent and valued in specific care settings. Health sensors (57%) and robotics (49.2%) were significantly more utilized and appreciated in nursing homes (p < 0.05), while virtual reality (VR) was more commonly used (25.4%) in ID care (p < 0.05). Additionally, the purpose of using websites, mobile applications, and web portals differed significantly between the two settings (p < 0.05). Websites were significantly more commonly used for diagnosing and early warning in nursing home care compared to ID care. Mobile apps were significantly more commonly used for information seeking in nursing homes than in ID care. Web portals were also more frequently used for early warning in nursing homes. Furthermore, the frequency in using websites (p = 0.017), serious games (p = 0.036), mobile applications (p = 0.017), and robotics (p = 0.043) differed between the settings, with the first two applications being more frequently used by HCPs in ID care and the last two applications more frequently used in nursing homes. Moreover, the use of different eHealth applications differed per job function (Supplement 1).
Applications such as websites, video calling, and web portals, which were highly valued in both settings (79%, 66%, 70% respectively for nursing homes and 62%, 58%, 58% respectively for ID care), were primarily used to search for and exchange information.
Unused eHealth
In the nursing home setting, 25.7% reported unused eHealth applications within their organization, with robotics (51.4%), VR (37.1%), and domotics (25.7%) being the most frequently cited. In the ID setting, 19.4% of the respondents indicated unused eHealth applications, primarily robotics (50.0%) and VR (40.0%), followed by websites and mobile applications (both 35.0%).
The primary reasons for not using robotics and VR were limited knowledge on how to use these technologies, reported by 61.1% (robotics) and 46.2% (VR) in nursing homes, and by 70.0% (robotics) and 87.5% (VR) in the ID setting. In the nursing homes, additional reasons for VR not being used included a perceived lack of added value for residents and HCPs (both 46.2%). Similarly, domotics in nursing homes remained unused due to limited knowledge (44.4%). In the ID setting, websites and mobile applications were often unused because they were considered too complex to operate (85.7% and 71.4%, respectively). A lack of knowledge also contributed to the underutilization of mobile applications (85.7%).
Motivation for eHealth use
Table 3 presents an overview of HCPs’ motivation to use eHealth per setting. In both settings, the mean total RAI was 4.3 (possible range −12 to 12), indicating a predominantly autonomous motivation to use eHealth rather than being driven by external pressures. Both settings showed similar scores across the various motivation scales, with slightly higher scores in the “identified” and “integrated” scales, suggesting that HCPs in both settings view eHealth as an important tool and have integrated its use into their practices. The perceived competence, motivation, and self-determined engagement with eHealth were comparable across settings.
Healthcare professionals’ motivation to use eHealth (intrinsic vs. extrinsic) in long-term care.

Scale 1–4: external, introjected, identified, and intrinsic, respectively.
RAI = (−2 × External) + (−1 × Introjected) + (1 × Identified) + (2 × Intrinsic).
Unmet informational needs
In both settings, HCPs reported unmet informational needs that hindered the effective use of eHealth. In total, 54.8% in the ID setting and 53.3% in nursing homes indicated a lack of information about the available forms of eHealth. Additionally, 40.5% of ID professionals and 46.7% of nursing home professionals felt they lacked guidance on how to use or implement eHealth. Information about the effectiveness of eHealth was also missed (33.3% of ID professionals vs. 38.3% of nursing home professionals). Furthermore, details on the functionality or operation of specific eHealth products were lacking (29.8% of ID professionals vs. 27.1% of nursing home professionals). Lastly, 23.8% of ID professionals and 10.3% of nursing home professionals felt they did not lack any information regarding eHealth.
To address these unmet needs, HCPs preferred to receive information through newsletters or webinars. They suggested that information about the range of available eHealth applications could be shared on a website. In contrast, scientific articles or dedicated eHealth courses were the least preferred methods for delivering this information.
(Dis)advantages for using eHealth in LTC
HCPs most commonly identified the advantages of using eHealth in LTC as increased effectiveness and efficiency, enhanced independence for care recipients, and improved facilitation of collaboration. On the other hand, the main disadvantages or objections included insufficient Wi-Fi or information and communication technology (ICT) infrastructure in healthcare organizations, limited knowledge about eHealth usage, and concerns about costs. Table 4 presents the perceived advantages and disadvantages of eHealth use in LTC, ranked by percentage based on the nursing home setting.
Perceived (dis)advantages of eHealth use in LTC.
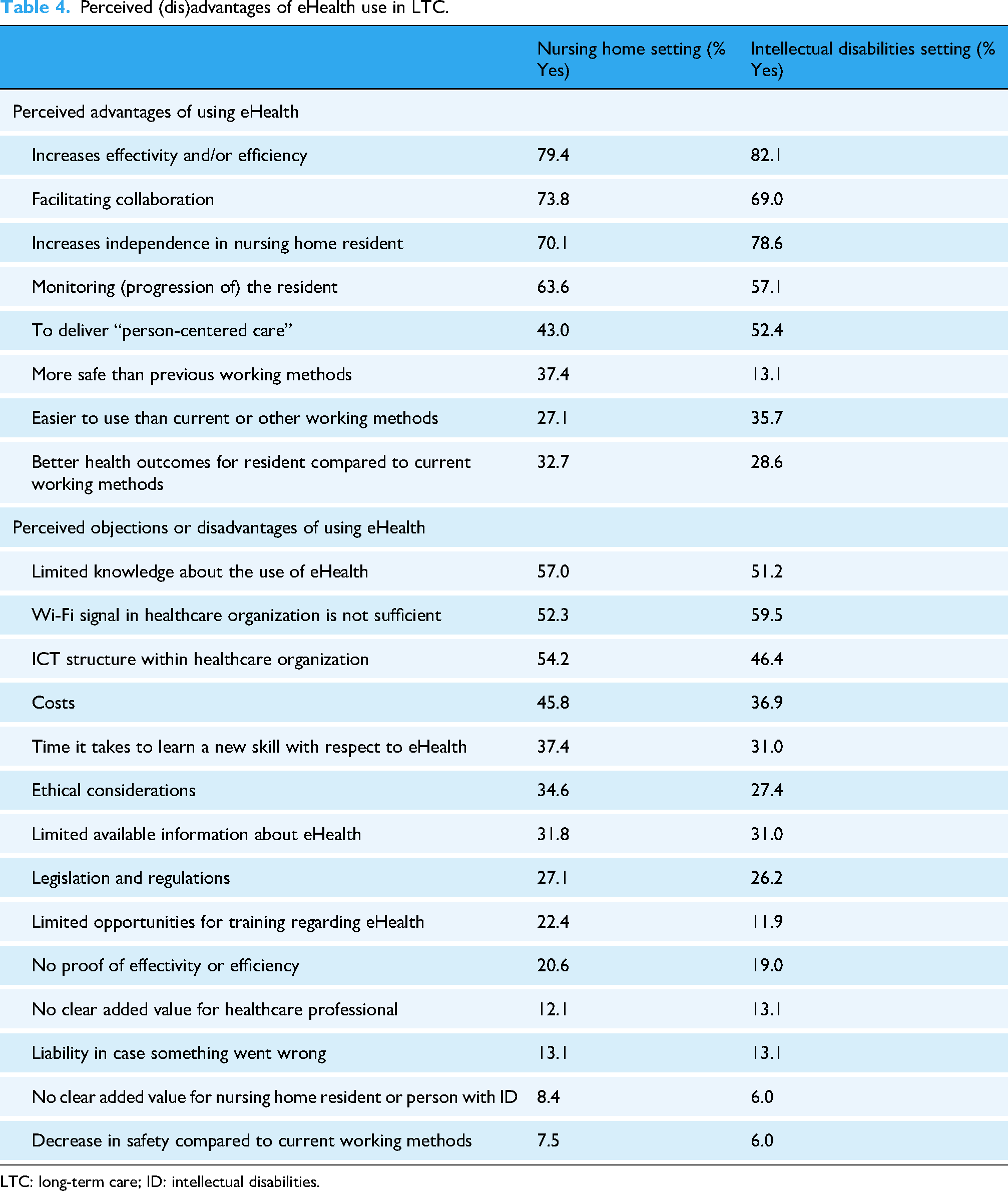
LTC: long-term care; ID: intellectual disabilities.
Discussion
This study examined which eHealth applications are utilized and perceived as valuable by HCPs in LTC. We explored what motivates HCPs to adopt eHealth applications in LTC. Overall, HCPs were positive about using eHealth and few differences were identified between nursing homes and ID care. Generally, eHealth had an added value and was used on a daily or weekly basis. The most used applications included websites, web portals, domotics, and videocalls. HCPs displayed an autonomous motivation to use eHealth, reflecting their willingness to integrate these technologies into their care practices.
eHealth use
Generally, eHealth products are frequently used in LTC yet certain innovations—such as robotics and VR—remain underutilized. This was often attributed to limited product knowledge and perceptions of low added value. These findings may partly be explained by the fact that robotics and VR are relatively novel in LTC, 24 which is—together with limited product knowledge—also the number one reported barrier in eHealth implementation. 22 Notably, when employed, robotics and VR have shown meaningful contributions to care, including facilitating social interaction, enhancing engagement, and preventing isolation.25,26 Moreover, HCPs in geriatric rehabilitation report VR as one of the more user-friendly eHealth tools. 18 These are all facilitating factors for implementation. 22 This suggests that robotics and VR hold untapped potential in LTC, warranting further exploration through targeted implementation strategies.
Domotics were widely available in LTC and primarily used for monitoring and early warning. Despite their perceived value—particularly among nursing home HCPs—only about half of respondents reported active use. A quarter attributed non-use to limited product knowledge, a common barrier to eHealth adoption.18,22 However, other factors likely also contribute, including technical issues, insufficient support, lack of standardized implementation, and competing clinical priorities that limit time for technology adoption.18,22,27
eHealth products valued most by HCPs (websites, video calling, and web portals) were often used to search and exchange information. Previous research found that eHealth products that facilitate the exchange of information, such as web portals or video calling, are support sustainable (inter-)professional collaboration. 28 This may explain why HCPs often value these specific eHealth products. Interestingly, eHealth applications focused on the resident, for example, for treatment or social purposes, were less valued by HCPs. These findings suggest that HCPs have a greater need for eHealth products that directly benefit themselves professionally (instead of the resident). However, these findings also resonate with the pillars of the person-centered care approach, which is now widely used in The Netherlands and worldwide. 29 In this approach, care is tailored to the individual needs and preferences of the resident. HCPs, as part of the person-centered care approach, might prefer to attend to the resident's social and treatment needs directly, reducing reliance on eHealth for such purposes. 30 This sentiment, about preserving the “human touch of care” is echoed in several studies.31,32
Motivation
HCPs demonstrated an autonomous motivation to use eHealth, with high levels of identified and integrated regulation. This indicates that they view eHealth as important and feel intrinsically driven to incorporate it into their work. Such a positive attitude is a critical factor for successful eHealth adoption and implementation.14,15 However, despite this positive attitude, certain eHealth applications remain underutilized. This suggests that the barriers to eHealth use in LTC may not stem from a lack of motivation but rather from structural, technical, or organizational challenges. According to the diffusion of innovations theory, the successful adoption of a new technology depends on several elements, including the innovation itself, the adopters, communication channels, time, and the social system. 33 Even when HCPs are motivated to adopt eHealth solutions, other elements—such as the perceived complexity of the technology or the relative advantage it offers- must also be in place. 33 In our study, some eHealth applications were seen as too complex or lacking in clear added value, which may hinder their widespread adoption. Additionally, structural barriers such as inadequate Wi-Fi or ICT infrastructure, or training were frequently cited and can also inhibit diffusion throughout an organization.22,33 Addressing these barriers could help bridge the gap between HCPs’ motivation and actual eHealth use.
Strengths and limitations
A strength of this study is its interdisciplinary sample, which included HCPs from multiple LTC settings. Additionally, the study's focus on motivation provides new insights into an understudied area of eHealth adoption. However, there are some limitations. The participants were predominantly mid- to highly educated and experienced in working with eHealth. This may have biased the findings toward more positive attitudes and higher autonomous motivation. 34 Furthermore, a number of questions in this survey are derived from a previously validated questionnaire. However, some questions were not yet validated. Lastly, The Netherlands, together with Scandinavian countries, ranks among the most digitally advanced nations in Europe. 35 As such, the findings of this Dutch survey may not be fully generalizable to countries with lower levels of digitalization. Nonetheless, the findings offer valuable insights into the factors influencing eHealth adoption in LTC.
Recommendations
Although HCPs in LTC are generally motivated to use eHealth and recognize its value, several applications remain underutilized due to barriers such as insufficient knowledge and inadequate ICT infrastructure. To address these issues, healthcare organizations should provide clear, accessible information about each eHealth product and its functionality. This could be achieved through newsletters, webinars, or dedicated online resources. Furthermore, organizations must invest in improving their ICT infrastructure, such as ensuring reliable Wi-Fi and technical support, to facilitate the seamless use of eHealth in daily practice. Finally, organizations should foster a culture that supports innovation and encourages the exploration of emerging technologies.
Conclusions and implications
HCPs in LTC generally view eHealth positively and recognize its added value in care delivery. Nevertheless, adoption remains uneven, with several applications underutilized due to barriers such as limited digital literacy and inadequate ICT infrastructure. To optimize eHealth adoption, healthcare organizations must address these structural challenges while investing in ongoing training and support for HCPs. By doing so, the right eHealth products can be optimally used in LTC, which may contribute to sustainable LTC.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076251376283 - Supplemental material for Toward successful eHealth adoption in long-term care: Insights from a national survey of healthcare professionals
Supplemental material, sj-docx-1-dhj-10.1177_20552076251376283 for Toward successful eHealth adoption in long-term care: Insights from a national survey of healthcare professionals by Esmee Adam, Noud Frielink, Monique Caljouw, Sascha Bolt, Petri Embregts, Sytse Zuidema, Wilco P Achterberg and Hanneke JA Smaling in DIGITAL HEALTH
Supplemental Material
sj-docx-2-dhj-10.1177_20552076251376283 - Supplemental material for Toward successful eHealth adoption in long-term care: Insights from a national survey of healthcare professionals
Supplemental material, sj-docx-2-dhj-10.1177_20552076251376283 for Toward successful eHealth adoption in long-term care: Insights from a national survey of healthcare professionals by Esmee Adam, Noud Frielink, Monique Caljouw, Sascha Bolt, Petri Embregts, Sytse Zuidema, Wilco P Achterberg and Hanneke JA Smaling in DIGITAL HEALTH
Footnotes
Acknowledgments
The authors would like to thank all healthcare professionals who participated in this study.
Ethical approval
The Leiden-The Hague-Delft Medical Ethical Committee reviewed the study protocol and waived the need for medical ethical approval.
Author contributions
All authors contributed to the conceptualization, methodology, and writing (review and editing) of this research. Furthermore, EA performed the investigation and formal analysis of the data, and wrote the original draft of this paper. HS contributed to the formal analysis.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by the University Network for the Care sector Zuid-Holland (UNC-ZH) and Leiden University Medical Center (LUMC) in Leiden, The Netherlands.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.