
Abstract
Objective
This study aimed to evaluate the effect of step-count monitoring interventions on objectively measured physical activity-related outcomes in children and adolescents.
Methods
This review was designed and conducted based on the Preferred Reporting Items for Systematic Review and Meta-Analyses (PRISMA) guidelines. The following five electronic databases were searched to identify relevant studies: PubMed, Web of Science, SCOPUS, SPORTDiscus, and Cochrane Library. The search was performed from the date of database inception to December 7, 2024. Meta-analyses were conducted to evaluate the pooled effects of the interventions on daily steps, accelerometer-measured moderate-to-vigorous physical activity (MVPA), light physical activity (LPA), and sedentary behavior (SB).
Results
Thirty-four studies were selected for this meta-analysis. Step-count monitoring interventions could significantly increase daily steps (MD 1588.83 steps/day; 95% CI 1033.94 to 2143.72; P < 0.01) and tended to significantly reduce SB (MD −3.42 min/day; 95% CI −6.83 to −0.01; P = 0.05). However, they had no significant effects on MVPA (MD 0.59 min/day; 95% CI −3.46 to 4.64; P = 0.78) and LPA (MD 1.29 min/day; 95% CI −1.44 to 4.03; P = 0.35). Subgroup analyses indicated that step-count monitoring interventions offered greater benefits for increasing MVPA in children (MD 6.09 min/day; P < 0.01) than in adolescents (MD −3.79 min/day; P = 0.13). Pedometer-based interventions (MD 1757.58 steps/day; P < 0.01) were more effective at increasing daily steps than those involving other emerging step-count monitoring devices (MD 406.12 steps/day; P = 0.37).
Conclusions
Step-count monitoring interventions may be appropriate and effective for increasing total physical activity and reducing SB in children and adolescents. Moreover, these interventions may serve as an optional approach for increasing MVPA in children. We recommend a “less is more” strategy with regard to step-count monitoring interventions for increasing physical activity in children and adolescents.
Introduction
Physical activity refers to any voluntary bodily movement that engages skeletal muscles and requires energy expenditure. 1 Physical activity plays a critical role in promoting and maintaining health in children and adolescents. 2 In this population, regular physical activity can address not only physical health issues, such as obesity and type 2 diabetes, but also psychological disorders, including depression and anxiety.2–7 Despite these well-documented benefits, nearly 80% of adolescents worldwide fail to meet the World Health Organization (WHO) recommendation of at least 60 min of moderate-to-vigorous physical activity (MVPA) per day.1,8 This highlights the urgent need for effective strategies to increase physical activity among children and adolescents, making it a key public health priority.
Given the importance of this problem, numerous intervention programs have been implemented to encourage physical activity among children and adolescents.9–12 While traditional approaches such as school-based group programs and interventions by professional agencies have shown positive short-term outcomes, their long-term effectiveness is often limited.13–16 Additionally, these interventions tend to be labor- and resource-intensive and are difficult to scale.17–20 Therefore, newer and more sustainable, scalable, and effective solutions to promote physical activity among children and adolescents are warranted.
Walking is a widely accessible and convenient form of physical activity, and its frequency and intensity can be easily regulated.21,22 Thus, walking can help children and adolescents meet the World Health Organization's daily activity recommendations.23–25 With advances in technology, a variety of devices (including pedometers and fitness trackers such as Fitbit) have been developed to monitor walking. These devices not only monitor daily steps but also serve as motivational tools to encourage physical activity.26–28 In addition, these devices are simple, inexpensive, and easy to use, making them particularly suitable for children and adolescents.24,29–31 Therefore, step-count monitoring interventions could present a promising option for increasing physical activity levels in this population.
Previous studies have investigated the effectiveness of step-count monitoring interventions in increasing physical activity among children and adolescents.32–37 However, due to contradictory evidence, clear conclusions are yet to be obtained. For instance, a study by Suksong et al. investigated the effects of a walking intervention program on self-efficacy and physical activity in children with obesity. 38 The results demonstrated statistically significant improvements in self-efficacy, daily steps, and MVPA in the intervention group. In contrast, a study by Evans et al. explored the use of Fitbit devices to monitor daily steps, set challenging step-count goals, and thereby promote physical activity in children. 39 However, the intervention group in this study did not show significant improvements in daily step counts or MVPA. This apparent lack of success could be because the participants’ baseline physical activity levels were already high, and the step-count monitoring interventions failed to motivate them to be more active. A previous meta-analysis synthesized the evidence regarding the effectiveness of pedometer-based interventions for promoting physical activity in children and adolescents. 40 The results suggested that the use of pedometers has a positive effect on increasing physical activity in this group, especially for female participants. Moreover, the findings indicated that intervention strategies that target 10.000 steps per day yield promising results. However, the meta-analysis had several important limitations. Notably, the meta-analysis was not exclusive to children and adolescents, since the study population also included adults. Additionally, it was published in 2009 and only considered interventions that used pedometers, neglecting other emerging step-count monitoring devices such as wearable activity trackers and smartphone applications. Moreover, the outcomes of this meta-analysis only included daily steps and did not include accelerometer-measured MVPA, light physical activity (LPA), and sedentary behavior (SB), which are the physical activity parameters recommended by the WHO. These limitations call for an updated meta-analysis that provides a more current and comprehensive synthesis of evidence regarding the effectiveness of step-count monitoring interventions for increasing physical activity among children and adolescents. This evidence could help inform the public and health policymakers on whether, and how, step-count monitoring interventions should be used to promote physical activity among children and adolescents.
The primary objective of the present systematic review and meta-analysis was to assess the effects of step-count monitoring interventions on objectively measured physical activity-related outcomes, such as daily steps and accelerometer-measured MVPA, in children and adolescents. The secondary objective was to explore how specific characteristics of intervention programs (such as the type of step-count monitoring device, intervention duration, goal-setting strategy, and overall intervention design) may influence their effectiveness. We hypothesized that step-count monitoring interventions would increase daily steps, MVPA, and LPA among children and adolescents while reducing SB.
Methods
Registration and approval
This review was designed and conducted in accordance with the Preferred Reporting Items for Systematic Review and Meta-Analyses (PRISMA) guidelines 41 (PRISMA checklist in Supplemental Material 1). The protocol for this review was registered in the PROSPERO database (CRD42025642254) on February 5, 2025.
Search strategy
The following five electronic databases were searched to identify relevant studies: PubMed, Web of Science, SCOPUS, SPORTDiscus, and Cochrane Library. The search was performed from the date of database inception to December 7, 2024. The complete search strategy is described in Supplemental Material 2. An updated search was conducted in January 2025 to ensure that the most up-to-date evidence was included in the meta-analysis. Additional studies were identified by reviewing the reference lists of the included studies and relevant reviews.
Inclusion and exclusion criteria
The inclusion criteria were established in accordance with the PICOS framework (population, intervention, comparison, outcomes, and study), 42 as follows: (1) Population: participants were children or adolescents ages 3 to 18 years; (2) Intervention: the program involved the use of step-count monitoring interventions to increase physical activity or reduce sedentary behavior; (3) Comparison: the control groups did not receive the interventions or did not use step-count monitoring devices; (4) Outcomes: the objectively measured physical activity-related outcomes included daily steps, accelerometer-measured MVPA, LPA, and SB; and (5) Study: in terms of design, the study design was a randomized controlled trial (RCT).
The exclusion criteria were as follows: (1) The articles were not written in English; (2) Step-count monitoring devices were only used as physical activity measurement tools and not intervention tools; (3) The outcomes were self-reported physical activity-related indicators; (4) The purpose of the study was to examine the feasibility (e.g., acceptance and perception) of using step-count monitoring devices among children and adolescents; and (5) The studies were protocols, systematic reviews, or meta-analyses.
Data extraction
Once the literature search was completed, the results identified from the different databases were imported into EndNote X9 to remove duplicate articles. Two authors (WW and YS) screened the titles and abstracts of potentially eligible articles to identify relevant studies. Two authors (JC and LW) independently evaluated the full text of the articles to determine if they should be included based on the aforementioned eligibility criteria. Any disagreements between the two authors regarding study inclusion were resolved by consulting a third author.
Information from each study was extracted independently by two authors (JC and LW). The extracted information included: authors, country of study, publication date, sample size, participant sex and age, health status, types of step-count monitoring devices, intervention durations, goal-setting strategies, intervention design, and physical activity-related outcomes.
Risk of bias assessment
Two independent authors (JC and LW) assessed the risk of bias for the included studies using the Cochrane risk of bias tool. 43 The tool considered the following seven domains of bias: (1) random sequence generation, (2) allocation concealment, (3) blinding of participants and personnel, (4) blinding of outcome assessment, (5) incomplete outcome data, (6) selective outcome reporting, and (7) other sources of bias. Studies were judged on each domain and classified under low, unclear, or high risk of bias. Disagreements about the risk of bias were resolved by consulting another author.
Statistical analysis
The outcomes of this meta-analysis included daily steps and accelerometer-measured MVPA, LPA, and SB. For outcomes with the same unit of measurement, effect sizes were measured by calculating the pooled mean difference (MD) with a 95% confidence interval (CI). If a study had multiple step-count monitoring intervention groups, each group was included in the analysis individually. If data from included studies were in the form of standard errors (SEs) or 95% CIs, the data were converted to standard deviations (SDs) using the RevMan calculator. Between-study heterogeneity was examined using I 2 statistics and the Cochran Q-test. I2 values of 0%–40%, 30%–60%, 50%–90%, and 75%–100% indicated insignificant, moderate, substantial, and considerable heterogeneity, respectively. 44 If I2 values were ≤50% (P ≥ 0.05), a fixed effects model was used for the meta-analysis. However, if I2 values were >50% (P < 0.05), a random effects model was used. Subgroup analyses were conducted to examine the influence of intervention program characteristics on daily steps and MVPA (children vs adolescents, healthy people vs patients with health disorders, pedometers vs other emerging step-count monitoring devices, intervention duration < 3 months vs intervention duration ≥ 3 months, individualized goals vs lack of individualized goals, single step-count monitoring interventions vs multi-component comprehensive interventions). Publication bias was assessed using funnel plots. All statistical analyses were completed using RevMan 5.4 software.
Results
Study selection
In total, 43.431 potentially relevant records were retrieved from five databases, and 25.375 duplicates were removed using EndNote X9 software. Following the screening of abstracts and titles, 586 studies were deemed eligible for full-text review. Finally, after the full text of these studies was screened, 34 studies were selected for meta-analysis. The details of the overall literature screening process are presented in Figure 1.

PRISMA flow chart of study selection.
RCT: randomized controlled trial.
Study characteristics
The characteristics of the 34 included studies are shown in Table 1. These studies were published between 2005 and 2024 and included a total of 4.311 participants. The ages of the participants ranged from 4 to 18 years. Of the 34 studies, 31 involved healthy children and adolescents, while three involved children and adolescents with health disorders (e.g., type 1 diabetes45,46 and cancer survivors 47 ). The mean duration of the intervention was 3.51 months (0.75–13 months). However, 17 of the 34 studies had an intervention duration of ≥ 3 months.35,45,46,48–61 All studies used pedometers as intervention tools, with the exception of seven studies that used other emerging step-count monitoring devices (Fitbit,35,39,47,60 Polar active activity watch, 45 SMARTFAMILY app, 62 and iEngage app 34 ). In total, 21 studies34–36,38,39,47–50,55–58,60,62–68 used individualized goals (setting step-count goals based on each individual's baseline step count) as a goal-setting strategy, while the other 13 studies32,33,37,45,46,51–54,59,61,69,70 used uniformity goals (step-count goals were the same for all participants, regardless of each individual's baseline levels)or had no goals. In terms of the intervention design, 19 studies32,33,35–39,46–49,51,53,56,58,60,63,67,68 involved programs focused primarily on step-count monitoring interventions, while the other 15 studies34,45,50,52,54,55,57,59,61,62,64–66,69,70 used step-count monitoring as part of a comprehensive intervention program. Regarding outcome indicators, 25 studies reported daily steps,32,33,35,37–39,45,46,49–51,53–56,58,59,61–66,68,70 17 studies reported MVPA,34–36,38,39,45,47,48,52,57,58,60,62,64,67,69,70 six studies reported LPA,36,38,60,67,69,70 and eight studies reported SB.35,36,38,47,48,60,67,69
Characteristics of included studies.
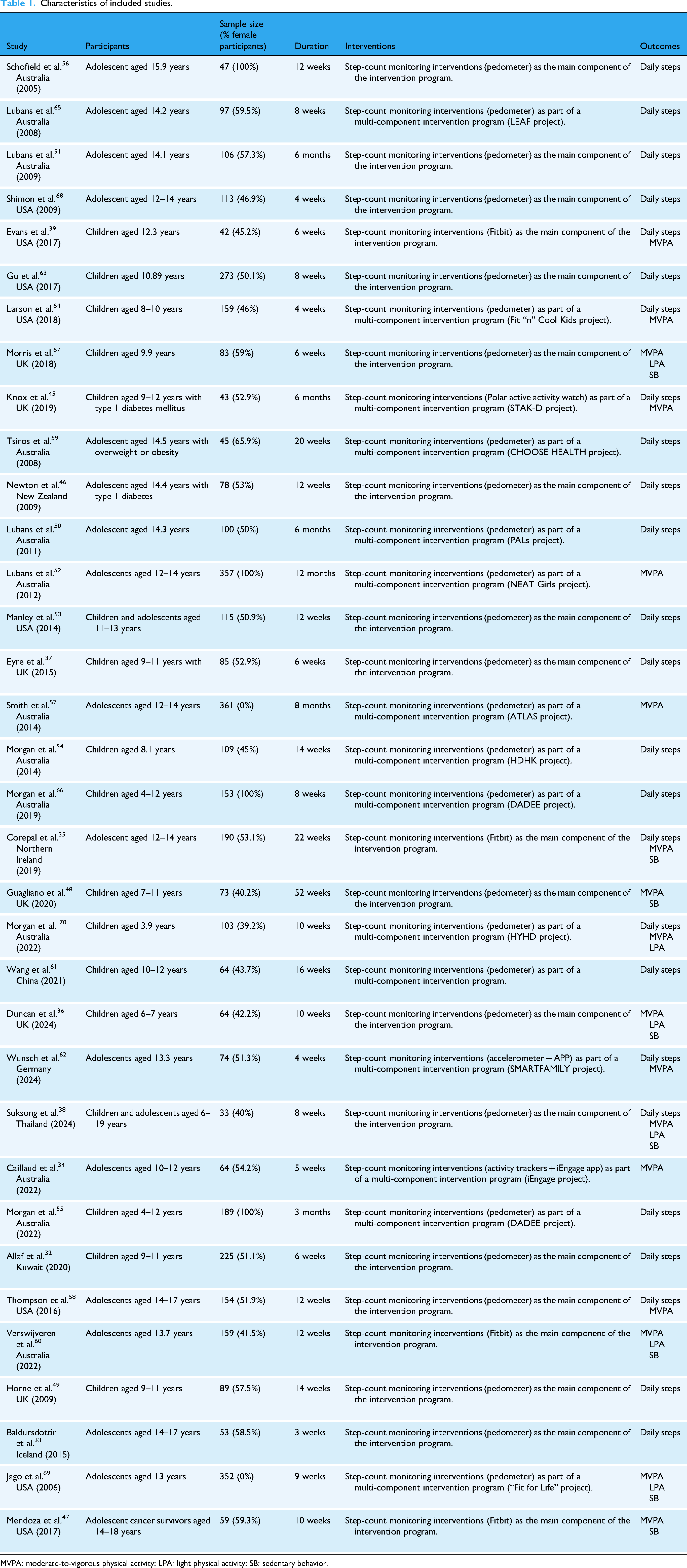
MVPA: moderate-to-vigorous physical activity; LPA: light physical activity; SB: sedentary behavior.
Risk of bias assessment
Figure 2 details the risk of bias for each included study. Overall, 28 of the 34 studies were deemed to have a low risk of bias in the random sequence generation domain. Moreover, 15 studies32–34,37,39,49,50,52,56,59,61,63–65,68 were judged to have a high or unclear risk of bias in the allocation concealment domain owing to a lack of detailed information in the methods section. With regard to the blinding of participants and personnel, all studies were classified as having a high risk of bias due to the nature of the physical activity. In contrast, on the blinding of outcome assessment domain, all studies were classified as having a low risk of bias due to the use of objective outcome measures. In total, 9 studies33,34,37,38,45,59,60,67,69 had >20% attrition rates and were thus deemed to have a high risk of bias in the incomplete outcome data domain. Meanwhile, all studies were classified as having a low risk of bias in the selective outcome reporting domain. Finally, four studies33,53,56,61 showed a high risk for other sources of bias due to significant differences in baseline physical activity between the intervention and control groups.

Risk of bias summary.
Meta-analysis results
Daily steps
In total, 25 studies reported changes in daily steps from the baseline to the post-intervention time point.32,33,35,37–39,45,46,49–51,53–56,58,59,61–66,68,70 A significant increase in daily steps was observed in the step-count monitoring intervention groups versus the control groups (MD 1588.83 steps/day; 95% CI 1033.94 to 2143.72; P < 0.01); considerable heterogeneity in this outcome was identified (I2= 98%; P < 0.01) (Figure 3).
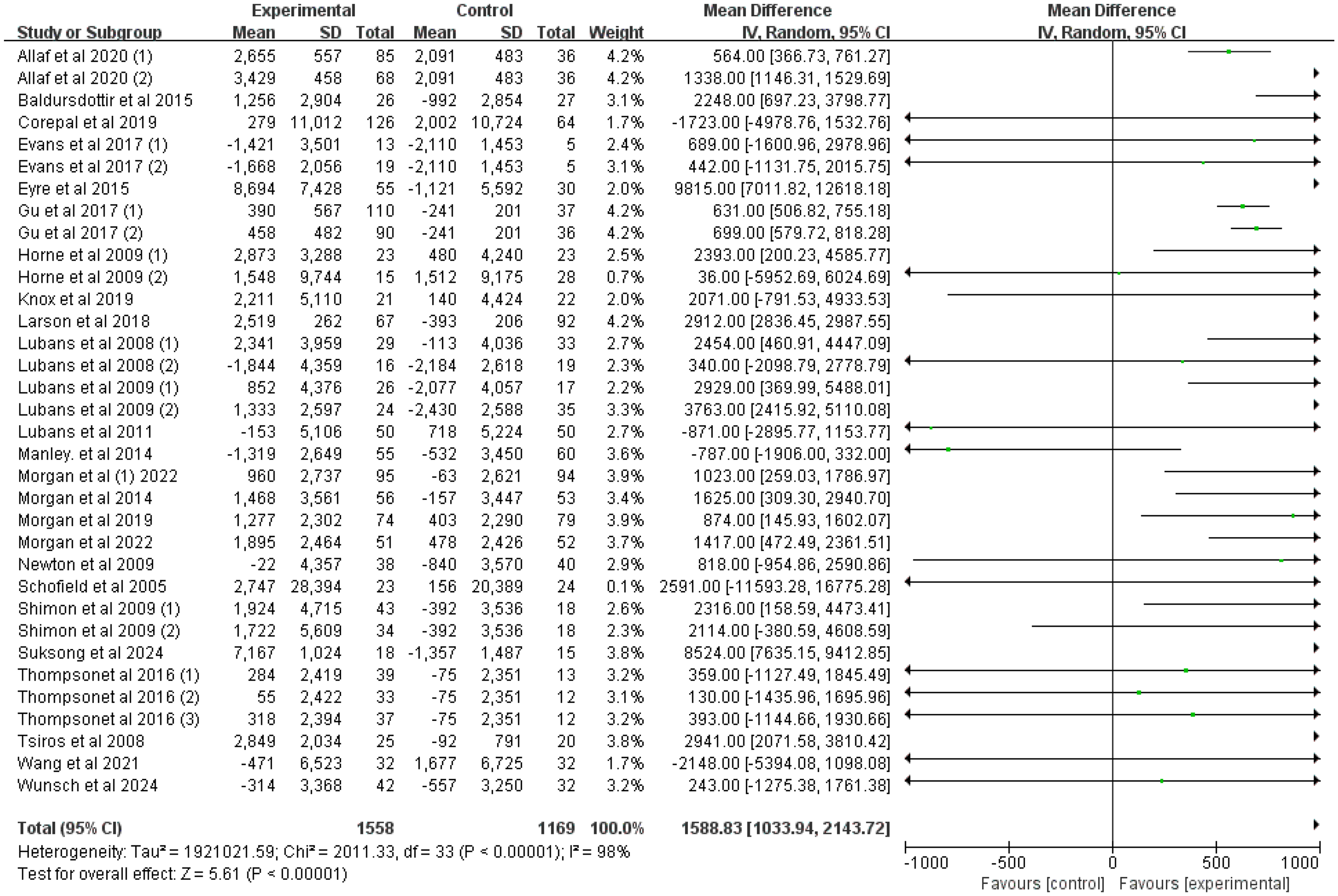
Forest plot of the mean difference in daily steps (steps/day) between the step-count monitoring intervention groups and the control groups.
MVPA
Seventeen studies reported changes in MVPA from the baseline to the post-intervention time point.34–36,38,39,45,47,48,52,57,58,60,62,64,67,69,70 Compared to the control groups, the step-count monitoring intervention groups did not present a significant increase in MVPA (MD 0.59 min/day; 95% CI −3.46 to 4.64; P = 0.78); substantial heterogeneity was detected with regard to this outcome (I2 = 83%; P < 0.01) (Figure 4).
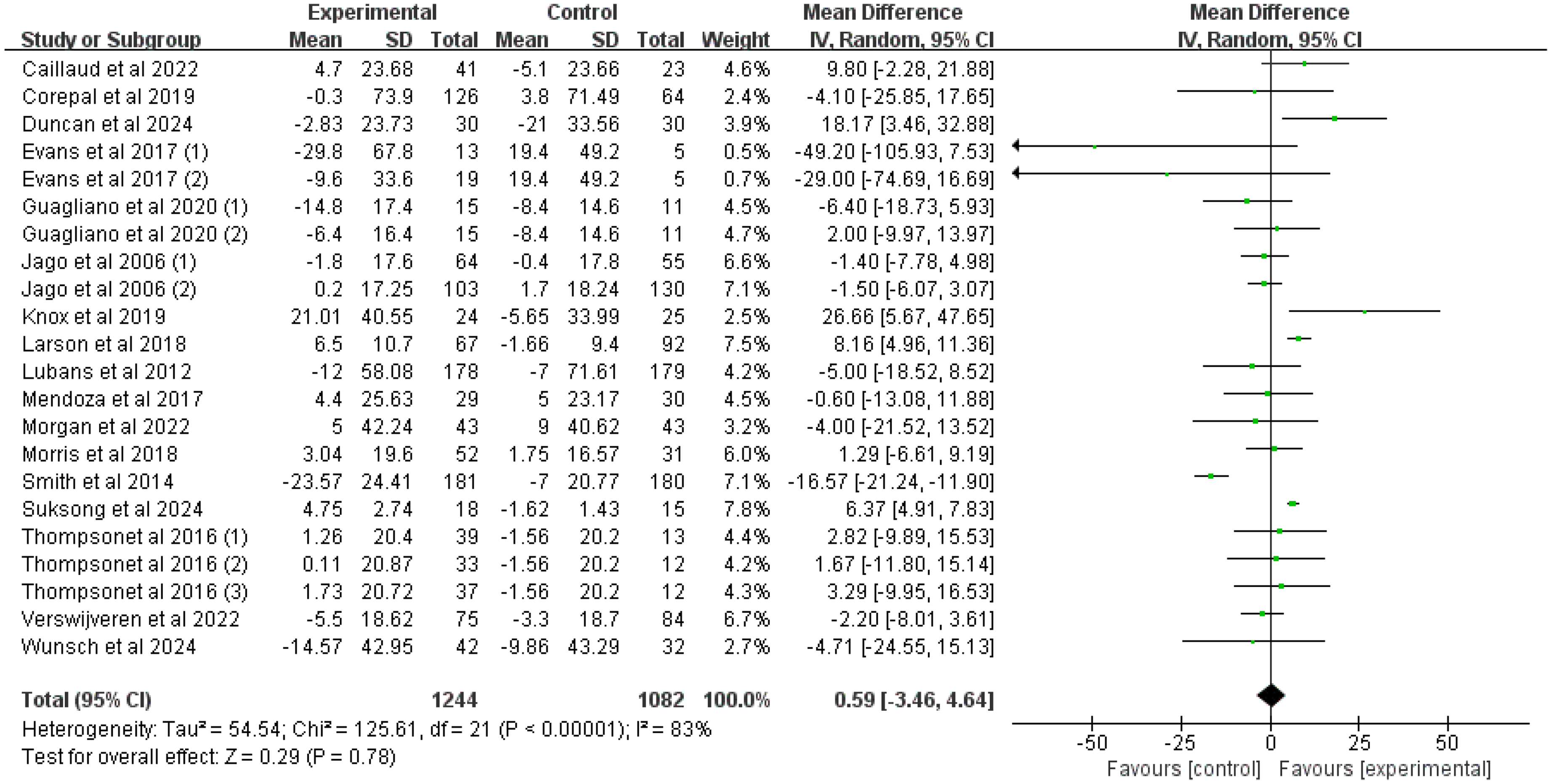
Forest plot of the mean difference in MVPA (min/day) between the step-count monitoring intervention groups and the control groups.
LPA
Six studies reported changes in LPA from the baseline to the post-intervention time point.36,38,60,67,69,70 The step-count monitoring intervention groups did not show a significant increase in LPA compared to the control groups (MD 1.29 min/day; 95% CI −1.44 to 4.03; P = 0.35); moderate heterogeneity was detected with regard to this outcome (I2 = 47%; P = 0.08) (Figure 5).
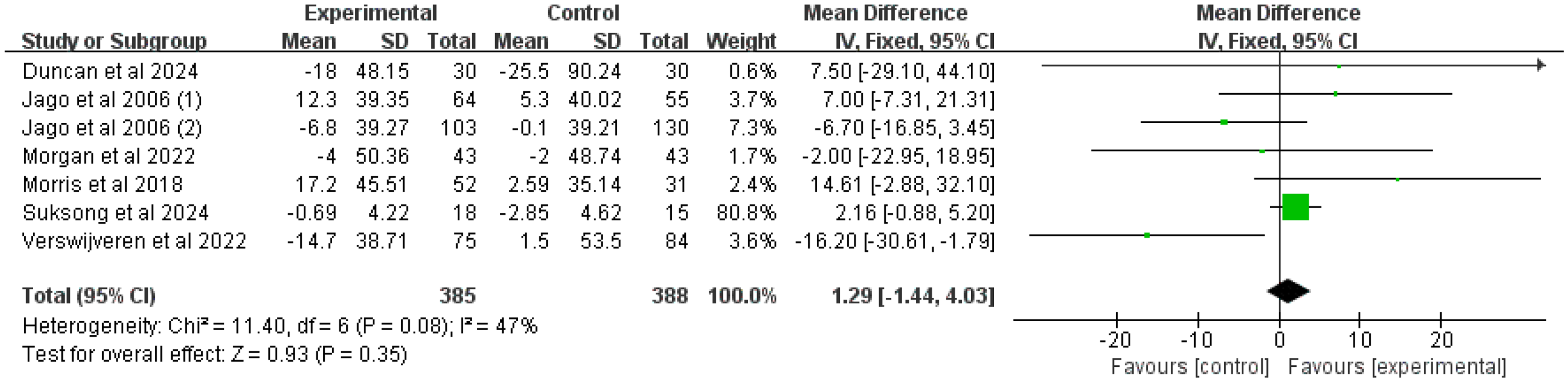
Forest plot of the mean difference in LPA (min/day) between the step-count monitoring intervention groups and the control groups.
SB
Overall, eight studies reported changes in SB from the baseline to the post-intervention time point.35,36,38,47,48,60,67,69 Compared to the control groups, the step-count monitoring intervention groups tended to show a significant reduction in SB (MD −3.42 min/day; 95% CI −6.83 to −0.01; P = 0.05); heterogeneity in this outcome was insignificant (I2 = 7%; P = 0.38) (Figure 6).

Forest plot of the mean difference in SB (min/day) between the step-count monitoring intervention groups and the control groups.
Subgroup analyses
The results indicated that step-count monitoring interventions had a stronger effect in increasing MVPA among children (MD 6.09 min/day; P < 0.01) than among adolescents (MD −3.79 min/day; P = 0.13). The programs using pedometers achieved a better effect in increasing daily steps (MD 1757.58 steps/day; P < 0.01) than those using other emerging step-count monitoring devices (MD 406.12 steps/day; P = 0.37). No significant differences in daily steps and MVPA were identified in the other subgroup analyses (Table 2).
Results of subgroup analyses.

MVPA: moderate-to-vigorous physical activity.
Discussion
Principal findings
To the best of our knowledge, this is the first meta-analysis to synthesize evidence regarding the effectiveness of step-count monitoring interventions on physical activity-related outcomes in children and adolescents. Our results indicated that step-count monitoring interventions significantly increase daily steps and tend to significantly reduce accelerometer-measured SB in this population. However, these interventions appeared to have no significant effects on accelerometer-measured MVPA and LPA. Finally, our subgroup analyses revealed that step-count monitoring interventions offer greater benefits in increasing MVPA among children than among adolescents. Moreover, pedometer-based intervention programs appear to be more effective at increasing daily steps than programs based on other emerging step-count monitoring devices.
Daily steps are an indicator of total physical activity, 71 and increasing daily steps has a positive impact on total physical activity levels. 72 Previous studies have shown that increasing daily steps by even 1.000 can reduce all-cause mortality and the risk of cardiovascular disease in adults.73,74 In children and adolescents, increasing daily steps can help in preventing and treating obesity and improving cardiorespiratory fitness.75–77 Therefore, the increase of 1588.83 steps/day observed following step-count monitoring interventions in the current meta-analysis appears to be important and clinically significant. These findings are in line with those reported by two previous meta-analyses.40,78 For instance, Kang et al. reported that pedometer-based interventions can significantly increase daily steps in both adults and children. 40 Recently, a study by Chaudhry et al. indicated that in adults, step-count monitoring interventions can increase daily steps by 1.126 steps/day at ≤ 4 months, 1.050 steps/day at 6 months, 464 steps/day at 1 year, 121 steps/day at 2 years, and 434 steps/day at 3–4 years. 78 In contrast to these meta-analyses, our study only focused on children and adolescents. Given our findings and the fact that step-count monitoring devices are easy to use for children and adolescents,24,29–31 we believe that step-count monitoring interventions may be an effective and suitable method for increasing total physical activity in this population.
The WHO recommends MVPA for maintaining physical and mental health in children and adolescents.1,2,79 Although the effect of step-count monitoring interventions on MVPA has not been explored so far in children and adolescents, two previous studies have examined the effects of wearable activity tracker-based interventions (including pedometers, smartwatches, fitness wristbands; excluding smartphone applications) on MVPA in this population.27,80 While Casado-Robles et al. reported that wearable activity tracker-based interventions have a significant effect on MVPA, 27 Whitney et al. found no such improvement in MVPA following these interventions. 80 Unlike these two studies, which combined step-count and physical activity monitoring interventions, our meta-analysis only focused on step-count monitoring interventions. Notably, our results were consistent with those reported by Whitney et al. 80 One potential reason for the failure of step-count monitoring interventions to achieve improvements in MVPA may lie in the importance of self-monitoring and goal-setting in promoting physical activity via mHealth.81–84 Since the step-count monitoring intervention programs included in this study did not provide MVPA feedback or set MVPA targets, the goal of increasing MVPA was not fulfilled. Moreover, different studies used accelerometers to measure MVPA based on different cut-off points and intervals, impacting the accuracy of MVPA data.80,85 Therefore, the results of our study must be interpreted with caution. According to Marshall et al., completing 3.000 steps in 30 min corresponds to moderate-intensity physical activity. 86 Thus, we recommend that step-count monitoring programs set a goal of completing more than 3.000 steps in a 30-min period to enhance the intensity of physical activity and increase MVPA among children and adolescents.
LPA, which includes activities of daily living and any body movement (e.g., walking, housework, and gardening), is the most common form of physical activity.87–89 LPA is inversely associated with the risk of all-cause mortality and correlates favorably with several cardiometabolic risk factors.2,90 Our findings suggested that step-count monitoring interventions cannot significantly improve LPA, consistent with Casado-Robles's study. 27 Nevertheless, it is important to interpret this result with caution, since only six studies that measured LPA were included in our meta-analysis. In addition, the primary goal of these studies was to increase daily steps or MVPA. LPA was often only a secondary goal, and no specialized intervention strategies were designed to increase LPA. According to time-use epidemiology, the sum of all human activities in a day is a fixed constant (24 h, and changes in any one activity inevitably lead to corresponding changes in other activities.91,92 Recent studies on compositional isochronous substitution have shown that the isochronous substitution of MVPA with LPA tends to have a negative effect on health, while the isochronous substitution of SB with LPA tends to have a positive effect.93–97 Therefore, future studies should explore how step-count monitoring interventions can be applied to convert SB time into LPA time in order to obtain health benefits.
SB is typically characterized by remaining in a sitting or lying position during waking hours and involves low energy expenditure.98,99 As electronic devices have become increasingly popular, children and adolescents are spending more time watching television and using cell phones and computers.100–102 As a result, the amount of SB among children and adolescents has increased dramatically. SB has been shown to increase the risk of cardiovascular disease, obesity, depression, and other disorders.103–106 Therefore, effective and scalable interventions are urgently required to reduce SB in children and adolescents. Our results suggested that step-count monitoring interventions tend to reduce SB in this population (MD −3.42 min/day, P = 0.05), similar to the findings reported by Casado-Robles. 27 The use of step-count monitoring interventions to increase total physical activity (whether LPA or MVPA) can reduce SB if the duration of sleep is not drastically changed.91,92 In addition, these interventions can easily be integrated into the daily lives of children and adolescents and can be implemented on a large scale.23,29,31,76 Therefore, step-count monitoring interventions may be a viable and effective method for reducing SB in children and adolescents.
Interestingly, our subgroup analysis suggested that step-count monitoring interventions are more effective at increasing MVPA in children than in adolescents. However, in the study by Casado-Robles, participant age was not found to influence the effectiveness of the intervention. 27 This could be because our study focused only on step-count monitoring, which is simple and interesting for children. 26 Moreover, children often do not have firmly established lifestyles and routines and are more adaptable to change.26,107,108 In contrast, adolescents are in a developmental phase characterized by mood swings and dramatic physiological changes. During this stage, they tend to exhibit rebellious behavior, which could create resistance and non-conformance with the intervention program, thus hindering its outcomes. 109
In addition, our subgroup analysis also showed that pedometer-based programs are more effective at increasing daily steps than programs based on other emerging step-count monitoring devices, in line with Chaudhry's findings. 78 This could be because other emerging step-count monitoring devices (e.g., wearable activity trackers and smartphone applications) not only provide information on daily steps, but also on aspects like heart rate and the intensity of physical activity. In contrast, pedometers only provide information regarding daily steps. 110 Such simple, direct feedback may be more useful for children and adolescents when they only focus on daily steps. Interestingly, our subgroup analyses also demonstrated that multi-component comprehensive interventions do not offer advantages over single step-count monitoring interventions. These results suggest that a “less is more” step-count monitoring intervention strategy may be more appropriate for increasing daily steps in children and adolescents.
Previous studies show that interventions based on tailored information offer greater benefits.111–113 One advantage of mHealth interventions lies in the ability to provide individualized service in a cost-effective manner.112–114 Therefore, we performed subgroup analyses to examine whether intervention programs with individualized goals (setting step-count goals based on each individual's baseline step count) can yield better effects. Unfortunately, our results indicated that intervention programs with individualized goals did not yield better improvements in daily steps and MVPA than programs without such goals. Meanwhile, another subgroup analysis suggested that the duration of the intervention did not influence its effectiveness. Future research should explore the best strategies to establish step-count goals and intervention durations for obtaining better outcomes.
Strengths and limitations
This meta-analysis has some advantages. First, to our knowledge, this study is the first to synthesize evidence regarding the effectiveness of step-count monitoring interventions on accelerometer-measured MVPA, LPA, and SB in children and adolescents. Second, the intervention tools used in this study only included step-count monitoring devices, which are simple, cost-effective, and suitable for children and adolescents. Third, subgroup analyses were conducted to determine the influence of intervention program characteristics on target outcomes. Finally, the study only included objectively measured physical activity-related measures, which are more reliable than self-reported measures.
Nevertheless, this meta-analysis also has some limitations. First, there was considerable heterogeneity in daily steps and MVPA among the different studies. This could be attributed to the variability in intervention designs, participants, intervention tools, intervention strategies, intervention durations, comparators, and study quality. Therefore, the results of this meta-analysis must be treated with caution. Second, because none of the studies blinded participants or staff to group allocation, there was a high risk of performance bias. Moreover, 15 studies showed a high risk of selection bias due to the lack of reporting on allocation concealment and random sequence generation. Additionally, 9 studies had > 20% attrition rates, thus presenting a high risk of attrition bias. These methodological shortcomings may lead to biased assessments of intervention effects, overestimating or underestimating the true effect of the intervention. Third, since only immediate post-intervention data were examined, we were unable to explore whether the effectiveness of step-count monitoring interventions could be sustained over time. Finally, funnel plots indicated the presence of possible publication bias in the daily step and SB indicators. Thus, more robust RCTs are needed in the future to validate our findings and to explore whether the effects of the intervention can be sustained over time.
Conclusions
The present study indicates that step-count monitoring interventions can significantly increase daily steps and may also reduce SB. However, these interventions do not appear to have significant effects on MVPA and LPA. Moreover, our findings show that step-count monitoring interventions are more effective at increasing MVPA in children than in adolescents, and that pedometer-based interventions are more effective at increasing daily steps than those based on other emerging step-count monitoring devices. These findings provide key insights, demonstrating to the public and health policymakers that step-count monitoring interventions can serve as an appropriate and effective method for increasing total physical activity and reducing SB among children and adolescents and also for improving MVPA among children. We recommend that step-count monitoring programs set a goal of completing more than 3.000 steps in a 30-min period to enhance the intensity of physical activity and increase MVPA among children and adolescents. Moreover, we recommend a “less is more” strategy of step-count monitoring interventions to increase physical activity among children and adolescents. In the future, investigations into the optimal strategies for establishing step-count goals and intervention durations to obtain improved outcomes will be required.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076251374249 - Supplemental material for Effectiveness of step-count monitoring interventions in increasing physical activity among children and adolescents: A systematic review and meta-analysis
Supplemental material, sj-docx-1-dhj-10.1177_20552076251374249 for Effectiveness of step-count monitoring interventions in increasing physical activity among children and adolescents: A systematic review and meta-analysis by Wentao Wang, Cong Huang, Yi Shen, Jing Cheng and Ling Wang in DIGITAL HEALTH
Supplemental Material
sj-docx-2-dhj-10.1177_20552076251374249 - Supplemental material for Effectiveness of step-count monitoring interventions in increasing physical activity among children and adolescents: A systematic review and meta-analysis
Supplemental material, sj-docx-2-dhj-10.1177_20552076251374249 for Effectiveness of step-count monitoring interventions in increasing physical activity among children and adolescents: A systematic review and meta-analysis by Wentao Wang, Cong Huang, Yi Shen, Jing Cheng and Ling Wang in DIGITAL HEALTH
Footnotes
Acknowledgments
We sincerely appreciate the support and assistance provided by Zhejiang University.
Consent statement
As the present study was a systematic review, patient consent statements were not necessary.
Contributorship
WW conceptualized the research, completed the data analysis, and wrote the original manuscript. JC and LW completed the risk-of-bias assessment and data extraction. CH and LW revised and edited the manuscript. All authors have read and approved the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Major Humanities and Social Sciences Research Projects in Zhejiang higher education institutions (Grant Number: 2024QN153).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Registration and protocol
The protocol for this review was registered in the PROSPERO (CRD42025642254).
Guarantor
WW.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.