
Abstract
Background
Children and adolescents who are overweight and obese represent a growing public health issue. The use of step-monitoring devices as an intervention tool may be a simple, cost-effective, and easily replicable solution for addressing obesity in children and adolescents. No prior systematic reviews have evaluated the effectiveness of utilizing step-monitoring devices as an intervention method for obesity in children and adolescents.
Methods
Previous studies on using step-monitoring devices to prevent and treat obesity in children and adolescents were identified in the following databases: Web of Science, EMBASE, PubMed, Cochrane Library, SPORTDiscus, and SCOPUS. The search period for each database ranged from the year of their inception to 8 March 2023 (updated in June 2024). Meta-analyses were performed for mean differences (MDs) in body mass index (BMI), BMI z-score (BMI-Z), body fat, waist circumference, and body weight.
Results
From 12,907 relevant records, 23 studies were included in this meta-analysis. The included studies were mainly at low risk of bias, except for blinding. Step-monitoring device-based interventions had significant effects in reducing BMI-Z (MD −0.06; 95% CI −0.10 to −0.02), body fat (MD −0.95%; 95% CI −1.35 to −0.54), and body weight (MD −1.23 kg; 95% CI −2.36 to −0.10). However, there was no significant effect on BMI (MD −0.16 kg/m2; 95% CI −0.55 to 0.22) and waist circumference (MD −0.33 cm; 95% CI −1.23 to 0.58). Subgroup analyses indicated that participants who were overweight or obese showed greater intervention effects on BMI and BMI-Z compared to participants with normal weight. The programs with an intervention duration of ≤6 months presented a greater intervention effect on BMI-Z than those with an intervention duration of more than 6 months. The programs that established goals had a greater intervention effect on body fat than those that did not.
Conclusions
Step-monitoring devices may be an effective and generalizable intervention tool for the prevention and treatment of obesity in children and adolescents. Future studies should further explore how to set step goals and the duration of interventions to achieve better intervention effects.
Introduction
Globally, more than 340 million children and adolescents were classified as overweight or obese in 2016. 1 Children and adolescents with overweight and obesity represent a large public health issue, while obesity in childhood and adolescence increases the risk of obesity in adulthood, 2 and it is strongly associated with incidences of chronic disease (e.g. cardiometabolic disease, 3 type 2 diabetes, 4 and hypertension 5 ). Physical activity is important in the prevention and treatment of obesity in children and adolescents.6–8 However, based on data from the World Health Organization, more than 80% of adolescents are insufficiently physically active. 9 Many studies use physical activity interventions to achieve weight loss in children and adolescents. However, these interventions are often labor-intensive and costly, and are difficult to implement on a large scale.10–14 Therefore, identifying innovative and effective physical activity intervention strategies to address obesity in children and adolescents is urgent.
Walking is a common, safe, convenient, and free form of physical activity that can be incorporated into daily life and easily controlled in duration and intensity.15–17 Notably, it is considered close to being the perfect physical activity.15,16,18,19 Furthermore, previous studies have published guidelines on public health physical activity for children and adolescents in steps.20–23 Moreover, the recommended standard of 10,000 or 12,000 steps per day is easier to understand for children and adolescents than the recommended standard of 60 min of moderately intense physical activity per day. Thus step-counting interventions may be more appropriate for child and adolescent populations.20,24–27 Additionally, technological advancement in a number of step-monitoring devices (e.g. pedometers, smartwatches, wristbands, and smartphone applications) have increased their popularity among children and adolescents, whereby they do not only objectively measure steps but also improve physical activity levels through self-monitoring, feedback, and goal-setting.26,28–31 Therefore, using step-monitoring devices to promote physical activity, increase energy expenditure, and thus weight loss may be a simple, cost-effective, and easily scalable option for addressing obesity in children and adolescents.
Many studies have been conducted to explore the effects of using step-monitoring devices to prevent and treat obesity in children and adolescents.32–42 However, the results of these studies have been largely inconclusive. Some studies into interventions, using step-monitoring devices, have effectively improved obesity-related indicators in children and adolescents.34,38–40 For example, a study by Staiano et al. showed that the intervention group using a pedometer with established goals demonstrated significant reductions in BMI z-scores (BMI-Z) (P = 0.01) and body mass index (BMI) (P = 0.02). 34 However, some studies have not achieved positive effects from interventions,36,41,42 such as the study by Bowen-Jallow et al., which suggested that there were no significant decreases in BMI, waist circumferences, and body weights in a Fitbit intervention group, whose goal was 10,000 steps per day. 32 Therefore, there is a need for a systematic review and meta-analysis to objectively analyze all available findings, and provide more accurate and convincing evidence for the public and researchers. Although previous meta-analyses have explored the effects of using pedometers to prevent and treat obesity, these meta-analyses were conducted using adult populations and only included pedometers, meaning other emerging step-monitoring devices (e.g. wristbands or smartphone applications) were not included.43,44 In addition, previous systematic reviews and meta-analyses have focused on exploring the use of wearable activity trackers (including step monitoring and physical activity monitoring) to promote physical activity in children and adolescents, with little attention paid to the use of wearable activity trackers to prevent and treat obesity in children and adolescents.30,31,45 Therefore, it is necessary to conduct an updated meta-analysis to explore the effectiveness of utilizing step-monitoring devices to prevent and treat obesity in children and adolescents.
The objectives of this study were to (1) assess the effectiveness of step-monitoring device-based interventions on obesity-related outcomes in children and adolescents, (2) identify whether the characteristics of the intervention population (e.g. weight status and age) influenced the effect size, and (3) determine whether the features of the intervention program (e.g. duration and goal-setting) influenced the effect size. The findings of this study will provide guidance to the public and researchers on whether to choose step-monitoring devices and how to use them to prevent and treat obesity in children and adolescents.
Methods
Study design
We performed and reported this systematic review following the Preferred Reporting Items for Systematic Review and Meta-Analyses (PRISMA) guidelines 46 (PRISMA checklist in Multimedia Appendix 1). The review protocol was registered with PROSPERO (CRD42024496990).
Search strategy
Previous studies on using step-monitoring devices to prevent and treat obesity in children and adolescents were identified in the following web-based databases: Web of Science, EMBASE, PubMed, Cochrane Library, SPORTDiscus, and SCOPUS. The search period for each database ranged from the year of their inception to 8 March 2023. An updated search was conducted in June 2024 and four eligible studies were found. Each search was conducted using a combination of subject and free terms, and the search strategies were formulated according to the characteristics of the different databases. The search strategies for all databases are available in Multimedia Appendix 2. We also performed a “snowball search” to identify additional studies by searching the reference lists of the included studies and earlier reviews and searching the reference citations in the Web of Science database.
Inclusion and exclusion criteria
According to the PICOS (population, intervention, comparison, outcomes, and study) model, the inclusion criteria were as follows:
Population: Children and adolescents aged 3–18 years Interventions: Intervention groups that used step-monitoring devices (e.g. pedometers, wristbands or smartphone applications) as motivational tools to promote physical activity Comparison: Control groups that did not involve step-monitoring devices (e.g. usual care, control or no intervention) Outcomes: Primary outcomes included obesity-related anthropometric indicators (e.g. BMI, body fat, body weight, BMI-Z, and waist circumference) The study used a randomized controlled trial (RCT) design. The participants were adults. Step-monitoring devices in the intervention groups were used to obtain objective measurements of physical activity rather than as intervention tools to promote physical activity. The outcome did not include obesity-related anthropometric indicators (e.g. blood pressure, stress parameters, and chronic low back pain). The study design was not an RCT. Studies that were reviews or conference papers.
The exclusion criteria were as follows:
Data extraction
The results of the literature searches in the different databases were combined to create a database of information in EndNote X9 software. According to the inclusion and exclusion criteria, two researchers independently screened the literature and read the full texts to determine whether to include or exclude each study. Where a disagreement occurred, a consensus was reached through discussion or reference to third-party opinions.
Two researchers created their extraction forms and extracted the following information: basic information on the included literature: first author, year of publication, country, and study title; basic information of the participants: sample size, sex, age, and weight status; intervention design: intervention method, intervention duration, and intervention tool; outcome indicators: BMI, BMI-Z, body fat, body weight, and waist circumference.
Cohen's kappa coefficient was used to test for differences between the two authors in data screening and selection.
Risk of bias assessment
The quality of the included literature was evaluated according to the criteria of the Cochrane Handbook for Systematic Reviews, version 5.1, which included seven items: sequence generation, allocation sequence generation, blinding of participants and personnel, blinding of outcome assessment, incomplete outcome data, selective outcome reporting, and other sources of bias. Meeting a criterion was considered low risk, while not meeting a criterion was considered high risk. It was noted as uncertain, alongside a reason if it was not mentioned in the text. Two investigators evaluated the quality of the literature independently, and in the case of a disagreement, a third investigator was added to discuss and reach a unified opinion. 47
Statistical analysis
Review Manager (RevMan) 5.4.1 was used for the meta-analysis, publication bias testing, and sensitivity analysis. Continuous variables were used as the outcome indicators in the included literature. Therefore, this study calculated pooled effect sizes using mean differences (MDs) with 95% confidence intervals (CIs). I2 statistics and Cochran's Q test measured the heterogeneity between studies. It was categorized as unimportant, moderate, substantial, and considerable if the I2 values were 0%–30%, 30%–60%, 60%–75%, and 75%–100%, respectively. 48 If there was no statistical heterogeneity between studies, a fixed effects model was used for the meta-analysis. If there was statistical heterogeneity among studies, a random effects model was used. If the study has multiple intervention groups, the data from each intervention group will be treated as an independent sample, and the sample size of the control group will be equally distributed to each intervention group. If the study had multiple measurement time points, immediate post-intervention data were used for meta-analysis. We converted these data to SD for included studies that reported standard error (SE) or 95% CI. Subgroup analyses were performed to determine whether the characteristics of the included studies (e.g. weight status, age, duration, and goal-setting) influenced the effect size. According to the Stages of Behavioral Change Model, the 6-month duration was used as the cut-off point for dividing into short term and long term.49,50 Publication bias was evaluated by visually inspecting funnel plot symmetry. The stability of the pooled results was tested by removing the studies with an assessed risk of bias for the sensitivity analysis.
Results
Study selection
The process of selecting the studies for inclusion is presented in Figure 1. A total of 12,754 related records were retrieved from 6 databases. An additional 153 records were found through a “snowball search.” After deleting duplicates, 6870 records remained. After screening the titles and abstracts, 6402 records were excluded. The remaining 468 studies were assessed based on their full texts. A further 135 studies were excluded owing to the participants being older than 18 years, 109 studies were excluded because they did not use step-monitoring devices to promote physical activity, 122 studies were excluded as their results did not include obesity-related anthropometric indicators, and 79 studies were excluded because they were not RCTs. Ultimately, 23 studies were included in this meta-analysis. The Cohen's kappa coefficient between the two authors was 0.92, suggesting high consistency.

The process of selecting the studies for inclusion.
Study characteristics
Table 1 summarizes the study characteristics included in the systematic review. The 23 included studies were published between 2008 and 2024. Eight were conducted in Australia,38,39,41,51–55 three in the United States,32–34 three in the United Kingdom,56–58 with three in Spain,40,59,60 one in China, 61 one in Germany, 37 one in Switzerland, 35 one in New Zealand, 36 one in Thailand, 62 and one in Singapore. 42 A total of 4817 participants were enrolled in this study, and the average age was 12.1 years (3.9–18 years). The dropout rate for the included studies averaged 15.67% (755/4817) and ranged from 0% (0/31) to 61.7% (29/47). The average intervention duration was 5.45 months (1.5–13 months). Participants in 16 of the 23 included studies had normal weight,36,37,39,41,42,51–61 whereas participants in seven studies were either overweight or obese.32–35,38,40,62 Pedometers were used as the intervention tool in 19 of the studies,33,34,36–42,51–58,61,62 while the four remaining studies used other step-monitoring devices (e.g. Fitbit and App).32,35,59,60 A total of 14 studies employed step intervention goals (e.g. 10,000 steps or 500 steps/day increase each week above the baseline) as the intervention strategy,32,34–37,39,40,42,56–60,62 while 9 studies used only step monitoring without goals.33,38,41,51–55,61 In terms of outcome indicators, 14 studies included BMI,32,34,38–42,51–53,56,59–61 11 studies included BMI-Z,33,34,36,39,51–57 13 studies included body fat,33,35,37–41,51,54,56,58,60,62 11 studies included waist circumference,32,35,38,39,41,52,53,56,59–61 and 7 studies included body weight.32,34,38,39,59–61
Characteristics of included studies.

BMI: body mass index; WC: waist circumference; BMI-Z: BMI z-score.
Risk of bias assessment
A summary of the risk of bias is provided in Multimedia Appendix 3. Due to the nature of the interventions, all studies were determined to have a high risk of bias in blinding participants and personnel. Most of the studies (20/23) were determined to have a low risk of bias in random sequence generation, except for 3 studies, which had a high risk of bias.34,56,61 In the allocation concealment, 9 studies were rated with a low risk of bias,37,41,42,51,52,54,55,57,58 11 studies were rated with an unclear risk of bias,32–35,38,40,53,56,59,60,62 and 3 studies were rated with a high risk of bias.36,39,61 Due to the objective outcome measures, all studies were considered to have a low risk of bias in terms of blinding of outcome assessment. Five studies had a high risk of bias regarding incomplete outcome data,32,33,37,38,62 all of which had a high attrition rate (>20%). Due to the baselines in the intervention and control groups being significantly different, five studies were assessed as having a high risk for other sources of bias.34,36,37,56,61 All studies had a low risk of bias regarding selective outcome reporting.
Effects of intervention
BMI
Fourteen studies assessed the effects of step-monitoring device-based interventions on BMI.32,34,38–42,51–53,59–61 The intervention group did not show a significant reduction in BMI (MD −0.16 kg/m2; 95% CI −0.55 to 0.22; P = 0.41) compared to the control group; heterogeneity was considerable and significant (I2 = 82%; P < 0.01) (Figure 2). There was no publication bias in BMI based on the visual assessment of the funnel plot (Multimedia Appendix 4).
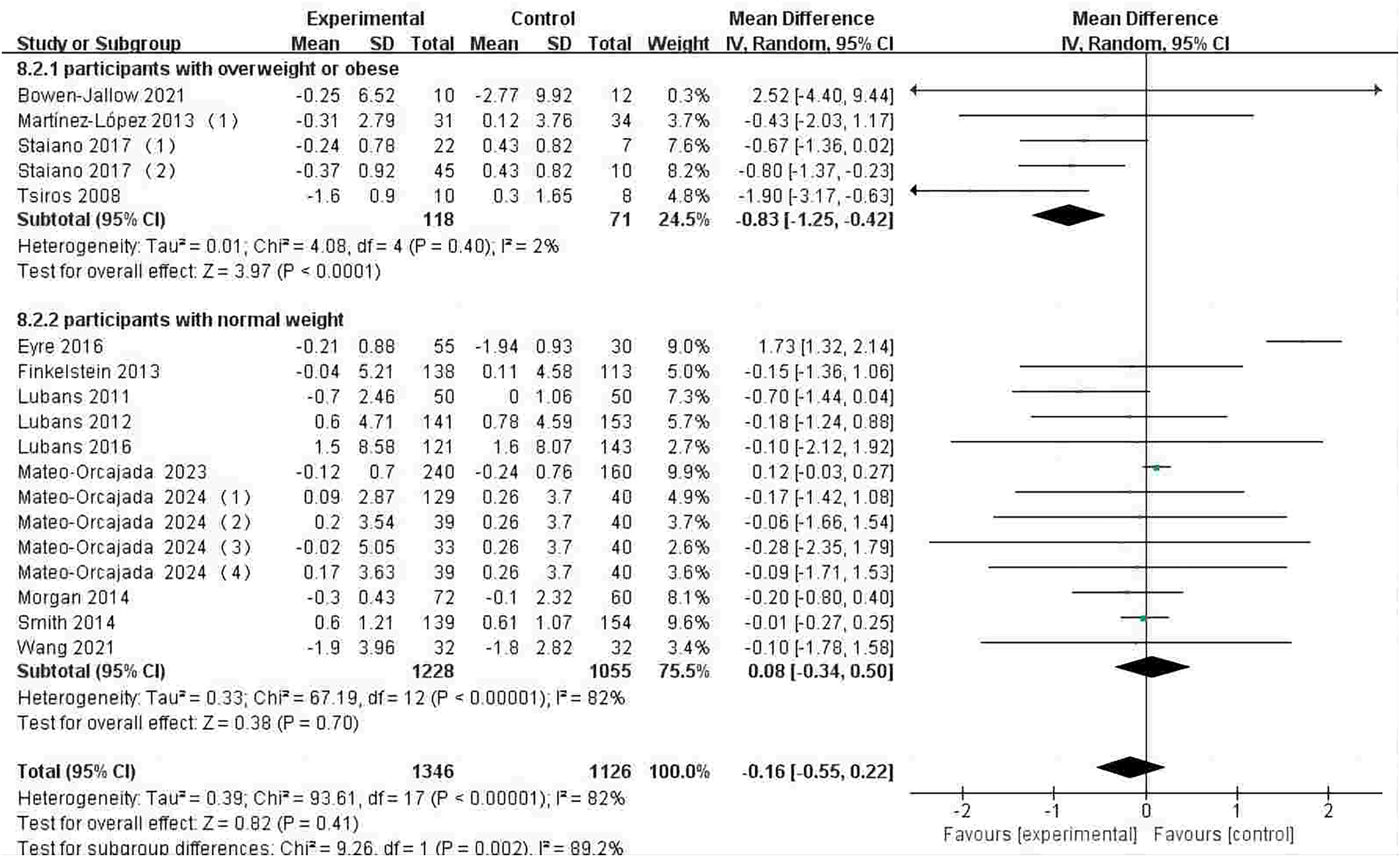
Forest plot of the effect of step-monitoring device-based interventions on BMI (kg/m2).
BMI-Z
Eleven studies assessed the effects of step-monitoring device-based interventions on BMI-Z.33,34,36,39,51–57 The intervention group showed a significant reduction in BMI-Z (MD −0.06; 95% CI −0.10 to −0.02; P < 0.01) compared to the control group; heterogeneity was moderate and significant (I2 = 47%; P < 0.05) (Figure 3). There may be publication bias in BMI-Z due to the visual assessment of the funnel plot (Multimedia Appendix 5).
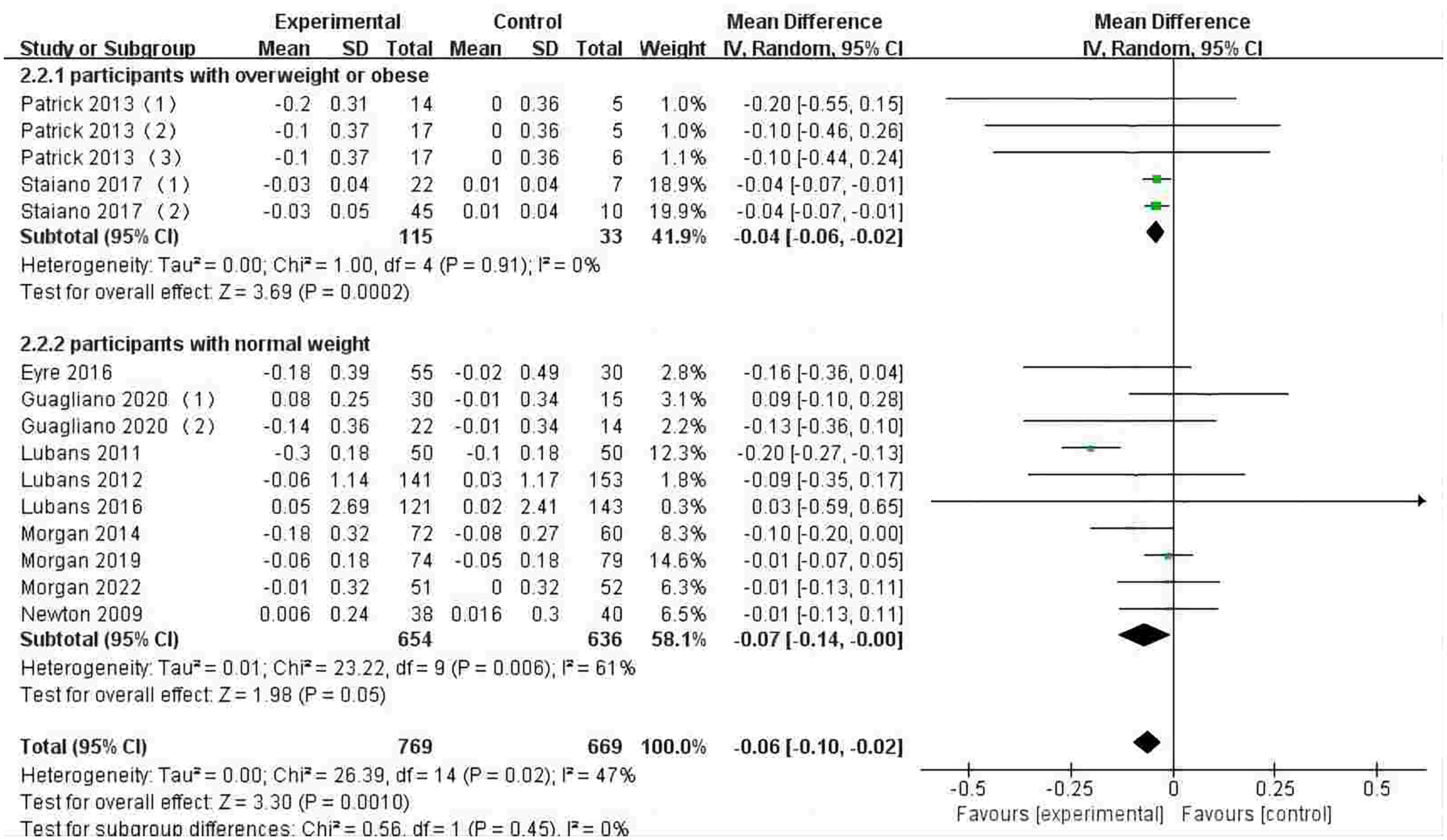
Forest plot of the effect of step-monitoring device-based interventions on BMI z-score.
Body fat
Thirteen studies assessed the effects of step-monitoring device-based interventions on body fat.33,35,37–41,51,54,56,58,60,62 The intervention group showed a significant reduction in body fat (MD −0.95%; 95% CI −1.35 to −0.54; P < 0.01) compared to the control group; heterogeneity was unimportant and insignificant (I2 = 10%; P = 0.33) (Figure 4). There was no publication bias in body fat by visual assessment of the funnel plot (Multimedia Appendix 6).

Forest plot of the effect of step-monitoring device-based interventions on body fat (%).
Waist circumference
The effects of step-monitoring device-based interventions on waist circumference were assessed in 11 studies.32,35,38,39,41,52,53,56,59–61 The intervention group did not show a significant reduction in waist circumference (MD −0.33 cm; 95% CI −1.23 to 0.58; P = 0.48) compared to the control group; heterogeneity was substantial and significant (I2 = 68%; P < 0.01) (Figure 5). There was no publication bias in waist circumference by visual assessment of the funnel plot (Multimedia Appendix 7).

Forest plot of the effect of step-monitoring device-based interventions on waist circumference (cm).
Body weight
The effects of step-monitoring device-based interventions on body weight were assessed in seven studies.32,34,38,39,59–61 The intervention group showed a significant reduction in body weight (MD −1.23 kg; 95% CI −2.36 to −0.10; P < 0.05) compared to the control group; heterogeneity was substantial and significant (I2 = 65%; P < 0.05) (Figure 6). There may be publication bias in body weight due to the visual assessment of the funnel plot (Multimedia Appendix 8).
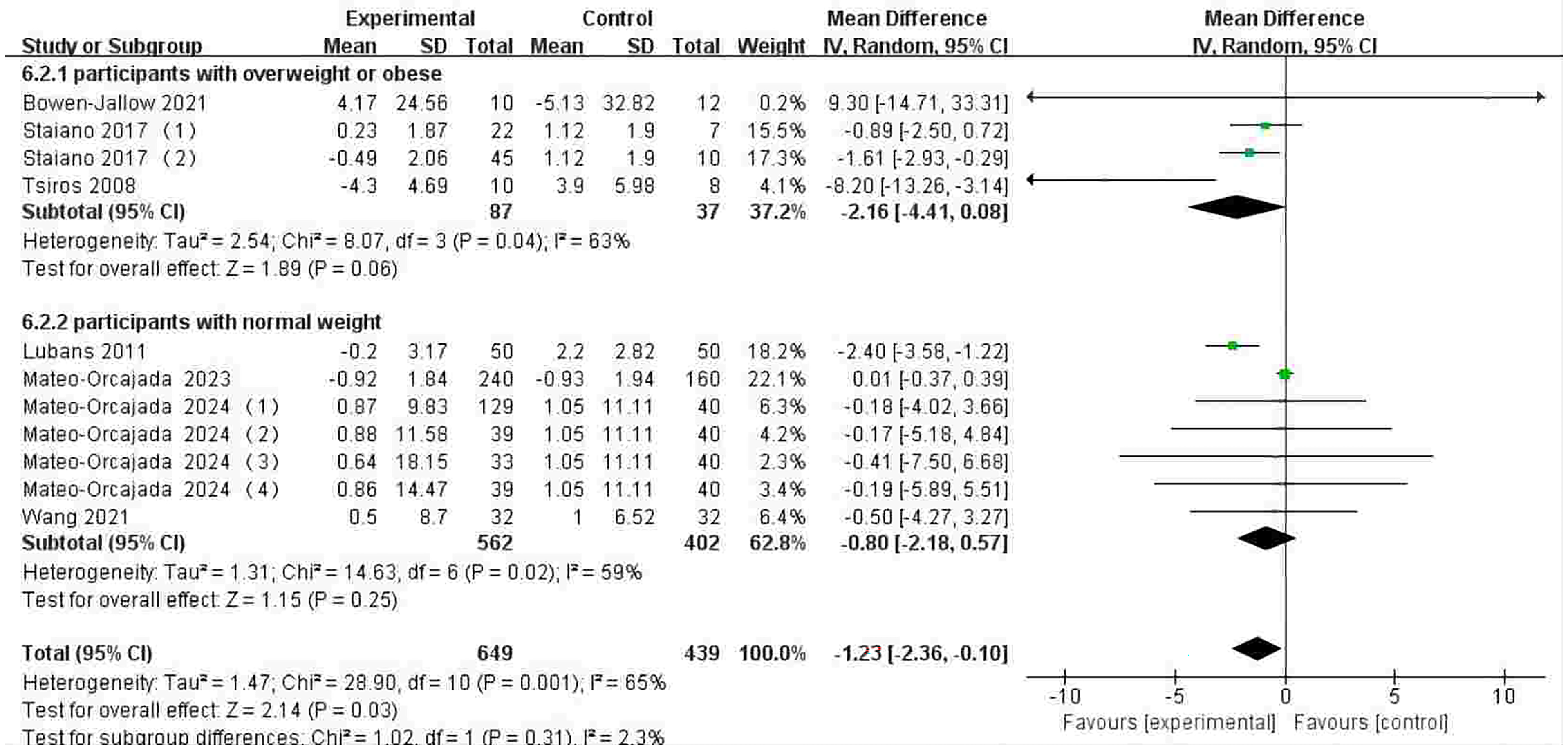
Forest plot of the effect of step-monitoring device-based interventions on body weight (kg).
Subgroup analyses
The subgroup analyses indicated that the participants who were overweight or obese showed greater intervention effects on BMI (MD −0.83 kg/m2; P < 0.01) and BMI-Z (MD −0.04; P < 0.01) compared to participants with normal weight. However, participants who were obese or overweight did not show greater intervention effects on body fat, waist circumference, and body weight.
The participants with a mean age >12 years showed greater intervention effects on BMI (MD −0.32 kg/m2; P < 0.05) and BMI-Z (MD −0.08; P < 0.01) compared to participants with a mean age ≤12 years. However, regardless of whether the participants had a mean age of >12 years or ≤12 years, all of the intervention groups achieved significant intervention effects on body fat.
The programs with an intervention duration of ≤6 months (MD −0.06; P < 0.01) presented a greater intervention effect on BMI-Z compared to the programs with an intervention duration of more than 6 months. However, all intervention groups presented significant intervention effects on body fat, regardless of whether the programs had an intervention duration of ≤6 months or more than 6 months. On the contrary, the intervention groups did not achieve a significant intervention effect on BMI.
The programs that established goals had a greater intervention effect on body fat (MD −1.11%; P < 0.01) than those that did not. However, the programs that did not establish goals had a greater intervention effect on BMI-Z (MD −0.04; P < 0.01) than those that did. Regardless of whether the programs established a goal, all of the intervention groups did not achieve a significant intervention effect on BMI (Table 2).
Results of subgroup analyses.

BMI: body mass index. BMI-Z: BMI z-score.
Discussion
Main findings
This study summarized the evidence on the effectiveness of step-monitoring device-based interventions in improving obesity-related indicators in children and adolescents. The meta-analysis showed that step-monitoring device-based interventions significantly reduced BMI-Z, body fat, and body weight. However, there was no significant effect on BMI and waist circumference. The subgroup analyses indicated that the participants who were overweight or obese showed greater intervention effects on BMI and BMI-Z compared to participants of normal weight. The participants with a mean age >12 years showed greater intervention effects on BMI and BMI-Z than those with a mean age ≤12 years. The programs with an intervention duration of ≤6 months presented a greater intervention effect on BMI-Z than the programs with an intervention duration of more than 6 months. Moreover, the programs that established goals were found to have a greater intervention effect on body fat than the programs in which no goals were established. However, the programs that did not establish goals had a greater intervention effect on BMI-Z than those that did.
Our results showed that step-monitoring device-based interventions led to statistically significant reductions in BMI-Z (–0.06) and body weight (–1.23 kg) in children and adolescents. However, according to previous studies, a reduction of at least 0.25 BMI-Z is clinically meaningful for improving cardiovascular health in children and adolescents.63–65 Our pooled effect sizes were small and lack of clinical significance. Although our results are not clinically meaningful, we still recommend using step-monitoring devices to prevent and treat obesity in children and adolescents. Because step-monitoring device-based interventions are easy to incorporate into your life and don't require considerable changes to your life, and a small change can have a positive effect, we think this is a recommendable option.65,66 In addition, there are two advantages to utilizing step-monitoring devices when preventing and treating obesity in children and adolescents: (1) step feedback is simpler and easier to understand for children and adolescents compared to metrics such as moderate-intensity physical activity, calories, and heart rate; (2) step-monitoring devices are popular and step-monitoring interventions are cost-effective and easy to implement on a large scale.17,20,22,24,27
Our meta-analysis showed that step-monitoring device-based interventions led to significant reductions in BMI-Z, body fat, and body weight of children and adolescents, which was in accordance with the results of two previous meta-analyses.43,44 The meta-analysis by Richardson et al. showed that pedometer-based walking interventions achieved an average weight loss of 1.27 kg (95% CI −1.85 to −0.70; P < 0.01) in adults with overweight or obese. 43 Furthermore, the findings by Cai et al. study demonstrated that pedometer-based interventions significantly decreased weight (MD −0.65 kg; 95% CI −1.12 to −0.17; P < 0.01) in adults with overweight or obese. 44 This suggests that step-monitoring devices can be used as intervention tools in weight loss programs for adults, children, and adolescents. According to the Behavioral Intervention Technique Model, step-monitoring devices are used mainly through self-monitoring, feedback, goal-setting, and competition to motivate participants to engage in physical activity, reduce their sedentary time, and increase their energy expenditure, to ultimately reduce obesity indicators.28,45,67–72 We also need to treat this result with caution. Because some of the included studies were multifaceted interventions and the step-monitoring intervention was only one part of the multifaceted intervention, we could not exclude the effects of other components (e.g. diet control, parental involvement, and reward) of the multifaceted interventions on the obesity indicators, meaning that these could have potentially affected the results of our meta-analysis.
Mobile health technology can be used to prevent and treat obesity, mainly through three strategies: promoting physical activity, enhancing communication and guidance, and monitoring food consumption. 73 Previous systematic reviews and meta-analyses have summarized the evidence for the effects of mHealth technology interventions on obesity in children and adolescents. However, most of these systematic reviews and meta-analyses involved a mix of the three intervention strategies, and the results were inconclusive.74–81 Therefore, these cannot be used to provide advice to the public and researchers on which strategy is more appropriate for the prevention and treatment of obesity in children and adolescents. In addition, the meta-analysis by Park et al. summarized evidence on the prevention and treatment of obesity in children and adolescents only through enhanced communication and guidance and showed no significant effects of information and communication technology interventions on reducing BMI, body weight, BMI-Z, waist circumference, and body fat. 82 However, the meta-analysis by Wang et al. summarized the evidence on the prevention and treatment of obesity in children and adolescents by only promoting physical activity. It showed that using wearable devices as physical activity interventions significantly reduced body fat, BMI-Z, BMI, and body weight. 83 Similarly, our meta-analysis also summarizes the evidence on the prevention and treatment of obesity in children and adolescents by only promoting physical activity and presenting positive results. This suggests that the strategy of promoting physical activity is an appropriate choice for mHealth technology to prevent and treat obesity in children and adolescents.
Our meta-analysis showed that step-monitoring device-based interventions did not lead to a significant reduction in BMI. This was inconsistent with the results of another meta-analysis. The meta-analysis by Richardson et al. showed that pedometer-based walking interventions significantly reduced BMI (MD −0.15 kg/m2; 95% CI −0.29 to −0.02; P < 0.01) in overweight and obese adults with type 2 diabetes. 43 As this meta-analysis has a considerable and significant heterogeneity, we must treat this result cautiously. Moreover, as our study participants were children and adolescents at a sensitive stage of physical development, the use of BMI to evaluate their obesity status may be inappropriate. In contrast, BMI-Z and body fat are more sensitive and accurate indicators of obesity.84,85
Our meta-analysis showed that step-monitoring device-based interventions did not lead to a significant reduction in waist circumference. Waist circumference is an important indicator of abdominal obesity. However, no previous meta-analyses have explored the effect of step-monitoring device-based interventions on waist circumference, meaning that we could not make any overall comparisons. Although our results suggest that it is necessary to add specialized training movements and training programs for waist circumference to reduce waist circumference, increasing physical activity using step-monitoring devices alone is not feasible. Due to the significant heterogeneity of this meta-analysis, we need to treat this result with caution.
With the development of technology, newly emerging step-monitoring devices (e.g. smartwatches, wristbands, and smartphone applications) are becoming more popular and offer functional advantages over traditional pedometers.86–88 Therefore, in this meta-analysis, we tried to use subgroup analyses to explore whether emerging devices with functional advantages can achieve better intervention outcomes. The results indicated that the use of traditional pedometers could achieve better effects on body weight (–1.94 kg; P < 0.01) and body fat (–0.98 kg; P < 0.01) than the use of emerging step-monitoring devices. In previous systematic reviews and meta-analyses, it has been suggested that the use of traditional pedometers can better promote physical activity compared to the use of emerging step-monitoring devices. 89 These results suggested that using single-function pedometers may be more effective than using multifunctional emerging step-monitoring devices when we perform step-monitoring interventions. However, because only four studies in this meta-analysis used emerging devices as intervention tools, we must treat this result with caution.32,35,59,60 Therefore, future studies are needed to further explore the efficacy of emerging step-monitoring devices as intervention tools in the prevention and treatment of obesity in children and adolescents.
The subgroup analyses indicated that participants who were overweight or obese showed greater intervention effects in reducing BMI and BMI-Z compared to the participants of normal weight. This finding was consistent with other systematic reviews and meta-analyses.70,83 The potential reason for this is that people with overweight and obesity tend to be physically inactive and may not realize that they are physically inactive.90,91 Step-monitoring devices can objectively record the user's physical activity and quantify the gap between the current level of physical activity and that recommended by the WHO, which can motivate them to be more physically active. Therefore, the intervention effect was significant.92,93 Conversely, people with normal weight tend to be physically active, meaning the quantified gap cannot motivate them to be physically active, so the intervention effect was not obvious.30,92–97 In addition, walking is a simple and accessible form of physical activity for people who are overweight and obese, and it is easy to control the intensity and frequency of exercise.17,89,98 Therefore, the use of step-monitoring devices for treating obesity is an ideal option, whereas the use of step-monitoring devices for preventing obesity requires further verification.
The subgroup analyses indicated that participants with a mean age >12 years presented greater intervention effects on BMI and BMI-Z than participants with a mean age ≤12 years. Older adolescents should generally respond better to step monitoring and goal setting/achievement than younger children. Therefore, using step-monitoring devices to intervene in adolescent populations can achieve better effects than in children. We recommend parental participation in the program for younger children, which may yield desirable effects.
The subgroup analyses indicated that the short-term (≤ 6 months) programs presented a greater intervention effect on BMI-Z than the long-term (>6 months) programs. This was inconsistent with the results of another meta-analysis. 43 A study by Richardson et al. concluded that long-term programs resulted in more weight loss than short-term programs. A possible reason for these contrasting findings was that the participants in this meta-analysis were children and adolescents who were more likely to lose interest and have poorer compliance. Their interest in the step-monitoring devices faded with interventions lasting longer than 6 months, thereby leading to a gradual diminution in the effectiveness of the intervention.45,92,99–101 In addition, four of the included studies performed additional follow-up measurements after the intervention.35,52,54,55 None of the intervention groups in these four studies showed significant reductions in BMI-Z and body fat at long-term follow-up compared to the control group. These results suggest that the effectiveness of step-monitoring device-based interventions to prevent and treat obesity in children and adolescents may not be sustained over time. We also must be cautious about the results of these subgroup analyses because the length that an intervention is more effective is also influenced by other factors (e.g. intervention intensity, frequency, setting, and whether or not the intervention design keeps the children and adolescents interested throughout).45,94,102,103 In addition, the subgroup analyses of BMI-Z and body fat did not further confirm this finding. Therefore, future studies are needed to further explore how to set the duration of interventions to achieve better effects.
Our subgroup analyses showed that the programs that established goals had greater intervention effects in reducing body fat than those that did not. This was consistent with another meta-analysis. 43 According to the Behavioral Intervention Technique Model, goal-setting is considered to be the most important behavioral change technique for promoting physical activity, especially in children and adolescents whose problem-solving and planning skills are limited.27,30,67,104 Goal-setting enhances self-efficacy and promotes perseverance, which can lead to better intervention effects.30,68,97 Surprisingly, the programs that did not establish goals had a greater intervention effect on BMI-Z than those that did. A possible reason for this was inappropriate goal setting. For example, setting goals that are too high may lead to low program adherence and high dropout rates, affecting intervention effectiveness.43,92 The present study explored whether different goal setting (e.g. adaptable versus fixed goals) impacted the intervention effects through subgroup analyses. The results suggested that the programs that established adaptable goals had greater intervention effects in reducing BMI (–0.60 kg/m2; P < 0.01) than those that established fixed goals. Therefore, we recommend that the use of step-monitoring devices for the prevention and treatment of obesity in children and adolescents needs to be based on self-monitoring and furthered by setting adaptable goals to achieve the desired results. Moreover, future studies should further explore how to set step goals to achieve better effects in the intervention of obesity in children and adolescents.
Strengths and limitations
There are some advantages to our systematic review and meta-analysis. First, to our knowledge, this systematic review and meta-analysis are the first to summarize the evidence regarding the effectiveness of utilizing step-monitoring devices to prevent and treat obesity in children and adolescents. Second, this study used subgroup analyses to identify whether the characteristics of the intervention population and features of the intervention program impacted the effect size. Third, the intervention tools chosen for this systematic review were step-monitoring devices whose data feedback (steps) was simple and easy to understand for children and adolescents, while these tools are also cost-effective and easy to implement on a large scale. Finally, all the studies included in this systematic review and meta-analysis were RCTs, meaning they provided high levels of evidence.
However, despite these advantages, there are some limitations within our systematic review. First, our systematic review and meta-analysis focused solely on using step-monitoring devices to promote physical activity to prevent and treat obesity in children and adolescents. We ignored the impact of other factors on the results (e.g. diet, sleep, and environment). Second, four of the included studies had a high risk of bias regarding incomplete outcome data due to more than 20% dropout rates. Third, the heterogeneity for the BMI, BMI-Z, waist circumference, and body weight indicator in our meta-analysis was significant, which meant that we must be cautious about the results. Finally, sensitivity analyses showed that the results of the BMI and body weight meta-analysis were not robust. Future step-monitoring device-based interventions should use multi-arm RCTs to assess how to set step goals and the interventions’ duration most effectively reduce obesity indicators. Moreover, we need to explore how to integrate the step-monitoring device into our daily lives perfectly, subconsciously enhance our awareness of self-regulation, and improve our quality of life.
Conclusion
Our findings suggest that step-monitoring device-based interventions significantly reduce BMI-Z, body fat, and body weight in children and adolescents. However, there was no significant effect on BMI and waist circumference. Based on our results and on the cost-effectiveness of step-monitoring devices, step-monitoring devices may be an effective and generalizable intervention tool for the prevention and treatment of obesity in children and adolescents. The subgroup analyses indicate that participants who were overweight or obese were better suited to use step-monitoring devices to treat obesity. Moreover, short-term step-monitoring device-based interventions may be more effective in the prevention and treatment of obesity in children and adolescents. Furthermore, the use of step-monitoring devices for the prevention and treatment of obesity in children and adolescents needs to be based on self-monitoring and furthered by setting adaptable goals to achieve the desired results. In future studies, we need to further explore how to set step goals and the duration of interventions to achieve better intervention effects.
Footnotes
Acknowledgments
We would like to thank the College of Education, Zhejiang University for providing support and assistance for this study.
Contributorship
WW conceptualized and designed the study and wrote the original draft. HR and JC completed literature search and article screening. YS and WS completed data extraction and the risk of bias assessment. WW and CH completed data analysis. CH critically revised the manuscript. All authors have read and agreed to the final version of the manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a Project Supported by the Scientific Research Fund of Zhejiang Provincial Education Department (Y202250464), a project of scientific research cultivation at the provincial and ministerial level or above (FRF23PY004); a “Faculty Professional Development Program” for domestic visiting scholars in colleges and universities in 2023 (FX2023176); and The Ministry of Education 2022 General Project of Specific Research by Ideological and Political Theory Course Teachers (22JDSZK045).
Guarantor
WW.
Registration and protocol
The review protocol was registered with PROSPERO (CRD42024496990).