
Abstract
Background
Despite the eruption of digital care systems for older adults, their benefits and challenges in clinical practice are uncertain.
Objective
We aimed to explore physiotherapists’ perspectives on technology-based gait and balance assessment systems for older adults and provide exploration insights to inform potential design requirements and candidate metrics for future systems.
Methods
Qualitative research based on semi-structured interviews with 20 physiotherapists was conducted to examine physiotherapists’ expertise in gait and balance evaluations (e.g., clinical processes, tests, and metrics), constraints and obstacles during clinical practices, and perspectives on the essential attributes and functionalities of optimal technology-infused systems.
Results
Findings indicate the Berg Balance Scale and movements of the pelvis, hip, knee, and feet are crucial for assessment. In addressing the constraints of conventional clinical assessments, technology-driven platforms enable the ongoing surveillance of daily movements and the quantification of kinematic measures. Physiotherapists also emphasized the significance of technology-integrated systems, accentuating physiotherapy-led evaluations, safety protocols, and non-intrusiveness.
Conclusion
This study serves as an effort to bridge the gap between technological progressions and real-world implementations through the lens of physiotherapists.
Introduction
Falls are the second leading cause of injury-related deaths globally. Approximately 30% of older adults aged 65 or above experience falls, with every 5-year increase in age reported to increase fall risk by over 10%.1–3 Gait and balance disorders are common causes of falls among older adults. Guidelines on fall prevention recommend that physicians annually examine older adults for difficulties with gait and balance. 4 However, the routine assessment of gait and balance requires extensive healthcare resources. By 2024, there were approximately 1.65 million residents aged 65 years or older in Hong Kong, representing around 22% of the total population. Particularly, 95.2% of older adults reside in community dwellings, while only 4800 registered physiotherapists are available in Hong Kong. 5 Therefore, there is a crucial need for an intelligent gait and balance assessment system to alleviate the care burden on specialists and caregivers for older adults.
Gait and balance disorders are usually multifactorial and require a comprehensive assessment. Clinical gait analysis traditionally relies on visual observation and specialists’ predetermined measurements. The widely used assessments include the Berg Balance Scale (BBS), Timed Up and Go (TUG) test, Tinetti Performance Oriented Mobility Assessment, Balance Evaluation System Test (BESTest), and Functional Gait Assessment (FGA).6–8 However, these conventional approaches have limitations like subjective and inconsistent visual observation, time-consuming and expertise-required assessment procedures, and limited information collection. Thus, due to limited healthcare resources and a rapidly growing aging population, accurate, user-friendly, and affordable technological approaches are urgently needed.9–12
Advancements in information and sensor technologies have facilitated more accessible and practical approaches for gait and balance assessment.13–15 Sensors have emerged as convenient and cost-effective tools for collecting gait and balance data. 13 Based on these sensor technologies, an increasing number of studies have explored the potential of using sensor data collected during conventional clinical tests or daily living, including kinematic, kinetic, and spatiotemporal parameters, to predict fall risk or evaluate gait and balance performance.14–16 In these studies, machine learning methods were used subsequently to analyze parameters and identify abnormal patterns of gait and balance. Current gait and balance assessment methods face significant challenges, including a lack of standardized assessment parameters, data acquisition protocols, reference values, and limited collaboration between researchers and clinicians.17,18 While initiatives such as Biomatrices and the Canadian Gait Consortium aim to address these issues,17,19 there remains a critical gap in understanding physiotherapists’ practical experiences and perspectives, 20 particularly in assessments for older adults. Given their expertise, physiotherapists are uniquely positioned to provide insights that can enhance system design by balancing accuracy, usability, and interpretability. Understanding their perspectives on existing systems and their expectations for future technologies is essential to advancing gait and balance assessment approaches.
In this study, we aimed to investigate physiotherapists’ clinical experience and explore their perspectives on technology-based gait and balance assessment systems for motor health management in older adults. In detail, we captured physiotherapists’ in-depth practical knowledge of gait assessment, including clinical tests, body motion metrics, and risk factors, and translated their tacit expertise into concrete qualitative and quantitative indicators. As a key stakeholder of intelligent gait and balance assessment systems, physiotherapists’ current challenges and expectations were further identified to inform the design of ideal systems. By understanding their specific needs, we aimed to provide valuable insights into user-centered design strategies and the potential opportunities for digital healthcare solutions in the aging era.
Methods
Study design
We conducted one-on-one semi-structured online interviews with 20 physiotherapists using a snowball sampling technique. No relationship existed between the researcher and participants prior to the study commencement. All participants were recruited through media posts, and no participants dropped out. Participants were informed of the researcher's institutional affiliation, general research objectives, and the purpose of the study. However, no personal motivations or detailed hypotheses were disclosed to maintain a neutral stance and avoid influencing participants’ responses. To maintain uniformity, all interviews were conducted by the same researcher with extensive experience in qualitative data collection in the field of human–computer interaction (Q.M., female, PhD candidate). The researcher was trained to conduct semi-structured interviews to minimize bias. Efforts were made to maintain neutrality and avoid leading questions. In detail, before the online interviews, participants were briefed on the objectives and procedures. Following verbal consent and confirmation for audio recording, the researcher proceeded with the interviews using a predefined guide, as shown in the section below, in the physiotherapists’ workplace through the Zoom platform. On average, each interview spanned approximately 60 min. No formal field notes were made during or after the interviews. However, the interviews were audio-recorded and transcribed verbatim for analysis. Verbal consent was obtained from all participants prior to the online interviews. This procedure was approved by the Institutional Review Board (approval number: HSEARS20210125001) and was deemed appropriate due to the remote nature of the study. Confidentiality and anonymity of the data were assured.
The findings were analyzed using R (version 4.3.2) and content analysis methodologies. The content analysis began with verbatim transcripts of the semi-interviews, which were then re-read to ensure in-depth familiarity. We then used open-ended coding (Q.M. and L.Y.) to mark significant text and categorize them according to similarity and association. These categories were further organized into themes through continuous comparison and refinement. The process was iterative and data-driven, and themes could be summarized from participants’ accounts. For the open-ended queries and detailed discussions, a professional transcription service was employed to transcribe the content post-completion of all 20 interviews. To ensure accuracy and reliability, a research assistant cross-verified the transcribed material against the original audio recordings.
Demographics of the participants
Table 1 summarizes the demographic information of the 20 physiotherapists who completed the study. The mean age of the physiotherapists was 32.8 years (SD = 4.2 years), ranging from 28 to 41 years. Most of the participants were male (70%). All interviewed physiotherapists held undergraduate degrees or diplomas, with 65% completing postgraduate studies. Nineteen of the physiotherapists have received training in the field of rehabilitation science, while 15 were trained in the field of physical therapy. All the physiotherapists were licensed by the Hong Kong Physiotherapists Board (HKPB), with two of them also being licensed by the Health and Care Professions Council (HCPC) and one by the Australian Physiotherapy Council (APC). The participants’ mean work experience was 9.6 years (SD = 4.5 years), ranging from 6 to 19 years. The 20 physiotherapists worked in a variety of units, including elderly centers (70%), private clinics (20%), and public hospitals (10%).
Demographics of the participants (n = 20).

Interview guide
According to previous research on gait and balance analysis, 21 clinical practices, 20 and technology adoption in healthcare and gerontechnology fields, 22 we developed the semi-structured interview including three parts: (1) demographic and professional background, (2) current practices in gait and balance assessment, and (3) perceptions on technology-based assessment systems.
The first part included seven questions about physiotherapists’ demographic information and clinical background, including age, gender, educational level, education background, certification board, work experience, and workplace.
The second part consisted of four questions (clinical tests, risk factors, sensor-based metrics, and body motions) to explore physiotherapists’ clinical experience and process on older adults’ gait and balance assessments. The first question involved compiling the literature's most used standard gait and balance assessment tools. Physiotherapists were asked to indicate which tools they commonly used in their clinical practice. The assessment tools included the BBS, Tinetti, BESTest, FGA, Activities-specific Balance Confidence scale, TUG, Romberg, sit-to-stand (STS) test, and straight walk (SWalk) test. Physiotherapists were allowed to select multiple tools, followed by explaining the clinical significance of score differences in the selected tests. The second question asked physiotherapists to select the effects of four chronic diseases on gait and balance assessments in older adults. These included cardiovascular diseases, neurologic disorders, musculoskeletal disorders, and sensory abnormalities. A Likert scale with five levels (ranging from “1 = negligible” to “5 = severe”) was used to indicate the severity of the effects. The third question explored the importance of sensor-available information from the perspective of physiotherapists. Eight categories of existing sensor-available information were presented, including joint angle, muscle control, step information, the center of mass (COM), body amplitude, foot pressure, body coordination, and vital signs. Physiotherapists were asked to rank the importance of these eight types of information for the gait and balance assessment, with a scale of 1–8, where 8 represented the most useful and 1 represented the least useful. For the fourth question, we aimed to gather physiotherapists’ opinions on the reference value of body parts in the evaluation process. A total of 15 body joints and parts were included, comprising 11 commonly used joint points (counting symmetric points as one) and four body parts commonly used for sensor placement, namely, the upper arm, lower arm, thigh, and calf. Physiotherapists were asked to provide insight on whether these body parts were considered important indicators for evaluating gait and balance abilities in elderly patients. Additionally, they sought their perspectives on specific details or features that should be attended to when assessing these body parts.
The third part of the interview contained two open questions (“Can you describe any difficulties or obstacles you face when evaluating gait and balance in elderly patients” and “What features or functionalities would you expect from an automated assessment system to better support your clinical work with older adults?”). The first question explored physiotherapists’ limitations and challenges in their current practice. Physiotherapists were encouraged to provide insights into any obstacles or difficulties they faced while evaluating these abilities in elderly patients. The second question aimed to gather physiotherapists’ perspectives on an ideal automated assessment system that could assist them effectively in their daily assessment work. Physiotherapists were invited to share their thoughts and ideas on the features, functionalities, and benefits they would expect from such technology-enhanced assessment systems.
After developing the interview guide, we conducted a pilot test with one participant and two human–computer interaction experts. Based on their feedback and comments, we further adjusted the structure, clarity, and applicability of the interview questions to ensure their relevance, comprehensibility, and alignment with the research objectives. However, no further formal validation process was performed, as expert feedback during the pilot phase was deemed sufficient for refining the guide.
Results and discussion
Test selections
Figure 1 presents the most used clinical evaluation tests among the participants. Physiotherapists emphasized that assessing older adults’ gait and balance ability is a multifaceted process involving various factors, such as assessment methods, reference scores, individual circumstances, and therapist experience. As shown in Figure 1, all physiotherapists selected the BBS test due to its comprehensive assessment of balance, ease of administration, and proven sensitivity in identifying balance impairments. As the gold standard for balance assessment, 23 BBS rated balance on a scale of 0 to 56, where a change of 3 to 4 points was considered standard for improvement or deterioration. The STS test typically assesses changes in older adults’ mobility by comparing the number of repetitions. In the TUG test, a 5–10-seconds increase in completed time may indicate a decline in older adults’ mobility, while step count and turning phase should also be considered. In the Romberg and SWalk tests, performance during the test and gait were the primary considerations, rather than time or scores.
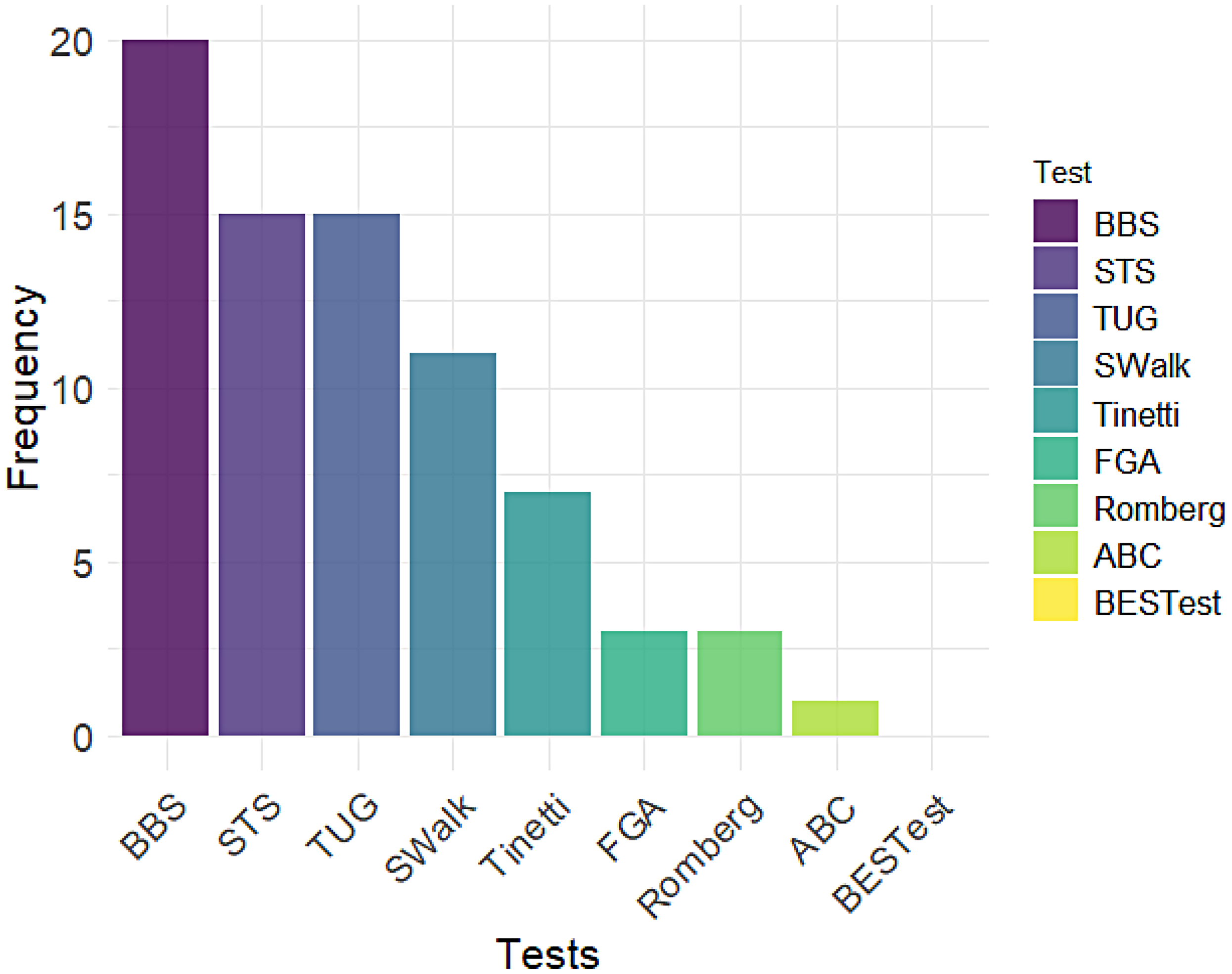
The most used clinical evaluation test by the 20 physiotherapists.
Despite the wide application of these clinical tests, they tend to require intensive physiotherapist resources and time in primary care. Thus, instruments providing objective and diverse indicators have been developed to assess gait and balance performance based on clinical tests. For example, wearable instruments equipped with sensors like an accelerometer on shoes have been shown to outperform shoe pressure sensors and hip-mounted accelerometers in predicting BBS accuracy. 24 Inertial sensors, widely used in mobility assessments such as STS, TUG, and SWalk,25,26 have demonstrated good validity (Pearson correlation coefficients: 0.68–0.99) and reliability (intraclass correlation coefficients: 0.85–0.94) in walking-related assessments. To optimize signal quality and analytical accuracy of inertial sensors, it has been recommended to place them on the lower back and shins. 26 Additionally, a previous study verified the predictive performance of the Wii balance board based on a single exercise of the BBS test. 27 We thus recommended that physiotherapists leverage the potential of sensor-based assessment tools combined with clinical tests to save time and reach a wider group in the community.
Impact of chronic diseases
We use a stacked bar chart (Figure 2) to present the various responses from physiotherapists regarding their views. In this figure, the lightest shade of red represents the category of “negligible,” while the darkest shade of red corresponds to the “severe” category. Neurological disorders, such as Parkinson's and dementia, appeared to have the greatest impact on gait assessment, with all 20 physiotherapists identifying them as either significant or severe. This result was consistent with previous studies, which found that neurological disorders cause abnormal acquisition, transmission, or perception of sensory signals, which is a main pathophysiological mechanism for gait and balance impairment.28–30 Since anticipatory postural adjustments differ in various neurological disorders, 30 wireless sensors, like inertial and surface electromyography sensors, can help identify and quantify the gait patterns or subclinical postural abnormalities for specific diseases. The assessment results from these technological instruments facilitate physiotherapists to develop individualized interventions. 31
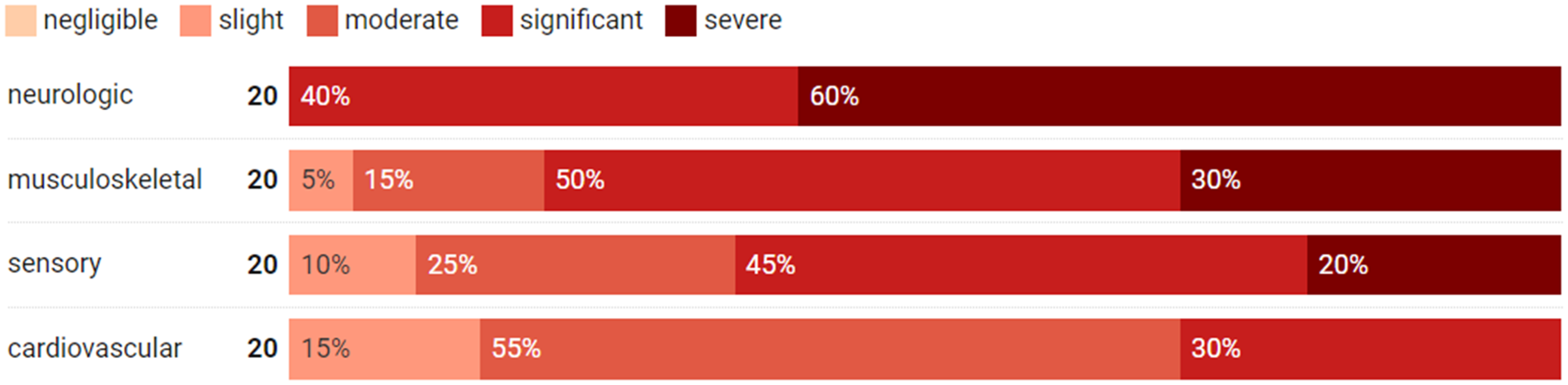
The impact of disease on gait assessment in older adults.
Most physiotherapists also recognized the substantial impact of musculoskeletal disorders and sensory abnormalities, with 10 and 9 physiotherapists, respectively, acknowledging the significance. This observation aligns with the understanding that impaired sensorimotor integration and the transmission of motor output are identified as two additional pathophysiological mechanisms contributing to balance impairments. 30 In particular, musculoskeletal disorders always cause pain, and their impact on gait depends on older adults’ pain levels. 32 Sensory abnormalities, such as cataracts, may considerably impact gait. However, it was notable that sometimes, older adults with such impairments can adapt to their vision and perform well in the assessment. The center of pressure (COP) and COM are typical metrics for balance assessment associated with these two types of disorders. 30 In detail, most researchers used inertial sensors to collect lumbosacral region motion as COM analyses. 30 To assess the effect of sensory and cognitive factors on balance, COP is commonly analyzed under amplitudes of the base of support, different from pressure sensors. 33 As individuals with different diseases present diverse gait and balance patterns, 30 we thus suggested physiotherapists use technologies to quantify mobility performance and create specific interventions.
Body features
Several contributing features have been proposed by researchers in past decades.1,34–37 This section aimed to understand what types of information physiotherapists would pay particular attention to in practical gait and balance assessments for older adults. The insights from physiotherapists would provide extremely significant support and consideration for dealing with gait and balance parameters using statistical or machine learning techniques. It is noted that this subsection only focuses on quantifiable details about older adults’ bodies for gait and balance.
Type of information
Differences in the sequencing of viewpoints can unveil how various physiotherapists may prioritize factors concerning human movement control. As illustrated in Figure 3, the significance of eight categories of information from the interviewed physiotherapists is depicted. Overall, muscle control, body coordination, and COM were identified as the most critical factors, whereas vital sign parameters were generally regarded to have a comparatively lower influence on gait performance.
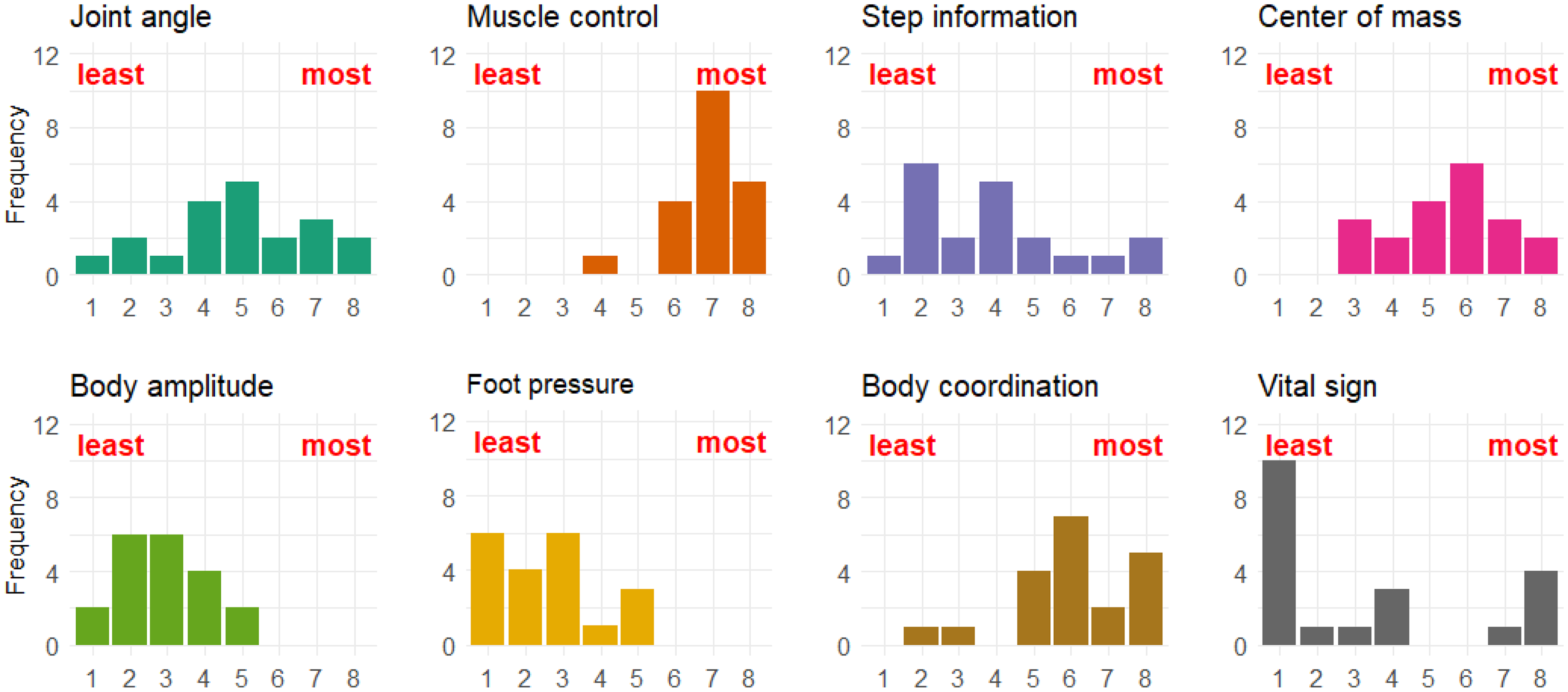
The level of information contributing to older adults’ gait and balance assessment.
With the development of wearable sensor-based gait and balance assessment, surface electromyography sensors typically assess muscle status by detecting and recording the electrical signals generated by the underlying skeletal muscles during motion.
38
This technology provides a noninvasive way to assess muscle activation patterns and fatigue, helping physiotherapists localize muscle injuries and identify physiological mechanisms of gait and balance disorders.
39
Moreover, inertial or pressure sensors commonly assess body coordination and COM in instrumented tests.38,40 A previous study suggested that 2-minute walking and 30-second standing tests with three inertial sensors (one at the pelvis and two on the feet) are reliable in assessing body coordination performance.
40
The inertial sensors placed at the sternum or lower back were considered the optimized combination of assessing COM.
38
Walking itself requires the use of different muscles. (…) body coordination, such as the coordination of hands and feet when walking, is necessary for maintaining balance. (PT8) Muscle strength and joint range are greatly related. If one lacks muscle strength, they move less, which makes the muscles tense and the joints stiffen, thus reducing the range. (PT10)
Body parts
Based on the illustration of body joints and parts shown in Figure 4, we solicited physiotherapists’ opinions on the reference value and features of these body parts for gait and balance assessment (see Figure 4). Based on the interviews, there were some variabilities in which body parts and joints were considered important for gait and balance assessment in older adults. The most recommended five body joints and points were the pelvis, hip, thigh, knee, and feet, consistent with previous studies.41–46 The detailed discussion with physiotherapists’ opinions on major body joints and parts are presented below.

Illustration of body joints and parts.
Upper body
- Shoulder and elbow: The motion of the shoulders and elbows plays a role in arm swing coordination during walking, influencing gait and balance. While the shoulders have less impact on gait and balance than the waist and pelvis, reduced arm swing, as detected by inertial sensors, was identified as the most sensitive and specific metric for detecting early-stage gait and balance impairments.
47
- Hand: If the person uses a walking aid, such as a cane or walker, the doctor will examine the hands and spine to ensure that the person can properly control the aid. Besides, previous studies verified a positive correlation between upper and lower extremity strength.48,49 As handgrip asymmetry is related to poor gait and balance performance, we thus suggested physiotherapists use force sensors to help assess older adults’ mobility.
Core body
- Waist and spine: The waist and spine are essential for examination for movement and limitations that could affect gait and balance. Its shape, stiffness, and flexibility can affect older adults’ ability to rotate their torso during walking. The waist affects spinal alignment and provides stability during walking. Any pain or conditions affecting the waist, such as nerve compression, can also affect gait and balance. The waist and spine speed and their turning jerk during postural transitions, such as STS, were significant objective biomarkers for identifying individuals with fall risk.
47
These instrument-based biomarkers from inertial sensors can help physiotherapists quantify the gait and balance performance and diagnose presymptomatic disease, tailoring individual treatments or prescriptions to prevent serious physical degeneration. - Pelvis: The pelvis is crucial for gait and balance assessment. It connects and stabilizes the lower limbs to the spine and supports the body's weight, affecting stability and support during walking. The movement of the pelvis during walking can affect older adults’ COM and increase the risk of falls. Thus, symmetry and balance of the pelvis are important for gait and balance. The stability and support the pelvis provides during walking contribute to maintaining balance and good posture. Anticipatory postural adjustments, typically assessed by the force plate under the feet, have been verified to be highly associated with the mediolateral amplitude of accelerometers on the pelvis.
47
The smaller amplitude of accelerometers indicated bradykinetic anticipatory postural adjustments and delayed onset of stepping. The subtle posture changes detected by sensors aid in diagnosing and treating diseases like Parkinson's and Stroke.They often have problems with their lumbar spine, leading to the pelvis walking at an incorrect angle. (PT4)
If the muscles surrounding the pelvis are well-controlled, their overall centre of gravity, balance, and gait will naturally improve. (PT10)
- Hip: The vitality and state of the abdominal muscles play a pivotal role in maintaining balance. These muscles are integral to the core muscle group. Proper control of the muscles surrounding the pelvis, including those in the buttocks and abdomen, is essential for sustaining balance and correct posture. Furthermore, the strength and flexibility of the hip joint, encompassing factors like range of motion, hold significant importance. Any disruptions in the COM can lead to forward-leaning or tilting to one side. Older adults grappling with balance issues often resort to hip movements as a compensatory strategy to offset postural imbalances. 50 Based on assessments using inertial sensors, individuals with balance disorders exhibited significantly greater motion angles in both the medial–lateral and anterior–posterior directions.A wider hip joint or feet clamped together will affect their base support stability. (PT6)
I would generally look at the overall range of the hip joint, including internal and external rotation, and an aspect that few people pay attention to is the range of extension. (PT5)
Lower body
- Thigh: The size, strength, and height of the thigh muscles play a significant role in bolstering the overall strength and stability of the lower body, which is crucial for sustaining balance. The thigh muscles provide essential support during ambulation when collaborating with other lower body muscles like those in the hips, knees, and lower legs. Assessing the thighs for any signs of muscular weakness or diminished strength that might impede mobility is imperative. In evaluations of lower body strength, such as the STS test, the mobility and strength of the thighs serve as pivotal indicators of functional capacity.
51
Notably, acceleration signals with more high-frequency content (higher spectral edge frequency) and greater variability, especially in the anterior–posterior and medial–lateral directions, have been verified to have high association with poor balance control and increased fall risk.
51
As muscle strength is difficult to measure in daily scenarios, motion sensors combined with clinical tests, such as using inertial sensors during the 5STS test, provide physiotherapists with quantitative metrics to infer thigh strength. While manual muscle testing remains a valuable clinical method, sensor-based assessments offer objective, repeatable measurements that can enhance traditional evaluations.If the thigh is lifted too high or too low, it can affect the gait, possibly due to insufficient strength. (PT13) - Knees: The condition, ability to bend and straighten, twisting, or instability of the knee joint during walking affects gait and balance. Assessing the knee joint for excessive bending or deformities while standing or walking is important. The condition of the knees, including any degeneration or inflammation, can affect gait and balance. Physiotherapists commonly examine the degree of flexion or extension of the knee joint and check for deformities or signs of muscle atrophy. However, conventional joint protractors can only measure the static angles of the knees. It is difficult for physiotherapists to quantify knee rotation during walking. Advanced techniques, such as strain gauges and inertial or optical sensors, have been developed to measure the dynamic and kinematic motion of the knees.
52
These devices can help physiotherapists monitor knee flexion during daily activities, predicting fall risk to assist in intervention.The knee joint should be examined for swelling, as inflammation is common in older adults. If normal, check the range because this can affect the hip area and posture, such as whether it can be straightened. How well the knees can bend and straighten affects balance and gait. (PT7) - Lower legs: Any signs of muscle atrophy or swelling in the lower legs can affect the ability to generate force when stepping, affecting gait and balance. The tension or tightness of the muscles in the lower legs, including the calves and shins, must be symmetrical and in good condition to maintain balance and stability during walking. The lower leg muscles, ankle joint, and feet are always considered whole for gait and balance assessment. Compared with other positions, such as the thigh and feet, time-domain features extracted from inertial signals of the lower legs achieved the best accuracy in identifying the walking patterns of participants with neurological disorders.
53
The angular velocity of the lower legs during walking also significantly contributed to recognizing fallers from non-fallers.
26
- Ankles and feet: The mobility and stability of the ankle joint and the condition of the feet play a vital role in maintaining support and mobility during walking, which is necessary for maintaining balance. Any issues with the ankle joint, such as inflammation, degeneration, inward rolling, or flattening of the foot arches, increase the risk of falls. The base of support provided by the feet is important for balance, too, and any deformities or issues with the feet can affect gait and balance. As early gait changes of neurodegenerative disorders are subtle and challenging to diagnose, sensor-based instruments can help clinicians identify gait events and quantify gait metrics, such as motion angles and foot clearance.40,54 Particularly, individuals with ataxia present smaller ankle angles and slower angular velocity during natural home-based activities.
40
The decreased foot clearance also indicates shuffling among individuals with Parkinson's disease.
54
Pressure platforms can also aid in identifying balance impairments such as uneven weight distribution, which is prevalent in conditions like Parkinson's disease and ataxia. Check for conditions like pronation, which could be due to flat feet or previous habits of twisting injuries. This could lead to some pronation when walking. If there is pronation while walking, naturally it can cause twisting in the knee joint. (PT15)
In summary, a comprehensive evaluation was crucial for older adults to evaluate their gait and balance performance. Sensor-based instruments enable physiotherapists to quantify the complex and dynamic gait and balance during daily activities. In detail, COP and COM are essential metrics for gait and balance assessment.
30
Inertial sensors placed at the pelvis and pressure sensors placed at the feet effectively measure these parameters.38,40 Besides, upper body motion measured by inertial or optical sensors provides assessment metrics for static postural sway,
47
and handgrip strength is significantly associated with lower limb strength.48,49 Meanwhile, the core body motion combined with clinical tests like the STS and BBS achieves great performance in measuring individuals’ postural transitions and balance ability.
47
The lower body motion metrics are related to the gait and posture coordination during dynamic activities.
40
By combining metrics from different body parts, physiotherapists can better understand a patient's gait and balance ability, enabling earlier detection of neurodegenerative disorders and more targeted therapeutic interventions.
Challenges and perspectives
Challenges
We summarize the challenges mentioned in the conversation into non-technical and technical challenges, as shown in Table 2.
- Environmental constraints: Physiotherapists reported that Hong Kong's dense living environments limit traditional gait and balance assessments. For example, a PT may need to assess an elderly person's gait by a 10-m straight walk, but if there is no space available in the testing environment, the assessment may not accurately reflect the elderly person's ability. - Safety concerns: Physiotherapists are concerned about the risk of falls when evaluating the elderly, particularly when no assistant is present. For example, if patients are asked to stand on one leg and lose balance, they may fall and injure themselves. This risk can be mitigated by having an assistant present to provide support and prevent falls. - Patient cooperation: Some elderly patients may have difficulty cooperating with the assessment process due to cognitive, hearing, or comprehension issues. For example, a patient with dementia may struggle to understand instructions or remember the task they are supposed to perform. Additionally, some elderly patients may not see the value of being assessed and may not want to participate. Physiotherapists may need to adapt their approach to suit the patient's needs, such as providing simpler instructions or using visual aids to help patients understand what to do. - Assessment method selection: When elderly patients have multiple health issues or comorbidities, it can be challenging to select an appropriate assessment method for their specific needs. Furthermore, a single test's minimal clinically important difference varies across diseases, complicating the selection of a universal tool.
55
- Lack of standardization: Physiotherapists showed that the current clinical tests cannot accurately reflect an individual's functional abilities. For example, the BBS test has 14 items, but some elderly may not be able to complete all of them, leading to inaccurate scores. PTs suggest breaking down each testing item into its individual components to more accurately assess an elderly person's gait and balance performance in practice.
Challenges identified by the physiotherapists in daily gait and balance assessment.

Perspectives
In this section, we present the insights shared by physiotherapists regarding developing and implementing future automatic gait and balance assessment systems, focusing on enhancing assessment and support for elderly gait and balance.
- Physiotherapist-led assessment: Physiotherapists showed that technology-based gait and balance systems should act as assistive tools to simplify and optimize their work rather than replace their expertise. If automated diagnostic results are inaccurate, additional burden and emotional strain will be generated for patients.
56
According to a previous study, technology-based systems should align with a human-centered design approach, offering preliminary assessments and data-sharing capabilities that ease the clinical workflow without removing the clinician's role in decision-making.
56
- Safety and independent assessment: Physiotherapists emphasize the importance of ensuring the safety of elderly individuals during assessments and tasks. They highlight the need for a system that allows older adults to complete assessments safely, even without a therapist. Thus, systems should only include tasks that can be performed without risk, integrating features that alert both the elderly and physiotherapists to potential risks.
26
- Convenience and support for physiotherapists: An accurate and convenient system that saves them time is needed. The system should streamline the process, provide data on potential issues, and reduce physiotherapists’ workload.
56
Guiding principles include ease of use, intuitive data outputs, practical usability, and consideration of older adults’ conditions. The ideal system could be a machine, tablet, or small device with a screen that facilitates information sharing, demonstration videos, and communication with physiotherapists.Some balance detectors on the market can provide some body data, but they are inconvenient. I have to set them up and turn them on. These technologies exist, but they are time-consuming. (…), Often, the workload increases when using them, which seems a bit backward to me. (PT17)
I would need to make one or two additional on-site assessments, then I could immediately provide a treatment. (PT18)
The best scenario is that after a patient completes a walking test, the system would provide some data indicating any problems. These issues could be a smaller range of motion than normal, uneven contact surfaces of the feet, or particularly weak muscle control in some areas. After (…), I can manually check whether these problems exist. If they do, I can determine what caused these issues and proceed with treatment. If it could reach this level, it would be excellent and save me a lot of time. (PT5)
- Information sharing and communication: Physiotherapists appreciate features that can automate routine tasks, track patient progress, and provide intuitive data visualizations, as these tools enhance clinical decision-making. 56 It is also suggested that the system be seamlessly integrated with existing healthcare workflows, enabling physiotherapists to focus more on patient care while maintaining efficient data management. 56
- Encouraging elderly involvement: Engaging older adults in their mobility care is crucial for the success of the assessment system. Notably, features like personalized exercise plans, progress tracking, and incentives can considerably boost older adults’ motivation and commitment to prescribed treatments. 57 Moreover, the system should consider the unique challenges older adults face, such as psychosocial and compliance difficulties, especially during the pandemic. These systems can improve patient engagement and adherence to assessments and interventions by fostering a collaborative and supportive environment.
Practical considerations for sensor-based technologies
Building on the challenges and opportunities identified by physiotherapists, sensor-based technologies present potential solutions for enhancing gait and balance assessments by incorporating risk-free tasks and real-time monitoring during daily activities. However, their adoption faces practical constraints such as cost, accessibility, and operational complexity. These systems are particularly valuable for including risk-free tasks and real-time monitoring during daily activities, but physiotherapists often face financial barriers that make them inaccessible for smaller clinics or resource-limited settings. Realistic alternatives, such as outsourcing assessments to specialized providers or leveraging affordable tools like smartphone-based applications, could help address these issues. Furthermore, adopting advanced sensor-based technologies may vary based on practical constraints and institutional priorities. For routine practice, these tools could serve as complementary options rather than standard requirements, highlighting their potential to enhance assessments when resources and expertise allow. To maximize usability, system designs should follow a human-centered approach, prioritizing physiotherapist-led assessments, safety, unobtrusiveness, and ease of use. Simplifying system operations with automated data processing and intuitive outputs can further reduce physiotherapists’ workload. Additionally, the lack of standardized protocols for digital biomarkers limits clinical applicability, highlighting the need for future research to develop validated metrics and workflows tailored to older adults. Finally, incorporating participatory design to engage older adults as key stakeholders actively can enhance system relevance, with personalized features like exercise plans and progress tracking, ensuring clinical relevance and patient adherence.
Limitation
While this study offers valuable insights into physiotherapists’ perspectives on technology-enhanced gait and balance assessment systems for older adults, certain limitations should be noted. First, the study involved 20 physiotherapists. Although data saturation was achieved, it prioritizes localized insights and may limit direct transferability to other healthcare systems (e.g. rural settings or countries with different aging care models). Future studies with larger samples could provide additional perspectives. Besides, the interview guide was developed based on expert input and literature but was not formally validated. This limitation should be considered when interpreting the findings. Last but not least, as the study was conducted in Hong Kong, the findings are most relevant to urban healthcare settings. Further research in diverse cultural and healthcare contexts would help enhance the generalizability of these results.
Conclusion
Our study has illuminated the current practices, challenges, and future development trends in automated gait and balance assessment systems from the perspectives of 20 physiotherapists. Data saturation was monitored throughout the interview and analysis process. After the 15th interview, no new themes or patterns emerged, confirming that data saturation had been achieved. This study could make significant contributions to various stakeholders. The insightful experiences of physiotherapists and their highlighted challenges could be a compelling catalyst for future research in related fields. For example, for engineers and data scientists, by quantifying the physiotherapists’ assessment experience, we have provided information on contributing factors, including both existing ones and previously overlooked ones, such as the flexion of the thigh and the range of its extension. Future research can incorporate these features to enhance the accuracy of gait and balance assessment algorithms. Additionally, future research can explore which sensors are more suitable for accurately capturing the observed points that physiotherapists examine during testing. For system designers, understanding the pain points of physiotherapists regarding current assessment methods and identifying the information that can assist them and other clinical professionals in their work will greatly benefit future developments. For caregivers and elderly individuals, we can enhance their awareness and acceptance of gait and balance assessment by involving them in co-designing the next generation of testing systems.
Our pioneering work could lay the foundation for the ongoing evolution of automated gait and balance assessment systems. Besides, for the future development of such a system, it is not enough for physiotherapists, older adults, caregivers, engineers, data scientists, or designers to work solely within their respective fields of expertise. We advocate for the active participation of all stakeholders to address specific challenges related to technological advancements and applicability concerns, ensuring that the system is comprehensive and tailored to specific healthcare settings.
Footnotes
Acknowledgements
The authors are grateful to all the participants in the interview.
Ethical approval
This research received approval from the Institutional Review Board (No. HSEARS20210125001).
Contributorship
L.Y: writing—original draft, writing—review and editing, conceptualization, data collection, quantitative analysis, qualitative analysis. Y.Z: writing—original draft, writing—review and editing, quantitative analysis, qualitative analysis, funding acquisition. Q.M: data collection, quantitative analysis. K.L.T: writing—review and editing, resource. M.Y.C.P: writing—review and editing, resource. H.G: writing—review and editing. H.W: writing—original draft, writing—review and editing, supervision, conceptualization, funding acquisition.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Shenzhen-Hong Kong-Macao Science and Technology Program Fund, Natural Science Foundation of Guangdong Province, Hong Kong Polytechnic University Grants (grant numbers SGDX20210823103403028, 2021A1515010987, P0042959, P0049627, P0045577).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Consent for publications
All authors are aware of and agree to publish.
Data availability
The datasets generated and/or analyzed during this study are available from the corresponding author upon reasonable request.