
Abstract
Background
With rising concerns over physical inactivity in children and adolescents, gamified digital exercise interventions have emerged as promising strategies to enhance engagement and adherence to physical activity (PA). However, their overall effectiveness and the key behavior change techniques (BCTs) that drive success remain unclear.
Methods
This systematic review will assess the effects of gamified and digital exercise interventions on PA and health outcomes in children and adolescents aged 6–18 years. We will include randomized controlled trials and non-randomized studies of interventions focusing on interventions using digital technologies such as exergames, mobile applications, virtual reality, augmented reality, and wearables, with at least one gamification element. A comprehensive search will be conducted in PubMed, Web of Science, Scopus, Embase, CINAHL, PsycINFO, Cochrane Library, IEEE Xplore, CNKI, and Wanfang Data, covering studies from January 2014 to August 2025. BCTs will be categorized using the BCT Taxonomy v1 (BCTTv1), and data will be synthesized through meta-analysis or narrative synthesis depending on study homogeneity. The Promise Ratio will be used to identify the most effective BCTs.
Conclusion
This review will provide valuable insights into the effectiveness of gamified and digital exercise interventions, helping to identify key BCTs that contribute to successful outcomes. The findings will guide the design and optimization of future exercise interventions among children and adolescents, with the goal of improving their overall health and well-being.
Prospero registration number
CRD420250651337.
Keywords
Introduction
Children and adolescents represent approximately one-quarter of the global population, and their health and well-being are vital to both current and future societal development. 1 Promoting physical activity (PA) in this population not only yields direct health benefits but also contributes to the achievement of the United Nations 2030 Sustainable Development Goals (SDGs), particularly SDG 3 (Good Health and Well-being), SDG 4 (Quality Education), and SDG 5 (Gender Equality). 1 According to the World Health Organization (WHO), children and adolescents aged 5 to 17 years should engage in at least 60 min of moderate-to-vigorous physical activity (MVPA) daily. 2 However, findings from a pooled analysis of 298 population-based surveys involving 1.6 million students aged 11–17 years across 146 countries and regions reveal that over 80% of adolescents do not meet these recommendations. 3 Insufficient PA during childhood and adolescence is associated with an increased risk of chronic conditions later in life, including obesity,4,5 cardiovascular diseases,5,6 and type 2 diabetes. 5 Moreover, low PA levels have been linked to mental health concerns such as anxiety and depression, 7 reduced social competence, 8 impaired cognitive development,7,9 and lower overall quality of life. 10
There is growing evidence that planned, systematic exercise training has demonstrated significant multidimensional benefits in improving the physical and mental health of children and adolescents.11–13 Adherence to regular exercise improves cardiorespiratory endurance,14,15 bone development, 16 motor coordination, and flexibility. 17 Moreover, structured exercise interventions have demonstrated positive effects on reducing body mass index (BMI) and improving body composition, while also playing a crucial role in preventing and mitigating risk factors associated with metabolic and cardiovascular diseases. 15 On a psychological and behavioral level, regular participation in exercise has been found to be associated with better mental health outcomes, 18 enhanced mood,8,19 and improved social interaction experiences.8,20 In addition, through sustained participation in structured exercise activities, children and adolescents are more likely to develop lifelong healthy exercise habits that result in long-term health benefits.21,22 Therefore, the development and promotion of effective exercise intervention strategies for this population has become a key measure for preventing multiple chronic diseases and improving overall health.
With the development of digital technology, numerous exercise interventions featuring gamification and digitalization have emerged, showing considerable promise in enhancing the interest, participation, and long-term adherence to exercise among children and adolescents.23,24 Gamification elements such as points, badges, competition, social interaction, and virtual story plots can effectively increase intrinsic motivation and long-term adherence to exercise behaviors in children and adolescents. 23 At the same time, digital exercise intervention modes represented by exergames, sports applications (apps), virtual reality (VR) and augmented reality (AR), and wearable devices can break the time and space constraints of traditional sports through the advantages of technological interactions and provide more convenient, personalized, and interesting sports participation experiences. 24
In this proposed systematic review, the term “gamified digital exercise interventions” refers to technology-delivered programs that use exercise or physical activity as the primary mode of intervention and incorporate gamification element. This definition distinguishes such interventions from broader digital health programs that may rely on education, counselling, or self-monitoring alone without involving physical movement.
However, despite the large number of relevant intervention studies that have emerged in recent years, there are currently no consistent conclusions about the overall effectiveness of gamified digital exercise interventions in child and adolescent populations.25–27 This inconsistency is not only reflected in the heterogeneity of study designs, technological platforms, and delivery quality, but also in the varying health outcomes targeted.28,29 For instance, active video game (AVG) interventions have shown significant improvements in BMI and body fat percentage among overweight or obese youth but yielded mixed or limited effects on muscle fitness, motor competence, and cardiorespiratory capacity. 30 Similarly, mobile health (mHealth) app-based interventions have demonstrated positive effects on reducing sedentary behavior and increasing general PA, yet their influence on MVPA, aerobic capacity, or musculoskeletal fitness remains inconclusive or minimal. 31 Moreover, studies on serious games targeting children with chronic diseases have found limited improvements in PA levels, despite some favorable changes in BMI, and highlighted issues such as low engagement, lack of personalization, and insufficient use of behavioral theories to support behavior change. 32 Therefore, simply embedding technology or gamification elements into an intervention is not sufficient to ensure that meaningful health improvements are achieved. A deeper understanding of the specific mechanisms behind effective interventions remains a critical but not yet fully addressed issue.
Behavior change techniques (BCTs) are those well-defined, replicable intervention components designed to change behavioral determinants such as goal setting, performance feedback, reward attainment, and promotion of social support. 33 By systematically classifying and evaluating BCTs through standardized frameworks such as the Behaviour Change Technique Taxonomy v1 (BCTTv1), researchers and practitioners are able to identify the most impactful intervention components. 34 However, despite their potential, systematic BCT analyses are still relatively rare in current exercise intervention studies focused on child and adolescent populations, leading to ambiguity regarding which specific intervention components are most effectively implemented.
Therefore, the aim of this systematic review is to (1) comprehensively summarize the evidence of the effects of gamified digital exercise interventions on multidimensional health outcomes, including physical performance, health-related indicators, and psychosocial behaviors, in children and adolescents; (2) systematically classify and extract BCTs in interventions based on the BCTTv1; and (3) apply the Promise Ratio to identify the most promising key BCTs. Through this review, we expect to provide a more targeted and evidence-supported behavioral design reference for the development of digital sports interventions for future youth populations.
Methods
Study design registration
This protocol has been developed following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses Protocols (PRISMA-P) 2015 statement 35 (seen as Supplemental file 1). The protocol has been prospectively registered in the International Prospective Register of Systematic Reviews (PROSPERO) under the registration number CRD420250651337.
Eligibility criteria
The eligibility criteria will be determined based on the principles of the Population, Intervention, Comparison, Outcome, and Study design (PICOS) framework, as shown in Table 1.
Selection criteria of studies in PICOS format.

Population (P). Studies must involve children and adolescents aged 6–18 years, regardless of gender, ethnicity, or baseline PA levels. We will include studies enrolling healthy participants or those with stable, non-disabling conditions (e.g. overweight, well-controlled asthma) who can participate in general PA programs. Studies targeting populations for whom exercise serves primarily a therapeutic or rehabilitative function will be excluded. This includes children with conditions such as autism spectrum disorder, cerebral palsy, severe psychiatric disorders, or active cancer, where interventions are typically individualized and clinically oriented.
Intervention (I). Eligible interventions should involve structured exercise activities delivered through digital technologies, such as AVGs, mobile apps, VR, AR, and wearable devices. The intervention must include at least one gamification element (e.g. points, badges). Non-digital interventions or those without gamification elements, as well as purely informational, non-interactive interventions, will be excluded.
Comparison (C). Eligible studies must include a control group to enable comparative analysis of intervention effects. Acceptable control conditions include the following: (1) passive controls such as no intervention, usual care, or waitlist groups that do not receive any structured exercise program; (2) active controls involving conventional exercise programs or educational interventions that promote PA but lack interactive digital or gamified components; and (3) minimal-intervention controls where participants receive only informational materials or self-monitoring tools without gamification or interactivity. Studies will be excluded if they lack a clear control group, compare only multiple gamified interventions without a distinct comparator, or focus solely on qualitative outcomes without assessing intervention effectiveness.
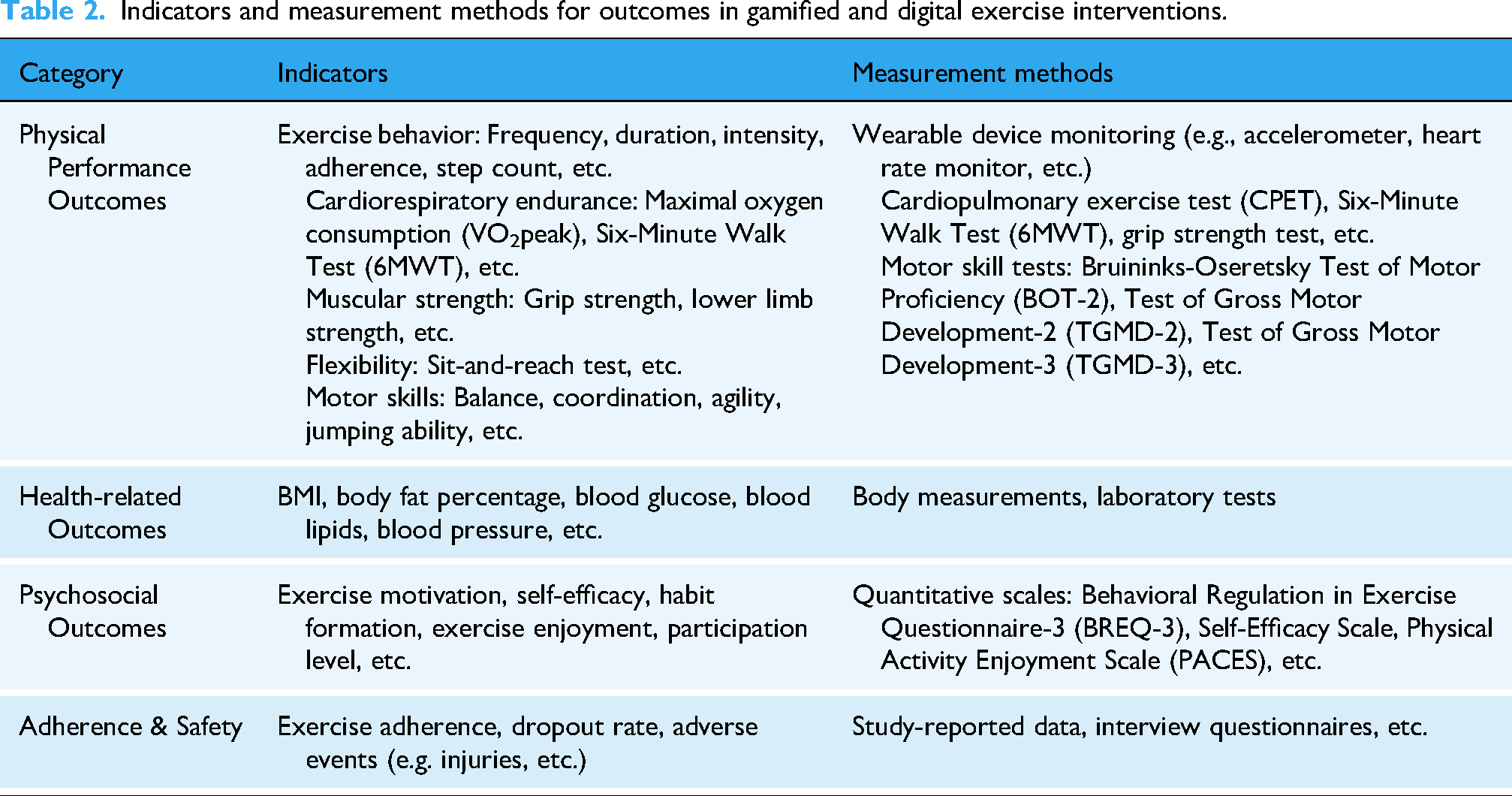
Outcome (O). Studies must report at least one quantitative outcome, such as physical performance, health-related indicators, psychological and behavioral measures, or intervention adherence. Studies relying solely on qualitative assessments or lacking measurable intervention effects will be excluded. Possible outcome categories, indicators, and measurement methods are shown in Table 2.
Indicators and measurement methods for outcomes in gamified and digital exercise interventions.
Study design (S). This systematic review will include randomized controlled trials (RCTs) and non-randomized studies of interventions (NRSIs), including quasi-experimental designs such as controlled clinical trials (CCTs), controlled before-after studies, and interrupted time series (ITS). To be eligible for inclusion in the meta-analysis, studies must include a concurrent control group (e.g. no intervention, waitlist, or usual care). Single-group pre-post studies without a control group will be included in the review for narrative synthesis only. Observational studies, cross-sectional studies, case-control studies, and qualitative studies will be excluded.
Language and publication date restrictions are set to include only studies in English and Chinese to manage translation challenges and ensure a broad international scope. Studies published since 2014 will be included to reflect the most recent advancements in digital and gamified exercise interventions.
Data sources and search strategy
The search strategy will be developed in collaboration with an experienced research librarian and adapted for multiple databases to maximize sensitivity and specificity. The review will include studies published between January 2014 and August 2025.
Electronic data
The search will be conducted in the following databases: PubMed, Web of Science, Scopus, Embase, CINAHL, PsycINFO (ProQuest), Cochrane Library, IEEE Xplore, China National Knowledge Infrastructure (CNKI), and Wanfang Data. These databases have been selected to comprehensively cover medical, psychological, behavioral, and technological aspects of gamification-based and digital exercise interventions. The inclusion of Chinese databases allows for a more complete representation of studies conducted in the Chinese academic community. A detailed PubMed search strategy is provided in the Supplemental File 2.
Search for other resources
To supplement the electronic database search, additional resources will be explored to ensure completeness. The reference lists of included studies and relevant systematic reviews will be manually screened for additional eligible studies. To ensure the inclusion of comprehensive intervention details, we will also search for study protocols and additional publications describing intervention components related to the included RCTs. This will help obtain more detailed information on the BCTs embedded within the interventions. If available, such supplementary publications will be included to enhance the accuracy of intervention characterization and BCT coding. Gray literature such as dissertations, theses, conference abstracts, and technical reports will be excluded. Given the methodological demands of risk-of-bias appraisal, accurate BCT extraction, and outcome synthesis, these sources often lack peer review and typically do not provide sufficient methodological detail for reliable quality assessment and data coding.
Data screening and extraction
Data management and screening
All retrieved records will be imported into EndNote X9.3 for reference management and deduplication. After removing duplicates, the remaining records will be transferred to Rayyan 36 for title and abstract screening. Two independent reviewers will screen the studies based on predefined eligibility criteria, and any disagreements will be resolved through discussion or consultation with a third reviewer if necessary. Full-text articles of potentially eligible studies will be assessed for final inclusion. The study selection process will be documented using a PRISMA 2020 flow diagram, 37 detailing the number of records screened, excluded, and included, along with reasons for exclusion. The research flowchart is presented in Figure 1.
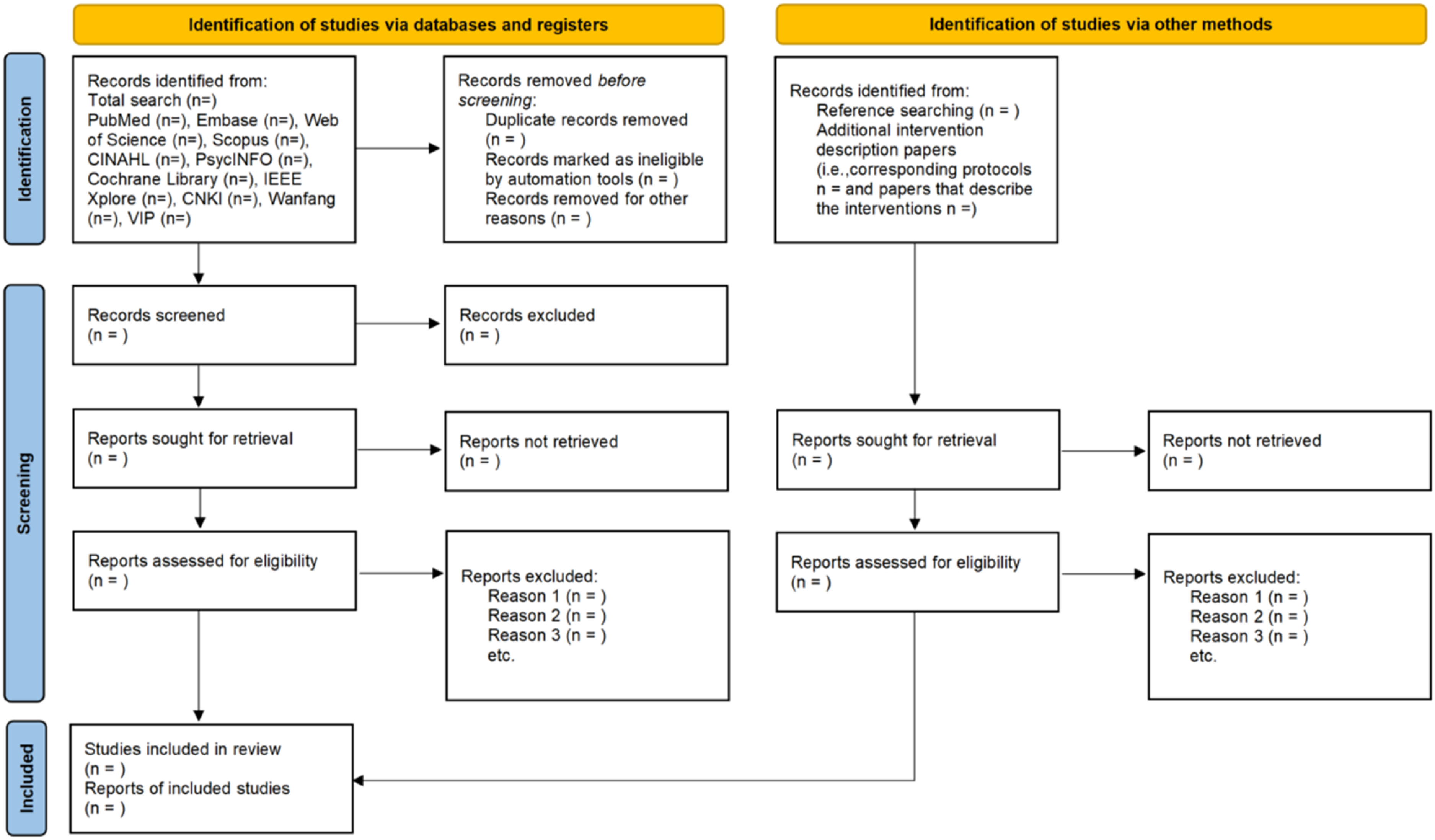
PRISMA flow diagram of article search and selection for the systematic review.
Data extraction
Two independent reviewers will extract data using a standardized extraction form. Extracted information will include the first author's name, publication year, country, study design, participant characteristics, sample size, intervention and control group details, follow-up duration, outcome measures, and key findings. Discrepancies in data extraction will be resolved through discussion, with a third reviewer consulted if necessary. The final extracted dataset will be securely stored for analysis.
Missing data
For studies with missing data, we will contact the corresponding authors to request the required information. If no response is received within 2 weeks, a follow-up email will be sent. If there is still no response after a total of 4 weeks, or if the authors decline to provide the requested data, the study will be excluded from the analysis. All instances of missing data and author contact outcomes will be documented and reported in the review.
BCT coding
The BCTs used in the included interventions will be identified and coded using the BCTTv1. Two independent reviewers, who have completed BCT coding training (http://www.bct-taxonomy.com/), will conduct the coding process. Only explicitly reported BCTs will be coded to ensure reliability, and BCTs will be analyzed separately for intervention and control groups to distinguish techniques unique to the intervention. 38
For studies with multiple intervention groups, BCTs will be extracted for each intervention arm separately. In studies comparing two active interventions, the primary intervention will be defined based on the study objectives, with the other serving as a comparator. 39 To ensure coding consistency, an initial double coding will be conducted on 10% of the included studies, and if inter-rater agreement reaches ≥90%, full coding will proceed. 40 Discrepancies will be resolved through discussion or consultation with a third reviewer if needed. All identified BCTs will be recorded in a structured data extraction table and analyzed to assess their frequency. Interventions with poorly reported or unclear BCTs will not be excluded; however, their limited reporting will be documented and considered a limitation during analysis and interpretation. Pre-defined form for coded BCTs in included studies as shown in Supplemental file 3.
Methodological quality assessment
The risk of bias for each included RCT will be assessed using the Cochrane Risk of Bias 2.0 (RoB 2.0) tool. 41 This tool evaluates the risk of bias across several domains, including random sequence generation, allocation concealment, blinding, outcome measurement, selective reporting, and data completeness. For NRSIs, the Risk of Bias In Non-Randomized Studies- of Interventions (ROBINS-I) tool will be used. 42 Two independent reviewers will conduct the assessments, categorizing each study as having a low, moderate, or high risk of bias. Any disagreements will be resolved through discussion or by consulting a third reviewer.
Grading the quality of evidence
The certainty of evidence for each outcome will be evaluated using the Grading of Recommendations Assessment, Development and Evaluation (GRADE) tool. 43 The assessment will consider five domains: risk of bias, inconsistency, indirectness, imprecision, and publication bias. Based on these factors, the quality of evidence will be rated as high, moderate, low, or very low. Two independent reviewers will conduct the GRADE assessments, with any discrepancies resolved through discussion or consultation with a third reviewer.
Data synthesis and analysis
Meta-analysis
Meta-analyses will be conducted only when comparable outcome data are available from at least three studies. 44 If fewer than three eligible RCTs are available for a given outcome, NRSIs assessed as having low or moderate risk of bias will be considered for inclusion. Effect sizes for each outcome will be extracted from the end-of-intervention time point, which will be prioritized in cases where multiple assessment time points are reported. When multiple measurement instruments are used for the same outcome, objective or observer-rated measures will be preferred over self-reported ones. If more than one validated scale of the same type is reported, the scale most commonly used across the included studies will be selected to minimize heterogeneity.
Heterogeneity will be assessed using the I² statistic in RevMan version 5.4, with I² values of 25%, 50%, and 75% representing low, moderate, and high heterogeneity, respectively. 45 A random-effects model will be applied when I² exceeds 50%; otherwise, a fixed-effects model will be used. 46 For continuous outcomes, mean differences (MDs) will be calculated when the same measurement instruments are used across studies. If different instruments are employed, standardized mean differences (SMDs) will be used instead. The magnitude of SMDs will be interpreted according to Cohen's thresholds: 0.20 indicating a small effect, 0.50 a moderate effect, and 0.80 a large effect. 47 If continuous data are unavailable, risk ratios (RRs) or odds ratios (ORs) will be used as effect sizes and converted to SMDs following the recommendations of the Cochrane Handbook. 46 Continuous outcomes are preferred, as dichotomizing continuous data may result in information loss, reduced statistical power, and artificial categorization. 48 All statistical tests will be two-tailed, and a p-value < 0.05 will be considered statistically significant.
Subgroup analyses will be conducted based on the following: (1) population characteristics (e.g. healthy children vs. children with various clinical conditions), (2) outcome types (e.g. physical performance, health-related outcomes, psychosocial outcomes), and (3) intervention features (e.g. type of digital platform, intervention duration). Sensitivity analyses will be performed by excluding studies with a high risk of bias to evaluate the robustness of the results. Publication bias will be assessed using funnel plots and Egger's test, 49 with all statistical analyses conducted in R version 4.4.3.
Narrative summary
If meta-analysis is not feasible due to high heterogeneity or insufficient data, a narrative synthesis will be conducted. The included studies will be summarized based on study design, participant characteristics, intervention components, outcome measures, and key findings. Interventions will be categorized by gamification elements, digital technology used, and BCTs applied. Findings will be synthesized based on primary and secondary outcomes, including physical performance, health-related outcomes, psychological and behavioral outcomes, and adherence/safety indicators. Potential sources of heterogeneity, such as differences in intervention duration, delivery method, and study settings, will be discussed. If feasible, qualitative comparisons across studies will be made to explore trends in effectiveness.
Effectiveness of BCTs
To assess the role of BCTs in intervention effectiveness, interventions will be classified into three categories based on behavioral outcome significance, following the approach of Gardner et al.
50
Very promising: Significant improvement in all assessed behavioral outcomes. Quite promising: Significant improvement in at least one behavioral outcome. Not promising: No significant behavioral changes or similar changes in intervention and control groups.
The Promise Ratio method will be used to evaluate the effectiveness of individual BCTs. This ratio compares the frequency of a BCT in effective interventions (those with significant positive outcomes) to its frequency in ineffective interventions (those with non-significant or negative results). The Promise Ratio is calculated as follows:
A Promise Ratio ≥2 suggests that the BCT is more commonly used in effective interventions, while Promise Ratio ≈1 indicates a limited impact.
Descriptive statistics will summarize BCT usage across studies, and inferential statistical analyses will examine the relationship between BCT frequency and intervention effectiveness. A sensitivity analysis will assess whether the risk of bias influences the Promise Ratio results. All BCT coding and analyses will be conducted using Microsoft Excel, NVivo, SPSS, and R software to ensure rigorous data processing.
Discussion
Despite the growing interest in gamified digital exercise interventions among children and adolescents, existing systematic reviews have predominantly focused on intervention effectiveness without systematically unpacking the behavioral mechanisms underlying success.30–32,51 Specifically, few reviews have applied standardized frameworks such as the BCTTv1 to analyze the active ingredients embedded within gamified digital interventions. This systematic review addresses this gap by not only evaluating the effectiveness of these interventions across multiple health domains, but also by identifying the specific BCTs associated with successful outcomes. By integrating the theory-driven classification of BCTs with intervention outcome data, this review aims to provide a more mechanistic understanding of what makes these exercise interventions effective for youth populations.
In the course of the actual research process, we may encounter various challenges and difficulties. This study relies on the reports of intervention implementation processes from publicly available literature, but many of the included studies lack complete descriptions of the intervention details, and some even fail to provide clear definitions or quantitative indicators for the application of BCTs. These discrepancies can affect the accurate identification and analysis of BCTs, leading to the omission or misjudgment of certain intervention elements, thereby impacting the reliability and accuracy of the systematic review results. Significant differences exist between studies in terms of intervention design, technological platforms, implementation duration, study populations, and measurement methods. Due to these variations, cross-study comparisons and integrations present certain challenges, especially when conducting meta-analyses, where sufficient homogeneity may not be achieved. In many intervention studies, there are considerable differences in participant compliance, particularly within child and adolescent populations. Participants may exhibit varying levels of engagement due to factors such as motivation, 52 technology acceptance, 53 or parental support. 54 This variation could influence the assessment of intervention effectiveness, which in turn may impact the analysis of the effectiveness of behavior change techniques. With the rapid iteration and updating of technology, some earlier intervention studies may have used outdated or no longer widely used technologies, which could limit the timeliness of the study results. Therefore, this research has selected literature from the past decade to ensure the relevance and applicability of the findings.
Additionally, this study relies on the BCTTv1 for classifying and coding BCTs in the interventions. However, the standardization framework for BCTs has certain limitations, and some innovative technologies or behavioral strategies used in the interventions may not be fully covered, which could affect the comprehensive evaluation of these interventions. There may also be language limitations in the literature screening process. Despite searching multiple international databases, non-English literature or gray literature may have been overlooked, potentially impacting the comprehensiveness of the study. Many of the interventions in the reviewed studies had short durations and lacked long-term follow-up, which limits our ability to assess the lasting impact of the interventions. Moreover, the interactions between multidimensional intervention outcomes, such as physical health and mental health, are complex, which adds to the difficulty in integrating intervention effects and affects the overall evaluation of intervention outcomes. Finally, while the Promise Ratio provides an intuitive indicator for identifying the effectiveness of certain BCTs, it does not reflect the synergistic effects between BCTs and their actual contributions to the final outcomes.
Conclusion
This systematic review and BCT analysis aim to address the knowledge gap regarding the underlying mechanisms of gamified digital exercise interventions for children and adolescents. By synthesizing evidence from RCTs and high-quality quasi-experimental studies, and applying the BCTTv1 framework, this review will identify which intervention components are most frequently associated with successful health and behavioral outcomes. Moreover, the use of the Promise Ratio will enable a quantitative assessment of the potential effectiveness of specific BCTs in driving positive intervention effects. The findings will offer valuable theoretical insights and practical guidance for the design, implementation, and optimization of future digital health interventions aimed at promoting PA in youth. Ultimately, this review will contribute to evidence-based practices that support sustainable behavior change and foster long-term physical and psychological well-being among children and adolescents.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076251365017 - Supplemental material for Gamified digital exercise interventions for children and adolescents: Protocol for a systematic review and behavior change technique analysis
Supplemental material, sj-docx-1-dhj-10.1177_20552076251365017 for Gamified digital exercise interventions for children and adolescents: Protocol for a systematic review and behavior change technique analysis by Jiajia Zhu, Mengyi Chen, Weihong Jiang, Jiajia Li, Xin Liu, Hongcheng Jin and Jihua Zhu in DIGITAL HEALTH
Supplemental Material
sj-docx-2-dhj-10.1177_20552076251365017 - Supplemental material for Gamified digital exercise interventions for children and adolescents: Protocol for a systematic review and behavior change technique analysis
Supplemental material, sj-docx-2-dhj-10.1177_20552076251365017 for Gamified digital exercise interventions for children and adolescents: Protocol for a systematic review and behavior change technique analysis by Jiajia Zhu, Mengyi Chen, Weihong Jiang, Jiajia Li, Xin Liu, Hongcheng Jin and Jihua Zhu in DIGITAL HEALTH
Supplemental Material
sj-docx-3-dhj-10.1177_20552076251365017 - Supplemental material for Gamified digital exercise interventions for children and adolescents: Protocol for a systematic review and behavior change technique analysis
Supplemental material, sj-docx-3-dhj-10.1177_20552076251365017 for Gamified digital exercise interventions for children and adolescents: Protocol for a systematic review and behavior change technique analysis by Jiajia Zhu, Mengyi Chen, Weihong Jiang, Jiajia Li, Xin Liu, Hongcheng Jin and Jihua Zhu in DIGITAL HEALTH
Footnotes
Acknowledgements
The authors would like to acknowledge the support of our institutional librarians and peer reviewers who provided guidance on search strategies and manuscript preparation. This work was supported by ZJU-GENSCI CHILDREN'S HEALTH RESEARCH & DEVELOPMENT CENTER.
Ethical approval
As this study is a systematic review and meta-analysis using published data, ethical approval is not required. Findings will be disseminated through peer-reviewed journal publications, conference presentations, and stakeholder engagement, following PRISMA 2020 guidelines for transparency and reproducibility.
Contributorship
Jiajia Zhu contributed to conceptualization, data curation, methodology, and writing—original draft. Mengyi Chen and Weihong Jiang contributed to conceptualization and methodology. Jiajia Li and Xin Liu contributed to supervision and validation. Hongcheng Jin contributed to writing—review and editing. Jihua Zhu contributed to conceptualization, methodology, validation, and writing—review and editing. All authors read and approved the final version of the manuscript.
Funding
This work was supported by the 2024 Research Program of the ZJU-GENSCI CHILDREN'S HEALTH RESEARCH & DEVELOPMENT CENTER (Grant No. ZJU-GENSCI2024YB006).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
As a protocol there are no publicly available data.
Guarantor
Jihua Zhu
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.