
Abstract
Background
Mental health problems among children and adolescents increased in recent years, while mental health services are overburdened with long waiting lists. eHealth interventions, that is, interventions delivered digitally via apps or websites, offer a promising approach to prevent and efficiently treat emerging mental health problems in youth. Over the past years, rapid technological progress has led to diverse eHealth interventions for youth mental health. However, a structured overview of effective eHealth elements and mechanisms through which interventions aim to improve mental health is lacking. The aim of this pre-registered systematic review is to identify elements of eHealth interventions that improve mental health and well-being in children and adolescents aged 10–25 from both clinical and general populations.
Methods
This systematic review conducted in April 2023 in accordance with the Preferred Reporting Items for Systematic Review and Meta-Analysis guidelines identified 108 studies and 103 distinct interventions between 2011–2023. The overall sample size was 33,435 participants (30.7% male, mean age = 18.4 years, SD = 2.5). Most studies (64.8%) were randomized controlled trials (RCTs) to test the interventions. The remaining studies utilized a pre-post or group-comparison design (non-RCTs).
Results
The interventions were heterogeneous in design, method of delivery, target group and outcome measures. Overall, 77.7% of the studies showed a positive significant association between eHealth intervention and mental health or well-being. Elements that were often related to improved mental health and well-being were cognitive behavioural therapy (CBT) or self-monitoring as therapeutic principles, blended approaches combining eHealth with traditional therapy, peer/parental involvement and technological gamification elements, such as rewards.
Conclusions
Elements of youth eHealth interventions that appear to positively impact mental health or well-being are (a) CBT-based, (b) self-monitoring (c) blended interventions, (d) peer or parental involvement or (e) gamification. Future directions for the development and implementation of eHealth interventions for youth are discussed.
Keywords
Introduction
Adolescence includes the life transition from childhood to adulthood and is marked by an increased vulnerability to mental health problems. 1 Currently, an estimated 13–25% of European adolescents suffer from depression or anxiety. 2 Current societal challenges, demands and major crises such as the COVID-19 pandemic, may further increase the risk of mental health problems.3–6 One of the major challenges ahead is the overburdened healthcare system; timely identification and treatment of mental health problems are difficult, with a shortage of healthcare professionals, long waiting lists for treatment and lack of effective prevention strategies. 7 Moreover, stigma associated with mental health problems and help-seeking, and complex ‘pathways to care’ further delay treatment.8,9 Overall, for adolescents with mental health problems, it may take several years to be diagnosed and receive adequate treatment.10,11 Therefore, alternative, easily accessible and sustainable approaches to promote resilience and prevent the onset of mental health problems in children and adolescents are urgently warranted.12,13
A promising approach to prevent and treat mental health problems and to build resilience in adolescents is eHealth. eHealth can be defined as ‘health services and information delivered or enhanced through the Internet and related technologies’. 14 Advantages of eHealth compared to face-to-face therapy for mental health problems include lower invasiveness, potential higher cost-effectiveness, lower threshold for help-seeking and efficient delivery of therapy.15,16 The field of eHealth for mental health has evolved rapidly, with an enormous increase in the number of eHealth interventions in recent years.17,18 This has resulted in a diverse range of existing eHealth interventions, varying in design, mode of delivery, content and mechanisms through which interventions aim to improve mental health. However, most eHealth interventions lack scientific substantiation. 19 To develop evidence-based future-proof and sustainable eHealth interventions it is essential to understand which elements are effective. In this study, we review the literature on different elements (mode of delivery, therapeutic principles, blended intervention and/or involvement of others and interactive elements) of eHealth interventions aimed at enhancing mental health or well-being in children and adolescents.
Elements of eHealth interventions
The first element we investigate in this review is the mode of delivering interventions, that is, via smartphone applications, web-based or text messages. Earlier eHealth interventions targeting mental health were mainly computerized versions of cognitive behavioural therapy (CBT) or included additional telecommunications (i.e. text messages or emailing) to face-to-face therapy. Some contemporary eHealth interventions still include these elements. However, the rapid technological development and the rise of mobile technology in the last decade led to the development of eHealth interventions via websites or smartphone applications. Currently, there are around 20,000 mental health apps in the app store and the popularity continues to grow. 20 Importantly, providing eHealth interventions appears particularly useful and feasible for youth, since the vast majority (∼95%) of adolescents in the United States and Europe have access to smartphones or laptops. 21
The second element in this review includes the therapeutic principles of eHealth interventions. According to recent systematic reviews of randomized controlled trials (RCTs), most eHealth interventions for youth are based on CBT and are related to improved mental health in children and adolescents.22,23 CBT is a treatment approach that aims to identify and modify maladaptive patterns of thinking, emotional responses and behaviours. 24 An essential element of CBT is the learning and application of adaptive coping strategies, such as seeking social support, self-acceptance, positive distractions and problem solving. In adolescents, CBT is commonly used to treat depressive symptoms and disorders and has been found to be effective in reducing mental health problems and increasing well-being in youth.25,26
The efficacy of eHealth interventions based on other therapeutic principles than CBT, such as positive psychology, mindfulness or self-monitoring, are less frequently investigated, resulting in inconclusive evidence. 27 However, there is empirical evidence on these therapeutic principles in regular care (non-eHealth contexts), which might be interesting to study further. Specifically, positive psychology is the scientific study of what makes life most worth living, focusing on both individual and societal well-being. 28 Interventions based on positive psychology specifically aim to enhance well-being instead of reducing psychopathological symptoms and can be used to complement clinical psychological interventions for mental health symptoms. Well-known examples of positive psychology interventions include practicing gratitude or forgiveness, being kind to others, writing about positive, meaningful or successful experiences and finding flow. Systematic reviews and meta-analyses found positive psychology interventions to be effective in increasing well-being, as well as decreasing depression and anxiety symptoms.29,30 Moreover, originating from Buddhist practice and philosophy, mindfulness can be described as the state of being attentive to and aware of what is taking place in the present. 31 Interventions to increase mindfulness often include meditation or relaxation practices and have been related to various mental health and well-being outcomes, both in adults 32 and youth. 33 Furthermore, self-monitoring can be used as an element to improve mental health by enhancing emotional self-awareness.34,35 Self-monitoring is nowadays mostly done via the experience sampling method (ESM) using the smartphone of the participant. ESM includes the repeated assessment of mood, behaviour and context per day. The collection of data on momentary positive and negative affect multiple times per day is thought to enhance self-insight and self-management, allowing for early identification of mood problems. Mood patterns can reveal important information for both the participant and the therapist if applied in a clinical setting. 35
The third element in this review is the addition of face-to-face therapy or inclusion of parents/peers in eHealth interventions. eHealth interventions can be administered as stand-alone (e.g. patients themselves play a mindfulness app), supported by peers or parents or blended in combination with face-to-face therapy. Recent reviews suggest that interventions are more likely to be effective when they include a face-to-face component compared to self-administered interventions.22,23 However, conclusive evidence based on more studies is needed.
Lastly, the fourth element in eHealth interventions include advanced gamification or interactive elements. Technological advancements have resulted in the development of chatbots and serious gamification.36,37 Chatbots are automated artificial intelligence (AI)-driven software. Through interactive interfaces, people can engage in conversations with chatbots via text or speech. Chatbots recently emerged in psychotherapy, providing guided psychotherapy via automated script-based dialogue. 36 In adults, chatbot-delivered psychotherapy seems to reduce depressive symptoms. 38 Gamification refers to the use of gaming elements in healthcare and digital health. It involves serious gaming, that is, teaching skills or knowledge through games and integrating game-like elements, such as earning points, rewards, challenges, group competition, to engage and motivate users in their healthcare activities.39–41 A meta-analysis of 42 studies showed a positive effect of gamification on mental health in children, adolescents and adults. 36 The effect was consistent across platforms (smartphone vs website) and goals of the game (mental health enhancement, physical health enhancement or learning). Similarly, gamification was effective in samples with different characteristics, that is, age and clinical status, indicating the potential of gamification in eHealth interventions in diverse populations.
Taken together, despite a strong increase in eHealth tools, it is not yet clear which elements improve mental health and well-being in children and adolescents. Previous systematic reviews suggest that eHealth interventions are effective in improving mental health and well-being, but these interventions are mostly limited to CBT targeting depression and anxiety.22,23,42 Other therapeutic principles, such as positive psychology, mindfulness or self-monitoring and other measures of mental health problems and well-being are not taken into account. This focus on CBT-based interventions leaves a significant gap in our understanding of how these alternative therapeutic approaches, which may offer unique benefits, contribute to mental health outcomes. Moreover, the rapid technological advancements and heightened interest in eHealth due to the COVID-19 pandemic have likely increased the variety and number of eHealth interventions beyond those previously reviewed. Therefore, there is a pressing need to evaluate these emerging interventions to identify which elements are most effective across different therapeutic approaches and outcomes.
Aims
In this systematic review, we describe elements of eHealth interventions aiming to reduce mental health problems and enhance well-being in children and adolescents aged 10–25 years both from clinical and general populations. We explicitly chose this broad age range from adolescence to young adulthood to provide a complete review that reflects the diversity of eHealth interventions available across different developmental stages (instead of focusing on only one developmental stage). This is in line with recent work that expanded the definition and timeframe of adolescence to include young adulthood, because adolescence mostly extends into the early 20 s, as more youth in modern societies are postponing traditional adult responsibilities such as starting a family, securing full-time employment or purchasing a house. By systematically exploring a broad range of therapeutic principles, we aim to provide a comprehensive understanding of the effective components of eHealth interventions. In particular, we include studies on eHealth interventions (both RCTs and non-RCTs) based on different therapeutic principles, assessing a wide range of mental health and well-being outcomes in clinical samples and samples from the general population. Understanding these elements is important for advancing the field, as it can inform the development of more targeted and effective eHealth solutions. First, we describe the elements of existing eHealth interventions, including the (a) mode of delivery, that is, smartphone application, web-based or text messages, (b) therapeutic principle of the intervention, such as CBT, mindfulness and positive psychology, (c) blended interventions and/or involvement of others, such as parents or peers and (d) interactive elements, such as chatbots or gamification. Second, we describe the mental health and well-being outcomes. Finally, we evaluate the effect of the different elements in improving mental health or well-being in children and adolescents.
Method
Search strategy and selection criteria
This systematic review is conducted and reported in accordance with the Preferred Reporting Items for Systematic Review and Meta-Analysis guidelines (Moher et al., 2009). Hypotheses and methods were pre-registered in PROSPERO (https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42023404110). The search was conducted in 02/2022 and updated in 04/2023 by the medical library of the Erasmus MC Rotterdam, The Netherlands. The electronic databases Embase, Medline ALL, PsycINFO, Web of Science, Cochrane and Google Scholar were used (see online supplemental materials A1 and A2 for search string queries).
Inclusion criteria included studies that investigated eHealth interventions aimed at reducing mental health problems (e.g. depression, anxiety and stress) or improving well-being in children and adolescents aged 10–25 years. Additionally, studies were included if they assessed the intervention effects using quantitative measures of mental health or well-being rather than qualitative approaches. Exclusion criteria were: (a) focus on a very specific target group (e.g. pregnant teenagers or paediatric patients), (b) no digital intervention, (c) intervention primarily targeting the support system of children/adolescents (e.g. parents), (d) evaluation via qualitative data, (e) no English article or full-text availability or (f) study protocols, systematic reviews, letters, case reports or conference abstracts.
Figure 1 provides an overview of the selection process and the reasons for exclusion. After the initial search, duplicates were manually removed. All remaining articles were assessed for relevance based on titles and abstracts. To ensure a robust selection process, five independent reviewers (SvE, ED, FB, MvdE, AV) participated, with a mean interrater reliability of 81.3%, indicating a strong level of agreement. Any discrepancies were resolved through consensus between two reviewers (SvE, ED). Full-text papers of the included 108 articles were independently assessed by two reviewers (SvE, ED) with a strong mean interrater reliability of 94.4%. Data extraction from all included papers was carried out by LdV, with validation and cross-checking performed by SvE and ED.
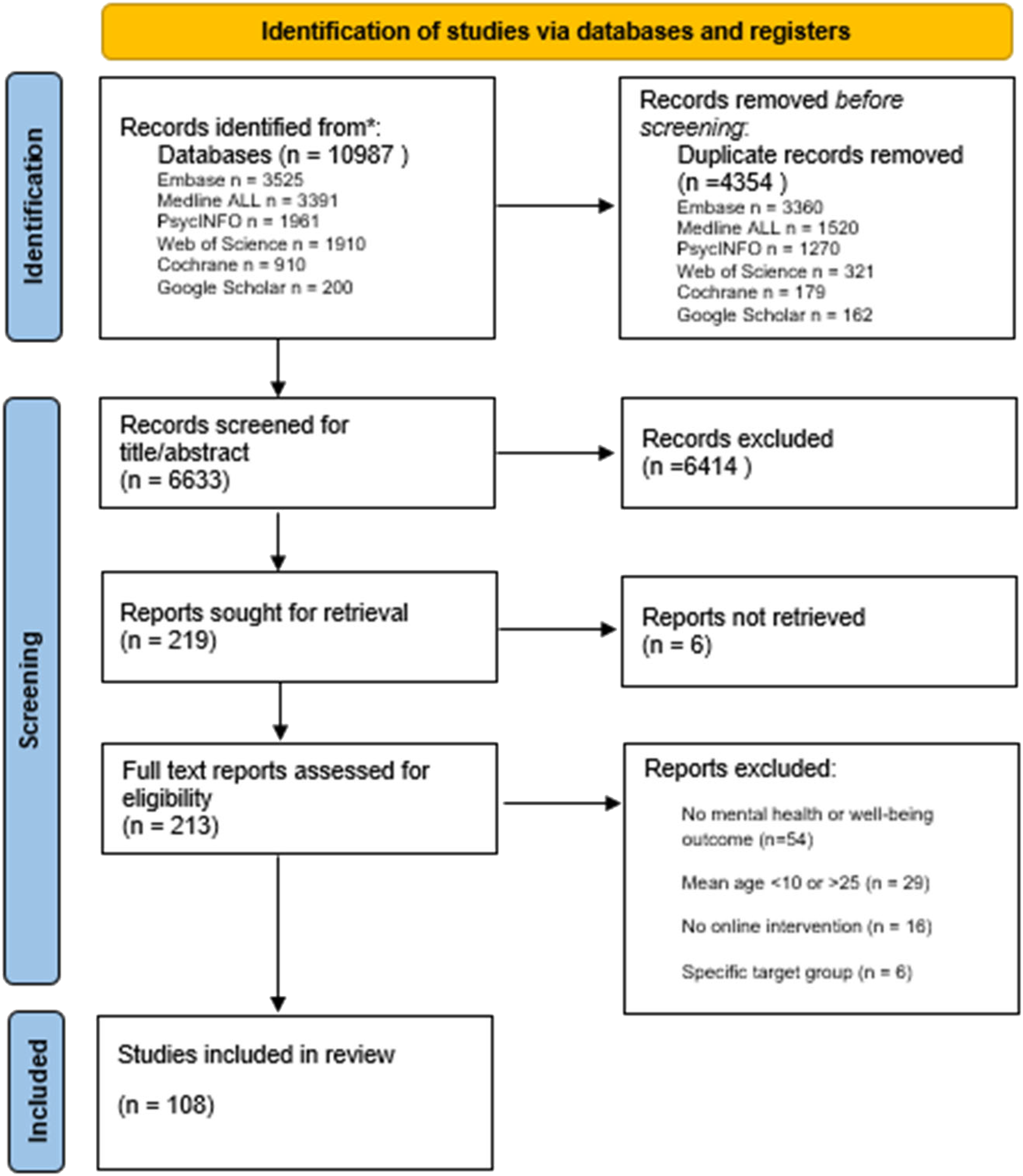
PRISMA flow diagram of the search and selection process.
Data extraction and quality assessment
Data on descriptives, design, elements and efficacy were extracted from the included studies. Quality assessment and risk of bias in the included studies were performed using the national institute of health Quality Assessment tool (https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools). This tool consists of a checklist with 14 (RCT) or 12 (non-RCT: pre-post/group comparison studies) questions, which can be answered with ‘yes’, ‘no’, otabr ‘cannot determine/not reported/not applicable’. To determine the quality rating of the studies, scores were assigned based on the percentage of items answered ‘yes’: >80% was considered good, 60–80% was considered fair, and <60% was considered poor quality (see online supplemental materials for details). The quality assessment was conducted by three reviewers (SvE, ED, LdV). Each study was evaluated by two reviewers. Initially, the reviewers individually rated the studies and, in case of inconsistencies between ratings, the differences were resolved through discussions until agreement was reached.
Results
Characteristics of studies and participants
In total, 108 studies were included. Table 1 shows the characteristics of the included studies. The studies were published between 2011 and 2023. The overall sample size was 33,435 participants. The average age of the participants ranged from 9.5 to 24.3 years, resulting in a mean age of 18.4 (SD = 2.5). The proportion of males was on average 30.7%. Studies were mostly conducted in Europe (knumber of studies= 34/108) followed by North America (k = 33/108), Oceania (k = 23/108), Asia (k = 17/108) and Africa (k = 1/108). Quality assessment indicated that a small proportion (17%) of the RCTs were considered to have poor quality, 64% had fair quality, and 19% had good quality (see Table A3 in the online supplemental materials). Of the non-RCTs, 50% of the studies had poor quality, and respectively, 37% and 13% of the studies had fair or good quality (see Table A4 in the online supplemental materials). Regarding power, among the RCTs, 53% (37/70) had an adequate sample size for detecting differences with at least 80% power. In non-RCTs, 32% (12/38) reported sufficient power. Over all studies, this means that 55% of the studies did not have an adequate sample size to detect effects. Furthermore, only 54% (58/108) of the studies pre-registered their methods and analyses.
Descriptive characteristics of included studies in the systematic review.

Note: N.R: not reported; Group: G.O./A.R./C.P.; G.O.: general population, A.R: at risk, C.P.: clinical population; Type: WL/TAU/AO; WL: waitlist, TAU: treatment as usual, AO: assessment only, AM: attention matched. The country abbreviations can be found at https://en.wikipedia.org/wiki/ISO_3166–1_alpha-3. Quality = >80% yes answers were considered good (green), 60%–80% were considered fair (yellow) and <60% were considered poor quality (red). Registration: pre-registration by means of a clinical trial registration for RCT or analyses pre-registration.
The 108 studies, including 103 distinct interventions, include a description of 112 evaluations of interventions (i.e. four studies compared two different interventions). The interventions Grow It! and Headspace were evaluated three times in different studies and samples, and the interventions Bite Back, CARE, EMIcompass, Intellect, and Whitu were each evaluated twice. Few eHealth interventions (24/103, 23.3%) were developed in co-creation or co-design with youth. The duration of the interventions differed substantially and ranged from a single session to 300 days, with an average of 54.4 days (SD = 46.2, median = 42 days).
Of the included studies, 70 (64.8%) were RCTs, 35 (32.4%) used a pre-post design (non-RCT), and the remaining three were group comparisons (non-RCT). Of the RCTs, 34 had a passive control group (assessment-only, k = 12, or a waitlist group, k = 22) and 37 studies had an active control group (attention-matched intervention, k = 27) or treatment as usual, k = 10). We report RCT results separately from non-RCT results because RCTs offer more rigorous control over confounding variables, reducing bias and providing clearer insights into the efficacy of interventions. The target population differed. Several studies (43/108; 39.8%) recruited children and adolescents from the general population, whereas 35.2% of the studies (38/108) included children or adolescents in clinical outpatient settings, and 25.0% (27/108) targeted participants at risk for mental health problems, such as adolescents exposed to family violence or those with parents diagnosed with mood disorders.
Elements
Tables 2 and 3 display the results regarding the elements of eHealth interventions in respectively RCT and non-RCT studies.
Mode of delivery. Approximately half of the interventions (54/103, 52.4%) were delivered through smartphone applications and this increased substantially over time (see Table 2) and Figure 2). Furthermore, 36/103 interventions (35.0%) delivered the intervention via websites, whereas seven studies, mostly older studies, utilized text messages. The remaining studies used a combination of either applications and websites (k = 4) or websites and text messages (k = 2). Therapeutic principles. The different therapeutic principles of the interventions can be found in Figure 3. The interventions mostly included CBT (57/103, 53%), self-monitoring of daily mood (17/103, 13%), mindfulness (14/103, 13%) or positive psychology (10/103, 9%). The remaining interventions included content based on a range of theories and therapies, including motivational interviewing, dialectical behavioural therapy, acceptance and commitment therapy and family focused therapy. One-third of the interventions (35/103, 33%) combined content from different therapeutic principles, for example, both CBT and positive psychology. For more information on the intervention elements used in the studies, see Table A5 in the online supplemental materials. Blended interventions and/or involvement of others. In 32 studies (28.6%), eHealth interventions were studied in a blended form, either by offering additional sessions with a therapist (26/32), classroom teaching (5/32), or in combination with a coach (1/32) or general practitioner (1/32). In 12 studies, parents were involved in the eHealth intervention and in five studies peers were involved. Interactive elements. In three interventions (3/103) a chatbot was included. The chatbots were Woebot (Fitzpatrick et al., 2017; Nicol et al., 2022) and XiaoNan (Liu et al., 2022). Both chatbots are CBT-based and help adolescents to understand and regulate their emotions, thoughts and behaviours via tailored conversations.

Mode of delivery used to deliver interventions by year. Note that the search was until April 2023, but in this figure, we included studies until 2022 to only include complete years.

The number of interventions that included the different therapeutic principles.
Results of randomized controlled trials on elements of eHealth interventions.
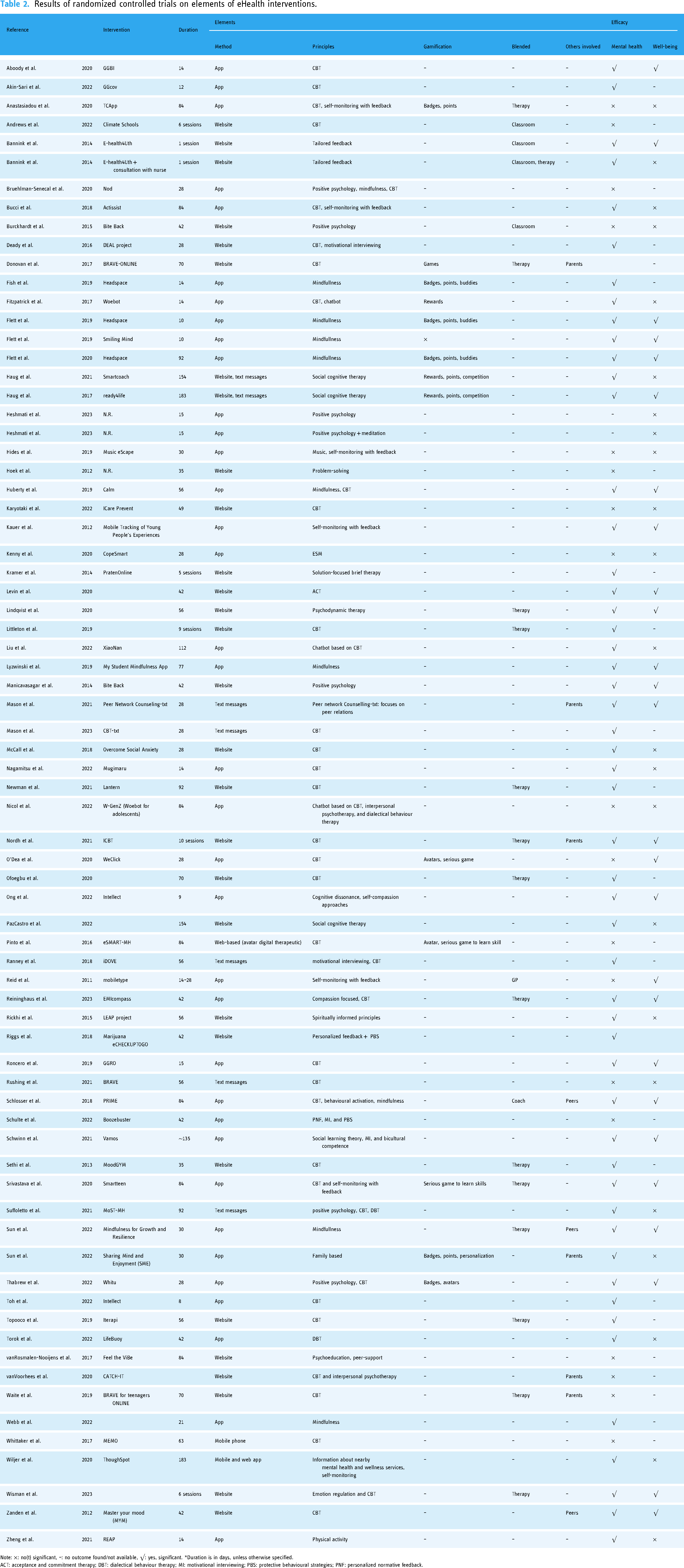
Note: ×: no(t) significant, –: no outcome found/not available, √: yes, significant. *Duration is in days, unless otherwise specified.
ACT: acceptance and commitment therapy; DBT: dialectical behaviour therapy; MI: motivational interviewing; PBS: protective behavioural strategies; PNF: personalized normative feedback.
Results of non-RCT studies on the elements of eHealth interventions.

Note: ×: no(t) significant, –: no outcome found/not available, √: yes, significant. *Duration is in days, unless otherwise specified.
Of the 103 interventions, 21 (20.4%) included one or more gamification elements (see online supplemental material A6). In 12 interventions, serious games were included to learn a specific skill, such as coping, exposure or communication. In 11 interventions, rewards, like badges or virtual gifts were included to enhance adherence. Similarly, in nine interventions the participants could earn points. In six interventions, participants could choose an avatar or personalize the intervention in another way. Finally, there was the opportunity to interact with peers, via a chat or buddy system in three interventions.
Mental health and well-being outcomes
Different outcome measures were used for mental health and well-being (see Figure 4 and Table A5 in the online supplemental materials). The most frequent mental health outcome measures included depressive symptoms or disorder (in 56% of the evaluations of interventions one or more measures of depression were included), anxiety (43%), alcohol use (13%) and stress (22%). The most frequent outcome measures of well-being included general well-being, such as quality of life or positive affect (32%), self-efficacy/self-esteem (16%), resilience (6%) and mindfulness (7%).
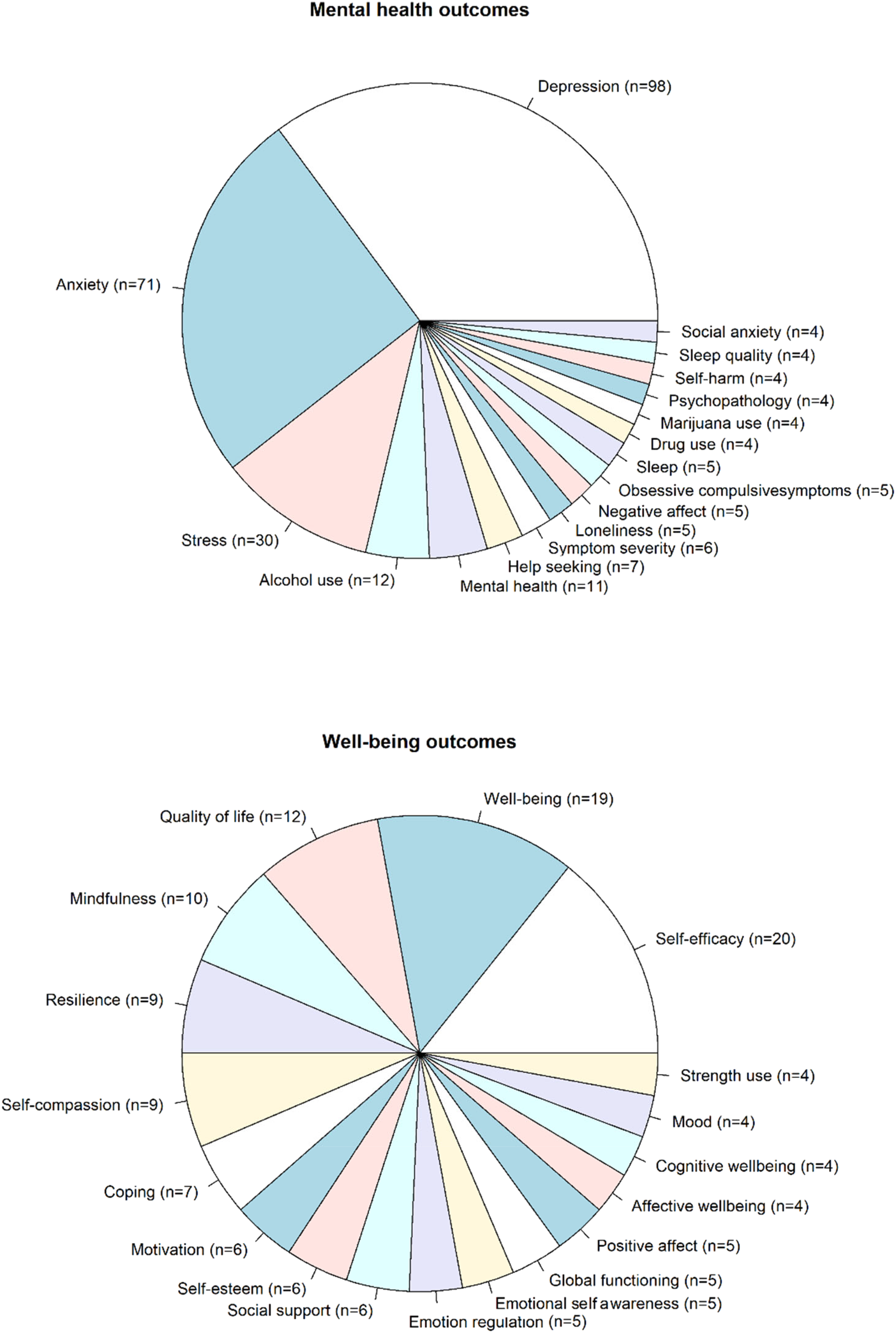
Pie charts of different mental health (top) and well-being outcomes (bottom) used in the included studies to assess the efficacy of the different interventions.
All studies included a follow-up assessment shortly or directly after the intervention to assess the intervention effects. In addition, 48 studies of interventions (45%) included one or more extra follow-up assessments. This follow-up time was on average 4.0 months (SD = 3.2, range = 1–18 months).
Effects of eHealth intervention on well-being and mental health
Overall, 77.7% (84/108 studies) of the studies reported a significant positive association between the eHealth intervention and one or more mental health or well-being outcome measures. The percentage of studies showing a positive effect of the eHealth intervention on mental health or well-being varied based on the elements (mode of delivery, therapeutic principles, blended intervention and/or involvement of others, interactive elements) as described below.
1. Effects of mode of delivery
Of the 62 studies on interventions delivered via smartphone apps, 50 showed improved mental health or well-being (80.6%). Among the 37 web-based interventions, 28 studies showed improved mental health or well-being (75.7%). Interventions utilizing text messages improved mental health or well-being in 85.7% (six out of seven) of the studies. Finally, four out of six intervention studies (66.7%) combining different modes of delivery, for example, smartphone application and web-based) showed an improvement in mental health or well-being.
2. Effects of therapeutic principles
Figure 5 shows the therapeutic principles of the interventions in four categories (CBT, self-monitoring, mindfulness and positive psychology) and the proportion of studies reporting improved mental health or well-being. A darker color indicates a higher proportion of studies that reported a significant positive effect of the eHealth intervention on the outcome measure. In 58% of the studies, a positive significant association between CBT and any mental health or well-being measure was reported. Similarly, across all outcomes, 59% of the studies reported improved mental health or well-being due to interventions including self-monitoring. Interventions based on mindfulness showed positive significant associations with mental health and well-being in 50% of the studies and interventions based on positive psychology only in 32% of the studies.
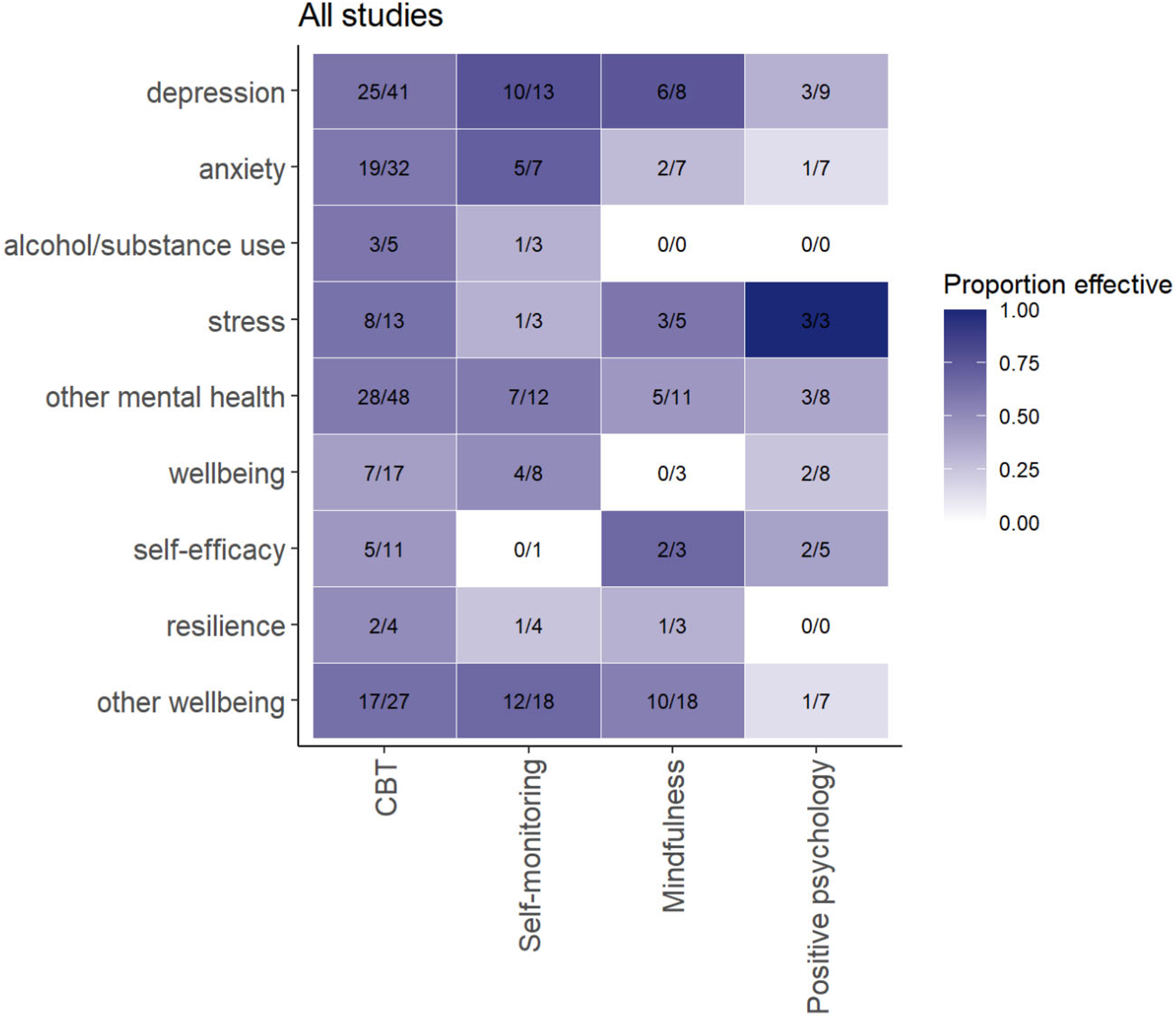
Effect of the therapeutic elements on mental health and well-being outcomes. The colours in the cells show the proportion of studies that reported improvements in mental health or well-being. A darker color indicates higher proportion of studies that reported a significant positive effect of the eHealth intervention on the outcome measure.
Besides the four described therapeutic principles, a large part of the studies included interventions based on other therapeutic principles, including motivational interviewing, dialectical behavioural therapy, acceptance and commitment therapy, or family focused therapy. The percentage of interventions based on these therapeutic principles that showed a positive significant association with mental health or well-being was not computed as this is uninformative due to the limited number of studies.
Taking into account the sustainability of intervention effects, we looked at the 48 intervention trials that included one or more additional follow-up assessments. Thirty of these trials included a CBT intervention, and 70% still showed effects on well-being and mental health 4 weeks to 6 months later. There were not enough follow-up assessments for other intervention elements to be able to say anything about sustainability.
3. Effects of blended interventions and/or involvement of others
Eighty studies provided the intervention as a stand-alone, and 60 (75%) of these showed a significant improved mental health or well-being. In 22/25 studies (88%) that combined the eHealth intervention with face-to-face therapy, there was an improvement in mental health or well-being. Additional classroom teaching, or sessions with a general practitioner (Reid et al., 2011) or coach (Schlosser et al., 2018), improved mental health or well-being in four of the six (67%) studies. The majority of the studies that involved parents (8/11, 72.7%) or peers (5/5100%) in the intervention showed an improvement in mental health or well-being.
4. Effects of interactive elements
Of the three interventions that included a chatbot, two studies showed reduced depression61,86 versus. 99 Of the interventions with one or multiple gamification elements, 88.5% (23/26) reported improved mental health or well-being, compared to 74.4% (64/86) of interventions without gamification.
Discussion
There is an enormous increase in available eHealth applications, mounting over 20,000 mental health apps in the app store. 20 However, few of them have a solid scientific body of evidence. In this systematic review, we evaluated scientific studies on eHealth interventions for mental health and well-being in children and adolescents and reviewed which elements (mode of delivery, therapeutic principles, blended intervention and/or involvement of others, interactive elements) are effective in improving mental health and well-being. In total, 103 distinct interventions over a total of 33,435 participants were studied. Overall, in 77.7% of the studies eHealth interventions were related to improved mental health or well-being. Elements that were often reported to result in improved mental health and well-being were CBT and self-monitoring as therapeutic principle, a blended approach of combining eHealth with traditional therapy, parent/peer involvement and gamification elements, such as rewards. This suggests that these elements can be effective in enhancing mental health and well-being in youth via eHealth interventions. However, the quality of the studies varied, and the majority of the studies did not have sufficient power to detect an effect. These results emphasize that eHealth is often studied and can be effective in improving mental health and well-being in youth, but the quality of the research design and methodology should be taken into account.
Effective elements of eHealth interventions
In contrast to what can be found in the app store, all of the here described apps were based on scientific insights. Compared to the earlier reviews mainly focusing on CBT,22,23,42 we evaluated a diverse range of therapeutic principles including CBT (57%), self-monitoring (13%), mindfulness (13%) and positive psychology (11%). One third of the interventions combined multiple therapeutic principles. We found that over half of the studies examining CBT-based eHealth interventions (58%) reported a significant improvement of mental health or well-being. This is comparable to findings described in earlier reviews.22,23,42 However, CBT-based interventions differed widely in their exact content. Due to large heterogeneity in the exact content and outcome measures, we did not dive into these differences. However, we expect that disorder-specific content may enhance the efficacy of an eHealth CBT-based intervention. Furthermore, whereas for anxiety and depressive disorders specific content related to mental health and a long-term treatment might be needed,25,26 improvements in well-being may require other content and possibly shorter interventions. Future research with standardized measures per outcome is needed to effectively compare such CBT-based eHealth interventions.
Significant improvements in mental health and well-being were reported in 59% of studies of eHealth interventions that included self-monitoring. The working mechanism of self-monitoring is improving mental health by enhancing emotional self-awareness, self-insight and self-management.34,35 However, accurate self-monitoring depends on sufficient compliance; that is, participants should complete mood surveys when requested. Yet, adherence and compliance are challenging in both offline and online interventions. 150 Options to maximize compliance include active monitoring of compliance and personalizing questionnaires. In clinical settings, self-monitoring can be stimulated as part of a collaborative process between the patient and clinician, in which discussion of mood surveys is part of the treatment. 151 Importantly, there were more non-RCT studies that reported a positive effect of self-monitoring (79% of 42 studies) than RCTs (30% of 27 studies; see online supplemental material A5). Although we did not conduct a meta-analysis and these results are not directly comparable, the difference in effectiveness between non-RCTs and RCTs is noteworthy. In RCTs, bias is reduced and cause-effect relationships between interventions and outcomes can be interpreted with more certainty than in non-RCTs. However, insights from studies in a less controlled environment (‘real world studies’ such as pre-post designs) on the intrinsic motivation for sustained engagement with a preventive app is essential if eHealth interventions are to be made publicly available for wider implementation. Therefore, evaluations in RCTs and non-RCTs could lead to different pieces of the puzzle in understanding the working mechanisms and effects of eHealth interventions.
Interventions based on mindfulness and positive psychology showed a positive significant effect on mental health or well-being in respectively 50% and 32% of the studies. The findings on mindfulness are partly in line with a meta-analysis of 20 studies on the effect of face-to-face mindfulness on anxiety, depression and stress among children. 33 The authors found that mindfulness had positive effects in 5/20 studies and reported a moderate meta-analytic effect of mindfulness (d = 0.37). The diversity in duration and exact content of mindfulness interventions differed. Therefore, the optimal conditions to benefit from mindfulness are not clear yet and need further investigation. Similarly, the effectiveness of positive psychology interventions in increasing mental health and well-being need future research.29,30 Interventions based on positive psychology specifically aim to enhance well-being and can be used to complement clinical psychological interventions for mental health problems. 28 An explanation for the relatively low percentage of effective interventions could be the diverse positive psychology interventions, from practicing gratitude or forgiveness, being kind to others, writing about positive or meaningful experiences, to finding flow. This indicates that more research is needed to the effective elements within positive psychology.
Reviewing studies on blended eHealth interventions seem to suggest effectiveness. Combining eHealth interventions with face-to-face therapy, 88% of the studies showed improved mental health or well-being. Furthermore, 73% of the studies with involvement of parents showed an improvement in mental health or well-being, whereas all five interventions with involvement of peers showed positive effects. These findings are in line with earlier reviews22,23 and indicate the potential importance of human interaction, and especially peers, in eHealth interventions for youth mental health.
Finally, interactive or gamification elements, such as rewards or avatars, were only included in 20% of the interventions described in this review. These elements might improve mental health or well-being: a slightly larger percentage of interventions with gamification elements showed improved mental health and well-being (89% versus 74% of interventions without gamification), replicating the consistent positive effects of gamification in the review of Cheng and colleagues. 36 One explanation of the mechanism behind the effects of gamification is that gamification increases adherence to the eHealth intervention due to positive reinforcement via rewards or points. This mechanism may be similar to face-to-face CBT where progress is recognized and rewarded in various ways, for example, using a sticker chart or praising the progress of behavioural change. 152 Positive reinforcement as part of the therapist toolkit is associated with higher self-esteem and self-efficacy. 153 In contrast to face-to-face CBT that is mostly individual, gamification in eHealth interventions allows for team elements, such as contact with peers, to further increase adherence and user experience.36,41 This indicates that gamification appears to have potential in eHealth interventions for mental health in youth. For a more detailed discussion about the role of gamification in eHealth see the focused review of Cheng and colleagues. 36
Strengths, limitations and future directions
In this systematic review we extend previous reviews22,23,42 by including the most recent eHealth studies and more diverse interventions and outcome measures. For example, whereas Garrido et al. 22 and Hollis et al. 42 only included RCTs to assess the efficacy of eHealth interventions, we included both RCTs and non-RCT studies to review newer interventions with more advanced technology; for new interventions, (pilot) non-RCT studies are often the first step to test efficacy and RCTs are not always available.
This study also has limitations. First, a quantitative meta-analysis to test the effect size of different elements of the eHealth interventions was not possible, because the studies were too heterogeneous in study methods, outcomes, therapeutic principles, analyses and reported effect sizes. To increase opportunities for meta-analyses, we advocate for strict adherence to standardized reporting of eHealth interventions and evaluations, such as CONSORT-EHEALTH. 154 These guidelines require complete reporting of the theoretical framework of the intervention, as well as content, duration, mode of delivery, involvement of others, outcome measures, implementation and analyses methods.
Without a meta-analysis we could not directly compare results between studies. Instead, we report the proportion of studies that found significant effects of interventions on mental health and well-being. However, publication bias could have influenced the results and limited the generalizability of our findings. Studies with significant outcomes are more likely to be published, while those with null or negative results may remain unpublished. The high percentage of studies that reported a significant positive association between the eHealth intervention and one or more mental health or well-being outcome measures (77.7%) could indicate a publication bias. This selective reporting can lead to an overestimation of effects and limit the interpretation of effective elements. Second, we focused on the effects of single elements of eHealth interventions. However, most eHealth interventions included multiple elements; for example CBT, self-monitoring and gamification. By describing the individual effects, it is possible that we miss the interactive effects of the different elements. Therefore, future research should study the potential accumulative effect of specific combinations of different eHealth elements on mental health and well-being. Conducting factorial designs or intervention mapping approaches could provide insights into the specific mechanisms underlying these interactions.155,156
Furthermore, although we grouped the therapeutic principles into commonly used definitions, such as CBT or mindfulness, the operationalization differed in various ways. For example, the content of CBT interventions widely differed between studies (e.g. conversations with chatbot, group-sessions or psychoeducation). Also, the duration of the intervention (8–300 days) differed widely. It is possible and likely that these differences in operationalization lead to differences in outcomes. The adherence to standardized reporting of eHealth interventions and evaluations as described above could help to further investigate associations between intervention designs and outcomes.
In addition, pre-registration should play an important role in new eHealth studies. Pre-registration can be seen as an indicator of the dedication to be transparent, rigorous and reproducible. The process of publicly registering study plans, hypotheses and methods, before conducting the study mitigates biases and enhances credibility of findings. 157 Of the studies included in this review only 54% of the studies was pre-registered. Furthermore, a substantial number of the studies had poor quality ratings. This could have affected the findings, as poor-quality studies may introduce various biases and errors that skew results. The high proportion of studies with poor quality, particularly among the non-RCT studies (50%), indicate the need for more high-quality research in this field. Similarly, power was not sufficient or not reported in 55% of the studies, limiting the reliability of the findings. Therefore, the overall conclusions drawn from this review should be considered with caution, and future research should focus on improving study quality to provide more evidence on the effectiveness of eHealth interventions.
In this review we included studies in adolescents between 12–25 years of age, and to be able to generalize the results to different populations, we included studies with adolescents from the general population, at-risk youth and clinical samples. The distribution of samples across these categories was mostly equal (39.8% general population, 35.2% clinical samples and 25.0% at risk for mental health problems). However, in other aspects the results could be less generalizable to the whole population. For example, the studies mostly included older adolescents (mean age of 18.4 years) mostly females (mean = 69.3%), and mostly adolescents from Europe and the United States. This indicates that future studies to eHealth interventions should include more diverse samples with respect to these sample characteristics.
Another important aspect to take into account is the perspective of youth on eHealth interventions themselves. Incorporating this perspective is important to ensure interventions are appealing for the target audience and working as intended.158,159 However, in most of the studies included (77%) the involvement of youth or co-creation was not reported or not included in the development of eHealth interventions. Earlier experience with co-creation of the Grow It! intervention app 160 in our research group proved this approach valuable in understanding the world through the lens of future generations. Co-creation can be applied in different ways, depending on the desired involvement of the youth in the different stages of developing an eHealth intervention. For example, incorporating youth perspectives in eHealth development can be done through discussion groups and iterative feedback sessions to optimize an intervention that is already developed. Alternatively, in what is also called Participatory Action Research, youth are included at the start of the study and act as experience experts during all stages of the developmental process. 161 Involving youth in some way in the process helps to ensure the intervention is user-friendly and relevant and this can enhance the effectiveness of the eHealth intervention. Therefore, we recommend co-creation with youth in the development of future eHealth interventions.
Furthermore, in recent years, the field of youth mental health has seen significant advancements through the integration of technology. This technological progress allows the inclusion of advanced elements in eHealth interventions, such as the use of generative AI and integration of large language models (LLMs) into mental healthcare. 162 An application of LLMs in mental health care are chatbots. As described, the chatbot Woebot seems to positively affect adolescent mental health.61,99 Woebot is based on CBT and uses generative AI to chat with users and to deliver personalized, in-the-moment support. The quick developments in the field of AI and LLM hold promise for creating more interactive, engaging and effective mental health interventions. These technologies can potentially provide scalable, accessible mental health support, bridging gaps in traditional care and reaching underserved populations. As AI continues to evolve, future research should focus on optimizing these tools, ensuring ethical standards and evaluating long-term impacts on youth mental health outcomes. For the opportunities and risk for AI-driven interventions in mental health see recent publications. 162
Technological advances can be used to further personalize interventions. Personalization can increase the involvement and therefore the efficacy of an intervention. For example, adolescents’ feeling of control can be enhanced by having them decide who will be involved (e.g. parent, peer, therapist) in different modules. Just-in-time adaptive interventions (JITAI) take personalization a step further. Unlike traditional interventions that follow a fixed schedule or set of rules, JITAIs dynamically adjust the intervention based on real-time data regarding an individual's current state or needs. The intervention can thus continuously evolve and delivers the right type of intervention precisely when it is needed. This adaptive approach aims to optimize its impact on the individual's mental health and well-being. 163
The next challenge of eHealth tools is to implement such tools in (clinical) practice. 164 While eHealth interventions hold significant promise for youth mental health, several challenges can hinder their successful implementation. For example, ensuring the privacy and security of users is crucial. To mitigate privacy risks, during the development of eHealth tools, attention should be paid to the anonymity of user data and adherence to strict data protection regulations, that is, the general data protection regulation. 165 Another challenge is the availability and continuity of technological support. If needed, support should be available for healthcare providers and users, but also continuous updates are needed to maintain the eHealth intervention. 166 Another important aspect of implementation is the target group. eHealth tools developed to be integrated in the clinical context have their own challenges such as the preference of patients and health-care professionals, and legal and ethical considerations. 167 Preventive eHealth tools aimed to be publicly available require a different dissemination strategy and face challenges in adoption and scale-up. 164 This review points to promising directions for effective eHealth interventions. However, the implementation of such tools in different groups remains challenging and requires future research. An eHealth implementation guideline has been developed that can help assess the determinants of successful eHealth intervention prior to the implementation. 166
Conclusion
Most of the 108 reviewed studies, covering 103 eHealth interventions, showed positive effects of eHealth interventions on mental health or well-being in children and adolescents. Specific elements of eHealth interventions that often enhance mental health or well-being include CBT, self-monitoring, a blended approach, involvement of parents or peers and gamification. More research to these potential effective elements and the accumulative effect of specific combinations of different elements, with standardized outcome measures are needed to understand under which circumstances and in which target groups eHealth interventions can be implemented in clinical practice and as preventive tool. With the continuing developments in technology, the development of eHealth interventions is expected to accelerate in the near future.
Key points and relevance
Youth mental health problems are increasing and mental health services are overburdened. eHealth tools can be promising to address mental health problems. Rapid technological progress has led to diverse eHealth interventions. A structured overview of effective eHealth elements through which interventions aim to improve mental health and well-being is lacking. We show elements of eHealth interventions aimed at improving mental health and well-being in children and adolescents aged 10–25 years from clinical and general populations. This review suggests that CBT and self-monitoring as therapeutic principles, blended interventions in combination with face-to-face therapy or the involvement of parents or peers, and gamification elements, such as rewards, can be effective elements of eHealth interventions for children and adolescents.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076241294105 - Supplemental material for Effective elements of eHealth interventions for mental health and well-being in children and adolescents: A systematic review
Supplemental material, sj-docx-1-dhj-10.1177_20552076241294105 for Effective elements of eHealth interventions for mental health and well-being in children and adolescents: A systematic review by Evelien Dietvorst, Lianne P. de Vries, Stephanie van Eijl, Esther Mesman, Jeroen S. Legerstee, Loes Keijsers, Manon H. J. Hillegers and Annabel Vreeker in DIGITAL HEALTH
Supplemental Material
sj-xlsx-2-dhj-10.1177_20552076241294105 - Supplemental material for Effective elements of eHealth interventions for mental health and well-being in children and adolescents: A systematic review
Supplemental material, sj-xlsx-2-dhj-10.1177_20552076241294105 for Effective elements of eHealth interventions for mental health and well-being in children and adolescents: A systematic review by Evelien Dietvorst, Lianne P. de Vries, Stephanie van Eijl, Esther Mesman, Jeroen S. Legerstee, Loes Keijsers, Manon H. J. Hillegers and Annabel Vreeker in DIGITAL HEALTH
Footnotes
Acknowledgements
The authors wish to thank Dr Sabrina (S.T.G.) Meertens-Gunput from the Erasmus MC Medical Library for developing and updating the search strategies. We would like to thank Famke Bos and Maaike van der Eijk for their invaluable contributions in coding the title and abstract, as well as to Kim van den Dool for her assistance in the coding.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
This work is supported by the Sophia Foundation (grant number B18-05). This publication is part of the ‘eHealth junior’ project (with project number [NWA.1292.19.226]) of the NWA research program ‘Research on Routes by Consortia (Onderzoek op Routes door Consortia)’, which is funded by the Netherlands Organization for Scientific Research (NWO). Furthermore, this research is part of the PROTECt ME project funded by Convergence, the alliance between Erasmus Medical Center Rotterdam, Erasmus University Rotterdam and Delft University of Technology.
Consent statement
Ethical approval and informed consent were not applicable for this systematic review as it involved the collection and analysis of data from previously published studies. All data sources were publicly available, and no primary data collection or direct involvement of human participants occurred.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.