
Abstract
Background
In the era of digital health, pharmacy services are rapidly evolving, yet remote service delivery remains legally restricted in South Korea. This study addresses the public perception of pharmacy services, with a particular focus on perceived importance and preferences for face-to-face interactions across the predispensing, dispensing, and postdispensing stages, especially in relation to patient–pharmacist communication.
Methods
A web-based survey was conducted with 1000 South Korean adults to quantify perceived service importance and delivery mode preferences across each service stage. Respondents were categorized into Assertive, Passive, and None groups based on their perceived style of communication with pharmacists.
Results
Participants were classified into Assertive (17.2%), Passive (54.0%), and None (28.8%) communication groups. Pharmacy services were analyzed by stage—predispensing, dispensing, and postdispensing—and perceptions of service importance, actual provision, and preferences for face-to-face delivery varied accordingly. The dispensing stage was consistently rated highest across all measures, and communication style was positively associated with each measure. Prior telemedicine experience was linked to greater openness to remote services, whereas digital health literacy showed no significant association.
Conclusion
Face-to-face interactions remain essential for pharmacy service delivery, particularly during the dispensing and counseling stages. Preferences for delivery methods vary by communication style, underscoring the importance of fostering effective patient–pharmacist communication. To enhance trust, satisfaction, and adherence, future models should integrate digital health technologies with meaningful in-person engagement.
Introduction
In recent years, the rapid integration of digital technologies into healthcare systems has transformed service delivery. Digital transformation harnesses these technologies to enhance healthcare accessibility, efficiency, and patient outcomes.1,2 Community pharmacies, as highly accessible healthcare providers, have also been impacted by this digital shift.3–7 They are expected to offer patient-centered services such as medication reviews and health education, with opportunities to incorporate digital technologies into these services.8,9
Despite South Korea's advanced digital infrastructure, pharmacy services continue to be legally restricted to in-person delivery.10–12 While pharmacy services have traditionally relied on face-to-face interactions, digital health solutions—such as electronic prescriptions, teleconsultations, and mobile applications—have broadened care delivery channels to include remote formats.13–18 However, South Korea remains one of the few Organisation for Economic Co-operation and Development countries where teleconsultations and remote medication dispensing are still prohibited by law, due to factors including stakeholder resistance and unresolved legal or safety concerns.19,20 While temporary measures permitted such services during the COVID-19 pandemic, this allowance was discontinued after the public health emergency ended, 21 though pilot programs are currently exploring pathways for institutionalization.
The introduction of remote service models has raised concerns about the impact on patient–pharmacist relationships.22–24 Face-to-face interactions remain essential for building trust, improving patients’ understanding of their therapy, and encouraging adherence and engagement.25–28 Evidence demonstrates that strong patient–pharmacist communication contributes to better health outcomes, emphasizing the importance of relational continuity and personalized counseling.28–30 However, individuals vary in their communication styles with pharmacists, which may influence how pharmacy services are perceived and delivered. Despite its relevance, limited research has examined how these communication differences shape preferences for service delivery formats.
Given the growing adoption of digital health technologies, this study examines public perceptions and preferences regarding face-to-face versus remote pharmacy dispensing and counseling services in South Korea. It focuses on the role of patient–pharmacist communication across three distinct service stages—predispensing, dispensing, and postdispensing—and how preferences vary by communication style. This study explores public perceptions of pharmacy services in the context of prescription medications and how communication behaviors between patients and pharmacists relate to preferences for face-to-face versus remote service delivery across different service stages.
Materials and methods
Overview
This study is part of a larger project examining the impact of technological advancements on pharmacy services, including both over-the-counter medication provision and prescription dispensing. The current analysis focuses on public perceptions of pharmacy services and preferences for face-to-face versus remote delivery methods in the context of prescription dispensing and counseling. Data was collected through a self-administered web-based survey, which assessed public perceptions and experiences with face-to-face pharmacy services and examined how preferences for delivery methods vary by patient–pharmacist communication style. The survey was conducted from August 29 to September 9, 2024, with technical support from the KopraLab.
Participant recruitment
Participants were South Korean adults aged 19 years or older. A target sample size of 1000 was determined based on a 95% confidence level, a 3.1% margin of error, and a standard deviation of 0.5%. Quota sampling based on sex, age, and region was applied using national census data. A total of 170 quotas were created by combining categories of sex (male and female), age group (20s, 30s, 40s, 50s, and 60 years and older), and residential region (n = 17). Participants were allocated to each quota in proportion to the national population distribution, with the total sample size set at 1000. KopraLab distributed survey invitations to registered panel members until the target number was met. Participants provided informed consent online before completing the questionnaire via a secure web platform. Upon completion, each participant received a $4 voucher. Of the 10,162 invitations sent, 1000 completed responses were obtained, yielding a response rate of 9.8%.
Questionnaires
The questionnaire consisted of five sections: Pharmacy service use, Evaluation of services, Telemedicine experiences, Digital health literacy, and Demographic characteristics. The Pharmacy service use section included items assessing their self-perceived communication style and their perception of the pharmacist's communication style. In the Evaluation of services section, participants were asked about six components involved in prescription dispensing and counseling, categorized into three stages: predispensing (patient identification), dispensing (prescription review and dispensing; medication counseling), and postdispensing (confirmation of medication counseling; handling patient inquiries; delivery of dispensed medications). For five of these components (excluding delivery of dispensed medications), participants rated both the perceived importance and actual provision of each service using a 5-point Likert scale (1 = not important at all; not performed at all, 5 = extremely important; performed very well). Furthermore, for all six components, participants indicated their preferred delivery method for each service 1 : face-to-face only 2 ; remote in limited situations 3 ; remote as a substitutive option; or 4 not sure. The Telemedicine experiences section assessed participants’ prior experience, satisfaction with remote services, and willingness to use them in the future. Digital health literacy was measured using 12 items adapted from a validated tool. 31 These items assessed four key domains: searching for online health information, composing health-related messages, evaluating information credibility, and determining information relevance. Participants rated their ability on each item using a 4-point Likert scale (1 = very difficult; 4 = very easy). Demographic data included sex, age, duration of education, and region of residence. The English-translated questionnaire is provided in Supplementary Material 1.
Except for the items related to health literacy, the questionnaire did not include structured items designed to directly measure specific theoretical constructs; therefore, statistical validity analyses such as factor analysis were not conducted. However, to ensure content validity, relevant previous studies were reviewed, expert consultations were obtained from three professionals (a public health specialist, a social pharmacy researcher, and a licensed pharmacist), and a pilot test was conducted with five members of the general public. Based on data from the main survey, Cronbach's alpha was calculated as follows: 0.864 for the perceived importance items, 0.858 for the actual provision items, and 0.932 for the digital health literacy items. These values indicate a high level of internal consistency across respective scales.
Statistical analyses
Participants were classified into three groups based on their communication styles in community pharmacies. We asked participants to rate both their own communication style (“Self-Perceived Communication”) and their perception of the pharmacist's communication style (“Perceived Pharmacist Communication”) using three categories: “Rarely communicating,” “Passive communication,” and “Assertive communication.” This resulted in a 3 × 3 classification, as detailed in Table 1. For further analysis, these participants were then categorized into three distinct communication groups. The Assertive group (n = 172) included respondents who reported both their self-perceived and the perceived pharmacist communication as “Assertive.” The Passive group (n = 540) consisted of respondents where at least one party engaged in “Passive communication” but neither engaged in “Rarely communicating,” encompassing those with “Passive-Passive” (n = 351), “Passive-Assertive” (n = 39), or “Assertive-Passive” (n = 150) styles. Finally, the None group (n = 288) comprised all remaining respondents, characterized by at least one party engaging in “Rarely communicating,” which includes “Rarely-Rarely” (n = 158), “Rarely-Passive” (n = 74), “Rarely-Assertive” (n = 5), “Passive-Rarely” (n = 44), and “Assertive-Rarely” (n = 7) styles.
Respondents’ perception of communication styles in community pharmacies.

Respondents were classified into three analytical groups based on this table: the Assertive group (n = 172) included those in the “Assertive-Assertive” cell; the Passive group (n = 540) included “Passive-Passive” (n = 351), “Passive-Assertive” (n = 39), and “Assertive-Passive” (n = 150) cells; the None group (n = 288) included all remaining cells where at least one party reported “Rarely communicating.”
Descriptive statistics summarized participant characteristics and mean importance and provision scores across communication groups. Chi-square tests were used for categorical variables, and one-way analysis of variance (ANOVA) or Welch ANOVA was applied to continuous variables as appropriate. Logistic regression identified factors associated with preferences for face-to-face service delivery. Independent variables included gender, age, residential region, duration of education, telemedicine experience, digital health literacy, communication style, overall pharmacy satisfaction, and perceived importance of each service component. Results are presented as adjusted odds ratios (ORs) with 95% confidence intervals (CIs). Statistical significance was defined as p < .05. The Hosmer–Lemeshow test was performed to evaluate model fit.
Results
Characteristics of respondent
Table 2 shows significant differences in respondent characteristics across communication groups. Individuals in the Assertive group were more likely to reside in metropolitan areas (55.8%; p = 0.032) and had a higher proportion of advanced educational attainment (79.7%; p = 0.005). Satisfaction with pharmacy services was substantially higher in the Assertive group (81.4%) than in the None group (24.3%; p < 0.001). Digital health literacy scores were also significantly higher in the Assertive group (mean = 2.91) compared to the None group (2.61; p < 0.001). In addition, prior telemedicine experience was more common among the Assertive group (30.2%) than those in the None group (12.5%; p < 0.001). However, no significant differences were observed in willingness to use telemedicine across the groups (p = 0.395).
Characteristics of respondents across communication groups.
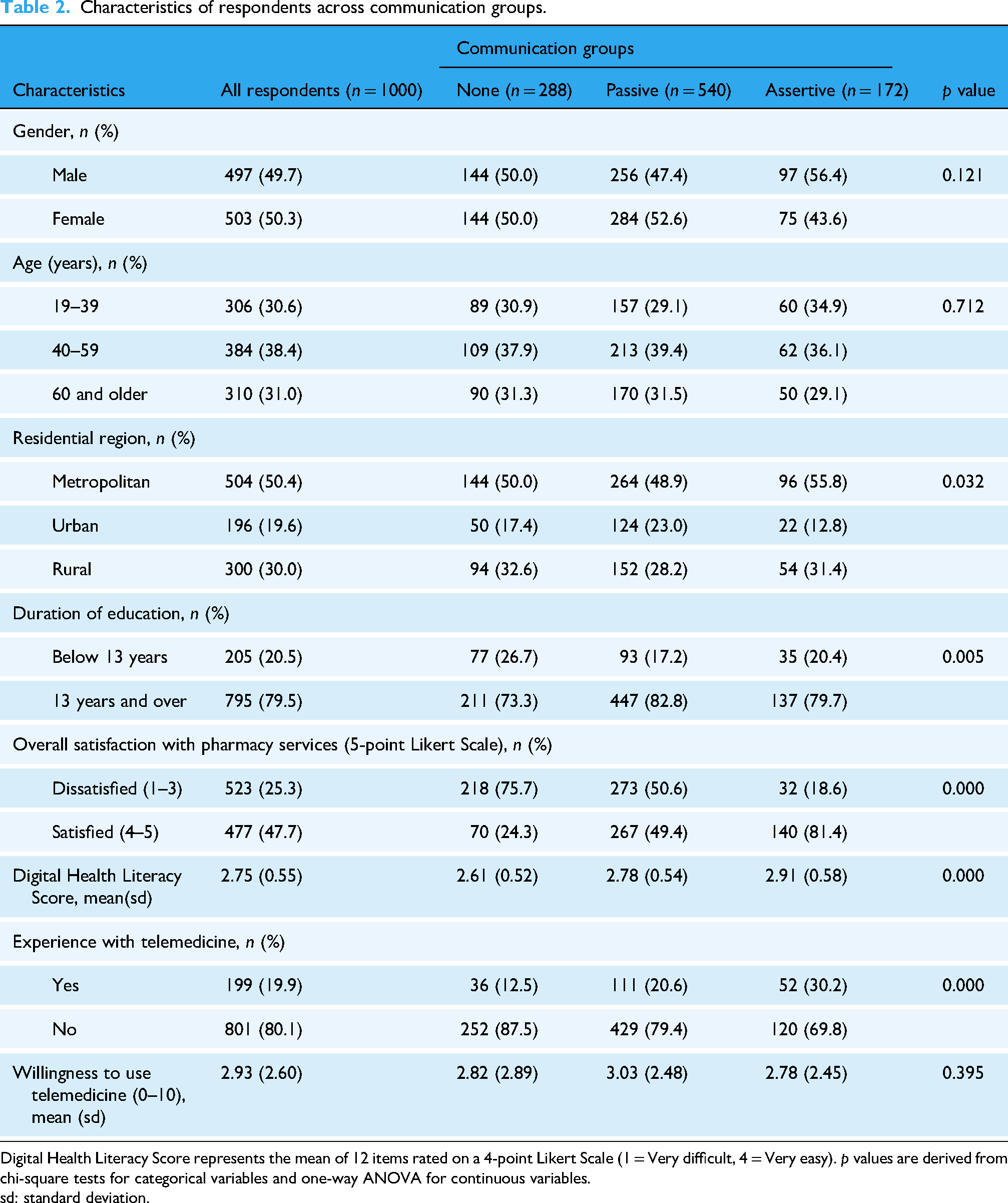
Digital Health Literacy Score represents the mean of 12 items rated on a 4-point Likert Scale (1 = Very difficult, 4 = Very easy). p values are derived from chi-square tests for categorical variables and one-way ANOVA for continuous variables.
sd: standard deviation.
Perceived importance and actual provision of pharmacy services
Table 3 summarizes participants’ ratings of the perceived importance and actual provision of five pharmacy service components. Services in the dispensing stage—namely, prescription review and medication counseling—were consistently rated as the most important. In contrast, services in the predispensing stage (patient identification) and postdispensing stage (confirmation of counseling and handling of patient inquiries) were rated as less important. Participants in the Assertive group assigned higher importance scores across all service components compared to those in the Passive and None groups. Notably, respondents in the None and Passive groups rated pre- and postdispensing services as less important. Regarding actual provision, postdispensing activities—particularly confirmation of counseling and inquiry handling—received the lowest ratings across all groups. The Assertive group reported the smallest gap between perceived importance and actual provision, whereas the Passive and None groups reported larger discrepancies, especially for postdispensing services.
Perceived importance and actual provision of pharmacy services across the three groups.

The “Difference” score was calculated by subtracting the mean score of “Actual Provision” from the mean score of “Perceived Importance” for each service component. P values are based on one-way ANOVA; Welch's ANOVA was applied when Bartlett's test indicated unequal variances.
sd: standard deviation.
Preferred delivery method for pharmacy services
Figure 1 illustrates participants’ preferences for the delivery method of pharmacy services across the predispensing, dispensing, and postdispensing stages. Across all components, participants in the Assertive group were more likely to prefer face-to-face delivery, indicating a clear association between communication style and preference for in-person services. Predispensing services—such as patient identification—had the highest proportion of respondents stating that these services “must be delivered face-to-face.” In contrast, postdispensing services—including confirmation of counseling and medication delivery—were more often considered suitable for remote delivery, underscoring stage-specific variation in service delivery preferences.

Preferred delivery method for pharmacy services by communication group.
Factors associated with preference for face-to-face delivery of pharmacy services
Table 4 presents the results of multivariable logistic regression analyses examining factors associated with preferences for face-to-face delivery across six pharmacy service components. The Hosmer–Lemeshow test indicated satisfactory model fit for all service models. Participants with prior telemedicine experience were significantly more likely to prefer remote delivery for most services, indicating a consistent association between digital experience and openness to remote formats. In contrast, digital health literacy was not significantly associated with delivery preferences after adjusting for other covariates. Communication style showed a significant association with service delivery preferences: participants in the Assertive group were more likely to prefer face-to-face delivery for all services except medication delivery. Perceived importance of each service was also positively associated with face-to-face preference, particularly for prescription review and counseling, although the association was weaker or nonsignificant for follow-up services.
Factors associated with preference for face-to-face delivery of pharmacy services.

*** p < 0.01, ** p < 0.05, * p < 0.1.
Discussion
Principal findings
This study identified several key findings regarding public perceptions of pharmacy services and preferences for face-to-face delivery in community pharmacies amid digital transformation. First, participants were categorized into three communication groups: Assertive (17.2%), Passive (54.0%), and None (28.8%), indicating that the proportion of individuals reporting mutually assertive communication was relatively small. This implies that there is ample room for intervention, and that promoting patient–pharmacist communication could lead to meaningful improvements in service engagement and delivery preferences; these are favorable and desired goals, as effective communication is crucial for building trust, enhancing adherence, and improving health outcomes.28,29,32,33 Second, perceptions of service importance, actual provision, and preferences for face-to-face delivery varied across the three stages. Services in the dispensing stage were consistently rated as the most important and were most preferred for in-person delivery. Communication style was positively associated with all three aspects, suggesting that higher engagement in communication enhances perceived value and preference for face-to-face interactions. Third, prior telemedicine experience was consistently associated with greater openness to remote service delivery, whereas digital health literacy was not a significant factor. These results suggest that direct experience with digital healthcare, rather than general digital competence, plays a more influential role in shaping patient preferences for remote pharmacy services.
Rethinking pharmacy services
These findings underscore the enduring importance of human interaction in pharmacy service delivery, even as digital transformation accelerates. 34 While remote services offer convenience and accessibility for routine tasks, patients continue to value interpersonal contact—especially for services involving clinical judgment and counseling. This is particularly evident in the dispensing stage, which requires nuanced communication and trust-building between patients and pharmacists. Digital tools may be limited in replicating essential relational elements such as empathy, active listening, and personalized guidance. These elements are central to building trust and shaping patient satisfaction, and patients indeed report concerns that digital services can feel “remote and impersonal,” highlighting their value for human interaction.32,35,36
Not all patients experience pharmacy services equally. The observed variation in communication engagement suggests that those with lower engagement may miss out on the depth of counseling needed to support trust and adherence.33,37 This gap may reflect not disinterest, but a form of communication inertia that can be reversed through proactive pharmacist engagement. Therefore, pharmacy practices should aim to foster interaction even among patients who do not actively seek it—particularly those who have never experienced meaningful pharmacist communication. Structured pharmacist-led interventions, personalized reminders, and tailored educational materials can help encourage patient questions and participation. Protocols that promote proactive outreach and standardized counseling practices can reduce disparities in service engagement and help bridge the gap between perceived importance and actual provision. Such strategies may create a virtuous cycle that strengthens the pharmacy service environment and improves patient outcomes.32,37
In addition, the undervaluation and limited provision of pre- and postdispensing services reveal blind spots in pharmacy care. Although tasks such as patient identification and follow-up counseling play critical roles in medication safety and continuity of care, they are often overlooked. Strengthening these components through standardized education and systematic follow-up protocols is essential. Rather than replacing face-to-face counseling, digital tools should be integrated as complementary support that extends pharmacist care beyond the in-person encounter. Hybrid service models that combine in-person counseling with digital follow-up tools represent a promising approach to sustaining therapeutic continuity and reinforcing key messages after patients leave the pharmacy.38–41
The strong association between prior telemedicine experience and openness to remote pharmacy services—despite the lack of influence from general digital literacy—highlights the role of direct, hands-on experience in shaping acceptance. Knowledge alone is insufficient; patients require repeated, positive exposure to build trust in the convenience, safety, and effectiveness of digital healthcare services. 23 Therefore, digital pharmacy service strategies should incorporate experiential learning opportunities, including pilot programs and simulated encounters. Practice-based digital training tailored to older adults and digitally marginalized populations will be critical to bridging the digital divide and ensuring equitable access to digital pharmacy services.42–44
Policy implications
As South Korea considers broader implementation of telepharmacy and digital health strategies, a balanced and inclusive approach is essential. Investment in digital infrastructure must be accompanied by efforts to strengthen pharmacists’ communication competencies and capacity for patient-centered care. Tailored strategies are needed to engage less communicative patients, while preserving trust-based, personalized care for those who actively engage. Such efforts can enhance adherence, improve clinical outcomes, and support the sustainable evolution of pharmacy services in the digital era. 25
Ultimately, while digital innovation holds great promise for enhancing efficiency and accessibility, community pharmacies must not lose sight of the irreplaceable value of human connection. 45 Although this study was conducted in South Korea, its implications are globally relevant. Health systems worldwide face similar challenges in integrating digital tools into pharmacy care without compromising trust and patient engagement. Strengthening pharmacists’ communication skills, promoting proactive patient interaction, and ensuring that digital solutions function as complements—not substitutes—for human care are universally important. In particular, low-resource settings and regions with significant digital disparities should prioritize scalable, inclusive approaches that reinforce trust, access, and continuity of care through both community-based and digital strategies. These approaches—adaptable across diverse healthcare systems and regulatory environments—can contribute to more sustainable, inclusive, and patient-centered pharmacy care globally. 45
Study limitations
This study has several limitations that should be acknowledged. First, the survey was conducted using an online panel, which may introduce selection bias, as participants are likely to possess higher levels of digital literacy compared to the general population. Therefore, caution is warranted when generalizing these findings to all pharmacy users, particularly older adults or individuals residing in rural areas with limited internet access or lower digital literacy. Second, the study relied on self-reported perceptions and preferences, which may be subject to response biases. Future research could incorporate objective data on actual pharmacy interactions or employ observational methods to strengthen validity. Third, given the cross-sectional design of the survey, causal relationships between communication styles and service delivery preferences cannot be established. Longitudinal or interventional studies are recommended to explore causal pathways and monitor changes over time. Finally, this study was conducted in the context of South Korea, where legal and cultural factors may shape public perceptions of pharmacy services. Comparative research across countries with differing regulatory environments regarding telepharmacy and digital health could provide valuable insights into these dynamics.
Conclusions
Face-to-face interactions remain essential to the delivery of pharmacy services, particularly during counseling and dispensing stages. Variations in service delivery preferences based on communication styles highlight the critical role of patient–pharmacist engagement. Enhancing communication, especially among less engaged patients, is vital to closing service gaps and promoting equitable access. Future care models should strive to balance digital innovation with meaningful in-person contact to build trust, enhance patient satisfaction, and improve medication adherence. As pharmacy practice continues to evolve globally, implementing tailored strategies that integrate technological advancement while preserving human connection will be key to delivering sustainable and patient-centered pharmacy services.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076251361630 - Supplemental material for Public perceptions of pharmacy services: Perceived importance and face-to-face preference across service stages in the era of digital health
Supplemental material, sj-docx-1-dhj-10.1177_20552076251361630 for Public perceptions of pharmacy services: Perceived importance and face-to-face preference across service stages in the era of digital health by Dong-Wook Yang, Youran Noh and Kyung-Bok Son in DIGITAL HEALTH
Footnotes
Ethics considerations and consent to participate
The study protocol was approved by the SungKyunKwan University Institutional Review Board (SKKU 2024-08-021), and conducted in accordance with the principles of the 1964 Helsinki Declaration and its later amendments, or comparable ethical standards.
Contributorship
DY designed the analysis, performed the analysis, and wrote the manuscript. YN designed the analysis and wrote the manuscript. KS conceived and designed the analysis, performed the analysis, and wrote the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by the National Research Foundation of South Korea (NRF- 2022R1F1A1071338).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
Data supporting the findings of this study are available from the corresponding author upon reasonable request.
Guarantor
K-BS.
Informed consent
Informed consent was electronically obtained from all participants.
Supplementary material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.