
Abstract
Background
Artificial intelligence (AI) offers transformative potential in healthcare, yet its adoption is hindered by cultural, organizational, and technological barriers, and little is known about their actual use in clinical practice. The aim of this study was to explore current trends in the adoption of AI applications across healthcare organizations in Lombardy, Italy.
Methods
This is a survey study that targeted public and private healthcare organizations in Lombardy and conducted between December 2023 and February 2024, with follow-ups between May and June 2024. It included three sections with up to 22 questions: mapping of clinical AI applications, organizational governance of AI, and perceived adoption barriers.
Results
Among the 46 responding organizations, 56 AI applications were identified. Most applications focused on analyzing images or structured health data, and supported diagnostic, prognostic, or treatment optimization activities. Routinely used applications were Conformité Européenne-marked, with radiology being the main clinical area of use. Three distinct approaches emerged. While most organizations (57%) have not yet adopted AI applications, among adopters, 13% are developing AI tools, while 30% exclusively purchase commercial solutions.
Conclusions
There is considerable variability in both the types and stages of AI applications adopted in clinical practice by healthcare organizations in Lombardy. In terms of functions, most implementations support diagnostic and prognostic tasks, with strong emphasis on imaging-based tools. Regarding innovation strategies, varying approaches, ranging from exclusively purchasing AI applications to hybrid models that include in-house development, were observed. These findings support broader ecosystem efforts to understand and guide AI implementation in healthcare.
Keywords
Introduction
Background
The potential of artificial intelligence (AI) in healthcare has grown exponentially in recent years, 1 driven by advances in the ability to collect, aggregate, and analyze vast amounts of data. 2 Through its ability to interpret external data, learn from them, and use those learnings to achieve specific goals and tasks through flexible adaptation, 3 AI enables machines to replicate complex human skills and support decision-making processes that were traditionally the exclusive domain of humans. A major subset of AI, machine learning (ML), leverages large datasets to train algorithms that may identify unique or new combinations of features and weights starting from first principles.4,5
While the potential applications of AI in healthcare span multiple areas of activity, 6 numerous compelling examples demonstrate its transformative role in clinical practice. Within this context, AI can play a crucial role in prognostic activities, helping predict disease progression and patient outcomes, as already demonstrated by ML models used to assess mortality risks in hospitalized COVID-19 patients through the analysis of clinical and laboratory data. 7 As for diagnostics, AI enhances image analysis (e.g., in radiology, dermatology, ophthalmology, and pathology) and signal interpretation (e.g., electrocardiograms, audiology, and electroencephalograms). 8 Furthermore, AI can aid treatment decisions, by integrating and contextualizing test results with other clinical data to streamline workflows, ultimately enhancing decision-making.9,10
Despite the transformative potential, significant challenges often impede or delay the practical implementation of such applications in routine settings, a phenomenon known as the “implementation gap.”11,12 Previous reviews have investigated the implementation challenges of AI. For instance, Tricco and colleagues examined the strategies employed to integrate ML tools into hospital settings, 13 while Chomutare and colleagues investigated barriers and facilitators to ML implementation based on empirical studies. 14 More recently, Preti et al. conducted a systematic review of empirical studies documenting implemented cases of ML in healthcare organizations, offering insights into the relevant dimensions of ML implementation in healthcare.15,16 These reviews are useful because they confirm that real-world cases of ML implementation do exist and highlight the (albeit rare) strategies adopted to facilitate their uptake, including the cultural, organizational, and technological challenges encountered in the process, as well as the actions undertaken to address them. However, broader cross-sectional analyses in specific territorial contexts remain largely unexplored, limiting a systematic understanding of how widespread and rooted these adoption processes are. Such an approach would also help identify emergent strategies that, while not yet well-documented, are shaping the diffusion of AI in healthcare systems.
Objectives
The overarching aim of this work was to explore current trends in the adoption of AI applications in clinical practice through a survey distributed across healthcare organizations in Lombardy, the most populous Italian region. In this setting, the study had two specific objectives:
to analyze the current state of AI adoption in healthcare organizations, by mapping available AI applications in clinical practice, exploring the strategic actions already in place to govern the transition toward AI, and investigating adoption challenges, either perceived or experienced; to identify different approaches to AI adoption observed in the study context, with the ambition to contribute to the broader discussion on viable strategies for implementing AI in clinical practice.
This exploration is relevant from multiple perspectives: clinically, as it helps identify which areas of care are currently benefiting most from AI integration and where further development may be needed; organizationally, as it provides insights that can inform strategic planning and policy design to support effective and scalable AI implementation; and socially, as it sheds light on governance challenges and the broader implications of AI use for healthcare professionals and patient communities.
Methods
Study design
A survey design was chosen as it enabled the efficient collection of self-reported data from a relatively broad sample of respondents and was well suited to gathering standardized information on AI adoption. This study is reported in accordance with the Consensus-Based Checklist for Reporting of Survey Studies (CROSS) 17 guidelines. The completed CROSS checklist, indicating where each item is addressed in the manuscript, is provided in Supplemental Material 1.
Data collection method
Survey development was informed by a prior literature review by Preti et al.,15,16 which examined the characteristics of ML applications and their implementation processes in clinical practice. The initial draft of the survey was prepared and subsequently refined through multiple iterative review rounds involving the entire research team. The survey draft was shared in advance with the head of the Unità Organizzativa Sistemi Informativi e Sanità Digitale of the Lombardy Region and the head of Assolombarda's Healthcare Group (Gruppo Sanità), both identified as knowledgeable stakeholders. This preliminary step aimed to gather informal feedback prior to large-scale dissemination.
Considering the target respondents, the survey was conducted in Italian. The survey was composed of up to 22 questions (including categorical, Likert scales, and free-text fields), structured into three sections:
Mapping of AI applications in clinical practice: This section extensively mapped all AI applications currently available, distinguishing those already used in clinical practice from those under development or testing. For each application, detailed information was collected, including features such as the type of data processed (structured data, unstructured data, images, or text), the targeted clinical activity (e.g., prognosis, diagnosis, treatment, workflow administration), and the therapeutic area or adopting unit. Organizational governance of AI: This section explored the presence of formalized or informal roles dedicated to the implementation of AI, the establishment of organizational units or structures for AI, the provision of educational sessions (covering broad AI topics or specific applications), partnerships with external stakeholders such as academic centers, technology providers, or other healthcare organizations, and the allocation of financial resources toward AI. Perceived barriers to AI adoption: This section identified key challenges associated with AI adoption, including regulatory issues (e.g., medical liability, privacy concerns), available evidence on clinical efficacy or organizational benefits, cultural factors (e.g., trust and openness to innovation), and IT-related considerations (e.g., interoperability, data management). Barriers were rated on a 5-point Likert scale, with higher scores indicating greater perceived barriers.
Table 1 reports at a high level the items of each section of the questionnaire, while the full version of the survey items is available in Supplemental Material 2.
Survey items, by section.

AI: artificial intelligence; CE: Conformité Européenne; IT: information technology.
Definitions of key concepts in the context of this study
In the survey, AI was defined as hardware and software systems equipped with human-like capabilities (e.g., learning, adapting, reasoning, and planning), including solutions dedicated to natural language processing, multimedia content, and data that can guide user decisions or autonomously initiate actions based on the extracted information. The survey generically referred to AI to ensure that respondents could associate the term with any AI-related concept they had in mind, without being constrained by technical distinctions. For consistency, we adopt the same broad and inclusive use of the term AI throughout this paper, without differentiating between its specific subfields.
Furthermore, adoption, as conceptualized in this work, can be characterized through three progressive stages, adapted based on Aaron et al. 18 The first stage, development and experimentation, includes internal development, clinical studies, and proof-of-concept projects. The second stage, piloting, refers to the testing and refinement of applications (particularly commercially available solutions) during a preparatory phase before their operational use. Finally, routine use marks the regular and consistent integration of these technologies into clinical practice, including the preliminary set-up necessary for externally purchased applications. In the present study, all these stages of adoption are considered to provide a comprehensive analysis of implementation processes.
Sample characteristics
The survey targeted both public and private healthcare organizations in Lombardy. Notably, the Italian healthcare system is a regionally based national health service, with each region holding administrative autonomy over the organization and provision of healthcare services. 19 Lombardy was chosen as the study setting being one of the largest regions by territory and the most densely populated, 20 consistently leading in technological and healthcare innovation.21–23 Its diverse landscape of healthcare providers, which includes highly specialized research hospitals, and its strong tradition of public-private mix in healthcare service delivery, 24 creates fertile ground for observing emerging trends in the uptake of AI. Specifically, all 41 public healthcare organizations were invited to participate. These include organizations that deliver health and social care services (Aziende Socio Sanitarie Territoriali, ASST), organizations recognized for their excellence in care and research (Istituti di Ricovero e Cura a Carattere Scientifico, IRCCS), and local health protection authorities (Agenzie di Tutela della Salute, ATS). As for private healthcare organizations, all members of the healthcare group of the Regional Trade Association Assolombarda, primarily hospitals, were contacted. This sample includes accredited hospital groups, independent IRCCS (not affiliated with larger groups), private hospitals, outpatient healthcare facilities, and diagnostic centers, encompassing the vast majority of private healthcare organizations in the region and representing the sector as a whole. Respondents from private groups could flexibly opt to complete a questionnaire for each hospital facility, for aggregated territorial groupings, or to provide a single consolidated response for the entire group. More details on the main types of healthcare organizations operating in Lombardy are provided in Supplemental Material 3.
The survey specifically targeted Chief Information Officers (CIOs) or the heads of the Information Systems Unit within these organizations, ensuring that responses were provided by individuals with direct oversight and expertise at the intersection between healthcare technology adoption and health information systems.
Survey administration
The survey was administered between December 2023 and February 2024 via the Qualtrics XM© platform, allowing for legislative-compliant data collection and management. The survey was disseminated via email by the Information Systems and Digital Health Unit (Unità Organizzativa Sistemi Informativi e Sanità Digitale) of the Lombardy Welfare Directorate for public organizations, and by the healthcare group (Gruppo Sanità) of Assolombarda for private organizations. As the survey was nominative and distributed to a single designated contact person (the CIO or the heads of the Information Systems Unit) within each organization, the risk of multiple participation was inherently prevented, with only one response expected from each center. To encourage participation, a follow-up email was sent as a recall. As a final step, to ensure clarity and consistency across responses, individual follow-ups were carried out via phone or email between May and June 2024, ultimately enhancing the overall reliability of the data collected.
Ethical considerations
The survey was granted ethical approval by Bocconi University's Institutional Review Board. Informed consent was presented and obtained from each study participant. While survey respondents were not anonymous since the questionnaire was specifically addressed to the CIO of each participating organization, the collected data were subsequently treated anonymously for analysis and reporting purposes.
Data analysis
Data analysis was performed using both Excel and Stata (version 18). For the survey questions, the distribution of responses was noted, using tables where relevant. First, an overview of respondents’ profiles is provided. Available AI applications are then illustrated at an aggregated level. After that, responses are clustered based on both the current availability (or lack thereof) of AI applications and the mode of adoption, examining the organizational initiatives on AI, and the adoption barriers. For adoption barriers, we used chi-square tests to compare differences across groups and detect potential differences in categorical responses across subgroups. Mean values, standard errors, and confidence intervals are reported. Statistical significance was set at p < 0.05. Results are purely observational and should be interpreted narratively.
Results
Respondents characteristics
Overall, 46 responses from both public and private healthcare organizations were collected, representing a significant share of Lombardy's healthcare system in terms of institutional nature (i.e., public and private organizations), institutional mission (i.e., health service delivery, excellence in research), and geographic coverage.
In terms of respondents’ profile, the vast majority of respondents (40 out of 46, 87%) were CIOs, while the remainder (6/46, 13%) reported holding other senior roles, such as Head of Clinical Engineering or similar positions.
In terms of institutional nature, 31 out of 41 public providers participated, resulting in an overall response rate above 75%, with similar rates across subgroups of participants: 21 out of 27 ASST (78%), 4 out of 6 public IRCCS (67%), and 6 out of 8 ATS (75%). Among private organizations, 15 responses were collected, representing over 50% of private healthcare groups and facilities in Lombardy by size and revenue. Most responses came from organizations within hospital groups, including four private hospitals and eight private IRCCS. The remaining responses came from accredited outpatient ambulatories and independent private hospitals. Table 2 summarizes the respondents’ profiles.
Overview of respondents by institutional nature and mission.

Mapping of AI applications in clinical practice
A total of 56 AI applications from 20 adopting organizations (20/46, 43%) were identified through the survey, representing diverse stages of adoption. Among these, 24 applications were still under development, either independently or jointly with technology providers (24/56, 43%), 20 were available for use in routine clinical practice or in the set-up phase (20/56, 36%), and 12 were undergoing piloting and experimentation (12/56, 21%).
Most applications supported diagnostic (30/56, 54%) or prognostic activities (27/56, 48%), with a smaller proportion focused on treatment optimization (6/56, 11%). Regarding their technical functioning, most applications processed images and signs (42/56, 75%), followed by the analysis of structured health data, such as electronic health records or personalized clinical-therapeutic pathways (26/56, 46%). Other functionalities included the analysis of patient-reported data, such as telemonitoring inputs (11/56, 20%), text analysis (8/56, 14%), and miscellaneous functions (5/56, 9%).
In terms of integration with existing IT systems, stand-alone applications accounted for the largest share (23/56, 41%), followed by those integrated with the organization's information systems (18/56, 32%) or paired with a medical device (15/56, 27%). The development processes varied, with most applications being developed by external technology providers (34/56, 60%). Internal development and joint efforts with technology providers each accounted for 11 applications (11/56, 20%). A total of 22 applications (22/56, 39%), primarily commercially available algorithms, had obtained the Conformité Européenne (CE) mark at the time of survey administration.
Finally, the clinical areas where these applications were employed showed a strong prevalence in radiology (17/56, 30%), with oncology and diabetology also being notable areas of use, each with five applications (5/56, 9%). This distribution highlights the predominance of AI in imaging and data-intensive specialties and prognostic applications is more likely to be in a development stage, whereas diagnostic applications—often in radiology—are more commonly in routine use (Figure 1).

Sankey diagram showing the flow between clinical areas, clinical use activities, and adoption levels.
Distinct pathways to AI adoption in healthcare organizations
The aggregated analysis of AI applications’ availability and modes of adoption allowed us to identify three distinct groups of organizations, corresponding to two strategic approaches to AI adoption: adopters engaging in independent or joint development of AI applications; adopters who only purchase commercially available AI applications; nonadopters.
Group 1: Adopters engaging in independent or joint development of AI applications
The first group includes six AI adopters (6/46, 13%) involved in the internal development of applications, either independently or with the support of external partners. These organizations have similar profiles in terms of institutional nature and mission, as five (5/6, 83%) of them are organizations recognized for their excellence in care and research (IRCCS), four of which are private.
In this group, 27 AI applications were identified in total, nearly all of which were in the development phase (22/27, 81%). Among these 22 applications, most were designed for prognostic use (17/22, 77%), while the remainder served diagnostic purposes (2/22, 9%%) or aimed to optimize treatment (3/22, 14%). Five applications were available for routine use (5/27, 19%), typically jointly developed by healthcare companies and external technology providers. Notably, no exclusively internally developed AI application was identified as having reached full implementation. The most represented disciplines included physical and rehabilitative medicine and neurology, de facto reflecting the areas of specialization of the adopting organizations, followed by oncology, laboratory medicine, and diabetology. As these applications were still under development, none had been CE-marked.
In terms of AI governance, this is the only group where formal organizational structures, either AI-specific or innovation-oriented, were established to manage AI-related projects (4/6, 67%). Regarding training activities, only two organizations reported organizing general AI training initiatives (2/6, 33%), while three offered training specific to individual AI applications (3/6, 50%).
Collaboration and partnership agreements with external institutions were widespread within this group (5/6, 83%), such as with academic entities and technology providers. Examples of the former involve joint management of development centers, with contributions from university-affiliated personnel. Examples of the latter primarily address resource and expertise gaps within the company and include sharing data, clinical knowledge, organizational structures, and specialized AI technical personnel.
Group 2: Adopters who only purchase commercially available AI applications
The second group includes 14 organizations (14/46, 30%) that exclusively purchased commercially available AI applications developed by technology providers. Of these, nine (9/14, 64%) were public organizations (eight ASST, one IRCCS), while the remaining five organizations were private entities, including two IRCCSs, two ambulatory groups, and one private hospital.
Overall, 29 AI applications at various stages of clinical practice adoption were identified. Being commercially available, most applications were CE-marked (22/29, 76%). The most common clinical areas of application were radiology (including neuroradiology and interventional radiology), digestive endoscopy, metabolic diseases, and cardiology. Of the total applications, the majority (17/29, 59%) were already used in routine practice, or in a set-up phase before full deployment. Among the AI applications in routine use, the majority were integrated within a medical device and supported diagnostic activities (12/17, 71%), while prognostic applications (4/17, 24%) or treatment optimization (1/, 6%) applications were less frequent.
In terms of governance structures, no formal structures responsible for AI-related projects were identified; instead, only informal organizational initiatives were mapped, involving various professionals, including personnel from information systems or clinical engineering departments, as well as clinicians with a particular interest or expertise in AI (9/14, 64%). As for training initiatives, three organizations (3/14, 21%) mentioned general AI training sessions, while seven (7/14, 50%) provided training focused on specific AI applications. Collaboration agreements with external institutions include partnerships with technology providers (3/14, 21%), academic institutions (2/14, 14%), and other public healthcare organizations (1/14, 7%) and could involve, for instance, the establishment of joint research centers with an academic institution, or the conduct of clinical experimentations to inform subsequent AI application adoption.
Group 3: Nonadopters
The third group includes organizations that reported not having adopted any AI applications in clinical settings at the time of the survey. This group is the largest, comprising 26 organizations (26/46, 57%). Of these, 20 are public (20/26, 77% of the group; 20/31, 65% of participating public organizations), namely 12 ASST, six ATS, and two public IRCCS. The private organizations (6/26, 23% of the group; 6/15, 40% of participating private healthcare organizations) include four accredited private hospitals and two private IRCCS.
Within this group, organizational initiatives supporting the governance and implementation of AI were sporadic. Only seven organizations (7/26, 27%) reported informal organizational measures, like the establishment of multidisciplinary internal working groups on AI. Similarly, training initiatives were rare (7/26, 27%) and primarily focused on specific areas of application. Lastly, eight organizations reported collaborations with external partners on projects for the development or testing of clinical applications, which could lead to their future adoption. Table 3 provides a summary view of the identified approaches to AI adoption.
Synthesis view of survey questions (selection), by group of respondents.
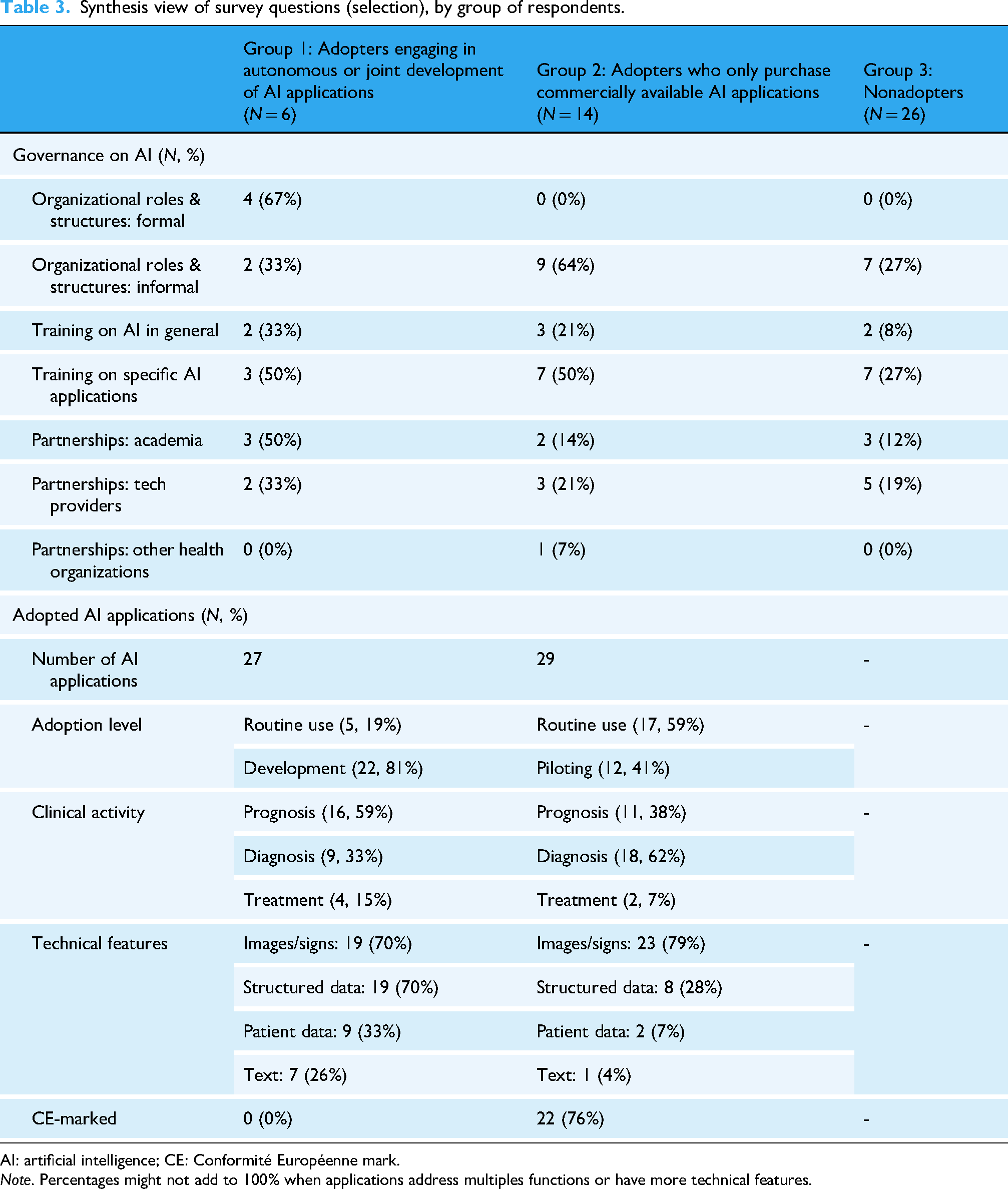
AI: artificial intelligence; CE: Conformité Européenne mark.
Note. Percentages might not add to 100% when applications address multiples functions or have more technical features.
Perceived barriers to AI adoption
Lastly, the third and final section of the survey explored respondents’ perceptions of 11 potential barriers to AI adoption, which were identified and shortlisted based on a prior literature review.15,16 Respondents were asked to rate the relevance of each barrier on a 1–5 Likert scale. Table 4 summarizes the perceived barriers to AI adoption across respondent groups to highlight differences among organizations engaged in AI development (group 1), those purchasing commercial AI solutions (group 2), and nonadopters (group 3).
Perceived barriers to AI adoption, by group.

AI: artificial intelligence; CI: confidence interval; SE: standard error.
Note. Differences were tested using Chi-square tests. Statistical significance was set at p < 0.05. A star system is used to indicate different significance levels: *p < 0.05; **p < 0.01; ***p < 0.001.
For organizations engaging in independent or joint development of AI applications (group 1), the highest-ranked barrier was privacy concerns (mean 4.50; 95% CI 3.21–5.00). We also found that data management, interoperability, and reimbursement and financial incentives were reported to be significantly higher barriers compared to the other two groups, based on chi-square tests, with p-values below 5%. In contrast, the lowest-ranked barrier was corporate culture (2.50; 1.05–3.95).
Organizations that exclusively purchase commercially available AI applications (group 2) ranked corporate culture (3.57; 2.98–4.16) as the most significant barrier, while the least critical challenge was reimbursement and financial incentives (2.71; 2.19–3.24).
Lastly, for nonadopters (group 3), the highest-ranked barrier was the lack of skilled personnel (3.38; 2.90–3.87). In contrast, the lowest-ranked barrier was the availability of evidence on organizational advantages associated with AI (2.65; 2.20–3.11).
Discussion
This study offers new insights on the landscape of AI adoption in clinical practice, providing a detailed mapping of AI applications available in Lombardy, and revealing diverse implementation approaches adopted by healthcare organizations. By exploring how different types of AI applications (externally purchased vs internally developed) entail different implications for their implementation in routine practice, this study contributes to advancing knowledge on the organizational arrangements that surround the adoption of AI through an in-depth analysis of healthcare organizations in the chosen study setting.
The adoption of AI applications in healthcare organizations remains a rapidly evolving field, with limited survey studies mapping system-wide implementation patterns and strategies. Previous studies of national or regional trends on the adoption of AI applications in clinical settings are scarce and offer only limited insights on the associated implications at the organizational level. For example, a study by Cadamuro and colleagues explored AI adoption in laboratory medicine across Europe, highlighting the growing use of AI in diagnostic workflows, particularly in pathology and clinical chemistry, while also identifying key challenges such as data standardization and regulatory compliance. 25 Another study analyzed the adoption of AI within hospitals in the United States in 2022, noting significant disparities based on hospital size and resource availability, with larger hospitals being more likely to deploy AI-driven tools. 26 While our study also confirms variations in AI adoption across healthcare organizations, the estimated adoption rates in Lombardy appear substantially higher than those reported in the US sample from 2022, with 46.5% of healthcare organizations in our study reporting some sort of adoption of AI in clinical practice, compared to 18.7% in the US study. Although the two studies differ in sampling and methodology, they provide valuable cross-sectional estimates that, if examined longitudinally, can offer powerful insights into AI adoption trends, which are widely expected to evolve rapidly. At the same time, new (yet already established) emerging trends in AI, like the use of generative AI, 27 are likely to further influence future adoption pathways.
The variability patterns extended to the typologies of AI applications currently adopted in clinical practice by healthcare organizations in Lombardy. Notably, among commercially available CE-marked solutions, no respondents mentioned the adoption of the same AI application, suggesting that adoption patterns remain scattered and highly diversified, even within a relatively uniform implementation setting, as is Lombardy. This variability observed aligns with recent reviews of empirical studies on real-world implemented ML applications, which emphasized the diversity of use cases across medical fields and clinical workflow activities.13–15 In Lombardy, identified applications primarily supported diagnosis, prognosis, and, to a lesser extent, treatment optimization. A strong emphasis was observed on diagnostic imaging–based applications, particularly in radiology, possibly reflecting the widespread availability of commercially developed, approved AI solutions in this field. 28 Prognostic applications, designed to enable the timely detection of at-risk situations, were equally common. However, unlike previous studies that reported a proliferation of available AI applications for sepsis management, 29 we found no such example in our sample. Instead, AI solutions for prognosis prediction were primarily focused on chronic conditions such as diabetes and cardiovascular diseases. Interestingly, differences in the type of AI applications (diagnostic vs. prognostic) seemed to align with the adoption approach of healthcare organizations. In particular, prognostic applications were more frequently observed among adopters engaged in the independent or joint development of AI applications (Group 1). This might be explained by the nature of prognostic tools, which often rely on the analysis of internal longitudinal datasets and predictive modeling tailored to specific patient populations or care processes. Conversely, diagnostic applications were more commonly reported by adopters who only purchase commercially available AI applications (Group 2), likely reflecting that these applications, especially those used in imaging, are typically CE-marked and more readily available on the market. This trend suggests that the availability and type of data, along with regulatory considerations, may influence the nature of AI applications adopted or developed by different organizations. Nonetheless, this interpretation remains exploratory, and further research is needed to confirm these considerations and better understand the underlying drivers of AI adoption strategies across different use cases.
This study expands on prior work by examining not only the extent of AI adoption, but also institutional priorities, available expertise, and AI governance at the organizational level. Our analysis highlights that AI applications are often introduced before formal governance structures or organizational strategies are in place. While adoption levels varied, informal initiatives, such as clinicians’ involvement in AI projects, were sometimes present, alongside more structured approaches, like dedicated AI units, though these remained rare and more typical of institutes with a research attitude.
The analysis of implementation barriers provides novel insights into how healthcare organizations perceive the challenges of AI adoption. Notably, organizations developing AI solutions internally or through partnerships reported higher concerns regarding regulatory and technical barriers, whereas those purchasing AI applications perceived organizational culture and clinical validation as more relevant challenges. Expectedly, nonadopters often perceived implementation barriers as more prominent compared to AI adopters. Our findings align with several themes identified in the literature on AI implementation barriers, as emerged from both studies documenting the perspectives of healthcare professionals and real-world implementation cases. As for the former, Hogg et al. highlighted regulatory concerns, data interoperability, and trust in AI as critical barriers across multiple stakeholders. 30 Similarly, our study found interoperability challenges and privacy concerns to be key obstacles for organizations involved in AI development, although trust in AI was perceived as a lesser challenge, particularly among adopters. Furthermore, a qualitative study with healthcare leaders in Sweden found that organizational readiness, resistance to change, and uncertainties regarding AI's long-term impact were major challenges to implementation. 31 Our findings reinforce the role of organizational culture as a barrier, particularly for organizations purchasing AI solutions, whereas for those actively contributing to the development of AI solutions financial and technical barriers seem to play a more central role.
Looking at studies analyzing barriers experienced in real-world implementation cases, Preti et al. identified financial constraints, lack of skilled personnel, and the complexity of integrating AI into existing workflows as major barriers, 15 which are consistent with our study, particularly in the perception of organizations that also engage in AI application development. Additionally, concerns regarding clinical validation and medical liability, which we observed in our findings among organizations purchasing AI solutions, were also emphasized in prior research. 14
While our results generally align with previous implementation barrier studies, we provide a more structured comparison of perceived implementation challenges based on different types of adopters and AI adoption maturity, allowing for a more nuanced understanding of the specific barriers faced by different actors for different types of AI applications.
Alternative approaches to AI adoption
This study inductively identified three groups corresponding to two alternative approaches to AI implementation. While the majority of respondents have yet to adopt clinical AI applications (26/46, 57%; nonadopter group), the remaining organizations can be grouped into two distinct categories: a core set of organizations engaged in independent or joint development of AI applications with technology providers (6/46, 13%), and another group implementing solutions solely through the procurement of AI technologies available in the commercial sector (14/46, 30%). These observed approaches are partly shaped by the institutional nature of the organizations, with implications for internal organizational decisions and their relationships with other players in the extended ecosystem. This variability in implementation strategies highlights that AI adoption is not a uniform process but rather one that is deeply influenced by each organization's specific context, resources, and strategic priorities, confirming that a one-size-fits-all approach is unlikely to be effective. 32
Organizations pursuing independent or joint development require a broad spectrum of competencies and resources, a model more typical of organizations with an emphasis on research. Unsurprisingly, respondents in this group have demonstrated a higher prevalence of structured organizational interventions, such as the establishment of specific roles and dedicated units with allocated resources. This aligns with findings from other studies, which have identified local AI champions as important predictors for the successful implementation of AI algorithms. 33 However, this pathway may entail longer lead times for moving from ideation to implementation, with only two of the joint-developed applications identified in this study being currently used in routine clinical practice. Despite these delays, the extended development timeline is likely to be offset by the enhanced adaptability of these solutions to their intended contexts and patient case mixes. Notably, the need to adapt AI systems to local implementation settings emerged from prior studies on clinical AI15,34,35 and is recognized as a key implementation domain in several established implementation science frameworks.36,37
Conversely, the procurement of existing solutions via dedicated purchasing processes appears characterized by distinct organizational approaches. While this strategy seems to demand fewer upfront organizational adjustments (none of the respondents in this group mentioned the establishment of structured organizational roles or units), it nevertheless requires the development of specialized internal competencies, necessary for conducting the preliminary scouting process of commercially available solutions, including make-or-buy decisions. While this approach may enable faster implementation overall, it requires careful management of the professional and organizational dynamics associated with integrating such complex external technologies. For instance, a recent study identified relevant factors in the procurement of AI applications, such as the clinical rationale for starting the acquisition process, ethical issues to be considered beforehand, or the feasibility of integrating such tools in existing workflows, to name a few. 38 When purchasing AI solutions, another element of complexity observed is the external pressures experienced by organizations through frequent approaches by vendors. 39 Similarly, the reputation of the technology provider may play a significant role, as the (perceived) complexity and opacity of AI applications introduce unique challenges in establishing trust, particularly crucial when selecting and integrating commercially available solutions. 15
Lastly, for organizations currently lagging behind in terms of AI-driven innovation, while both adoption strategies remain viable in principle, our analysis revealed that independent or joint development seems to align more closely with a research-focused mission, which involves a unique set of organizational elements that may not be easily replicated across all contexts. In any case, ensuring a smooth and effective implementation of AI into clinical practice requires a clear understanding of an organization's unique needs and capabilities. 32
Compared to the findings of the aforementioned study on US hospitals, 26 which found that large teaching hospitals were more likely to adopt AI, our study introduces a complementary perspective. By grouping healthcare organizations based on their mode of adoption rather than institutional capacity (e.g., the number of beds), we propose a new interpretative lens that seeks to contextualize AI implementation trends at the intersection between institutional missions and strategic orientation at the organizational level. This study should be viewed as a pilot, in which a newly designed survey instrument was tested to explore organizational patterns of AI adoption, providing a foundation for future studies aiming to develop more scalable insights. All in all, this study illustrates that AI adoption is not a uniform process, underscoring the importance of considering distinct pathways to AI implementation, with implications for multiple actors involved in the ecosystem, from policymakers to industry stakeholders seeking to support AI integration in healthcare systems. By mapping these adoption patterns, our findings contribute to a more granular understanding of AI diffusion in health care and offer a foundation for future research on understanding AI applications across diverse institutional settings.
Limitations
The findings of this research should be intended as purely observational and interpreted narratively, considering the following limitations.
First, the study offers a cross-sectional view based on data collected between December 2023 and February 2024, with follow-up until June 2024, reflecting a context that is rapidly and continuously evolving. The reported data may not provide a fully comprehensive or up-to-date representation of all organizational initiatives and AI applications adopted in clinical practice by healthcare organizations in Lombardy. In addition, survey responses (and survey responses’ quality checks via dedicated follow-ups) were collected from December 2023 to June 2024; therefore, this time lag may affect the overall consistency of the findings. Lastly, while the sample is extensive and highly representative of regional healthcare organizations, the mapping of AI applications is inevitably partial, as it primarily reflects the self-reported perspective of CIOs, who were the survey's target respondents. These individuals might not be fully aware of technological solutions acquired directly by individual clinical units, especially when such solutions do not require integration with enterprise information systems or are embedded within hardware medical devices. Consequently, certain categories of AI applications currently in use within Lombardy healthcare organizations may be underrepresented in this overview. At the same time, it might also be the case that the survey reflects regional specificities that cannot be generalized in other regional contexts.
To address these limitations, future iterations of this survey could involve additional key stakeholders, such as clinical engineers, physicians involved in early development and experimentation phases, and technology providers.
Conclusions
The adoption of AI applications in clinical settings is poised to accelerate significantly in the coming years, bringing with it substantial managerial and professional challenges. Initiatives like the one documented in this study, involving the entire regional ecosystem, can promote a deeper understanding of the use and potential of these technologies, while also creating opportunities for dialogue and the exchange of ideas and solutions. To further accelerate the adoption of AI applications in clinical practice, policymakers and healthcare organizations are encouraged to invest in cross-sector collaboration; support training programs for clinical, managerial, and administrative staff; and establish clear frameworks for evaluating AI-related innovations. Going forward, future research should evaluate the costs and benefits associated with the alternative approaches outlined in this work, as well as others that may emerge in the future, with the ambition to ultimately provide strategic guidance to healthcare organizations, in Lombardy and beyond, as they navigate the critical challenge of AI adoption.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076251355680 - Supplemental material for Adoption of artificial intelligence applications in clinical practice: Insights from a Survey of Healthcare Organizations in Lombardy, Italy
Supplemental material, sj-docx-1-dhj-10.1177_20552076251355680 for Adoption of artificial intelligence applications in clinical practice: Insights from a Survey of Healthcare Organizations in Lombardy, Italy by Vittoria Ardito, Giulia Cappellaro, Amelia Compagni, Francesco Petracca and Luigi M. Preti in DIGITAL HEALTH
Footnotes
Acknowledgments
The authors would like to thank our colleagues from Politecnico di Milano, Department of Management, Economics and Industrial Engineering—Cristina Masella, Chiara Sgarbossa, and Mattia Vincenzo Olive—for their valuable contribution in designing and disseminating the survey. The authors would also like to to thank the Unità Organizzativa Sistemi Informativi e Sanità Digitale of Lombardy region and Assolombarda's Healthcare Group (gruppo sanità) for their involvement and support in disseminating the survey to target healthcare organizations.
Ethical considerations
The study was approved by the Ethical Committee of Bocconi University (EA000672).
Consent to participate
All participants agreed to the consent form.
Author contributions
VA: Conceptualization, data curation, formal analysis, methodology, writing—original draft, and writing—review and edits. GC: Conceptualization, methodology, project administration, writing—review and edits, and validation. AC: Conceptualization, methodology, writing—review and edits, and validation. FP: Conceptualization, data curation, formal analysis, methodology, and writing—review and edits. LP: Conceptualization, data curation, formal analysis, methodology, and writing—review and edits.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was performed within the MUSA (Multilayered Urban Sustainability Action) project funded by European Union—NextGenerationEU under the National Recovery and Resilience Plan (NRRP) Mission 4 Component 2 Investment Line 1.5: Strengthening of research structures and creation of R&D “innovation ecosystems,” set up of “territorial leaders in R&D.”
Declaration of conflicting interests
The authors declared no conflicts of interest with regards to the conduct of the research, authorship, and/or publication of this article.
Data availability statement
Survey data without specifications of survey respondents, nor participating organizations, may be provided by the corresponding author upon reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.