
Abstract
Objective
This study examined the delivery of telehealth for behavioral health services among Critical Access Hospitals (CAH). More specifically, we describe how CAHs representatives reported using telebehavioral health (TBH) to meet the behavioral health needs of patients, identify ways in which Medicare billing flexibility did or did not affect TBH use and behavioral health staffing among CAHs, and explore opportunities and challenges CAHs face for using TBH in the future.
Methods
We conducted semi-structured interviews of CAH administrators and providers to examine the circumstances under which TBH was used.
Results
The extent of TBH use varied across CAHs in our sample; however, provider-to-provider consultations were generally more common in the inpatient and ED settings, with provider-to-patient encounters being more common in outpatient clinics. Medicare flexibilities, such as allowing a patient's home as an eligible originating site and reimbursement for audio-only visits, were reported to be useful by many participants, although staffing changes resulting from the flexibilities were not commonly reported. Concerns about reimbursement levels for behavioral health and uncertainty about reimbursement telehealth in the future were common. Lack of availability of behavioral health providers and administrative staff to support telehealth compounded challenges of planning for telehealth within uncertain policy and reimbursement conditions.
Conclusion
Telehealth has potential to close the rural-urban access gaps, but CAHs likely will need supportive policies and technical assistance to meet their communities’ needs with TBH.
Introduction
In the United States, Critical Access Hospitals (CAHs) are designated Medicare providers having no more than 25 acute inpatient beds and specific geographic parameters. 1 Over 95% of CAHs serve rural areas and are often the only source of community care as most rural areas are also Health Professional Shortage Areas.2,3 Within rural areas, in particular, concerns about adequate access to behavioral health (BH) services have been well documented. 4 Telehealth has been viewed as a solution for barriers to access in rural areas. 5 However, prior to January 2020, Medicare reimbursement was subject to restrictions on the type of originating site and geographic location of the site; specifically, patients were required to be located within a healthcare facility (not within their home) in a rural area. Furthermore, CAHs were not eligible to serve as a distant site for telehealth services. 6 However, the Coronavirus Aid, Relief, and Economic Security (CARES) Act of 2020, in response to the COVID-19 Public Health Emergency (PHE), provided flexibility in Medicare billing for telehealth services, specifically, allowing providers who are otherwise eligible to bill Medicare for their services, including those employed by CAHs, the flexibility to serve as distant site providers for telehealth services. 7 CMS also identified more than 135 new reimbursable telehealth services, including emergency department visits, initial and subsequent observation, initial hospital care, critical care and services, intensive care services, and therapy services. 7 Based on a 2020 survey of CEOs in 216 CAHs across eight states, telehealth flexibility was used by 90% of CAHs and was viewed as the single most beneficial waiver by almost 60% of CAHs. 8 The flexibility to serve as a distant site provider was extended through December 2024, and the flexibility to serve as an originating site provider for behavioral telehealth services was made permanent allowing patients to access telehealth without restrictions on type of originating site or geographic location. 9
Although CAHs are important for providing access to BH services in rural communities, little information has been available on the impact of Medicare flexibilities on the use of telebehavioral health (TBH) and behavioral health staffing within CAHs. This study used qualitative methods to (a) describe trends and scenarios in which TBH was used in CAHs to meet the behavioral health needs of patients; (b) identify ways in which Medicare billing flexibility did or did not affect TBH use and behavioral health staffing among CAHs; and (c) explore opportunities and challenges CAHs face for using TBH in the future. Our findings are useful for policymakers and health systems leaders interested in understanding the types of reimbursement changes that are impactful for CAHs as well as factors unrelated to reimbursement that affect TBH use in CAHs.
Methods
Recruitment strategy
The population of interest for this study comprised CAH employees, either administrators or providers, knowledgeable about TBH services to be sampled from a population identified in an associated quantitative study. The quantitative study used the 2019–2021 Medicare files for a nationally representative sample of CAHs to explore the provision of TBH services. We identified CAHs by the facility type code and the provider number field. We also identified the types of CAH providers who billed for TBH services during the PHE policy flexibilities. To determine rurality and census regions we used zip codes linked to the Rural Urban Commuting Area (RUCA) codes to establish whether CAHs were in Large Rural, Small Rural, or Isolated Small Rural areas as well as the census regions. As CAHs can be located in rural or urban areas, urban-rural classifications were based on the definition provided by the Federal Office of Rural Health Policy (FORHP). 10 Approximately 1300 CAHs (40% in the Northeast, 24% in the Midwest, 16% in the South, and 20% in the West) providing TBH services were identified. We intentionally recruited 115 CAHs that represented a range of BH service capacity and telehealth utilization as well as Census regions.
Participants were recruited via email after email addresses were identified via web confirmation. Our recruitment efforts sought to speak to the individual who could best address our questions about TBH services. Participants reviewed project information and consent documents via email. Eligible and interested participants provided verbal consent prior to beginning the interviews. Our semi-structured interview guide was drafted based on information from the literature and included questions on types of BH and TBH services offered, staff involved in delivering those services, and the effects of the Medicare reimbursement flexibilities.
Data collection and analysis
Two researchers (CS and ST) conducted semi-structured interviews between 12/20/2022 and 6/8/2023. Both interviewers have experience with prior studies involving rural health and telehealth. Interviews lasting approximately 45 min were conducted via Zoom and audio-recorded. Digitally recorded audio files were then professionally transcribed. For some participants, we sent an email after the interview requesting clarification and/or additional information. Transcribed data and any additional data obtained via email were uploaded to the qualitative data analysis tool Dedoose.
Data analysis within Dedoose took place after data collection. All data, regardless of the data being from the CAH administrator or provider, were treated the same as the semi-structured interview guide was the same. Codebook development and coding followed an iterative and adaptive process. The preliminary codebook included deductive codes that aligned with pre-established subject areas (like reimbursement or workflow) and organizational characteristics. Next, a subset of the transcripts were coded by two members of the research team (MM and ST). These codes were discussed until consensus was reached and comprised the initial codebook. MM and ST then divided the remaining interviews to code. The team met multiple times to discuss codes, reach consensus, and revise the codebook if needed. Once coding was complete, coding summaries were utilized to identify themes that emerged within the three overarching topics of the study listed above (i.e. trends and scenarios of TBH use, impacts of Medicare flexibilities, and opportunities and challenges for future TBH use). Because our study employed a descriptive approach, not Grounded Theory, we view the concept of “saturation” as not directly applicable. That being said, during data collection, we used dimensions of the concept “information power,” including scope of the aim, sample specificity, quality of dialogue, and cross-case analysis, to assess the sufficiency of our sample and data. 11 We also applied techniques to drawing and validating conclusions in qualitative research, including looking for negative evidence, considering rival hypotheses, and triangulating multiple perspectives (i.e. administrators and providers) to assess the sufficiency of our sample, data quality, and validity of conclusions. 12 The University of North Carolina at Chapel Hill's IRB approved this project as exempt research (IRB# 22-2468), allowing for verbal consent from participants.
Results
We interviewed 16 administrators (e.g., CEO, Director of Emergency Services) and 6 providers (e.g., physician, licensed clinical social worker). The 21 CAHs represented all four US Census regions (Northeast = 2, Midwest = 7, South = 5, West = 8). Of the 21 hospitals, 20 were rural, 19 were in a state participating in the Psychology Interjurisdictional Compact (PSYPACT), 11 were affiliated with an integrated health system, and 10 were utilizing third-party telehealth services. Participants reported both provider-to-provider (n = 8) and provider-to-patient (n = 11) telehealth. 13 Approximately half (n = 12) of participants reported having BH clinics integrated within or affiliated with their CAHs. Moreover, many participants (n = 14) indicated having either full or part-time dedicated BH specialists within their affiliated clinics. Some participants discussed outpatient BH care integrated into primary care practices where mental health practitioners are contracted (n = 5). CAH-affiliated clinics employed various BH specialists. Below we summarize findings related to trends and scenarios in which TBH was used in CAHs, the impact of Medicare billing flexibility on TBH use and behavioral health staffing, and opportunities and challenges for TBH in the future. Each section includes a table of illustrative quotations to complement the quotations provided in the main text.
Trends and scenarios for using TBH
In general, participants reported an increase in telehealth use during 2020, followed by a decrease. The initial implementation of BH telehealth during the pandemic was described as a necessity: “So we were already doing it [telehealth]. We were still visiting the clinics, though. And then once COVID happened in March, it became necessary.” [Interview 7]. However, after PHE-related restrictions eased or were lifted altogether, the amount of in-person BH care increased, with many participants reporting a hybrid model of in-person and TBH services. Reasons offered for needing a hybrid model, instead of solely telehealth, included better comprehension by the provider for some patients’ physical condition in person, provider concerns about patients feeling isolated at home, and patient concerns about privacy and access to needed technology. However, there was not a universal preference for in-person care compared to telehealth. Some participants indicated that patients appreciated the flexibility of not having to miss school or work to make their appointments or receive care and not having to find transportation to a BH clinic, particularly when trying to avoid exposure to SARS-CoV-2 or influenza. Similarly, some providers preferred providing care from their homes for health reasons or for saving travel time to clinics. In general, a hybrid model facilitated increased telehealth use compared to prior to the PHE, with telehealth usage being highest when deemed absolutely necessary (e.g., during 2020) and dependent on provider and patient preferences after PHE restrictions were eased.
Because many of the CAHs in our sample were affiliated with an integrated delivery system or had affiliated outpatient clinics, some of their patients received TBH services in multiple settings. One participant described such a scenario as follows: Here's the classic example. We have a patient who has a substance misuse disorder, they come into their emergency department, they're in crisis, we help them right there. We have peer counselors in the ED who then typically would link that patient up with services at [the substance use service methadone clinic], right? They might get extensive intensive treatment through [the methadone clinic], and then when they reach a point of stability then they transmission back into maintenance at the spoke which is probably one of our RHCs. [Interview 6]
Below we provide additional detail about TBH scenarios within outpatient clinics, emergency rooms, and inpatient departments.
Much of the provider-to-patient telehealth reported was delivered in CAH-affiliated primary care or BH clinics, which in some cases are physically located within the CAH: “[O]n the primary care side. That's where we've seen that expansion, where people are at home, home bound for one reason or another, whether physically or whatnot.” [Interview 2]. According to one participant: [W]e do have a integrated behavioral health psychologist that's embedded within our primary care for more shorter term care. So, the model there is that they're working shoulder to shoulder with our primary care group, which on any day, we usually have between 10 and 12 primary care clinicians within our clinic. And so, we get referred to our integrated therapist one to four sessions before the issue is considered resolved or she's acting like a care navigator to get connected in more longer term treatment options, whether it's through our behavioral health clinic or one of our neighboring sites. [Interview 19]
As illustrated by this example, participants described follow-up outpatient TBH services, typically involving referral from a primary care physician, nurse practitioner, or emergency room provider. Upon receipt of the referral, the BH provider's administrative staff or case managers scheduled the telehealth appointment for the patient to connect with the behavioral health specialist.
In addition to referrals to outpatient BH services, TBH use in the emergency department was discussed for substance misuse, suicidal ideation, self-harm, and risk of harm to others. Such instances primarily involved provider-to-provider consultations to support crisis management, determine placement, manage medications, and provide referrals: [W]e do have a behavioral health connection in our ED with psychiatry, and it's really to make a determination on what's the best disposition for that patient after that emergent event. Can they go back to home and get community-based counseling or do they have to be admitted into an inpatient unit? [Interview 21].
The reported processes for referrals or placement in other facilities varied—with some led by the distant-site provider and others led by CAH staff, for example: [L]let's say it's a suicidal person and they're in the ER and they activate the telehealth. Usually the group that we use, they become responsible for that person essentially, in a sense. They work on doing all of the admissions because they work with their hospitals in [city name] and they get them admitted. All we do at that point then is, the ER doc on our end is just guided by their psychiatrist or psych NP or whoever is talking to them on, “Here's what meds to give,” and then we work on just getting them transported to the facility. I would say outpatient wise, we're more utilized for a follow-up after they return or they get discharged. [Interview 18]
Although less frequently reported, evaluations and crisis management via telehealth also could involve provider-to-patient interaction. Some participants indicated that having behavioral health providers who work in their clinics available for in-person or telehealth support in the ED would be beneficial but that this was not feasible: [I]f we could have some kind of triage in the ER, someone could do the assessments and then get them placed or the resources they need for those in crisis, that would be great. Because right now, we have the three [behavioral health clinicians] that work in the clinic. They have full outpatient clinic schedules. When one person presents to one of our clinics in crisis, they pretty much, takes the rest of the day. Yeah. So it'd be nice to have them to be able to do an initial assessment and then get them to somebody that could deal with the crisis right then and there. Preferably in ER, preferably telehealth. [Interview 11]
Similar to emergency departments, provider-to-provider telehealth was more commonly reported within inpatient units compared to provider-to-patient telehealth. Such interactions involved telehealth consultations provided either by (a) CAH-affiliated psychiatrists or other behavioral health staff or (b) clinicians employed by another entity with a contract or agreement to provide TBH. These consultations commonly focused on medication management, evaluations, and treatment planning. One participant described the following medication management scenario: [F]or a medication management, “Hey, I have this patient here. He's usually on these medications, but maybe they're on a ventilator and NPO, unable to take anything by mouth. So what would your recommendation be for, are these medications safe to continue?” That sort of thing. And it's just because our hospitalists are usually managing these patients, and they're not comfortable with a lot of the psychiatric medications, and they have a basic knowledge. But as far as some things and maybe some more at-risk patients or some complicated patients, they might seek some guidance from a telepsych provider. [Interview13]
The same participant went on to describe an actual event involving evaluation and treatment planning: So we had a patient that was brought in … she had some addiction issues, and we'd kind of taken her through the withdrawal process, but cognitively she was having a very difficult time coming around. She was very kind of impulsive and erratic, and we were having trouble determining, is this residual from her maybe alcohol withdrawal symptoms or is this an underlying mental health or behavioral health issue? But also, this woman lives by herself and is independent and doesn't have family or a spouse that is able to kind of care for her or take responsibility for her. So then we also have some competency questions that are coming up. And so, we were able to use the acute telepsychiatry service to do multiple evaluations on her, recommend medications for treatment and appropriate treatment plans, and then provide some competency evaluations. Is she capable of making decisions for herself? Is she capable of signing herself out AMA? Does she understand these? And providing that support for our hospitalists because often they're uncomfortable making those decisions. And eventually, she was at a point where we were actually considering having to seek, try and seek emergency guardianship for her. But through the recommendations through telepsychiatry medication management, and I think probably just time, she was able to clear up 100% and resume, regain competency and resume her normal independent life. So I think they were instrumental in that. [Interview 13]
Overall, participants discussed TBH as being useful in the inpatient setting for patients admitted to the hospital for medical reasons who have behavioral health needs, which are sometimes unknown at the time of admission. Because some CAHs are not licensed for inpatient psychiatry beds, TBH can be an option for patients who require medical care prior to going to a psychiatric facility. (See Table 1 for additional quotations.)
Trends and scenarios for using TBH.

Impact of medicare flexibilities on TBH use and staffing
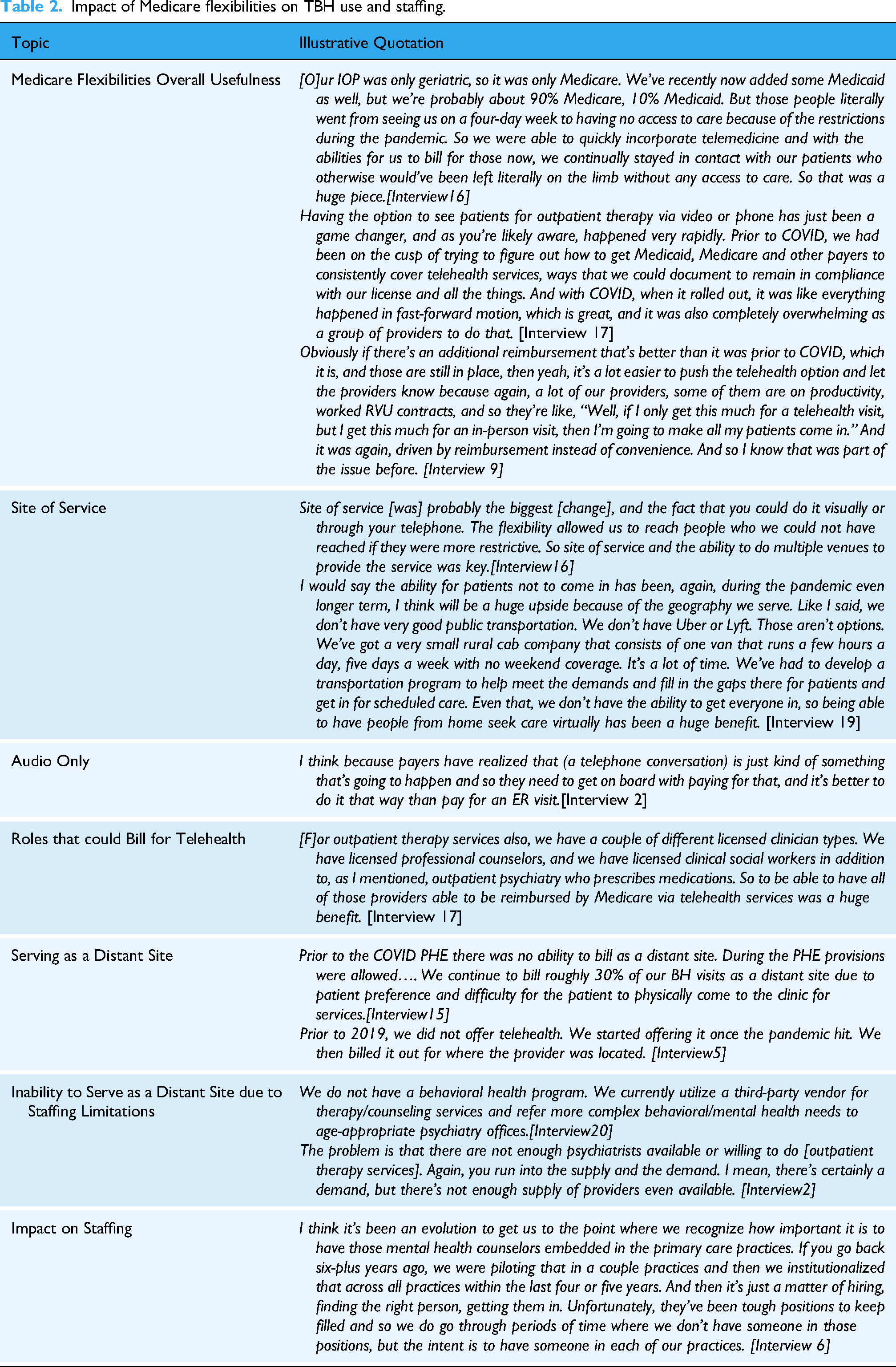
As described above, TBH services were provided in outpatient, inpatient, and emergency departments to address various patient conditions and needs. Several participants reported that modified telehealth reimbursement policies were critical to their ability to do so during the PHE. According to one participant: “First off, Congress lessening or changing the rules for rural health clinics and critical access hospitals in the telemedicine field was a lifesaver” [Interview 16]. Allowing patients to access telehealth services from any location (i.e. site of service) and allowing audio-only calls were notable parts of the flexibilities for many participants. The site-of-service flexibility was considered highly valuable for outpatient TBH services, in particular, for increasing access and convenience for patients. Reimbursement for audio-only was described as a way of reducing the technology burden for patients and as formal recognition that a telephone call is sometimes the most feasible, if not the only, option for an encounter.
Some participants also highlighted the importance of the flexibility to serve as a distant site, particularly from outpatient clinics. However, flexible reimbursement policies did not enable all CAHs to serve as a distant site, specifically, those that lacked BH staff. In such cases, CAHs could serve as an originating site, contracting for external TBH services. Notably, most participants reported no staffing increases, or impending plans for new staff, despite increased opportunity for telehealth reimbursement. There were a few exceptions. For example, a participant indicated that her role as a psychiatric mental health nurse practitioner—the only behavioral health provider in her rural primary care clinic—was developed in response to the PHE, greatly expanding access to services: “With telehealth, I actually have patients all over the state.” [Interview 8]. Others reported a desire to hire more BH providers to meet the needs within their community but were unable to do so due to a lack of availability of individuals to hire. (See Table 2 for additional quotations.)
Impact of Medicare flexibilities on TBH use and staffing.
Opportunities and challenges for TBH in the future
Although the Medicare flexibilities were important for providing services during the PHE, several participants noted ongoing concerns about the level of reimbursement for telehealth going forward and/or for behavioral health services in general, whether in person or TBH. Generally speaking, organizations must be willing to financially invest in telehealth to cover the costs (e.g., equipment, contracts with vendors). Because provider-to-provider consultation with third-party TBH providers is not always reimbursed, hospitals must absorb the cost of the services provided or the cost of the contract with the third-party provider.
Clearly, Medicare flexibilities improved reimbursement for TBH in many ways; however, uncertainty about future reimbursement policy makes planning for future telehealth services challenging. For example, the following participant discusses uncertainty about reimbursement policy and the likely risk-averse decision taken as a result—that is, not offering the telehealth service: The problem now as you know, going forward, I know we have a two-year window, but if they revert back to where we were, that whole possibility, particularly as we offer new services in the RHC [rural health clinic], that whole game plan will change. And that really leaves us in a dilemma because we're trying to plan for the future without knowing what the future holds, and reimbursement obviously is a big part of that. So if we can't plan our future based on reliable revenue, we either don't plan at all or hedge on just not offering service because we don't know the viability. [Interview16]
Although some organizations use grant funds to provide telehealth services, alleviating the need for enhanced reimbursement, relying on grants may not be sustainable.
Hiring and retaining staff was identified as another challenge. Participants talked about the challenge of hiring both behavioral health providers and administrative staff to support telehealth. Notably, CAHs compete with organizations in other sectors for administrative support, particularly in a strong job market. According to one participant, this challenge is a key barrier to the growth of outpatient TBH use, in particular: [T]o be able to provide more services in an outpatient setting is you need more staff because a physician isn't going to do it on their own. They're not going to get it all set up, do it on their own. And I mean, they'll do it if it's simple. And that's what we made it for them. And especially during Covid, it was simple for them, but because they weren't having a lot of inpatient visits, it wasn't that difficult to say, “Okay, I'll just spend half the day doing this.” And so that's where I think the struggle is providing dedicated, specific staff just to do telehealth. If we were able to do that, I think the numbers would actually grow. [Interview 9]
Without sufficient administrative staff to support the logistics of telehealth services, suboptimal workflows may hinder the efficiency of providers and/or providers may be less willing to provide telehealth services.
Medicare reimbursement flexibility regarding types of providers eligible to bill for telehealth was viewed positively, not only for CAHs but for addressing the national problem of staffing shortages, despite the fact that most participants in our sample did not report increasing staffing as a result of the reimbursement flexibility. This may have been due to the uncertainty about whether that flexibility would be made permanent, a shortage of available staff to hire, or a combination of factors. That being said, telehealth was discussed as a vehicle for addressing staffing shortages, with leaders selecting staffing solutions that fit the needs, capabilities, and available resources of their CAH. Examples of such solutions included contracting with another institution, third-party vendor, or individual providers who were licensed to work across state lines.
Another challenge embedded within discussions about TBH use included the need for optimizing a hybrid in-person/telehealth model of delivery. Decisions to adopt a hybrid model are based, at least in part, on patient and provider preferences. Once adopted, the hybrid model has implications for staffing, scheduling, workflows, and other operational decisions. Related to these operational decisions are the awareness, willingness, and technological access—at the community and individual patient level—to participate in a hybrid model. Although a few hospitals took it upon themselves to help educate the community about telehealth, this was not the norm, and most hospitals likely would need some external support to do so. All in all, there is much still unknown about how best to structure and support a hybrid model.
Finally, our interviews highlighted the clear commitment that CAH administrators and providers have to address the overall health needs of their communities and their prioritization of addressing behavioral health needs, in particular. Despite the challenges identified, participants conveyed a sincere interest in finding creative, feasible solutions tailored to their CAHs and communities. (See Table 3 for additional quotations.)
Opportunities and challenges for TBH in the future.

Discussion
Through interviews with CAH administrators and providers, our study described various ways in which TBH services benefit patients within CAH communities, described the impacts of Medicare flexibilities on TBH use and staffing, and identified opportunities and challenges for TBH use in the future. The emerging themes presented a variety of subthemes describing the landscape of telebehavioral health care. First, hybrid models presented as the new norm of behavioral healthcare delivery post the public health emergency due to the COVID-19 pandemic. Many CAHs implemented an approach that integrated telehealth and in-person visits, motivated by patient and provider preferences and technological access. Second, the importance of provider-to-provider consultations in emergency, inpatient care, crisis management, medication management, and care planning was demonstrated by its commonality. Crisis intervention in emergency rooms leverages telebehavioral health for immediate psychiatric evaluations and support for providers lacking specialized training in behavioral health presented as subthemes. Third, the impact of Medicare flexibilities on access and operations during the public health emergency due to the COVID-19 pandemic was essential in expanding telehealth access and financial feasibility for CAHs. Policy support including reimbursements related to audio-based care presented as an important subtheme. Fourth, administrative and staffing barriers to telebehavioral healthcare expansion illustrated the significant role administrative support plays in sustaining telehealth operations. Subthemes centering on workforce recruitment and retention beyond clinical care providers presented. Finally, a theme on the uncertainty about reimbursement policies in the future described general concern about the temporary nature of reimbursement flexibilities and the challenge of planning services amidst political uncertainty. The important subthemes presenting here describe CAH providers's risk aversion in decision making due to uncertain policies and CAH executives's understanding of the threat to sustainability resulting from reliances on grant funding for certain related services.
These qualitative findings complement statistical analyses on the trends and effects of TBH by offering insight into why those trends and effects are occurring. Our interviews highlighted the importance of the Medicare flexibilities for CAHs for meeting the behavioral health needs of their patients while also receiving much-needed reimbursement for the services. These flexibilities appeared most impactful for outpatient services, commonly delivered through clinics affiliated with the CAH, as compared to provider-to-provider consultations in the emergency or inpatient settings. Despite the overall usefulness of the flexibilities, concerns about reimbursement for behavioral health and availability of behavioral health providers were prevalent, consistent with other studies.14–16
In general, CAHs established TBH arrangements that aligned with their staffing and their community needs; however, most participants conveyed at least some concern about being able to do so sufficiently and/or in a sustainable way. They described the challenge of planning for telehealth within uncertain policy and reimbursement conditions. The uncertainty, coupled with difficulty recruiting BH staff, contributes to hesitancy among many CAH leaders to take on the financial risk of investing in new staff and telehealth infrastructure. The unfortunate outcome of this uncertainty could be the risk-averse decision to not expand TBH services, despite the need for them.
Our findings also highlighted that the availability of administrative staff to support telehealth was a challenge for some CAHs, due to low unemployment rates and increasing wages offered by non-health organizations. Inadequate administrative support is a barrier to scaling up telehealth services and is an issue that, to our knowledge, has not been well documented in prior literature.
Despite the challenges raised, our participants conveyed a clear commitment to meeting the needs of their communities and their approaches to doing so demonstrate persistence and creativity. Many CAHs and affiliated clinics use a hybrid model of telehealth and in-person services for behavioral health to account for provider and patient preference, a finding that is consistent with studies of other settings and types of telehealth services.17–20 In CAH emergency and inpatient settings, in particular, our findings highlighted the usefulness of TBH for addressing the information needs of emergency physicians and hospitalists who do not have specialized training in medications and care planning for patients with behavioral health conditions. Addressing those needs with TBH could improve the performance and satisfaction of these physicians working under stressful conditions.
Future research and policy could build upon our findings in several ways. For example, more research is needed to document strategies employed in CAHs and affiliated clinics for educating communities about telehealth to increase willingness and ability to use TBH. Also, research is needed to clarify how to optimize hybrid telehealth/in-person models, from both the patient and provider perspectives, particularly in outpatient settings. Some CAHs also would benefit from additional support related to caring for patients with substantial behavioral health needs who present in their emergency rooms or who are being treated for medical issues in CAHs that do not have psychiatric beds. Finally, efforts from policymakers to increase reimbursement for behavioral health while also reducing uncertainty about reimbursement for telehealth would be impactful for CAH leaders planning for the expansion of TBH services and/or behavioral health staffing.
Limitations
Our study focused on CAHs, which serve rural communities and have different reimbursement models than other hospitals in the United States; therefore, the TBH experiences of other types of hospitals may be different from our study sample. Furthermore, our interviews were conducted in a six-month period from the end of 2022 to mid-2023. The information available to participants about Medicare flexibilities may have changed during that time period and subsequently; therefore, our interviews captured only a snapshot of perspectives about a dynamic situation. Additionally, the varying dates on which the PHE ended across different states may further limit the generalizability of findings due to differences in policy environments during data collection. Nevertheless, documenting these perspectives is valuable for understanding both the similarities and differences of experiences within a particular type of setting (CAH), with the differences likely attributable to important contextual factors, such as staffing and relationships with other medical and non-medical organizations.
Conclusions
CAH administrators and providers in our sample conveyed a sincere interest and high commitment toward addressing behavioral health needs in the inpatient, outpatient, and emergency settings. Furthermore, TBH has the potential to improve care quality, close access gaps, and reduce BH disparities. However, uncertainty about reimbursement for behavioral health and telehealth may hinder efforts to invest in the infrastructure and staffing needed to support ongoing TBH service delivery.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076251353364 - Supplemental material for Use of telebehavioral health services by critical access hospitals in the United States: A qualitative study of the impacts of medicare flexibilities and future opportunities
Supplemental material, sj-docx-1-dhj-10.1177_20552076251353364 for Use of telebehavioral health services by critical access hospitals in the United States: A qualitative study of the impacts of medicare flexibilities and future opportunities by Christopher M. Shea, Sharita Thomas, Marah Maaita, Heidi O’Connor and Yvonne Jonk in DIGITAL HEALTH
Supplemental Material
sj-docx-2-dhj-10.1177_20552076251353364 - Supplemental material for Use of telebehavioral health services by critical access hospitals in the United States: A qualitative study of the impacts of medicare flexibilities and future opportunities
Supplemental material, sj-docx-2-dhj-10.1177_20552076251353364 for Use of telebehavioral health services by critical access hospitals in the United States: A qualitative study of the impacts of medicare flexibilities and future opportunities by Christopher M. Shea, Sharita Thomas, Marah Maaita, Heidi O’Connor and Yvonne Jonk in DIGITAL HEALTH
Footnotes
Acknowledgements
Acknowledgments are not applicable to this study.
Ethical considerations
The research plan for this study was reviewed by the Office of Human Research Ethics at UNC-Chapel Hill. As the study does not fall within the scope of the Human Research Act, no further approval is required for its conduct.
Consent to participate
Informed consent is not applicable to this study.
Author contributions
CS: conceptualization; formal analysis; funding acquisition; investigation; methodology; project administration; resources; software; supervision; validation; visualization; writing—original draft; writing—review and editing. ST: formal analysis; investigation; project administration; software; validation; writing—review and editing. MM: formal analysis; investigation; software; validation; visualization; writing—review and editing. YJ: funding acquisition; validation; writing—review and editing. HO: writing—review and editing.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Office for the Advancement of Telehealth (OAT), Health Resources and Services Administration (HRSA), U.S. Department of Health and Human Services (HHS) under Cooperative Agreement 6 U3GRH40003-01-03. The information and conclusions are those of the authors and no inferred endorsement by OAT, HRSA, or HHS.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
Not applicable to this study.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.