
Abstract
Background
Given the steady increase of emergency department (ED) visits related to opioid overdoses, this study aims to determine the design and usability of an ED-centered mHealth patient-to-peer referral prototype tool that allows patients to refer peers to comprehensive HIV/HCV and opioid misuse prevention services.
Methods
Two iterative focus group discussion (FDG) sessions and one use-case session were conducted. Eligible participants who were ≥18 years, had a history of injection drug use (IDU), and had utilized the ED in the past year were recruited through the distribution of flyers at the study institution, including the study ED. Human-centered design process was completed by using participant feedback on perceived utility, usability/accessibility, tool design, and clarity/readability to fine-tune prototype version and drive subsequent discussion sessions.
Results
Sixteen consented individuals participated in at least one of the sessions. Feedback revealed that participants favored the inclusion of the webpage link on the referral card as means to bypass QR code if needed, more descriptions highlighting the exact services offered, and the fact that no personal information was required to complete the referral process. The prototype underwent several adjustments between user-centered FDG sessions, which ultimately ended in including features such as an online webpage with educational videos, SMS text-message communication system, and QR code usage into the final patient-to-peer referral tool prototype.
Conclusion
The findings of this study suggest a human-centered designed patient-to-peer referral tool could be a feasible approach to linking community members at risk of IDU to HIV/HCV and opioid use-related preventive services from ED patients.
Introduction
The opioid crisis in the U.S. has been steadily increasing during the last decade. In 2017, the U.S. Department of Health and Human Services declared the opioid crisis a national public health emergency. 1 Opioid-related overdose deaths account for over 70% of all drug overdose fatalities in 2019. 2 People who inject drugs (PWID) are also at high risk of acquiring blood-borne viral infections, including human immunodeficiency virus (HIV) and hepatitis C virus (HCV). 3 Approximately 20–30% of people living with chronic HCV infection in the United States will progress to liver cirrhosis in 25–30 years if left untreated, 4 while chronic HIV infection can lead to systemic complications involving liver disease, cardiovascular disease, lung disease, and bone disease. 5 A total of 7% of the 37,968 new HIV diagnoses in the U.S. in 2018 were among PWID, while 72% of the 3,621 new cases of acute hepatitis C reported injection drug use.6,7
Although rapid screening tests and treatment have become increasingly available, PWID report a lack of HCV testing in syringe exchange programs, as well as significant accessibility barriers for those who suffer from drug user stigma, have poor access to primary care, and have less education. 8 Additionally, visits by PWID to primary care health professionals have been associated with higher HIV testing. 9 Considering that Emergency Department (ED) visit rates for opioid overdose quadrupled from 1993 to 2010, the ED is growing into a unique position to help address the barrier between PWID and HIV/HCV testing. 10
U.S. EDs, with an estimate of >130 million total ED visits in 2018 mainly for substance abuse and mental health issues, provide extensive opportunities for emergency clinicians to improve care for substance use disorders (SUDs) by screening, initiating treatment, and directly linking patients to treatment.10–12 A novel patient-to-peer referral program that engages patients in the ED to refer peers and family members from their social networks to HIV/HCV testing services, as well as naloxone training, could take advantage of this unique opportunity in the ED setting. Naloxone, also known as Narcan, is commonly used in both community and hospital settings as a rapid-acting opioid antagonist that effectively reverses an opioid overdose.13,14
Mobile Health (mHealth), the practice of medical and public health via mobile communication devices, advances a new way of engaging with patients from vulnerable patient populations, by using the internet and text messages as means to promote better digital communication.15,16
Studies have demonstrated that mHealth interventions have proven effective at improving knowledge regarding HIV/HCV transmission and risk behaviors in opioid users. 17 The concept of an ED-based mHealth patient-to-peer referral program to HIV/HCV testing and naloxone has been perceived favorably by PWID. 18 Additionally, smartphone usage for video watching among PWID suggests favorable possible outcomes regarding education, such for HIV and HCV or naloxone. 18 Consequently, a human-centered design process, known for bringing end-users and developers together to co-design health services or delivery strategies that identify, and address barriers to usability, has shown the potential to improve the effective implementation of programs addressing diseases such as HIV. 19
Due to the ongoing opioid crisis, as well as health implications related to HIV/HCV risk for PWID, there is a clear need for increased access to both substance abuse prevention services and HIV/HCV testing for PWID. Although previous studies have shown improved results for programs including mHealth practices and human-centered design development,15–19 research related to the design, perceived utility, and accessibility for patient-to-peer referral mHealth tool in the ED is limited.
This study aims to improve and fine-tune a prototype mobile phone-based referral tool for an ED-centered patient-to-peer referral program for a prevention program that delivers comprehensive HIV and substance abuse prevention services (i.e., HIV/HCV testing and linkage to care, and naloxone training). Using a human-centered design process (Figure 1), we gathered iterative feedback and comments from a series of focus groups with PWID to develop a prototype mHealth patient-to-peer referral tool.

Human-centered design process of the patient-to-peer referral tool.
Methods
Study setting
The study site was an urban ED in Baltimore, Maryland, that had 67,500 annual visits with 2% of the ED patients indicating opioid use in the past 7 days in 2019. 20 The patient population in this ED is socioeconomically disadvantaged, with an estimated 15% of patients having a history of injection drug use.21,22 The most recent seroprevalence study has estimated an HCV antibody positive rate of 14% and an HIV antibody positive rate of 6%.23,24 This study was approved by The Johns Hopkins University School of Medicine Institutional Review Board (IRB00162605).
Study participants
Participants were recruited by contacting a subset of participants in a previous IRB-approved study (IRB00125414), which investigated the effectiveness of ED-initiated buprenorphine for moderate/severe opioid use disorder, with the same target population who consented to be contacted for future research, if they were 18 years or older, had a history of injection drug use, and had utilized the ED in the past 12 months. Individuals were also encouraged to bring one close family member or social network peer to participate in the study as a dyad. Injection drug use is often a social activity between two or more individuals, and dyadic interventions have been utilized previously to promote behavior change as it relates to HIV and HCV prevention. 25 Of approximately 50 previous study participants contacted by research coordinators, 4 agreed to attend the first focus group discussion and 3 agreed to bring one peer to the session. Attendants of the first session were encouraged to participate in the second and third sessions, with or without peers. All participants were provided a $20 gift card for their attendance at each session. Participants who brought a family member or peer were provided an additional $20 gift card. There was no prior participant knowledge of any of our study team members regarding personal goals or reasons for doing the research..
Some quotes from participants regarding perceived utility of the prototype.

Some quotes from participants in their opinion regarding usability/accessibility of the prototype.

Some quotes from participants in their opinion regarding tool design.

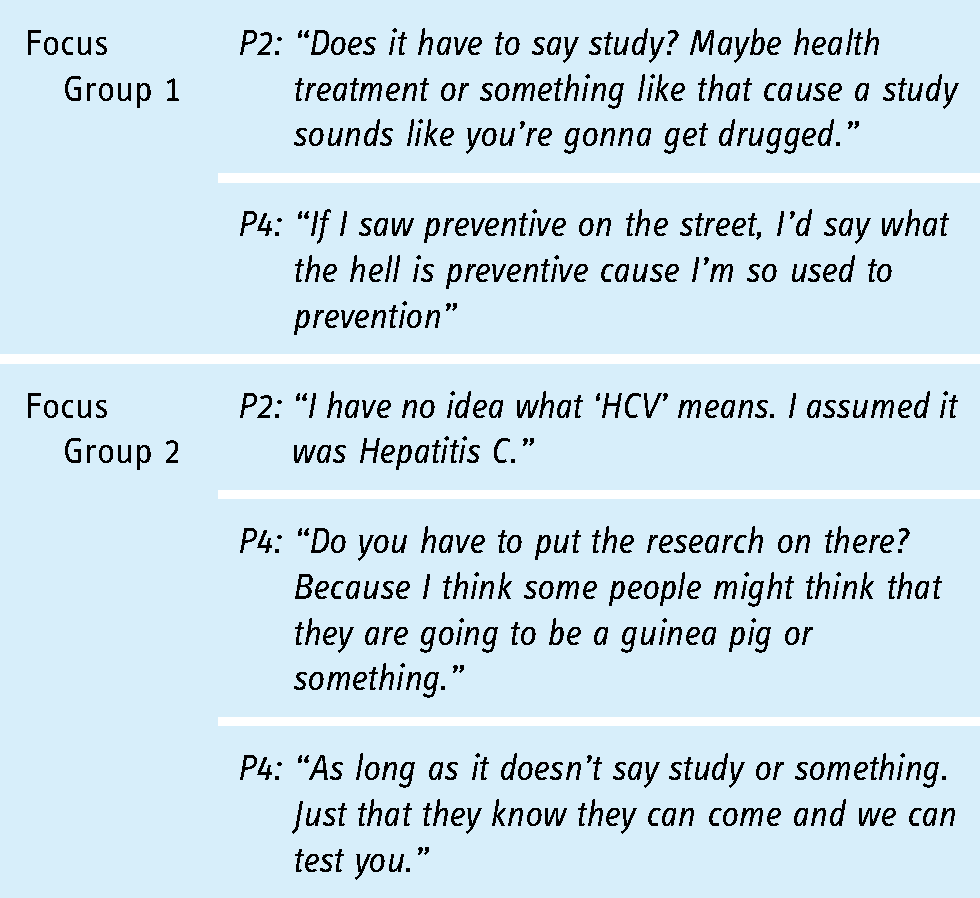
Some quotes from participants in their opinion regarding the clarity/readability of the materials.
mHealth tool design
The concept of a mHealth patient-to-peer referral tool was formulated based on in-depth interviews and focus group discussions conducted in an earlier phase of this study. 14 Prototype 1.0 and program materials were created by ZH and KV to demonstrate the peer referral concept. The tool consisted of a two-sided peer referral business card (Figure 2(A)), a webpage with an embedded interest form, and SMS communication templates. These components were designed to facilitate each phase of referral: 1) Index patients distribute cards to refer peers; 2) Peers access webpage to get information and sign up via the form; and 3) Clinic contacts peer via SMS to schedule appointments. The tool was created such that the referred patient would not have to identify themselves until they attended their scheduled appointment at the clinic. Instead of asking for the peer's name, the website form asks only for their phone number, the index patient's referral code or nickname (located on the card), and which services the peer is interested in receiving. The program also incorporated an incentive structure such that index patients and peers would be compensated for accessing services via the peer referral process.

(A) Prototype 1.0 Peer Referral Card. (B) Prototype 2.0 Peer Referral Card. (C) Prototype 3.0 Peer Referral Card.
Human-centered design process
The human-centered design process was conducted through two focus group sessions and one use-case session. All sessions were one hour long and were hosted in an ED conference room in April and May 2019. The three sessions were facilitated by study staff (TM, ZH, and KV) to determine the usability of the peer referral mHealth tool and adapt the program design to meet the needs and preferences of the patient population. All participants provided verbal consent and were given an overview of the study's intentions, materials, and proceedings at the beginning of each session. No identifiers were obtained from study participants in the focus group and use-case sessions.
During the two focus group sessions, study staff asked a series of questions regarding the usability and design of the mHealth tool. Questions were focused on four major categories: Perceived Utility, Usability/Accessibility, Tool Design, and Clarity/Readability. Alterations to Prototype 1.0 and associated materials were made after the first focus group based on participant feedback, and Prototype 2.0 was discussed in detail throughout the second focus group (Figure 2(A) and (B)). The goal of the focus group discussions was to develop new iterations of the prototype, and data saturation was established once the study staff gathered enough information in each category to create a new version of the tool. Consensus was determined on a given topic if a majority of participants indicated agreement verbally or nonverbally, and no participant expressed a differing opinion.
Following the two focus group sessions, a use-case session was conducted with participants to test the viability and intuitiveness of the tool in a practical scenario. Participant dyads were asked to try and refer to one another using the peer referral tool Prototype 3.0, which was developed following feedback from the second focus group session (Figure 2(C)). Study staff observed the use-case exercise and identified areas of ease and difficulty for participants. This session was not recorded since multiple dyads were completing the use-case exercise simultaneously.
Data and statistical analysis
The focus group sessions were audio-recorded and manually transcribed in Microsoft Word by ZH following their completion. Session transcripts were compared to the field notes and then analyzed by ZH, RR, and Y-HH to group participant quotes by question category. Key thoughts from participant responses were identified and compared based on the assessment of quotes in each a priori “Perceived Utility,” “Usability/Accessibility,” “Tool Design,” and “Clarity/Readability” category, and basic constant comparison analysis was performed to identify potential themes, if there were any. Any uncertainties were adjudicated by the primary investigator (Y-HH). COREQ (COnsolidated criteria for REporting Qualitative research) Checklist was used in reports of qualitative research (See Supplement Materials).
Results
A total of 16 individuals participated in at least one of the sessions with attendance of 7, 8, and 9 for the first, second, and third sessions, respectively. Of the 16 participants, 10 identified as male, and 6 identified as female. Although no age or race data was gathered, staff observed that all participants were middle-aged or older adults, with 8 participants appearing African American and 8 appearing white. For the purposes of this study, participants were identified as “P1, P2, P3…” to differentiate quotes between peers in the focus group discussions.
Focus group #1
Perceived utility
When describing the goals of the patient-to-peer referral program to participants at the beginning of the first focus group, P3 and P1 immediately validated the need for increased access to public health resources and training within their community: P3: “Yeah for the older population we need things like this cause I don't want to die from drugs.” (Table 1)
P1: “I had a friend OD at my apartment. It was pretty bad and we had to wait for paramedics to come. If I had [Narcan] training, we may have been able to give the Narcan sooner.”
P4 and P5 also emphasized the importance of privacy and anonymity, as illustrated by the following quotes: P5: “There's a lot of people who don't want to put their voice out there.”
P4: “When it comes to health, more likely to want it private.”
Usability/accessibility
Participants were asked their opinions about using text messages as contact methodology for referring peers. All of them expressed confidence in access to texting, as illustrated by the following quotes: P4: “Now, everything is mobile. Even if they don't have a phone, more likely than not there is a government phone they can text on. They just need something really quick, really clear, and that's it”
P5: “What I do is when somebody sends me a text and I just click on the URL and it goes straight to the website.”
P1: “If someone calls me and I don't have the number then I don't answer it. If it is a text I will read it.” (Table 2)
Additionally, participants were asked about the accessibility to the internet in their phones. They expressed consensual agreement in the notion that most peers have access, as illustrated by the following quotes: P5: “Yeah 99% of the people have the internet.”
P4: “I don't know a phone carrier that doesn't have the internet. Even government phones have the internet.”
P6: “And even if you don't, you can go get Wi-Fi. Barnes and Noble, McDonald's all have Wi-Fi.”
When discussing the use of QR codes on the referral cards, some participants were familiar with scanning the codes. One participant knew how to scan the codes since they had used them for other purposes: P4: “I do because it's the same one they use at the grocery store for coupons.”
P4: “There's also the same code on the back of a lottery ticket, they scan it cause you get so many points you get a free lottery ticket.”
However, two participants found the QR codes unfavorable and would rather access the website via an alternative method: P3: “I wouldn't know what to do, but I’m older. Though I see a lot of older people play lotteries and they know how to do it for the lottery.”
P1: “I tried to do it one time on something different, line your camera up yadda yadda, after like two tries I was like screw it.”
Although participants expressed familiarity with texting, mobile internet, and QR codes, a few participants preferred having an active contact number for the program: P1: “Also good to have the contact number cause many of them are not on the internet. All the guys that I got high with, half of them don't even know how to use the internet. They’re gonna be interested in calling the number that's the easiest way for them.”
P3: “Oh, I would call.”
P4: “Yeah I wanna talk to a person when it's something important to me.”
Tool design
Participants discussed their first impressions of the peer referral card. They all nodded in agreement when P1 voiced their approval of size and simplicity: P1: “Business card, fit what you need. People aren't going to carry around bigger things.” (Table 3)
P4 and P3 also provided thoughts on font size and color as illustrated in the following quotes: P4: “So, for most people with a drug history, the attention span is really short. Brighter colors and a bolder print. If its not gonna get your attention in the first couple seconds than you might as well toss it out the window. A little larger print and a bolder color. Your eye catches it and your more likely to read it than just toss it.”
P3: “I would give my friends this card, but it's gonna need to be a little bigger and bolder text for me to read.”
Three participants agreed that there are advantages in providing information through videos for education about HIV and HCV on the peer referral webpage. In their opinion, video provides higher odds of retaining information and keeps their attention for longer periods, as illustrated by the following quotes: P4: “I’d rather have a video.”
P3: “Me too.”
P5: “Video is the best If you’re watching the video, you’re more likely to get something out of the video even if it's just one thing. They may be more likely to go back and watch it again 2–3 times if it's only a 2-min long video and end up learning a bunch. You can divide it up too and have one for HCV and maybe other short ones for different things. Have them all like 2–3 min. That will divide people up and maybe keep them paying attention longer”
Additionally, three participants expressed that survey information of referred peers should go first, followed by videos. They expressed the importance of order as peers could potentially zone out after watching video information, as illustrated in the following quotes: P3: “I think the survey should be first”
P2: “Right, cause you want them to fill it out first”
P4: “Once you see the video you may feel you got what you need and are out.”
Clarity/readability
Participants also expressed their thoughts on the language of peer referral cards. One participant expressed concern over the use of specific words and negative connotations that may follow when reading them, as illustrated in the following quote: P2: “Does it have to say study? Maybe health treatment or something like that cause a study sounds like you’re gonna get drugged.” (Table 4)
Two participants were also confused about the use of specific wording. P4 and P5 expressed knowledge of the meaning of the word “prevention,” while disoriented when reading the word “preventive,” as illustrated in the following quotes. P4: “I would lean more to prevention that preventive, cause in the drug world it is clear that prevention, that is help.”
P5: “I think prevention is definitely a better word.”
Prototype modifications
Following the first focus group, significant changes were made to the referral card and webpage based on participant feedback. Language on the referral card was altered to remove the unfamiliar term “preventative” and the word “study” to describe the program. Additionally, text size was increased across the entire card with key terms bolded for further emphasis. The webpage layout was also changed to have the sign-up form more prominently located above educational video content. A question was also added to the sign-up form that would allow individuals to select which services they were most interested in receiving, including HIV testing, HCV testing, Narcan training, and opioid use counseling.
Focus group #2
Perceived utility
In the second focus group, P4 and P7 noted that consistent access to the program services offered could mitigate barriers to care for people experiencing drug dependence: P4: “Yeah once you get treated you might fall back into addiction but with all these services maybe that can help them stay clean.”
P7: “Yeah there are some places that won't even treat you until you are six months clean.”
Additionally, P2 and P4 discussed the noticeable demand for hepatitis C testing within their communities: P2: “There are people literally crying out to get tested for hepatitis C. They are willing to take the test no problem, and the information is pretty clear that there is a cure for it. They can't really have a normal life with HepC, not only is there an addiction but knowing HepC is treatable can help them with addiction and not being depressed.” (Table 1)
P4: “I just had a situation where my daughter's boyfriend has HepC. She doesn't have it, she was tested about a month ago but I don't know if she has it yet from sharing the needle. I don't know how he has it and she doesn't. I know a lot of people need to be tested.”
Usability/accessibility
Participants also asked whether they would have to call to make an appointment before accessing services at the clinic. When notified that calling ahead was necessary, one participant identified the benefits of having an open phone line to call for support and care navigation: P5: “They need to be mentally ready to get there, so maybe another thing could be a hotline where you could talk to somebody and they could urge you to go get tested as well. Sometimes you don't have a way out or people to talk to. We teach each other about support groups and working with each other but sometimes you might not want to share their health information with somebody so a hotline or possibly specifying on the card that there is help and there is someone to guide you through it might be good as well.”
However, two participants expressed concerns about calling to make appointments: P4: “If I call this phone number am I gonna get press 1, press 2, etc? That makes me angry when you have to wait forever just to get the answers to simple questions like where to go and what to do.” (Table 2)
P5: “Sometimes knowing there is someone there who cares is enough. I hate the automated this and that.”
Tool design
When asked to compare the first iteration of the peer referral card to the second iteration, at least three participants responded favorably to the new version: P3: “Yeah I like the new one better.” (Table 3)
P2: “Yeah I think it's clear”
P5: “Again we are talking about addiction with the memory and loss of focus. I think this new one is way better than the first one.”
Yet, two participants still expressed concern about the text size and text color on the card: P5: “But the print is not big enough for some people with eye problems or if you were actually high. In our world, you run into people using all over the place, so information to help is what everybody is looking for…If I’m high then color is what is going to catch my attention. Short, sweet, and bold.”
P2: “Us drug addicts we don't read very well or see very well.”
All participants agreed that the program's affiliation with healthcare is important to ensure privacy and legitimacy, as represented in these quotes from three participants: P5: “Yeah they need to know that you are working in health because in health everything is confidential.”
P2: “This is a good hospital.”
P3: “Everyone knows it is one of the top ones.”
Overall, participants said that the business-card size was preferable to easily carry with them and keep track of the program information. P6: “I think it is good the card is this size.”
P5: “This card I have from Healthcare for the Homeless is that size and it is good because it has their contact information but also the date of the last time you got tested. It's hard to remember sometimes. Something as important as your health, it is important to be able to keep up with those things. I wouldn't be able to give you that date from my mind.”
When discussing the services offered at the clinic, one participant expressed that it would be helpful to have more information on the card describing which tests and treatments were available for free: P1: “I think you should put exactly what you are testing for and if there is more, add more.”
Two other participants also responded favorably to a new question on the website form that allows peers to select which services they are interested in during the referral process: P5: “Yeah because then you could also break it down to see what people need the most”
P2: “Yeah I like being able to pick and mark which services.”
Clarity/readability
In the second focus group, P2 was confused by the acronym “HCV” and did not immediately associate the acronym with hepatitis C virus when looking over the materials: P2: “Can I say something? Well, first of all, I have no idea what ‘HCV’ means. I assumed it was hepatitis C… What I am trying to say is that everybody out there is interested in curing their HepC and there is enough press these days about how you can cure HepC easily. So if the ‘HCV’ could be worded in a way that screamed HepC.” (Table 4)
One participant in the second focus group expressed uneasiness with the inclusion of the words “research” and “study” on the referral card: P4: “Do you have to put the research on there? Because I think some people might think that they are going to be a guinea pig or something. I mean of course you would study them, because that is what I think you wanna analyze.”
P4: “Yeah so the focus should be testing is the whole thing, not researching.”
Prototype modifications
Participants in the second focus group validated changes made following the first session, with recommendations for minor changes to the peer-referral card and webpage. On the card, we changed the abbreviation “HCV” to “HepC” since this was more easily recognized as hepatitis C. While participants continued to express uneasiness with the word “research”, we felt it was important to identify the hospital's ED Research Team as the main point of contact for the program. The hospital logo remained prominently visible on the card to ensure legitimacy, while text size could not be further augmented while including the necessary information on such a small card. Lastly, the nickname identifier in the referral link was changed to a unique referral code. Although the nickname was not intended to be the individual's actual name, a completely depersonalized code was decided to be a better approach given participants’ privacy concerns.
Use-case session
A third and final iteration of the prototype and program materials was created based upon participant feedback from the first and second focus group discussion sessions. During the use-case session, participants attempted to refer another participant to the program using the provided materials and website prototype.
All nine participants were familiar with QR codes; however, only two participants were able to scan the codes using their mobile phones without downloading another application. The inclusion of the webpage link on the referral card allowed for the participants to bypass the QR code by typing the link into their internet browser. This was a source of frustration, as the participants who were unable to use the QR code would prefer the code to take them straight to the webpage rather than having to type in the full URL.
Once on the website, all participants were easily able to fill out the embedded form and watch the informational video. Participants felt that the website was formatted well for their mobile browsers, and the video was able to be played regardless of mobile phone manufacturer or operating system. All participants agreed that more information on the exact services being offered would make the website more informative.
Once the participants signed up on the website form, study staff sent SMS messages to each participant with example instructions for scheduling appointments. When asked about privacy, all participants found it favorable that no personal information was required to complete the referral process.
Discussion
The two focus groups and one use-case session conducted in this study enabled the refinement of a mHealth patient-to-peer referral tool designed to connect local community members with a history of injection drug use to relevant HIV, HCV, and opioid use public health and prevention services. Participants not only emphasized the need for these services among their peers but also highlighted the importance of privacy, convenience, and clarity in connecting them to care. Through the utilization of an iterative human-centered design process, we developed a final prototype that protected patient privacy while facilitating linkage to services. The results of this study were crucial to the formation of our specific program and tool design, yet the insights shared during feedback sessions can also be widely applied to future linkage to care or referral to interventions for similar target populations.
Throughout the sessions, study participants discussed current technological access, communication preferences, and language accessibility. They all stated that they have continual and stable access to text messaging and the internet via mobile phones, even for those with government phones distributed to low-income individuals. Although discussion of communication via the internet or text message was largely positive, conversations around calling to make appointments rendered some participants concerned. They commented on the frustrating nature of not being able to reach someone or having to navigate an automated phone menu in their attempts to seek care. Participants responded much more favorably to the idea of a consistently open hotline for support and making appointments. When reviewing program materials, some participants were confused by words such as “preventive” and the abbreviation “HCV.” They were also not immediately aware of which health services would be provided via the program and preferred a list of all the available services on the card. These insights informed the simplicity and clarity of the final prototype iteration, which included clear language and allowed patients to select the services they were interested in on the website form.
The utilization of QR codes to facilitate the referral process was met with mixed reactions from study participants. Although most participants expressed familiarity with QR codes and how to scan them during the focus groups, the use-case session was not reflective of these initial discussions. Only one out of four dyads in the use-case session were able to successfully scan the QR code without assistance, which is concerning for the eventual usability of the prototype. At the time of the study, QR code readers were not built into many Apple and Android mobile phone cameras. Thus, some participants had difficulties due to differences between the operating systems of their phones and did not want to download a separate QR code reader application. The inclusion of a URL on the card was beneficial as a back-up option to the QR code but was less convenient and frustrating to type in for participants. QR codes have been utilized extensively in the area of health education, 26 but there is no current research exploring the use of QR codes for linkage to preventive care services. In the case of our intervention, more use-case testing with potential program participants may be required to determine the viability of using QR codes in our referral process.
Discussions of privacy and stigma during the sessions also elucidated significant considerations for the design of the patient-to-peer referral tool. The anonymity inherent to the program design was initially met with favorability as participants described their desire to keep health information private. Yet even with the anonymous referral method, there was some concern regarding the words “study” and “research” on program materials. This feedback revealed a certain level of mistrust from the community toward human subjects research, which may be a remnant of historical tensions between medical research and disenfranchised communities.27,28 Although research language caused uneasy feelings, the affiliation with the world-renowned hospital bolstered trust in the program since participants associated confidentiality with the healthcare system. Ultimately, we combined these participant perspectives to emphasize our healthcare affiliation and free services on program materials, while keeping the association with research more discrete. Participants also echoed the need for this program in the face of stigma from other healthcare organizations that have sobriety requirements that prevent individuals from accessing essential health services. Our program design in its final iteration was able to facilitate a destigmatized referral process but will need improvement in the future to provide continual access to services for those with the greatest barriers to treatment access.
The visual design of the program materials evolved significantly throughout the focus group sessions. Participants were consistently pleased with the business card size and presence of the hospital logo but were adamant about using bolder fonts and brighter colors. They emphasized the need for the card to catch individuals’ attention and be easily readable for those who are visually impaired or under the influence of substances. Although the second and third iterations of the tool had increased visual accessibility, much of the information on the back of the card could not be augmented or bolded due to space limitations. Participants also found short, informational videos on the website preferable to a paragraph of text since videos were better able to catch their attention, and they could easily share it with peers. However, they also recognized that having the sign-up form above the video on the webpage would be best to facilitate the most referrals. We incorporated most of the participants’ feedback into the visual design by the final prototype, and the card and web page designs were not a source of difficulty or confusion during the use-case session.
The usability of our patient-to-peer referral tool was dependent on a human-centered design process that combined technological practicality with the perspectives of community members. By involving the end-user in the iterative design cycle, we were able to tailor the technology design to meet the unique needs and preferences of our target population. Human-centered design has been utilized in mHealth tool creation to inform the development of targeted interventions,19,29–31 and adopt these principles was paramount to the eventual usability of our final prototype. Involving dyads of participants in this study further strengthened the human-centered design process since our program was focused on the relationship between an index participant and their peers. Previous studies have described the clustering of drug-injection behavior, and couple-based interventions have been shown to be promising approaches in HIV and HCV prevention.32,33 Dyads were particularly beneficial in the use-case session to illustrate a referral between social networks of close friends and family members. Interventions that utilize social networks have been shown to reach and change the behaviors of hard-to-reach populations, including PWID. 34 For HCV prevention specifically, a peer-facilitated point-of-care testing program in Toronto was successful in reaching local individuals who inject drugs for HCV testing and referral to care. 35 Similar social network strategies for HIV testing have not only been effective but also have identified a higher proportion of new cases than traditional testing methods in healthcare settings. 36 Participant feedback throughout our human-centered design process validated the potential of our program to reach the social networks of PWID and connect these at-risk individuals to appropriate testing and care.
This qualitative usability study has several limitations that may affect the interpretation of results. Foremost, the method of participant recruitment did not ensure a diverse sample. This is especially relevant in our study since half of the individuals were friends or family members of recruited participants who likely share similar qualities and life experiences. Although sociodemographic information was not systematically collected, study staff also noted that all participants were middle-aged or older adults. PWID who were in an acute or withdrawal phase of substance use were also ineligible for study recruitment due to their inability for informed consent. The use of incentives in both the study design and program design could have possibly skewed participant feedback throughout the focus group sessions. It may be challenging to discern whether participants found the program to be viable based on its design or its incentive structure. Furthermore, the initial program design and prototype were shown singularly to the focus groups without a point of comparison or reference. Participants may have felt compelled to provide favorable feedback due to social desirability bias along with the incentives they received for participation.
Conclusion
The findings of this mHealth tool usability study suggest a patient-to-peer referral tool could be a feasible approach to linking community members at risk for injection drug use to HIV, HCV, and opioid use-related services from ED patients. The human-centered design process applied throughout the focus group sessions facilitated the inclusion of unique privacy, design, and technological considerations in our final usable prototype. The methods utilized and perspectives gathered in this study may be useful for developing future mHealth innovations that seek to connect similar difficult-to-reach populations to services.
Supplemental Material
sj-doc-1-dhj-10.1177_20552076221143238 - Supplemental material for Human-centered design development of mHealth patient-to-peer referral tool in the emergency department
Supplemental material, sj-doc-1-dhj-10.1177_20552076221143238 for Human-centered design development of mHealth patient-to-peer referral tool in the emergency department by Zak Hyde, Raúl Roura, Kesav Varanasi, Tanner McGinn, Julie Evans, Benjamin Verschoore, Cui Yang, Alain Labrique, Erin P Ricketts, Richard E Rothman, Carl A Latkin and Yu-Hsiang Hsieh in Digital Health
Footnotes
Acknowledgment
The authors would like to thank the study participants for sharing their thoughts with us.
Contributorship
Y-HH, RER, JE, CY, AL, and CAL contributed to the conception of the study and study design. KV and ZH developed and designed the prototype of the patient-to-peer referral tool. ZH, KV, TM, BV, and EPR contributed to patient enrollment and conduct focus group discussion sessions and the user session. ZH transcribed the discussion sessions. ZH, RR, and Y-HH analyzed and interpretation of data. ZH and RR drafted the manuscript. Y-HH and CAL contributed to the significant revision of the manuscript. All the authors read and approved the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
This study was approved by The Johns Hopkins University School of Medicine Institutional Review Board (IRB00162605).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Center for AIDS Research, Johns Hopkins University (grant number P30AI094189).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.