
Abstract
Background
In the digital era, parental digital competence is being recognized to be essential for effective parenting and improved child health. To address a gap in existing tools that lack specificity for assessing digital competence within the childcare context, this study aimed to develop and validate a novel Parental Digital Competence Scale (PDCS).
Methods
The PDCS was developed through a four-phase process: (1) Clarifying the content to be measured based on the European Commission's Digital Competence Framework; (2) Creating an item pool through a literature review; (3) Refining items with expert panel feedback and a pilot test; and (4) Conducting a psychometric validation to evaluate item characteristics. The validation study included 477 family caregivers selected from Northwest China. Construct validity with exploratory (EFA, n = 248) and confirmatory factor analysis (CFA, n = 229) was carried out to identify the factor structure of the scale. Convergent and discriminant validity were evaluated. The reliability was assessed through internal consistency, split-half reliability, and test–retest reliability.
Results
Twenty-three items were included in the final instrument. The content validity index of the PDCS reached 0.975. The EFA results revealed a three-factor structure that explained 80.499% of the total variance. The CFA results further demonstrated that the second-order three-factor model achieved a satisfactory fit. The final version of PDCS included three dimensions: Digital Methods Application, assessing parents’ skills in leveraging digital tools for information creation, problem-solving, and communication; Digital Security, covering online safety, privacy protection, and responsible digital behaviors; and Information Retrieval and Evaluation, measuring parental ability to locate, understand, and critically appraise online child-related information. The PDCS demonstrated high internal consistency (Cronbach's α = 0.981).
Conclusions
The PDCS seems to be a valid and reliable tool. Its potential application enables researchers to identify parental digital competence gaps, track improvements following targeted interventions and promote safer, more productive digital family environments.
Introduction
Addressing child development and health is a significant aspect of the Sustainable Development Goals. 1 Although global survival rates for children under the age of 5 have improved in recent decades, more than 250 million children in low- and middle-income countries still face the risk of not reaching their developmental potential. 2 As child health services shift toward more proactive, empowering, and family-centered approaches, the role of parents and family caregivers in promoting child development and health has become increasingly crucial. 3 It is essential to prioritize and support their involvement to ensure that children can reach their full developmental potential.
With the ongoing advancement of digital transformation in social and health services, 4 parents are increasingly tasked with managing their children's health and development through the use of digital technology. 5 While this rapid integration presents significant opportunities, 6 it also introduces new challenges for parents, requiring them to develop strong digital competencies to navigate, assess, and apply online health information effectively. Surveys indicate that parents frequently utilize digital technology to access internet-based information on child health, development, and parenting. 7 A study conducted in Switzerland found that nearly all parents (91%) used digital media to obtain child health information, with search engines (55%) and parenting websites (47%) being the most frequently used sources. Approximately 70–80% of parents turned to the internet for guidance on parenting skills, medical insights, and social support. 8 Moreover, healthcare practitioners were increasingly employing digital tools to disseminate information, identify health needs, and implement interventions, thereby enhancing convenience and accessibility for parents. 9 Despite the widespread use of digital resources for child-related health information, associated challenges are gradually emerging. Many parents expressed skepticism about the accuracy of online information, 8 and studies showed that individuals with lower educational or socioeconomic backgrounds tend to access online health information less frequently. 10 A digital divide may exist due to lower digital competence among those with less educational attainment, potentially limiting their ability to locate and critically evaluate relevant information. 11 In light of these challenges, a certain level of digital competence is essential for parents to effectively engage with health services and accurately navigate, assess, and utilize internet-based childcare information. This competence enables parents to make informed decisions and take a proactive role in managing their child's health and development. 12
Digital competence is recognized as a transverse competency that not only enables individuals to acquire other essential skills, but also plays a crucial role in active participation in the socioeconomic fabric of the 21st century. 13 The European Commission's Digital Competence Framework (DigComp 2.2) identifies digital competence as encompassing a comprehensive set of digital skills, including (1) Information and Data Literacy (IDL), (2) Communication and Collaboration (CC), (3) Digital Content Creation (CCr), (4) Digital Security (DS), and (5) Problem Solving (PS). Digital competence is the ability to use these digital skills confidently, critically, and responsibly in specific contexts. 13 In this study, parental digital competence refers to the ability of parents to use these digital skills within the context of child care. Conclusions on parental digital competence have highlighted its role in facilitating access to information and enhancing social status. 14 Parents with limited digital skills may struggle to fully engage and effectively support the care and development of their children. Studies showed that parental digital competence can help improve parents’ comprehension of their children's health needs, as well as providing valuable information and resources to alleviate stress, anxiety, and depression in families with chronically ill children. 15 Furthermore, recent studies indicated that parents with higher digital competence are better equipped to navigate and evaluate digital health information, which can enhance their understanding of child health issues and lead to more effective health management practices. 16 This enhanced access to information supports better-informed decisions regarding preventive care and health interventions, potentially leading to improved child health outcomes. Strengthening parental digital competence improves their capacity to access, communicate, and utilize information related to child care, which has a significant impact on child development and health outcomes. 17
Despite increased awareness for the importance of parental digital competence, a significant barrier to enhancing these skills lies in the absence of specialized assessment tools specifically designed for caregiving contexts. 18 Accurate measurement of parental digital competence provides valuable insights into areas where parents may struggle, such as evaluating the reliability of online health information, effectively using digital communication platforms, or safeguarding digital privacy for both parents and children. By identifying these gaps, it becomes possible to design tailored educational programs and supportive interventions that address parents’ unique needs, enabling them to build the necessary skills to confidently engage with digital technologies. Ultimately, such efforts not only foster greater parental engagement in digital environments but also contribute to improved child care practices, better health outcomes, and a reduction in inequalities stemming from the digital divide. 18
Various digital competency assessment tools have been developed for diverse populations, such as general citizens, university students, and workplace professionals.19–21 However, in the realm of childcare, there is a scarcity of instruments explicitly designed for measuring parental digital competence. Although previous studies on the digital competence of parents or caregivers frequently employed tools designed for general use, such as the Digital Literacy Scale, 22 the Technological Ease and Computer-based Habits Inventory, 23 and the eHealth Literacy Questionnaire, 24 these instruments present significant limitations when applied to the specific context of parenting and childcare. First, almost all of these studies have not systematically evaluated the reliability and validity of these tools within parent populations, raising concerns about measurement accuracy and construct applicability. 25 Furthermore, these tools often lack sufficient content and ecological validity, as they are not tailored to the unique digital tasks and complex decision-making parents face in guiding their children's development, safety, and health in the digital era. 26 Top et al. 22 further highlighted critical skills, such as evaluating pediatric health information amidst misinformation, effectively communicating with healthcare or educational providers via digital platforms, and acting as informed proxies for their children, are largely unaddressed by these generic scales. As a result, reliance on generic digital competence tools may lead to significant construct underrepresentation and measurement bias, ultimately impeding accurate assessment and the development of effective, contextually relevant interventions for families. 27 While Alharbi et al. 18 developed a digital skills scale specifically tailored for parents, its design was inherently shaped by the urgent digital demands imposed by the rapid shift to remote schooling during the COVID-19 pandemic. This instrument predominantly evaluated operational and instrumental proficiencies relevant to parents’ management of online education platforms and related communication. Consequently, this narrow and crisis-specific focus may limit its capacity to comprehensively capture the broader, more nuanced, and multifaceted digital competence parents require in everyday contexts.
To address the lack of tools specifically tailored for assessing parental digital competence in the context of childcare, this study aimed to develop and psychometrically validate a novel Parental Digital Competence Scale (PDCS). The content and outcomes to be measured by the PDCS derive from the five domains outlined in the DigComp 2.2 framework, focusing particularly on scenarios where parents interact with digital resources related to child health, development, and parenting. The scale is intended for use by both researchers and practitioners to identify gaps in parental digital competencies and to track improvements in parental digital skills through targeted interventions.
Methods
Following the scale development guidelines published by Devellis et al., 28 the PDCS was developed through a structured four-phase process, as illustrated in Figure 1. In Phase 1, the target population and the content to be measured were identified, with reference to the DigComp 2.2 framework for clarity. In Phase 2, an item pool was generated through a thorough review of relevant literature. In Phase 3, the initial scale underwent expert review, leading to modifications based on their feedback. The refined instrument was subsequently pilot-tested to screen items. In Phase 4, the psychometric properties of the scale were further validated, resulting in the final version of the scale.

Diagram for the procedures followed to develop the Parental Digital Competence Scale.
Development stage
Phase 1: Conceptual framework
Utilizing the DigComp 2.2 framework, 13 which was widely recognized and highly adaptable across various regions and age groups, 29 we identified the content and outcomes to be measured by the PDCS. These cover five dimensions of essential digital skills: IDL, CC, CCr, DS, and PS. Concurrently, we consulted studies that focused on the development or examination of digital competence instruments for different demographic groups, including undergraduate students, 19 teachers, 20 young individuals, 21 and parents. 18 This contributed to further enriching and refining the definitions and connotations of these dimensions. Supplemental Table S1 outlines the scale size, target subjects, countries, dimensions, and definitions of each dimension from the studies cited. In addition, by collaborating with experts in child healthcare, the research team synthesized insights from these studies and considered the specific healthcare and parenting needs of parents within a digital environment to adapt the dimensions and connotations for the childcare context.
In this study, parental digital competence refers to the holistic capacity of parents to confidently, critically, and responsibly leverage digital technologies and resources within the childcare context, thereby ensuring effective support for their children's health, development, and parenting practices. IDL represents parents’ ability to retrieve, comprehend and critically evaluate child-related digital information. CC relates to parents’ proficiency in communicating in a digital environment, sharing child-related digital resources, and engaging in online community interactions. CCr involves parents’ capability to process child-relevant images and videos, integrate prior knowledge and content, and generate or modify new digital content. DS encompasses parental competence in protecting personal privacy, digital identity, and overall security, as well as responsible online behavior. PS relates to the selection and application of digital technology to address childcare problems effectively.
Phase 2: Item generation
Item development began with a thorough review of research on the definitions and measurement of digital competence in childcare settings. The initial item pool was developed by a research team of seven researchers, including two professors in the field of childcare, three PhD students and two MSc students. Through an extensive literature review, the team integrated items related to the application of digital technologies from previous instruments, eliminating or combining those with overlapping meanings. Following these stages, an item pool consisting of 25 items and covering five dimensions was generated, including four items in IDL dimension, three items in CCr dimension, eight items in PS dimension, five items in CC dimension, and five items in DS dimension.
Phase 3: Item modification
Modified expert panel
A collaborative committee comprising 14 experts specializing in pediatric health service (six experts), smart health monitoring (two experts), digital healthcare (two experts), public health (two experts), and scale development (two experts) was established. The inclusion criteria involved at least 10 years of experience in pediatric care, familiarity with child healthcare provision, and possession of an intermediate or higher professional qualification. The demographic characteristics of these experts are detailed in Supplemental Table S2. The experts had an average of 23.07 ± 5.44 years of professional experience and an average age of 46.25 ± 4.81 years, with all holding a master's degree or higher. Most experts had relevant research experience with digital competence or the DigComp 2.2 framework. Several members had also contributed to the development of a Nursing Digital Application Skill Scale based on the DigComp 2.2 framework, 30 which further ensured their familiarity with its structure and application. Before the consultation, the Expert Consultation Form provided a detailed overview of the DigComp 2.2 framework and the study's objectives, ensuring that they were well-prepared to offer informed and valuable feedback on the study.
The experts were tasked with evaluating the content validity of the scale, providing valuable feedback on the suitability, clarity, and difficulty of the items. Experts evaluated the importance of each item using a 5-point Likert scale, ranging from 1 (“not important”) to 5 (“extremely important”) for item validity. The Content Validity Index (CVI) was computed for both individual items (I-CVI) and the overall scale (S-CVI). Items were considered valid if they received ratings of 4 or 5, with an overall S-CVI > 0.90 and I-CVIs > 0.78. 31 Items falling below these thresholds were flagged for further review. A dedicated section for comments was incorporated into the review form, enabling experts to provide detailed suggestions, note ambiguities, and propose alternative phrasings. For items that were flagged, one-on-one discussions were conducted with the experts who raised specific concerns. These discussions, combined with subsequent internal deliberations among the research team, led to final decisions regarding the deletion or modification of certain items. Based on expert feedback, two items in the Problem Solving dimension were removed. Additionally, it was suggested to rename the “Information and Data Literacy” dimension to “Information Retrieval and Evaluation.” Finally, the preliminary version of the PDCS comprised 23 items.
Pilot test
The preliminary version of the PDCS underwent a pilot test involving 30 family caregivers from Northwest China, selected via convenience sampling. All participants completed the scale and participated in interviews to identify any ambiguous or unclear items, leading to necessary wording revisions. The interview outline included the following questions: Q1. Do you have any suggestions for improving the instructions of the scale? Q2. Which items did you find difficult to understand? And Q3. Do you have any recommendations for refining the wording of the items?
Validation stage
Phase 4: Validation of the scale
The psychometric properties of the PDCS were assessed. Reliability was determined using internal consistency, split-half reliability, and test–retest reliability. An exploratory factor analysis (EFA) was conducted to determine the factor structure of the PDCS. Additionally, convergent and discriminant validity were examined. Given the absence of a criterion (or “gold standard”) for parental digital competence, we hypothesized, based on prior research, that higher levels of parental education and income would correlate with enhanced PDCS scores. 32
Research design
A cross-sectional study was conducted between August 2023 and October 2023 across four kindergartens in Northwest China, encompassing both urban and rural districts.
Participants
The primary family caregivers, comprising parents, grandparents, and other caregivers of children, were the targeted participants. Each family was represented by a single primary caregiver, selected for their consistent and close interaction with the child. The digital competence of these caregivers influences their ability to access and use child-related health information, which is crucial for supporting the child's well-being and fostering informed health practices.
Inclusion criteria required participants to be capable of both verbal and written communication with investigators, alongside a willingness to participate. The exclusion criteria comprised acute or severe illnesses. Participants with chronic diseases were not specifically excluded unless their condition was unstable or significantly interfered with their daily functioning. To validate the preliminary version of the PDCS, we ensured that the sample size for EFA was at least five times the number of items in the scale. 33 A total of 477 participants were recruited and administered the questionnaire.
Instruments
The preliminary version of PDCS
The initial 23-item PDCS utilized a 5-point Likert scale for scoring. Participants responded to each item on the scale with a rating that reflected their frequency of engaging in certain digital competence-related activities or demonstrating specific skills. Responses were rated as follows: 5 = “almost always,” 4 = “often,” 3 = “sometimes,” 2 = “rarely,” 1 = “never.” The overall score was calculated by summing the scores of each item, with a higher total reflecting greater digital competence in the respondent.
General information questionnaire
Sociodemographic data of children and their parents were obtained with the General Information Questionnaire that we designed. The questionnaire covered details, including the relationship to the child, the child's and caregiver's age, the child's gender, the caregiver's education, occupation, residence, monthly household income per person, only-child or not, channels for accessing child health information and caregivers’ reports of children's health status.
Data collection
To select the participants, we collaborated closely with the kindergarten administration to identify eligible families. Invitations to participate in the study were issued during a parent–teacher conference, allowing families to voluntarily participate after a clear explanation of the research objectives and procedures. Written informed consent was obtained from all participants. We emphasized maintaining anonymity and confidentiality, assuring participants of their right to withdraw at any time without repercussions. Following recruitment, participants completed questionnaires distributed via an online link (https://www.wjx.cn/). The study received ethical approval from the Ethics Committees of Xi’an Jiaotong University (No. 2021-1511). All procedures performed in studies involving human participants were in accordance with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Data analysis
Statistical Package for the Social Sciences (SPSS) version 19.0 and Amos version 23.0 were utilized for data analysis. Demographic variables were statistically described through frequency tables, means, and standard deviations (SD). Item analysis was conducted to evaluate the appropriateness of individual items in the scale using extreme group testing. Participants were divided into high- and low-scoring groups based on the top 27% and bottom 27% of total scores, and an independent samples t-test was used to compare the mean scores of each item between these groups. The critical ratio (CR) of the item was obtained. A CR greater than 3, along with statistically significant differences (p < .05) between the high and low groups, indicates that the item has adequate discriminative capacity. 34 Internal consistency was assessed using the Cronbach alpha coefficient. The Cronbach's alpha value of 0.7 or higher was deemed adequate. 35 Two weeks after the first survey, 30 participants who had completed the first survey were recruited to fill out the same scale once more to measure the test–retest reliability of the scale. Test–retest reliability was ascertained through the intraclass correlation coefficient (ICC) for both the entire scale and its individual dimensions. 36 ICC values ranging from 0.5 to 0.75 indicated moderate reliability, values between 0.75 and 0.9 indicated good reliability, and values greater than 0.90 indicated excellent reliability. 37 Split-half coefficient reliability was assessed using half of the odd and even items.
The total sample (n = 477) was randomly divided into two subsets using SPSS version 19.0, with one subset (n = 248) allocated for EFA and the other (n = 229) for confirmatory factor analysis (CFA). This split-sample approach allowed for independent validation of the factor structure across two distinct samples. 38 The sample sizes for both EFA and CFA met commonly recommended guidelines, requiring samples to be at least five times the number of items in the scale (in this case, >115) and no less than 200, as recommended by Kline. 39 EFA was conducted to ascertain the scale's factor structure, employing principal component analysis (PCA) and Varimax rotation. 40 The number of factors was determined using the following approaches: (a) factor-loading coefficients and the Kaiser Criterion (factor-loading coefficients exceeding 0.50, along with extracted factors having eigenvalues greater than or equal to 1.0), (b) the “elbow” point in the scree plot, (c) the factor meaningfulness. Items with communalities below 0.30, loadings below 0.50, or those loading on multiple factors should be excluded.41,42 CFA was performed using Amos V.24.0 software to further validate the factor structure and determine whether the dimensions appropriately represent the intended construct. The model fit was evaluated through the following indices: chi-square/degrees of freedom (χ2/df) < 3, standardized root mean square residual (SRMR) ≤ 0.08, Parsimony Comparative Fit Index (PCFI) and Parsimony Goodness-of-Fit Index (PGFI) > 0.50, Comparative Fit Index (CFI), and Incremental Fit Index (IFI) > 0.90. 42 For complex models, a χ2/df value of <5 is also considered acceptable. Factor loadings were assessed with a threshold of 0.5. 43 Additionally, Composite Reliability (CR) and Average Variance Extract (AVE) values were computed for each factor to evaluate convergent validity. CR values greater than 0.70 44 and AVE values exceeding 0.50 were considered acceptable. 42 Discriminant validity was evaluated using the Fornell–Larcker criterion. 45 The significance level was set at p < .05.
Results
Development stage
Item modification and content validity
The expert panel reviewed the 25-item pool and confirmed its comprehensive coverage of the necessary digital competencies for parents. The S-CVI reached 0.975, indicating excellent content validity. I-CVIs were above 0.78, with the exception of Item 9 (I can complete the digital tasks assigned by the kindergarten.) and Item 15 (I am willing to let children learn some digital skills.) in the Problem Solving dimension. Experts deemed Item 9 as too broad and nonspecific, and Item 15 as reflective of parental attitude rather than competence. Consequently, these items were removed for their low validity.
The expert review led to the rephrasing of three items: (1) Item 10: Originally stated as “I can identify and choose appropriate digital resources according to the specific requirements of childcare,” it was deemed overly complex and in need of clearer focus. After discussions within the research team, it was revised to “I can select digital resources based on parenting needs.” (2) Item 14: The original phrasing was “I can use digital technologies to make health-related decisions for children.” Experts recommended replacing the word “make” with “support” to better highlight the role of digital tools as facilitators rather than sole decision-makers. The revised item reads, “I can use digital technologies to support health decision-making for children.” (3) Item 17: The original item stated, “I can proficiently use social media platforms for communication and interaction.” Experts suggested shifting the emphasis from technical proficiency on specific platforms to a broader assessment of digital communication skills. As a result, the item was revised to “I can communicate effectively with others on the Internet.” Additionally, experts suggested renaming the “Information and Data Literacy” dimension to “Information Retrieval and Evaluation (IRE)” to emphasize the greater importance of parents’ proficiency in retrieving and evaluating digital information over understanding data-related concepts. A summary of the expert feedback on the scale items is provided in Supplemental Table S3. Finally, the initial version of the scale consisted of 23 items, including four items in the IRE dimension, three items in CCr dimension, six items in PS dimension, five items in CC dimension, and five items in DS dimension.
Pilot test
The pilot study included 30 family caregivers: 23 mothers (76.7%), six fathers (20.0%), and one grandparent (3.3%). The caregivers had a mean age of 34.90 ± 6.71 years, while the children had a mean age of 5.38 ± 1.08 years. 53.3% (n = 16) of the caregivers had attained a university degree or higher level of education, and 56.7% (n = 17) of the children were girls. Regarding occupational status, 10 (33.3%) caregivers were employed by state organs, enterprises, or institutions; three (10.0%) were workers or service employees; three (10.0%) were self-employed; six (20.0%) were involved in farming; and eight (26.7%) held other occupations. Additionally, 16 (53.3%) participants resided in urban areas.
All participants completed the scale in less than 12 min. Several participants expressed difficulty in understanding the term “digital.” To address this issue, clarifying instructions were added at the beginning of the scale, defining “digital” to include various aspects of digital technology, such as web browsers, social media, and communication through smartphone apps. Additionally, some participants suggested that arranging simpler, more easily understood items at the start of the scale would help alleviate any apprehension associated with the assessment. Based on this insight and subsequent discussions within the research team, we adjusted the item sequence. Specifically, we repositioned the item “I can search for information on the Internet” to the beginning of the scale. These modifications were implemented to improve clarity, enhance the overall respondent experience, and ultimately strengthen the validity of the assessment instrument.
Validation stage
Social and demographic characteristics of participants
Table 1 presents the social and demographic characteristics of the participants, along with their overall PDCS scores. The study included 477 participants: 332 mothers (69.6%), 120 fathers (25.2%), and 25 grandparents and other caregivers. Caregivers and children had a mean age of 34.10 ± 6.589 years and 5.19 ± 0.820 years, respectively. 54.9% (n = 262) of caregivers attained a vocational school or higher education. 50.1% (n = 239) of the participating children were boys. In addition, 41.3% (n = 197) of the participants reported a monthly household income exceeding RMB 3000 per person. Three hundred seventy-seven participants (79.0%) reported using digital technologies to obtain health information. Other commonly used sources included healthcare professionals (62.7%), family and friends (51.4%), lectures or training (39.6%), and print media (41.9%). The findings indicated that caregivers with higher education levels, higher monthly incomes, urban residences, employment in state organizations, enterprises, or institutions, and those who rated their children's health as very good scored higher on the PDCS (p < .05).
Demographic characteristics and the overall PDCS a scores of participants (n = 477).

PDCS: the Parental Digital Competence Scale.
Item analysis
The PDCS items were categorized into high and low-scoring groups based on participants’ total scores, with the top 27% comprising the high group and the bottom 27% comprising the low group. Subsequently, an independent samples t-test was used to compare the mean scores of each item in these groups and determine the CR for each item. As shown in Table 2, the results indicated a statistically significant difference in item scores between the high and low groups (p < .001). All items displayed a CR greater than 3, denoting significant discriminative capacity without floor or ceiling effects. At this stage, no items were excluded.
Item analysis of the parental digital competence scale (n = 477).

CR: critical ratio.
Independent samples t-test.
Construct validity
Exploratory factor analysis
The total data (n = 477) were randomly split into two subsets. EFA was conducted on the first subset of 248 samples, encompassing all 23 items. PCA was employed as the extraction method, chosen for its effectiveness in data reduction and identifying underlying dimensions in novel scale development. 33 Varimax rotation was subsequently applied. This orthogonal rotation method was selected for its ability to produce a simple structure, yielding a clearer and more interpretable factor solution where items load distinctly on single factors, which was beneficial for conceptually defining the emergent dimensions. 46
The correlation matrix verified an adequate sample size (Kaiser–Meyer–Olkin measure was 0.960), and the Bartlett test (χ2 = 7388.486, p < .001) rejected the zero-correlations hypothesis. Following Kaiser's criterion, a three-factor structure (see Figure 2) was identified (Factor 1 = 16.147, Factor 2 = 1.317, Factor 3 = 1.051), accounting for 80.499% of the data variance. The first factor explained 33.880% of the variance, which was below the commonly referenced 40% threshold for common method bias. 47 The second and third factors explained 24.054% and 22.565% of the variance, respectively. As shown in Table 3, factor loadings for the scale items ranged from 0.557 to 0.836, all exceeding the threshold of 0.50. Each item's communality value was above 0.702, surpassing the acceptable minimum of 0.30, with no items loading on multiple factors. 42 The combination of the scree plot results (see Figure 2), the Kaiser criterion (eigenvalue) and the factor meaningfulness led to the identification of a three-factor structure. Factor 1, encompassing items 5–8, 10–14, and 16–20, was renamed the “Digital Methods Application (DMA)” dimension as it included all items from the CCr, PS, and CC dimensions. Factor 2 comprised five items (items 21–25) from the DS dimension, and Factor 3 included four items (items 1–4) from the Information Retrieval and IRE dimension.

Scree plot of the PDCS (n = 248).
Factor loadings on items of the PDCS a (n = 248).

PDCS: the Parental Digital Competence Scale.
Confirmatory factor analysis
The second subset of 229 samples was then subjected to CFA using maximum likelihood (ML) estimation to verify the factor structure derived from EFA. ML estimation provides efficient and consistent parameter estimates, enabling rigorous hypothesis testing of the proposed model's fit through various goodness-of-fit indices. 38
Initially, two models were tested: a first-order three-factor model derived from EFA and a one-factor model. As shown in Table 4, results indicated that the first-order three-factor model generally met psychometric standards (with the exception of CFI and IFI) and demonstrated superior fit compared to the one-factor model, suggesting that the three-factor structure provides a more reliable representation of the construct. High inter-factor correlations (0.822, 0.779, and 0.845) in the first-order model indicated the potential relevance of a second-order factor.
Fit indices of confirmatory factor analysis (n = 229).

Note: SRMR: standardized root mean square residual; PGFI: Parsimony Goodness-of-Fit Index; PCFI: Parsimony Comparative Fit Index; CFI: Comparative Fit Index; IFI: Incremental Fit Index.
Consequently, a second-order three-factor model was established, and results showed that model fit indices were consistent with those of the first-order three-factor model. This outcome aligns with findings by Haozheng Qiu, 48 where equivalent fit indices are obtained when three correlated first-order factors are replaced by a single higher-order factor, as degrees of freedom remain unchanged in such cases.
To further improve the fit of the second-order three-factor model, modification indices were applied to guide necessary adjustments. These modifications resulted in enhanced fit indices, with all values meeting acceptable standards in the modified model: χ2/df = 3.915, SRMR = 0.040, PCFI = 0.797, CFI = 0.901, and IFI = 0.901. As shown in Figure 3, all factor loadings in the second-order three-factor model exceeded 0.50, indicating that each observed item strongly corresponded to its respective latent variable. The modified second-order three-factor model provided a satisfactory fit, supporting the use of a higher-order factor structure. This outcome permits the interpretation of the PDCS as a comprehensive construct with three dimensions that can be summed into a total score, representing overall parental digital competence.
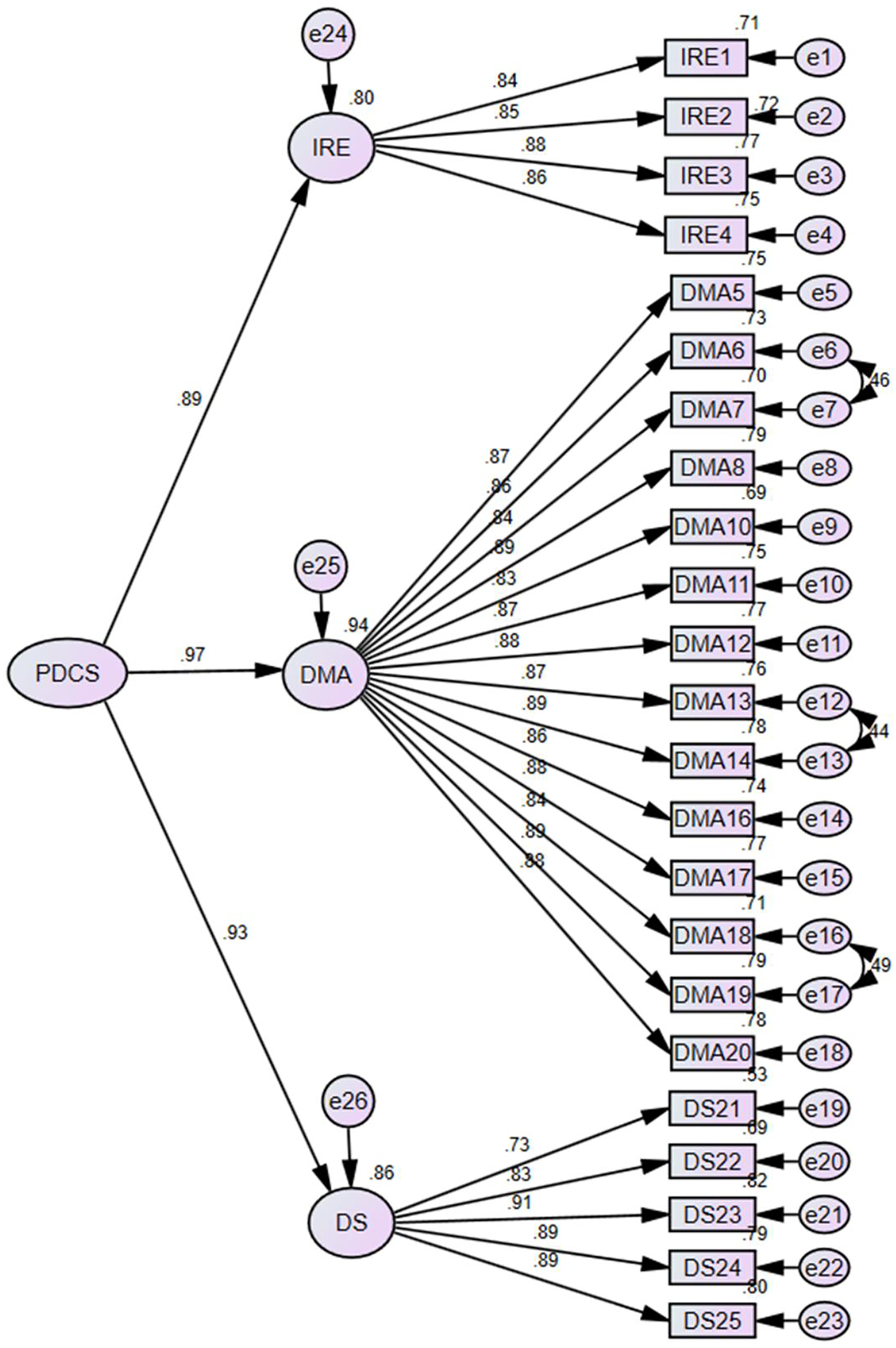
A schematic diagram of standardized model fitting of the scale (n = 229).
The progression from identifying distinct components through EFA to rigorously validating a higher-order, integrated structure through CFA is a standard psychometric approach in scale development. 28 While EFA initially helped delineate conceptually distinct facets of parental digital competence for clarity during scale development, the subsequent CFA, revealing high interfactor correlations among the first-order factors, provided empirical support for a second-order factor. 38 This hierarchical structure suggests that these dimensions, though distinct, are interrelated and collectively contribute to an overarching construct of Parental Digital Competence.
Convergent and discriminant validity analysis
Convergent and discriminant validity were evaluated using the CFA model with the 229-sample subset. The results indicated that the standardized regression weight of the standardized factor loading values ranged from 0.729 to 0.968 (see Table 5). Composite reliability (CR) values varied between 0.918 and 0.977, while average variance extracted values varied from 0.726 to 0.865, satisfying the standard criteria (CR > 0.7, AVE > 0.5). 44
Convergent validity of the parental digital competence scale (n = 229).

PDCS: the Parental Digital Competence Scale.
IRE: the dimension of information retrieval and evaluation.
DMA: the dimension of digital methods application.
DS: the dimension of digital security.
CR: composite reliability.
AVE: average variance extracted values.
Discriminant validity was evaluated using the Fornell–Larcker criterion, 45 which involved comparing the square root of the AVE value for each dimension with the corresponding correlations between dimensions. According to Fornell and Larcker, 45 discriminant validity was achieved when the square root of the AVE of each dimension was greater than its correlations with other dimensions. The square root of the AVE values for dimensions of IRE, DMA, and DS were 0.859, 0.867, and 0.852, respectively, which were greater than all correlations between the factors of the PDCS (see Table 6). This result confirms the discriminant validity of the scale.
Discriminant validity of the parental digital competence scale (n = 229).

Represents the square root of the average variance extracted values of each dimension.
Reliability
The 23-item PDCS demonstrated robust internal consistency (Cronbach's α = 0.981) and split-half reliability (Spearman–Brown coefficient = 0.958). The ICC value for the scale was 0.840, indicating good test–retest reliability. 37 For the three dimensions, Cronbach's α coefficients were 0.978 for DMA, 0.923 for DS, and 0.926 for IRE, respectively. The Spearman–Brown coefficients were 0.951 for DMA, 0.921 for DS, and 0.928 for IRE. The test–retest reliability coefficients were 0.828 for DMA, 0.751 for DS, and 0.741 for IRE (see Table 7).
Reliability analysis of the PDCS a (n = 477).

PDCS: the Parental Digital Competence Scale.
Discussion
In the present study, we developed and validated a novel parental digital competence scale. The PDCS was designed to assess parents’ digital competence, focusing on their ability to use digital technology to access and critically evaluate childcare information, communicate in digital environments, and maintain digital security. It may serve as both a trait measure and a process assessment, with the potential to track improvements in digital skills during specific interventions. The final 23-item PDCS encompasses three dimensions: Information Retrieval and Evaluation, Digital Methods Application, and Digital Security. It covers a range of content areas, making it suitable for measuring digital competence in family childcare settings.
The development and psychometric validation of the scale adhered to an established guideline to ensure scientific rigor. The first three phases were dedicated to item development and refinement. The utilization of the European Commission's Digital Competence Framework provided clarity on the content and outcomes to be measured by the PDCS. An item pool of 25 items was generated, covering the areas of Information Retrieval and Evaluation (four items), Communication and Collaboration (five items), Digital Content Creation (three items), DS (five items), and Problem Solving (eight items). Badr A. Alharbi developed the Parents’ Digital Skills Scale based on the results of previous studies. The scale included eight theoretical dimensions (Technological skills, Personal security skills, Critical skills, Hardware locking skill, Information skills, Communication skills, Knowledge navigation, and Electronic social skills) and was empirically verified to reach three dimensions. It focused on assessing specific digital skills essential in the context of the COVID-19 pandemic (e.g. I can control the opening or closing of geolocation in social media). 18 In contrast, the PDCS developed in our study takes a broader approach, focusing on parents’ competence in using digital technology for childcare beyond pandemic-specific contexts. By incorporating dimensions such as DS and Information Retrieval and Evaluation, the PDCS aims to help parents access reliable health information and adopt informed practices in childcare. This health-focused perspective highlights the potential significance of parental digital competence in promoting child well-being, particularly in the evolving digital health landscape.
Phase 4 assessed the psychometric properties of the 23-item PDCS. The EFA yielded a three-factor structure with a cumulative variance contribution rate of 80.499%. Factor 1, Digital Methods Application, consisted of items reflecting the use of digital technologies or resources to create digital content, address childcare issues, and engage in online communication and collaboration. This factor assessed parental proficiency in leveraging digital technology for a diverse range of purposes (Sample item: I can use digital resources to develop parenting strategies). Compared to the five dimensions defined and adapted in Phase 1 of the study, it included all items from the dimensions of Content Creation (items 5–7), Problem Solving (items 8 and 10–14), and Communication and Collaboration (items 16–20). This may be due to the interconnected nature of the ability to create digital content, address childcare challenges, and communicate online. 49 Factors 2 and 3 were DS (Sample item: I can prevent and address online risk behaviors) and IRE, respectively, aligning with the previously defined and adapted dimensions in Phase 1. In the Information Retrieval and Evaluation dimension, items 1 (I can search for information on the Internet) and 2 (I can express information needs using appropriate search query) reflected parents’ competence in retrieving child-related information. Items 3 and 4 measured their comprehension and critical evaluation of the information obtained. The CFA results further validated the adoption of a second-order three-factor model, allowing the PDCS to be interpreted as a comprehensive construct with three dimensions that can be summed into a total score, representing overall parental digital competence. Several measures of digital proficiency/literacy/attitude designed for general use, such as the Computer Proficiency Questionnaire, 50 the Adapted Technology Acceptance Model, 51 and the Attitude Toward Technologies Questionnaire 52 also encompassed domains related to digital communication, internet usage, and the application of digital technology. However, these existing measures rarely address aspects of digital security in depth. Choy et al. 26 highlighted the importance of digital literacy in healthcare, noting that parents’ understanding of digital security directly impacts their ability to safeguard their children's health information and navigate online health resources. This emphasized that digital security is not merely a technical skill but a necessary aspect of digital competence that influences health outcomes for children. 53 This alignment with our findings underscores the necessity of integrating digital security and health-related information skills into comprehensive parental support programs.
The study found that parents who were well-educated, had higher monthly incomes, lived in urban areas, worked in state organs, enterprises, or institutions, and reported their children's health as very good, achieved higher scores on the PDCS. This was consistent with previous research showing that parents’ digital skills varied across different social strata. 18 Parents with higher education, higher monthly income and living in urban areas often had better access to technology and resources that facilitated digital engagement. Additionally, well-educated parents were more likely to develop strong learning skills, including critical thinking and problem-solving, which were crucial for navigating and understanding new technologies. 54 For those parents who worked in state organs, enterprises or institutions, the nature of their work required them to be trained in digital skills, leading to continuous skill enhancement to meet job demands. Their familiarity with digital skills enabled them to gain experience and find new ways to solve problems more realistically and wisely. As a result, they may have increased access to health knowledge and promote child health by applying it to life. 32 These findings underscore that socioeconomic factors play a pivotal role in shaping parental digital competence. Understanding these disparities is crucial for designing targeted interventions and policies aimed at bridging the digital divide. Such interventions should include, but not be limited to, subsidized internet access and devices for low-income families, culturally relevant digital competence training programs offered in multiple languages and formats, and community-based digital inclusion initiatives that provide ongoing support and mentorship. These efforts are essential to ensure that vulnerable parental groups receive the support needed to enhance their digital competence for better childcare practices and overall family well-being.
Implications
Unlike general digital competence scales or eHealth literacy questionnaires, the PDCS appears to address a critical gap by focusing specifically on the digital competencies parents need to support their children's health and well-being. It may extend beyond the pandemic-specific focus of some recent tools, offering potential applicability to the broader, ongoing digital needs of parents. Rooted in the comprehensive DigComp 2.2 framework and uniquely adapted to the childcare context, the PDCS offers a more targeted and nuanced assessment. Its empirically validated three-dimensional structure provides useful insights for designing focused interventions. Low scores on Digital Methods Application may indicate a need for training on how to use digital tools for childcare-related tasks. The DS dimension could highlight the importance of educating parents about protecting children's online privacy and fostering healthy digital habits. Additionally, the PDCS was developed and validated with a sample of parents and caregivers, which enhances its relevance and psychometric suitability for this population. It represents a purpose-built tool that could serve as a valuable measure for assessing parental digital competence in the context of childcare.
Limitations
Despite the results of the PDCS being satisfactory, the study has several limitations. Firstly, family caregivers in this study were recruited exclusively in Northwest China. While digital technologies are widely used in this region, specific cultural and social characteristics may continue to influence how parents engage with, interpret, and apply digital health information. Longstanding traditions of information sharing within families and local communities might lead some parents to prioritize digital content from trusted local sources, or to integrate online advice with input from elders and community members. Moreover, collective social values could shape attitudes toward privacy and information sharing, such that parents may feel more comfortable exchanging information within familiar digital groups rather than on broader public platforms. These contextual factors may affect not only actual digital competence, but also parents’ responses to items on the PDCS. Therefore, caution is warranted when generalizing these findings to regions with different cultural, social, or economic backgrounds, and further research to validate and adapt the scale in diverse settings is recommended. Secondly, as a self-reporting instrument, the PDCS is susceptible to biases such as social desirability or inaccurate self-perception, which might affect the reliability of the results. Thirdly, criterion validity remains undetermined due to the lack of a definitive gold standard. Future research should prioritize long-term, multicenter studies to further validate the applicability of PDCS across diverse settings and to examine how its relevance and utility evolve over time. Additionally, future research could incorporate complementary objective measures, such as task-based assessments, to provide a more balanced evaluation of parental digital competence.
Conclusions
In conclusion, this four-phase study presents the development and validation of the PDCS, a novel 23-item instrument designed to assess parental digital competence in the context of childcare. The PDCS demonstrated robust psychometric properties, including high internal consistency, split-half and test–retest reliability, as well as strong content, construct, and discriminant validity. The three dimensions of DMA, DS, and IRE appear to capture essential aspects of parental digital engagement effectively. Theoretically, this work contributes to the emerging understanding of parental digital competence as a potentially significant factor influencing parenting practices and, indirectly, child health and well-being. Practically, the PDCS offers a valuable tool for researchers and practitioners to identify gaps in parental digital skills and evaluate the effectiveness of targeted interventions. This is important for identifying parental needs and tailoring support in healthcare settings. From a policy perspective, the findings highlight the potential of digital competence enhancement initiatives to become a valuable asset for parenting and child health. However, future research should prioritize long-term, multicenter studies to further validate the applicability of the PDCS across diverse cultural and demographic contexts and to examine its sensitivity to changes over time.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076251353319 - Supplemental material for A novel digital competence assessment tool for parents: Development and validation study
Supplemental material, sj-docx-1-dhj-10.1177_20552076251353319 for A novel digital competence assessment tool for parents: Development and validation study by Yitong Jia, Bojun Xu, Yuxuan Li, Xinqi Zhuang, Jianzhong Zhang and Yin-Ping Zhang in DIGITAL HEALTH
Footnotes
Acknowledgements
The authors thank all participants who voluntarily contributed to this study.
Ethical considerations
This research complies with the Declaration of Helsinki. The studies involving human participants were reviewed and approved by the Ethics Committees of Xi’an Jiaotong University (No. 2021-1511). Participants were engaged in and contributed to the validation of the Parental Digital Competence Scale in this study. Written informed consents were obtained from all participants.
Author contributions
Yitong Jia: investigation, formal analysis, and writing-original draft; Bojun Xu: writing—review and editing, and methodology; Yuxuan Li: conceptualization, methodology, and investigation; Xinqi Zhaung: investigation and formal analysis; Jianzhong Zhang: investigation; Yin-Ping Zhang: conceptualization and methodology. All authors reviewed and edited the draft of the manuscript. All authors read and approved the final manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Xi’an Jiaotong University Fund (Grant No. 20231296).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.