
Abstract
Background
Children's mental health issues are widespread in the United Kingdom, yet access to traditional services remains limited. Digital mental health interventions (DMHIs) offer a scalable alternative by reducing barriers such as cost, stigma, and location. However, most DMHIs target either children or parents individually, overlooking the potential of combined approaches.
Objective
This review assessed the effectiveness of DMHIs that include both parent- and child-delivered components for children aged 12 and under. The review also examined user experiences and compared DMHIs with traditional mental health support services.
Methods
A systematic review was conducted following PRISMA guidelines, searching six electronic databases. Studies were included if they evaluated DMHIs involving both children and parents/guardians, focused on mental health outcomes, and were peer-reviewed. Data extraction and risk-of-bias assessments were performed independently by reviewers.
Results
Of 3703 screened studies, three randomised controlled trials (n = 630) met inclusion criteria. These showed improvements in child anxiety, social competence, and parental nurturing behaviours. Parents reported positive engagement, citing flexibility and ease of use. However, therapists raised concerns about long-term implementation. Due to study heterogeneity and small sample sizes, a meta-analysis was not feasible; a narrative synthesis was conducted.
Conclusions
DMHIs that incorporate both parent and child components are comparatively rare but show promise as a valid means of enhancing child and parent well-being. However, further research is needed to refine these interventions, address barriers to engagement, and optimise their broader application, particularly in community settings, to help reduce the pressure on clinical services.
Keywords
Introduction
There is a high prevalence of children experiencing mental health difficulties, with 20.3% of children aged between 8 and 16 years old in the United Kingdom reported to have a probable mental health challenge. 1 Despite this, children and young people's access to mental health support has deteriorated significantly since 2020/21.2–5 More than a quarter of a million (270,300) children and young people in the United Kingdom in 2024 are reported to be still waiting for mental health support after being referred to Children and Young People's Mental Health Services (CYPMHS) in 2022–2023. 6 Early intervention during childhood is crucial to prevent emotional issues from worsening and becoming entrenched and disabling, possibly perpetuating into adulthood.7–9 Therefore, timely support is essential for long-term well-being. 10
Digital mental health interventions (DMHIs) offer an accessible alternative to traditional face-to-face therapy and have emerged as a significant innovation in mental health care, particularly over the past two decades. Within CYPMHS, face-to-face psychological therapies have historically been the primary mode of treatment, often delivered alongside pharmacological interventions for more severe presentations. The integration of DMHIs into mental health care began gaining traction in the last decade, with a growing body of evidence supporting their efficacy in improving mental health outcomes, such as symptoms of anxiety, depression, and stress, among children who experience mild to moderate symptoms.11–18
Such interventions have also been shown to successfully overcome barriers to treatment, including cost, geographical limitations, and the stigma often associated with seeking mental health care.12,14,17,19–21 However, it is important to note that DMHIs are not intended to replace face-to-face treatment for all service users.22–24 Rather, they can offer a valuable, scalable option that can complement existing care pathways or for individuals who may not require intensive intervention.22,23
Much of the existing research on DMHIs has focused on clinically diagnosed populations25–27 and there remains a significant gap in understanding their potential for children who experience mental health challenges but do not meet the criteria for a clinical diagnosis or formal support (e.g., CYPMHS).28,29 Despite evidence that subclinical symptoms can cause substantial distress and impairment, these children are frequently overlooked in both research and service provision.30,31 To address this, the current review focuses solely on studies that evaluate interventions without requiring a mental health diagnosis for participant inclusion.
Research on DMHIs specifically designed for children under 12 is also notably limited, which is surprising given approximately 50% of mental health challenges have their onset before the age of 14, 32 with one in three diagnosed mental health difficulties (including depression, anxiety, and behavioural disorders) emerging before this age. 33 Previous studies indicate that only a small proportion of existing literature focuses DMHIs on younger children aged 12 and below,34,35 leading to a lack of high-quality evidence available for this age group. To address this gap, the current review exclusively focuses on studies developed for children aged 12 or under and their families, addressing the need for targeted interventions in this critical developmental period.
DMHIs vary widely in their delivery formats and may include components aimed at parents exclusively (e.g., psychoeducation), or children exclusively (e.g., games played by the child). For the purposes of the current review, these exclusive modes of delivery will be referred to as ‘parent-delivered components’ and ‘child-delivered components’, defined as components of a DMHI completed by the child separated from the parent/guardian (and vice versa).22,36
DMHIs that provide only parent-delivered components function under the premise that parenting is a critical determinant of children's social, emotional, and behavioural development37–40 and that by equipping parents/guardians with the necessary knowledge and skills, they can subsequently apply these strategies at home with their children.39,41–43 This approach has been shown to promote improvements to the psychological well-being of both parties.12,37,44–48 On the other hand, DMHIs comprised solely of child-delivered components typically provide psychoeducational content in an age-appropriate format, including gamified mental health tools and interactive storytelling, designed to engage children and improve their mental health and well-being15,16,21
It is noteworthy that the majority of DMHIs have primarily focused on delivering treatment solely to either parents/guardians or children, rather than incorporating distinctive components aimed at each party.12,49 This singular approach may overlook the benefits of a more collaborative model that includes a bi-directional direct child and parent involvement.49–51 For instance, family systemic therapy posits that disturbances within one family member affect the entire family unit. While this form of therapy considers the broader contexts surrounding the child, including schools, peer networks, and other service systems, this paper focuses specifically on the role of the family, given its strong influence on child mental health outcomes. 52 As such, addressing issues at the familial level is argued to be essential given that children are wholly reliant and embedded in their family environment.11,32–37 Furthermore, the systemic approach fosters regular practice, communication, and mutual motivation between the child and parent/guardian, increasing the chances that the positive effects of the intervention will be integrated into daily routines and maintained long term.53,54,55 Moreover, this collaborative approach may also help address the common challenges of low adherence and high dropout rates frequently encountered in DMHIs, as a systemic approach promotes shared responsibility and engagement throughout the intervention process.12,15,54–57
Despite the well-known benefits of combining child and parent engagement, current interventions are primarily limited to traditional face-to-face sessions or online therapy that relies on therapist support.58–66 Self-guided, web-based DMHIs that incorporate both parent and child components, delivered via internet or mobile applications without therapist involvement, appear to be limited in existing literature67,68 and further research is necessary to explore and validate this approach.15,17,42,43,49,69 For instance, a recent study 70 revealed that both children and parents/guardians found a DMHI developed to reduce negative over-reactions to making mistakes (a risk factor for anxiety) in children between 5 and 7 years old, which provided independently delivered child and parent modules to be largely acceptable and appropriate. However, the efficacy of this intervention on mental health outcomes was not examined, and a randomised controlled trial (RCT) of an elaborated version of the programme is currently underway. The originality of this current review stems from its exclusive focus on DMHIs that incorporate components for both parents/guardians and children.
The objectives of the current review were to: (a) describe the current landscape of people's attitudes, beliefs, and experiences of digital health interventions as tools to support the mental health and well-being of children and their parents; (b) determine the efficacy of digital health interventions as tools to support the mental health and well-being of children and their parents; and (c) compare the efficacy of digital health interventions versus formal support channels (e.g., CYPMHS and NHS services).
Methods
Protocol and registration
This systematic review was conducted and reported in accordance with the most recent Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. 71 The review protocol was pre-registered in the Prospective Register of Systematic Reviews (PROSPERO), under identification number CRD42024568152.
Inclusion and exclusion criteria
Studies were included if they met the following criteria: (1) evaluated a DMHI delivered directly to parents and guardians and their children aged 12 years old or under, (2) assessed outcomes for both children and parents/guardians, (3) peer-reviewed, (4) original empirical data, and (5) published in English. Unpublished studies, dissertations, and grey literature were not included.
Studies were excluded if they (1) did not report on a mental health intervention, (2) did not have a full text available on any of the electronic databases detailed below, (3) were published prior to 2014, or (4) included participants on the basis of a clinical diagnosis (e.g., depression or anxiety). The rationale for excluding studies published prior to 2014 is that the use of DMHIs became more widespread and developed in the past decade.
Search strategy
Systematic searches of the following electronic databases were conducted from May 2024 to July 2024: Clinicaltrials.gov, ProQuest, Cochrane Library, PubMed, Scopus, and Web of Science. Search terms included (1) ‘Digital health interventions + young people + children + families’, (2) ‘Digital mental health interventions + young people + children + families’, (3) ‘Online mental health interventions + young people + children + families’, (4) ‘Teletherapy + young people + children + families’, (5) ‘Mobile phone application intervention + young people + children + families’, (6) ‘Self-help + young people + children + families’, (7) ‘Internet delivered intervention for children and parents’, (8) ‘Internet delivered intervention for children and families’, (9) ‘Online intervention + child + parent + outcomes’, 1 AND 5, 1 AND 7. Study screening was conducted using the Covidence software. Of the 7093 records identified, 3390 (47.79%) were duplicates. Initially, the titles of the 3703 remaining records were screened for relevancy by one reviewer (JC), which led to the elimination of 3592 (97%) of the 3702 records. The remaining 111 records were then reviewed by two authors (DF and PR) who independently screened the titles and abstracts for potential eligibility. Any disagreements were then discussed until a consensus was reached. This discussion led to 26 papers being eliminated (for reasons see PRISMA flowchart), leaving 85 papers for a full-text screen. Of these 85 papers, 82 were excluded (for reasons please see PRISMA), and 3 papers were included in the review. The intraclass correlation coefficient (ICC) was calculated to assess the reliability of ratings provided by three independent reviewers. An ICC of 0.78 (95% CI [0.42, 0.65]) was found, indicating good reliability. 72 Figure 1 presents the PRISMA flow diagram.

PRISMA flow diagram 71 illustrating the systematic search and study selection process.
Data extraction
Extraction of data from the full-text reports was conducted independently by one reviewer (JC). Data was extracted for: authors, date, study location, sample size, mean age, gender, intervention details, control condition details, length of intervention, outcome measures, and main findings.
Risk of bias assessment
Risk of bias was assessed independently by two reviewers (JC and DF), using the Cochrane risk-of-bias tool for randomised trials (Risk of Bias 2 [RoB 2]), 73 which comprises five domains: (1) bias related to the randomisation process; (2) bias related to deviations from the intended interventions; (3) bias related to missing outcome data; (4) bias related to measurement of the outcome; and (5) bias related to the selection of the reported result. Bias is scored using three different categories: ‘low risk’, ‘some concerns’, and ‘high risk’. Each domain was evaluated, and the overall bias was determined according to the five domain scores. A study was considered to have an overall ‘high risk of bias’ if it received a ‘high risk of bias’ rating in at least one domain. 73 Disagreements between the review authors over the risk of bias in particular studies were resolved by discussion.
Results
Study characteristics
Due to the heterogeneity and the limited number of studies included in the review, meta-analysis was not possible. The findings of these studies were synthesised descriptively. Three studies (n = 630 participants) were included in this review. The year of publication ranged from 2021 to 2024. Two studeis74,75 were conducted in the United Kingdom, and one study 76 was conducted in Portugal. The mean age of child participants ranged from 4.50 (SD not reported) to 9.20 years (SD = 1.79). The mean age of adult participants was reported to range from 37.25 (SD = 3.70) 76 to 38.64 (SD = 5.80), 75 but this was not reported by one study. 74 The majority of participants (both children and adults) were female in two studies.75,76 However, this was not the case for a child sample in one study. 74 This study 74 also did not report the proportion of female adult participants. All studies74–76 used web-based platforms as the format to deliver the intervention. The duration of the interventions ranged from 7 to 8 weeks. Interventions were designed to address a range of outcomes, including the child's level of anxiety,75,76 child social adjustment/competence 76 and parental responses to the behaviour of their child. 74 The included studies are described in Table 1.
Study and participant characteristics for each study.

Note: NR = not reported.
Efficacy outcomes
The measures used to assess child and parent-related well-being outcomes at post-intervention/follow-ups varied between studies. Two studies75,76 focused on anxiety in children by measuring parent's perceptions of it. The first study 75 assessed this using the Child Anxiety Impact Scale–parent report (CAIS-P) to assess parents’ perceptions of the impact of their child's anxiety on school, social and home contexts; the Revised Child Anxiety and Depression Scale–parent-reported child anxiety symptoms (RCADS-P) to assess parent's perceptions of their child's anxiety symptoms; the Outcome Rating Scale to assess parent's perceptions of any changes to their child's emotional functioning as a result of the intervention; and the Strengths and Difficulties Questionnaire–parent report (SDQ-P), which assesses the parent's perceptions of their child's strengths and difficulties across five dimensions (emotional problems, conduct problems, hyperactivity, peer problems, and prosocial behaviour). The second study 76 assessed children's behaviours using the Behavioural Inhibition Questionnaire (BIQ) by measuring the parent's perceptions of their child's inhibited behaviour in a range of contexts (e.g., with unfamiliar adults, peers, situations, etc.); the Social Competence and Behaviour Evaluation Scale–Parent version (SCBE-30) to assess parents’ perceptions of their child's prosocial behaviours, communication skills, and self-control; and the Preschool Anxiety Scale–parent version (PAS) which measures the parent's perceptions regarding the frequency of anxiety symptoms in their children. Only one of these studies 75 examined child anxiety via measures that were required to be completed by the child directly. These were via the child-reported anxiety interference (CAIS-C), used to assess the child's perception of how their anxiety impacts their daily functioning in school, social and home contexts, as well as the Revised Child Anxiety and Depression Scale (RCADS-C), which assesses the child's perceptions of their anxiety symptoms.
Two studies74,76 investigated parent-related outcomes. One study 74 assessed parents’ discipline responses to children's behaviours via the Parenting Scale (PS). The PS assesses parents’ laxness (i.e., lenient responses to a situation), over-reactivity (i.e., strict responses to a situation), hostility (i.e., aggressive responses to a situation), and overall parental responses. The other study 76 administered the child-rearing practice report questionnaire (CRPR-Q), which assesses the values, attitudes, and goals of parents about child-rearing.
Psychological models used
One study 75 utilised a cognitive behavioural therapy (CBT) framework in a parent-led, therapist-supported programme. Another study 76 applied a multimodal approach combining Parent–Child Interaction Therapy (PCIT) and Social Skills Facilitated Play. The remaining study 74 drew on principles from social learning theory and self-determination theory to guide the design of its digital content and resources.
Adherence outcomes
To measure adherence, one study 76 asked parents to rate how much prescribed homework they did on a scale from ‘none’ to ‘all’ to indicate adherence. The other two studies74,75 did not report any adherence outcomes.
Modalities of online mental health interventions
Two studies74,75 used web-based platforms to deliver the intervention. One study 75 used a website consisting of seven modules, each taking approximately 30 minutes to complete. Parents were required to complete questionnaires at the start of each module, followed by content delivery and optional quizzes and feedback. The modules were released weekly and supplemented by 20-minute weekly telephone or video sessions between the parent and therapist. The child-delivered component of the intervention was an optional game app called ‘Monster's Journey: Facing Fears’, which participants could access on smartphones or tablets. The other study 74 used a website to provide two animated episodes, videos designed for children aged 2–7, and activities that could be downloaded by parents to complete with their children. Schools were also provided with lesson plans and additional parenting resources. The child-delivered component of the intervention was the animated episodes developed for children. One study 76 adapted its original face-to-face intervention to an online format using a video conferencing platform. The sessions were conducted via Zoom, where families interacted with therapists. The child-delivered component of the intervention was the animation videos.
Treatment duration and intensity
The length of the interventions ranged from 7 to 8 weeks. One study's 76 intervention spanned 8 weeks, with families and therapists conducting sessions via Zoom. Each family participated in eight sessions, and parents were assigned home exercises between sessions. One study 75 released modules weekly over the course of 7 weeks. The modules are supported by weekly 20-minute telephone/video call sessions between the parent and a therapist and a review session 4 weeks after the final treatment session. One study 74 gave parents access to the website and administered measures at 8 weeks but did not specify that access to this website was constrained by any time limits.
Quality of evidence
The risk of bias was assessed based on the Cochrane RoB 2 tool, 77 two74,76 of the three included studies were considered at high risk of bias; the remaining study 75 showed low bias. The results of the risk of bias assessment are shown in Figure 2.
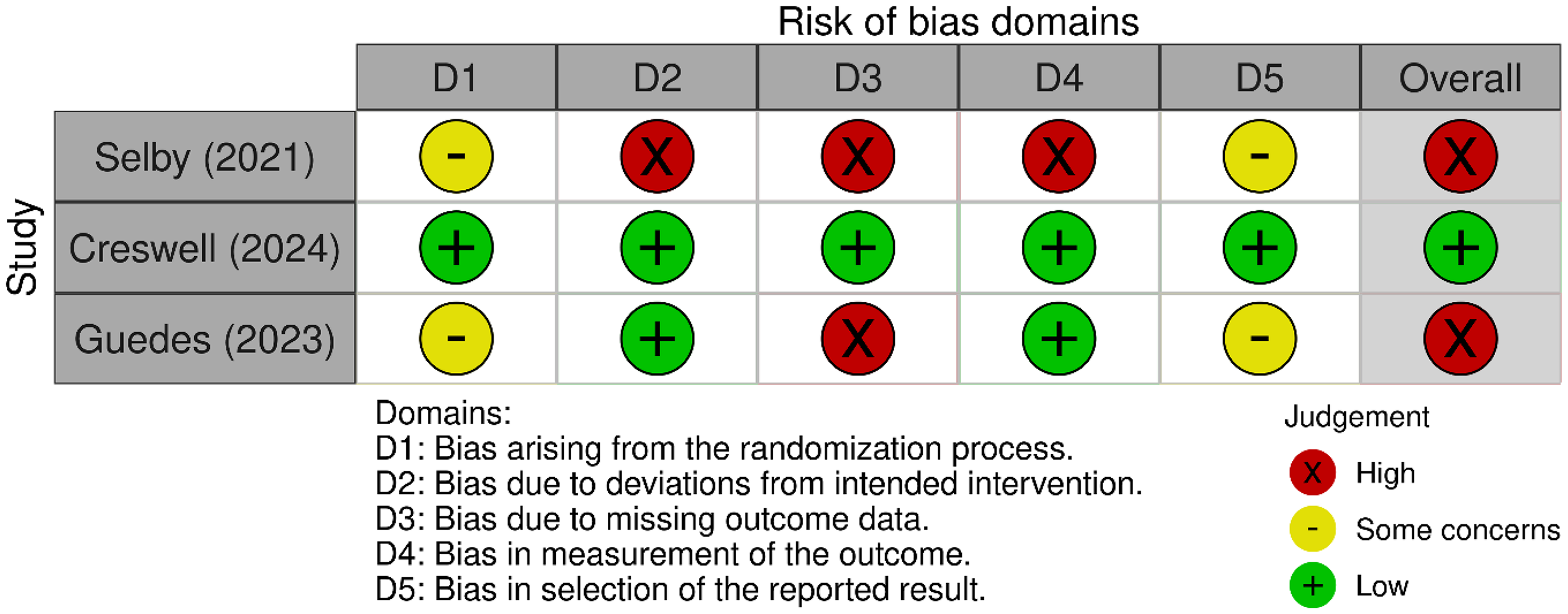
Risk of bias classification for each study included in this systematic review, assessed across five domains using the Cochrane Risk of Bias 2 (RoB 2) tool. 73 Each cell indicates the level of bias for a specific domain: D1 (randomisation process), D2 (deviations from intended interventions), D3 (missing outcome data), D4 (measurement of the outcome), and D5 (selection of the reported result). Judgements are colour-coded as follows: green ‘+’ for low risk, yellow ‘−’ for some concerns, and red ‘X’ for high risk. The final column presents the overall risk of bias for each study.
Attitudes, beliefs, and experiences of digital health interventions for mental health
Qualitative interviews were used in two studies74,75 to investigate people's experiences and perceptions of an intervention. Parents and children were interviewed in one study, 74 and parents and therapists were interviewed in another study. 75 In one study, 75 parents and therapists were invited to participate in interviews upon reaching the 14-week point following randomisation. The topics covered in the interview included what participants found helpful and unhelpful about the intervention, potential improvements, the involvement of others in treatment, and how things had been since treatment ended. The authors reported that parents who were initially sceptical about the programme recognised its benefits upon engagement and appreciated its user-friendly design and flexibility that easily allowed for integration into daily life. Some parents reported that they would have preferred their child to take part in the sessions as well. Having to manage other significant stressors in life was cited as a barrier to engaging with the intervention. Therapists were reportedly satisfied with the intervention as a whole and noted that it reduced their administrative burden through online content delivery and monitoring of parent engagement. However, they also highlighted limitations, noting that the programme might be less effective for older children with severe anxiety or those unable to articulate their concerns, as well as instances where parents needed more support to engage with the intervention fully. In the other study, 74 interviews were conducted pre- and post-intervention with parents and children. The interviews explored details from the children and parents about their current emotional well-being and coping strategies rather than directly gathering feedback on the intervention itself (e.g., likes, dislikes, or suggestions for improvement). Of these two studies, one study 75 also administered the Credibility and Expectation of Improvement Scale to parents prior to starting the intervention and week 14 after randomisation to assess how logical the treatment was, confidence in its success at reducing symptoms, and the parents’ likelihood to recommend the therapy to a friend with similar symptoms. Therapists were also required to complete this measure at week 14 after randomisation. Prior to the intervention, the authors reported there were no significant differences across the two arms in parents’ perceptions of how logical the treatment seemed and how confident they were in it, but those in the intervention condition were reportedly more certain that the intervention would be successful compared to treatment as usual (TAU). Post-intervention, there were no reported differences in perceptions of treatment logic, confidence, or expected success between parents across the two arms. How therapists responded to the scale was not reported, with the only information available being that they felt more comfortable in delivering TAU compared to the intervention, and they felt that they were unlikely to use the intervention in the future.
One study 76 used a satisfaction questionnaire to assess the acceptability of the intervention. Parents were asked to complete this after the intervention. The questionnaire assessed: (1) the perceived appropriateness of the intervention sessions; (2) the satisfaction with post-intervention parenting outcomes (i.e., report of how much the participation in the intervention changed their parenting when their child is anxious and their satisfaction as a parent); (3) the satisfaction with post-intervention child outcomes (i.e., how satisfied they were with progress in their child's behaviours); and (4) parental overall satisfaction with the intervention programme and suggestions for improvements. The authors reported that for the purposes of the present study, only parental responses to the questions from the second and third parts of the questionnaire were examined. The authors reported that parents were satisfied with both child and parent post-intervention outcomes, and importantly, that this level of satisfaction was the same regardless of whether the intervention was delivered in person or online. As these were the only items assessed in this study, no direct feedback about the intervention itself was reported.
Efficacy of digital health interventions as tools to support the mental health and well-being of children and their parents
All studies reported on the success of the interventions on child and parent-related outcomes. One study 74 found significant improvements in parenting style (i.e., laxness, over-reactivity, hostility, and overall parental responses) in the intervention group.
One study 75 compared the digitally delivered, therapist-supported, parent-led CBT intervention with child mental health service TAU for child anxiety problems, with TAU primarily consisting of face-to-face CBT sessions. It was revealed that child anxiety and anxiety symptoms, as perceived by parents and children, were significantly reduced from pre- to post-intervention. Additionally, parents’ perceptions of any changes to their child's emotional functioning resulting from the intervention and their child's strengths and difficulties across five dimensions (emotional problems, conduct problems, hyperactivity, peer problems, and prosocial behaviour) were significantly improved by post-intervention. Notably, the digitally delivered intervention was found to be non-inferior to TAU, achieving comparable clinical outcomes while using significantly less therapist time, indicating its potential as a scalable and efficient alternative for treating child anxiety. Despite these findings, qualitative feedback from therapists indicated a preference for TAU methods and an unlikelihood that they would use the novel intervention in the future.
One study 76 reported that post-intervention, perceived child overall anxiety and social anxiety decreased significantly in the online intervention arm compared to the waiting-list condition. Additionally, child social competence improved across both conditions from pre- to post-intervention. Finally, parenting nurturance (i.e., parenting practices focusing on care, affection, and sharing feelings) increased in the online intervention arm, but decreased in the waiting list condition.
The findings from the qualitative interviews further support the effectiveness of the interventions. One study 74 reported that children had developed more creative ways of communicating their emotions and coping strategies compared to pre-intervention. Parents reportedly felt more confident in their parenting and ability to respond to their children's emotional development needs post-intervention. The other study 75 reported that parents had a heightened sense of self-efficacy and felt more equipped to support their child's emotional well-being. According to parents, this translated into improved familial relationships and increased confidence in their children.
Discussion
The present systematic review provides a synthesis of DMHIs that incorporates both ‘parent-delivered’ components and ‘child-delivered’ components. Three studies met the inclusion criteria, with only one demonstrating low bias. Overall, the findings across the three studies revealed improvements in both child- and parent-related outcomes. For children, there was a reduction in anxiety symptoms as perceived by both parents and children. 75 This finding is particularly noteworthy as it was the only study that assessed a child's mental health outcomes through both direct self-report by the child and indirect report by the parent. Improvements to children's emotional literacy were also highlighted, indicated by their ability to recall a broader range of emotions and coping strategies. 74 Finally, parents perceived there to be improvements in their child's social competence (i.e., pro-social behaviours). 76 For parents, self-reported improvements were observed for both nurturing behaviours 76 and parenting styles. 74 Specifically, parents reported increased greater care, affection, and emotional connection with their children 76 and confidence in responding to their children's emotional needs. 74 These findings underscore the potential of DMHIs using a combined approach in promoting children's emotional well-being, addressing mental, social, and emotional development while fostering healthier family dynamics and more supportive parenting.
The psychological models used within the interventions varied across the included studies. One study 75 utilised a CBT framework, delivered via a digitally augmented, parent-led programme with therapist support. Another study 76 applied a multimodal approach combining PCIT and Social Skills Facilitated Play, targeting both parenting behaviours and child social-emotional learning (SEL) skills. The third study 74 stated that principles from social learning theory and self-determination theory guided the design of its digital content and resources. While all three studies articulated their theoretical foundations, the degree to which these models were operationalised as structured therapeutic interventions varied. This variation limits the ability to draw firm conclusions about mechanisms of change and highlights the need for future interventions to clearly define and apply their theoretical underpinnings.
Importantly, one study 75 found no significant difference in clinical outcomes between a digitally delivered, parent-led CBT programme and traditional face-to-face therapy, supporting the use of DMHIs as credible alternatives to in-person care. Moreover, such interventions offer unique advantages, including reducing therapist time, associated costs for families, and broadening access to mental health services, especially for families in underserved areas or those unable to attend in-person sessions. These findings underscore the potential of DMHIs not only to deliver outcomes equivalent to conventional face-to-face therapy but also to enhance the scalability and accessibility of child mental health care. In addition to demonstrating efficacy, the DMHIs reviewed were generally perceived as acceptable by both parents and therapists. Parents valued the flexibility of the programmes, which facilitated integration into daily routines and helped overcome logistical barriers such as time constraints and geographical limitations. Therapists also cited several advantages, including reduced administrative burden, suggesting potential improvements in service efficiency.
Despite these strengths, barriers to engagement remain. For instance, some parents mentioned that managing other stressors in life hindered their ability to fully engage with the intervention. This suggests that while the modality itself may be acceptable, external factors (e.g., family stress, financial burdens, or lack of support systems) still influence the feasibility and effectiveness of the intervention. Importantly, while therapists expressed satisfaction with the intervention, a subset reported hesitancy in adopting DMHIs in future practice. This preference for in-person delivery was particularly evident among therapists without prior training in digital modalities or those in the early stages of their careers. These findings align with research indicating that some clinicians feel less confident delivering online treatments and often perceive in-person care as offering greater therapeutic depth and relational connection.78–80 This highlights a broader implementation challenge where therapists may need more than technical guidance when using DMHIs. Addressing this barrier is essential for improving their confidence and competence in digital delivery and increasing the likelihood that such interventions will be integrated into clinical practice. For instance, future implementation efforts may benefit from blended training models that combine technical guidance with experiential learning, such as role-playing, supervised practice, and feedback sessions. Importantly, there also needs to be ongoing support, including regular supervision, peer consultation, and opportunities for reflective practice, to help therapists consolidate skills and maintain confidence in digital delivery over time. With appropriate training and support, digital interventions can become not only viable but also scalable and sustainable within real-world mental health systems.
In addition to therapist-related barriers, it is important to consider the potential challenges faced by marginalised communities in accessing DMHIs. 81 While digital interventions offer flexibility and scalability, these benefits may not be equitably distributed.82–84 Families from lower socioeconomic backgrounds or those with limited digital literacy and access to reliable internet or devices may struggle to engage with such programmes.83,84 These disparities risk exacerbating existing inequalities in mental health care access. 83 Future research and implementation strategies should therefore prioritise digital inclusion by exploring low-tech delivery options, providing digital literacy support, and engaging communities in co-design to ensure cultural relevance and usability.83,84 Addressing these structural barriers is critical to ensuring that DMHIs are not only effective but also equitable and accessible to all families.
The current review also highlights an important gap in the literature regarding a lack of DMHIs using a combined approach whereby both parent and child components are delivered simultaneously. While interventions targeting either group individually have shown promise, the combined approach remains underexplored. This gap is crucial to address, as mental health challenges often affect the entire family system. However, implementing DMHIs that engage both parents and children presents distinct challenges, particularly in terms of scheduling and time constraints. These logistical issues are especially pronounced in studies involving children with clinical mental health diagnoses, where families often face additional demands.36,75,81 Such studies offer valuable insights into these complexities, suggesting that while dual-component approaches are feasible, they require careful attention to engagement, timing, and tailoring for both participants.36,75,85
In addition to the gaps identified in the wider literature, it is important to acknowledge a methodological limitation within the current review. While our search strategy was designed to be comprehensive and included a wide range of keywords related to DMHIs, we did not explicitly include terms such as eHealth and mHealth. These terms are commonly used in the literature to describe digital health technologies and may have captured additional relevant studies. Their omission may have limited the breadth of included studies, under conditions in which eHealth and mHealth were mentioned, but the specific mode (e.g., teletherapy, digital intervention, etc.) were not. Future systematic reviews may benefit from incorporating these terms to ensure broader coverage of digital intervention modalities.
A further limitation relates to the number of studies included in the review. The inclusion of only three studies significantly constrains the scope and generalisability of the findings and precludes meta-analysis. This narrow yield reflects a gap in the literature in that there is a notable lack of available digital DMHIs that include both parent and child components, specifically developed for children under the age of 12 who require mental health support but do not meet criteria for a clinical diagnosis. While this may appear to be a highly specific inclusion criterion, it was intentionally designed to capture a growing interest in early intervention and preventative approaches for children who fall below diagnostic thresholds yet experience significant emotional challenges. The limited number of studies reduces the strength of the evidence base and underscores the need for further high-quality research. Future studies should aim to develop and evaluate DMHIs tailored to this population, particularly those that integrate both parent and child components. Expanding the availability of such interventions could help address unmet needs in early support and prevention and contribute to a more robust evidence base for non-clinical populations.
Alongside this methodological consideration, it is also important to reflect on the quality of the existing evidence base. Although the existing literature carries a high risk of bias, this review emphasises the potential benefits of a collaborative model that includes both parent and child components. Further research into the development and implementation of such DMHIs is therefore warranted.
Conclusion
The current review highlights the potential of DMHIs that incorporate both parent and child components to improve outcomes for both children and parents. By engaging both parties, these interventions can help to improve emotional well-being, strengthen family dynamics, and deliver results comparable to traditional therapies for milder mental health challenges. Their flexibility and accessibility make them particularly valuable for families facing barriers to in-person care. However, the current evidence base is limited in both quantity and quality, and further research is needed to understand the long-term impacts, what factors influence engagement, and how to support integration into routine practice. Addressing these gaps will help ensure that such DMHIs will adequately meet the diverse needs of families.
Footnotes
Acknowledgements
All contributions to this review are fully reflected in the authorship and funding statements. No further acknowledgements are applicable.
Ethical considerations
There are no human participants in this article, and informed consent is not required.
Consent to participate
Not applicable.
Consent for publication
Not applicable.
Contributorship
JC conducted the literature search, selected and reviewed the articles, and wrote the manuscript. DF and PR assisted with reviewing the selected articles and provided comments and feedback on the review write-up. CA contributed by giving comments and feedback on the review write-up. The corresponding author attests that all listed authors meet authorship criteria and that no others meeting the criteria have been omitted.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work is supported by the NIHR i4i Connect programme awarded jointly to LSBU and Embers the Dragon Ltd. (funder grant number: NIHR204516). Embers the Dragon Ltd. administers the grant and subcontracts LSBU for the evaluation.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.